 Open access peer-reviewed chapter
Open access peer-reviewed chapter
Abstract
The constant technological evolution allows health professionals possibilities until then only imagined in the pages of science fiction. The three-dimensional reconstruction of real anatomical models, with the help of Virtual Reality, Augmented Reality, and the impression of realistic shadows, provides surgical teams with the possibility of performing complex surgeries without exposing the patient well in advance, allowing us to achieve excellent results, increasing surgeons’ precision, and decreasing operating room time and patient exposure to anesthesia. In this way, the results are cost containment and increased the productivity and quality of care. Realistic simulations are an advent that allow not only surgeons but also the entire multidisciplinary team to plan each step of the assistance that will be dedicated to patients throughout the surgical process with greater safety and caution, improving the quality of life and assistance provided to our patients.
Keywords
- realistic simulation
- surgical nursing
- patient safety
- pediatric neurosurgery
- quality
1. Introduction
1.1 The need for simulations in pediatric neurosurgery
Surgical procedures involving the Central Nervous System are complex by themselves and require specific skills from the neurosurgeon and the entire team involved in the surgical procedure, these skills can take years of practice to be acquired. With technological development; these skills change more quickly when compared to the others, as we can anticipate the learning curve using it as a shortcut. In the case of pediatric surgeries, there are also specific implications with anatomical development, which further limit the acquisition of these skills in the short term. The simulation strategy can be considered as a great facilitator in the acquisition of tactile skills and in the construction of logical reasoning for decision-making and behavior changes, as the experience in simulated situations will be able to provide the surgeon with skill and safety in real situations.
1.2 The use of simulations and their characteristics
The concept of simulation can be defined as the technique where a “simulator” is used in which techniques or behaviors can be replicated in a non-real event so that participants acquire motor skills and/or specific behaviors for each type of event, without exposing them to such situations before they have acquired skills [1, 2].
We can also broaden the concept of “simulator”, placing it not only as a real replica of something or someone but also as an event where the interpretation and imitation of a potentially real situation contribute not only to the improvement of motor skills but also to the acquisition of logical and critical reasoning, in addition to more accurate decision-making [1, 2].
These concepts have been widely used in the areas of human knowledge for centuries, in the military field and in the development of technologies, equipment, and products, in addition to medical areas and other segments of human health, such as emergency care or complex surgeries [2, 3, 4].
Some areas of human development have among their attributions the use of simulations as a basic requirement in academic training or professional development. From complex equipment simulators such as airplanes and robots to complex neurosurgical procedures.
Graduations in the various areas of human health have been demanding from future professionals a minimum number of hours of simulations or improvement in equipment that can faithfully reproduce the functionalities of specific situations. Thus, they provide the future professional with the experience of contact with materials and equipment or experience with complex situations in a safe place before exposing the professional and the patient to a real situation that exposes them to risks [2, 4, 5].
In this context, Pediatric Neurosurgery becomes one of the medical specialties most benefited from the technological advent of realistic simulations, as we can safely and assertively replicate procedures of different complexities, from a simple trephination to a complex process for separating craniopagus twins, significantly reducing the learning curve of new and experienced surgeons with the acquisition of motor and intellectual skills, preserving the integrity of patients, and minimizing the entire process of caring for children undergoing surgery.
2. Methods
This chapter is a literature review, associated with the experience report of a large Brazilian Hospital in the areas of realistic simulation for specific cases of pediatric neurosurgery.
3. A brief history of simulations
The beginning of the use of simulations dates to the 5th century BC where Greek generals used a board game called Petteia to simulate field battles between two armies and thus define their war strategies, with progression and division of troops across the battlefield. This game was described by Plato in his dialogs with Socrates as the science for logical and strategic reasoning; it was also cited several times by Aristotle and reproduced in Greek art countless times [6, 7, 8].
In the Middle Ages, there are reports of generals who played chess and other variations with the same objective. Kings and high-ranking generals used the famous “war tables”, on which commanders moved pieces representing military units across the battlefield, simulating maneuvers and decision-making. This strategy was decisive for the Allies in World War II due to territorial proportions and remains active until the twenty-first century (Figure 1) [1, 2, 5].

Figure 1.
The operations room at RAF fighter Command’s No. 10 Group Headquarters, Rudloe manor (RAF box), Wiltshire, showing WAAF plotters and duty officers at work, 1943. Public domain.
More complex war games were developed and introduced in training as true situational simulators, so the commanders involved can fight battles between two or more armies and develop more advanced strategies, anticipating behaviors and situations on several fronts and managing to project problems and improve decision-making [6].
From the 1940s, with the invention of computers, virtual simulations also gained ground among the military and gave rise to new simulation technologies. During the Cold War, the United States Department of Defense developed networking; this was the world’s first multiuser virtual simulator, which simulated real-time strategies with participants from different areas; this program broke major paradigms at the time, as it managed to simulate battles virtually for the first time in history [3, 7, 9].
As seen, the military has benefited from complex simulation strategies throughout history; however, other areas also benefit from simulated situations and simulators, not only for training reasoning but also for acquiring tactile skills. Descriptions of the use of anatomical simulators for education and training are present throughout the development of known civilizations, benefiting patients and health professionals for at least 20,000 years [10, 11, 12].
3.1 The importance of anatomical development for simulation
Differently from the military area, the evolution of simulations around human health took place with the use of human and animal cadavers and with the construction and manipulation of anatomical models, which totally or partially replicated human body systems, tissues, or isolated organs [9]. In this context, we cannot talk about simulations without going back to the whole course of anatomical discoveries and how they evolved throughout the history of civilization and influenced the development of these techniques (Figure 2) [10, 11, 12].
24,000 BC: The first human models began with rudimentary sculptures and cave paintings.
4000 BC: The first pathological studies began in Eurasia and developed significantly in the Egyptian civilization [11, 12, 13].
510 BC: Alcménon of Crotona, disciple of the Pythagorean School of Philosophy, dissected a human corpse for the first time with an academic objective and opened up concepts hitherto unknown to men [11, 12].
322 BC: Hippocrates dissected several animals and compared his discoveries with similar human characteristics, ended up building the first medical concepts and tracing what would become physiological studies in the future [11, 12].
250 BC: Herophilus of Chalcedon carried out relevant anatomical studies and the first public dissections in the ancient world and even wrote the first books on human anatomy [11].
200: The works of the Roman physician Claudius Galen provided vital information for human anatomy and for solving complex problems [11, 12].
1240: The medical school of Naples introduced the subject of Human Anatomy into the curriculum, a decisive step toward scientific developm4444ent [9, 10, 11].
1500: Artists such as Leonardo da Vinci and Michelangelo expanded the human view on the anatomy and concepts of the human body [11, 12, 13].
1550: The results published by physician Andreas Vesalius in the book “De Humani Corporis Fabrica Libri Septum” were the watershed and transformed rudimentary anatomy into what we know as modern anatomy, with descriptions and drawings of all systems in the most complex form ever seen until then (Figure 3) [11, 12, 13].

Figure 2.
Surgical simulation timeline. Silva, AR. Ribeirão Preto. 2023.
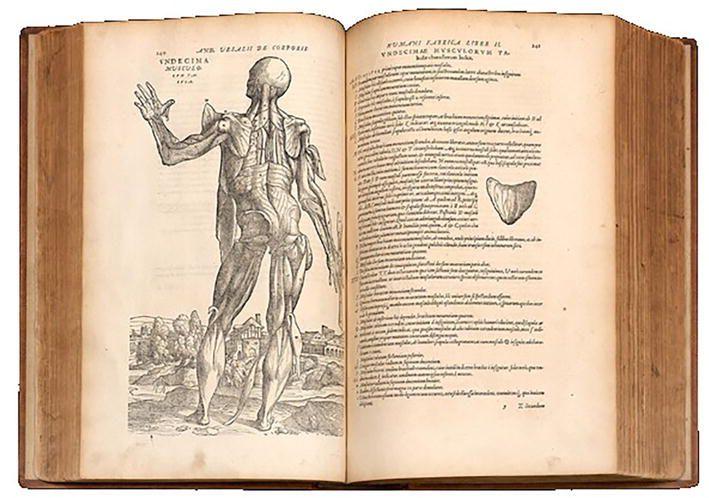
Figure 3.
Book: De Humani Corporis Fabrica Libri septum. Andreas Vesalius. 1555. Museum Für Medizinhistorische Bücher Muri. Available. Muri, Switzerland. 2023.
3.2 The development of simulators
The use of cadavers remained standard in European medical schools; however, their use had considerable limitations, such as tissue deterioration and lack of malleability and vascularity, which made the use of these models unfeasible for a long time; in addition, cadavers are difficult to obtain. In view of these limitations, the creation of the first simulators was considered so that educators and professionals would have permanent access to a realistic model of training and teaching [9, 10].
The first models designed for this purpose were described in ancient India, using nasal simulators made with leaves, twigs, and clay, dating from the 6th century BC for the acquisition of specific skills in anatomical manipulations and rudimentary surgical instruments (Figures 4–6) [11, 12, 13].
Figure 4.
Anatomy lesson, Dr. van der Meer. Van Mierevelt, 1617. Delft museum. Amsterdam, Nederlands. Starling IG. 2023.
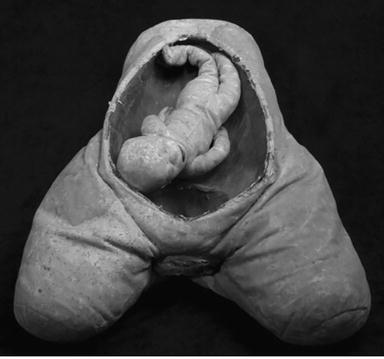
Figure 5.
Obstetric birth simulator dating from the 18th century. Dittrick medical history center, Case Western Reserve University, Cleveland, OH, United States. 2023.

Figure 6.
Dr. Stephen Abrahamson and Dr. Judson Denson with Sim one. Cooper, Taketi. 2004.
The first non-rudimentary models developed specifically for medical procedures date back to the 18th century with anatomical simulators created for training obstetricians and midwives [13].
More complex simulators and with more elaborate materials were developed over the years; in this context, we can consider anatomists like Richard Manningham and Marguerite Le Boursier du Coudray as great precursors of surgical simulation and Obstetrics as a pioneering discipline in the development of these technologies [11, 12, 13], including the first simulators with simulated venous circulation, which appeared at the same time [14].
The twentieth century, with its technological development, provided the modernization of simulators, mainly from the 1950’s, and they gained a new concept among teachers and health professionals [9, 12, 13].
In the late 1960’s, Abrahamson and Denson, from the University of Southern California, created the first computer-controlled anesthesia simulator, a device capable of simulating airway definition techniques, changes in vital signs, and physiological responses such as anisocoria, for example (Figure 7) [15].

Figure 7.
Brain microsurgery simulation and aneurysm clipping using human placenta. Santos Filho JAM. Belo Horizonte. Brasil. 2015.
Since then, the concept of “simulators” has also been expanded and real situations have been introduced in a replicated and simulated way in medical schools. Using interpretation techniques as an ally and hiring actors to perform simulations of meetings with patients for physical examinations and data collection. That is, in this context, the actors, their bodies and their interpretive techniques, are considered simulators [13, 15].
Although the practice presents excellent results, only in 1993 was the first incorporation of this method by the Medical Council of Canada and this practice gained strength and in 2004 became a requirement for medical licensing in the United States [16].
The concept continued to expand in the main academic centers of the world, and currently, the simulation is directly associated with specialized and effective surgical planning, which makes the teams gain time and precision, in addition to reducing the costs generated with the steps of the chain of care [13, 15, 16, 17, 18].
3.3 Different techniques for different needs
With technological advancement and nonlinear teaching techniques, we can currently experience two major fronts of surgical simulations: those performed in virtual environments and those performed in physical environments. Therefore, we need to define the simulators and simulation events and know the functionalities of each one.
3.4 Neurosurgical physical simulators
Specifically in Neurosurgery, in most cases, we use biological simulators; these are cadavers or human and animal tissues, where techniques are created and/or trained, with their known and significant limitations, such as difficulties in obtaining fresh cadavers and lack of vascularization and tissue malleability; we will place greater emphasis on non-biological simulators (Figure 8) [19].

Figure 8.
Specific simulators used for planning the separation of craniopagus twins. HC collection. HCFMRP-USP. Ribeirão Preto. Brazil. 2023.
The technology of printed simulators has been gaining a lot of space among neurosurgery professionals; these can be just for demonstrations of techniques or equipment, such as models for endoscopic third ventriculostomy or aspiration and resection of tumors, where surgeons with experience can test new equipment in practice or even for complex cases; its great advantage is the development of tactile ability (Figure 9) [20, 21].

Figure 9.
High fidelity simulator for Neuroendoscopy training for third Ventriculostomy. Caselato GCR. São Paulo, Brazil. 2019.
Printed simulators can be divided into three subgroups: low, moderate, and high fidelity. This definition comes from the ability of the equipment to reproduce situations with high fidelity, which may include anatomical and/or physiological reactions, the presence of blood and secretions, and the use of sounds and images:
3.5 Virtual simulators
With the development of high-fidelity neuroimaging reconstruction, virtual simulators began to gain ground in academia and medicine. They are generally used for specific situations and are able to serve teams due to their high level of detail and practical interaction [20, 21].
They also have important limitations, as there is no tactile experience with the patient and the interaction of the instruments with the model; therefore, this type of simulator is not indicated for the development of manual skills. The great advantages of this type of simulator in relation to the physical simulator are the economy with printing and the possibility of restoring the process and restarting it in its initial position; that is, there is no permanent damage to the simulator, which allows its reuse without limits (Figure 10) [20, 21].

Figure 10.
Virtual simulator for craniopagus separation. HC collection. HCFMRP-USP. Ribeirão Preto. Brazil. 2022.
3.6 Virtual environments for simulation
When we think of a virtual simulation, we need to understand in which environment this simulation takes place; in relation to this technological advent, we can think of three different scenarios: one that takes place entirely in a virtual world, another that takes place in the real world, and one that be able to unify the two realities in real time.
Virtual Reality: In this scenario, the entire universe involved in the simulation is reconstructed in a virtual environment; that is, the Operating Room, those involved, the instruments, and the patient are reconstructed and designed completely in a virtual way. This technique allows placing participants in separate locations in the same virtual room, using the concept of shared virtual environment.
Augmented Reality: This scenario does not reconstruct the universe to be simulated but allows the possibility of applying the virtual simulator as a single object in a non-virtual environment, superimposing the images through glasses or screens and allowing interaction with the object.
Mixed Reality: This scenario combines the overlapping of augmented reality elements with the ability of virtual reality to interact and visualize the elements but in a real environment [20, 21].
3.7 Simulations and their subdivisions
Individually, we can use physical or virtual simulators to define and train specific interventions in complex cases and have the first contact with real-size models, allowing the professional to define with greater precision the surgical positioning, instruments, equipment, disposable materials, and techniques necessary for each case, in addition to a considerable decrease in the learning curve of surgical techniques [20, 21, 22].
3.8 Situational simulation
Situational simulations are performed for situations or procedures in the same segment, for example, clipping aneurysms or endoscopic surgeries for resection of skull base tumors. They have as their main objective the acquisition of tactile skills; the development of logical and critical reasoning remains as a secondary objective in a situational event, such as the conduct to be taken in a hemorrhage in endoscopic skull base surgeries or the rapid replacement of an engine that malfunctions at the time of craniotomy.
This type of simulation often occurs in pre-congress, extension, or professional training courses. Other segments of the health area use many simulated events for training and skills improvement; and among these, Pediatric Nursing stands out [20, 21, 22].
3.9 Realistic simulation of specific patient case
In complex single cases or for the implementation of new techniques in large health services, realistic simulations can be great allies for the quality of surgical intervention.
This type of simulation is used for the surgical planning of complex cases, where each stage of the surgery is simulated, narrated, and discussed among the team, and its main objective is to project a real situation that will happen soon, identify the critical points, and thus plan the intervention before the actual surgery [21, 22].
Neurosurgeons from large centers such as São Paulo, London, Tokyo, or New York, for example, use this technique for extreme cases, thus managing problems even before scheduling surgery, making surgery safer and more economical. As the simulators are built from the child’s neuroimaging, it is possible to perform tomography or magnetic resonance imaging of the shadow in the postoperative period and in this way even evaluate the result of the surgical intervention.
3.10 The simulation stages
For the simulations to reach their main objective, it is necessary to be attentive to the three fundamental stages within the process that compose it and to understand the totality of the patient, where the Central Nervous System is just one component of all systems. In this context, these steps are important to define the objectives of the simulation.
Briefing: Step that occurs before the simulation event. Dedicated to the case study, clinical evaluation, and discussion among the participating team about the main objectives to be achieved; it is also important to define the place where the simulation will take place, the projection of all the steps and all the necessary instructions in these variables.
Action: This step is the simulation event where all pre discussed points will be inserted in a simulated surgical event.
Debriefing: Moments after the simulation, where all participants carry out a critical reflection on the simulated event, whether the objectives were fully or partially achieved, where failures occurred, and where intervention is necessary.
It is essential for the simulation leader that all these steps are performed. The critical and constructive vision of this professional must be exposed to the team, and in this way, the disciplines must be reviewed if the objectives are not achieved, and thus, it will be up to the organizer to remind everyone what can be improved and simulated again [21, 22, 23].
4. The experience of a University Center in Brazil
The quality in neuroimaging definition already allows 3D reconstructions to be carried out in offices, clinics, and even on home computers that have access to the necessary programs and files. That is, the use of the virtual world in the programming and simulation of large neurosurgical procedures need not be restricted to large health centers. The University Hospital of the Faculty of Medicine of Ribeirão Preto of the University of São Paulo is an example; it already uses this reality and obtains fantastic results (Figure 11).

Figure 11.
Realistic simulation for separating craniopagus Siamese. HC collection. HCFMRP. Ribeirão Preto. Brazil. 2023.
In 2018, we carried out the first successful Craniópagus separation in Latin America and the simulation events were decisive for the success of this process; the printing of specific shadows was a watershed for the institution and placed Pediatric Neurosurgery at the forefront of this type of surgical process in the interior of the state of São Paulo.
Until the beginning of the Covid-19 pandemic, 3D printing for specific patients had a unique growth in the institution, with the implementation of new procedures; the anticipation of problems was detected in the first situational simulations and corrected before the realistic simulation, which allowed us to a shorter hospital stay and anesthetic exposure of patients.
After the full resumption of the Surgical Center in the post-pandemic period, we implemented new processes for pediatric neurosurgery with the addition of virtual simulations, even managing to apply augmented reality by integrating a microscope and neuronavigator.
Simulations are used for new procedures and complex surgeries where we need to involve more than one surgical team at the same time, as for fetal surgical corrections of myelomeningocele, for example (Figure 12).

Figure 12.
Virtual simulation for separating craniopagus Siamese. HC collection. HCFMRP. Ribeirão Preto. 2023. HC collection. HCFMRP. Ribeirão Preto. Brazil. 2023.
In 2022, the institution received a new case of Craniópagus, where the combination of simulations with physical shadows is merging with virtual simulations, bringing fantastic results to children, experienced by the team for the first time.
5. Conclusion
With the popularization of peripherals such as virtual glasses and 3D printers in expansion, we will be able to advance even more in the printing speed of specific simulators for complex simulated events. As the use of realistic simulations is already part of the training curriculum for health professionals in various segments around the world, these are inserted in the daily life of health institutions with much more naturalness for each new generation of professionals.
Would we have imagined mixed reality in the programming of a surgery 15 years ago? Or perform an entire surgery in a virtual environment shared with multidisciplinary teams?
Today, we already use these resources and get fantastic results. Where the future will take us is still a question with many possibilities; the only common answer to these questions is that the objective of providing safer, more assertive, and quality assistance will always guide professionals of this and the next generations.
References
- 1.
Pazin Filho A, Scarpelini S. Simulation: Definition. Medicine Magazine. 2007; 40 (2):162-166. Available from:https://www.revistas.usp.br/rmrp/article/download/312/313/618 [Accessed: June 15, 2023] - 2.
Ziv A, Wolpe PR, Small SD, Glick S. Simulation-based medical education: An ethical imperative. Academic Medicine. 2003; 78 (8):783-788. Available from:https://www.researchgate.net/publication/10616959_Simulation-Based_Medical_Education_An_Ethical_Imperative [Accessed: July 20, 2023] - 3.
Smith R. The long history of games in military training. Simulated Games. 2010; 41 :6-19. Available from:https://apps.dtic.mil/sti/pdfs/ADA550307.pdf [Accessed: June 15, 2023] - 4.
Connoly P. The Art of Medieval Warfare: From Rome to Constantinople. Rio de Janeiro: Zahar; 1998 - 5.
File: The Operations Room at RAF Fighter Command's No. 10 Group Headquarters, Rudloe Manor (RAF Box), Wiltshire, showing WAAF plotters and duty officers at work, 1943. Available from: https://commons.wikimedia.org/wiki/File:The_Operations_Room_at_RAF_Fighter_Command%27s_No._10_Group_Headquarters,_Rudloe_Manor_(RAF_Box),_Wiltshire,_showing_WAAF_plotters_and_duty_officers_at_work,_1943._CH11887.jpg [Accessed: June 15, 2023] - 6.
Chris B. Science for war and peace: Military use has helped advance science, but science's role in the quest for peace is critical. Science Culture. 2022; 74 (4):1-6. Available from:http://cienciaecultura.bvs.br/scielo.php?script=sci_arttext&pid=S0009-67252022000400020&lng=en [Accessed: June 18, 2023] - 7.
Brazil. Air force agency. In: Peccini J. Flight Simulator of the C-105 Amazonas of the Brazilian Air Force is Homologated by ANAC. Brasilia: Brazilian Air Force; 2016. Available from: https://www.fab.mil.br/noticias/mostra/28285/CERTIFICA%C3%87%C3%83O%20-%20Simulador%20de%20voo%20do%20C-105%20Amazonas%20da%20For%C3%A7a%20A%C3%A9rea%20Brazilian%20%C3%A9%20approved%20by%20ANAC [Accessed: November 11, 2023] - 8.
Santos CA, Neto JP, Silva JN. 10 books, 10 regions, 10 games to learn and have fun. Norprint. 2008. Available from: http://jnsilva.ludicum.org/hm2008_9/1grecia.pdf [Accessed: June 18, 2023] - 9.
Rehder R, Abd-El-Barr M, Hooten K, Weinstock P, Madsen JR, Cohen AR. The role of simulation in neurosurgery. Child's Nervous System. 2016; 32 (1):43-54. DOI: 10.1007/s00381-015-2923-z. Epub 2015 Oct 5. Available from:https://pubmed.ncbi.nlm.nih.gov/26438547/ [Accessed: June 18, 2023] - 10.
Coelho G, Vieira T. History of surgical simulation and its application in neurosurgery. Scientia Medica. 2018; 28 (1):13-19. Available from:https://revistaseletronicas.pucrs.br/ojs/index.php/scientiamedica/article/view/29688/16668 [Accessed: June 18, 2023] - 11.
Persaud TVN. A history of anatomy: The post-vesalian era. In: Thomas CC, editor. Illinois: Springfield; 1997 - 12.
Bradley P. The history of simulation in medical education and possible future directions. Medical Education. 2006; 40 :254-262. Available from:https://pubmed.ncbi.nlm.nih.gov/16483328/ [Accessed: June 18, 2023] - 13.
Owen H. Early use of simulation in medical education. Simulation in Healthcare. 2012; 7 (2):102-116. Available from:https://pubmed.ncbi.nlm.nih.gov/22374231/ [Accessed: July 16, 2023] - 14.
Bates AW. Dr Kahn’s museum: Obscene anatomy in Victorian London. Journal of the Royal Society of Medicine. 2006; 99 :618Y624. Available from:https://www.ncbi.nlm.nih.gov/pmc/articles/PMC1676337/ [Accessed: July 27, 2023] - 15.
Cooper JB, Taqueti VR. A brief history of the development of mannequin simulators for clinical education and training. Postgraduate Medical Journal. 2004; 13 (1):11-18. Available from:https://www.ncbi.nlm.nih.gov/pmc/articles/PMC1765785/ [Accessed: July 26, 2023] - 16.
Singh et al. History of simulation in medicine: From Resusci Annie to the Ann Myers medical center. Neurosurgery. 2013; 73 (4):9-14 - 17.
Barreto DC, Silva KGN, Moreira SSCR, Silva TS, Magro MCS. Realistic simulation as a teaching strategy for the nursing undergraduate course: Integrative review. Bahia Journal of Nursing, Salvador. 2014; 28 (2):208-214. Available from:https://www.hindawi.com/journals/nrp/2012/765212/ [Accessed: July 21, 2023] - 18.
Santos Filho JAM. Human Placenta as a Training Model for Brain Aneurysm Surgeries [thesis]. Brazil: Federal University of Minas Gerais; 2015. 71 f. Available from: https://periodicos.ufba.br/index.php/enfermagem/article/view/8476/8874 [Accessed: July 21, 2023] - 19.
Silva AR, Miyazaki AH, Caridade CD, Tassi E. The Advent of Realistic On-Site Simulations for Complex Surgical Cases: A Strategy to Ensure Excellence in Patient Safety. Ribeirão Preto: HC Quality Magazine; 2022. pp. 79-85. Available from: https://www.hcrp.usp.br/revistaqualidadehc/uploads/Artigos/454/454.pdf [Accessed: July 21, 2023] - 20.
Silva AR. Surgical Planning for the Process of Separation of Conjoined Craniopagus Twins. Ensuring Quality and Excellence in the First Stage. Ribeirão Preto: HC Quality Magazine; 2022. pp. 9-16. Available from: https://www.hcrp.usp.br/revistaqualidadehc/uploads/Artigos/452/452.pdf [Accessed: July 21, 2023] - 21.
Caselato GCR. Use of Realistic Simulators in Pediatric Neurosurgery [thesis]. Brazil: University of Sao Paulo; 2019. 129 f. Available from: https://www.teses.usp.br/teses/disponiveis/5/5138/tde-01072019-144748/publico/GiselleCoelhoResendeCaselato.pdf [Accessed: July 21, 2023] - 22.
Carneiro MMG, Kobashikawa. Virtual Reality and its Applications in the Medical Area. São Paulo: Pet-Si Group Newspaper; 2019. Available from: http://www.each.usp.br/petsi/jornal/?p=2628 [Accessed: July 21, 2023] - 23.
Kolbe M, Grande B, Spahn DR. Briefing and debriefing during simulation-based training and beyond: Content, structure, attitude and setting. Best Practice & Research. Clinical Anaesthesiology. 2015; 29 (1):87-96. DOI: 10.1016/j.bpa.2015.01.002. Epub 2015 Jan 28. Available from:https://pubmed.ncbi.nlm.nih.gov/25902470/ [Accessed: July 21, 2023]