 Open access peer-reviewed chapter
Open access peer-reviewed chapter
Abstract
Adenoid, also known as the Luschka’s or nasopharyngeal tonsil, is a mass of lymphoid tissue located in the roof of nasopharynx. The term ‘adenoid’ was coined by Meyer. Earliest records of adenoid surgery date back to 1842, when Yearsley reported removal of mucus membrane from behind the uvula to improve ear function. Other techniques for adenoidectomy included bare fingernails or finger ring knife, which are considered obsolete now. From mid-1930s to early 1960s, radiation therapy of the adenoid was used extensively. Transoral adenoid curetting and electrical dissection techniques followed and became mainstay of treatment for a long time. Infact, these are still in use in many centres across the world. Like any other surgery, introduction of nasal endoscopes and powered instruments revolutionised adenoid surgery by greatly increasing the precision and minimising collateral damage. Plasma-mediated ablation (Coblation) promises ‘blood-less’ surgery. Presently, the trend is focussed towards using powered instruments (Microdebrider and/or Coblation) under endoscopic visualisation for complete adenoidectomy.
Keywords
- adenoid
- adenoidectomy
- coblation
- microdebrider
- adenoid curette
1. Introduction
The adenoid forms part of Waldeyer’s ring of lymphoid tissue at the portal of the upper respiratory tract. In early childhood this is the first site of immunological contact for inhaled antigens. Santorini was the first one to describe the nasopharyngeal lymphoid aggregate or ‘Luschka’s tonsil’ in 1724. Wilhelm Meyer coined the term ‘adenoid’ to apply to ‘nasopharyngeal vegetations’ in 1870.
Adenoid hypertrophy is considered to be a culprit of upper airway obstruction, a focus of sepsis, and persistence of otitis media with effusion.
2. Development and anatomy of the adenoid
Earliest identification of lymphoid tissue can be made at 4- to 6-weeks of gestational period, lying within the mucous membrane of nasopharynx. The adenoid is clearly identified at third month of gestation.
Adenoid tissue is anatomically located in the roof of posterior wall of nasopharynx. It can extend to the fossa of Rosenmüller and to the Eustachian tube orifice as Gerlach’s tonsil. Non- keratinised stratified squamous epithelium is the lining epithelium of adenoid tissue. The arterial supply is mainly from the branches of facial artery, maxillary artery and thyrocervical trunk. Venous drainage is to the internal jugular and facial veins. Lymphatics drain into retropharyngeal lymph nodes and upper deep cervical nodes, especially the posterior triangle of the neck.
Nerve supply is from sensory branches of CN IX (Glossopharyngeal Nerve) and CN X (Vagus Nerve) [1].
Adenoid is visible using magnetic resonance imaging (MRI) from the age of 4 months in approximately 18% of the paediatric population [2]. At the age of 5 months, adenoid is identifiable in almost all children. Adenoid continues to grow rapidly during infancy and the growth plateaus between the ages of 2 and 14 years. Regression of adenoid occurs quite rapidly after 15 years of age in majority of the children. Adenoid is at the relative largest size in relation to the volume of the nasopharynx in the 7-year old age group [3]. Clinical symptoms are more common in younger age groups, due to relatively small volume of nasopharynx and the increased frequency of upper respiratory tract infections (Figures 1 and 2).
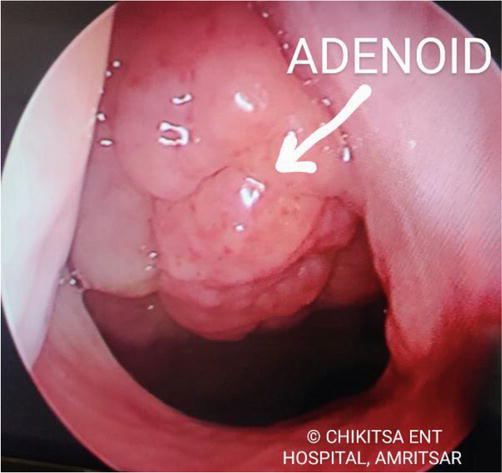
Figure 1.
Endocsopic view of adenoid tissue in nasopharynx. © Chikitsa ENT hospital, Amritsar. Used with permission.

Figure 2.
X-ray nasopharynx (lateral view) showing adenoid hypertrophy.
3. Immune function of the adenoid
The function of the lymphoid tissue of Waldeyer’s ring is production of antibodies. Adenoid produces B-cells, which gives rise to IgG and IgA plasma cells. Exposure to antigens via the oral and nasal route is an important part of natural acquired immunity in early childhood. Adenoid appears to have an important role in the development of ‘immunological memory’ in younger children [4]. While some studies have found that adenoidectomy in early childhood can be immunologically undesirable [5]. Other studies have concluded that adenotonsillectomy does not cause significant immune deficiency [6].
Nevertheless, a careful decision has to be made for every patient individually whether to perform adenoidectomy or not.
4. Pathological effects of the adenoid
Pathological manifestations of adenoid include adenoiditis, rhinitis, rhinosinusitis, otitis media and otitis media with effusion [7].
The adenoid, due its anatomical position, is implicated in upper respiratory tract diseases due to partial or complete obstruction of the nasal choanae or as a result of sepsis. This also causes severe sleep disturbances in children. It is also a common cause of obstructive sleep apnea (OSA). Sleep- disordered breathing and habitual snoring, results in neurobehavioural morbidity, poor academic performance and hyperactive behaviour [8, 9]. The respiratory improvement following adenotonsillectomy also results in a significant increase in serum insulin-like growth factor-1 (IGF-1) [10], accounting in part for the frequently observed growth spurt following surgery.
Additionally, adenoidal hyperplasia may reduce olfactory sensitivity and, in particular, retronasal smell and taste, which improves following adenoidectomy [11].
Adenoid mass is the most common culprit for recurrent otitis media with effusion (OME) episodes in paediatric population. Owing to its proximity to the eustachian tube orifice in nasopharynx, it can cause its anatomical obstruction. Moreover, adenoid tissue acts as source of bacterial harborization and ‘biofilm’ formation. Recurrent acute and chronic inflammation of the adenoid and increased bacterial load (especially Haemophilus influenzae) [12, 13, 14], contributes in a more severe way to OME episodes.
As adenoid acts as a reservoir for pathogenic bacteria, it also contributes in a major way to rhinosinusitis, especially in children [15]. ‘Biofilm’ formation is particularly implicated in failure of medical therapy for chronic rhinosinusitis in children with adenoid hypertrophy.
Extremely rarely, Non-Hodgkin’s lymphoma can also develop in the adenoid tissue [16]. Atypical lymphadenopathy, with persistent and asymmetric enlargement of the adenoid, in the absence of infection is suspicious and should prompt early imaging and biopsy to rule out malignancy.
Thus adenoid needs to be adequately managed. Over the years, various modalities for treatment of adenoid have been developed. These include observation alone, medical therapy, radiation therapy, surgical removal or a combination of these.
5. Treatment of the adenoid
5.1 Observation (wait and watch)
Adenoid size is age dependent. Adenoid mass increases in size rapidly after birth. It reaches its maximum size by 7–10 years of age. After that, it begins to regress and gradually diminishes in size throughout adulthood [3].
Although, exceptions are not unheard of. Infact, the adenoid is at its relative largest in relation to the volume of the nasopharynx in the 7-year old age group [3]. Persisting large adenoid mass in adults, filling up the entire nasopharyngeal volume, is a common finding.
In conclusion, if the adenoid mass is small in size and relatively asymptomatic, observation alone can be taken as a standalone modality, especially in children, as there is a high chance that it might regress in due course of time.
5.2 Medical therapy
Traditionally, surgery and watchful waiting were the only viable options for symptomatic adenoid disease. There is now a evidence that topical nasal steroid sprays can cause reduction in adenoid size with improvement in symptoms, although at present that role is unclear [17].
Recent studies have proven that Vitamin D3 deficiency is linked with adenoid hypertrophy [18]. Therefore adequate supplementation of Vitamin D3 needs to be done in patients being treated for adenoid hypertrophy.
5.3 Radiation therapy
Radiation therapy for ablating adenoid mass is more of historical importance only.
From the mid-1930s to the early 1960s, radiation therapy of adenoid was in extensive use, both for children and for army aviators and navy submarine crews during WWII [19].
However, radiation therapy is a thing of past owing to its immense side effect profile and development of better and more effective treatment modalities.
5.4 Surgery for adenoid
A symptomatic adenoid often warrants its surgical removal. An ideal adenoidectomy aims at complete removal of adenoid tissue, without damaging surrounding structures (eustachian tube opening, torus tubaris, soft palate, superior constrictor muscle). Over the years various techniques for adenoidectomy have been developed, and are discussed below.
5.4.1 Evolution of adenoid surgery
The adenoid surgery has evolved over the years on the basis of visualisation of the adenoid. While the earliest documented adenoid surgeries were blind procedures, the advent of endoscopes in nasal surgeries has seen a paradigm shift in how adenoidectomy is performed today.
5.4.2 Blind procedures for adenoidectomy
5.4.2.1 Adenoid curettes and adenotomes
Since the earliest descriptions of adenoidectomy, a great number of different techniques have been described and used successfully. All of these techniques are based on the principle of adequate removal of the adenoids without damage to the surrounding structures, such as the torus tubarus, the palate, the posterior pharyngeal wall, and the choana. Recent minimally invasive and endoscopic technologies have also been applied for adenoidectomy.
The first mention of adenoidectomy was done by Meyer in 1867 [20]. He used a sharp ring curette inserted blindly through oral cavity by just palpating the ‘nasopharyngeal vegetations’.
Soon after, many new methods were developed for the removal of adenoids, most of which approached the adenoids transorally.
A ring knife was invented by Gottstein in 1885 [21]. Beckmann modified this ring knife in 1897 [22]. Punch forceps and adenotome were also developed for removal of adenoid mass. Sir St Clair Thomson developed the famous adenoidectomy curette, complete with its cage to ensure safety and to entangle the tissue fragments and blood during adenoidectomy. This curette is still used in the conventional curettage adenoidectomy [23].
The current standard procedure for blind adenoidectomy is curettage. Patient is placed in Rose position and an appropriate sized mouth gag is placed in the oral cavity. St Clair Thompson adenoidectomy curette is inserted in the oral cavity, bypassing the oropharynx in order to reach the nasopharynx and is engaged at the adenoid pad. The adenoid mass is removed from superior to inferior with a single pass of the curette. Care should be taken to avoid injury to the deep muscular and vertebral plane, to the torus region or to the choanal area. The resultant adenoid bed is packed with a sponge to achieve heamostasis. Saline irrigation also helps in achieving haemostasis. Completion is confirmed by digital palpation.
The limitations of this technique is less precise removal and thus less effective treatment, increased bleeding, velopharyngeal insufficiency, and lack of surgical visualisation. Blind curettage procedure does not always completely remove the adenoid tissue, thus recurrence is common with this technique (Figure 3) [24].
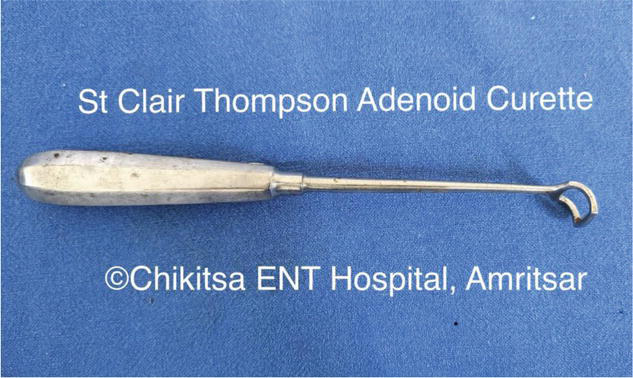
Figure 3.
St. Clair Thompson adenoidectomy curette. © Chikitsa ENT hospital, Amritsar. Used with permission.
5.4.3 Indirect visualisation using mirrors
Blind techniques of adenoidectomy were particularly accompanied by high complication rates. Damage to surrounding structures like eustachian tube caused stenosis, leading to ear problems. Soft palate injury resulted in velopharyngeal insufficiency. Superior constrictor/prevertebral injury was often accompanied by primary or secondary haemorrhages and neck stiffness. Moreover, complete adenoidectomy was seldom possible with these techniques and residual adenoid tissue was often left at upper nasopharynx, Fossa of Rosenmuller and choana [25, 26, 27, 28, 29].
To rectify these shortcomings, a lot of surgeons started to prefer indirect visualisation of nasopharynx using a laryngeal mirror/dental mirror introduced through oral cavity.
5.4.3.1 Microdebrider- adenoidectomy under indirect visualisation
A few surgeons started to use a curved shaver or microdebrider for adenoidectomy under continuous indirect visualisation through a laryngeal mirror [28, 30, 31]. Both the shaver and the mirror were introduced transorally. The oscillating shaver tip is under continuous visualisation while it removes adenoid tissue in a superior to inferior manner. The enhanced precision enables safe tissue removal from earlier ‘inaccessible areas’ like choana, upper nasopharynx and peri-tubal area.
5.4.3.2 Suction diathermy assisted adenoidectomy under indirect visualisation
A laryngeal mirror is introduced transorally to visualise adenoid mass in nasopharynx [26, 32]. Adenoid mass is ablated using an insulated, curved Frazier-type suction system or, a disposable, malleable, hand-switching suction coagulator. As the diathermy cauterises the adenoid mass, it shrinks, while the suction evacuates the smoke. This method gained widespread acceptance owing to its advantages of being precise, easy to perform, fast, bloodless and relatively inexpensive (Figure 4).

Figure 4.
Bipolar and monopolar cautery unit (diathermy). © Chikitsa ENT hospital, Amritsar. Used with permission.
5.4.3.3 Laser adenoidectomy
Laser adenoidectomy, using a CO2 laser, has also been described in literature. Jaw and palate are retracted using laser-compatible retractors and lips and teeth are covered with foil. Wet towels are used to cover the rest of the face. A microscope mounted CO2 laser is then reflected onto the adenoid mass through a polished mirror kept in oropharynx. The mirror also assists in indirect visualisation of adenoid mass being ablated.
Although an interesting technique, laser adenoidectomy never gained popularity, probably owing to its greater cost, and development of better tools and techniques (Microdebrider/Coblation) [33].
5.4.4 Endoscopic visualisation
(See Figure 5)
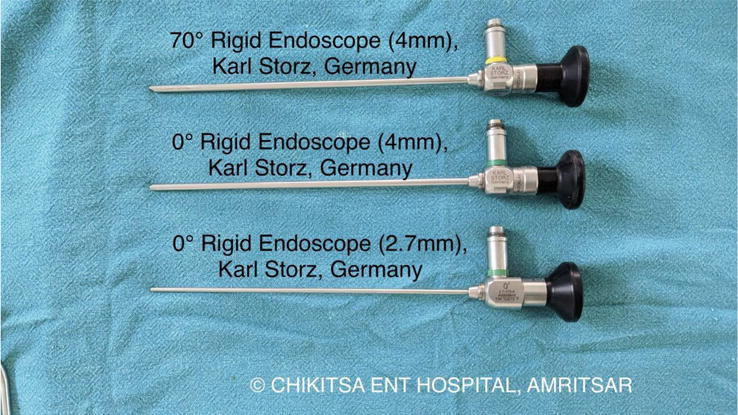
Figure 5.
Karl Storz rigid endoscopes. © Chikitsa ENT hospital, Amritsar. Used with permission.
5.4.4.1 Nasal endoscopic adenoid curettage
The nasal cavities and nasopharynx are examined using a 0° nasal endoscope [34]. Boyle- Davis mouth gag is used to open the mouth wide. An adenoidectomy curette is placed into the nasopharynx via the transoral route. Under endoscopic guidance, the blade of the adenoid curette is placed just above the superior border of the adenoid. Care should be taken to avoid touching the eustachian tube on both sides. The nasal endoscope is then taken out from the nose and the curettage is done as per conventional protocol.
5.4.4.2 Transoral endoscopic adenoidectomy using suction diathermy
A 45° rigid scope is introduced into the oral cavity to the oropharynx with the camera pointing upwards to the nasopharynx [35]. A suction coagulator is introduced alongside the endoscope. Adenoidectomy is performed under direct endoscopic vision by using a combination of monopolar coagulation and suction.
5.4.4.3 Transnasal endoscopy along with powered transnasal adenoidectomy
A zero degree rigid endoscope (2.7 mm/4.0 mm) is passed through the nasal cavity to visualise adenoid mass in nasopharyhnx [27, 36]. A straight (zero degree) microdebrider blade is passed through the nasal cavity under endoscopic visualisation to reach the nasopharynx. The oscillating microdebrider blade is then switched on to debride the adenoid tissue in an anterior to posterior fashion. Continuous irrigation and suction in the microdebrider system provides for better visualisation. Its major advantage lies in clearing the adenoid tissue from around choana and eustachian tube, without injuring the surrounding structures.
5.4.4.4 Transoral endoscopy with transoral powered adenoidectomy
This approach uses a 70-degree rigid endoscope (4.0 mm) and a posterior facing- 40 degree curved microdebrider blade, both introduced through oral cavity [37]. Palate can be retracted using feeding tubes introduced through nose. The adenoid tissue is debrided and sucked by the microdebrider system. Continuous irrigation and suction of the system facilitates the process. A gauze piece is kept in the end to achieve haemostasis. This technique is considered to have a better clearance of the peritubal adenoid mass without any injury of nasal septum/turbinates.
5.4.4.5 Transnasal endoscopy with transoral powered adenoidectomy
Transnasal endoscopy with transoral powered (Microdebrider/Coblation) adenoidectomy is the authors’ preferred technique. This technique was first described by Dr. Satish Jain (Jaipur, India) and has become now the most commonly used technique across Indian subcontinent. The patient lies in a supine position under general anaesthesia using an orotracheal tube. The head end is elevated at 15–30 degrees. A zero degree rigid endoscope (2.7 mm/4.0 mm) is used to visualise the adenoid mass in the nasopharynx. A mouth gag opens the mouth to allow introduction of powered instruments. An anterior facing −40 or 60 degree curved microdebrider blade, introduced transorally, allows for precise removal of adenoid mass under continuous endoscopic visualisation. The removal of adenoids is done in three phases. First phase allows gross debulking of the adenoid tissue. The second phase allows fine removal of adenoid tissue anterior to perimysial layer of superior constrictor muscle. While the third phase allows removal of adenoid tissue from the peritubal region (especially fossa of rosenmuller on either side) and upper nasopharynx. Coblation is then used to achieve complete haemostasis. Alternately, all three phases can be done using Coblation alone using its adenoidectomy wand. This technique has major advantages as against all other techniques in the form of better visualisation, complete removal of adenoid tissue and minimum blood loss. Eustachian tube, torus tuboris and posterior pharyngeal wall also remain well protected with this technique (Figures 6–10).
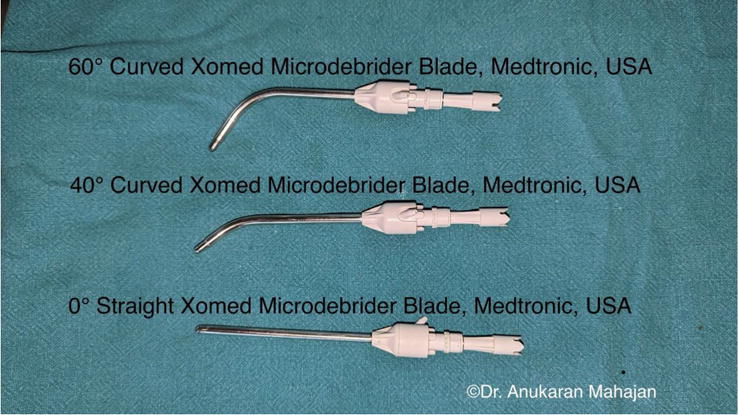
Figure 6.
Xomed microdebrider blades, curved and straight.

Figure 7.
IPC medtronic (USA) microdebrider unit. © Chikitsa ENT hospital, Amritsar. Used with permission.
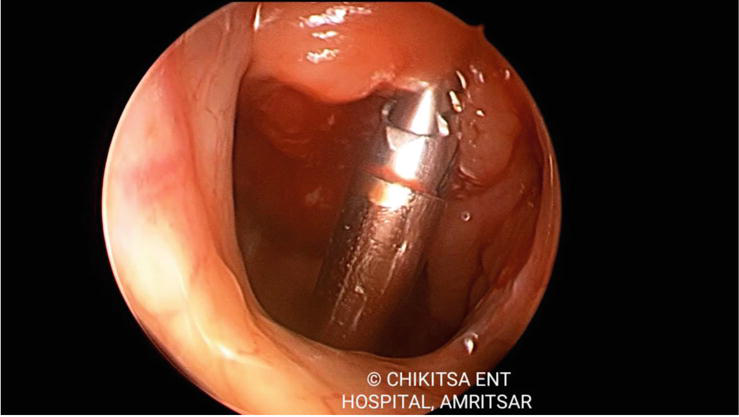
Figure 8.
Transnasal endoscopic view of transoral powered adenoidectomy using microdebrider (60O curved xomed blade). © Chikitsa ENT hospital, Amritsar. Used with permission.
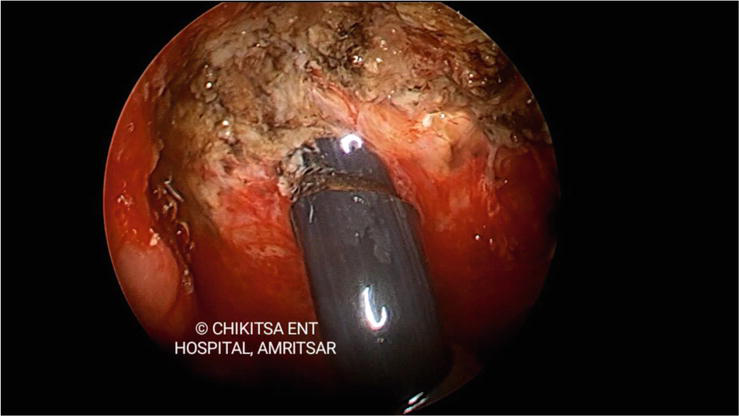
Figure 9.
Transnasal endoscopic view of transoral powered adenoidectomy using coblator. © Chikitsa ENT hospital, Amritsar. Used with permission.

Figure 10.
Arthrocare coblator unit, Smith and Nephew (USA). © Chikitsa ENT hospital, Amritsar. Used with permission.
6. Conclusion
Adenoid is nasopharyngeal lymphatic tissue, present in all children. Symptomatic adenoid warrants treatment, more often than not, in the form of surgery. Over the decades surgical techniques and tools have evolved to make adenoidectomy a safe and effective procedure. Transnasal endoscopic visualisation with transoral powered adenoidectomy using microdebrider/coblation is the most advanced and authors’ preferred method.
Acknowledgments
I wish to express my sincere gratitude towards Dr. Arun Dhanuka, Vibha Dhanuka and Dr. Aishwarya Dhanuka for their constant moral support. I am fortunate to have worked with Dr. Stuti Mahajan and Dr. Anukaran Mahajan on numerous adenoid cases. A special vote of thanks to Dr. Anupama Mahajan, HOD Anatomy and Director Principal, SGRDIMSR, Amritsar for providing valuable insight into the anatomy and pathology of this disease. I shall always be indebted to Dr. Karunesh Gupta and Dr. Rajeev Kapila for their unparalleled mentorship.
References
- 1.
University of Texas Medical Section Grand Rounds. Tonsillitis, Tonsillectomy, and Adenoidectomy. 1999. Available from: https://www.utmb.edu/ - 2.
Jaw TS, Sheu RS, Liu GC, Lin WC. Development of adenoids: A study by measurement with MRI images. The Kaohsiung Journal of Medical Sciences. 1999; 15 :12-18 - 3.
Vogler RC, Ii FJ, Pilgram TK. Age-specific size of the normal adenoid pad on magnetic resonance imaging. Clin Otol Allied Sci. 2000; 25 :392-395 - 4.
Wysocka J, Hassmann E, Lipska A, Musiatowicz M. Naïve and memory T-cells in hypertrophied adenoids in children according to age. International Journal of Pediatric Otorhinolaryngology. 2003; 67 :237-241 - 5.
Brandtzaeg P. Immunology of the tonsils and adenoids: Everything the ENT surgeon needs to know. International Journal of Pediatric Otorhinolaryngology. 2003; 67 :69-76 - 6.
Ikinciogullari A, Dogu F, Ikinciogullari A, et al. Is the immune system influenced by adenotonsillectomy in children? International Journal of Pediatric Otorhinolaryngology. 2002; 66 :251-257 - 7.
Richardson MA. Sore throat, tonsillitis and adenoiditis. The Medical Clinics of North America. 1999; 83 :75-83 - 8.
Brockmann PE, Bertrand P, Pardo T, et al. Prevalence of habitual snoring and associated neurocognitive consequences among Chilean school aged children. International Journal of Pediatric Otorhinolaryngology. 2012; 76 :1327-1331 - 9.
Owens JA. Neurocognitive and behavioral impact of sleep disordered breathing in children. Pediatrics Pulm. 2009; 44 :417-422 - 10.
Bar A, Tarasuik A, Segev Y, et al. The effect of adenotonsillectomy on serum insulin like growth factor-I and growth in children with obstructive sleep apnea syndrome. The Journal of Pediatrics. 1999; 135 :76-80 - 11.
Delank KW. Olfactory sensitivity in adenoid hyperplasia. Laryngo- Rhino- Otologie. 1992; 71 :293-297 - 12.
Suzuki M, Watanabe T, Mogi G. Clinical, bacteriological and histological study of adenoids in children. American Journal of Otolaryngology. 1999; 20 :85-90 - 13.
Brook I, Shah K, Jackson W. Microbiology of healthy and diseased adenoids. Laryngoscope. 2000; 110 :994-999 - 14.
Yasan H, Dogru H, Tuz M, et al. Otitis media with effusion and histopathologic properties of adenoid tissue. International Journal of Pediatric Otorhinolaryngology. 2003; 67 :1179-1183 - 15.
Shin KS, Cho SH, Kim KR, et al. The role of the adenoids in pediatric rhinosinusitis. International Journal of Pediatric Otorhinolaryngology. 2008; 72 :1643-1650 - 16.
Tilford DL. Unsuspected non-Hodgkins lymphoma of the tonsils and adenoids in children. Pediatrics. 1987; 79 :399-402 - 17.
Chohan A, Lal A, Chohan K, et al. Systematic review and meta-analysis of randomized controlled trials on the role of mometasone in adenoid hypertrophy in children. International Journal of Pediatric Otorhinolaryngology. 2015; 79 (10):1599-1608 - 18.
Shin JH, Kim BG, Kim BY, Kim SW, Kim SW, Kim H. Is there an association between vitamin D deficiency and adenotonsillar hypertrophy in children with sleep-disordered breathing? BMC Pediatrics. 2018; 18 (1):196. DOI: 10.1186/s12887-018-1178-8 - 19.
Crowe SJ, Baylor JW. The prevention of deafness. JAMA. 1939; 112 :585-590 - 20.
Meyer W. On adenoid Vegetations in the Naso-pharyngeal cavity: Their pathology, diagnosis, and treatment. Med Chir Trans. 1870; 53 :191-216 - 21.
Weir N. Otolaryngology--an Illustrated History. Boston: MA, Butterworths; 1990 - 22.
Feldmann H. The nasopharynx and pharyngeal tonsil in the history of otology and rhinology. Pictures from the history of otorhinolaryngology, presented by instruments from the collection of the Ingolstadt medical history museum. Laryngorhinootologi. 1999; 78 (5):280-289 - 23.
Dilesh M, Adenoidectomy- A. Historical Review. Glob J Oto. 2017; 8 (3):555740. DOI: 10.19080/GJO.2017.08.555740 - 24.
Cannon CR, Replogle WH, Schenk MP. Endoscopic-assisted adenoidectomy. Otolaryngology-Head and Neck Surgery. 1999; 121 (6):740-744 - 25.
Buchinsky FJ, Lowry MA, Isaacson G. Do adenoids regrow after excision? Otolaryngology-Head and Neck Surgery. 2000; 123 (5):576-581 - 26.
Elluru RG, Johnson L, Myer CM. Electrocautery adenoidectomy compared with curettage and power-assisted methods. Laryngoscope. 2002; 112 (8) Pt. 2 Suppl. 100:23-25 - 27.
Havas T, Lowinger D. Obstructive adenoid tissue: An indication for powered shaver adenoidectomy. Archives of Otolaryngology-Head and Neck Surgery. 2002; 128 (7):789-791 - 28.
Stanislaw P, Koltai PJ, Feustel PJ. Comparison of power-assisted adenoidectomy vs adenoid curette adenoidectomy. Archives of Otolaryngology-Head and Neck Surgery. 2000; 126 (7):845-849 - 29.
Ark N, Kurtaran H, Ugur KS, Yilmaz T, Ozboduroglu AA, Mutlu C. Comparison of adenoidectomy methods: Examining with digital palpation vs. visualizing the placement of the curette. International Journal of Pediatric Otorhinolaryngology. 2010; 74 (6):649-651 - 30.
Koltai PJ, Chan J, Younes A. Power-assisted adenoidectomy: Total and partial resection. Laryngoscope. 2002; 112 (8) Pt. 2 Suppl. 100:29-31 - 31.
Rodriguez K, Murray N, Guarisco JL. Power-assisted partial adenoidectomy. Laryngoscope. 2002; 112 (8) Pt. 2 Suppl. 100:26-28 - 32.
Walker P. Pediatric Adenoidectomy under vision using suction-diathermy ablation. Laryngoscope. 2001; 111 (12):2173-2177 - 33.
Martinez SA, Akin DP. Laser tonsillectomy and adenoidectomy. Otolaryngologic Clinics of North America. 1987; 20 :371-376 - 34.
Wan YM, Wong KC, Ma KH. Endoscopic-guided adenoidectomy using a classic adenoid curette: A simple way to improve adenoidectomy. Hong Kong Medical Journal. 2005; 11 (1):42-44 - 35.
Lo S, Rowe-Jones J. How we do it: Transoral suction diathermy adenoid ablation under direct vision using a 45 degree endoscope. Clinical Otolaryngology. 2006; 31 (5):436-455 - 36.
Al-Mazrou KA, Al-Qahtani A, Al-Fayez AI. Effectiveness of transnasal endoscopic powered adenoidectomy in patients with choanal adenoids. International Journal of Pediatric Otorhinolaryngology. 2009; 73 (12):1650-1652 - 37.
Costantini F, Salamanca F, Amaina T, Zibordi F. Videoendoscopic adenoidectomy with microdebrider. Acta Otorhinolaryngologica Italica. 2008; 28 (1):26-29