Open Access is an initiative that aims to make scientific research freely available to all. To date our community has made over 100 million downloads. It’s based on principles of collaboration, unobstructed discovery, and, most importantly, scientific progression. As PhD students, we found it difficult to access the research we needed, so we decided to create a new Open Access publisher that levels the playing field for scientists across the world. How? By making research easy to access, and puts the academic needs of the researchers before the business interests of publishers.
We are a community of more than 103,000 authors and editors from 3,291 institutions spanning 160 countries, including Nobel Prize winners and some of the world’s most-cited researchers. Publishing on IntechOpen allows authors to earn citations and find new collaborators, meaning more people see your work not only from your own field of study, but from other related fields too.
To purchase hard copies of this book, please contact the representative in India:
CBS Publishers & Distributors Pvt. Ltd.
www.cbspd.com
|
customercare@cbspd.com
Sarcoidosis is a multi-organ disease characterized by the formation of non-caseating epithelioid granulomas in many organs. The kidneys are not commonly affected but when the disease involves these organs. It is comprised of non-caseating granulomatous interstitial nephritis (GIN) and hypercalcemia-related disorders. In the latter case, acute kidney injury as initial presentation of the disease is a rare entity, and it is postulated to appear due to several pathogenic processes: (1) interstitial nephritis with or without granulomas, (2) nephrocalcinosis with or without nephrolithiasis, and (3) urethral obstruction. A 71-year-old man presented to the clinic with a history of lethargy, nausea, short memory loss and a 10 kg weight loss all of which appeared within the past 6 months. He was also known with prostate adenoma and was under the care of a urologist. Upon physical examination the following aspects were noted: blood pressure of 160/100 mmHg, heart rate 60 bpm and an irregular enlarged prostate. The chest X-ray was normal and blood samples revealed anemia, hypercalcemia, and increased values of urea and creatinine. An ultrasound of the kidneys was performed and no abnormalities were noted. The urinalysis showed the presence of protein +, glucose+, blood 2+, a few white cells and some granular casts. The next step was to perform a renal biopsy that revealed areas of lymphocytic tubulitis, mild mononuclear interstitial infiltrate, some non-necrotizing epithelioid granulomas comprised of Langerhans-type giant cells and epithelioid macrophages. Peri-tubular interstitial calcifications were also noted. As a result a histological diagnosis was summarized as acute or chronic granulomatous interstitial nephritis with nephrocalcinosis. A CT scan pf the chest was subsequently performed and it revealed calcified lymph nodes in the mediastinum involving the space between the aorta and the trachea and numerous nodules scattered bilateralally over the entire lung parenchyma with no apparent periseptal or perivascular association. These findings were diagnosed as sarcoidosis. The serum ACE level was found abnormal and therefore, a clinical diagnosis of sarcoidosis was made and the patient was started on 40 mg of oral prednisone daily with rapid improvement in the overall general condition. Sarcoidosis is an uncommon disease that should be suspected in front of a patient that presents with hypercalcemia and acute kidney injury. After excluding other causes of hypercalcemia such as multiple myeloma, primary hyperparathyroidism, and paraneoplastic phenomena, a renal biopsy is then indicated to confirm the diagnosis of sarcoidosis.
“Carol Davila” University of Medicine and Pharmacy, Bucharest, Romania
“Dr Ion Cantacuzino” Clinical Hospital, Bucharest, Romania
*Address all correspondence to: marilenastoian@yahoo.com
1. Introduction
Sarcoidosis is a rare condition of unknown etiology characterized by systemic inflammation. In more than 90% of patient sarcoidosis mainly involves the respiratory and lymphatic systems [1]. The pathogenesys is not completely understood and it relies on an aberrant T cell response to unidentified antigens together with a genetic predisposition and the effect of environmental factors in predisposed individuals. The hallmark feature of sarcoidosis is the formation of non caseating granulomas in the affected organs. These structures are characterized by increased expression of polarized macrophages together with a defective link between regulator and effector T cells. There is a very complex interplay of immune cells which include macrophages, dendritic cells, T helper lymphocytes, T regulatory cells (Tregs) and their medators [2]. The exact etiologic agent (s) is still unknown although studies of T cell antigen receptor (TCR) Vbeta interactions suggest conventional antigenic stimulation. The most investigated agents are infectious agents (components of cutibacteria and mycobacteria), occupational and environmental exposures, Kveim-Siltzbach reagent and vimentin [3, 4].
Kidney involvement in sarcoidosis is rare and not well understood and it is defined either by histologic changes or just by a decline in kidney function. Several small studies showed that the disease can affect the kidneys in 10 to 50% of the patients [5, 6] and most of the times the disease remains silent or undetected for many years. In a large cohort that included some 1200 patients with pulmonary sarcoidosis kidney disease was detected in 12% of cases [7]. The ACCESS study revealed that renal involvement detected at 6 months after the initial diagnosis was present in only 5 patients (0.7%) out of a total of 736 cases investigated [8].
The main kidney abnormalities in sarcoidosis are noncaseating granulomatous interstitial nephritis (GIN) and hypercalcemia-related disorders, with a difficult clinical diagnosis. With regards to outcome, there is a large variability with some patient that progress to end-stage kidney disease (ESKD) and some that experience spontaneous remision. We now know that early disgnosis and the rapid onset of corticotherapy can improve the prognosis. The acute kidney injury (AKI) is thought to appear by means of hypercalcemia that induces vasoconstriction of the afferent arterioles. The most common causes of hypercalcemia include: hyperparathyroidism, multiple myeloma, bone metastases and humoral hypercalcemia associated with malignancy. Less common causes are sarcoidosis, hyperthyroidism, Addison’s disease, drug related hypercalcemia and vitamin D excess. The most prevalent complications are nephrocalcinosis and renal stones. The interstitial nephritis associated with sarcoidosis is suspected in patients who present with an elevated creatinine and a bland urine sediment and have a known diagnostic or a characteristic presentation of extrarenal sarcoidosis. In patients that develop ESKD dialysis and transplantation can offer results similar to those with other causes of kidney failure. Even if renal involvement is a rare occurence in sarcoidosis it can nevertheless influence the prognosis of the disease. It is therefore important to detect early changes in kidney function in order top revent the progression to ESKD.
Sarcoidosis by means of the associated inflammation can affect virtually every organ but with a great predisposition for pulmonary involvement. In up to 30% of cases the presentation involves sarcoid lesions in the skin, the eyes, reticuloendothelial and musculoskeletal systems, in the exocrine glands, the heart, the kidneys and the central nervous system.
In a retrospective multicenter study (EpiSarc) that included 562 men and 675 women there were 5 distinct phenotypes of sarcoidosis detected with a non-random distribution of organ involvement [7]. These phenotypes are distinctive by means of sex, geographical origin and socio-professional category:
pulmonary involvement with fibrosis and heart involvement (associated with being non-European/non-White)
hepatosplenic, peripheral lymph node and bone involvement (associated with being non-European/non-White)
erythema nodosum, joint involvement and hilar lymph nodes (associated with being European/White and female)
eye, neurological, digestive and kidney involvement nodes (associated with being European/White)
lupus pernio and a high percentage of severe involvement
In contrast to the EpiSarc an earlier European study of White/ CAUCASIAN patients with sarcoidosis (The Genotype-Phenotype Relationship in Sarcoidosis study) identified five different subgroups:
abdominal organ involvement
ocular-cardiac-cutaneous-central nervous system (CNS) disease involvement,
musculoskeletal-cutaneous involvement,
pulmonary and intrathoracic lymph node involvement,
Kidney involvement in sarcoidosis has not been studied thoroughly. The are several small and larger studies that determined that renal disease occurs in 10–50% of patients with sarcoidosis. The characteristic lesions have different causes and prevalance:
nephrocalcinosis is estimated to occur in 5% of patients with sarcoidosis [10];
nephrolithiasis occurs in approximately 1–14% of patients with sarcoidosis [11, 12];
interstitial nephritis with granuloma formation occurs in approximately 20% of patients [13];
glomerular involvement include membranous nephropathy, IgA nephropathy, minimal change disease, proliferative or crescentic glomerulonephritis, and focal segmental glomerulosclerosis [14];
urinary tract obstruction resulting from retroperitoneal lymph node involvement, retroperitoneal fibrosis, kidney stones, and direct ureteral involvement by sarcoid [15];
retroperitoneal fibrosis involve the renal artery, which may be affected by sarcoid angiitis associated with hypertension [16].
Acute kidney injury (AKI) was detected in 0.7% to 4.3% of patients with sarcoidosis it has several causes: (1) nephrocalcinosis with or without nephrolithiasis, (2) interstitial nephritis with or without granulomas [17] and (3) ureteral obstruction. Acute kidney injury rarely appears as the initial presentation of the disease. To make a correct diagnosis the clinical presentation needs to be combined with paraclinical tests and with renal pathology. The treatment with steroids usually produces a good effect on AKI.
End stage renal disease (ESRD) appears most likely due to hypercalcemic nepropathy rather than granulomatous nephritis or a glomerulonephropathy. This happens in spite of the fact that nephrocalcinosis is less common overall than interstitial nephritis. Risk factors for ESKD included advanced age at the time of kidney disease diagnosis, granulomatous tubulointerstitial nephritis, and interstitial fibrosis [17]. Even though many patients with sarcoidosis and ESKD have a reduced eGFR they rarely require some form of kidney replacement therapy. Sarcoid reccurence in the kidney after renal transplantation has been observed at a median of 13 months after the surgical intervention in 27% of patients and this suggests that specific clinical and histologic monitoring may be warranted during the early posttransplant period [18, 19].
Hypercalcemia represents a well known complication of sarcoidosis and is found in 10 to 20% of patients. It can directly cause acute kidney injury due to renal vasoconstriction and volume depletion as a result of nephrogenic diabetes insipidus [20]. It appears because of hyperproduction of 1,25-dihydroxy vitamin D.. The normal conversion of 25-hydroxyvitamin D (calcidiol) to 1,25-dihydroxyvitamin D (calcitriol) occurs in the kidney through 1-α hydroxylase, a cytochrome p 450 enzyme [21, 22]. In sarcoidosis and other granulomatous diseases pulmonary macrophages express 1-α hydroxylase, which is often resistant to negative feedback mechanisms causing overproduction of calcitriol [21, 23] which in turn leads to increased calcium uptake by the gut. Adams et al. demonstrated that calcitriol is the hypercalcemia-causing factor in sarcoidosis and that macrophages from patients with sarcoidosis are the synthetic source of hormone in the disease [24]. In sarcoid granulomas incubated with 25-hydroxy vitamin D, Mason et al. identified a similar metabolite [25]. It has also been shown that in sarcoidosis but also in other granulomatous conditions, some activated mononuclear cells (particularly macrophages) located in the lungs and lymph nodes can produce calcitriol from calcidiol in a mechanism independent of PTH [24, 25, 26]. The evidence for extrarenal calcitriol production is comes from several observations [24, 25, 26, 27]:
hypercalcemia and serum calcitriol concentrations have been described in an anephric patient with sarcoidosis;
calcidiol conversion to calcitriol can be demonstrated in vitro in alveolar macrophages or lymph node tissue obtained from hypercalcemic patients with sarcoidosis;
production of the messenger RNA for CYP27B1, the 1-hydroxylase, is markedly increased in alveolar macrophages isolated from hypercalcemic patients with sarcoidosis.
In some patients with sarcoidosis parathyroid hormone-related protein (PTHrP), the usual etiologic agent of humoral hypercalcemia of malignancy, may also contribute to the hypercalcemia. In one series, PTHrP was found in 85% (17 of 20) of biopsies of granulomatous tissue from patients with sarcoidosis, and a few patients with both sarcoidosis and hypercalcemia had high serum PTHrP concentrations [28].
Hypercalciuria is three times more common than hypercalcemia [20] in patients with sarcoid and some studies show a frequency of up to 60% of cases [29]. Even though hypercalciuria appears in 30–60% of patients with sarcoidosis an abnormal calcitriol metabolism is seen in subjects who are normocalciuric and also normocalcemic [30]. In normal people if we increase the calcium intake then we obtain a lowering of serum calcitriol concentration but this does not happen in patients with sarcoidosis.
Both hypercalcemia and hypercalciuria can lead to acute and chronic kidney injury in sarcoidosis by causing nephrolithiasis and nephrocalcinosis. Hypercalcemia by means of preglomerular arterial vasoconstriction may cause a decreased glomerular filtration rate (GFR) [31]. The formation of calcium oxalate crystals is the likely cause of nephrolithiasis and it comes from the interplay between hypercalcemia and hypercalciuria. Interstitial calcium oxalate deposition is also seen in association with granulomas in sarcoidosis [32]. Measurement of serum calcium, 24-hour urinary calcium concentration, and a serum angiotensin-converting enzyme (ACE) concentration may provide support for the diagnosis of sarcoidosis. The causes of hypercalcemia are listed below in Table 1. The most frequent are: multiple myeloma, hyperparathyroidism, bone metastases and humoral hypercalcaemia of malignancy. Less common causes include sarcoidosis, Addison s disease and drugs.
I. Parathyroid hormone-related
1. Primary hyperparathyroidism
2. Sporadic, familial, associated with multiple endocrine neoplasia I or II
3. Tertiary hyperparathyroidism
4. Associated with chronic renal failure or vitamin D deficiency
II. Vitamin D-related
1. Vitamin D intoxication
2. Usually 25-hydroxyvitamin D2 in over-the-counter supplements
1. Immobilization, with high bone turnover (e.g., Paget’s disease, bedridden child)
2. Recovery phase of rhabdomyolysis
Table 1.
Causes of hypercalcemia.
The aim of compensatig the hypercalcemia and hypercalciuria associated to sarcoidosis is reducing intestinal calcium absorption and calcitriol synthesis. The main requirements are reducing calcium intake to a maximum of 400 mg per day, reducing oxalate intake, avoidance of sun exposure and eliminating all types of vitamin D supplements. Treatment with glucocorticoids decreases inflammation and therefore calcitriol synthesis while bisphosphonates are used to successfully treat the hypercalcemia. Apart from these,; chloroquine, hydroxychloroquine, and ketoconazole can improve calcium metabolism in patients with sarcoidosis.
Urinary tract obstruction appears in sarcoidosis due to the following factors: Retroperitoneal lymph node involvement, retroperitoneal fibrosis, kidney stones, and direct ureteral involvement by sarcoid. Type AA amyloidosis in association with the characteristic inflammation has been described in the renal biopsy of one patient with systemic sarcoidosis [33]. The renal artery can suffer from sarcoid angiitis also associating hypertension which can also appear due to retroperitoneal fibrosis. All of the above conditions are hallmarks and causes of AKI and may respond to corticosteroids, urologic decompression and hemodialysis [34].
Granulomatous interstitial nephritis (GIN) is one of the lesions that are identified in renal biopsieis in patients with sarcoidosis. It is usually silent but occasionally it may present as acute kidney injury [35]. GIN is encountered in 0.5–0.9% of native renal biopsieis and in 0.6% of renal transplant biopsies [36, 37, 38, 39]. However, some 7–27% of patients with sarcoidosis have evidence of granulomatous tubulointerstitial nephritis on post-mortem series, although this may not result in clinically significant renal disease. In a small number of patients with sarcoidosis GIN can precede the diagnostic but as a general rule it is now known that GIN can develop at any time during the course of the disease [40]. There are several causes of granulomatous interstitial nephritis among which are: drugs (cephalosporins, vancomycin, nitrofurantoin, ciprofloxacin and NSAIDs) (9–45%), sarcoidosis (9–29%), mycobacterial or fungal infections, crystal deposits, paraproteinemia, granulomatosis with polyangiitis (GPA), and very rarely inflammatory bowel diseases. GIN also appears as a idiopathic entity (>40%) [13, 41]. The relative contribution of different etiologies to GIN is unknown since our knowledge is based on case series and case reports for the description of this condition. In a report by Mignon et al. [42] of 32 cases, ∼28% were due to drugs, 16% were caused by granulomatosis with polyangiitis (GPA) and 9% were attributed to sarcoidosis and tuberculosis. Furthermore, in a retrospective of 40 consecutive renal biopsiei where GIN was defined as the presence of at least one epithelioid granuloma in the interstitium, Javaud et al. [40] found that the majority of cases were caused by sarcoidosis (50%), followed by medication induced (17.5%) and tuberculosis associated in 7.5% of cases. Membranous nephropathy can be detected in conjunction with GIN in patients with sarcoidosis with a good response to glucocorticoid therapy [43].
In the granulomas of sarcoidosis,secretion of tumor necrosis factor (TNF) by macrophages is followed by a complex interplay of T helper (Th) 1 and Th17 cells with subsequent synthesis of interleukin-6 (IL-6), IL-12, IL-18, IL-23 and transforming growth factor (TGF)-β [38, 44]. All these cytokines further stimulate the macrophages and lead to functional changes and maturation into epithelioid cells and eventually giant cells [45, 46]. Natural killer (NK) cells are also involved and they produce interferon (IFN)-γ which also promotes inflammation. Glucocorticosteroids exert their beneficial effect on granulomas by repression of NF-κB-related gene transcription with lymphocyte apoptosis [46]. Until recently, the granuloma was seen as a static structure but research in tuberculosis has revealed that these structures are highly dynamic [44]. An improved understanding of granuloma formation and interactions may reveal useful therapeutic targets for the future [44].
Mild proteinuria and/or sterile pyuria can appear in association with the interstitial nephritis but usually the urinalysis looks normal. Significant proteinuria is uncommon. In a review of 52 cases of sarcoidosis interstitial nephritis, sterile pyuria, hematuria, glycosuria, and hypercalciuria were identified in 33, 21, 12, and 8% of cases, respectively [10]. In a prospective review of 191 sarcoid patients, proteinuria, defined as urine protein/creatinine ratio equal to or exceeding 0.3 mg/mg, was found in 7% of cases [47]. More than half of these patients had another known risk factor for proteinuria (diabetes, hepatitis B or C infection, human immunodeficiency virus [HIV], systemic lupus erythematosus, or congestive heart failure).
3. Acute kidney injury -an atipical modality of the onset of sarcoidosis: clinical case
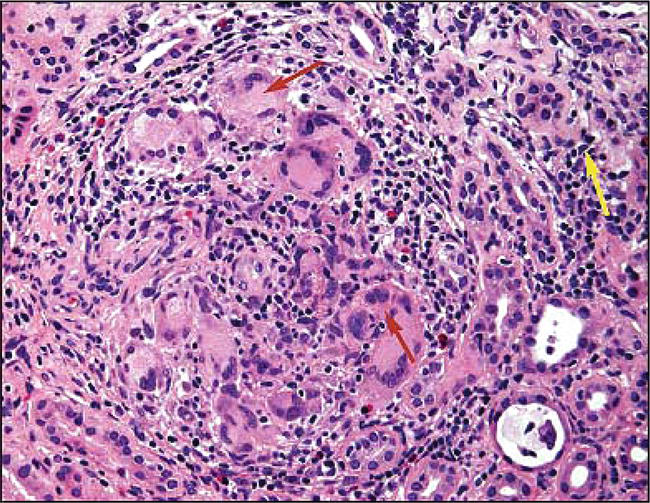
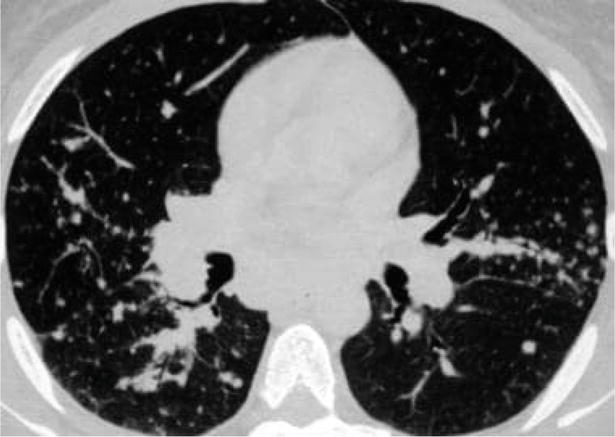
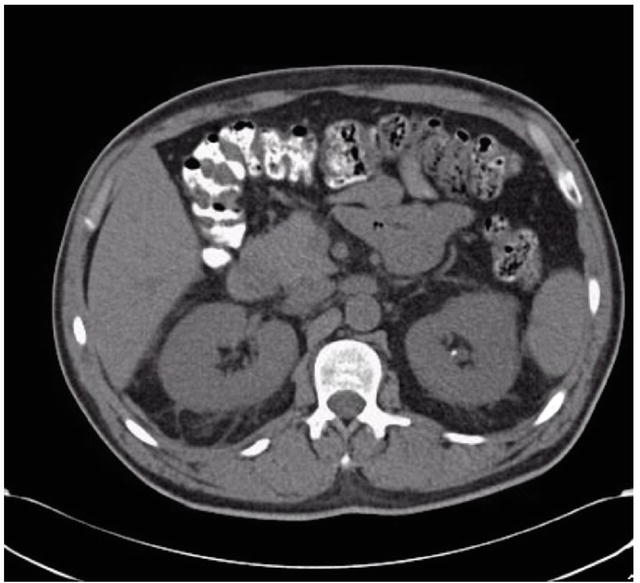
A 71-year-old man presented to the clinic with a 6-months old history of lethargy, nausea, weight loss (10 kg) and short-term memory loss. He was also under urologist observation for a PSA of 34 μg/l (normal range ˂ 4 μg/l) associated with benign prostatic hypertrophy. Upon physical examination it was noted that the patient had a blood pressure of 160/100 mmHg, heart rate pf 60 bpm and an enlarged prostate gland. The chest X ray was normal. Biological examination showed anemia (hemoglobin 10.4 g/dl) with normal range of white and platelet cells, raised serum urea (40 mmol/l) and serum creatinine (680 μmol/l) and also hypercalcaemia (3 mmol/l). There were no antibodies detected suggesting of autoimmune disease. Furthermore the renal ultrasound was normal, urinalysisi showed erythrocytes 2+, protein +, glucose +, a few leucocytes and granular casts. The decision was then to perform a renal biopsy which showed foci of lymphocytic tubulitis and a mild mononuclear interstitial infiltrate; focal peri-tubular interstitial calcification; several discrete non-necrotizing epithelioid granulomata comprised of epitheliod macrophages and Langerhans-type giant cells. The histological diagnosis was then made as acute or chronic granulomatosis interstitial nephritis with nephrocalcinosis (Figure 1). The patient was then subjected to a CT scan of the chest which revealed calcified mediastinal lymph nodes between the aorta and the trachea, intra-pulmonary nodules scattered throughout the upper and lower lobes without any apparent perivascular or peri- septal association (Figure 2). The native pelvic and abdominat CT scans showed the presence of a non obstructing 3 mm calculus in the left kidney with normal size organs and no nephorcalcinosis (Figure 3). The scan findings were consistent with sarcoidosis. The serum ACE level was abnormal (200 U/l – normal range: 27-82 U/l), PTH was low <3 (11–67 pg./mL), also with low serum level of 25-hydroxyvitamin D 23.8 (30–95 ng/mL), but a high level of 1,25-dihydroxyvitamin D 79 (18–72 pg./mL). A clinical diagnosis of sarcoidosis was made and the patient was started on 40 mg prednisone /day orally. A rapid improvement of the patient’s condition was then noted.
Figure 1.
Renal biopsy on light micrography shows noncaseating granulomata (red arrows) and patchy interstitial infiltrate (yellow arrow), with giant cells, inflammation, and moderate tubular atrophy and interstitial fibrosis.
Histological findings in GIN may help to define the etiologic causes of granuloma. In sarcoidosis granulomatous inflammation is usually non-necrotizing, in contrast to those associated with antineutrophil cytoplasmic antibody (ANCA)-positive diseases such as granulomatosis with polyangiitis and infections such as tuberculosis [46]. Giant cells and granulomas also vary in number and can give some additional information but there is no clear pattern for a specific diagnosis [13, 48]. Bijol et al. reported that abundant granulomata are observed in GIN associated with sarcoidosis but are fewer in number when drugs are involved [38]. Moreover, the granulomas of sarcoidosis are described as ‘naked’ (i.e., without a rim of lymphocytes) [13] while abundant neutrophils and eosinophils, with ill-formed granulomas in a diffuse distribution, point again towards a drug-induced etiology [38]. Advanced sarcoidosis affecting the kidneys is characterized by marked interstitial fibrosis although the literature shows that many different causes of GIN associate various degrees of fibrosis. The presence of eosinophils was not helpful in diagnosing drug related pathology [13]. Immunofluorescence and electron microscopy are also not very helpful [46].
Granulomatous interstitial nephritis related to pyelonephritis or systemic infection has been noted to have an intense inflammatory infiltrate with lymphocytes, neutrophils and plasma cells, micro- abscess formation, white cell casts with or without papillary necrosis and vessel thrombosis and infarction. The number of macrophages, T and B cells are similar to those seen in GIN from other causes with an increase only in the number of neutrophils [49]. Infections with mycobacterial or fungal pathogens are usually associated with necrotizing granulomatous inflammation. The finding of caseous necrosis is more suggestive of tuberculosis (although this can be seen in other infections) [50]. However, this was only seen in 18.7% of cases of tuberculosis-GIN in one series [51]. In some cases, the infective agent can be readily identified with special stains (periodic acid-Schiff, Masson Trichrome, Silver and Ziehl-Nielsen or Auramine) [37, 38]. However, in certain cases, necrosis is absent, and granulomas may be poorly formed, therefore a high index of suspicion is needed.
Renal biopsies should be examined for possible etiologies of GIN especially micro-organisms (acid fast bacili, fungi or viral inclusions) and some cases may require polymerase chain reaction (PCR) testing to support the diagnosis. Culture of fungi and mycobacteria is highly specific, but the result is often too delayed to be clinically meaningful at the time of the biopsy. Sometimes serologis tests like anti-Histoplasma antibodies may be helpful but one must keep in mind that early in the cpurse of the disease or in cases of immunocompromised patients the tests can have false-negative results [52]. Serum or urine detection of fungal antigens allows for a faster diagnosis but unfortunately the sensitivities vary [52]. A newer point-of-care test (XPert MTB/Rif) has been developed for detection of tuberculosis, but this has yet to be studied in histological specimens.
The diagnosis is even more difficult for the immunosuppressed patient as is shown in a recent study of HIV infected subjects [53]. In this population and in renal transplant recipients’ infection is the leading cause of GIN. Tuberculosis is not only more frequent among the immunosuppressed, but immunosuppression may also alter the clinical picture and thereby obscure the diagnosis. An even more difficult situation appears in cases with the need to differentiate the acute interstitial nephritis in graft rejection from tubulitis of interstitial nephritis.
Oxalosis represents another etiology of GIN and renal biopsieis should be examined closely for crystals. Granulomas in the vicinity of vessels must be distinguished from vasculitis with granulomatous inflammation as seen in granulomatosis with polyangiitis. Fortunately both oxalosis and ANCA vasculitis are accompanied by other signs and symptoms which will aid in making the final and correct diagnosis. Finally, tubulorrhexis in acute tubular necrosis can be associated with granulomatous inflammation and must be distinguished from true GIN.
In our patient the initial differential diagnosis of hypercalcemia included many conditions. Hyperparathyroidism, malignancy (multiple myeloma, lymphoma, PTHrp associated malignancy and metastatic bone disease), infections (tuberculosis), sarcoid and vitamin D intoxication were all considered. Laboratory assessment narrowed the differential with an appropriately suppressed PTH and a low 25-hydroxyvitamin D level. The absence of lythic or blastic bone lesions made malignancy less likely. The elevated ACE level made sarcoid a strong possibility, and lymphomas was not readily considered as it can induce increased production of 1,25-D. Intrinsic renal disease was high on the differential rather than renal failure from nephrocalcinosis based on the following reasons: (1) while the hypercalcemia was slowly improving with intravenous hydration, the serum creatinine did not improve (2) the CT of the abdomen and pelvis showed a 3 mm non obstructing left renal calculus with normal size kidneys and no nephrocalcinosis. Moreover, the renal biopsy was required for definitive diagnosis.
Sarcoidosis, a multi-organ inflammatory disease that can also affect the kidney, should be considered as a potential diagnosis in any patient with hypercalcaemia and acute kidney injury. A renal biopsy will then have to be performed if other obvious causes such as myeloma, carcinoma with secondary metastases and primary hyperparathyroidism have been excluded. Acute kidney injury as the initial presentation of sarcoidosis is a rare entity. In some cases a number of patients with sarcoidosis have no extra renal manifestations of the disease upon presentation. Thus, all patients who have granulomatous interstitial nephritis detected on biopsy should have a chest radiograph, pulmonary function tests, and, if these are nondiagnostic, a high-resolution chest computed tomography (CT) scan should be performed to evaluate for pulmonary sarcoidosis.
Acute kidney injury without an “apparent” cause or resolution is an indication for an immediate renal biopsy to prevent further renal deterioration and allow for immediate treatment. Although usually sarcoidosis presents with more than one sign or symptom sometimes it may solely present as acute kidney injury. This type of sarcoidosis is a steroid-responsive disease and it is mandatory that a rapid diagnosis should be made and treatment should start as soon as possible in order to revent irreversible kidney damage.
1.Rossi G, Cavazza A, Colby TV. Pathology of sarcoidosis. Clinical Reviews in Allergy and Immunology. 2015;49:36
2.Sakthivel P, Bruder D. Mechanism of granuloma formation in sarcoidosis. Current Opinion in Hematology. 2017;24:59
3.Eberhardt C, Thillai M, Parker R, et al. Proteomic analysis of Kveim reagent identifies targets of cellular immunity in sarcoidosis. PLoS One. 2017;12:e0170285
4.Grunewald J, Kaiser Y, Ostadkarampour M, et al. T-cell receptor-HLA-DRB1 associations suggest specific antigens in pulmonary sarcoidosis. The European Respiratory Journal. 2016;47:898
5.Gorsane I, Zammouri A, Hajji M, et al. Renal involvement in sarcoidosis: Prognostic and predictive factors. Néphrologie & Thérapeutique. 2022;18:52
6.Bergner R, Hoffmann M, Waldherr R, Uppenkamp M. Frequency of kidney disease in chronic sarcoidosis. Sarcoidosis, Vasculitis, and Diffuse Lung Diseases. 2003;20:126
7.Lhote R, Annesi-Maesano I, Nunes H, et al. Clinical phenotypes of extrapulmonary sarcoidosis: An analysis of a French, multi-ethnic, multicentre cohort. The European Respiratory Journal. 2021;57
8.Baughman RP, Teirstein AS, Judson MA, et al. Clinical characteristics of patients in case control study of sarcoidosis. American Journal of Respiratory and Critical Care Medicine. 2001;164:1885
9.Schupp JC, Freitag-Wolf S, Bargagli E, et al. Phenotypes of organ involvement in sarcoidosis. The European Respiratory Journal. 2018;51
10.Berliner AR, Haas M, Choi MJ. Sarcoidosis: The nephrologist’s perspective. American Journal of Kidney Diseases. 2006;48:856
11.Muther RS, McCarron DA, Bennett WM. Renal manifestations of sarcoidosis. Archives of Internal Medicine. 1981;141:643
12.Rizzato G. Sarcoidosis in Italy. Sarcoidosis. 1992;9(Suppl. 1):145
13.Joss N, Morris S, Young B, Geddes C. Granulomatous interstitial nephritis. Clinical Journal of the American Society of Nephrology. 2007;2:222-230
14.Bergner R, Löffler C. Renal sarcoidosis: Approach to diagnosis and management. Current Opinion in Pulmonary Medicine. 2018;24:513
15.Godin M, Fillastre JP, Ducastelle T, et al. Sarcoidosis. Retroperitoneal fibrosis, renal arterial involvement, and unilateral focal glomerulosclerosis. Archives of Internal Medicine. 1980;140:1240
16.Gross KR, Malleson PN, Culham G, et al. Vasculopathy with renal artery stenosis in a child with sarcoidosis. The Journal of Pediatrics. 1986;108:724
17.Mahévas M, Lescure FX, Boffa J-J, et al. Renal sarcoidosis: Clinical, laboratory, and histologic presentation and outcome in 47 patients. Medicine. 2009;88(2):98-106
18.Aouizerate J, Matignon M, Kamar N, et al. Renal transplantation in patients with sarcoidosis: A French multicenter study. Clinical Journal of the American Society of Nephrology. 2010;5:2101
19.Mann DM, Fyfe B, Osband AJ, et al. Sarcoidosis within a renal allograft: A case report and review of the literature. Transplantation Proceedings. 2013;45:838
20.Sharma OP. Vitamin D, calcium, and sarcoidosis. Chest. 1996;109(2):535-539
21.Manjunath V, Moeckel G, Dahl NK. Acute kidney injury in a patient with sarcoidosis: Hypercalciuria and hypercalcemia leading to calcium phosphate deposition. Clinical Nephrology. 2013;80(2):151-155
22.Gardner DG. Hypercalcemia and sarcoidosis—Another piece of the puzzle falls into place. American Journal of Medicine. 2001;110(9):736-737
23.Reichel H, Koeffler HP, Barbers R, Norman AW. Regulation of 1,25-dihydroxyvitamin D3 production by cultured alveolar macrophages from normal human donors and from patients with pulmonary sarcoidosis. The Journal of Clinical Endocrinology & Metabolism. 1987;65(6):1201-1209
24.Adams JS, Sharma OP, Gacad MA, Singer FR. Metabolism of 25-hydroxyvitamin D3 by cultured pulmonary alveolar macrophages in sarcoidosis. The Journal of Clinical Investigation. 1983;72(5):1856-1860
25.Mason RS, Frankel T, Chan YL, Lissner D, Posen S. Vitamin D conversion by sarcoid lymph node homogenate. Annals of Internal Medicine. 1984;100(1):59-61
26.Insogna KL, Dreyer BE, Mitnick M, et al. Enhanced production rate of 1,25-dihydroxyvitamin D in sarcoidosis. The Journal of Clinical Endocrinology and Metabolism. 1988;66:72
27.Inui N, Murayama A, Sasaki S, et al. Correlation between 25-hydroxyvitamin D3 1 alpha-hydroxylase gene expression in alveolar macrophages and the activity of sarcoidosis. The American Journal of Medicine. 2001;110:687
28.Zeimer HJ, Greenaway TM, Slavin J, et al. Parathyroid-hormone-related protein in sarcoidosis. The American Journal of Pathology. 1998;152:17
29.Iannuzzi MC, Rybicki BA, Teirstein AS. Sarcoidosis. The New England Journal of Medicine. 2007;357(21):2153-2165
30.Basile JN, Liel Y, Shary J, Bell NH. Increased calcium intake does not suppress circulating 1,25-dihydroxyvitamin D in normocalcemic patients with sarcoidosis. The Journal of Clinical Investigation. 1993;91:1396
31.Levi M, Peterson L, Berl T. Mechanism of concentrating defect in hypercalcemia. Role of polydipsia and prostaglandins. Kidney International. 1983;23:489
32.Reid JD, Andersen ME. Calcium oxalate in sarcoid granulomas. With particular reference to the small ovoid body and a note on the finding of dolomite. American Journal of Clinical Pathology. 1988;90(5):545-558
33.Komatsuda A, Wakui H, Ohtani H, et al. Amyloid A-type renal amyloidosis in a patient with sarcoidosis: Report of a case and review of the literature. Clinical Nephrology. 2003;60:284
34.Mariano RT, Sussman SK. Sarcoidosis of the ureter. AJR. American Journal of Roentgenology. 1998;171:1431
35.Casella FJ, Allon M. The kidney in sarcoidosis. Journal of American Society Nephrology. 1993;3:1555-1562
36.O’Riordan E, Willert RP, Reeve R, Kalra PA, O’Donoghue DJ, Foley RN, et al. Isolated sarcoid granulomatous interstitial nephritis: Review of five cases at one center. Clinical Nephrology. 2001;55:297-302
37.Naidu GD, Ram R, Swarnalatha G, et al. Granulomatous interstitial nephritis: Our experience of 14 patients. Indian Journal of Nephrology. 2013;23:415-418
38.Bijol V, Mendez GP, Nosé V, Rennke HG. Granulomatous interstitial nephritis: A clinicopathologic study of 46 cases from a single institution. International Journal of Surgical Pathology. 2006;14:57-63
39.Javaud N, Belenfant X, Stirnemann J, Laederich J, Ziol M, Callard P, et al. Renal granulomatoses: A retrospective study of 40 cases and review of the literature. Medicine. 2007;86:170-180
40.Javaud N, Belenfant X, Stirnemann J, et al. Renal granulomatoses: A retrospective study of 40 cases and review of the literature. Medicine (Baltimore). 2007;86:170-180
41.Balafa O, Liapis G, Duni A, Xiromeriti S, Kalaitzidis R, Elisaf M. An unusual case of acute kidney injury – Idiopathic granulomatous tubulointerstitial nephritis. Clinical Nephrology. 2015;84:247-250
42.Mignon F, Mery JP, Mougenot B, et al. Granulomatous interstitial nephritis. Advances in Nephrology from the Necker Hospital. 1984;13:219-245
43.Ikeda A, Nagai S, Kitaichi M, et al. Sarcoidosis with granulomatous interstitial nephritis: Report of three cases. Internal Medicine. 2001;40:241-245
44.Ramakrishnan L. Revisiting the role of the granuloma in tuberculosis. Nature Reviews. Immunology. 2012;12:352-366
45.Rosen Y. Pathology of sarcoidosis. Seminars in Respiratory and Critical Care Medicine. 2007;28:36-52
46.Broos CE, van Nimwegen M, Hoogsteden HC, et al. Granuloma formation in pulmonary sarcoidosis. Frontiers in Immunology. 2013;4:437
47.Chopra A, Brasher P, Chaudhry H, et al. Proteinuria in sarcoidosis: Prevalence and risk factors in a consecutive outpatient cohort. Sarcoidosis, Vasculitis, and Diffuse Lung Diseases. 2017;34:142
49.Viero RM, Cavallo T. Granulomatous interstitial nephritis. Human Pathology. 1995;26:1347-1353
50.Chung S, Park CW, Chung HW, et al. Acute renal failure presenting as a granulomatous interstitial nephritis due to cryptococcal infection. Kidney International. 2009;76:453-458
51.Chapagain A, Dobbie H, Sheaff M, et al. Presentation, diagnosis, and treatment outcome of tuberculous-mediated tubulointerstitial nephritis. Kidney International. 2011;79:671-677
52.Qian Q , Humayun H, Humayun Y, et al. Granulomatous interstitial nephritis associated with disseminated histoplasmosis in an immunocompetent patient. American Journal of Kidney Diseases. 2011;58:1018-1102
53.Nel D. A Retrospective Review of Granulomatous Interstitial Nephritis (GIN) amongst HIV-Infected Patients at Groote Schuur Hospital Cape Town. Cape Town: Faculty of Health Sciences, University of Cape Town; 2014
Written By
Marilena Stoian
Submitted: 07 May 2023Reviewed: 13 May 2023Published: 29 August 2023
 Open access peer-reviewed chapter
Open access peer-reviewed chapter