Open Access is an initiative that aims to make scientific research freely available to all. To date our community has made over 100 million downloads. It’s based on principles of collaboration, unobstructed discovery, and, most importantly, scientific progression. As PhD students, we found it difficult to access the research we needed, so we decided to create a new Open Access publisher that levels the playing field for scientists across the world. How? By making research easy to access, and puts the academic needs of the researchers before the business interests of publishers.
We are a community of more than 103,000 authors and editors from 3,291 institutions spanning 160 countries, including Nobel Prize winners and some of the world’s most-cited researchers. Publishing on IntechOpen allows authors to earn citations and find new collaborators, meaning more people see your work not only from your own field of study, but from other related fields too.
To purchase hard copies of this book, please contact the representative in India:
CBS Publishers & Distributors Pvt. Ltd.
www.cbspd.com
|
customercare@cbspd.com
Osteoporosis (OSP) decreases bone mass and affects millions of people; the diagnosis is often late. Considering the side effects of conventional treatments, search for natural therapies should be a constant. Among natural treatments, herbal medicines stand out with very promising results. One of the plants that has drawn a lot of attention to prevent OSP is Plinia cauliflora (PC) Kausel. The objective was to evaluate the effect of PC extract in the OSP prevention in ovariectomized rats. In total, 60 female Wistar rats were divided into six experimental groups: positive control, negative control, sham, and three groups to test different doses (37.5, 75, and 150 mg) of PC bark extract. Bone mineral density (BMD), bone mineral content (BMC), hormone dosage, and osteocalcin were evaluated. One of the regions evaluated was the legs, where prolonged treatment with extract of PC in 75 mg, had a gain of 1.4 times of BMC. The levels of osteocalcin were found to be high at the lowest dose (37.5 mg), increasing the BMC by 70%, and moderately increasing the levels of dehydroepiandrosterone, proving that the pathway that increases BMC is through osteocalcin. PC resulted in increased BMC related mainly to increased osteocalcin, at the lowest dose preserving the bone matrix.
*Address all correspondence to: dcboleta@prof.unipar.br
1. Introduction
Osteoporosis (OSP) is an ancient pathology, first observed in Egypt in 990 before Christ [1]. With the aging population in Brazil, the prevalence of osteoporosis has been increasing [2]. It causes more than 8.9 million fractures per year worldwide, without previous symptoms [3].
It is a systemic, progressive, and silent disease, with osteometabolic character [2]. Physiological processes occurs permanent bone remodeling throughout the patient’s life. This process is altered in osteoporosis due to an increase in resorption and reduction of bone formation, causing it to lose its structural integrity, due to the cortical bone being porous and thinner [4].
This structural loss is responsible for the most common sign in osteoporotic individuals, which are bone fractures caused even by low impact [5] most frequently in the spine, distal radius, and proximal femur. Hip fractures are the most severe bringing a mortality of 12–20%, and about 50% of survivors of the condition of proximal femur fracture are unable to have an independent life [6].
OSP is effectively diagnosed by bone densitometry. However, the sensitivity of the method is low for assessing fracture risk, so there is no indication for population screening in menopausal women [7]. Due to the high prevalence of secondary causes of osteoporosis, one of the main examples being post-menopausal osteoporosis, characterized by hypoestrogenism can directly influence the proliferation and differentiation of osteoblasts, leading to changes in the levels of bone remodeling markers [8]. Several bone remodeling markers, especially those synthesized by osteoblasts (such as osteocalcin), are clinically used as predictors of postmenopausal osteoporosis. Unlike other biochemical markers of bone metabolism, osteocalcin can increase in all conditions in which there is bone remodeling, such as during childhood, after bone fractures or after osteoporosis induced by estrogen deficiency [9].
Osteocalcin, is a protein that plays an important role in bone mineralization, originates from osteoblastic synthesis and is deposited in the bone or released into the circulation, where it correlates with histological measures of bone formation [10]. In addition, osteocalcin can activate monocyte differentiation, resulting in an increase in the number of active bone resorption cells and promoting osteoclastic differentiation [11].
It is recommended for all patients, before starting any treatment, a laboratory evaluation that includes complete blood count, calcium, phosphorus, alkaline phosphatase, thyroid function, serum 25 (OH) vitamin D, 24-hour calciuria, and osteocalcin, as well as radiography of the thoracic and lumbar spine and proximal femur [12], dehydroepiandrosterone (DHEA), estradiol, and testosterone.
In view of the multifactorial nature of OSP, it is necessary that professionals are willing to treat, evaluate, and consider all the factors involved. For example, lifestyle changes, such as reduced smoking, healthy eating, and physical exercise [13], are essential for a better prognosis.
In some cases, not only a change in lifestyle will be enough to control and/or prevent the development of the disease but the introduction of specific drugs becomes indispensable.
Regarding the drug therapy used for the treatment and prevention of OSP, there are several classes, with major side effects, such as breast cancer, ovarian cancer, endometrial cancer, muscle damage, and a higher incidence of thrombosis. Due to the severe adverse effects, there is a need to seek natural alternatives for the treatment and prevention of OSP.
The jabuticaba (Plinia cauliflora (PC) Kausel) is native to South America, more precisely to the mountainous region around Rio de Janeiro and Minas Gerais in Brazil; as well as around Santa Cruz, Bolivia; Asunción, Paraguay and Northeastern Argentina. The fruits when ripe are highly nutritious and are mainly consumed as fresh fruits, but are also processed to make juice, wine, candy, liquor, ice cream, jams, and jellies [14].
One of the main actions of this plant is its function as a natural antioxidant, due to the anthocyanins of the flavonoid group, which have the characteristic to inhibit the oxidation of free radicals, protect, and stimulate collagen-rich tissues [15].
Quercetin presents an antioxidant effect and is within the group of flavonoids [16]. This antioxidative function inhibits the reaction of free radicals in osteoblastic cells, thus allowing the formation of bone matrix.
In addition to having antioxidant effects, they also have effects on hormone regulation through binding to steroids. The synthetic isoflavone that belongs to ipriflavone, within the metabolism of flavonoids, increases and aids in the maintenance of bone density in postmenopausal women [17].
In view of the above, the aim of the present work was to evaluate the effect of different doses of the bark extract of P. cauliflora in the treatment and prevention of osteoporosis in rats.
In total, 90-day-old female Wistar rats weighing between 250 and 300 g were randomized and housed in plastic cages with environmental enrichment at 22°C ± 2°C under a 12 h/12 h light-dark cycle and 55% ± 10% humidity. The animals had access ad libitum to food and water. All experimental procedures were reviewed by the Research Ethics Committee of Paranaense University (Protocol 37086/2020), and conducted according to the National Institutes of Health Guide for the Care and Use of Laboratory Animals (NIH Publications No. 8023).
2.2 Experimental design
Sixty rats distributed in 6 groups of 10 animals were used. The rats were anesthetized intramuscularly with ketamine (80 mg/kg) and xylazine (10 mg/kg). Forty animals underwent bilateral ovariectomy (OVX) (OVX groups). For OVX, the skin and muscles were incised longitudinally and the ovaries were identified and extirpated. The suture of the muscle layer was performed com single # 4.0 catgut threads, and the skin was sutured with # 4.0 nylon (Ethicon-Johnson & Johnson, São José dos Campos, SP, Brazil). Ten animals were subjected to sham OVX to simulate surgical stress (sham group). After exposing the ovary, it was removed from the abdominal cavity and after this procedure, the muscle layer and skin were sutured as described above. After surgery, all animals received enrofloxacin (10 mg/kg, subcutaneous, single dose) and ibuprofen (15 mg/kg, oral, once a day for 3 days) for infectious prophylaxis and analgesia, respectively. The rats also received 2 mL of saline solution subcutaneously for hydration. The surgical wound was cleaned with iodine and hydrogen peroxide once a day until complete healing.
Thirty days after surgery, the animals were divided into six groups (n = 10/group). There was a sham-operated group (fake operated to simulate surgical stress) (sham) anda negative control (NC) (which did not undergo any surgical procedure). The remaining ovariectomized animals were randomly included in the groups: positive control (OVX), and treatment with Plinia cauliflora in different doses: OVX + PC1 (37.5 mg/kg), OVX + PC2 (75 mg/kg) and OVX + PC3 (150 mg/kg). All animals underwent initial bone densitometry, 30 days after the surgery. For the densitometry examination, the animals were sedated with an intraperitoneal injection of 5 mg/kg diazepam.
The animals in the positive control (OVX), negative control (NC), and sham groups received vehicle (filtered water) daily in a volume of 5 mL/kg. The animals in the other groups (treatment) received the following doses of Plinia cauliflora: 37.5, 75, and 150 mg/kg, administered by oral wash (GO) once daily for 45 days. The animals were weighed weekly for regular dose adjustments.
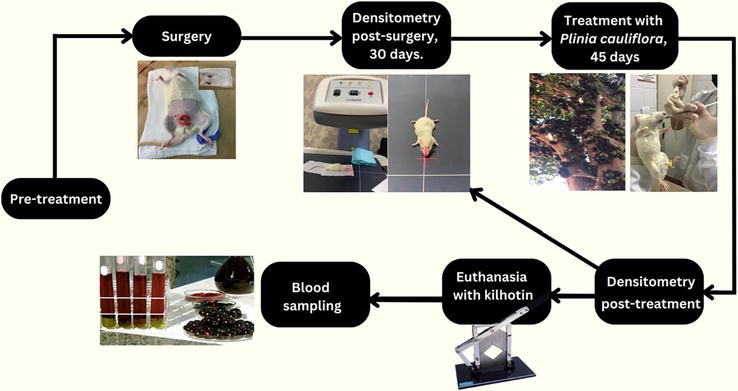
The sequence of the experimental protocol is shown in Figure 1.
Figure 1.
Sequence of the experimental design.
2.3 Drugs and solvents
Diazepam was obtained from Cristália (Itapira, SP, Brazil). All other reagents were obtained in analytical grade.
2.4 Obtaining the standardized extract of Plinia cauliflora
The aqueous extracts of P. cauliflora were obtained by infusion, using the fruit peel, as recommended by popular use [18] with minor modifications. The dried and ground plant extract (100 g) was submitted to the extraction process by infusion with 1 L of boiling water. The extraction was performed, for approximately 5 h, until the extraction medium reached room temperature. The solid residue (plant drug) was separated by filtration and the extract obtained was concentrated in a rotary evaporator to a volume of 200 mL.
The final product obtained was treated in a proportion of 1:3, that is, 600 mL of ethanol to 100 mL of the infusate so that the precipitation of proteins and polysaccharides occurs, secondary metabolites that arouse little interest in our area of studies. In this way, an ethanolic precipitate of the infuse (PEI) was obtained, which was discarded, and an ethanolic supernatant of the infuse of P. cauliflora (SEIPC). The SEIPC obtained was lyophilized and stored in a freezer (−20°C) until use.
2.5 Doses of the extract for the experimental set
The PC doses (37.5, 75, and 150 mg/kg) that were used in this study were calculated from the studies performed with atherosclerosis models by our research group with the same standardized extract [19].
2.6 Evaluation of serum levels of estradiol, progesterone, and DHEA
At the end of the experiments, the animals were euthanized by decapitation for total serum collection. Blood samples were collected in tubes containing ethylenediaminetetraacetic acid (EDTA) to obtain plasma. For analysis, serum was obtained by centrifugation (800 g, 10 minutes, 4) and stored at −20°C until analyzed. Estradiol and progesterone levels were determined by chemiluminescence immunoassay. DHEA levels were measured using an enzyme-linked immunosorbent assay. Serum osteocalcin levels were measured by electrochemiluminescence on an automated photomultiplier analyzer (PMT).
2.7 Bone mineral density measurements
Bone densitometry was performed using DXA (Lunar iDXA; General Electric, Boston, MA, USA) with software specially developed for small animals. Total body scanning was performed and total bone mineral density (g/cm2) and bone mineral content (g) were analyzed. This scan was performed at two different times during the experiment: (1) 30 days post-OVX and (2) 45 days post-PC. The reason that bone mineral density was assessed after 30 days post-OVX was due to the significant bone loss that is typically observed [20]. For DXA, animals were sedated intraperitoneally with 5 mg/kg diazepam.
2.8 Statistical analysis
Results were expressed as the mean ± standard error of the mean of n = 6 animals per group. Statistical analyses were performed using one-way analysis of variance followed by Dunnett’s test or Tukey’s test. Values of P < 0.05 were considered statistically significant. Graphs were prepared and statistical analyses were performed using Prism 5.0 software (GraphPad, San Diego, CA, USA).
3.1.1 Validation of an imaging model of osteoporosis induced by ovariectomy
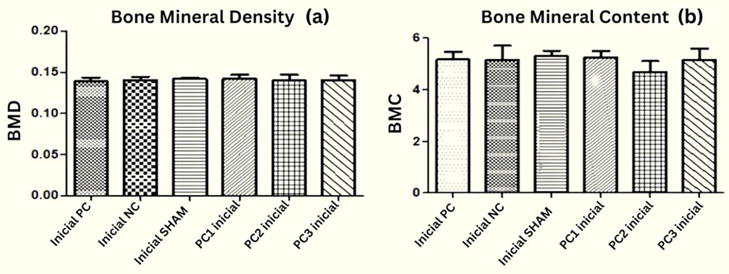
After 30 days of the ovariectomy procedure, the first measurement of total body composition was performed. When analyzed in general, considering all the body areas evaluated, a similarity was observed in the density and bone mineral content of all groups (Figure 2).
Figure 2.
Total bone mineral density (g/cm2) (a) and bone mineral content (g) (b) after 30 days of performing ovariectomy (*p < 0.05; **p < 0.01; ***p < 0.001). Using one-way ANOVA followed by t-test. OVX: ovariectomized; NC: negative control; sham: sham ovariectomized; OVX + PC1: extract 37.5 mg/kg, OVX + PC2: extract 75 mg/kg; OVX + PC3: extract 150 mg/kg).
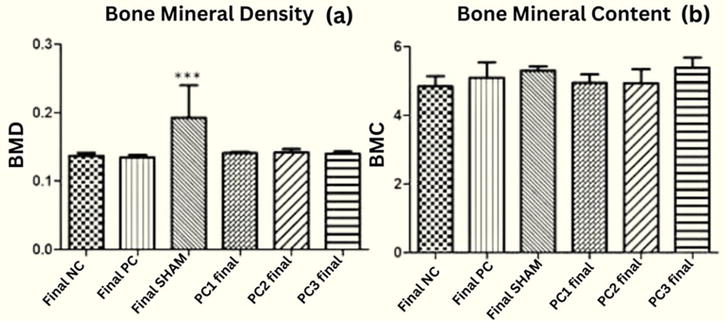
After the first densitometry, the groups were treated with the respective doses for a period of 45 days. Then a new measurement of the total body composition was made. When analyzed in general, considering all the body areas evaluated, a similarity was observed in the density and bone mineral content of all groups, however, the ovariectomized groups had a significantly lower increase than the sham group (Figure 3a). Regarding the bone mineral content, there was no significant difference in overall body bone mineral content between the groups evaluated (Figure 3b).
Figure 3.
Total bone mineral density (g/cm2) (a) and bone mineral content (g) (b) after 45 days of instituted treatment (*p < 0.05; **p < 0.01; ***p < 0.001). Using one-way ANOVA followed by T-test. OVX: ovariectomized; NC: negative control; sham: sham ovariectomized; OVX + PC1: extract 37.5 mg/kg, OVX + PC2: extract 75 mg/kg; OVX + PC3: extract 150 mg/kg).
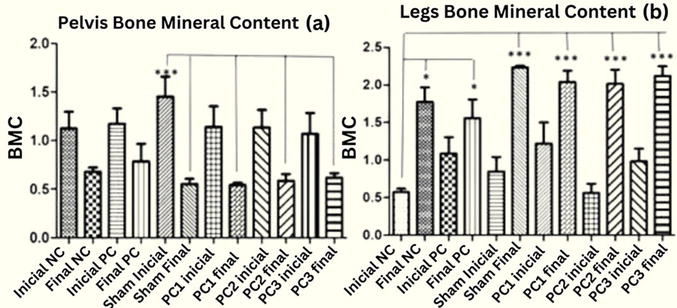
3.1.2 Evaluation of bone mass in pelvis and leg
Considering that densitometry evaluates parameters in different body regions and that the areas to evaluate osteoporosis through this exam in humans are lumbar spine and distal hip and radius, we chose to evaluate data in these regions alone. Although the prolonged treatment with standardized extract of P. cauliflora was not able to maintain the bone mineral content of the pelvis, it had an expressive positive result in the leg region, in the three doses evaluated (Figure 4).
Figure 4.
Bone mineral content (g) of pelvis (a) and leg (b) after 45 days of instituted treatment (*p < 0.05;**p < 0.01; ***p < 0.001). Using one-way ANOVA followed by t-test. OVX: ovariectomized; NC: negative control; sham: sham ovariectomized; OVX + PC1: extract 37.5 mg/kg, OVX + PC2: extract 75 mg/kg; OVX + PC3: extract 150 mg/kg).
3.1.3 Evaluation of bone mass in the trunk
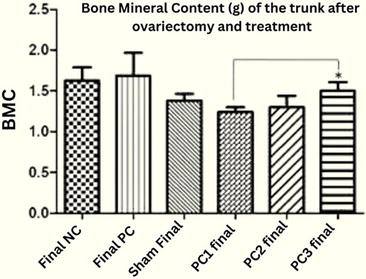
An interesting result was the dose-dependent effect found in the groups treated with sequential doses of Plinia cauliflora in the trunk region. As expressed in Figure 5.
Figure 5.
Bone mineral content (g) of the trunk after 45 days of instituted treatment (*p < 0.05; **p < 0.01; ***p < 0.001), demonstrating a dose-dependent effect in increasing bone content. Using ANOVA unidirectional followed by the t-test. OVX: ovariectomized; NC: negative control; sham: sham ovariectomized; OVX + PC1: extract 37.5 mg/kg, OVX + PC2: extract 75 mg/kg; OVX + PC3: extract 150 mg/kg).
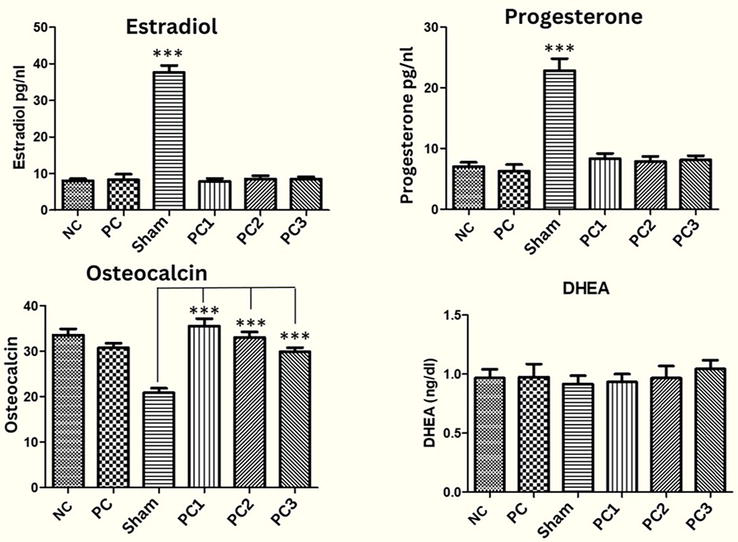
3.1.4 Hormonal analyses
Serum estradiol and progesterone levels in the ovariectomized groups were significantly lower than in the sham group. Prolonged treatment with CP at all three doses significantly elevated serum osteocalcin levels and moderately elevated DHEA levels, without significantly altering estradiol or progesterone levels. The analyses also showed preservation and maintenance of bone turnover in the PC-treated groups compared with the sham operation group (Figure 6).
Figure 6.
Serum levels of (a) estradiol (pg/ml), (b) progesterone (ng/dl), (c) DHEA (ng/ml), and (d) osteocalcin in the groups after 45 days of treatment (*p < 0.05; **p < 0.01; ***p < 0.001). Using one-way ANOVA followed by Tukey’s test. OVX: ovariectomized; NC: negative control; sham: sham ovariectomized; OVX + PC1: extract 37.5 mg/kg, OVX + PC2: extract 75 mg/kg; OVX + PC3: extract 150 mg/kg).
3.1.5 Histological analysis
The histological analysis of the tibiae showed the following results as shown in Table 1.
Groups
OSP (%)
Cell restoration (%)
Simple regeneration (%)
Tissue regeneration (%)
NC
0
100
0
0
OVX
25
75
0
0
sham
33.33
66.6
0
0
OVX + PC1
40
60
0
0
OVX + PC2
0
66.6
0
33.33
OVX + PC3
0
66.6
0
33.33
Table 1.
Percentage of bone changes in the different groups after oral administration of Plinia cauliflora (PC) extract standardized doses.
The OVX, sham, and OVX + PC1 groups developed 25%, 33.3%, and 40% osteoporosis, respectively. Animals in groups OVX + PC2 and OVX + PC3 did not develop osteoporosis in tibiae.
Cell restoration, which consists of reconstitution by own cells of disintegrated organelles, allowing them to survive and recover their functional capacity, occurred in 100% of the animals in the NC group, in 70% of the animals in the PCO group, 60% of the animals in the OVX + PC1 group, and in 66.6% in those in the sham, OVX + PC2, and OVX + PC3 groups.
Of the animals that received P. cauliflora at doses of 75 and 150 mg/kg, 33.33% developed tissue regeneration that is dependent on blood supply.
No group showed simple repair or scarring, which is the replacement of destroyed structures, without possibility of restoration, by elements of the regional support framework, in this case, a considerable increase in mineralization and fewer viable cells.
Osteoporosis (OSP) is a systemic and silent disease, which generates an important oxidative stress in its pathophysiology. In recent years, there has been a significant increase in prevalence, due to the increased life expectancy of the population and also due to new medical technologies to make a more accurate diagnosis [1].
There are several classes of medications for OSP, with different mechanisms of action. Some of them act in increasing bone mass, others in preventing fractures, or, in the most current classes, allow the success of these two projections in the same medication. However, it is important to note that the side effects that these drugs can be significant, as some have the potential to cause irreversible adverse effects. This risk arises not only from the inherent properties of the drug, but also from the patient’s clinical condition and the metabolic changes associated with aging [21]. It is worth emphasizing that osteoporosis is more prevalent among the elderly, and comorbidities tend to be more pronounced in this population.
One of the impacting factors in this pathology is the socioeconomic conditions of our country, since the classes of these medications have quite high values, often leaving patients without access to treatment. However, alternative medicine has been gaining shape to assist in the treatments, thus decreasing the adverse effects and even the costs of medication, making them more accessible to the population, without losing the effectiveness and the goal of the final treatment.
Among the herbal medicines, there are several alternatives that can help in the prevention and treatment of osteoporosis. One of the species that draws attention for its properties is the Plinia cauliflora (jabuticaba), a typical plant in our country.
Although the peels are generally discarded, according to the phytochemical study, they are rich in ellagic acid, quercetin (flavonoids), and anthocyanins, representing a great potential in antioxidant action [19].
Cells with higher levels of mitochondria are considered to have higher energy generation capabilities. RANKL-induced osteoclastogenesis results in increases in the size and number of mitochondria. In osteoporosis, this process is in a disorganized manner generating significant oxidative stress. Due to the antioxidant potential that P. cauliflora presents, it is hypothesized that it may control this bone resorption process [22].
Previous work by our group [2] demonstrated that in 30 days, there was a significant bone loss, which was not observed in the present study, considering the bone structure as a whole. Although no differences were observed in the general bone structures evaluated (BMD and BMC), as shown in Figure 2, when specific regions were compared, such as pelvis and legs, which represent the bone areas of greatest impact in rodents, significant differences were observed, mainly in the legs, in relation to bone mineral content, as observed in Figure 4, demonstrating the potential of Plinia cauliflora as a protective agent of this loss.
Because Plinia cauliflora is a plant extract from a fruit, which is considered a phytocomplex, and not an allopathic drug, it is more difficult to define exactly which active ingredients are responsible for the results obtained. However, the proposed model promoted a protective effect on bone loss in specific regions.
If we consider the cumulative effect of the plant’s use over the period of the onset of diagnostic bone loss, we can suggest that in the long term, it has a positive impact on stemming the loss and consequently controlling the development of bone diseases such as osteoporosis.
The jabuticaba presents effects in the protection and stimulation of tissues rich in collagen and osteoblastic cells, helping in the formation of the bone matrix, in its two characteristics, both in the inorganic formation through the antioxidant actions on the ions, and in the organic formation, in which 95% is formed by collagen type 1, the union of these two formations generates a greater resistance to the bone. Within the inorganic formation, we find hydroxyapatite and calcium, two important ions for the formation of the bone matrix. Osteocalcin (OC) is responsible for fixing these two ions in the extracellular matrix thus affecting bone mineralization, therefore, OC is an important marker of osteoporosis [23].
Elevated levels of this protein (OC) during the absence of estrogen may indicate increased bone turnover. Since the main role of OC is bone mineralization, the body’s calcium levels can profoundly alter its production and homeostasis. Calcium metabolism is very important during postmenopausal osteoporosis, the close relationship between reduced estrogen levels and bone loss may be directly related to this ion [11]. In the present study, it was observed that the three evaluated doses of P. cauliflora were able to increase the levels of OC, which can be hypothesized as a protective factor of bone mineral density, and in the highest dose (150 mg/kg), there was a 70% increase of bone mineral density.
Likewise, as the general structures of BMC and BMD were evidenced, the dosages of all hormones, including osteocalcin, which is a more expressive marker of bone mass loss, were analyzed quantitatively, that is, the total analysis of the animals was included, and not separately in the bone structures, where we verified the protective factor in the studied model. Additionally, a dose-dependent trend toward a protective response of PC against osteocalcin was observed, as illustrated in Figure 6.
P. cauliflora may be promising in the sense that it not only aids in cellular matrix formation but also in preventing bone loss. After the analysis of bone mineral content, we observed that treatment with the PC at three doses equaled the sham group and the control group, showing the effect of prevention against the loss of bone mineral content. The likely route of action of Plinia cauliflora for this result was through osteocalcin and not due to DHEA, which would be the most common route, due to the relationship that the sex hormone part presents in postovariectomy bone mineralization. Despite the effects already attributed to CP, its use had not yet been correlated to bone metabolism.
Other studies using extracts of Tropaeolum majus and Tribulus terrestris demonstrated protective bone effects when there is a decrease in urinary calcium with preservation of osteocalcin levels [11]. In Ref. [2], the authors evaluated the effect of Tribullus terrestris using the same methodology as the present study and demonstrated that increased bone mass was related to increased DHEA, respectively.
The works described in the literature correlate the increase of DHEA as an important factor in the increase of bone mass [24]. The decrease in DHEA is strictly related to changes found in postmenopause such as decrease in bone mass, decrease in muscle mass, increase in body fat accumulation, and diabetes mellitus [25]. However, the results of the present study demonstrated that Plinia cauliflora, at the three doses evaluated, despite having increased bone mass, the increase in DHEA levels was not significant, which leads us to suggest that the protective effect presented by Plinia cauliflora, and even bone mass gain, especially in the leg regions, may have been due to a greater impact generated in this region, a bone mass gain of 140% in the average dose (75 mg), through the osteocalcin pathway.
Study [26] revealed that OC is important in the process of alignment of collagen fibers parallel to hydroxyapatite, which would increase bone strength in long bones, and could justify the results of the present work. OC has a correlation with the formation of bone matrix, which is a precursor of mature osteoblastic cells, being one of the main markers of osteoblastic activity. Importantly, osteocalcin is an essential marker of bone matrix formation and not resorption, because it is completely destroyed by osteoclasts; its function is not well defined yet. However, studies indicate that its structure has an interaction with calcium and hydroxyapatite crystals and that its increase coincidentally correlates with the beginning of the mineralization process [27].
It has already been shown that 3-O-methyl gallic acid has the potential to prevent osteoporosis [28]. This molecule significantly suppressed osteoclast formation by blocking Akt and Btk-PLCγ2-Ca2+ signaling. Considering that Plinia cauliflora is rich in ellagic acid, a derivative of gallic acid, it is justified that the results obtained in bone protection may be related to the role of this compound in reducing osteoclasts.
Therefore, the antioxidant action that Plinia cauliflora presents through its chemical constituents, such as anthocyanins, ellagic acid, and quercetin, protect the osteocalcin pathway to act in the formation of bone mineralization, using in a more significant way the osteoblasts.
Although the effects attributed to P. cauliflora may be due to the increase in osteocalcin, after analysis of the trunk of the animals (rats), we observed that the three doses resulted in an equalization of bone mass gain, with the highest therapeutic dose PC3 (150 mg/kg/day) showing a more significant increase of 22% compared to the dose PC1. Therefore, it is possible that there are other osteoprotection mechanisms correlated to the extract since it is a phytocomplex from the peel of the Plinia cauliflora fruit, and thus there may be an increase in bone mass without correlation with the increase in hormones, for example, changes in inflammatory cytokines and antioxidant enzymes.
Treatment with Plinia cauliflora extract resulted in improved bone mineral density. The results suggest that this increase is not related to DHEA or sex hormones but to the increase of osteocalcin. The elevation of osteocalcin preserved the bone matrix after 45 days of treatment in ovariectomized rats. The three doses evaluated maintained an equal pattern for the prevention of matrix loss, suggested to be the probable responsible for the osteoporosis prevention effects. In the model used, it should be considered that the protection analysis was evaluated over a period of 45 days against the proposed treatment groups, but it should be taken into account that osteoporosis, being a chronic disease, can manifest itself more intensely over longer periods, which is suggested to be analyzed in future studies, in different periods. Further work is needed to evaluate its role as a protective agent in this experimental model. Additional preclinical and clinical studies may clarify the mechanism of action of this natural product in the treatment and prevention of osteometabolic diseases.
1.Bucholz RW et al. Fraturas em Adultos de Rockwood & Green. 7th ed. Barueri, SP: Manole; 2013. 492-590 pp
2.Marques MAA, Lourenço BHLB, Reis MDP, Pauli KB, Soares AL, Belettini ST, et al. Osteoprotective effects of Tribulus terrestris L.: Relationship between dehydroepiandrosterone levels and Ca2+-sparing effect. Journal of Medicinal Food. 2019;22(3):241-247. DOI: 10.1089/jmf.2018.0090
3.Pisani P, Renna MD, Conversano F, Casciaro E, Di Paola M, Quarta E, et al. Major osteoporotic fragility fractures: Risk factor updates and societal impact. World Journal of Orthopedics. 2016;7(3):171-181. DOI: 10.5312/wjo.v7.i3.171
4.Amadei SU, Silveira VÁS, Pereira AC, Carvalho YR, Rocha RFD. A influência da deficiência estrogênica no processo de remodelação e reparação óssea. Jornal Brasileiro de Patologia e Medicina Laboratorial. 2006;42:5-12. DOI: 10.1590/S1676-24442006000100003
5.Lee DR, Lee J, Rota M, Lee J, Ahn HS, Park SM, et al. Coffee consumption and risk of fractures: A systematic review and dose-response meta-analysis. Bone. 2014;63:20-28. DOI: 10.1016/j.bone.2014.02.007
6.Orwig DL, Chan J, Magaziner J. Hip fracture and its consequences: Differences between men and women. Orthopedic. Clinics. 2006;37(4):611-622. DOI: 10.1016/j.ocl.2006.08.003
7.Wannmacher L. Manejo racional da osteoporose: onde está o real benefício. Organização Pan-Americana da Saúde/Organização Mundial da Saúde-Brasil; 2004. pp. 1-7. DOI: 10.1055/S-0033-1346697. Available from: https://core.ac.uk/download/pdf/48116592.pdf
8.Swaminathan R. Biochemical markers of bone turnover. Clinica Chimica Acta. 2001;313(1-2):95-105. DOI: 10.1016/S0009-8981(01)00656-8
9.Bikle DD. Biochemical markers in the assessment of bone disease. The American Journal of Medicine. 1997;103(5):427-436. DOI: 10.1016/S0002-9343(97)00137-X
10.Atalay S, Elci A, Kayadibi H, Onder CB, Aka N. Diagnostic utility of osteocalcin, undercarboxylated osteocalcin, and alkaline phosphatase for osteoporosis in premenopausal and postmenopausal women. Annals of Laboratory Medicine. 2012;32(1):23-30. DOI: 10.3343/alm.2012.32.1.23
11.Barboza LN, Prando TBL, Dalsenter PR, Gasparotto FM, Gasparotto F, Jacomassi E, et al. Prolonged diuretic activity and calcium-sparing effect of Tropaeolum majus: Evidence in the prevention of osteoporosis. Evidence-Based Complementary and Alternative Medicine. 2014. Article ID 958291. DOI: 10.1155/2014/958291
12.Papaioannou A, Morin S, Cheung AM, Atkinson S, Brown JP, Feldman S, et al. Clinical Practice Guidelines for the Diagnosis and Management of Osteoporosis in Canada: Background and Technical Report. Canada, Ontario: Scientific Advisory Council of Osteoporosis; 2010. Available from: https://osteoporosecanada.ca/wp-content/uploads/Osteoporosis_Guidelines_2010_Background_And_Technical_Report.pdf
13.Marques MAA, Lima DA, Andreotti CE, Junior AG, ELB L. Caracterização das plantas medicinais e medicamentos fitoterápicos para tratamento da osteoporose utilizados no Brasil. Arquivos de Ciências da Saúde da UNIPAR. 2016;20(3):183-188. DOI: 10.25110/arqsaude.v20i3.2016.5870
14.Lin CY, Yin MC. Renal protective effects of extracts from guava fruit (Psidium guajava L.) in diabetic mice. Plant Foods for Human Nutrition. 2012;67:303-308. DOI: 10.1007/s11130-012-0294-0
15.Maia JL. Desenvolvimento de microcápsulas contendo as antocianinas presentes no corante do extrato do jambo por polimerização interfacial [thesis]. Natal, RN: Universidade Federal do Rio Grande do Norte; 2013. Available from: https://repositorio.ufrn.br/handle/123456789/15845
16.Knekt P, Isotupa S, Rissanen H, Heliövaara M, Järvinen R, Häkkinen S, et al. Quercetin intake and the incidence of cerebrovascular disease. European Journal of Clinical Nutrition. 2000;54(5):415-417. DOI: 10.1038/sj.ejcn.1600974
17.Knight DC, Eden JA. Phytoestrogens-a short review. Maturitas. 1995;22(3):167-175. DOI: 10.1016/0378-5122(95)00937-G
18.Lorenzi H, Matos FJA. Plantas Medicinais no Brasil: Nativas e Exóticas. 2ª ed. Instituto Plantarum: Nova Odessa; 2008
19.Romão PVM, Palozi RAC, Guarnier LP, Silva AO, Lorencone BR, Nocchi SR, et al. Cardioprotective effects of Plinia cauliflora (Mart.) Kausel in a rabbit model of doxorubicin-induced heart failure. Journal of Ethnopharmacology. 2019;242:112042. DOI: 10.1016/j.jep.2019.112042
20.Lelovas PP, Xanthos TT, Thoma SE, Lyritis GP, Dontas IA. The laboratory rat as an animal model for osteoporosis research. Comparative Medicine. 2008;58(5):424-430. Available from: https://www.ncbi.nlm.nih.gov/pmc/articles/PMC2707131/
21.Wimalawansa SJ, Razzaque MS, Al-Daghri NM. Calcium and vitamin D in human health: Hype or real? The Journal of Steroid Biochemistry and Molecular Biology. 2018;180:4-14. DOI: 10.1016/j.jsbmb.2017.12.009
22.Park-Min KH. Metabolic reprogramming in osteoclasts. Seminars in Immunopathology. 2019;41(5):565-572. DOI: 10.1007/s00281-019-00757-0
23.Zanatta LC, Boguszewski CL, Borba VZ, Kulak CA. Osteocalcina, metabolismo energético e da glicose. Arquivos Brasileiros de Endocrinologia & Metabologia. 2014;58:444-451. DOI: 10.1590/0004-2730000003333
24.Jankowski CM, Gozansky WS, Schwartz RS, Dahl DJ, Kittelson JM, Scott SM, et al. Effects of dehydroepiandrosterone replacement therapy on bone mineral density in older adults: A randomized, controlled trial. The Journal of Clinical Endocrinology & Metabolism. 2006;91(8):2986-2993. DOI: 10.1210/jc.2005-2484
25.Labrie F, Bélanger A, Bélanger P, Bérubé R, Martel C, Cusan L, et al. Metabolism of DHEA in postmenopausal women following percutaneous administration. The Journal of Steroid Biochemistry and Molecular Biology. 2007;103(2):178-188. DOI: 10.1016/j.jsbmb.2006.09.034
26.Komori T. Functions of osteocalcin in bone, pancreas, testis, and muscle. International Journal of Molecular Sciences. 2020;21(20):7513. DOI: 10.3390/ijms21207513
27.Vieira JGH. Considerações sobre os marcadores bioquímicos do metabolismo ósseo e sua utilidade prática. Arquivos Brasileiros de Endocrinologia & Metabologia. 1999;43:415-422. DOI: 10.1590/S0004-27301999000600005
28.Baek JM, Kim JY, Lee CH, Yoon KH, Lee MS. Methyl gallate inhibits osteoclast formation and function by suppressing Akt and Btk-PLCγ2-Ca2+ signaling and prevents lipopolysaccharide-induced bone loss. International Journal of Molecular Sciences. 2017;18(3):581. DOI: 10.3390/ijms18030581
Written By
Maxuel Fidelis de Padua Almeida, Guilherme Donadel, Mariana Dalmagro, Gabriel Maciel, Gabriela Zanuto de Lima, Marcia Alessandra Arantes Marques, Salviano Tramontin Bellettini, Ezilda Jacomassi, Giuliana Zardeto, Emerson Luiz Botelho Lourenço and Daniela de Cassia Faglioni Boleta Ceranto
Submitted: 19 July 2023Reviewed: 04 August 2023Published: 06 November 2023
 Open access peer-reviewed chapter
Open access peer-reviewed chapter