Open Access is an initiative that aims to make scientific research freely available to all. To date our community has made over 100 million downloads. It’s based on principles of collaboration, unobstructed discovery, and, most importantly, scientific progression. As PhD students, we found it difficult to access the research we needed, so we decided to create a new Open Access publisher that levels the playing field for scientists across the world. How? By making research easy to access, and puts the academic needs of the researchers before the business interests of publishers.
We are a community of more than 103,000 authors and editors from 3,291 institutions spanning 160 countries, including Nobel Prize winners and some of the world’s most-cited researchers. Publishing on IntechOpen allows authors to earn citations and find new collaborators, meaning more people see your work not only from your own field of study, but from other related fields too.
To purchase hard copies of this book, please contact the representative in India:
CBS Publishers & Distributors Pvt. Ltd.
www.cbspd.com
|
customercare@cbspd.com
Minimally invasive surgeries continue to advance at an immensely fast pace, moving from open discectomy surgeries to microscopic ones using tubular systems, to do fusions, to correct deformities, until we reached a place where we are tackling most spinal pathologies in a minimally invasive fashion, For many spine surgeons, the field of spine endoscopy, whether uniportal or biportal, is still unexplored, to some extent due to their mastery in open and microscopic techniques, and to another extent the learning curve that it takes to master endoscopic spine, as well as a lack in well-structured clearcut data regarding its indications and limitations, and this chapter will hopefully shed the proper lighting on the field of spinal endoscopy, making surgeons understand its utility in treating different pathologies, discussing the research and data comparing spinal endoscopy with more traditional techniques, as well as understanding endoscopic spine surgery’s learning curve, and how to overcome the timeline in mastering its basic techniques.
Mustansiriyah University College of Medicine - Department of Orthopedics, Baghdad, Iraq
*Address all correspondence to: dr.bayaty@gmail.com
1. Introduction
In the 70s, Hijikata, a Japanese surgeon, who was famous for performing diagnostic discographies. He developed tubes to introduce this approach to the posterolateral annulus under fluoroscopic control. He could incise the annulus, and, using pituitary rongeurs; he could remove the nucleus of the disc in what he described to be a “percutaneous necluotomy”.
He published this procedure in the Japanese language. This was one of the reasons why this procedure did not gain widespread attention among the surgical community, but it was definitely the starting point [1, 2].
Forst and Hausmann [3] described the use of an arthroscope to visualize the contents of the intervertebral disc in 1983, and the first description of an endoscopic discectomy by Kambin et al. followed soon after in 1988 [4]; however, a spine surgery still stayed behind other specialties in the inclusion of indirect visualization. Nonetheless, the need for less invasive spine procedures and surgeon drive to provide these solutions and improve care quality has driven the global advancement of spinal endoscopy [5].
And keeping up with such the swift pace and such great advances, spine surgeons should be open and ready to tackle the field of endoscopic spine surgeries, as it is only a matter of time (and research papers) that stand between us now, and between standardizing spinal endoscopy as a potential gold standard technique in most spinal pathologies.
The endoscope will be defined as a visualization device placed into the body with an integrated working channel that provides a surgical corridor for tools to manipulate, ablate, and resect tissue [6].
There are two different approaches to divide the world on spinal endoscopy [7].
According to the property of the endoscopy used:
A full endoscopic system (percutaneous endoscopic system), which is the most commonly used system in endoscopic spine surgery, the working channel and the optics being in the same tubular device with utilization of a monoportal approach with continuous saline irrigation.
A microendoscopic system, which is the second most frequently used endoscopic device, this category involves using a rigid endoscope (microendoscope) attached to a tubular retractor with tissue dilators, which help minimize muscle retraction, and unlike the other endoscopic systems; this system is not a water-based procedure, and constant saline irrigation is not used. So it’s more of a MIS microscope than an endoscope.
Biportal endoscopic system, which is the third category of endoscopic spine surgery, with separate optical and working channels. The endoscopic portal is used for viewing the surgical field with constant saline irrigation, whereas the instrumental portal is used for surgical instrumentation and procedure.
According to the method of approach:
The transforaminal approach refers to a posterolateral minimally invasive approach to the disc or epidural space through the foraminal window.
Interlaminar approach, which is similar to the usual open or microscopic approach.
Anterior/Posterior approach to the cervical spine.
Caudal or trans-sacral approach.
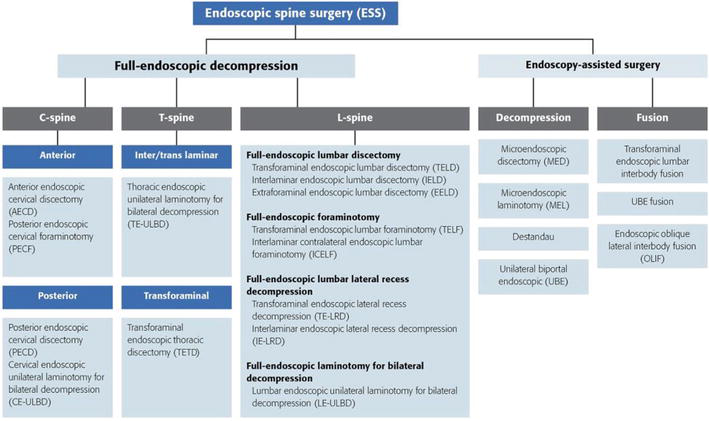
So as the technology and techniques have advanced, the terminology used to describe these procedures has developed organically and has become heterogeneous and sometimes confusing to patients, providers, and payors [7]. Because of that issue, a formal consensus regarding the proper naming of such newly developed procedures had to be implemented to clear up the confusion and avoid any miscommunication. This was why the AOSpine minimally invasive spine surgery taskforce developed the definitions and nomenclature consensus in 2020 (Figure 1). They developed the concept “full- endoscopic” to describe procedures performed with a working-channel endoscope. This distinguishes those procedures from “endoscope-assisted”operations, where tools are passed through trajectories separate from the working endoscopic channel [7] and according to the consensus guidelines, the procedures are named according to the following formula:
Figure 1.
The AOspine endoscopic spine surgery nomenclature consensus.
Approach corridor/Visualization/Segment of spine/Procedure
There are three important main indications in endoscopic spinal surgery:
Discectomies.
Spinal stenosis decompression.
Fusions.
Let us begin by dividing the endoscopic indications according to spinal regions and their approach:
3.1 Lumbar spinal endoscopy
3.1.1 Transformational lumbar discectomy
Indications:
Soft lumbar disc herniation (LDH) of various types, the advancement in technology and experience, and its practical application have widened to include migrated, recurrent, foraminal, extraforaminal, and even partially calcified LDH (Figures 2 and 3) [8].
The patient is positioned prone on a radiolucent table with a pelvic and a thoracic roll.
The desired level’s midline, inferior, and superior vertebral plates are marked under visualization of the image intensifier, and lateral markings to the midline of 8, 10, and 12 cm will be the possible entry points.
The patient is submitted to light sedation, and at the point of entry, an infiltration with local anesthetic without a vasoconstrictor is performed. The sedation should be light since the patient must be aware of being alert if some nerve root is stimulated during the procedure.
The entire procedure is performed through the intervertebral foramen between the exiting and traversing nerve roots (Kambin’s safety triangle) without needing to resect bony or ligamentous structures (Figures 5 and 6).
The intervertebral disc is punctured, and discography with methylene blue or indigo carmine, associated with non-ionic contrast, is done.
Through the guides, the endoscope is inserted into the intervertebral disc, and an indirect intervertebral disc decompression is performed (Figure 7) (inside-out technique), followed by a thermal nucleoplasty.
Figure 2.
Sagittal MRI view of L2–3 soft disc herniation.
Figure 3.
Axial MRI view of L2–3 soft disc herniation.
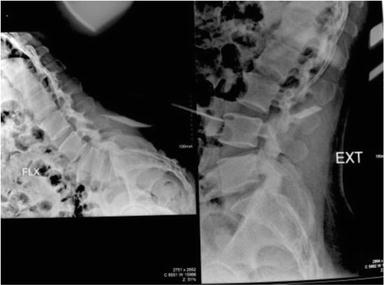
Figure 4.
Assessment of instability by flexion extension X-ray shows no contraindication to such approach.
Figure 5.
Disc extraction using the transforaminal approach.
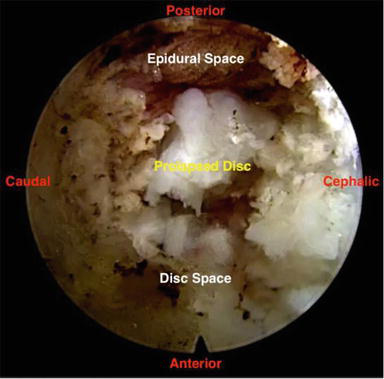
Figure 6.
The endoscopic view in the transforaminal approach.
Figure 7.
Disc material after extraction by transforaminal approach.
Until recently, tubular microdiscectomy was the golden standard surgical option when it comes to dealing with degenerative stenotic pathological changes such as superior articulating process (SAP) or ligamentum flavum (LF) hypertrophy, osteophyte formation or associated dynamic or static instability [10], however, in recent years the endoscopic approach has risen to be a strong competitor.
docking the port at the lower foramen (caudal surface of the SAP).
The tip of the SAP is excised by reaming. It is done blindly under fluoroscopic control with the medial pedicle line as the limit, and the giveaway feeling suggests the completeness of bony resection. It, though, appears risky for early endoscopy surgeons. However, there is a soft layer of capsule and ligamentum flavum that is still between the reamer and the traversing root.
Visualized endoscopic burred foraminoplasty can also be done, which is apparently safe.
exposed ligamentum flavum and capsule are removed
For foraminal stenosis, the focus is on the cranial aspect of foramen and removal of the tip of SAP, capsule, and ligamentum flavum.
For the lateral recess stenosis, the caudal foramen is focused.
Visualization of the pulsatile exiting nerve root is the end point of decompression.
3.1.3 Interlaminar lumbar discectomy
Indications: (Soft LDHs that were technically inaccessible in the transforaminal approach) [8, 11, 12, 13]
L5-S1 level with high iliac crest level.
High-grade migrated disc herniation, either cranial or caudal direction.
Calcified discs.
The sufficient interlaminar window between the cranial and caudal lamina and the midline and mediodorsal borders of the inferior articular process (IAP) measuring at least 6 mm.
Central canal stenosis
Ligamentum flavum hypertrophy
Lateral recess stenosis and Foraminal stenosis (shared with transforaminal approach)
The patient is positioned in the prone position, on a radiolucent table, under general anesthesia (In this technique, general anesthesia is necessary because it is vital to move away from the neural root).
The interlaminar window at the level is marked on the skin with the use of X-ray, and a 1-cm longitudinal access is made near the midline.
dilator is put in the interlaminar space
the endoscope is inserted.
musculature is dissected to the ligamentum flavum, which is opened to expose the descending root and the epidural fat.
The opening of the yellow ligament is a fundamental step during endoscopic surgery by the interlaminar approach, to access the nerve structures and the intervertebral disc.
The nerve root is protected with a beveled cannula.
The intervertebral disc is perforated and decompressed.
At the end of the procedure, a thermal nucleoplasty is done.
3.2 Thoracic spinal endoscopy
Indications:
Soft thoracic disc herniation in paracentral and lateral locations.
The neck is extended and the head is fixed in place with tape.
The arms are positioned towards the caudal on the body with gentle tension.
The line of spinal joints is marked X-ray (2 cm lateral from the midline).
Insertion of the sheath with the dilator beveled opening.
The dilator is removed.
operation is performed under visual control and continuous irrigation with saline solution.
foraminotomy is done with resection of the lateral aspect of the ligamentum flavum, and identification of the lateral edge of the spinal cord and branching of the spinal nerves.
Bipolar coagulation of the venous plexus.
If disc herniation occurs, the nerves should be immobilized, and the herniated disc material should be resected.
Depending on the pathology, the foraminotomy can be extended.
The patient is set in the supine position with her neck in slight extension.
A 3 cm anterolateral incision, centered at C/6 as localized using a radiographic image intensifier, allowed exposure of the anterior spine medial to the carotid sheath.
Under lateral fluoroscopic guidance, needle is inserted obliquely into each affected disc.
After guide-wire insertion, guiding rods and a dilating tube are then passed, followed by a working cannula with an outer diameter of 4.8 mm.
After resection of the margin of the uncinate process, the endoscope is then used to visualize the disc.
The posterior part of the nucleus pulposus is first partially removed with grasping forceps for preliminary decompression.
The endoscope is then advanced to the posterior annular margin of the disc to identify the target fragments, with particular care taken not to damage the nerve roots or the dura mater.
So, what about other indications, such as fusion? In other words, can spinal endoscopy expand its indications to fill the role of conventional open spine surgery? [19].
To answer that question, you must know that the development process of spinal endoscopic surgery can be divided mainly into four generations (Table 1) [20].
The first generation: the transforaminal approach
The second generation is an interlaminar approach which was developed to tackle herniations that were difficult to access with a transforaminal approach.
The third generation, spinal stenosis could be approached. Moreover, endoscopic treatment was possible the cervical and thoracic spine as well.
The fourth generation endoscopic lumbar interbody fusion can be attempted.
1st generation
2nd generation
3rd generation
4th generation
Endoscopy systems
Uniportal
Uniportal
Uniportal/Biportal
Uniportal/Biportal
Indication
Disc herniation
Disc herniation
Disc herniation Central stenosis Foraminal stenosis
Stenosis Instability
Lesion
Lumbar
Lumbar
Lumbar Thoracic Cervical
Lumbar Lumbar interbody fusion
Approach
Transforaminal
Interlaminar
Posterior interlaminar Transforaminal
Trans-Kambin Posterolateral
Table 1.
The advancing generation of endoscopic spine surgery.
Image-guided assistance is feasible and applicable in endoscopic spinal approach.
It will provide several advantages over conventional C-arm fluoroscopy.
On the other hand, the method is still heavy, time consuming, and might be improved according to the radiological facilities [21].
It comes as no surprise that the field of endoscopic spine surgery, like any other novel field in surgery, requires the surgeon to overcome the barriers that come along the transition from open or microscopic spine surgery to more minimally invasive yet technically demanding approaches, Therefore, to guarantee a successful transition from conventional open spine surgery to an endoscopic spine practice surgeons should aim to [22, 23].
Have a good fundamental grasp the pathophysiology of neurogenic pain
Correlate surgical anatomy with symptomatic pain generators.
Employ a staged management approach going from least invasive to most invasive.
Avoid doing fusions for pain management unless there is gross instability or deformity.
When it comes to data entailing the number of cases in a learning curve, Hsu et al. showed that the plateauing of the learning curve for the transforaminal approach occurred around the 10th case [9, 24], Lee et al. reached a similar finding by observing a significant reduction in the operative time after the17th patient was treated by percutaneous endoscopic lumbar discectomy [9, 25]. At the same time, Choi et al. recommended supervision by an experienced surgeon in the initial 10 cases to overcome the learning curve for the interlaminar procedure at L5-S1 [9, 26] and the approximate cutoff point of the learning curve of biportal endoscopy surgery was around 54 cases [27].
Therefore, certain considerations must be put in mind to tackle this learning curve [22]:
Define the patient target group.
Identify endoscopic surgeries to learn.
Attend professional and society meetings and courses.
Practice in cadaver workshops.
Identify mentors and observe live surgeries.
Employ reliable diagnostic prognosticators.
Start with selective blocks.
Then start with simple far lateral soft disc herniations.
Expand to paracentral and central disc herniations.
Expand to foraminal and lateral recess stenosis.
Analyze outcomes and contribute.
Present and publish your outcomes.
Teach others and become a mentor.
And always remember that a learning curve is not an achievement curve, proper guidelines and goal setting for education and training are more important than ever, and it is necessary to discuss creating a consensus between endoscopic academic societies and experts [28].
Dura tear rate is approximately 3% in endoscopic spine surgery [29, 30]. The rate is higher in decompression and fusion than in discectomy.
To give a general estimation of the magnitude of such complications, let us look at the study conducted by Lewandrowski et al. covering more than 64,000 cases of spinal endoscopy; where the durotomy incidence was that of 1.07% [31].
Medium-sized dural tears (1–10 mm) were the most common (52.2%; 48/93). Small pinhole durotomies (less than 1 mm) were the second most common type (46.7%; 43/93). Rootlet herniations were seen by 46.2% (43/93) of responding surgeons.
The posterior dural sac injury during the interlaminar approach (57%; 53/93) occurred more frequently than traversing nerve-root injuries (31.2%) or anterior dural sac (23.7%; 22/93).
Exiting nerve-root injuries (10.8%;10/93) were less common.
The majority of participating surgeons (64%; 57/89) reported that the long-term outcome was unaffected. Only 18% of surgeons reported having seen the development of a postoperative cerebrospinal fluid (CSF)-fistula (18%;16/89). However, the absolute incidence of CSF fistula was only 0.025% (16/64 470).
Severe radiculopathy with dysesthesia; sensory loss; and motor weakness in association with an incidental durotomy were reported by 12.4% (11/89), 3.4% (3/89), and 2.2% (2/89) of surgeons, respectively [31].
5.2 Vascular injury
Injuries to the segmental artery are the main concern.
Segmental artery injury mainly occurs during transforaminal work, especially when decompressing the exiting nerve root; because the segmental artery passes under the exiting nerve root, this segmental artery injury may induce serious retroperitoneal hematoma [32, 33].
5.3 Infections
Discitis or any other SSI after lumbar endoscopic surgery is very rare.
One study reported an infection rate of 0.11% [32, 34].
5.4 Water irrigation-related neck and head pain
Postoperative raised ICP can occur secondary to high endoscopic saline inflow and it can lead to cerebral edema and seizure, which can also be intraoperatively [35]. Prevention is key.
The ideal water pressure used is said to be around 30 mmHg (25–50 mmHg) [29, 35, 36].
5.5 Hematoma
Kim et al. showed approximately 25% hematoma rate in biportal endoscopic spine surgery, with only 1.2% requiring revision due to the hematoma.
Careful hemostasis is key to preventing postoperative hematoma formation. In the presence of an increase in the neurological deficit of bilateral limbs postoperatively, a low threshold for revision decompression and hematoma drainage is necessary [29, 37].
5.6 Postoperative dysesthesia
Postoperative dysesthesia is a common complaint.
Minimal dorsal root ganglion retraction is essential for preventing postoperative dysesthesia. Kim et al. showed interlaminar contralateral approach has less postoperative dysesthesia rate than transforaminal endoscopic lumbar discectomy [29, 38].
5.7 Missed fragments
Even in experienced hands, some herniations remain technically difficult. In literature, huge central disc herniations and highly migrated disc herniations have high failure rates [30, 39, 40].
The success of the procedure is attributed to proper preoperative planning based on the MRI.
Avoidance of complications is enhanced by the ability to visualize normal and pathoanatomy clearly, and use of local anesthesia and conscious sedation rather than general or spinal anesthesia [41].
With advancements in implant and instrument technology and the incorporation of robotic technology, surgical indications may be expanded into motion-preserving scoliosis surgeries, tumor resections, and more complex surgical procedures. As we move towards a patient-centered and cost-effective healthcare model, we may see endoscopic spine surgery become increasingly relevant to the future of spine surgical practice with improved patient outcomes and decreased medical costs [42].
The reasons behind the hindered widespread acceptance and uptake could, in part be the parallel explosions in other potentially more lucrative fields within spinal surgery, such as instrumentation, expandable technologies, biologics, navigation, and robotics [43] along with the unfamiliarity with the equipment and approach.
Over the few years, increasing recognition of the physiological footprint imparted upon the patient by traditional open surgery, combined with a historically nihilistic approach to operating upon the elderly and infirm, a population that often needs our help the most, and traditionally negative public perceptions of spinal surgery, have led to the rise of enhanced recovery after surgery (ERAS) programs, with endpoints of reducing pain and narcotic consumption, hastening postoperative mobility and recovery, improving patient satisfaction, and reducing the length of stay and costs [44, 45].
So all data suggests that there will be a decisive shift towards such techniques in the upcoming years once we set up plans to overcome the difficulties, tackle the learning curve, and set up systemized training programs.
Spinal endoscopy is a minimally invasive procedure used to diagnose and treat spinal disorders. It involves inserting a small camera and specialized instruments into the spinal canal through a small incision in the skin. Spinal endoscopy is less invasive than traditional open surgery, which can result in less blood loss, less pain, and faster recovery times.
Recent advances in technology and surgical techniques have made spinal endoscopy a safe and effective option for many spinal conditions. Spinal endoscopy is being used to treat conditions such as spinal stenosis, herniated discs, and spinal tumors. It has also been used in spinal fusion procedures and to address failed back surgery syndrome.
While spinal endoscopy has shown promising results, it is not always the best option for every patient or condition. The decision to use spinal endoscopy should be made by a skilled and experienced surgeon who can evaluate each patient’s unique needs and medical history.
The learning curve for spinal endoscopy can be steep, as the procedure requires a high level of technical skill and expertise. The surgeon must be able to navigate the instruments and camera through the narrow spinal canal while avoiding damage to the delicate spinal structures.
Training in spinal endoscopy typically involves a combination of didactic instruction, observation of experienced surgeons, and hands-on practice in cadaveric and animal models. Surgeons may also participate in live surgery courses and attend conferences to develop their skills further.
In addition to technical skills, surgeons must thoroughly understand spinal anatomy and pathology to perform spinal endoscopy safely and effectively. They must also be able to recognize and manage potential complications, such as nerve damage or cerebrospinal fluid leaks.
While the learning curve for spinal endoscopy is steep, many surgeons can perform the procedure safely and effectively with appropriate training and practice. As with any surgical procedure, patient outcomes depend on the surgeon’s skill and experience, as well as the patient’s medical history and condition.
The future for spinal endoscopy is bright, and it is a trend that every spine surgeon should seek and a skill that each acquires.
References
1.Michael Mayer H. A history of endoscopic lumbar spine surgery: What have we learnt? BioMed Research International. 2019, Article ID 4583943;2019:8. DOI: 10.1155/2019/4583943
2.Hijikata S, S. A. A method of percutaneous nuclear extraction. Journal of Toden Hospital. 1975;5(5):39
3.Forst R, Hausmann B. Nucleoscopy--a new examination technique. Archives of Orthopaedic and Trauma Surgery. 1978). 1983;101(3):219-221. DOI: 10.1007/BF00436774
4.Kambin P, Nixon JE, Chait A, Schaffer JL. Annular protrusion: Pathophysiology and roentgenographic appearance. Spine (Phila Pa 1976). 1988;13(6):671-675
5.Simpson AK. Spinal endoscopy: Evidence, techniques, global trends, and future projections. The Spine Journal. 2022;22(1):64-74
6.Hofstetter CP, Ahn Y, Choi G, et al. AOSpine consensus paper on nomenclature for Working-Channel endoscopic spinal procedures. Global. Spine Journal. 2020;10(Suppl. 2):111S-121S. DOI: 10.1177/2192568219887364
7.Ahn Y. Current techniques of endoscopic decompression in spine surgery. Annals of Translational Medicine. 2019;7(S5):S169-S169. DOI: 10.21037/atm.2019.07.98
8.Krishnan A, Kim HS, Raj A. Bharat R Dave: Expanded indications of full endoscopic spine. Journal of Minimally Invasive Spine Surgery and Technique. 2020;6(Suppl. 1):S130-S156. DOI: 10.21182/jmisst.2021.00129
10.Englund J. Lumbar spinal stenosis. Current Sports Medicine Reports. 2007;6:50-55. DOI: 10.1007/s11932-007-0012-0
11.Ahn Y. Endoscopic spine discectomy: Indications and outcomes. International Orthopaedics. 2019;43(4):909-916. DOI: 10.1007/s00264-018-04283-w Epub 2019 Jan 5
12.Wagner R, Haefner M. Indications and contraindications of full-endoscopic Interlaminar lumbar decompression. World Neurosurgery. 2021;145:657-662. DOI: 10.1016/j.wneu.2020.08.042 Epub 2020 Aug 15
13.Yue JJ, Long W. Full endoscopic spinal surgery techniques: Advancements, indications, and outcomes. International Journal of Spine Surgery. 2015;9:17. DOI: 10.14444/2017
15.Ruetten S, Komp M, Merk H, Godolias G. Full-endoscopic cervical posterior foraminotomy for the operation of lateral disc herniations using 5.9-mm endoscopes: A prospective, randomized, controlled study. Spine (Phila Pa 1976). 2008;33(9):940-948. DOI: 10.1097/BRS.0b013e31816c8b67
16.Ahn Y. Percutaneous endoscopic cervical discectomy using working channel endoscopes. Expert Review of Medical Devices. 2016;13(6):601-610. DOI: 10.1080/17434440.2016.1180245 Epub 2016 Apr 27
17.Ruetten S, Komp M, Merk H, Godolias G. Full-endoscopic anterior decompression versus conventional anterior decompression and fusion in cervical disc herniations. International Orthopaedics. 2009;33(6):1677-1682. DOI: 10.1007/s00264-008-0684-y Epub 2008 Nov 18
18.Middleton SD, Wagner R, Gibson JNA. Multi-level spine endoscopy: A review of available evidence and case report. EFORT Open Reviews. 2017;2(7):317-323 Retrieved Feb 28, 2023, from https://eor.bioscientifica.com/view/journals/eor/2/7/2058-5241.2.160087.xml
19.Kim HS, Wu PH, Raorane HD, Jang IT. Generation change of practice in spinal surgery: Can endoscopic spine surgery expand its indications to fill in the role of conventional open spine surgery in Most of degenerative spinal diseases and disc Herniations: A study of 616 spinal cases 3 years. Neurology India. 2020;68(5):1157-1165. DOI: 10.4103/0028-3886.299145
20.Dong H, Dong L, Hyeun-Sung K, Hungtae C. Recent trends and changes in the endoscopic spinal surgery. Journal of Minimally Invasive Spine Surgery and Technique. 2021;6:S81-S83. DOI: 10.21182/jmisst.2021.00136
21.Assaker R, Reyns N, Pertruzon B, Lejeune JP. Image-guided endoscopic spine surgery: Part II: Clinical applications. Spine (Phila Pa 1976). 2001;26(15):1711-1718. DOI: 10.1097/00007632-200108010-00016
22.Ransom NA, Gollogly S, Lewandrowski KU, Yeung A. Navigating the learning curve of spinal endoscopy as an established traditionally trained spine surgeon. Journal of Spine Surgery. 2020;6(Suppl. 1):S197-S207. DOI: 10.21037/jss.2019.10.03
23.Hasan GA. How to Go Further with My Clinical Practice on Unilateral Biportal Endoscopy. In Springer eBooks. 2022. pp. 125-135. DOI: 10.1007/978-3-031-14736-4_10
24.Hsu HT, Chang SJ, Yang SS, Chai CL. Learning curve of full-endoscopic lumbar discectomy. European Spine Journal. 2013;22(4):727-733. DOI: 10.1007/s00586-012-2540-4 Epub 2012 Oct 17
25.Lee DY, Lee SH. Learning curve for percutaneous endoscopic lumbar discectomy. Neurologia Medico-Chirurgica (Tokyo). 2008;48(9):383-388; discussion 388-9. DOI: 10.2176/nmc.48.383
26.Choi G, Lee SH, Raiturker PP, Lee S, Chae YS. Percutaneous endoscopic interlaminar discectomy for intracanalicular disc herniations at L5-S1 using a rigid working channel endoscope. Neurosurgery. 2006;58(Suppl. 1):ONS59-ONS68; discussion ONS59-68. DOI: 10.1227/01.neu.0000192713.95921.4a
27.Xu J, Wang D, Liu J, Zhu C, Bao J, Gao W, et al. Learning curve and complications of unilateral Biportal endoscopy: Cumulative sum and risk-adjusted cumulative sum analysis. Neurospine. 2022;19(3):792-804. DOI: 10.14245/ns.2143116.558 Epub 2022 Aug 15
28.Bae J, Kim JS. Building a successful practice of endoscopic spine surgery: Learning, setting the goal, and expanding the border. Neurospine. 2022;19(3):571-573. DOI: 10.14245/ns.2244712.356 Epub 2022 Sep 30
29.Wu PH, Kim HS, Choi DJ, Gamaliel Y-HT. Overview of tips in overcoming learning curve in Uniportal and Biportal endoscopic spine surgery. Journal of Minimally Invasive Spine Surgery & Technique. 2021;6(Suppl. 1):S84-S96. DOI: 10.21182/jmisst.2020.00024
30.Kim HS, Sharma SB, Wu PH, Raorane HD, Adsul NM, Singh R, et al. Complications and limitations of endoscopic spine surgery and percutaneous instrumentation. Indian Spine Journal. 2020;3:78-85
31.Lewandrowski KU, Hellinger S, De Carvalho PST, Freitas Ramos MR, Soriano-SáNchez JA, Xifeng Z, et al. Dural tears during lumbar spinal endoscopy: Surgeon skill, training, incidence, risk factors, and management. International Journal of Spine Surgery. 2021;15(2):280-294. DOI: 10.14444/8038 Epub 2021 Apr 1
32.Lewandrowski K-U, Telfeian AE, Hellinger S, León JFR, Teixeira PS, de Carvalho MRF, et al. Anthony Yeung: Difficulties, challenges, and the learning curve of avoiding complications in lumbar endoscopic spine surgery, international journal of spine. Surgery. 2021;15(suppl. 3):S21-S37. DOI: 10.14444/8161
33.Zhou C, Zhang G, Panchal RR, Ren X, Xiang H, Xuexiao M, et al. Unique complications of percutaneous endoscopic lumbar discectomy and percutaneous endoscopic Interlaminar discectomy. Pain Physician. 2018;21(2):E105-E112
34.Lewandrowski KU. Incidence, management, and cost of complications after transforaminal endoscopic decompression surgery for lumbar foraminal and lateral recess stenosis: A value proposition for outpatient ambulatory surgery. International Journal of Spine Surgery. 2019;13(1):53-67. DOI: 10.14444/6008
35.Parpaley Y, Urbach H, Kovacs A, Klehr M, Kristof RA. Pseudohypoxic brain swelling (postoperative intracranial hypotension-associated venous congestion) after spinal surgery: Report of 2 cases. Neurosurgery. 2011;68(1):E277-E283. DOI: 10.1227/NEU.0b013e3181fead14
36.Choi G, Kang HY, Modi HN, Prada N, Nicolau RJ, Joh JY, et al. Risk of developing seizure after percutaneous endoscopic lumbar discectomy. Journal of Spinal Disorders & Techniques. 2011;24(2):83-92. DOI: 10.1097/BSD.0b013e3181ddf124
37.Kim JE, Choi DJ, Park EJ. Evaluation of postoperative spinal epidural hematoma after Biportal endoscopic spine surgery for single-level lumbar spinal stenosis: Clinical and magnetic resonance imaging study. World Neurosurgery. 2019;126:e786-e792. DOI: 10.1016/j.wneu.2019.02.150 Epub 2019 Mar 14
38.Kim HS, Kim JY, Wu PH, Jang IT. Effect of dorsal root ganglion retraction in endoscopic lumbar Decompressive surgery for Foraminal pathology: A retrospective cohort study of Interlaminar contralateral endoscopic lumbar Foraminotomy and discectomy versus Transforaminal endoscopic lumbar Foraminotomy and discectomy. World Neurosurgery. 2021;148:e101-e114. DOI: 10.1016/j.wneu.2020.12.176 Epub 2021 Jan 11
39.Choi KC, Lee JH, Kim JS, Sabal LA, Lee S, Kim H, et al. Unsuccessful percutaneous endoscopic lumbar discectomy: A single-center experience of 10,228 cases. Neurosurgery. 2015;76(4):372-380; discussion 380-1; quiz 381. DOI: 10.1227/NEU.0000000000000628
40.Lee SH, Kang BU, Ahn Y, Choi G, Choi YG, Ahn KU, et al. Operative failure of percutaneous endoscopic lumbar discectomy: A radiologic analysis of 55 cases. Spine (Phila Pa 1976). 2006;31(10):E285-E290
41.Percutaneous Endoscopic Spine Surgery (History, Indications and Complications) [internet]. Available from: http://www.axis-hospital-croatia.com/percutaneous-endoscopic-spine-surgery-history-indications-and-complications/
42.Moon ASM, Rajaram Manoharan SR. Endoscopic spine surgery: Current state of art and the future perspective. Asian Spine Journal. 2018;12(1):1-2. DOI: 10.4184/asj.2018.12.1.1 Epub 2018 Feb 7
43.Yoon J, Wang M. The evolution of minimally invasive spine surgery. Journal of Neurosurgery: Spine. 2019;30:149-158. DOI: 10.3171/2018.11.SPINE181215
44.Dietz N, Sharma M, Adams S, Alhourani A, Ugiliweneza B, Wang D, et al. Enhanced recovery after surgery (ERAS) for spine surgery: A systematic review. World Neurosurgery. 2019;130:415-426. DOI: 10.1016/j.wneu.2019.06.181 Epub 2019 Jul 2
45.Is There a Bright Future for Endoscopic Spinal Surgery?[internet]. Available at: https://spinalnewsinternational.com/is-there-a-bright-future-for-endoscopic-spinal-surgery/
Written By
Ghazwan Abdulla Hasan and Mustafa Hayder Qatran
Submitted: 10 March 2023Reviewed: 13 March 2023Published: 15 November 2023
 Open access peer-reviewed chapter
Open access peer-reviewed chapter