Open Access is an initiative that aims to make scientific research freely available to all. To date our community has made over 100 million downloads. It’s based on principles of collaboration, unobstructed discovery, and, most importantly, scientific progression. As PhD students, we found it difficult to access the research we needed, so we decided to create a new Open Access publisher that levels the playing field for scientists across the world. How? By making research easy to access, and puts the academic needs of the researchers before the business interests of publishers.
We are a community of more than 103,000 authors and editors from 3,291 institutions spanning 160 countries, including Nobel Prize winners and some of the world’s most-cited researchers. Publishing on IntechOpen allows authors to earn citations and find new collaborators, meaning more people see your work not only from your own field of study, but from other related fields too.
To purchase hard copies of this book, please contact the representative in India:
CBS Publishers & Distributors Pvt. Ltd.
www.cbspd.com
|
customercare@cbspd.com
Recently we have coined the term 3Des (3D exoscopic surgery) to describe the use of the 3D Vitom Exoscope System for transoral surgery of oropharyngeal cancers. This surgical approach can also be employed for tonsillectomy performed for obstructive sleep apnea and recurrent tonsillitis. Decreasing pain, maintaining hydration, and minimizing the risk of post-operative hemorrhage has brought attention to novel surgical technique and instrumentation. The search for the most cost-effective, safe, and efficient modality that provides the maximum relief while minimizing morbidity is still ongoing. During the period from January 2022 to May 2022, 8 patients with recurrent tonsillitis were treated by tonsillectomy with the 3Des approach at our center. A comfortable transoral exposure of the tonsillar fossa and the excellent space to move the surgical instruments are the best features of this procedure, along with the great utility in the learning process, especially for residents, fellows, students.
In the last 3 years, some studies in the ENT literature have highlighted the emerging role of exoscopes with 3D technology mainly using the VITOM [1, 2, 3, 4]. The increasing application of 3D exoscopic technology worldwide is becoming remarkable. Exoscopic surgeries maintain the same safety profiles as those using previous surgical techniques and allow ENT surgeons to achieve better vision and illumination of small anatomic structures. In order to evaluate the exoscope potential in visualization, magnification, and dissection of deeper structures in the oral cavity we applied the 3D Vitom Exoscope System for tonsillectomy.
2. History of tonsillectomy from literature review
Tonsillectomy is one of the most commonly performed surgical procedures worldwide and since the original description of tonsillar tissue removal by Cornelius Celsus in the First century AD, a lot of tonsillectomy techniques have been performed to decrease complications and post-operative morbidity.
The uvulotomy performed in the sixteenth century for the treatment of acute catarrhal inflammation can be considered the forerunner of tonsillectomy. This procedure inspired the scientists of the time to design suitable tools for tonsillectomy that were able to remove tonsils with a method that involved as few steps as possible to reduce complications such as the dreaded hemorrhage.
The first instrument so consisted of a metal wire which allowed the removal of the tonsil by strangulation of it. However, the operation was technically complex, took a long time, needed the management of copious bleeding, and allowed only partial excision of the tonsil which, in most cases, grew back causing recurrence. For this reason, it was during the nineteenth century that increasingly sophisticated instruments were developed to remove all the tonsil tissue in a single step. To the famous Greenfield Sluder (Washington, 1865–1928) we must give the honor of the invention of the guillotine technique made by a futuristic instrument very similar to the uvulotome used ages ago, that drastically changed the fate of patients. According to this procedure, the tonsil, placed inside the instrument, is excised from the base through a guillotine blade actioned by the surgeon. It became very famous at that time (and it’s still largely used in some centers) because it was quick, almost painless, and easy both for the surgeon and for the patient, and last but not least, it responded to the knowledge and anesthesiological availability of the time. The Guillotine excision also known as the Sluder technique, despite many advantages, reported also disadvantages such as the lack of control of blood loss, a not residual tonsil tissue, accidental uvulectomy, partial accidental glossectomy, and pillar damage, as well as blood aspiration into the lower respiratory trees [5].
Soon it became clear that surgeons must look for a more anatomical and systematic approach to tonsillectomy. It’s in this background that Samuel Crowe, Director of the Department of Otolaryngology at Johns Hopkins Hospital in Baltimore, stood out. Between 1911 and 1917, he performed 1000 operations with a new method and a much more cautious approach to the patient, which would inevitably revolutionize the surgical procedure: the patient was hospitalized and in the preoperative period he underwent blood tests (until then the tonsillectomy was performed during the day, without preoperative tests) and a “sharp dissection” with a scalpel was performed [6]. Above all, the position of the patient was revolutionary, with the bottom of the operating bed lower, the anesthetic gas administered through a mask, and the patient’s mouth kept open with an instrument that took its name from the same surgeon (Crowe-Davis mouth gag) with the property of keeping the tongue retracted and motionless; the hemostasis is accurate and all the hemorrhagic points tied with black suture and finally, in the post-operative period the patient is not discharged until any complications are resolved.
Ideally, tonsillectomy should be a procedure that is as fast as possible, bloodless, painless, and susceptible to prompt recovery. Post-operative pain after tonsillectomy is one of the most important causes of morbidity restricting oral intake, causing dehydration and daily activity limitation [7]. In addition, restriction of the pharyngeal muscle activity due to pain, leads to a reduction in the clearance of the tonsil bed and, as a consequence of this, to infection and bleeding [8]. In 2009, some Authors [9] systematically analyzed the usefulness of the literature of the past 20 years concerning tonsillectomy technique in children and found deficits in the precise reporting of surgical techniques, adequate study design, and useful outcome measures, all of which making the literature less useful than it could be. According to the Author, the recent advances in technology, with aggressive marketing both to physicians and patients, have created additional dilemmas in clinical decision-making as far as which method of tonsillectomy will best serve the patient is concerned. As a consequence of this, many Authors suggested guidelines for studying design parameters which could lead to more valuable information for the clinician to choose the best technique for the patients.
Nowadays, the main classification of surgical tonsillectomy by dissection divides conventional and cold techniques from new hot techniques. The former includes the cold knife technique, cold dissection, sharp dissection, steel dissection, blunt dissection, snare tonsillectomy, and dissection-ligation technique. The latter, include monopolar or bipolar diathermy tonsillectomy, laser dissection (mainly represented by CO2 laser, ultrasonic dissection, radiofrequency tonsil ablation (coblation and ligasure tonsillectomy) and microdebrider tonsillectomy. In the matter in question, hot techniques, improving hemostasis, have soon replaced cold dissection techniques for most surgeons. They combine the possibility of performing cut and coagulation simultaneously taking advantage of the use of the most recent technological innovations. Due to their diffusion, versatility, and contained cost, the monopolar and bipolar electrodissections are the most used tools in tonsillectomy operations worldwide.
As far as the monopolar electrodissection is concerned, the current technical characteristics of monopolar electrodissection were instead developed simultaneously by Hall and Mann in 1984. According to them, the operation is carried out with flat-tip or sharp-tip electrosurgical units, maintaining an intensity equal to slightly higher than 20 watts (the range can however vary from 10 to 40 watts) [10]. This technique results in greater dissection precision and less intraoperative bleeding. It’s perhaps the most widely used variety of tonsillectomy, so much so that in 2003 it was described by Kay and Koltai as probably the most popular method in the USA, above all due to the advantage of the short duration of the procedure and, indeed, the minimum losses intraoperative blood pressure [11] as well as for the variety of its operative tips.
It should be kept in mind that monopolar diathermy acts at a very high temperature, equal to or higher than 400°C 35, splitting the tissues thanks to the use of a radiofrequency electric current, which is transferred directly from the electrode to the tissue [12]. Similarly to bipolar and laser electrosurgery, it allows cutting and hemostasis at the same time, through overheating of the tissues generated by the resistance they oppose to the passage of the current. The heat is then able to cause cell rupture, due to a drying phenomenon, and to form a clot that obliterates the small vessels, through protein denaturation [13].
Depending on the wattage adopted (as mentioned, a power close to 20 watts is suggested), the dispersion of energy in the tissues is considerable, in particular, due to the distance between the operating electrode and the dispersive “grounding” pad. The result is large lateral damage. As a consequence of this, post-operative pain and even deferred hemorrhage episodes constitute a problem for this technique that should not be underestimated [14]. However, these aspects were not confirmed by studies by some surgeons thanks to the use of Erbe electrosurgery generator (ERBE USA). This device, contrary to what occurs in conventional systems, is characterized by the production of current at constant voltage and variable power. It is placed in theory in an intermediate position between monopolar and bipolar diathermy and can coagulate causing less thermal damage, compared to traditional monopolar electrosurgery [15].
In the study they conducted, the authors observed in particular, in the Erbe group compared to the control group, a significant reduction in pain symptoms, which was however associated with greater intraoperative bleeding and prolongation of surgical times. The application of bipolar diathermy to tonsillectomy started in the 1990s.
Initially used only for the control of hemostasis but in 1994 it was proposed as a true method of dissection. In Pang’s original presentation, straight pincers with fine points were used, with the intensity of the current regulated at 30 watts [16]. Once the correct peritonsillar cleavage plane has been identified, we proceed with a practically bloodless dissection with the possibility of identifying and coagulating in a preventive and focused way most of the blood vessels afferent to the tonsil.
The introduction of bipolar electrodissection made it possible to reduce the intensity of post-operative pain, compared to the monopolar variety, thanks to the coagulation precision of the diathermic clamp, which, by transferring energy to a very limited surface, as it is included between two proximally coupled electrodes, can minimize the depth of tissue thermal damage [17]. Compared to the “hot” monopolar technique, the operation takes longer, also due to the frequent need to clean the tips of the forceps.
This drawback can be partially overcome with the use of special non-adhesive (non-stick) pliers in nickel. In bipolar diathermy, direct contact between electrodes and tissue produces a local temperature generally between 150 and 400°C, with overheating of the cellular content and consequent cellular vaporization. As regards the intensity of post-operative pain, from the investigation by Silveira et al. [18] a statistically insignificant increase emerged, particularly after the 3rd day.
In recent years, intracapsular tonsillectomy has been proposed as an alternative technique to total tonsillectomy. It consists of the resection of all the extra-velic portion of the tonsil which protrudes from the lodge: in practice, the operation will involve a drastic and progressive leveling of the profile of the tonsillar parenchyma, up to the free edge of the palatine pillars. The reason for this rediscovered interest about it is that, by preserving the tonsil capsule, it is possible to reduce post-operative pain significantly if we compare it to conventional tonsillectomy.
It can be performed with many methods such as laser, monopolar diathermy with flat tip electrode, ultrasound scalpel, plasma scalpel, and microdebrider but since it’s reserved only for cases of obstructive tonsillar hypertrophy with sleep apnea, the discussion about intracapsular tonsillectomy goes beyond the aim of this chapter and will be debate elsewhere.
Tonsillectomy was widely practiced in the western world as a procedure to cure a vast range of conditions from respiratory tract infections to chronic systemic diseases throughout the twentieth century [19].
In our time, the indiscriminate use of tonsillectomy that was made in past years has diminished. This was due to an increased awareness of the natural history of pharyngotonsillar infections which, together with the use of targeted antibiotic therapy and the development of specific immunomodulatory therapies, led to the creation of sophisticated and shared guidelines among ENT specialists and pediatricians.
According to clinical practice guidelines developed by the American Academy of Otolaryngology—Head and Neck Surgery Foundation and the last Italian Guidelines written in the document “Clinical and organizational appropriateness of tonsillectomy and/or adenoidectomy operations” the indications of tonsillectomy are recommended as follows:
Airway Obstruction
Obstructive sleep apnea,
Feeding problems,
Hypernasal speech secondary to enlarged tonsils.
Infections
Recurrent tonsillitis,
Peritonsillar abscess,
PFAPA (Periodic Fever, Aphthous stomatitis, Pharyngitis and cervical Adenitis) syndrome.
Others
Asymmetric enlargement with suspicious of neoplasm.
Main contraindications are:
Acute tonsillitis: Acute infectious pathology of the tonsils or upper respiratory tract may cause an increased risk of bleeding or surgery-related pulmonary complications.
Age: Tonsillectomy is not recommended before 5 years of age for:
We report our preliminary results on eight tonsillectomies performed between 06 January 2022 and 31 May 2022 non-consecutively at a single ENT Department using the 3Des approach (San Giovanni Bosco Hospital ENT Department, Turin).
The median patient’s age was 21 years (15–28 years).
The gender distribution was 5 females vs. 3 males.
There were no exclusion criteria.
The patient cohort shows a history of recurrent tonsillitis in all cases and a history of drainages of parapharyngeal abscesses in three cases.
All the 8 operated patients had undergone previous antibiotic treatment for their disease for various exacerbations.
Three had undergone one or more parapharyngeal abscesses drainages (Table 1) under local anesthesia.
Age (median 21 years)
28 ♀
25 ♂
16 ♀
18 ♂
21 ♀
15 ♀
23 ♀
Female
*
*
*
*
*
Male
*
*
Recurrent infection
*
*
*
*
*
*
*
Previous parapharyngeal abscesses drainages
* (1)
*(2)
*(3)
Table 1.
Tonsillectomy group demographics.
The procedure was performed under general anesthesia by nasopharyngeal intubation.
The patient was placed in the supine position without any interscapular support.
The mouth was held open using a Boyle Davis mouth opener.
The VITOMR 90°, mounted on a mechanical support and fixed to the operating table between 25 and 50 cm from the operating field, was connected to a camera and a light cable, while the 3D monitor(s) (which could be single or multiple) were positioned in front of the operators (Figure 1).
Figure 1.
3D monitor position.
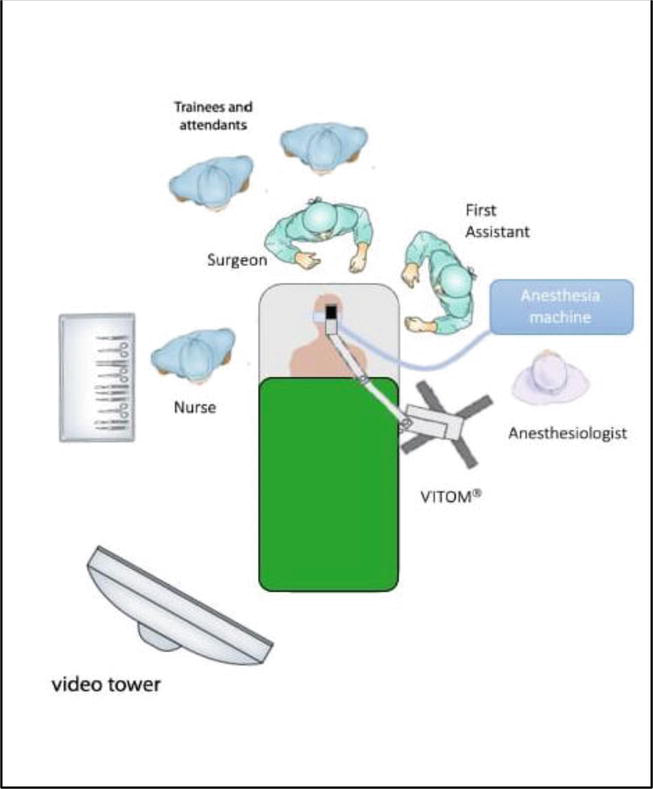
The second operator was positioned to the left or right of the first one depending on the side of the lesion, while the scrub nurse and the various trainees were positioned behind the first operator (Figure 2).
Figure 2.
Operating room setting (VITOM® Exoscope).
This setting allows everyone to follow carefully the procedure, looking at the surgical field projected onto the 3D monitor (Figure 3) .
Figure 3.
Surgical team looking at the surgical field projected onto 3D monitor.
Trainees can follow step by step the procedure, then they can try to perform the procedure under constant supervision by a senior surgeon, who could follow the trainees step by step thanks to the exoscopic view.
The excision was performed using the electrocautery (Force TriVerse Electrosurgical Device, Covidien, Dublin, Ireland).
The electrical current creates a temperature from 400 to 600°C allowing dissection with minimal intraoperative bleeding.
Sixteen tonsillectomies were assessed in 8 patients from 15 to 28 years of age. Of the patients, 5 (62.5%) were female and 3 (37.5%) were male. The mean age of the patients was 20.87 (min–max: 21–36).
There was no significant occurrence of post-operative complications including post-operative fever, voice changes, ear and neck pain, immediate or delayed hemorrhage, and suture placement. Three patients reported post-operative bleeding, with a minimal amount of blood, and had spontaneous resolution with no intervention. No patient required to return to the operative room for delayed bleeding. No residual tissue was seen in any of the patients (Table 2).
Age (median 21 years)
28 ♀
25 ♂
16 ♀
18 ♂
21 ♀
15 ♀
23 ♀
Voice changes
Ear and neck pain
Immediate hemorrhage with spontaneous resolution
*
*
*
Delayed hemorrhage
Suture placement
Table 2.
Results.
The mean operation calculated as the time from the mouth gag to removal was 23 ± 5.6 minutes.
No preoperative and/or post-operative anesthetic or analgesic drugs were injected into the tonsils. Patients were kept in the hospital for 24 hours for post-operation observation; all patients were discharged with stable vital signs and provided oral feeding. Patients were questioned for pain on post-operative day 1 and all the patients were discharged on post-operative day 1.
Outpatient follow-up included one visit every week for the first month. During the visit, we investigated the presence of bleeding episodes, the pain degree, and nutrition. All patients reported excellent subjective well-being, no bleeding episodes, and slight pain when feeding in the first two weeks.
On every visit, we performed an oropharyngeal examination through which we observed a regular fibrin formation at the tonsillectomy site.
Optimal vision and ergonomics are important factors contributing to the achievement of good results during transoral surgery. Everyone knows the surgical difficulty of this district in the past when two surgeons had to working together in a narrow space, made even tighter by the presence of anesthesia equipment and with limited lighting possibilities.
Modern instruments make it possible to overcome the surgical difficulties related to factors such as uncomfortable posture and poor visibility in a very difficult anatomical district such as that of the oral cavity. Naturally, all of this favors the surgical result and minimizes the dreaded complications such as hemorrhagic complications.
Nowadays transoral tonsillectomy under naked eye is the most common procedure performed. However, this procedure does not allow an enlargement of the surgical field and this entails on the one hand the persistence of an always very high risk of bleeding especially in cases of particular anatomical narrowness of the oral cavity and on the other hand the extreme difficulty for neophyte surgeons and trainees to learn the surgical technique well from the expert surgeon who is unable to share the operating field with them. To overcome these problems, the robotic technique TORS [20] and recently endoscopic tonsillectomy [21] have been proposed to replace conventional transoral tonsillectomy, the latter with apparent interesting benefits and low costs. On the contrary, as far as TORS is concerned, the high cost of the equipment strongly limits its use in the field of benign pathology.
As far as tonsillectomy is concerned, the operating exoscope has been recently introduced and has proven to be a promising and effective tool for transoral surgery. It is in this context we coined the term 3Des (3D exoscopic surgery) to describe the use of the 3D VITOM® Exoscope System for transoral surgery especially tonsillectomy performed for obstructive sleep apnea and recurrent tonsillitis.
VITOM is the acronym for Video Telescope Operating Microscopy 3D (VITOM®—Karl Storz GmbH, Tuttlingen, Germany). Introduced in the first decade of 2000, it is an exoscope that combines 4 K resolution view with three-dimensional technology. This device is well-known and widely employed in other surgical fields such as neurosurgery, urology, and gynecology. Its introduction in head and neck surgery is quite recent but it’s reaching even greater importance over time. At the moment, it is chosen in numerous otolaryngology subspecialties, such as laryngology, otology, skull base surgery, head and neck reconstruction, and of course intraoral surgery. The exoscope consists of a high-definition (HD) or 4 K (Ultra HD) 3D video camera (0° or 90°) with optical and digital zoom integrated and a fiber optic-delivered or L.E.D. light source [22]. Zoom and, focus functions and integrated illumination can be upgradeable using a double cable and light source.
This system, being covered by a sterile sheath making it suitable to be placed proximal to the area where the surgical procedure takes place, is suspended above the surgical field with a manually actuated articulating holder or robotic arm, and it is connected to a 3D monitor (55′′), with a maximum screen resolution and 16:9 image format. 3D passive-polarized glasses, with anti-fog coating, or 3D clip-on glasses, circularly polarized, are worn by all staff in the operating room (OR) to view the monitor. The combination of the VITOM® system with the 3-chip sensor technology in the camera head enables excellent image quality and optimal color rendering even in non-optimal lighting conditions. The magnification power of 8–30x is possible through the 3D camera, depending on the working distance, and the size and resolution of the monitor used, while the depth of field ranges from 7 to 44 mm, with a focal distance of 20–50 cm, allowing the surgical field to be observed and illuminated at various distances from the patient. Different directions of view are possible depending on the surgical site. For tonsillectomy, 0° is considered the best option.
A comfortable transoral exposure of the lesion is sought to visualize the lesion and its boundaries completely and to have sufficient space for moving the surgical instruments. Therefore, different types of autostatic retractors can be used. For example, Boyle Davis mouth gag, with its set of tongue depressors of varying sizes supplied along with the gag, holds the tongue thereby preventing it from falling into the surgeon’s field. Long surgical instruments from 24 to 30 cm need to be used because of the depth of the structures to be reached. Different kinds of cutting instruments could be used (bipolar forceps, CO2 fiber laser, ultrasound tools), and various types of angled tools were also required.
Concurrent hemostasis shortens surgical time; however, increased delivery of energy results in increased pain and odynophagia. Additionally, because of the monopolar current applied to the patient, electrocautery may interfere with or damage pacemakers, vagal nerve stimulators, and cochlear implants.
The value of transoral surgery with the 3D exoscope appears incredible in the field of surgical education of neophyte surgeons and trainees who have the opportunity to actively participate in all the surgical steps in real time, realizing the difficulties and possible complications.
The visual accuracy allows on the one hand the minimization of the dangerous bleeding complications as the identification of the small vessels is made absolutely easy and on the other hand a better accuracy in the removal of the tonsillar parenchyma avoiding injury to the surrounding tissues and reducing painful post-surgical complications.
The 3D exoscope provides surgeons with a feasible and potentially excellent alternative to traditional operating microscopes and endoscopes in head and neck surgery. Producing a high-quality video of small surgical fields, with high magnification capacity and a large depth of field, allows working in a setting that is similar to endoscopic surgeries but, unlike endoscopes, the 3D exoscope allows you to appreciate the depth and volume of anatomical structures and has a greater focal distance with a wider working space and the possibility of easy adjustment of vision. The VITOM 3D, given its excellent ability to provide three-dimensional images, depth of field, quality, and fidelity of the color and contrast of the image, is competitive in the 3D visualization of the operating field with the da Vinci robotic platform.
At present, the main disadvantages of the exoscope are represented by the mechanics of the supporting arm (it is not always comfortable to move during surgery) and the need to wear 3D glasses for a long period. Although tonsillectomies remain one of the most commonly performed surgeries in otorhinolaryngology, there is an absence of universal agreement on the surgical method and extent of removal [2]. The potential for significant morbidity, even death is inherent in the procedure. The operating exoscope with a digital camera system provides a high-definition image of the surgical field projected in a three-dimensional (3D) high-definition monitor. It allows the surgical team to operate by visualizing the magnified image of the surgical field on a screen. Recently we have coined the term 3Des (3D exoscopic surgery) to describe the use of the 3D Vitom Exoscope System for transoral surgery of oropharyngeal cancers. This surgical approach can also be employed for tonsillectomy. We performed eight tonsillectomies using this surgical approach. All the surgical steps were performed using the VITOM 3D exoscope.
The term 3Des (3D exoscopic surgery) was coined to describe the technique used for transoral surgery with the exoscope system as visual tool. The use of the exoscope enhanced the visualization of the oral cavity, thus facilitating the effectiveness of obtaining adequate surgical spaces avoiding damage to contiguous anatomical structures and giving the surgeons the possibility to maintain a more ergonomic posture [23]. The surgeon can choose to stay in a sitting or standing position, having the screen in front at the same height: the screen is placed frontally, and at the same height as the operators’ eyes. This system ensures also an extensive surgical field visualization by the second surgeon and the best coordination between surgeons and nurses. Indeed, in the conventional approach, a possible disadvantage of the procedures was related to the poor precision of the second surgeon’s movements due to the reduced visibility of the operating field. The same extensive surgical field visualization is enjoyed by fellows, students, and residents who want to learn this surgical technique and by the operating room staff [3]. The VITOM 3D approach allows excessively accurate hemostasis, and very precise identification of anatomical structures like the anterior and posterior tonsillar pillars, the uvula, and the palatal muscle planes.
Tonsillectomy is a surgical procedure that can be performed with multiple techniques, none of which has been recognized as the best. Nowadays transoral tonsillectomy without magnification represents the standard of care worldwide.
However, due to the advancement of technology, new procedures are being used, such as the operating exoscope. The operating exoscope has recently been introduced in various surgical specialties. In otorhinolaryngology, it has been introduced in numerous subspecialties such as laryngology, head and neck reconstructive surgery, otology, and skull base [4].
In tonsillectomy and more generally for transoral surgery, the introduction of the 3D exoscope into the surgical equipment can be of great interest for several reasons. First of all, the surgeon can operate with more precision. The exoscope magnifies the surgical image on a display and the surgeon can clearly identify all the anatomical structures of the operating field. In this way the surgeon can remove the tonsillar tissue without damaging the adjacent muscles or palatal pillars, reducing the possibility of post-operative pain. Furthermore, this allows precise identification of small vessels and accurate hemostasis, reducing the risk of intraoperative and post-operative bleeding. Furthermore, the exoscope has the advantage of standing at a distance of 20–50 cm from the patient, while the endoscope must be positioned inside the patient’s mouth, limiting the surgical space.
Another invaluable advantage of the 3D exoscope is the possibility to use it for educational purposes. The first surgeon can share the operating field with all the operating room members. The surgeon can explain the procedure step-by-step, and the trainees can follow the procedure projected on the screen. During active surgical training, the use of the exoscope allows the surgeon to continuously monitor the resident without interruptions or changes of position.
The exoscopic technology also allows the surgeon to maintain a comfortable position, avoiding positions that can potentially cause muscle pain.
However, this technique also has disadvantages. First of all, during direct transoral procedures, it is difficult for the first surgeon to share the view of the surgical field with the assistants, because the exoscope instrumentation reduces the field of view. Then the lack of magnification of the surgical field may result in an imprecise visualization of the anatomical structures and hemostasis, and thus a higher risk of post-operative bleeding.
In conclusion, the use of a 3D exoscope for tonsillectomy is a valid alternative to the conventional transoral procedure. This technology offers many surgical and educational improvements and represents a major advance in one of the most common surgical procedures in otolaryngology. This technology is new and requires more retrospective or even prospective studies to investigate its superiority [24].
1.Crosetti E, Arrigoni G, Manca A, et al. 3D Exoscopic surgery (3Des) for transoral oropharyngectomy. Frontiers in Oncology. 2020;10:1-8
2.De Virgilio A, Costantino A, Ms TM, Conti V, Pirola F, Russo E, et al. Pre-clinical experience with the VITOM 3D and the ARTip cruise system for Micro-laryngeal surgery. The Laryngoscope. 2021;131:136-138
3.Ferlito S, La Mantia I, Caruso S, Cammaroto G, Chiesa-Estomba CM, Iannella G, et al. High definition three-dimensional exoscope (VITOM 3D) in E.N.T. surgery: A systematic review of current experience. Journal of Clinical Medicine. 2022;11(13):36-39
4.Pirola F, Leone F, Di Bari M, Salamanca F, Bianchi A, Catalani M, et al. 3D 4K exoscope in snore surgery simulation: Pre-clinical experience. Sleep & Breathing. 2022. DOI: 10.1007/s11325-022-02684-1. Epub
5.Crowe SJ, Watkins SS, Rotholz AS. Relation of tonsillar and naso-pharyngeal infections to general systemic disorders. Bulletin of the Johns Hopkins Hospital. 1917;28:1-25
6.Polites N, Joniau S, Wabnitz D, Fassina R, Smythe C, Varley P, et al. Postoperative pain following coblation tonsillectomy: Randomized clinical trial. ANZ Journal of Surgery. 2006;76(4):226-229
7.Belloso A, Morar P, Tahery J, Saravanan K, Nigam A, Timms MS. Randomized-controlled study comparing post-operative pain between coblation palatoplasty and laser palatoplasty. Clinical Otolaryngology. 2006;31(2):138-143
8.Mink JW. Shaha S S, Brodsky L making sense out of the tonsillectomy literature. International Journal of Pediatric Otorhinolaryngology. 2009;73:1499-1506
9.Maddern BR. Electrosurgery for tonsillectomy. Laryngoscope. 2002;2(suppl):11-13
10.Weimert TA, Babyak JW, Richter HJ. Electrodissection tonsillectomy. Archives of Otolaryngology – Head & Neck Surgery. 1990;116:186-188
11.Shah U, Galinkin J, Chiavacci R, Briggs M. Tonsillectomy by means of plasma-mediated ablation. Archives of Otolaryngology – Head & Neck Surgery. 2002;128:672-676
12.Raut VV, Bhat N, Sinnathuray AR, Kinsella JB, Stevenson M, Toner JG. Bipolar scissors versus cold dissection for pediatric tonsillectomy: A prospective, randomized pilot study. International Journal of Pediatric Otorhinolaryngology. 2002;64:9-15
13.Tay HL. Post-operative morbidity in electrodissection tonsillectomy. The Journal of Laryngology and Otology. 1995;109:209-211
14.Neumann AM Jr, Wiatrak BJ. Erbe constant voltage electrocautery versus conventional variable voltage electrocautery for tonsillectomy in children. International Journal of Pediatric Otorhinolaryngology. 1997;40:35-40
16.Sheahan P, Miller I, Colreavy M, Sheahan JN, McShane D, Curran A. The ultrasonically activated scalpel versus bipolar diathermy for tonsillectomy: A prospective, randomized trial. Clinical Otolaryngology. 2004;29:530-534
17.Silveira H, Silveira Soares J, Almeida LH. Tonsillectomy: Cold dissection versus bipolar electrodissection. International Journal of Pediatric Otorhinolaryngology. 2003;67:345-351
18.Kornblut AD. A traditional approach to surgery of the tonsils and adenoids. Otolaryngological Clinic North America. 1987;20:249-263
19.Younis RT, Lazar RH. History and current practice of tonsillectomy. The Laryngoscope. 2002;112(Suppl):3-5
20.Weinstein GS, Quon H, Newman HJ, et al. Transoral robotic surgery alone for oropharyngeal cancer: An analysis of local control. Archives of Otolaryngology - Head and Neck Surgery. 2012;138(7):628-634
21.Nakaya M, Kimura Y, Onuki Y, et al. Endoscopic-assisted tonsillectomy. Laryngoscope. 2013;123:360-361
22.Colombo G, Ferreli F, Di Bari M, Cugini G, Miceli S, De Virgilio A, et al. Introducing the high-definition 3D exoscope in ear surgery: Preliminary analysis of advantages and limits compared with operative microscope. European Archives of Oto-Rhino-Laryngology. 2021;278:4217-4223. DOI: 10.1007/s00405-020-06510-w
23.Ridge SE, Shetty KR, Lee DJ. Heads-up surgery: Endoscopes and exoscopes for otology and Neurotology in the era of the COVID-19 pandemic. Otolaryngologic Clinics of North America. 2021;54:11-23
24.Festa BM, Zuppardo J, Costantino A, Ferreli F, Spriano G, Mercante G, et al. High-definition 3D exoscope-assisted tonsillectomy. American Journal of Otolaryngology. 2023;44(1):103674. DOI: 10.1016/j.amjoto.2022.103674
Written By
Sebastiano Bucolo, Matteo Pezzoli, Maria Vittoria Pomara, Umberto Visentin and Gianni Succo
Submitted: 22 December 2022Reviewed: 18 January 2023Published: 23 February 2023
 Open access peer-reviewed chapter
Open access peer-reviewed chapter