 Open access peer-reviewed chapter
Open access peer-reviewed chapter
Abstract
Vascular access (VA) is the life line for hemodialysis (HD) but also Achilles’ heel. VA consists of HD catheters, arterio-venous fistula and arterio-venous grafts. From the earlier ‘Fistula First’ initiative, we later moved to ‘Fistula First, catheter last’ approach and have now realized that we need to follow the recommendation for End Stage Kidney Disease (ESKD) patients, given by Kidney Disease Outcome Quality Initiative (KDOQI). It says, “Patient First: ESKD Life-Plan” to attain the “right access, in the right patient, at the right time, for the right reasons”. However, this applies to the creation of VA. It is essential to monitor and do VA surveillance to maintain the VA, as it can malfunction. When the VA malfunctions, it needs intervention. Depending upon the type of VA, the intervention varies. It could be endovascular or surgical. These issues will be highlighted in this chapter.
Keywords
- chronic kidney disease
- hemodialysis vascular access
- hemodialysis catheters
- arterio-venous fistula for hemodialysis
- arterio-venous grafts for hemodialysis
- problems of vascular access for hemodialysis
1. Introduction
A better HD VA leads to better survival, the ideal HD conduit is elusive and one has to really strive hard to capitalize on the already scare resource of vascular estate. HD VA remains the leading cause of morbidity and mortality among HD patients. The types of VA include HD catheters (non-cuffed and tunneled cuffed), arterio-venous (AV) shunt, AV fistula (AVF) and AV graft (AVG). The heroes and themes of Greek mythology have had a great impact in the medical literature. For example, we use the term hydra-headed for the kind of problem caused by VA, which is like a multifarious evil, not to be overcome by a single effort, a problem that poses more problems. One would call it Herculean task, that’s difficult and needs enormous strength. It’s a process that once begun has potential to generate many complicated problems, like Pandora’s Box. HD access related problems are called Achilles’ heel, a term used to describe the weak point. Recently another term has been added, dedicated to disentanglement of factors hindering our efforts to create a perfect VA for dialysis—a truly Sisyphean task [1].
In the 1950’s, though the technical devices were available for regular HD treatments like Kolff 's twin-coil kidney [2], the Achilles heel was a reliable access to the circulation for multiple use which did not exist. The VA situation has not changed over the years. One has to create, allow it to mature (AVF, AVG), maintain it and salvage in case of malfunction before ultimately deciding to abandon it. The earlier VA guidelines of last decade have been replaced by end stage kidney disease (ESKD) life plan [3], where the emphasis is on the individualization of VA care on the basis of patient and disease characteristics. With increasing observation that AVF-prioritized care is particularly ineffective in certain patient groups, these latest VA guidelines have shifted recommendations from a standardized to a customized approach, recommending placement of the “right access, in the right patient, at the right time, for the right reasons”. In this chapter, we shall deal with VAs creation, maintenance and salvage, except AV shunts. One has to keep local practice factors, values, preferences and varying clinical needs in mind while considering all the aspects.
Sometimes, VA is created for urgent start HD, or as a bridge to AV fistula maturation or kidney transplantation. An ideal bridge device would allow for immediate use following placement, provide blood flow rates sufficient to ensure adequate HD, have a low complication rate, and have sufficient length of technical survival to allow AVF development and maturation without the need for device replacement [4]. There were various devices. Scribner’s shunt in 1960, had external silicone rubber/Teflon tubing connected to a vein and artery at the wrist enabling relatively high rates of blood for HD. In 1964, Dr. Shaldon used two single lumen catheters in the femoral vein as an HD access for daily home dialysis for acute renal failure. 1980s saw development of hybrid transcutaneous access devices comprising an AVG and a port, and totally implanted blood ports for HD treatment were introduced in 1996. The shunts and ports are no more used.
In 1965, Drs. Cimino and Brescia described AVF [5] and in 1976, chronic HD with an expanded polytetrafluroethylene graft (ePTFE) was described [6]. 1982 saw development of double lumen non cuffed double ‘D’ configuration HD catheter, and 1987 saw availability of Dacron cuffed double lumen HD catheters. Both these could be used immediately, whereas, after the creation of AVF and AVG, maturation occurs in the form of morphological changes in the body (venous remodeling for AVF) and these accesses should be used for HD only after they have matured. Recently, early cannulation AVG are in use with median time to first cannulation of 3 days [7]. HeRO Graft ® (Hemodialysis Reliable Outflow) is a fully subcutaneous AV access device currently available to maintain long-term access for HD patients with
2. The ‘temporary’ non-cuffed, non-tunneled acute HD catheters: (non-TCC)
2.1 Creation
There is no timing for creation of this access as this is for ‘emergency’ HD, though it is also used for elective HD. The usual sites are internal jugular vein or femoral vein, with tip position in superior (SVC) or inferior vena cava (IVC). The use of non-TCC dialysis catheters in acute situations can be justified. The use of non-cuffed catheters should be restricted to critically ill intensive care unit patients or for “in and out” purpose of those with temporary loss of a permanent access. Use of femoral non-TCC should be restricted to those unable to lie down, and for not more than 7 days. Many centers across the world use internal jugular vein (IJV) catheters for acute situations and for initiation of chronic HD as per local factors and customs [8]. Internal jugular catheters may be left in place for up to 3 weeks without a high risk of bacteremia, but femoral catheters should be removed after 1 week [9]. There should be a plan to discontinue or convert any short-term catheter to a long-term catheter. These catheters should not be used as stop gap access while waiting for AV fistula to mature, because the AV fistula, if created after initiation of dialysis in ESKD situation will take at least 6 weeks to mature. There is a great variability of the vein caliber and its position in relation to the common carotid artery. Ultrasound guidance is therefore strongly recommended during insertion to reduce the 7–10% risk of carotid puncture to virtually zero.
2.2 Problems during creation
Risks of arterial puncture, hematoma, tracheal compression, pneumothorax (Figure 1) or hemothorax, injury to local structures, air embolism and catheter malposition (Figure 2) are well described complications. Problem of guide wire breaking and catheter tip banding was encountered by the author (Figure 3). This is a rare complication, which was recognized immediately, otherwise it could have caused the embolization of the broken piece of the guide wire and more complications. The clue to avoid such complications is to ensure that the entry and movement of the wire while inside the vein should be very smooth, and stop if any resistance is encountered. Always check the shape of the guide wire once it comes out of the body, it should be straight and almost in the original shape, to ensure that no complication of the kind described has happened. Proper length should be chosen to place the tip of non-TCC in the SVC for IJV catheters or within the IVC above the confluence of iliac veins for femoral HD catheters and the tip of the catheter should be in the middle of the vein away from the vessel wall so that the ‘arterial’ end of the catheter (withdrawal lumen – which is under negative pressure), does not cause flow problems during HD by becoming occluded due to the vessel wall being sucked across it. If shorter length is used by mistake, especially for left IJV site, it could touch the wall of SVC and cause flow problems. The femoral non-TCC could also cause flow problem in obese patients.

Figure 1.
Pneumothorax with non-TCC.
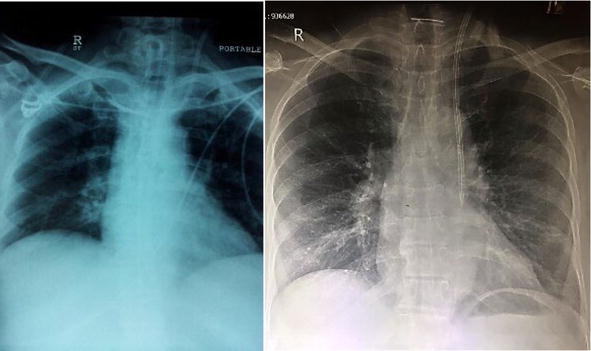
Figure 2.
IJV non-TCC tip malposition (more common with left sided non-TCC).
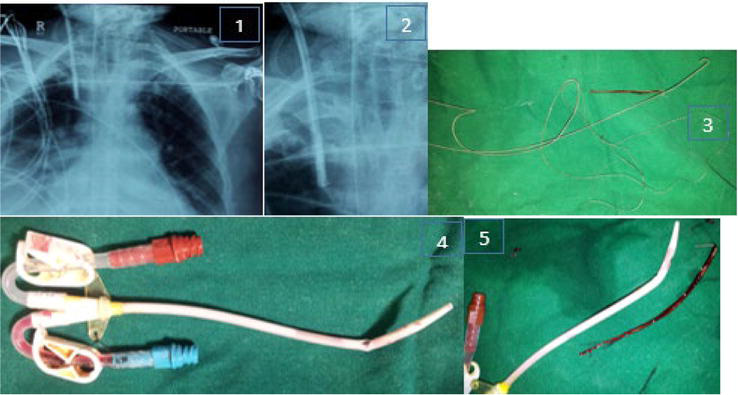
Figure 3.
Complication of non-TCC insertion. 1) chest X-ray after insertion, showed that the tip was blunted (which should be tapering, as per the catheter design). 2) close look at the X-ray, something visible within the lumen and jutting out of the catheter. 3) broken guide wire. 4) the catheter bend. 5) the broken and retained piece of guide wire, corresponding to the catheter bend.
2.3 Maintenance
The catheter care is required to prevent infection and clotting. The catheter dressing should be clean and dry. The caps and clamps of the catheters should be kept tightly closed to prevent bleeding and air embolism. The ‘scrub the hub’ protocol suggested by ‘Making dialysis safer coalition’ and Center for disease control, USA, should be followed during connection and disconnection process. The caps of the catheter should kept in a sterile bowl containing compatible antimicrobial solution during the duration of HD. To maintain patency of the catheter between the dialysis treatments, heparin is instilled into the lumens. The amount of heparin to be filled is mentioned on the catheter and varies by manufacturer and by the size of the catheter. The concentration of heparin used could be 1000 to 5000 units per ml as per center protocol.
2.4 Salvage
If the non-TCCs are kept in place within stipulated time interval, usually they work well. However, they can develop problems of poor flows and infection if not handled properly, within 1–2 weeks also. Thrombosis occurs due to infection or due to improperly placed catheter tip touching the vessel wall. If such situations have occurred, it is advisable to change catheter (may be railroaded) to appropriate size and proper tip position. Infected non-TCC should be removed immediately and re-sited. Exchange of infected non-TCC over a wire should be avoided.
3. The tunneled cuff HD catheters (TCC)
3.1 Creation
A high proportion of ESKD patients (>50%) need to be initiated on HD urgently by a central venous catheter. The ‘Fistula First’ initiative was meant to increase the AVF prevalence and reduce catheter dependency, introduced by Centers for Medicare and Medicaid Services (CMS) and End Stage Renal Disease (ESRD) network in 2003, which transitioned to Fistula First Breakthrough Initiative (FFBI) in 2005, and in 2007, the proposal was to have “Fistula First, Catheter Last’ initiative. This was necessary, because the success of Fistula First initiative had a downside of increased HD catheters incidence, probably because the focus on increasing fistulas may have inadvertently diverted attention away from decreasing dependence on HD catheters [10]. In spite of all efforts, around 80% of patients get initiated on HD with catheters, in USA [11] and remain on catheters beyond 90 days. It is apparent that TCCs are going to be around till all CKD patients have AV fistula created in the pre HD stage. Complete avoidance of TCCs seem unlikely at this moment, and it’s like sleeping with the enemy. The catheter conundrum exists where one hates living with them but cannot live without them [12]. Hence it is necessary that nephrologist’s must be aware about its insertion techniques, usage and tackle complications, from first day of insertion so as to improve TCC performance and prolong its life, to reduce the morbidity, mortality, and overall cost of the catheters, but with an aim to avoid extended catheter use.
3.2 Insertion of TCCs
As per the KDOQI vascular access guidelines of 2019 [3], it is considered reasonable in valid clinical circumstances to use TCCs for short-term or long-term durations for incident patients. The indications of insertion are varied and include ESKD patient starting on planned long term HD without AV fistula in place, or as a bridge to transplantation. It could also be used for elderly patients if it fits into the patient’s ESKD L-I-F-E plan (Patient Life-Plan First then Access Needs). Another situation where it is used is for likely prolonged recovery from AKI, or patients requiring prolonged extra-corporeal therapies, like plasma exchange etc.
Short term duration for TCCs includes AVF or AVG created but not ready for use and dialysis is required, acute transplant rejection or other complications requiring dialysis, peritoneal dialysis (PD) patient with complications that require time-limited peritoneal rest or resolution of complication (e.g. pleural leak), patient has a living donor transplant confirmed with an operation date in the near future (<90 days), and AVF or AVG complication such as major infiltration injury or cellulitis that results in temporary nonuse until problem is resolved. As per the same guidelines, long-term or indefinite duration TCC indications include multiple prior failed VA with no available VA creation options, limited life expectancy, valid patient preference and special medical circumstances. KDOQI considers it reasonable to use TCC in preference to non-TCC due to the lower infection risk with TCC.
The insertion should be in the sterile environment with standard aseptic precautions. The Center for Disease Control (CDC) guidelines for the prevention of intravascular catheter related infections (2011) states that use maximal sterile barrier precautions, including the use of a cap, mask, sterile gown, sterile gloves, and a sterile full body drape, for the insertion or guide wire exchange. The COVID 19 mitigation measures have shown further reduction in catheter related blood stream infection (CRBSI) during the pandemic, superimposed on the non-pandemic related reductions in some facilities before the pandemic, emphasizing the role of aseptic measures. Even after the pandemic, it may be prudent to continue COVID 19 mitigation measures to prevent CRBSI [13].
Use of USG guidance and image intensifier is mandatory. Contrary to this recommendation, COVID 19 pandemic has brought out studies on bed side TCC insertion and its safety [14], where authors concluded that bedside right internal jugular TCC placement in COVID-19 patients, using ultrasound and anatomic landmarks without fluoroscopic guidance, may potentially reduce the risk of COVID-19 transmission among healthcare workers without compromising patient safety or catheter function. In another study, the authors concluded that bedside TCC placement has served to conserve resources, prevent complications with transport to and from the operating room, and decrease personnel exposure during the COVID-19 pandemic. This strategy warrants further consideration and could be used in critically ill patients regardless of COVID status [15]. In the pre-COVID era, a study showed that the placement of TCC by Nephrologist, with the help of USG Doppler & post placement x-ray chest was found to be a safe procedure where access to fluoroscopy was not available [16]. The TCC is recommended to be inserted (in order of preference), in the internal jugular veins (IJV), external jugular veins (EJV), femoral veins, subclavian veins, trans lumbar, trans renal and trans hepatic locations. These are adaptations as per circumstances and cannot be generalized. Except for right IJV insertions, (and rarely left IJV, authors’ personal experience) other sites cannot be used for insertion without fluoroscopic guidance. Fluoroscopic guidance is also required as left sided SVC or double SVC are known (Figure 4).
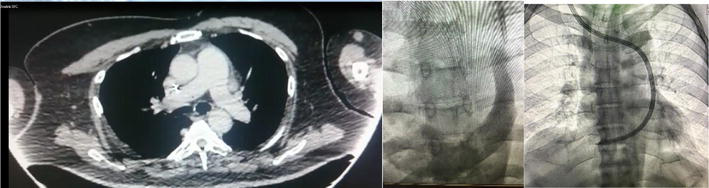
Figure 4.
Double SVC, left sided SVC.
The length and diameter of the TCC should be appropriate and chosen keeping Hagen-Poiseuille equation in mind, which states that flow is inversely proportional to length. The resistance to blood flow is directly related to catheter length and inversely proportional to the fourth power of the diameter of the hemodialysis catheter. A slight increase in the inner diameter of the arterial and venous lumens will result in a large increase in the rate of blood flow through the catheter [17]. So the chosen catheter should be long enough that the tip can reach the intended target site, but it should otherwise be as short as possible to minimize resistance to flow. As per Dr. Gerald Beathard, father of interventional nephrology in USA, (personal data), diameter is the major factor and 19% increase in diameter leads to increase in the flow by 2 times and 50% increase in diameter by 5 times. Increasing the diameter from 2 to 2.1 mm will increase the flow by 21%. Catheter length is less important, as 19% increase in diameter will compensate for doubling of length. The mechanical catheter design helps improve rheology. The ideal catheter should give maximum flow, and reduce the risks of clotting or fibrin sheath formation. This needs good tip design. Various tip designs are available e.g. step tip, split tip, symmetrical tip etc.
TCC tip design and position plays very important role in the working of the catheters. Catheter tip should ideally be in the right atrium, such that it moves within the atrium during breathing or patient sitting up during dialysis (Figure 5). The problem of TCC getting pulled up in the SVC, causing flow problem during dialysis is encountered more with staggered tip TCC when the tip is not placed within RA, and the proximal arterial end abutting against the SVC wall during inspiration and due to ultrafiltration. We should be aware that the right atrial morphology, configuration and geometry varies among individuals.
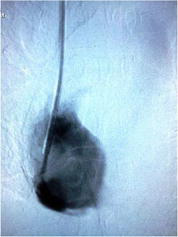
Figure 5.
The proper tip of TCC.
3.3 Problems during insertion
Experience in practice placement and referral to interventional nephrologists would decrease complication rate and may decrease subclavian vein usage for catheter placement. However, complications like pneumo or hemothorax do happen, as also air-embolism, bleeding from local site or cardiac arrhythmias. There is a chance of arterial puncture in spite of USG guidance (Figure 6), catheter malposition in the posterior mediastinum (Figure 7), tip in the azygous vein, outside SVC, or have a kink inside the SVC when fluoroscopic guidance is not used (Figure 8a and b). A kink in the catheter after insertion would not give a proper flow (Figure 9). TCC re-inserted in the vein which already had a catheter, which malfunctioned, could result in problems of flow (Figure 10), where the inserted TCC malfunctioned within few days, due to presence of a clot around the catheter tip and in the SVC, with a suspicious catheter related sheath (CRS, also called fibrin sheath), probably both pre-existing. Improper size of catheter (Figure 11) would cause flow problems immediately or after few days.

Figure 6.
TCC in the arterial system (courtesy Dr. Ravindra Madraki, Bijapur, India).
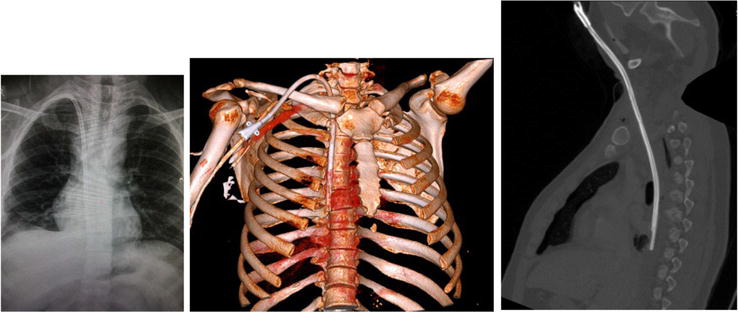
Figure 7.
TCC appeared to be well placed is actually in the posterior mediastinum, with hydro pneumothorax.
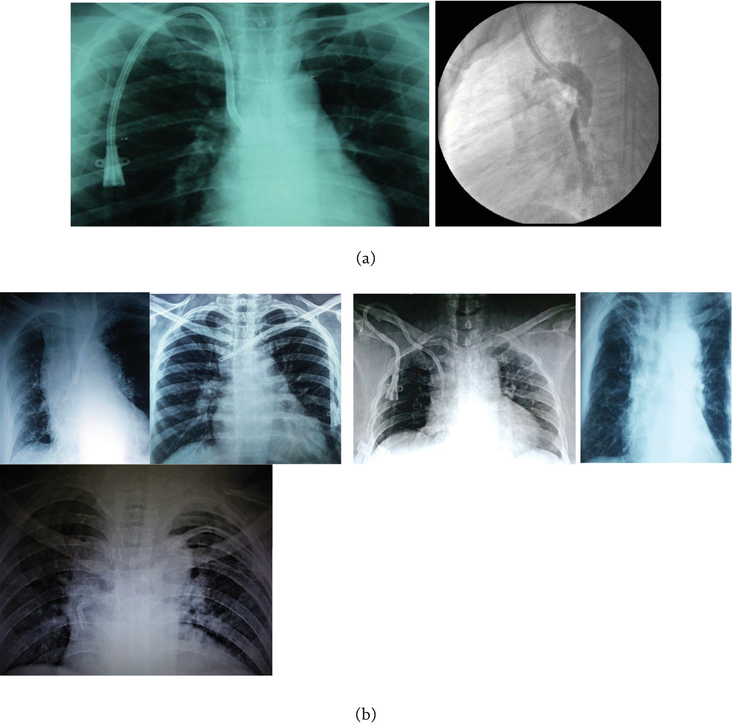
Figure 8.
A: Catheter tip misplaced in the azygous vein (courtesy Dr. Sampath Kumar, Madurai, India). b: Catheter tip misplacement, right IJV catheter in the wrong positions, left subclavian catheter left out of the right atrium.
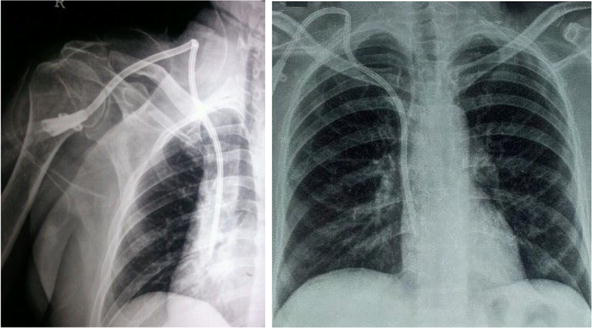
Figure 9.
Catheter kink TCC in right EJV, corrected.

Figure 10.
TCC with poor flow, due to clot in SVC and around catheter tip, with double shadow on right side of TCC suggestive of CRS (catheter related sheath, also known as fibrin sheath) (figure courtesy Dr. Nikhil Rathi, Pune, India).
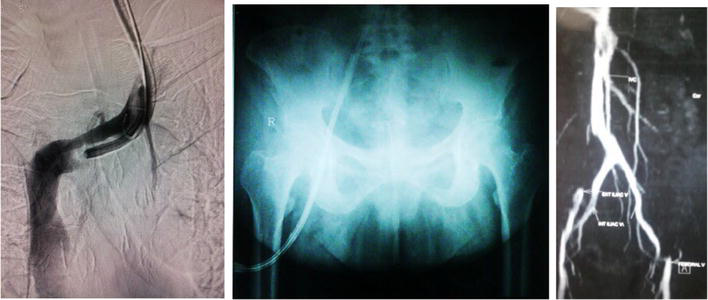
Figure 11.
Improper size of TCC in left IJV with clot and (removed) short length TCC in right femoral vein resulting in complete thrombosis of right external iliac vein.
As a general rule, when the TCC insertion is planned with prior use of the same vein in the past, one should always be prepared to perform angiography to delineate the venous system (Figure 12). In such situations, it would be ideal to use Surfacer® device if available for in-side out venous access. In absence of the same, authors have used long Chiba needle to puncture the completely occluded venous segment to gain the guide wire entry, do angioplasty and insert TCC.
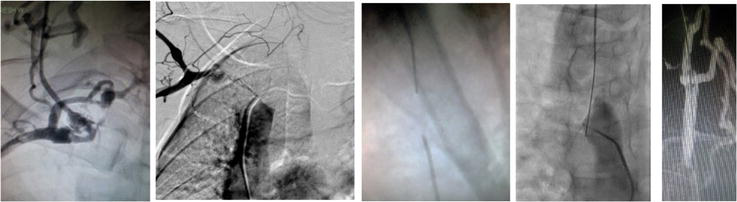
Figure 12.
Crossing the CTO with Chiba needle to get the wire across for TCC insertion.
3.4 Maintenance of TCC
Complications of TCC are CRBSI and clot and cause poor TCC performance. The sterile precautions mentioned while handling non-TCC also apply to TCC during connection and disconnection process of HD. Catheter dysfunction leading to inadequate dialysis has been defined based solely upon blood flow measurement. However, there is concern that using the blood flow rate as the only criterion can be misleading and has the potential to result in a significant number of unnecessary interventions. Other factors besides blood flow rate that are important for determining the adequacy of hemodialysis include the weight of the patient, recirculation, ultrafiltration variables, duration of hemodialysis, and frequency of hemodialysis [18].
As the blood flow decreases, the delivered dialysis dose (measured as kt/v) decreases, and leads to reduced quality of life and increased morbidity and mortality risk. The reduced blood flow also increases the thrombosis, which in turn leads to infection. Heparin is used as a catheter locking solution to prevent thrombosis and hence infection. The TCC has 2–5 fold higher risk of infection compared to AVF or graft. Catheter related infections include exit site infection, tunnel infection and bacteremia. The TCC has 15 fold higher risk of catheter related blood stream infection (CRBSI) and all-cause mortality rate of 12–25%. Bacterial biofilm is a key reason for the contamination of medical devices like TCC and the generation of microbial and chronic infections in the body. The critical adherence of the organisms to the catheter surface initiates the common pathway of biofilm formation which has microorganisms protected by exopolysaccharide matrix. The organisms include Staphylococcus, Pseudomonas, and Candida among others. An aseptic handling provided, the citrate 4% might be the best catheter lock solution [19]. If the local risk of CRBSI is high the taurolidine + citrate + heparin lock should be used [20]. When malfunction prevails the alteplase/ urokinase block combined with citrate + taurolidine will have advantages [21]. In centers where both complications must be addressed the taurolidine + urokinase + heparin lock could be preferred [22]. The taurolidine-citrate-heparin lock solution effectively eradicated pathogens from nontunneled and tunneled catheter biofilms and helped to maintain catheter lumen sterility [23]. 60% Ethanol alone or 30% ethanol with 4% citrate and ethylene EDTA have also been tried as lock solutions.
In healthcare organizations providing dialysis services, where the case mix includes a lower proportion of patients using catheter-based dialysis, those patients may experience higher rates of catheter-associated infections [24]. Infection control measures may be stronger in organizations dealing with higher proportions of this patient group.
Another way to reduce infection is to use Curos® caps containing 70% isopropyl alcohol, which is to be attached to Tego® hemodialysis connector. ClearGuard HD antimicrobial barrier caps have a rod which is coated with dry chlorhexidine, as are the threads of the cap, and have been found to reduce CRBSI. Tego-Curos caps used with The Arrow-Clark™
The catheter exit site should be covered by a dressing which should be routinely changed, and patient instructed to maintain hygiene and integrity of the dressing and not to soil it.
Catheter tip can get migrated after several months of TCC working (Figure 13). TCC can develop a crack in the ‘Y’ limb of external part of catheter or in the sub-cutaneous tunnel, between the cuff and the exit site or at the ‘Y’ end of TCC and the ‘silver ion sleeve’ of the TCC. The cuff can get extruded or the skin over the tunnel can get eroded (Figure 14). It can develop CRS and / or CRAT to cause catheter malfunction. The CRS should always be suspected whenever TCC malfunctions, especially with inability to aspirate but easy to inject. There may be a thrombus at the tip responsible for TCC malfunction. CRAT may or may not cause TCC malfunction, but it’s a risk for pulmonary embolism. The CRAT could be infected which can cause septic emboli to lungs. The CRAT can be tackled as per the algorithm [Abstract at Annual conference of American Society of Diagnostic and Interventional Nephrology, 2018, and published in Journal of Vascular Access, doi:10.1177/1129729818780571]. The CRS can be tackled with balloon disruption or snared out (Figure 15).

Figure 13.
Catheter tip migration after several months of functioning TCC.

Figure 14.
Cracks in the TCC a) at the junction of silver ion sleeve with TCC b) on the TCC within the subcutaneous tunnel, cuff extrusion and erosion of skin over the tunnel.
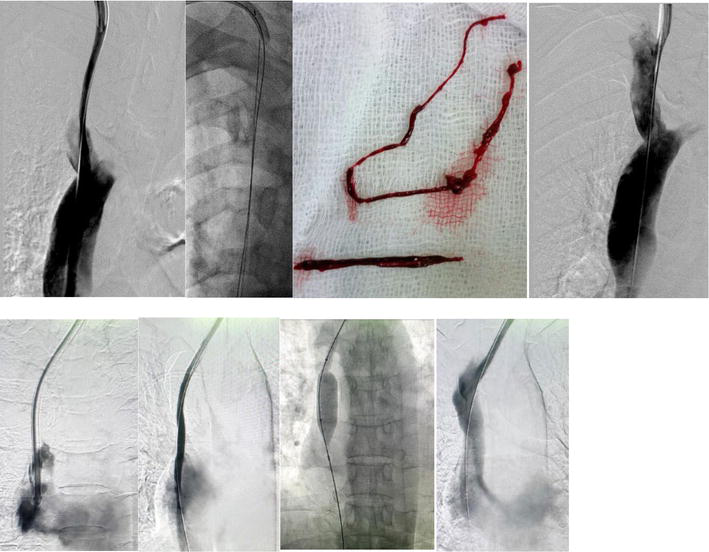
Figure 15.
CRS (fibrin sheath), snared out or balloon disrupted.
3.5 TCC salvage
TCC can malfunction at any time after being in regular use. The situations to salvage the TCC arises when it malfunctions due to CRS, CRAT, combination of CRS and CRAT and SVC stenosis around the TCC tip in SVC (Figure 16), or clot at the tip (Figure 17), when the presentation is with poor flow. Infected TCC causes fever, or rigors during HD but no fever on non-HD days.
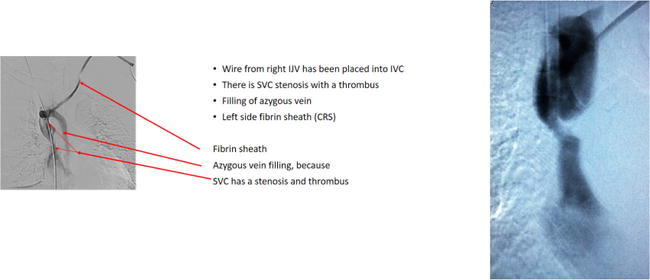
Figure 16.
The reason for left IJV TCC malfunction; stenosis at SVC-RA junction.

Figure 17.
Clots at tip of TCC.
An infected TCC causing CRBSI sometimes needs to be removed but can also be exchanged over a guide wire, and has been found to be safe [25]. This is necessary when the existing TCC is the only dedicated vascular access and there is no other alternative option available for the continuation of HD. Antibiotics locks have been shown to be effective adjunctive therapy to systemic antibiotics in the treatment of CRBSIs [26]. Antibiotic locks should be used when immediate catheter removal is not possible and when catheter needs to be salvaged.
A meta-analysis of hemodialysis patients with TCC, with CRBSI, compared 3 treatment protocols for CRBSIs: (1) systemic antibiotics alone, (2) systemic antibiotics plus antibiotic lock (catheter not removed), and (3) systemic antibiotics plus guide wire exchange. It included 28 retrospective and prospective studies, with a total of 1596 patients. Patients treated with systemic antibiotics and antibiotic lock had similar cure rates to those treated with systemic antibiotics and guide wire exchange, and both were superior to the rates obtained when antibiotics were used alone. Recurrence of infection with the same organism was not different between the systemic antibiotics plus antibiotic lock group and the systemic antibiotics plus guide wire exchange but was much higher in patients treated with systemic antibiotics alone, which further supports the practice to use an antibiotic lock or guide wire exchange in conjunction with systemic antibiotics [27]. Prompt catheter removal with delayed placement of a new TCC is a good option provided it is also viable with alternative venous site availability. All CRBSIs require a minimum 2 to 3 weeks’ systemic antibiotic therapy. However,
CRAT either alone or with CRS is another cause when TCC salvage is necessary. The CRAT, if minor and causing TCC dysfunction can be resolved by removal of catheter itself. A bigger clot of >0.5 cm or a CRAT attached to the TCC tip by a thin peduncle hanging in the right atrium carries the risk of detachment and embolization if TCC is attempted to be pulled back. In such cases, thrombolysis with alteplase after negative blood cultures have been attempted with success (Figure 18). Alteplase is given at 0.1 mg/kg/hour for 6 hours in each lumen and may have to be repeated at incremental dose at 0.15, 0.20 and up to .025 mg/kg/hour for 6 hours (18 cases, personal experience). Chronic CRAT with functioning TCC can be treated with oral anticoagulants for 6 months if it works. Large CRAT (>6 cm) needs either surgical removal or using Angiovac® device (Angiodynamics) which is an alternative method to manage intra-atrial or intravenous thrombi. Patients with hypercoagulable states and unsuitable for any intervention needs lifelong anticoagulation if the patient continues to receive HD through TCC. The TCC malfunction due to stenosis around catheter tip, usually at SVC-RA junction or in the SVC is tackled with TCC removal, venous angioplasty and new TCC insertion with tip placement in the RA. The venous stenosis can also occur when there is presence of lead (cardiac rhythm device) and TCC in the same vein (Figure 19).

Figure 18.
CRAT, thrombolysed with alteplase.
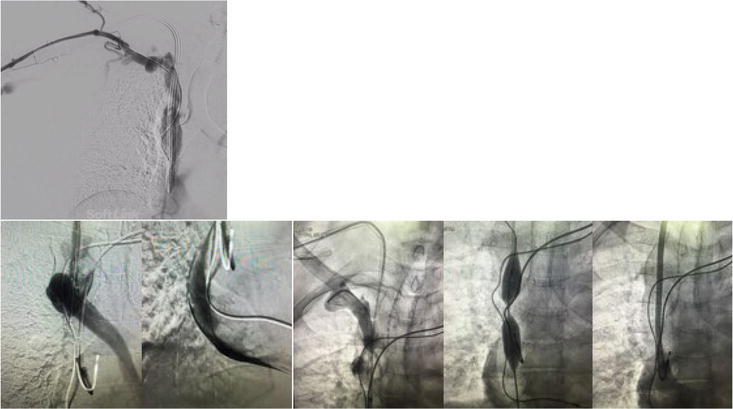
Figure 19.
SVC stenosis with pace-maker leads the azygos vein usually originates from the posterior aspect of the inferior vena cava, at the level of the renal veins. It ascends within the posterior mediastinum to the level of T4 before it arches above the right pulmonary hilum. It drains into the superior vena cava just before it pierces the pericardium, which has been illustrated above.
3.6 Complications of TCC removal
TCC is removed when not required to be used or when infected or clotted. The removal is done after cuff dissection. One has to be careful as instances of TCC getting cut inadvertently and lodging in heart or IVC while removing or fracture of the catheter have been known. Author has personal experience of two cases, one in which the broken piece of TCC was retrieved with endovascular device and delivered through femoral vein venotomy, whereas another patient required thoracotomy for removal of fractured end of TCC. Also, while removal, one has to be gentle and aware that CRS could be existing and should be pulled out along with catheter pull back. In once such instance where the TCC was removed due to CRBSI at another center before patient presented to us, the 2 D echocardiography showed retained piece of CRS (Figure 20).
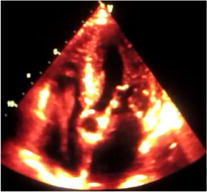
Figure 20.
Retained piece of TCC.
4. Surgical AV fistula
AVF are the preferred mode of dialysis VA due to low long-term rates of infection and stenosis. In 1943, Willem Kolff did successful dialysis, but regular HD through a reliable access was made possible with the advent of the externalized Quinton-Scribner shunt in 1960 introduced by Scribner, Dillard and Quinton, from the University of Washington. First human surgical AVF was created on 19 February 1965, followed by 14 others till 21 June 1966, leading to publication ‘Chronic hemodialysis using venipuncture and a surgically created arteriovenous fistula’, which became widely known as ‘Cimino-Brescia AV fistula’, both of whom were nephrologists, and the surgery was performed by Dr. Apple [5]. Twelve out of these 14 AV fistulae resumed primary function without complications, two never functioned showing an early failure rate which would be admirably low even today [28]. Other types of external devices like winged-in-line shunt of Ramirez, subcutaneous shunt of Buselmeier, femoral shunt of Thomas and Allen Brown shunt for femoral vessels were used for urgent start and chronic HD, however, they all have been abandoned and replaced by TCC.
An AVF is closest to the ideal model of VA, better than grafts and TCC. The most important complications of fistulae for HD are lymphedema, infection, aneurysm, stenosis, congestive heart failure, steal syndrome, ischemic neuropathy and thrombosis. AV fistulae are known to fail, due to juxta anastomotic venous stenosis secondary to venous neointimal hyperplasia. It is important to do surveillance of AV fistula once it is created to gain information about early clinical symptoms of AVF dysfunction, so as to diagnose and adequately treat potential complications early before the access fails.
4.1 Creation
Failure to mature AVF is a huge problem and increases cost and morbidity. A fistula that fails early is one that either never develops adequately to support dialysis or fails within the first 3 months of its use. When dealing with AVF, one would follow rule of 3 for creation of AV fistula (personal data, Prof. Ramesh Tripathi, A/Professor at Faculty of Medicine, School of Biomedical Sciences, University of Queensland, Brisbane City, Australia) which includes anatomical parts (inflow, conduit, outflow), stages of AV fistula development (selection, creation, maturation), types of AV fistula failure (thrombosis, failure to mature, late failure), and AV fistula care providers (nephrologists, vascular surgeons, interventional radiologists). Not to forget the role of dialysis staff who are the back bone of any dialysis unit for perfect care of AVF.
Multiple steps vary for the creation of different types of fistulas. The steps in creating any fistula involve preoperative evaluation of the vasculature, the possible harvest of a vessel for transposition or use of autogenous graft, the creation of an anastomosis, and ligation of branch vessels and wound closure. Artery should be looked at for diameter, wall calcification and anatomical variation. For the vein, look at diameter, pre-existing thrombus or narrowing, distensibility and anatomical variation are necessary.
Risk Equation Determining Unsuccessful Cannulation Events and Failure to Maturation (FTM) in Arteriovenous Fistulas (REDUCE FTM I) was a study which proposed the risk equation to determine the likelihood of AVF failure in individual patients [29]. It gave scores based on age (+2 for >65), white race (−3), peripheral vascular disease (+3), coronary artery disease (+2.5), and base line score of 3 to all patients. So the total score could range from 0 to 10.5. FTM predicted risk categories as per the scores were as follow: Score < 2 is low risk (<25%), score of 2.0–3.0 is moderate risk (35%), score of 3.1–6.9 is high risk (50%), and score > 7% is very high risk (70%). These factors vary from population to population, and have different interpretation and outcome among the non-white population. It is important to investigate local rates of AVF FTM and associated predictors of AVF patency in order to guide appropriate VA decision making. Clinical predictors of AVF FTM may not be sufficient on their own to improve vascular access functional patency rates and it is suggested that the FTM score be revised as per population, and the categories be changed as follow for non-white population: Low to moderate, moderate to high and very high risk categories.
The anastomosis can be completed between artery and vein on one of two techniques. These techniques include side to side anastomosis or artery side to vein end anastomosis. Proximity and diameter of the vasculature are determinants in consideration of either technique used for anastomosis. Dr. Appel in the ‘Cimino-Brescia AV fistula’ did a side-to-side-anastomosis between the radial artery and the cephalic antebrachial vein at the wrist after a 3–5 mm incision had been made in the corresponding lateral surfaces of the artery and the vein. The suturing was using arterial silk in continuous fashion. An end to end anastomosis is no longer used as it requires ligation of distal flow, and has a higher rate of complication. The artery-side-to-vein-end-anastomosis has become a standard procedure. The handling of the artery and the ‘free end’ of the vein should be done with utmost care without pull or stretch as the torsion and kinking of the vessel are common errors that predispose to fistula failure. The mechanical trauma will chronically lead to juxta-anastomotic segment stenosis. There is a risk of kinking if venous segment is excessive and it increases further during maturation of the AV fistula, as the vein will further elongate secondary to the increase in blood flow rate and vascular remodeling.
Various measures are in place to minimize the occurrence of juxta-anastomotic stenosis, which is due to neointimal hyperplasia (NIH). This is to improve hemodynamic flow and reduce areas of low wall shear stress. One such way is to look at the angle of anastomosis between radial artery and cephalic vein of ‘end-to-side’ (end of vein to side of artery) AV fistula and reduce low wall shear stress. Among the four geometries of 30°, 45°, 60° and 90°, the smaller angle (30°) would be the preferred choice that minimizes the development of NIH [30].
The AVF is described as per the type of creation as surgical or percutaneous fistula. The surgical fistulae are described as per its location as wrist fistula (radio-cephalic including snuffbox fistula, radio-basilic, ulno-basilic, proximal radio-cephalic below the elbow, the Gracz elbow fistula with proximal radial artery to deep communicating vein AVF, upper arm AVF (brachio cephalic/brachio basilic) and brachial artery-brachial vein AVF, and lower extremity AVF - superficial femoral artery and the saphenous or femoral/femoral or popliteal vein in the thigh. The brachiobasilic fistula (basilic vein transposition) requires a more extensive surgery to create either as single stage or two stage surgery, involving superficialization as the second stage. Similarly brachio-brachial AVF is also performed as single stage or two stage transposition.
Sometime, there is a high bifurcation of radial artery up in the arm, and elbow AVF is created without knowledge of such situation. What is thought to be brachio-cephalic AVF is actually proximal radio-cephalic AVF (Figure 21).
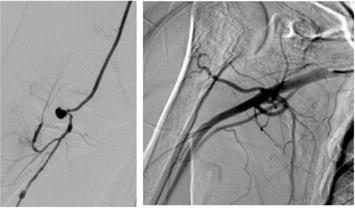
Figure 21.
High radial artery bifurcation, resulting in proximal RC AVF, and not BC AVF.
The percutaneous AV fistula is available as Ellipsys and WavelinQ devices, which use specially designed catheters to join the walls of the artery and vein to create the fistula. These techniques are only beginning to be used on a larger scale. The configuration of Gracz fistula is same as in Ellipsys percutaneous AV fistula. These were compared and the conclusion showed that both Ellipsys percutaneous AVF and Gracz-type surgical AVF demonstrate 100% technical success with similarly high cumulative patency rates [31].
4.2 Maintenance
Once the AV fistula is created, it must mature to a point of being used for HD with repeated needle cannulation. They need clinical monitoring and if indicated, surveillance with a device to see the progress in maturation. The physical examination should include inspection, palpation, auscultation, augmentation test for inflow stenosis and hand raising test to look for outflow stenosis. If not maturing, imaging and early intervention is required to rescue the AV fistula which are failing to mature. For non-maturing fistulae, KDOQI suggests that the use of adjuvant Far-infrared therapy to improve AVF primary patency be based on individual circumstances, feasibility, and the clinician’s best judgment and expertise. Fish oil, aspirin, clopidogrel, prostacycline, simvastatin or ezetimibe are not recommended for maturation.
AVF should also be examined for recirculation, as the most common cause of recirculation is high grade venous stenosis and moderate to severe recirculation can be picked up. To test for recirculation on physical examination, the examiner should occlude the fistula between the two needles during dialysis and observe the venous and arterial pressure gauges. If the needles have been placed too closely together, this examination will not be possible. A hard object such as a closed hemostat occludes the fistula more efficiently than a finger. With a normal fistula, very little or no change is observed in either the venous or arterial pressure readings.
If recirculation is secondary to outflow venous stenosis, the pressure will increase in the venous return because the lower-resistance recirculation route has been occluded. As pressure limits are exceeded, the alarm will sound, and the blood pump will quickly stop. The arterial pressure may become slightly more negative as the pressure head generated by the venous side is no longer transmitted through the occluded site in the fistula.
If recirculation is due to poor inflow (arterial stenosis or insufficiency), the occlusion will cause a decrease in pressure since the blood pump will demand more blood than is available (since the recirculation route will have been occluded). In this instance, the arterial alarm will sound very quickly, but the venous pressure may change very little.
4.2.1 Cannulation
The four cannulation techniques, rope ladder (RL), area puncture (AP), buttonhole with blunt needles (BHb), and buttonhole with sharp needles (BHs), affects the arteriovenous fistula (AVF) in different ways. AP should not be used because it cause complications such as aneurysms and bleeding. Other complications include stenosis, thrombosis, infiltration, cannulation difficulty and infection.
Fistula should be cannulated and decannulated by experienced staff with standard techniques. Difficult cannulation should be attempted with duplex ultrasound guidance. Failed cannulation should be attempted after rest to the part. In between dialysis sessions, patients are instructed to keep the fistula clean and avoid blood pressure measurements, vein puncture, wearing any watch, clothing, jewelry, or other activities that can put pressure to the fistula and restrict the flow, and sometimes, AVF closure.
4.3 Salvage
4.3.1 Nonmaturing AV fistula
Gold standard of salvage is percutaneous trans luminal angioplasty (PTA) or surgical revision. There are stimulatory (promote dilatation and/or wall thickening) and inhibitory (prevents or inhibits NIH) approaches which can either salvage a dysfunctional AV fistula or help prevent future malfunction which would require salvage procedure. The stimulatory approach includes balloon assisted maturation (BAM) of juxta-anastomotic lesion (Figure 22) as we practice, cutting balloon angioplasty, angioplasty with stent (Figure 23), elastase therapy etc. the inhibitory approach includes drug eluting angioplasty, cryoplasty, brachytherapy, adventitial wraps, mechanical support devices (The VasQ® device for improved outward and inward remodeling) and gene therapy.
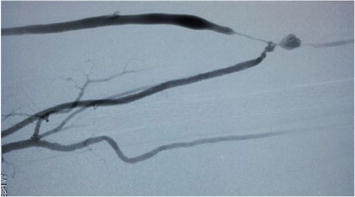
Figure 22.
Balloon assisted maturation angioplasty (v/s new AVF proximal to the juxta-anastomotic venous stenosis?).
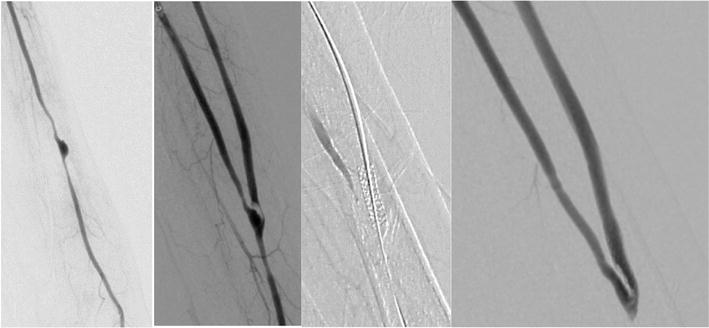
Figure 23.
Acute thrombosis in AVF treated with stent.
4.3.2 Bam
in the true sense is a more aggressive approach to AVF maturation failure in which repeated long segment angioplasty procedures are used to sequentially dilate up the peri-anastomotic venous segment, converting it at times into a “collagen tube”. Although arterial angioplasty is generally angioplasty of the lumen, intima, and media, when the venous angioplasty is performed for the purpose of fistula maturation, it involves rupture of the entire vessel wall with a reliance on subcutaneous tissue to contain fistula flow and pressure.
4.3.3 High risk AV fistula: Thrombosis
Factors which can cause fistula dysfunction and thrombosis include pre-existing stenotic lesion/s, cannulation injury due to same site puncture or more frequent cannulations (daily HD), infiltration, hematoma and pseudoaneurysm. The AVF can thrombose overnight or gradually. The sudden thrombosis is sometimes associated with high hematocrit values (over dose of erythropoiesis stimulating agent). Gradual thrombosis will have prior sessions of poor flows, high venous pressure or prolonged bleeding after needle removal at the end of dialysis. AVF thrombosis is treated with infusion of a thrombolytic such as tissue plasminogen activator, tPA in conjunction with using a lacerating device or a balloon catheter to remove the clot. Following mechanical or pharmacologic thrombolysis, an angioplasty is done to correct any underlying stenosis.
4.3.4 Venous stenotic lesions
These can occur along the venous outflow segment. Commonest lesions are juxta-anastomotic, but it could be elsewhere also. The cephalic arch stenosis occurs most commonly with BC AVF, rarely with RC AVF (Figure 24).

Figure 24.
Cephalic arch stenosis.
Thrombosis without identified stenotic lesion are tackled either with catheter directed thrombolysis with tPA, thrombosuction or mechanical thrombectomy (Figures 25 and 26).

Figure 25.
Catheter directed thrombolytic therapy required.
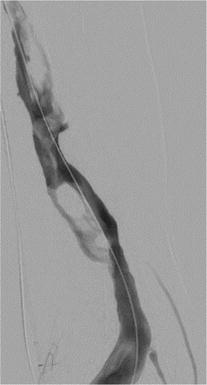
Figure 26.
Chronic thrombus, mechanical thrombectomy with Angio-jet® required.
4.3.5 AV fistula with aneurysm
It is a common but difficult to treat complication of AVF and is defined by an expansion of the intimal, medial and adventitial layers of the vessel wall to a diameter of more than 18 mm. and classify it on the basis of true aneurysm or false (pseudo) aneurysm, location (arterial/venous/graft) and site (anastomotic/puncture site/native vessel and whole outflow vein). Patient can be observed if asymptomatic and AVF is working well, or treat if there is pain, risk of bleeding and flow issues (either low or high flow). If infected or risk of rupture, it can be surgically repaired. Infected but no immediate risk of rupture aneurysm can be treated with covered graft as shown in our case (Figure 27).

Figure 27.
AVF aneurysm with functioning fistula, treated with covered stent, after treating blood cultures positive for
4.3.6 Infected fistula
Superficial infection is generally around a cannulation site. Deep infections cause swelling, redness, tenderness, and pus formation. Deep infection can cause venous thrombosis, leading to life threatening pulmonary thromboembolism [personal experience].
4.3.7 Extremity ischemia
Two clinical variants are recognized, both with characteristic findings on physical examination. Dialysis access related ischemic steal syndrome (DASS) has four stages of presentation. Stage I: Pale/blue/cool hand without pain and no or slight cyanosis of nail beds, mild coldness of skin or hand, reduced arterial pulsations at the wrist, reduced systolic finger pressures. Stage II: Pain during hand exercise and/or with dialysis or pain, cramps, numbness or disturbing coldness in fingers or hand. Stage III: Pain at rest or motor dysfunction of fingers or hand. Stage IV: Tissue loss, including ulcers, necrosis or gangrene. It is also known as distal hand hypoperfusion ischemia syndrome (DHHIS).
Second variety is called Ischemic monomelic neuropathy (IMN), it presents with severe pain, numbness, diffuse motor weakness, usually in the absence of significant ischemic changes in the tissues of the hand and fingers.
4.3.8 High flow fistula
Though the ideal flow through AVF should be about 600–800 ml/minute, sometimes, it can become high flow fistula with blood flow in the range of 3–4 liters/minute. It can be repaired surgically or endovascularly with MILLER’s (Minimally Invasive Limited Ligation Endoluminal-assisted Revision) banding procedure (Figure 28). MILLER’s banding is also used to treat DASS.
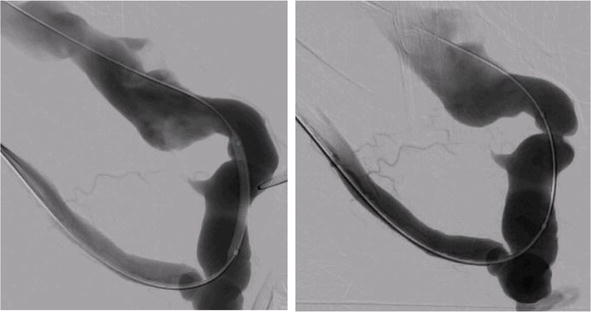
Figure 28.
MILLER’s banding: Flow volume reduced from 4 liters/minute to 800 ml/minute.
5. AV graft
AVG are divided as biological grafts (xenografts) (bovine mesenteric vein, bovine carotid artery, bovine ureter), or synthetic grafts (Dacron, PTFE, ePTFE, polyurethane and polyether urethane urea). PTFE grafts are the most common type of graft and are considered to be the graft of choice for HD access around the world. Allografts with cryopreserved femoral vein and human mesenchymal cell engineered graft (when available) are other options. Variations among PTFE grafts are available. Use of saphenous vein translocation to the upper limb (autograft) for creation of AVF is an option.
The primary failure rate for grafts is less than that for fistulas but the risk of infection (up to 4 times higher risk than AVF) and clotting is higher. Also, given the increased number of interventions required for graft maintenance, the primary patency rate for grafts is less than that for fistulas.
5.1 Creation
The ePTFE grafts can be cannulated after 2 weeks following placement, but new generation grafts with early cannulation properties are available, allowing use as an alternative to central venous catheters for prompt access.
AVG are described as per anatomic location. Inflow artery, outflow vein, graft material, and graft configuration are considered for AVG along with location as looped forearm (brachial artery to cephalic vein), straight forearm (radial artery to cephalic vein), looped upper arm (axillary artery to axillary vein), and straight upper arm (brachial artery to axillary vein). Lower extremity grafts, looped chest grafts, axillary-axillary (necklace) grafts, and axillary-atrial grafts have also been constructed but are uncommon [32]. Like in AVF, graft to vessel angle of 30° has been found optimal.
Complications related to AVG creation can be either local problems e.g. bleeding, seroma, infection, pseudoaneurysm, and neuropathy; or access flow-related problems like swelling of graft arm, cardiopulmonary problems, DASS, IMN; or due to AVG dysfunction and failure due to thrombosis and / or infection. Thrombosis can occur in AVG, immediately after creation (technical issues) or later due to stenosis. Local antiproliferative drugs like sirolimus eluting stents or paclitaxel wrap are being studied for stenosis prevention.
5.1.1 Hemodialysis reliable outflow (HeRO) grafts
It consists of two parts, 6 mm ePTFE portion and nitinol-reinforced silicone single-lumen outflow catheter, meant to provide outflow to patients with central venous stenosis. It is fully subcutaneous VA. However, it is considered as last resort for VA. The ePTFE portion is anastomosed to brachial or other inflow artery and the central tip is positioned in the middle of right atrium. HeRO graft could be an acceptable option for complex dialysis patients who are catheter dependent.
5.2 Maintenance
Physical examination can assist in the early detection of thrombosis and stenosis in AVGs. Proper graft maintenance and graft cannulation technique are important for preventing complications. Self-examination for a thrill over AVG should be taught to the patients. Preventing thrombosis with prophylactic antithrombotic medications (antiplatelet or anticoagulation) have not been found to be useful. Warfarin may be used in presence of hypercoagulable state with strict monitoring for bleeding complications.
5.3 Salvage
Besides thrombosis, other causes of AVG failure include primary or recurrent stenosis after angioplasty, cannulation injury, infiltration, hematoma, thrombosis of pseudo aneurysm, hypercoagulable states and presence of stent. Thrombosis is tackled with percutaneous thrombolysis or thrombectomy, mechanical or surgical. Stenosis usually occurs at vein-graft anastomosis site (Figure 29), but could occur along the draining vein or even the central vein. Stenosis could also be in the inflow or intra-graft. Salvage is attempted with balloon angioplasty. Stenting may be required for graft-vein anastomotic junction stenosis or for the traumatic aneurysm in the AVG (Figure 30). Recurrent stenosis may need surgical (alone or combined with endovascular) revision of AVG, though drug eluting balloon using paclitaxel have been used to prevent restenosis.
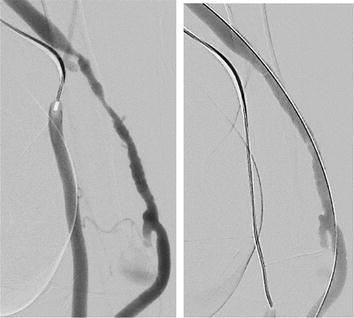
Figure 29.
AVG stenosis at venous end anastomosis with the vein. Before and after angioplasty.

Figure 30.
Traumatic aneurysm in AV graft, covered stent deployed.
6. Conclusion
The profile of kidney failure has changed over last 6 decades, with advances in the VA. Starting from Scribner’s shunt to endovascular AVF has changed the epidemiology of ESKD. However, none of these are failure proof, and involves cost for its maintenance and salvage. These modalities should be cost effective, and should result in improved patient outcome. Also, these should be widely available. Better understanding of VA pathophysiology, and involvement of VA as a curriculum in the basic nephrology training may lead to more nephrologists getting interested in the VA care and result in better delivery of dialysis, so as to achieve maximum rehabilitation of the patients (social and economic) and provide high quality patient centered care. VA is an exciting field and more nephrologist should join it and work as a team with vascular surgeons and interventional radiologists.
Acknowledgments
The author acknowledges the support of COO, department of interventional radiology, cardiac catheterization lab, and its staff at Lilavati hospital and Research center. Special thanks go to Dr. Gireesh Warawadekar, interventional radiologist and past president of the Indian Society of Interventional Radiology, and Dr. Nikhil Karnik, interventional radiologist. Special thanks to my friends and guidance (whenever required) from ASDIN (Dr. Tushar Vachharajani, Dr. Anil Agrawal, Dr. Bharat Sachdeva, De Vandana Niyyar Dua, Dr. Arif Asif, Dr. Lalataksha Kumbhar etc), all the fellows, clinical associates, and junior consultants in the department of nephrology, Lilavati Hospital, for patient care.
Conflict of interest
The author declares no conflict of interest related to this presentation.
References
- 1.
Bartolomeo K, Vachharajani TJ, Shingarev R. The Sisyphean task of getting the arteriovenous fistula to mature. Kidney360. 2021; 2 (12):1873-1875 - 2.
Kolff WJ. First clinical experience with the artificial kidney. Annals of Internal Medicine. 1965; 62 :608-619 - 3.
Lok CE, Huber TS, Lee T, Shenoy S, Yevzlin AS, Abreo K, et al. KDOQI Clinical Practice Guideline for Vascular Access: 2019 Update. American Journal of Kidney Diseases. 2020; 75 (4):S1-S164 - 4.
Moran JE, Prosl F. Totally implantable subcutaneous devices for hemodialysis access. Contributions to Nephrology. 2004; 142 :178-192 - 5.
Brescia MJ, Cimino JE, Appel K, Hurwich BJ. Chronic Hemodialysis using Venipuncture and a surgically created arteriovenous fistula. The New England Journal of Medicine. 1966; 275 :1089-1092 - 6.
Baker LD, Johnson JM, Goldfarb D. Expanded polytetrafluoroethylene(PTFE) subcutaneous arteriovenous conduit: An ImprovedVascular Accessfor chronic Hemodialysis. Transactions of the American Society for Artificial Internal Organs. 1976; 22 :382 - 7.
He J, Fen Q, Lang F, Yang M, Liu Z, Liang R, et al. Early cannulation arteriovenous graft (Acuseal) versus standard arteriovenous graft in patients with end-stage renal disease. Hemodialysis International. 2021; 25 (4):465-472 - 8.
Mehta H. An insight into the sites of non-cuffed hemodialysis catheters. Indian Journal of Nephrology. 2015; 25 (5):261-262 - 9.
Oliver MJ, Callery SM, Thorpe KE, Schwab SJ, Churchill DN. Risk of bacteremia from temporary hemodialysis catheters by site of insertion and duration of use: A prospective study. Kidney International. 2000; 58 (6):2543-2545 - 10.
Lacson E Jr, Lazarus JM, Himmelfarb J, Ikizler TA, Hakim RM. Balancing fistula first with catheters last. American Journal of Kidney Diseases. 2007; 50 (3):379-395 - 11.
System USRD. USRDS Annual Data Report: Epidemiology of Kidney Disease in the United States. 2021. Available from: https://www.usrds.org/annual-data-report/ - 12.
Schwab SJ, Beathard G. The hemodialysis catheter conundrum: Hate living with them, but can’t live without them. Kidney International. 1999; 56 (1):1-17 - 13.
Johansen KL, Gilbertson DT, Wetmore JB, Peng Y, Liu J, Eric D. Weinhandl ED. Catheter-associated bloodstream infections among patients on Hemodialysis: Progress before and during the COVID-19 pandemic. Clinical Journal of the American Society of Nephrology. 2022; 17 (3):429-433. CJN.11360821; DOI: 10.2215/CJN.11360821. - 14.
Sohail MA, Hanane T, Lane J, Vachharajani TJ. Safety of bedside placement of Tunneled Hemodialysis catheters in the intensive care unit: Translating from the COVID-19 experience. Journal of Clinical Medicine. 2021; 10 (24):5766. DOI: 10.3390/jcm10245766 - 15.
Williams AD, Qaqish M, Elnagar J, Michos L, Nantermet S, Meisner R, et al. Bedside Tunneled Hemodialysis catheter placement in patients with COVID-19. Annals of Vascular Surgery. 2021; 73 :133-138 - 16.
Swami R, Jadhav S, Mehta KS, Pilgulwar G, Jawale S, Pajai A. Tunnelled cuffed catheters for Hemodialysis, placed by nephrologists: Success rate, Efficacy & Complications. International Journal of Medical Research Professionals. 2018; 4 (6):65-70 - 17.
Vesely TM. The Challenges of hemodialysis catheter use. thrill seekers, bold explorations in dialysis. Endovascular Today; Eur. June. 2013:61-63 Available from: https://evtoday.com/articles/2013-june/the-challenges-of-hemodialysis-catheter-use - 18.
Beathard GA. Malfunction of Chronic Hemodialysis Catheters. Uptodate, June 2021. Available from: https://www.uptodate.com/contents/malfunction-of-chronic-hemodialysis-catheters - 19.
Wurster M, Keller F, FP558. What is the best dialysis catheter lock solution - a systematic analysis of published studies. Nephrology, Dialysis, Transplantation. 2018; 33 (S-1):i228. DOI: 10.1093/ndt/gfy104.FP558 - 20.
Reidenberg B, Wanner C, Polsky B, Castanheira M, Shelip A, Stalleicken D, et al. Postmarketing experience with Neutrolin® (taurolidine, heparin, calcium citrate) catheter lock solution in hemodialysis patients. European Journal of Clinical Microbiology & Infectious Diseases. 2018; 37 :661-663 - 21.
Ali FA, Hamdy AF, Hamad A, Elsayed M, Iqbal ZZ, Elsayed A, et al. Safety and efficacy of taurolidine/urokinase versus taurolidine/heparin as a tunneled catheter lock solution in hemodialysis patients: A prospective, randomized, controlled study. Nephrology, Dialysis, Transplantation. 2018; 33 (4):619-626 - 22.
Wolfgang W, Harald H, Matthias L, Handisurya AH, Željko K, Bernhard B, et al. Taurolidine-based catheter lock regimen significantly reduces overall costs, infection, and dysfunction rates of tunneled hemodialysis catheters. Kidney International. 2018; 93 (3):753-760 - 23.
Zwiech R, Adelt M, Chrul S. A Taurolidine-citrate-heparin lock solution effectively eradicates pathogens from the catheter biofilm in Hemodialysis patients. American Journal of Therapeutics. 2016; 23 (2):e363-e368 - 24.
Brown RS, Brickel K, Davis RB. Two-year observational study of bloodstream infection rates in Hemodialysis facility patients with and without catheters. Clinical Journal of the American Society of Nephrology. 2018; 13 (9):1381-1388 - 25.
Saleh HM, Mohamed MT, Hesham A. Prospective, randomized study of long-term hemodialysis catheter removal versus guide wire exchange to treat catheter-related bloodstream infection. Journal of Vascular Surgery. 2017; 66 (5)7:1427-1431 - 26.
Aslam S, Vaida F, Ritter M, Mehta RL. Systematic review and meta-analysis on management of hemodialysis catheter-related bacteremia. Journal of the American Society of Nephrology. 2014; 25 (12):2927-2941 - 27.
Miller LM, Clark E, Dipchand C, Hiremath S, Kappel J, Kiaii M, et al. Hemodialysis Tunneled catheter-related infections. Canadian Journal of Kidney Health and Disease. 2016; 3 :2054358116669129. DOI: 10.1177/2054358116669129 - 28.
Konner K. History of vascular access for haemodialysis. Nephrology, Dialysis, Transplantation. 2005; 20 (12):2629-2635 - 29.
Lok CE, Michael Moist AL, Oliver MJ, Shah H, Zimmerman D. Risk equation determining unsuccessful cannulation events and failure to maturation in arteriovenous fistulas (REDUCE FTM I). Journal of the American Society of Nephrology. 2006; 17 (11):3204-3212 - 30.
Konner K, Lomonte C, Basile C. Placing a primary arteriovenous fistula that works—More or less known aspects, new ideas. Nephrology, Dialysis, Transplantation. 2013; 28 (4):781-784 - 31.
Shahverdyan R, Beathard G, Mushtaq N, Litchfield TF, Vartanian S, Konner K, et al. Comparison of Ellipsys percutaneous and proximal forearm Gracz-type surgical arteriovenous fistulas. American Journal of Kidney Diseases. 2021; 78 (4):520-529 - 32.
Woo K. Arteriovenous Graft Creation for Hemodialysis and Its Complications. Available from: https://www.uptodate.com/contents/arteriovenous-graft-creation-for-hemodialysis-and-its-complications