Open Access is an initiative that aims to make scientific research freely available to all. To date our community has made over 100 million downloads. It’s based on principles of collaboration, unobstructed discovery, and, most importantly, scientific progression. As PhD students, we found it difficult to access the research we needed, so we decided to create a new Open Access publisher that levels the playing field for scientists across the world. How? By making research easy to access, and puts the academic needs of the researchers before the business interests of publishers.
We are a community of more than 103,000 authors and editors from 3,291 institutions spanning 160 countries, including Nobel Prize winners and some of the world’s most-cited researchers. Publishing on IntechOpen allows authors to earn citations and find new collaborators, meaning more people see your work not only from your own field of study, but from other related fields too.
To purchase hard copies of this book, please contact the representative in India:
CBS Publishers & Distributors Pvt. Ltd.
www.cbspd.com
|
customercare@cbspd.com
Tonsils are lymphoid tissues in the oral cavity and nasopharyngeal region arranged in Waldeyer’s ring. The Waldeyer’s ring consists of pairs of pharyngeal (adenoids), tubal, palatine, and lingual tonsils. These are usually hyperplastic at a younger age and decrease with age. However, asymmetric enlargement might be a sign of pathology. It could be due to tonsillitis, abscess, and benign tumors, such as fibromas, teratomas, and angiomas such as lymphangioma, hemangioma, and inclusion cyst. Benign tumors of the tonsils are usually rare but not uncommon. It could be due to malignancies such as lymphoma, squamous cell carcinoma, or metastasis. This chapter focuses on clinical, histopathological and radiographic features of benign and malignant tumors of palatine and lingual tonsils.
Oral Diagnostic Sciences, Virginia Commonwealth University School of Dentistry, Richmond, Virginia, USA
Shravan Renapurkar
Oral and Maxillofacial Surgery, Virginia Commonwealth University School of Dentistry, Richmond, Virginia, USA
Sonam Khurana
Department of Oral and Maxillofacial Pathology, Radiology and Medicine, New York University College of Dentistry, New York, USA
*Address all correspondence to: vaddia@vcu.edu
1. Introduction
Tonsils are developed from the second branchial cleft. This location corresponds to the intersection of oral epiblast and intestinal hypoblast. According to embryology, an organ formed from combining two different tissues has more potential for neoplastic growth [2]. Although benign and malignant tumors of the tonsillar region are more common, there is very scarce literature regarding the definitive classification of tonsillar tumors. In the WHO classification of tumors of the oropharynx, tonsillar tumors are included along with the base of the tongue and adenoids. This chapter focuses exclusively on palatine and lingual tonsillar tumors. These tumors are comprehensively classified according to the histologic nature of the lesion (Table 1).
Benign tumors of the tonsils are rarer than malignant tumors. Most benign tumors of the tonsils are reported in the younger age group. Most patients are asymptomatic, and a benign tumor is often detected as an incidental finding. Other clinical symptoms include the presence/sense of mass, sore throat, and difficulty swallowing/breathing. Most benign tumors of the tonsil manifest in the form of a polyp, and clinical signs and symptoms are identical. The histopathological examination provides a definitive diagnosis of the lesion based on the tissue of origin. Table 1 provides a list of benign tumors. The clinical features of common benign tonsillar tumors are discussed below.
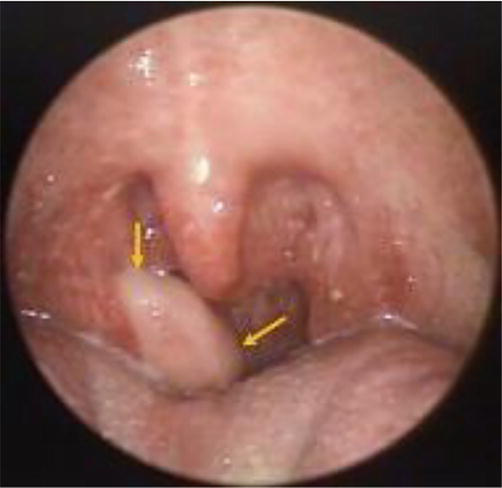
These present as a polypoid mass attached to the tonsil. It may be sessile/pedunculated (Figure 1). The patient recognizes mass after it attains a specific size and interferes with functional movements such as deglutition. The most common clinical features include pale pink color, lymphadenopathy, and asymptomatic lesion. However, patients might present with cough or foreign body sensation. Reports of airway obstruction due to benign tonsillar mass are scarce. The rate of malignant transformation is significantly less.
Figure 1.
Well-defined, smooth-surfaced fibroepithelial polyp (yellow arrows) arising from the superior pole of the right palatine tonsil [3]. Source: https://www.ncbi.nlm.nih.gov/pmc/articles/PMC8556748/. License: https://creativecommons.org/licenses/by/4.0/.
Histopathology: Most tonsillar fibromas demonstrate stratified squamous epithelium with fibrous/collagenous stroma.
Lymphangiomatous polyps are congenital tumors of the lymphatic system. They are hamartomatous malformations. They are present at birth or manifest in early life (Figure 2). The clinical presentation would be similar to a fibroma. Bilateral occurrence is rare, although few cases are reported in the literature [5].
Figure 2.
Pedunculated polyp of lymphoid origin in the right palatine tonsil [4]. Source: https://www.hindawi.com/journals/crim/2011/183182/. License: http://creativecommons.org/licenses/by/3.0/.
Histopathology: Foci of well-organized lymphoid tissue would be present within the tonsillar mass.
2.3 Papilloma
It is one of the common benign neoplasms of the tonsil. Clinically they present as grayish-white exophytic lesions with a wrinkled surface. The lesions may be either sessile/pedunculated.
Histopathology: Papilloma has characteristic, multiple finger-like projections with hyperplastic squamous epithelium and fibrovascular core.
2.4 Lipoma
Lipomas are mesenchymal tumors of fat cells. They are seen less frequently in the head and neck region, especially the tonsillar area. They are benign, slow-growing tumors. The clinical presentation would be similar to other benign tumors. Lipomas can be lobulated. Extensive lipoma might cause airway obstruction.
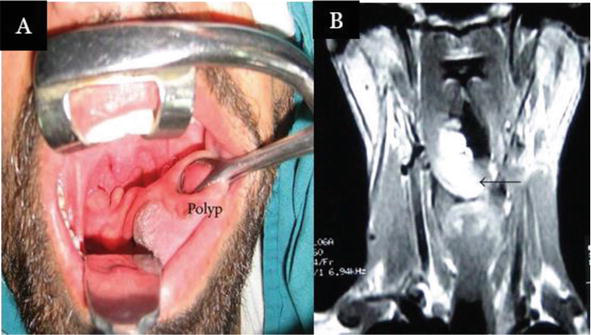
Imaging: Lipomas have characteristic computed tomography (CT) and Magnetic Resonance imaging (MRI) features. In CT imaging, they appear as well-defined, non-enhancing low, attenuation homogeneous lesions (Figure 3). MRI demonstrates a hyperintense lesion on both T1-weighted (T1W) and T2-weighted (T2W) images. Loss of the signal is evident in Fat-saturated images and STIR sequences. Both CT and MRI post-contrast images do not demonstrate enhancement of the lesion (Figure 4).
Figure 3.
Axial section of contrast-enhanced CT demonstrating a pedunculated lipoma arising from right palatine tonsil. Notice the non-enhancement of the lesion [6]. Source: https://www.eurorad.org/case/17083. License: http://creativecommons.org/licenses/by-nc-sa/4.0/.
Figure 4.
Clinical presentation of tonsillar lipoma (A) and coronal section of T2-weighted MRI image demonstrating hyperintense lesion (B) [7]. Source: https://www.hindawi.com/journals/crim/2014/480130/. License: http://creativecommons.org/licenses/by/3.0/.
Histopathology: Adipose tissue divided into lobules with collagenous septa and interspersed vascular channels. Histologically there are different variants of lipoma, such as fibro lipoma, chondrolipoma, and myolipoma.
2.5 Management of Benign tumors of tonsils
Most benign tumors, such as lipoma, fibroma, papilloma, and lymphangioma, present as polypoid masses. Tonsillectomy and surgical excision of the lesion, followed by histopathologic examination, is the most common treatment option. The definitive diagnosis is based on the predominant tissue in the excised specimen. Few cases can be managed with the excision of polypoid mass without tonsillectomy, especially if the polypoid mass is pedunculated [7]. There is less chance for recurrence and malignant transformation of benign tumors of the tonsils. The prognosis is usually good for benign tumors.
Oropharyngeal (OP) cancers include tumors arising from the palatine tonsil, the base of the tongue, the walls of the pharynx, and the soft palate. Palatine tonsils constitute lymphoid tissue embedded in the tonsillar fossa located in the lateral walls of the oropharynx between the tonsillar pillars. Palatine tonsils cancers comprise tumors of the anterior and posterior tonsillar pillar, tonsillar fossa, and plica triangularis. The lingual tonsil constitutes lymphoid tissue in the base of the tongue. Lingual tonsillar cancers comprise tumors of the base of the tongue.
Tonsilar squamous cell carcinomas (SCC) are the most common malignant tonsillar neoplasms, followed by non-Hodgkin’s lymphoma. Most oropharyngeal SCCs (OPSCC) are associated with human papillomavirus (HPV). Tobacco, smoking habits, iron deficiency, avitaminosis, and syphilis have been implicated as other etiology factors for tonsillar neoplasms. The overall incidence of Head and neck SCC (HNSCC) has been reducing since the 1980s due to declining smoking. However, there is a rapid increase in human papillomavirus (HPV) induced OPSCC in younger patients [8].
The presenting symptoms for most tonsillar neoplasms are sore throat, local pain, and the sensation of a mass in the neck. The tonsillar growth begins as a superficial granular ulcer in the tonsillar region. Eventually, the ulcer erodes the surface. They produce a submucosal mass with or without surface ulceration. Tonsillar tumors might spread to alveolar ridges and buccal mucosa. Tonsillar neoplasms metastasize to uni/bilateral lymph nodes and present as lymphadenopathy. Radiating pain in the ear is characteristic of advanced tonsillar malignancy. During initial medical diagnosis, most malignant tonsillar tumors are in advanced stages or extended beyond the tonsil. The poor tactile sensation in the tonsillar region compared to the oral cavity could be the reason for the occult nature of tonsillar malignancies [9].
Both carcinomas and lymphomas present as asymmetric enlargements of the tonsil. It is challenging to differentiate from clinical examination. Some lymphomas present as bilateral tonsillar masses. There is conflicting literature regarding the excision of unilateral asymmetric enlarged tonsils without other suspicious features of malignancy. However, a tumor should always be considered in the differential diagnosis of these cases, and judicious follow-up is recommended [10].
3.1 Squamous cell carcinoma (SCC)
Due to the inherent lack of afferent lymphatic channels, carcinoma in the tonsils is likely a primary malignancy rather than metastasis [11].
Tonsillar pillar SCC: The most common locations for primary tonsillar SCC are the anterior tonsillar pillar and the tonsils. The palatoglossus muscle forms the anterior tonsillar pillar. The anterior tonsillar pillar tumors may spread to masticator space. In such cases, patients might experience pain and trismus due to the involvement of pterygoid muscles. The tumor can spread anterolaterally to involve pharyngeal constrictors, pterygomandibular raphe, and retromolar trigone region of the oral cavity. The anterior tonsillar pillars drain into the level I, II, and III nodes. The majority of patients will have nodal involvement at the initial presentation.
The palatopharyngeus muscle forms the posterior tonsillar pillar. Tumors in this region can spread to the soft palate, thyroid cartilage, pterygomandibular raphe, and oral cavity. The posterior tonsillar pillar drains only into level II nodes. But if a tumor spreads to the oropharynx, this region drains into level V and retropharyngeal nodes [12].
Tonsillar fossa SCC: Tumors of the tonsillar fossa are often occult. In this region, the tumor can spread to the parapharyngeal, carotid, and masticator space, the tonsillar pillars, and the gnathic region. The tonsillar fossa drains into the level I to IV nodes.
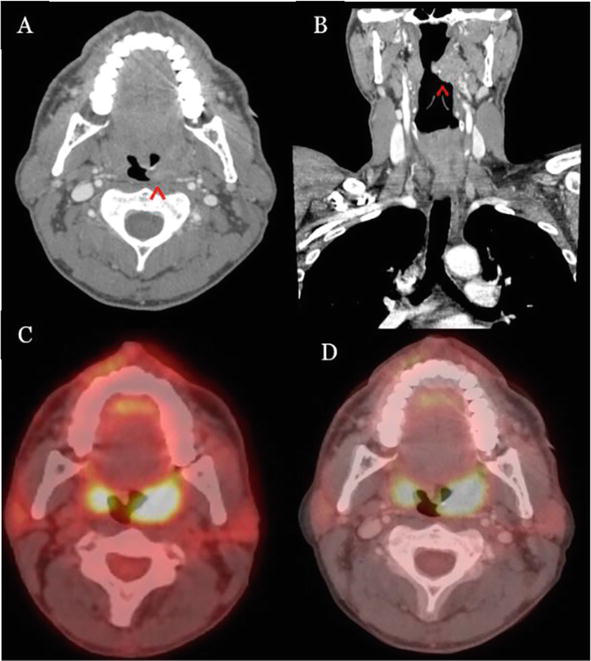
CT Imaging: A small squamous cell carcinoma lesion is difficult to delineate from the surrounding normal tissues on CT imaging. The large lesions are usually exophytic and invasive. The contrast-enhanced CT (CECT) typically presents with heterogeneous uptake. Positron emission tomography (PET)/CT imaging demonstrates the extent of the tumor and helps in treatment planning (Figure 5). If there is nodal involvement, the node appears enlarged, often round with central necrosis or entirely cystic.
Figure 5.
Bilateral tonsillar squamous cell carcinoma [13]: (A) Axial CT neck with contrast demonstrating left palatine tonsillar mass (red arrowhead) extending towards the midline; (B) Sagittal CT neck with contrast showing the medial extension of mass (red arrowhead) towards the uvula within the oropharynx; (C) Fluorodeoxyglucose (FDG) PET/CT axial view demonstrating increased radiotracer uptake in both the left and right palatine tonsils. But no soft tissue abnormality right palatine tonsil was noted in CT (Figure 5A and B); and (D) PET/Ct superimposed at 55% opacity for improved visualization of tumor margins in the oropharynx. Source: https://onlinelibrary.wiley.com/doi/10.1002/cnr2.1615. License: http://creativecommons.org/licenses/by/4.0/.
MRI Imaging: The typical characteristic of SCC is enlarged tonsils that appear isointense to hypointense on T1W images relative to normal lymphoid tissues. These characteristics on T1W make it challenging to differentiate from muscles. On T2W images, the tumor appears hyperintense, which helps to distinguish it from surrounding lymphoid tissues. On T1W with gadolinium administration, the tumors show marked enhancement due to the uptake of the contrast. Most often, tumors are diagnosed when they progress to stage 3 or 4. The reason for delayed diagnosis could be normal asymmetric variation in the shape and contour of the tonsils. It is generally hard to differentiate tonsillitis from an early malignancy, including carcinoma and lymphoma. The advanced stage SCC can invade adjacent anatomical structures such as the pharyngeal wall, palate, and tongue base, which helps differentiate from benign lesions. Contrast-enhanced MRI can differentiate malignant lesions due to their superior soft tissue resolution [14].
Histopathology: The epithelium of tonsils originates from ectoderm, and mesoderm and lymphocytes are populated in the crypts. The epithelial lining of both palatine and lingual tonsils and crypts is the stratified squamous epithelium and ciliated pseudostratified columnar for the pharyngeal tonsils. The origin of HPV and non-HPV-associated SCC is different. The SCC associated with HPV originates from the epithelium lining the crypts, whereas non-HPV originates from the tonsillar surface epithelium. The characteristic feature of SCC is squamous differentiation and invasion of the basement membrane. Due to invasion, it can extend to underlying tissues along with desmoplastic stromal reaction and inflammatory infiltrate. The inflammatory cells mainly include lymphocytes and plasma cells. The most common SCC are moderately-differentiated variants, showing nuclear pleomorphism and mitosis and less keratinization than the well-differentiated variety. The poorly differentiated type has predominantly immature cells with typical and atypical mitoses, less keratinization, and rarely necrosis [15].
Management: The treatment is based on the size of the tumor. Recently, Trans Oral Robotic Surgery (TORS) is a popular treatment option, followed by neck dissection and radiotherapy for nodal involvement. The T1 or T2 tumors are usually treated with chemotherapy, radiotherapy, and TORS with nodal dissection. Large tumors with extensive nodal involvement are mainly treated with chemoradiotherapy [15].
3.2 Lymphoma
Lymphoma accounts for the second most common malignancies of the head and neck. Most head and neck lymphomas are Hodgkin, and only 5% are non-Hodgkin. The tonsils are the most common site of non-Hodgkin lymphoma (NHL) in the head and neck region. The clinical symptoms of primary non-Hodgkin lymphoma of the tonsils include a sore throat or feeling of a lump in the throat, lymphadenopathy, dysphagia, and occasionally systemic symptoms such as fever, weight loss, and night sweats. It usually has a rapid onset with a short clinical course of a few weeks and predominantly occurs in the older age group.
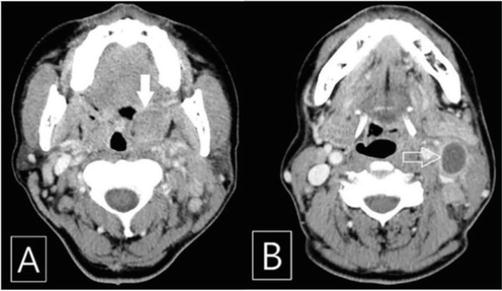
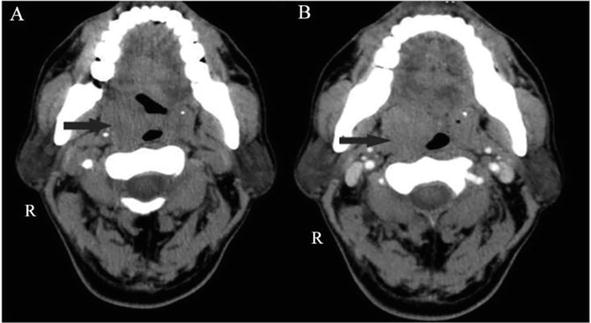
CT Imaging: On CT soft tissue window with contrast, lymphoma has a slightly homogenous enhancement, with density higher than muscle (Figure 6). In contrast to NHL, SCC shows heterogeneous enhancement due to necrosis and invasion of adjacent structures [17].
Figure 6.
Contrast-enhanced CT (CECT) scan of the patient. (A) Hypertrophic and slightly enhanced left palatine tonsil (solid arrow) and (B) enlarged ipsilateral cervical lymph node demonstrating central low attenuated lesion (arrow) [16]. Source: https://synapse.koreamed.org/articles/1129387. License: http://creativecommons.org/licenses/by-nc/4.0/34:78-82.
MRI Imaging: The T1W images show homogenous intermediate signals similar to normal tonsillar tissues, mild hyperintensity on T2, and minimal gadolinium enhancement on T1 contrast. The occasional, mild heterogeneous signal indicates areas of focal necrosis. Because signals of NHL are similar to normal tonsillar tissues, MRI is not a reliable imaging modality. MRI is primarily used to locate the tumor and detect nodal metastasis. Tonsillar lymphoma has a higher incidence of cervical node metastasis. Like SCC, lymphomas present as a round or lobulated exophytic mass. But unlike SCC, most lymphoma displaces adjacent structures rather than invasion. On an MRI, the presence of a large tumor that displaces the adjacent structure instead of invasion is highly suggestive of lymphoma [18].
Histopathology: According to WHO classification [19], 66–75% of lymphomas noted in the Waldeyer’s ring are diffuse large B-cell types. The other types, such as small lymphocytic, follicular large cell, lymphoblastic, Burkitt’s lymphoma, and peripheral T Cell types are rare.
Management: The treatment protocol is dependent upon the stage of the disease. The treatment includes radiotherapy alone or combined therapy for stages I and II occurring in the Waldeyer’s ring. The radiotherapy targets anatomic sites, including the nasopharynx, bilateral tonsils, soft palate, hard palate, and the root of the tongue. The lymph nodes included are cervical, supra, and sub-clavicular. Combined radio and chemotherapy improve the 5 years prognosis. For stages III and IV, chemotherapy is the primary treatment. The prognosis depends on the stage and whether the tumor is primary or recurrent. The low-grade NHL has a better prognosis, whereas recurrent and/or intermediate/high-stage NHL might recur beyond the primary site. Currently, combined chemo and radiotherapy are universally accepted treatment modalities [16].
3.3 Mucoepidermoid carcinoma (MEC)
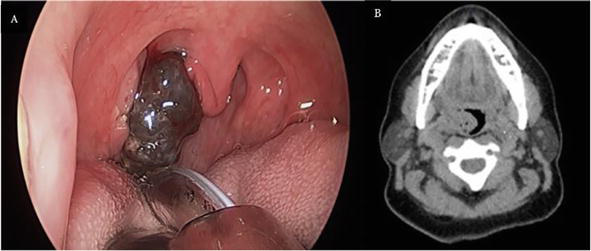
It is the most common primary salivary gland malignancy. It can occur in the minor salivary glands of the palatine tonsils. Patients might present with asymptomatic swelling that eventually progresses to an ulcerated mass. Few tumors present as fluctuant masses with a blue or red hue identical to mucocele.
CT Imaging: On CECT, low-grade lesions appear heterogeneous with well-defined margins. The mucous deposits show low-intensity areas similar to cysts. High-grade lesions have infiltrative, ill-defined margins with heterogeneous contrast uptake and nodal metastasis (Figure 7).
Figure 7.
Axial CT image demonstrating solid lesion of MEC with lobulated and ill-defined margins [20]. Source: https://www.hindawi.com/journals/crionm/2015/827560/. License: http://creativecommons.org/licenses/by/3.0/.
MRI Imaging: On T1W, low-grade lesions appear heterogeneous, well-defined mass with mainly low signals, and high-grade mass shows intermediate signals with infiltrative margins. On T1W with contrast, the lesion shows heterogeneous uptake with no uptake by mucous deposits. On T2W, the mucous deposits show hyperintense signals, like cysts. Low-grade lesions have heterogeneous signals, and high-grade lesions have intermediate signals with infiltrative margins.
Histopathology: Histopathology of palatine MEC demonstrates fragments of oral mucosa with non-keratinized stratified squamous epithelium showing dysplastic features such as atypia and mitotic figures. The lamina propria reveals features of glandular origin. A combination of mucous-producing cells and epidermoid (squamous cells). An intermediate progenitor cell is found in some cases. Immunohistochemistry is also a valuable diagnostic tool for salivary gland tumors.
Management: Tonsillectomy with total tumor excision is the treatment of choice for MEC. Some cases might require radical tonsillectomy and ipsilateral neck dissection based on the extent of the lesion. In advanced-stage cases, chemo and radiotherapy are used before or after surgery [20].
3.4 Adenocarcinomas
Most of the adenocarcinomas in the palatine tonsils are metastatic from the lung and gastrointestinal tract. In recent times, the number of tonsillar carcinomas associated with HPV 16 has increased, and most of them were SCC. There are few case reports of HPV p16-positive adenocarcinomas. HPV-associated adenocarcinomas occur in younger patients. They comprise less than 1% of all malignancies of palatine tonsils.
Imaging: Like other malignancies of the tonsillar region, CT and MRI are helpful in locating the extent and treatment plan of the adenocarcinoma. In one case report, standardized uptake values (SUVs) of the radiotracer were 14.2 for the tonsillar mass and 7.2 for retropharyngeal nodes in the initial PET scan. There was adenopathy of the cervical lymph nodes.
Histopathology: A few case reports have demonstrated tumor mass made up of glandular and cribriform structures centered around the tonsillar crypts. The cancer cells have a basaloid appearance with pleomorphic nuclei. Along with pleomorphic nuclei, vesicular chromatin and inconspicuous nucleoli were also noted. Sometimes cells grow in cystic spaces. Infiltration into underlying bone or muscle is noted in some cases. Perineural invasion can occur. Immunohistochemical staining helps in distinguishing adenocarcinomas from other salivary gland tumors.
Management: HPV-associated adenocarcinoma responds more to radiotherapy or surgery and has a better prognosis than non-HPV lesions. Usually, tonsillar cancers are diagnosed at advanced stages after distant metastasis. In such cases, extensive neck dissection with adjuvant chemo-radiotherapy has better outcomes. Immunotherapy has a good influence on the prognosis of tonsillar carcinomas [21, 22].
3.5 Melanoma
Primary mucosal melanoma accounts for 1.3% of cases in the head and neck region. In descending order, the primary sites in the head and neck region include the nose and paranasal sinuses, oral cavity, pharynx, and larynx. The oropharynx is not a common site of mucosal melanoma. Mucosal melanoma is more common in males than females; the average age is 61–65. Melanoma usually has a poor prognosis, so an early diagnosis has a better outcome.
Imaging: For diagnosis of melanoma, MRI is the modality of choice. The imaging features of MRI are more sophisticated than CT densities (Figure 8). The characteristic features of melanoma on MRI are attributed to melanotic pigment and hemorrhage within the lesion. T1W has hyperintense signals and hypointense on T2W due to the paramagnetic properties of melanin and free radicals produced by the metals within the pigment. Metastasis due to primary mucosal melanoma is difficult to diagnose. PET/CT helps assess the suspected metastasis due to the high fluorodeoxyglucose avidity.
Figure 8.
(A) Clinical image demonstrating extensive, pigmented exophytic lesion (metastasis to palatine tonsil from a cutaneous melanoma); and (B) Non-contrast CT axial section demonstrating exophytic right tonsillar mass [23]. Source: https://academic.oup.com/jscr/article/2022/2/rjac022/6524980. License: https://creativecommons.org/licenses/.
Histopathology: Primary mucosal melanoma has the characteristic presence of proliferation of malignant melanocytes. The malignant melanocytes have variable phenotypes, viz. plasmacytoid, spindle, and epithelioid cells with hyperchromatic nuclei with prominent nucleoli. The malignant cells display high mitosis and invasive patterns to submucosa and destroy underlying tissues. Mucosal melanoma with mixed cell phenotypes is more prone to metastasis and vascular invasion.
Management: The recent guidelines for the treatment of mucosal melanoma dictates that localized cases without distant metastasis should be removed surgically with negative margins. If margins are positive, adjuvant radiotherapy and immunotherapy are treatments of choice. For cases with distant metastasis, combination immunotherapy is the first line of treatment, and chemotherapy is the second line of treatment [24].
3.6 Sarcoma
Tonsillar sarcomas are not very common. Unlike tonsillar squamous cell carcinomas, sarcomas grow rapidly and spread through visceral metastasis. The etiopathogenesis of sarcoma is unknown. Detailed knowledge of tonsillar anatomy is important to understand sarcoma’s signs and symptoms and decide on treatment. The superior boundary of the tonsils is formed by the junction of the soft palate and facial pillars and is inferiorly continuous as vallecula. Inferiorly, if lymphoid tissues are more, no line of distinction is present between facial and lingual tonsils. Tonsils are separated from the carotid sheath by the middle constrictor muscle of the pharynx. Tonsils are not directly attached to the anterior pillar or the plica triangularis. A fairly moderate size sarcoma at the superior aspect of the tonsils can cause displacement of the supratonsillar fossa. A larger mass at this site can cause displacement of the uvula and soft palate bulging. A large tumor mass at the inferior aspect can mimic an indurated fixed lymph node due to displacement of the tissues below the jaw angle. Tumor present between the superior and inferior extent (middle third) can be visualized by tongue depression.
Imaging: Computed tomography and magnetic resonance imaging (MRI) provides information about the extent and the tissue composition of sarcomas due to their heterogeneity in tissue types. For example, fibrosarcoma has intermediate intensities on both T1W and T2W images, and liposarcoma is hyperintense on T1 due to lipid component and intermediate on T2W. These modalities also help in the treatment planning and assessing the prognosis. Most tumors have clearly defined margins, either because of surrounding soft tissue planes or because of significantly different attenuation values from the surrounding soft tissue. On the CT scan, there was no correlation between the CT densities and the histologic type of the tumor (Figure 9).
Figure 9.
(A) CT scan demonstrating a well-circumscribed, homogeneously enlarged 4.6 × 2.5 × 2.5-cm right tonsil; and (B) post-contrast image demonstrating slight continuing heterogeneous enhancement [25]. Source: https://www.spandidos-publications.com/10.3892/ol.2014.2726. License: https://creativecommons.org/licenses/by-nc-nd/4.0/.
Histopathology: Sarcomas are malignant mesenchymal tumors that are rare in the tonsillar region. Tonsils are composed of three different types of tissues, viz. Squamous epithelium, reticular connective tissues, and lymphocytes. Lymphocytes and supporting reticulum of lymphoid tissues tend to differentiate into sarcomas of tonsils. The most common tumor types include fibrous histiocytoma, leiomyosarcoma, liposarcoma, fibrosarcoma, synovial sarcoma, epithelioid sarcoma, hemangiopericytoma, lymphangiosarcoma, and follicular dendritic cell sarcoma. The histological features vary based on the grade, type, and site of the origin.
Management: The mainstay of treatment of sarcomas is surgery, except in Ewing sarcoma and angiosarcoma cases. These sarcomas are responsive to chemoradiation or neoadjuvant chemotherapy. Larger size, metastasis, and positive margins have a poor prognosis. The sarcomas of the tonsils and/or head and neck region are a diverse group of malignant mesenchymal tumors. Their improved histological classification and combination treatment modalities are important to improve the prognosis and overall impact on the quality of life of the patients [26].
3.7 Metastatic malignancies
Metastasis to palatine tonsils is extremely rare. Only a few cases have been reported in the literature. The mechanism of metastasis is unclear. It could occur through the retrograde lymphatic spread, hematogenous or paravertebral plexus from lungs, or through direct inoculation of lung tumor through bronchoscopy. Physical examination might reveal swollen and edematous tonsils. The patient may have difficulty in breathing, pain, and discomfort. Tonsillar metastasis is often detected as an incidental finding during the routine oral examination. In some cases, the patient might have symptoms such as a sore throat and the sensation of a mass in the neck. Tonsillar metastasis can be uni/bi-lateral depending on the primary neoplasm [27].
Imaging: Imaging studies such as PET/CT are used to identify, diagnose, and stage metastasis to different organs.
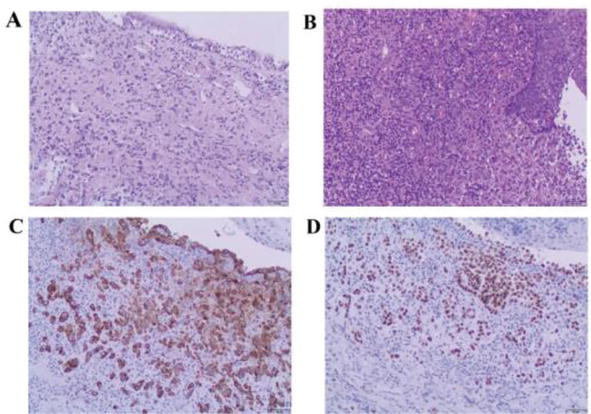
Histopathology: Histopathology provides a definitive diagnosis and information on the primary tumor of origin (Figure 10).
Figure 10.
(A) Respiratory columnar epithelium of the right medial main bronchus undermined by a poorly differentiated carcinoma with lymphovascular invasion hematoxylin and eosin staining (magnification, ×100); (B) Stratified squamous epithelium of the right palatine tonsil demonstrating histologically identical cancerous infiltrate (magnification, ×100); (C) Cytokeratin 7; and (D) thyroid transcription factor-1 positivity establish the diagnosis of metastatic pulmonary adenocarcinoma (magnification, ×100) [28]. Source: https://www.spandidos-publications.com/10.3892/mco.2018.1776. License: http://creativecommons.org/licenses/by/4.0/.
Management: A combination of surgery, radiotherapy, and chemotherapy are the treatment options depending on the extent and primary tumor of origin. There is no definitive treatment for metastatic malignancy of the tonsils, and the prognosis is poor [28].
3.8 Extramedullary Plasmacytoma (EMP)
Plasmacytomas are malignancies of plasma cells that primarily involve bone. Sometimes, plasmacytomas occur in soft tissues, called extramedullary plasmacytomas (EMP). These tumors are usually rare and occur mostly in the upper aerodigestive tract. EMPs are extremely rare in the tonsillar region. Clinical presentation includes painless mass, unilateral swelling in the tonsillar region, and lymphadenopathy. There are case reports of bilateral EMP. FNAC might be inconclusive in some cases due to difficulty in distinguishing from reactive lesions.
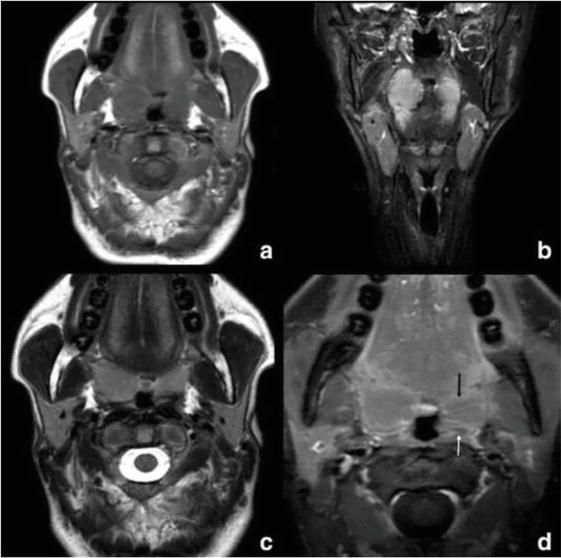
Imaging: CT, MRI, and PET/CT imaging provide information regarding the extent of the lesion (Figure 11).
Figure 11.
Tonsillar plasmacytoma: (a) Axial non-contrast T1W; (b) coronal STIR; and (c) Axial T2W and d. postgadolinium T1W with fat saturation MR images. The arrow in image d demonstrates the obliteration of the right palatine tonsillar crypts combined with linear horizontal enhancement to the left [29].
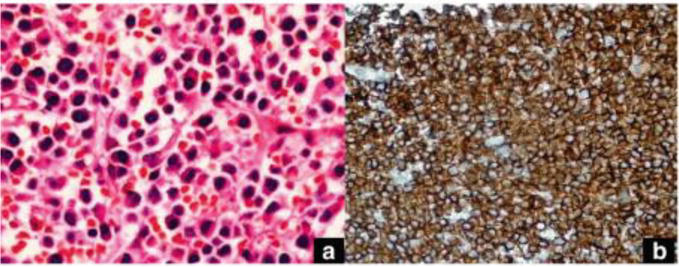
Histopathology: Effacement of normal tonsillar architecture and diffuse infiltration of sheets of neoplastic cells with plasmacytoid morphology (eccentric nuclei, cart-wheel appearance of nuclear membrane) (Figure 12).
Figure 12.
(a) Plasma cells with an eccentric nucleus and abundant cytoplasm (hematoxylin–eosin × 40); and (b) Diffuse cytoplasmic, focal membranous CD138 staining on the plasma cells (streptavidin-biotin peroxidase × 400) [29]. Source: https://bmcmedimaging.biomedcentral.com/articles/10.1186/s12880-018-0261-9. License: http://creativecommons.org/licenses/by/4.0/.
Management: Excisional biopsy of lesion for definitive diagnosis. Referral to a hematologist is recommended to rule out multiple myeloma. Solitary EMP is managed with a combination of surgery and radiotherapy. Periodic follow-up is recommended to monitor the recurrence and progression of the lesion as multiple myeloma [29].
Majority of benign tumors of the tonsils are managed with surgical excision of tumors with or without tonsillectomy. There is a low chance of recurrence and the prognosis is usually good for benign tumors. Early diagnosis and intervention determine the prognosis for malignant tonsillar tumors. The overall survival rate is better with HPV-positive tumors than with HPV-negative. The high survival rate in HPV-positive cases can be reduced by smoking. The other factors that help to improve prognosis include young age, localized tumor with lack of metastasis, and low comorbidities. CECT/MRI are recommended imaging modalities. The diagnosis of CECT sequences in the maxillofacial region is limited due to the streak artifact. The small primary mucosal tumors are difficult to diagnose; hence clinical evaluation is complimentary, and the thin CT sections help for better assessment. Underdiagnosing the primary lesion by failure to recognize invasion and lymph node metastasis can lead to poor prognosis. Careful evaluation of adjacent soft tissues and osseous structures, involvement of retropharyngeal lymph nodes on ipsilateral/contralateral sites, and detailed knowledge of anatomy are vital for better disease control and prognosis.
1.Hyams VJ. Differential diagnosis of neoplasia of the palatine tonsil. Clinical Otolaryngology and Allied Sciences. 1978;3:117-126
2.Hara HJ. Benign tumors of the tonsil: with special reference to fibroma. Archives of Otolaryngology. 1933;1:62-69
3.Marini K, Garefis K, Skliris JP, Peltekis G, Astreinidou A, Florou V. Fibroepithelial polyp of palatine tonsil: A case report. The Pan African Medical Journal. 2021;39:276
4.Balatsouras DG, Fassolis A, Koukoutsis G, Ganelis P, Kaberos A. Primary lymphangioma of the tonsil: A case report. Case Reports in Medicine. 2011;2011:31
5.Gan W, Xiang Y, He X, Feng Y, Yang H, Liu H, et al. A CARE-compliant article: Lymphangiomatous polyps of the palatine tonsils in a miner: A case report. Medicine. 2019;98(1)
6.Unzué G, Viteri G, Alberdi N, López P, de Llano L, Lage T, et al. Lipoma of palatine tonsil. Section head and neck imaging. Eurorad. 2020. DOI: 10.35100/eurorad/case.17083
7.Kanotra SP, Davies J. Management of tonsillar lipoma: Is tonsillectomy essential? Case Reports in Otolaryngology. 2014;2014:4
8.Filion E, Le QT. Oropharynx: Epidemiology and treatment outcome. In: Functional Preservation and Quality of Life in Head and Neck Radiotherapy. Berlin, Heidelberg: Springer; 2009. pp. 15-29
9.Martin H, Sugarbaker EL. Cancer of the tonsil. The American Journal of Surgery. 1941;52(1):158-196
10.Cinar F. Significance of asymptomatic tonsil asymmetry. Otolaryngology-Head and Neck Surgery. 2004;131(1):101-103
11.Heffner DK. Pathology of the tonsils and adenoids. Otolaryngologic Clinics of North America. 1987;20(2):279-286
12.Corey A. Pitfalls in the staging of cancer of the oropharyngeal squamous cell carcinoma. Neuroimaging Clinics. 2013;23(1):47-66
13.Rossi NA, Reddy DN, Rawl JW, Dong J, Qiu S, Clement CG, et al. Synchronous tonsillar tumors with differing histopathology: A case report and review of the literature. Cancer Reports. 2022;5(9):e1615
14.Weber AL, Romo L, Hashmi S. Malignant tumors of the oral cavity and oropharynx: Clinical, pathologic, and radiologic evaluation. Neuroimaging Clinics of North America. 2003;13(3):443-464. DOI: 10.1016/s1052-5149(03)00037-6
15.Rousseau A, Badoual C. Head and Neck: Squamous cell carcinoma: An overview. Atlas of Genetics and Cytogenetics in Oncology and Haematology. Mar 2012;16(2):145-155
16.Kim YC, Kwon M, Kim JP, Park JJ. A case of malignant lymphoma misdiagnosed as acute tonsillitis with subsequent lymphadenitis. Kosin Medical Journal. 2019;34(1):78-82
17.Wang XY, Wu N, Zhu Z, Zhao YF. Computed tomography features of enlarged tonsils as the first symptom of non-Hodgkin’s lymphoma. Chinese Journal of Cancer. 2010;29(5):556-560
18.King AD, Lei KI, Ahuja AT. MRI of primary non-Hodgkin’s lymphoma of the palatine tonsil. The British Journal of Radiology. 2001;74(879):226-229
19.Vardiman JW. The World Health Organization (WHO) classification of tumors of the hematopoietic and lymphoid tissues: An overview with emphasis on the myeloid neoplasms. Chemico-Biological Interactions. 19 Mar 2010;184(1-2):16-20
20.Teixeira LN, Montalli VA, Teixeira LC, Passador-Santos F, Soares AB, Araújo VC. Mucoepidermoid carcinoma of the palatine tonsil. Case Reports in Oncological Medicine. 2015;2015:15
21.Damato S, Thavaraj S, Winter S, Shah K. Human papillomavirus-associated adenocarcinoma of the palatine tonsil. Human Pathology. 2014;45(4):893-894
22.Sethi A, Sundermann J, Neeta P. Human Papillomavirus induced adenocarcinoma of tonsil: A rare entity. Clinical Oncological Case Report. 2022;5:2
23.Barton BM, Ramsey T, Magne JM, Worley NK. Delayed metastatic melanoma to the pharyngeal tonsil in an African American female. Ochsner Journal. 2019;19(2):181-183
24.Manolidis S, Donald PJ. Malignant mucosal melanoma of the head and neck: A review of the literature and report of 14 patients. Cancer. 1997;80(8):1373-1386
25.Lu ZJ, Li J, Zhou SH, Dai LB, Yan SX, Wu TT, et al. Follicular dendritic cell sarcoma of the right tonsil: A case report and literature review. Oncology Letters. 2015;9(2):575-582
26.O’Neill JP, Bilsky MH, Kraus D. Head and neck sarcomas: Epidemiology, pathology, and management. Neurosurgery Clinics. 2013;24(1):67-78
27.Bar R, Netzer A, Ostrovsky D, Daitzchman M, Golz A. Abrupt tonsillar hemorrhage from a metastatic hemangiosarcoma of the breast: Case report and literature review. Ear, Nose & Throat Journal. 2011;90(3):116-200
28.Zaubitzer L, Rotter N, Aderhold C, Gaiser T, Jungbauer F, Kramer B, et al. Metastasis of pulmonary adenocarcinoma to the palatine tonsil. Molecular and Clinical Oncology. 2019;10(2):231-234
29.Celebi İ, Bozkurt G, Polat N. Tonsillar Plasmacytoma: Clues on magnetic resonance imaging. BMC Medical Imaging. 2018;18(1):1-4
Written By
Anusha Vaddi, Shravan Renapurkar and Sonam Khurana
Submitted: 22 December 2022Reviewed: 16 January 2023Published: 17 February 2023
 Open access peer-reviewed chapter
Open access peer-reviewed chapter