 Open access peer-reviewed chapter
Open access peer-reviewed chapter
Abstract
Polyethylene glycol is a product with many pharmaceutical and industrial uses due to its hydrophilic nature. As a medication, it is part of a laxative class of drugs which is minimally absorbed in gastrointestinal tract increasing osmotic pressure resulting in softening of stools and increased bowel movements. There are certain FDA and non FDA-approved indications for its use. Its main use is for the treatment of constipation, fecal impaction, chronic constipation, and colonoscopy preparation. Its administration is elaborated according to different age groups and indications. Polyethylene glycol is over-the-counter medication as there is easy access to this drug, but as a health care provider, we need to emphasize the directions for its appropriate use with proper counseling regarding the onset of action as well as when to discontinue it which will yield improved patient results while minimizing adverse events.
Keywords
- polyethylene glycol (PEG)
- constipation
- colonoscopy preparation
- laxative
- awareness for its use
1. Introduction
Polyethylene glycol is a polyether compound mainly derived from petroleum. They are synthesized by polymerization of polyethylene oxide. These are available over a wide range of products with many applications including biomedical, pharmaceutical, industrial, chemical, commercial, and entertainment industry. Due to its hydrophilic nature, it is mainly utilized in cosmetic products, surfactants, emulsifiers, humectants, skin conditioners [1], and cleansing agents. It is used as an anti-foaming agent in foods and drinks [2]. It is used as an excipient in many pharmaceutical preparations in oral, parenteral, and topical forms [3]. The use of PEG hydrogels has been theorized by Ma et al. They proposed its use to address periodontitis (gum disease) by encapsulating stem cells in the gel which promotes healing in the gum [4]. PEGylated lipid is used as an excipient in both Pfizer and Moderna vaccines for SARS-CoV-2. Both vaccines contain mRNA encased in a bubble of molecules that is made up of polyethylene glycol. As of Dec 2020, there was a concern about polyethylene glycol causing hypersensitivity/allergic reactions [5], and also reported that two individuals recovered from anaphylactic shock [6, 7]. In Dec, US CDC stated in their jurisdiction that six cases of allergic reactions were recorded from over 250,000 vaccinations, and of those six, only one person had history of vaccination reaction [8].
The production of Polyethylene glycol was first reported in 1859. Both A. V. Lourenco and Charles Adolphe Wurtz independently isolated these products [9]. Polyethylene glycol is produced by the interaction of ethylene oxide with water, ethylene glycol oligomers, or ethylene glycol. The reaction is catalyzed by acidic or basic catalysts. Polyethylene glycol is a hydrophilic (water-loving) polymer that is made by reacting ethylene oxide with ethylene glycol (the simplest member of glycol family) or with ethylene glycol oligomers (molecules that contain repeating units) or water.
As a medication, it belongs to laxative class of drugs. It works by causing water to be retained in stool resulting in softening of stool as well as increasing the number of bowel movements.
It is used in the management and treatment of chronic constipation and fecal impaction with polyethylene glycol powder being mixed with liquid and then taken by mouth, As an osmotic laxative, the compound works by forming hydrogen bonds with water molecules which prevents the re-absorption of water in the gastrointestinal tract, causing water retention in the stool and increasing osmotic pressure. Water retention softens the stool making it easier to pass; the number of bowel movements also increases. Potential side effects include nausea, bloating, and intestinal cramping; more serious effects include diarrhea and in sensitive individuals, hives. It is also used for colonoscopy preparation as a way to cleanse the bowel to help provide a clear image. It is typically mixed with two liters of sports drink, the day before the procedure.
This chapter includes polyethylene glycol used in chronic constipation and for colonoscopy preparation, its potential side effects, contraindications, method of administration, and when and how to discontinue it in case of chronic constipation. It is over-the-counter medication. There is an easy access to this drug. The objective is to spread awareness among the patients and healthcare teams which will yield improved patient results while minimizing adverse effects that are still possible with over-the-counter medication (like PEG).
2. Indications
2.1 FDA-approved indications
Treatment of constipation in patients 17 years or older.
It is preferred over other agents due to its limited side effects and better testing profile.
Polyethylene glycol laxative is safer than Polyethylene glycol electrolyte lavage Solution as there is no salt absorption.
2.2 Non-FDA approved indications
Colonoscopy preparation
Fecal impaction
Chronic constipation
Constipation in pediatric patients
2.3 Mechanism of action
Polyethylene glycol is hydrophilic, and minimally absorbed in the gastrointestinal tract as a medication. It forms hydrogen bonds with water molecules. For this reason, it can prevent the re-absorption of water which causes water retention in stool and increases the osmotic pressure. As a result, stool softens and bowel movements occur more frequently [10, 11].
3. Administration
Polyethylene glycol-3350 comes as a powder to be mixed with liquid and taken by mouth.
It is usually taken once a day as needed for up to 2 weeks.
To use powder, follow these steps [11];
If using polyethylene glycol from the bottle, use the measuring line on the bottle cap to measure a single dose (about one a heaping tablespoon).
If using a polyethylene glycol packet, each packet contains a single dose.
Pour the powder into the cup containing 08 ounces (about 240 ml) of water, juice, soda, coffee, or tea.
Stir to dissolve the powder.
Drink immediately
It may be habit-forming. Do not take a larger dose, take it more often or take it for a longer period of time.
It may take two to 4 days for polyethylene glycol-3350 to produce a bowel movement.
In the adult population, polyethylene glycol should not be used for more than 2 weeks as an over-the-counter medication unless instructed by a physician. If needed more chronically, it can be taken for up to 6 months [12].
It is also used for the preparation of colonoscopy. Polyethylene glycol is used to cleanse the bowel to help in providing a clear image of the mucosa.
It is administered by mixing 238 g in 2 liters of sports drinks on the day before the procedure. Guidelines also recommend doing split dose when colonoscopy is in the afternoon, administer one liter on the day before the procedure and one liter on the day of procedure.
4. Dietary instructions
To treat constipation, along with using polyethylene glycol as a laxative, eat a well-balanced diet that includes fiber-rich foods such as unprocessed bran, whole grains, bread, fresh fruits, and vegetables.
Drink plenty of fluid.
Exercise regularly
5. Special patiena: Population
Pregnancy
It is a pregnancy category C drug.
The systemic absorption of polyethylene glycol is believed to be minimal, therefore it is less likely to cause any severe effect on neonate.
Breast feeding women
No specific recommendation, as it has poor systemic absorption [13], so there should be minimal to no excretion in the breast milk.
Pediatrics
For children more than 2 years of age, it can be used for chronic constipation and fecal impaction on a weight-based dosage adjustment.
For fecal impaction; 1–1.5 g/kg/day for 3–6 days with a maximum of 6 consecutive days.
For Chronic constipation; initial dose. 0.4 g/kg/day orally
Maintenance dose; 0.2–0.8 g/kg/day adjusted to response
The recommendation is to continue for at least 2 months and discontinue gradually once symptoms resolve for at least months [14].
Patients with hepatic impairment; No dose adjustment is required.
Patients with renal impairment; No dose adjustment required.
Geriatric patients; No dose adjustment is required.
6. Adverse effects
In adults
Flatulence/Diarrhea
Nausea
Stomach cramps
After using polyethylene glycol Electrolyte Lavage Solution following topical administration---Urticaria [12, 17]
Acidosis reported in literature and case reports with intravenous administration of drugs utilizing polyethylene glycol as a vehicle and repeated topical dermal exposure of polyethylene glycol in burn patients [18, 19].
Proximal renal tubular necrosis with oliguria, azotemia, and renal failure following intravenous administration of polyethylene glycol and topical application in burn patients [20].
In children
Seizures
Tremor
Obsessive-compulsive behaviors (including repetitive chewing and sucking)
Paranoia/mood swings
Headache
Sedation/lethargy
Aggression/anxiety
7. Contraindications
Patient with known or suspected bowel obstruction, appendicitis, inflammatory bowel disease, perforated bowel, and hypersensitivity to polyethylene glycol or any component of formulation.
Precautionary measures are necessary for patients with electrolyte imbalances and patients with renal impairment [21].
8. Monitoring
Before initiating, rule out symptoms and signs of bowel obstruction.
Patient education regarding proper use of PEG and monitoring for therapeutic efficacy including decreased abdominal discomfort, pain, and bowel movement in two to 4 days.
Electrolyte imbalances should be monitored periodically with prolonged, frequent, or excessive use [21].
Pediatric patients on long-term use of polyethylene glycol should also be monitored for neuropsychiatric symptoms.
Patients should discontinue use of polyethylene glycol if they experience loose stools.
Clinicians should taper down patients on chronic therapy.
9. Toxicity/overdose
Due to limited exposure, toxicity to polyethylene glycol is very rare.
Diarrhea leading to dehydration especially if water intake is minimal, can result in confusion and potentially seizures [22].
Renal injury and metabolic acidosis.
There is no antidote in case of polyethylene glycol overdose
10. Polyethylene glycol use in colonoscopy preparation
A colonoscopy is the principal diagnostic tool to inspect mucosa of the colon for any pathology such as inflammation, polyp, adenoma, or cancer. It is preferred over other imaging modalities like barium enema or computed tomography (CT) colonography in many situations because of its capacity to intervene and sample or remove pathology encountered.
The pre-requisite for optimal endoscopic visualization is adequate bowel cleansing as it affects safety, quality, efficacy, and diagnostic accuracy of the procedure. The colonoscopic detection rate of lesions is affected by bowel preparation quality [23]. Previous studies showed that at the time of colonoscopy, about 20% of patients had inadequate bowel preparation [24]. Inadequate bowel preparation may result in an increased risk of missing lesions, decreased cecal intubation rate, increased patient discomfort due to repeated washings and suctioning, prolonged procedure time, higher risk of complications, increased rate of the canceled procedure with increasing costs and need to repeat the procedure [25]. So ideally the colon cleansing method should be fast, safe, and able to do proper cleaning with minimal side effects and discomfort for the patient [26]. There are different agents used for colonoscopy preparation, including polyethylene glycol, sodium phosphate, pyrosulphate solution, and oral sulfate solution. There are two regimens used for colonoscopy preparation including split dose and day before cleansing method [27]. The agents which are used commonly include sodium phosphate and polyethylene glycol electrolyte solution. PEG and sodium phosphate, both are osmotic laxatives that cause water retention in stools and increase stool frequency. The preference for one preparation over the other is guided by consensus regarding two preparations, relative safety, tolerability, and effectiveness [28]. Preferentially PEG-based preparations are given in patients who have renal insufficiency. It is also preferred in patients who have diabetes mellitus or congestive cardiac failure [29].
10.1 Patient selection
Patient selection for colonoscopy focuses on the indication for the procedure and patient comorbidities to enable proper risk stratification.
The American Society of Gastrointestinal Endoscopy has outlined general principles for the appropriate use of endoscopy [30]. Endoscopy may be pertinent if any of the following criteria are fulfilled:
There is an effective change in the patient’s management after results
There is failure of empiric treatment of a benign disease
There is anticipation of therapeutic intervention
It is used as an alternative to radiologic evaluation
On the other hand, when the results are not expected to change the management plan appropriately or just for the sake of benign disease follow-up that hase healed, there is no need to undergo a colonoscopy, except to do a surveillance colonoscopy for anticipated pre-malignant condition (Figures 1–5).
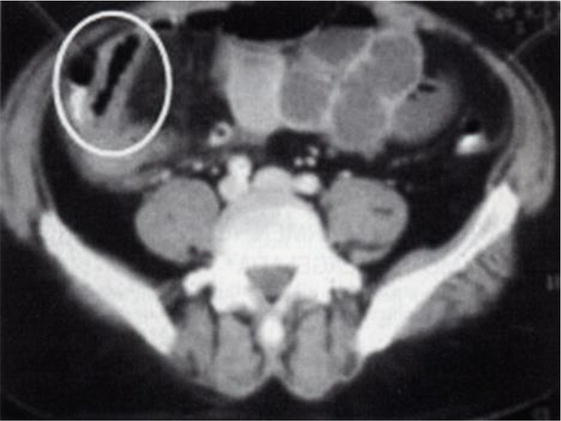
Figure 1.
Abdominal computed tomography scan showing thickening of the distal ileum.
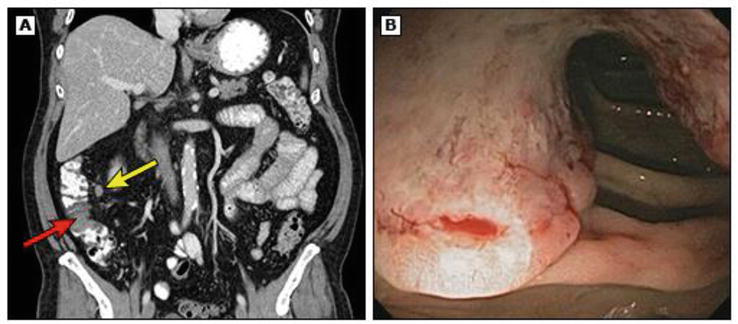
Figure 2.
Colon cancer is seen on CT scan and colonoscopy. (A) Computed tomographic (CT) scan showing a filling defect in the ascending colon (red arrow) along with an involved lymph node (yellow arrow). (B) Colon cancer identified in the ascending colon on subsequent colonoscopy.

Figure 3.
Cancer of the colon as seen on barium enema. Double-contrast barium enema shows an apple-core lesion surrounding the lumen of the descending colon.
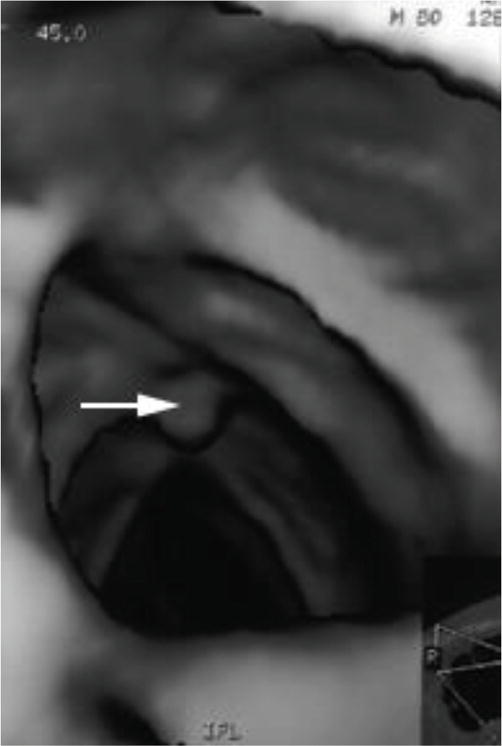
Figure 4.
Colonic polypVirtual colonoscopy shows a small polyp (arrow) in the transverse colon.
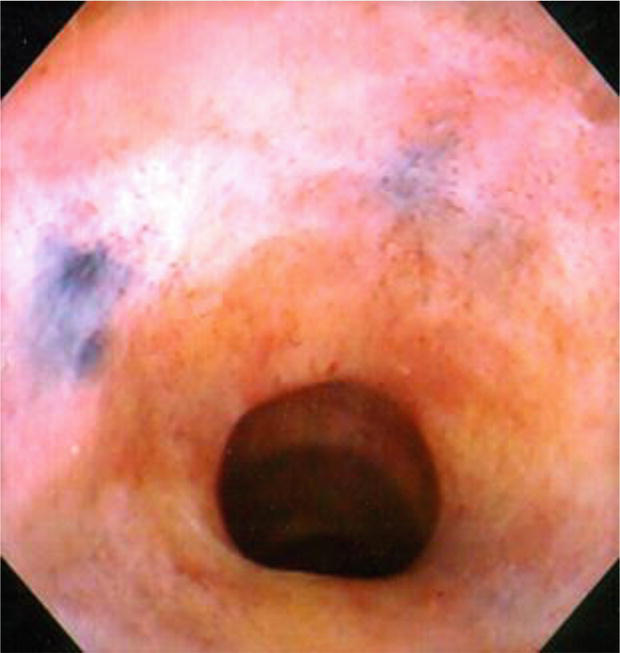
Figure 5.
India ink at polypectomy scar. India ink staining is visible at the site of a polypectomy scar.
10.2 Indications; both diagnostic and therapeutic
Lower GI Bleeding
Screening and surveillance for colon cancer
Lower GI symptoms
Abnormal imaging
Evaluation for metachronous or synchronous cancer in patients with colon cancer
Evaluation of terminal ileum
10.3 Therapeutic
Foreign body removal
Removal of polyp
Decompression of sigmoid volvulus or colonic pseudo-obstruction
Secure hemostasis in lower GI bleed
Palliative treatment of bleeding or stenosed neoplasms
Percutaneous endoscopic cecostomy tube placement
10.4 Contraindications
When the risks of colonoscopy outweigh the expected benefits
Consent cannot be obtained for non-urgent procedure
A perforation is known or expected
Documented acute diverticulitis
Fulminant colitis
10.5 Important considerations
It is important to consider certain factors in the pre-procedure evaluation of the patient that may affect the successful and safe completion of a colonoscopic examination. These include:
Anatomic issues, such as history of abdominal and/or pelvic surgeries, recent colonic surgery, presence of a colostomy, and abdominal hernias.
Comorbidities that may increase sedation-associated risks.
Comorbidities that may affect to position of the patient properly during colonoscopy or to application of abdominal pressure during the procedure may impact the assistant’s ability to do it appropriately.
The presence of some pacemakers and an implanted cardiac defibrillator need special consideration while using specific management for example. During the application of electrocautery
The patients on chronic use of certain medications such as narcotics or benzodiazepines, may increase their tolerance of the patient to the effects of sedation
A history of difficult intubation by anesthesia
10.6 Patient preparation
10.6.1 Diet
Prior to elective colonoscopy, patients need to consume clear liquids or a low-residue diet for at least 1 day. A low-residue diet is low in fiber. So the patients should be instructed to avoid foods that are high in fiber such as whole grains, vegetables,and fruits. Clear liquids include water, tea (without milk), coffee, gelatine, ices, and fruit juices such as grapefruit, apple,and lemonade. Liquids that are red should be avoided as they can be mistaken for blood in the colon and can obscure mucosal details. One trial found that there was no significant difference in preparation quality between patients treated with 4 L of polyethylene glycol who were assigned to receive either a low-residue diet or clear liquids the day prior to the examination [31]. Similarly, a randomized trial with 230 patients who were receiving a sodium sulfate-based preparation assigned patients to either a low-residue diet for breakfast and lunch the day prior to the colonoscopy or to clear liquids [32]. Again, there was no difference between the groups with regard to preparation quality. However, patients in the low-residue arm reported greater satisfaction with the preparation and were less likely to cancel their procedure (9 versus 20 percent). Whether similar results would be seen outside of a randomized trial is not yet known. Our approach is to recommend a low-residue diet for 5 days prior to colonoscopy, with only clear liquids allowed the day prior to the examination.
Patients typically take no food by mouth for four to 8 hours prior to the procedure (sometimes longer if there is known or suspected delayed gastric emptying) and no liquid (other than sips with medications) for 2 hours [33]. Recommendations differ with regard to pre-procedure fasting for elective procedures. The American Society for Anaesthesiology (ASA) guidelines state that prior to a procedure, patients should fast a minimum of 2 hours following clear liquid ingestion or 6 hours for a light meal [34]. By contrast, the American College of Emergency Physicians states “Recent food intake is not a contraindication for administering procedural sedation and analgesia, but should be considered in choosing the timing and target level of sedation” [35]. The usual practice is to follow the ASA approach.
10.6.2 Medications
Most medications may be continued up to the colonoscopy time and can be taken with a small sip of water on the day of the colonoscopy. Some medications may need adjustment prior to colonoscopy, such as medications for diabetes as oral intake is decreased prior to the procedure and there is a risk of hypoglycemia. It is also advised to stop oral iron at least 5 days before the colonoscopy since it can interfere with the results by making the residual feces black, viscous, and difficult to purge.
Decisions regarding the patients taking anti-platelet agents or anti-coagulants, risk- benefit ratio must be carefully assessed keeping in mind the bleeding probability from the procedure while on medications with the probability of thromboembolic event in case of interruption of anti-thrombotic medication [36]. Furthermore, the urgency of the procedure and the availability of alternative tests must be evaluated. So a detailed discussion should be done with the patient and the clinician prescribing the medication for appropriate management plan regarding anti-thrombotic agents.. Aspirin and non-steroidal anti-inflammatory drugs may be continued safely in standard doses in patients having colonoscopy.
Routine antibiotic prophylaxis is not recommended for colonoscopy as the risk of infection is low related to routine diagnostic or therapeutic colonoscopy.
10.6.3 Pre-procedure testing
General recommendation is that routine pre-procedure laboratory testing, electrocardiography, or chest radiography is not required in all patients [37]. Instead, they emphasize testing the selected patients depending on their medical history, physical examination, and risk factors associated with the procedure itself.
The American Society for Gastrointestinal Endoscopy guidelines in 2014 recommended pre-procedure testing in the following settings [37]:
All the women of childbearing age who give uncertain pregnancy history or whose history is suggestive of a current pregnancy (especially if fluoroscopy is going to be used), should undergo pregnancy testing.
Coagulation studies for patients who are actively bleeding, or at increased risk of bleeding due to certain medication (e.g. ongoing anti-coagulant use or dual anti-platelet agents), suspected to have bleeding disorder (when there is a history of abnormal bleeding), malnutrition, prolonged biliary obstruction, or other conditions associated with acquired coagulopathies.
The patients with decompensated heart failure or having respiratory symptoms, chest radiograph should be done.
The patients with pre-existing clinically significant anemia or who are actively bleeding, or when they are at high risk of significant blood loss during the endoscopic procedure, fresh hemoglobin/hematocrit report should be available.
Blood typing and cross-match for the patients with active bleeding or anemia who are likely to have a blood transfusion.
The patients with significant hepatic, endocrine, or renal dysfunction, serum biochemistry is required particularly if need to use medications that may further impair function.
Routinely, most of the centers do not check the coagulation profile of the patients on anticoagulants if the medication has been stopped for an appropriate amount of time before the planned procedure.
10.7 Colonoscopy prepared by sodium phosphate vs. polyethylene glycol
Polyethylene glycol (PEG).(NuLYTELY, Half Lytely, and. GoLYTELY; Braintree Laboratories, Inc., Braintree, MA; Colyte;. Schwarz Pharma, Milwaukee, WI, and MoviPrep; Salix Pharmaceutical, Inc., Morrisville, NC.) and sodium phosphate (NaP) tablets. (Visicol and OsmoPrep Tablets; Salix. Pharmaceuticals, Inc., Morrisville, NC), NaP solution. (Fleet Phospho-soda; C.B. Fleet Company, Inc., Lynchburg, VA), are the most widely. Used agents for colon cleansing. Polyethylene glycol.is an orally administered isotonic solution introduced in 1980 [38]. Since PEG is non-digestible and. Non-absorbable, it cleanses the colon by purging. of intraluminal contents [39]. Because it is iso-osmolar. With plasma, the large volume of PEG does not result in significant fluid shifts. It has been shown to be highly effective when taken as instructed (4 L of PEG.solution). However, the efficacy of standard 4 L PEG outside of clinical trials is compromised by poor patient compliance. The large volume and taste are the main factors that contribute to poor patient compliance and tolerability [40, 41, 42], which led to the development of reduced-volume PEG solution. With or without laxatives, sulfate-free, and. Flavored PEG solutions (Half Lytely, NuLYTELY) in an attempt to reduce the sulfate odor and improve the taste [43]. In some studies, split-dose PEG has been more effective than standard 4 L PEG [44, 45].
All patients are asked to avoid eating seeds containing vegetables, berries, fruits, and bread in the week before the colonoscopy. Patients are told to drink 3–4 liters of PEG-EL solution (1.2–1.8 L/h) starting in the afternoon (02:00 pm) on the day before the colonoscopy. Analgesia is given with IV tramadol and phloroglucinol and sedated with midazolam prior to the procedure.
10.8 Assessment of bowel preparationl
Bowel preparations are often described with terms such as unsatisfactory/inadequate, poor, fair, good, and excellent. To standardize descriptions, systems for reporting bowel preparation quality have been developed, including the Boston bowel preparation scale [46]. The score ranges from 0 to 3 (Figure 6) for individual colonic segments: the right side of the colon (including the cecum and ascending colon), the transverse colon (including the hepatic and splenic flexures), and the left side of the colon (including the descending colon, sigmoid colon, and rectum). These segment scores are summed for a total Boston bowel preparation scale score, which ranges from 0 (poor) to 9 (excellent):
Score 0: Unprepared colon with mucosa not seen because of solid stool that cannot be cleared
Score 1: A portion of the mucosa of the colon segment was seen, but other areas of the colon segment were not seen well because of staining, residual stool, and/or opaque liquid
Score 2: Minor amount of residual staining, small fragments of stool and/or opaque liquid, but most mucosa of the colon segment is seen well
Score 3: Entire mucosa of colon segment seen well with no residual staining, small fragments of stool, and/or opaque liquid
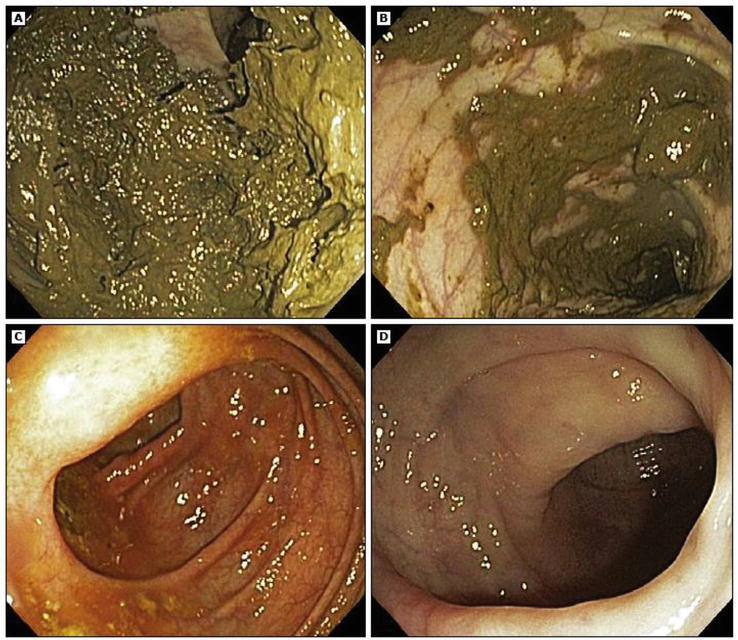
Figure 6.
Boston bowel preparation scale.
The BBPS. A: Segment score 0, unprepared colon segment with mucosa not seen because of solid stool that cannot be cleared. B: Segment score 1, portion of mucosa of the colon segment seen, but other areas of the colon segment not well seen because of staining, residual stool, and/or opaque liquid. C: Segment score 2, minor amount of residual staining, small fragments of stool and/or opaque liquid, but mucosa of colon segment seen well. D: Segment score 3, entire mucosa of colon segment seen well with no residual staining, small fragments of stool and/or opaque liquid.
11. Conclusion/awareness to enhance the health care team outcomes
Polyethylene glycol is a polyether compound derived from petroleum having wide range of applications in so many industries including medical, biological, chemical, industrial, commercial and entertainment industries. As a medication, it belongs to laxative class of drugs. It is used in the management and treatment of chronic constipation and fecal impaction due to its water retention property. It is also used for colonoscopy preparation to cleanse the bowel providing clear image for detailed diagnostic evaluation of the colon. It causes side effects which are mostly minor and tolerable. It is an over the counter medication. As such there is increased access to the drug.
Polyethylene glycol is considered to be biologically inert and safe by US FDA. The large percent of population can develop antibodies to PEG because of its ubiquity in multitude of products. Allergic reactions to polyethylene glycol are increasing concern [47, 48].
Healthcare providers need to emphasize the directions for its use and misuse. Patients should be counseled about the onset of action as well as when to discontinue it.
They should also be counseled regarding dietary and lifestyle modifications with treatments.
Nutritionists and nurses can play a role in educating patients on a highly nutritious, fibrous diet and increased fluid intake to help with bowel movement.
This approach will yield improved patient results while minimizing adverse events which are still possible with over-the-counter medication like polyethylene glycol (Level 5).
References
- 1.
Jang HJ, Sachin CY, Kim KB. Safety evaluation of PEG compounds for cosmetic use. Toxicology Research. 2015; 31 :105-136 - 2.
US Government–Food and Drug Agency. Food Additive Status List. Food and Drug Administration; 2023 - 3.
Polyethylene Glycol as Pharmaceutical Excipient. Available from: pharmaceutical.basf.com [Accessed: April 27, 2021] - 4.
Ma Y, Ji Y, Zhong T, Wan W, Yang Q, Li A, et al. Bioprinting-based PDLSC-ECM screening for in vivo repair of alveolar bone defect using cell-laden, injectable and photocrosslinkable hydrogels. ACS Biomaterials Science & Engineering. 2017; 3 (12):3534-3545. DOI: 10.1021/acsbiomaterials.7b00601. PMID 33445388 - 5.
Cabanillas B, Akdis CA, Novak N. Allergic reactions to the first COVID-19 vaccine: A potential role of polyethylene glycol? Allergy. 2021; 76 (6):1617-1618. DOI: 10.1111/all.14711. PMID 33320974. S2CID 229284320 - 6.
Bostock N. MHRA Warning after Allergic Reactions in NHS Staff Given COVID-19 Vaccine. GP; 2020. Archived from the original on December 9, 2020. Accessed: December 9, 2020 - 7.
Health Canada. Pfizer-BioNTech COVID-19 Vaccine: Health Canada Recommendations for People with Serious Allergies. Health Canada; 2020 - 8.
Furtula A, Jordans F. EU Regulator Gives Conditional Approval to Pfizer-BioNTech COVID-19 Vaccine. The Globe and Mail Inc. Reuters; 2020 - 9.
Bailey FE, Koleske JV. Alkylene Oxides and their Polymers. New York: Dekker; 1990. pp. 27-28. ISBN 9780824783846. [Accesed: July 17, 2017] - 10.
IJN K, Broekaert IJ, Wilschanski M, Papadopoulou A, Ribes-Koninckx C, Thapar N, et al. Role of PEG in the treatment of functional constipation in children. Journal of Pediatric Gastroenterology and Nutrition. 2017; 65 (4):361-363 - 11.
American College of Gastroenterology Chronic Constipation Task Force. An evidence based approach to the management of chronic constipation in North America. The American Journal of Gastroenterology. 2005; 100 (Suppl. 1):s1-s4 - 12.
Dipalama JA, Cleveland MV, Mc Gowan J, Herrera JL. A randomized multicenter, placebo controlled trial of PEG laxative for chronic constipation. The American Journal of Gastroenterology. 2007; 102 (7):136-141 - 13.
National Institute of Child Health and Human Development. Drugs and Lactation Database (Lact Med). Bethesda (MD): National Institute of Child Health and Human Development; 2022 - 14.
Tabber MM, Di Lorenzo C, Berger MV, Feure C, Langendam MW, Nurkos Staiano A, et al. European Society for Pediatric Gastroenterology. Evaluation and treatment of functional constipation in infants and children: Evidence based recommendation from EGPGHAN and NASPGHAN. Journal of Pediatric Gastroenterology and Nutrition. 2014; 58 (2):258-257 - 15.
Dipalma JA, Cleveland MB, McGowan J, Herrera JL. A comparison of PEG laxative and placebo for relief of constipation from constipating medications. Southern Medical Journal. 2007; 100 (11):1085-1090 - 16.
Di Palma JA, Cleveland MV, Mc Gowan J, Herrera JL. An open label study of chronic PEG laxative use in chronic constipation. Alimentary Pharmacology & Therapeutics. 2007; 25 (6):703-708 - 17.
Bajaj AK, Gupta SC, Chatterjee AK, Singh KG. Contact sensitivity to PEG. Contact Dermatitis. 1990; 22 (5):291-292 - 18.
Belaiche J, Vesin P, Cattan D, Payen D, Rapin M, Ventura M, et al. Acidotic coma after colonic preparation using PEG. Gastroentérologie Clinique et Biologique. 1983; 7 (4):26-27 - 19.
Tayar J, Jabbour G, Saggi SJ. Severe hyperosmolar metabolic acidosis due to large dose of intravenous lorazepam. The New England Journal of Medicine. 2002; 346 (16):1253-1254 - 20.
Jacksongg M. Treatment of chronic pyelonephritis III. Comparison of several drugs combined and one member of the combination, colistin. The American Journal of the Medical Sciences. 1960; 240 :754-763 - 21.
DiPalma JA, Cleveland MV, McGowan J, Herrera JL. A randomized multicenter comparison of PEG laxative tegaserod in the treatment of patients with chronic constipation. The American Journal of Gastroenterology. 2007; 102 (9):1964-1971 - 22.
Saradnna A, Shankar S, Soni P, Pendkar C, Saxena A, Kupfer Y, et al. Hyponatremic seizures after PEG bowel preparation: The elderly at risk. American Journal of Therapeutics. 2018; 25 (6):e779-e780 - 23.
Lee TJW, Nair S, Beintaris L, Rutter MD. Recent advances in colonoscopy. Version 1. F1000Res. 2016; 5 : F1000 Faculty Rev-328 - 24.
Kim TK, Kim HW, Kim SJ, Ha JK, Jang HH, Hong YM, et al. Importance of the time interval between bowel preparation and colonoscopy in determining the quality of bowel preparation for full-dose polyethylene glycol preparation. Gut Liver. 2014; 8 (6):625-631 - 25.
Hurwitz H, Fehrenbacher L, Novotny W. Bevacizum-ab plus irinitecan, flurouracil and leucovorin for metastatic colorectal cancer. The New England Journal of Medicine. 2004; 350 (23):2335-2342 - 26.
Chu E, De Vita VT. Physicians’cancer Chemotherapydrug Manual. Jones and Bartlett Publishers; 2008 - 27.
Martel M, Barkun AN, Menard C, Rastellini S, Kherad O, Vanasse a. Split-dose preparations are superior to day-before bowel cleansing regimens; a meta-analysis. Gastroenterology. 2015; 149 (1):79-88 - 28.
Wexner SD, Beck DE, Baran TH, et al. A consensus document on bowel preparation before colonoscopy: Prepared by a task force from the American Society of Colon and Rectal Surgeons, The American Society for Gastrointestinal Endoscopy and The Society of American Gastrointestinal and Endoscopic Surgeons. Surge Endose. 2006; 20 (1147):60 - 29.
Brunelli SM, Feldman HI, Latif SM, Gupta M, Weiner MG, Lewis JD. A comparison of sodium phosphosoda pugative to polyethylene glycol preparation prior to colonoscopy. Family Medicine. 2009; 41 (1):39-45 - 30.
American Society for Gastrointestinal Endoscopy. Appropriate use of gastrointestinal endoscopy. Gastrointestinal Endoscopy. 2000; 52 :831 - 31.
Park DI, Park SH, Lee SK, et al. Efficacy of prepackaged, low residual test meals with 4L polyethylene glycol versus a clear liquid diet with 4L polyethylene glycol bowel preparation: A randomized trial. Journal of Gastroenterology and Hepatology. 2009; 24 :988 - 32.
Sipe BW, Fischer M, Baluyut AR, et al. 726 effect of low residual diet on colonoscopy bowel preparation. Gastrointestinal Endoscopy. 2012; 75 :AB163 - 33.
Faigel DO, Eisen GM, Baron TH, et al. Preparation of patients for GI endoscopy. Gastrointestinal Endoscopy. 2003; 57 :446 - 34.
American Society of Anesthesiologists Task Force on Sedation and Analgesia by Non-Anesthesiologists. Practice guidelines for sedation and analgesia by non-anesthesiologists. Anesthesiology. 2002; 96 :1004 - 35.
Godwin SA, Caro DA, Wolf SJ, et al. Clinical policy: Procedural sedation and analgesia in the emergency department. Annals of Emergency Medicine. 2005; 45 :177 - 36.
ASGE Standards of Practice Committee, Anderson MA, Ben-Menachem T, et al. Management of antithrombotic agents for endoscopic procedures. Gastrointestinal Endoscopy. 2009; 70 :1060 - 37.
ASGE Standards of Practice Committee, Pasha SF, Acosta R, et al. Routine laboratory testing before endoscopic procedures. Gastrointestinal Endoscopy. 2014; 80 :28 - 38.
Davis GR, Santa Ana CA, Morawski SG, Fordtran JS. Development of a lavage solution associated with minimal water and electrolyte absorption or secretion. Gastroenterology. 1980; 78 :991-995 - 39.
Hsu CW, Imperiale TF. Meta-analysis and cost comparison of polyethylene glycol lavage versus sodium phosphate for colonoscopy preparation. Gastrointestinal Endoscopy. 1998; 48 :276-282 - 40.
Aronchick CA, Lipshutz WH, Wright SH, Dufrayne F, Bergman G. A novel tableted purgative for colonoscopic preparation: Efficacy and safety comparisons with colyte and fleet phospho-soda. Gastrointestinal Endoscopy. 2000; 52 :346-352 - 41.
Radaelli F, Meucci G, Imperiali G, Spinzi G, Strocchi E, Terruzzi V, et al. High-dose senna compared with conventional PEG-ES lavage as bowel preparation for elective colonoscopy: A prospective, randomized, investigator-blinded trial. American Journal of Gastroenterology. 2005; 100 :2674-2680 - 42.
Hayes A, Buffum M, Fuller D. Bowel preparation comparison: Flavored versus unflavored colyte. Gastroenterology Nursing. 2003; 26 :106-109 - 43.
Fordtran JS, Santa Ana CA, Cleveland MVB. A low-sodium solution for gastrointestinal lavage. Gastroenterology. 1990; 98 :11-16 - 44.
El Sayed AMA, Kanafani ZA, Mourad FH, Soweid AM, Barada KA, Adorian CS, et al. A randomized single-blind trial of whole versus split-dose polyethylene glycol-electrolyte solution for colonoscopy preparation. Gastrointestinal Endoscopy. 2003; 58 :36-40 - 45.
Aoun E, Abdul-Baki H, Azar C, Mourad F, Barada K, Berro Z, et al. A randomized single-blind trial of split-dose PEG-electrolyte solution without dietary restriction compared with whole dose PEG-electrolyte solution with dietary restriction for colonoscopy preparation. Gastrointestinal Endoscopy. 2005; 62 :213-218 - 46.
Lai EJ, Calderwood AH, Doros G, et al. The Boston bowel preparation scale: A valid and reliable instrument for colonoscopy-oriented research. Gastrointestinal Endoscopy. 2009; 69 :620 - 47.
Wenande E, Garvey LH. Immediate-type hypersensitivity to polyethylene glycols: A review. Clinical and Experimental Allergy. 2016; 46 (7):907-922. DOI: 10.1111/cea.12760. PMID 27196817. S2CID 1247758 - 48.
Stone CA, Liu Y, Relling MV, Krantz MS, Pratt AL, Abreo A, et al. Immediate hypersensitivity to polyethylene glycols and polysorbates: More common than we have recognized. The Journal of Allergy and Clinical Immunology in Practice. 2019; 7 (5):1533-1540.e8. DOI: 10.1016/j.jaip.2018.12.003. PMC 6706272. PMID 30557713