 Open access peer-reviewed chapter
Open access peer-reviewed chapter
Abstract
The clinical reasoning model is a theoretical framework that facilitates the transformation of information into practical knowledge within the context of clinical practice. It serves as a valuable resource for healthcare professionals, offering a structured approach for the assessment and development of treatment plans. Biomedical disability models often influence clinical reasoning models in pediatric neurorehabilitation, emphasizing diagnostic reasoning and using a shared vocabulary and language to guide thinking and communication during information gathering, assumption formulation, and care action planning. This method prioritizes physical symptoms over psychological, social, cultural, and environmental factors of a given condition. This idea assumes that the health condition or pathology is the sole fundamental factor contributing to any form of physical dysfunction and that the reduction of the disease will lead to a restoration of the previous state of “normalcy”. The International Classification of Functioning, Disability, and Health (ICF) framework can be used as a clinical reasoning tool as it guides cognitive processes and decision-making based on the interdependent relationships between the three primary components and contextual factors. The ICF framework recognizes that changes in the child’s environmental and psychological context, activity and social involvement, and pathology can affect child outcomes without emphasizing changes in pathology.
Keywords
- clinical reasoning
- neurorehabilitation
- ICF
- pediatric
- WHO-ICF
1. Introduction
Pediatric neurorehabilitation is heavily impacted by biomedical model, which is based on acute care medicine. Consider how we treat sudden severe chest pain: a history is taken, the child is evaluated, other options are ruled out to make the appropriate diagnosis, the right treatment is found, the child is intervened, and the condition is monitored after treatment. This approach focuses on fixing to imply that a specific diagnosis will result in suitable treatment. In pediatric neurorehabilitation, body mechanics and biopsychosocial factors are considered. Heterogeneous groups in the same health condition as the treatment may address signs and symptoms underlying biomedical aspects of the condition, but since the intervention is obvious, the evidence to support or refute it is not enough [1].
This way of thinking has several limitations toward fixing, which refers to the expectation that an appropriate diagnosis will lead to the right interventions. A common diagnosis, Cerebral Palsy (CP) and Autism Spectrum Disorder (ASD), seems specific in pediatric neurology, while the heterogeneous nature of those disorders can affect children’s development for a number of biological reasons with a wide range of impacts. Some of our “treatments” may address biomedical aspects of the condition. For instance, the utilization of botulinum toxin to manage spasticity and anticonvulsants to treat seizure disorders has been observed. However, due to the restricted comprehension and complexity nature of the underlying biomedical processes associated with illnesses such as CP and ASD, even when the biological “impairments” of these disorders can be changed, there are generally few links between bodily alterations and functional outcomes [2, 3]. Development is fast, yet many of our treatments are slow. It is difficult to find causal links between interventions and results due to natural changes influenced by growth and development.
Health is “the ability to adapt and to self-manage” [4]. WHO provided a set of concepts about how we could think about health in 2001 [5]. The International Classification of Functioning, Disability, and Health (ICF) framework is a conceptual framework used to record the positive and negative aspects of every person’s functioning and puts every person in a context: functioning and disability are results of the interaction between the health conditions of the person and their environment (in Figure 1). The ICF framework provides a standard language for the definition and measurement of people’s health and function [5].

Figure 1.
International classification of functioning, disability, and health (copied from WHO [
The clinical reasoning model is a theoretical framework that facilitates the transformation of information into practical knowledge in the context of therapeutic practice. It serves as a valuable resource for therapists, offering a structured approach for both assessment and treatment planning. This method is executed by using a coherent sequence of activities [6].
The reciprocal interactions between the three core ICF components and environmental factors can influence clinical reasoning and decision-making. The ICF framework allows changes in the patient’s environmental and personal context, activity and social participation, and pathology to affect patient outcomes. Improved outcomes without pathological changes are a useful clinical reasoning tool for pediatric neurorehabilitation. The ICF framework allows all health issues to be considered in a border social-ecological setting, which might turn the paradigm upside down. This shows that any section of the framework may have influenced others in this dynamic system [7, 8].
2. The international classification functioning, disability, and health (ICF) model
The International Classification of Functioning, Disability, and Health (ICF) “are functional frameworks that classify health outcomes; they can be used to describe the functioning of all people, not only persons with a health condition(s).” The ICF model is derived from a framework developed by the World Health Organization (WHO) (see Figure 1) [9].
This framework presents an individual’s functioning and disability as consequences resulting from the interplay between health problems and other contextual factors, including both environmental and personal factors. The term “functioning” encompasses the entirety of bodily functions, activities, and participation in many living circumstances, including work, family, and leisure. The term “disability” encompasses a range of conditions, encompassing impairments in bodily function and structure, limitations in activities, and restrictions in participation [9].
The ICF model encompasses body functions and structures, as well as activities and participation. A significant innovation offered by the ICF model, the concept of a child’s environmental and personal/social context are conceptualized and implemented. The consideration of the child’s needs is situated within the framework of the family, taking into account how the nature and types of participation undergo significant transformations from dependent ties during infancy to intricate and more independent life circumstances during adolescence [10]. This innovation also addresses the notion of developmental changes in participation through the imitation of actions and behaviors. The ICF model acknowledges that variations in the environment and the timing of developmental milestones may indicate delays in development rather than functional impairments or limitations [9, 10].
The ICF is founded upon an integration of social and medical theories of disability and places emphasis on the constituents of health rather than the outcomes of illness [9]. The several dimensions of the ICF framework integrate biological, psychological, social, and environmental factors that contribute to child functioning [10]. Research findings have indicated that just the process of diagnosing a child does not serve as an accurate guide for determining the level of treatment provided or the functional results experienced by the patient [9]. The utilization of a medical diagnostic as an individual instrument may result in the omission of crucial information required for effective healthcare planning and management [11].
According to the data presented in Figure 1, the ICF framework categorizes health conditions into three distinct health outcomes: bodily function and structure, activities, and participation. Disease, disorder, or injury might potentially lead to the reduction of three different health outcomes: impairment, activity limitations, and participation restrictions. The interplay among the three components is subject to the influence of contextual factors, which can be categorized into two components: environmental factors and personal factors [9].
The “body” domain (body structure and body function) covers physical and mental functions, sensory responses, multiorgan system structure and function, movement, and reproduction. The “activities and participation” domain evaluates the patient’s capacity to learn, apply knowledge, complete general tasks, communicate, and care for themselves. The ICF also described two types of contextual factors, namely environmental and personal factors. Environmental domains include patient-assistance items and technologies, community services, and relationships, support, and care outside the clinical setting. Each component has a hierarchy of categories and codes in the ICF. Personal factors such as age, sex, education, social class, culture, past experiences, personal character traits, lifestyle, coping style, and occupation are not coded [10, 11].
3. Pediatric neurorehabilitation services
Pediatric neurorehabilitation services include a variety of therapeutic disciplines, such as rehabilitation medicine, physiotherapy, occupational therapy, speech therapy, orthotics and prosthetics, nutrition, psychology, and social services. These services are characterized by their interdisciplinary nature. The presence of divergent governance and policy frameworks among health professionals presents challenges for implementing uniform standards for working practices within the healthcare system. The presence of diversity may influence the quality of services provided to such patients by healthcare professionals [12].
Pediatric neurology affects the child’s psychological, social, and emotional well-being as well as their physical health. This can affect children’s daily physical functioning, including body structure and function and task performance. These tasks include their everyday activities, what they desire to do in their environment, and personal characteristics that help or hinder their functional activities (e.g., at home, in the community, or at school) [13]. Thus, it is important to consider social and family circumstances in pediatric neurorehabilitation.
Healthcare, education, and social services can struggle to support neurologically manifested children and their families. This condition is complicated, so a model like the ICF that considers bodily impairments, personal effects, and environmental effects is needed to manage pediatric neurorehabilitation holistically.
4. Clinical reasoning model in pediatric neurorehabilitation
Clinical reasoning is important as it promotes knowledge acquisition by utilizing simple phrases to explain complicated relationships [12]. The clinical reasoning models utilized in the field of neurorehabilitation are frequently inspired by the biomedical model of disability. As a result, therapists might prefer diagnostic reasoning that aligns with the principles of the biomedical model [13, 14]. The biomedical model applies standard terminology and discourse in the various stages of treatment decision-making, including initial consultation, data collection, hypothesis formulation, and care planning. However, it primarily concentrates on the physical symptoms of a condition and does not adequately consider the psychological, social, cultural, or environmental dimensions [15]. The biomedical paradigm is based on two fundamental assumptions. Firstly, it posits that disease or disorder is the primary and only factor responsible for all physical dysfunction. Secondly, it asserts that the elimination or reduction of the disease would lead to a restoration of the individual’s state to what is considered “normal” [16].
The models considered significant to the practice of pediatric neurorehabilitation include analytical, non-analytical, and hypothetico-deductive reasoning. The analytical model predominantly focuses on a systematic approach to assessment prior to decision-making, whereas the nonanalytical model includes a more spontaneous process that is influenced by the recognition of similar earlier cases [17]. Hypothetico-deductive reasoning involves the formulation and evaluation of diagnostic hypotheses by analytical testing methods, such as patient history and physical examination. These methods are employed to either validate or disapprove of solutions that have been developed through nonanalytical means [18].
4.1 Analytical clinical reasoning model
Theoretical frameworks for clinical reasoning suggest the existence of a sequential set of analytical procedures utilized to establish a correlation between a patient’s symptoms and the ultimate diagnosis [19]. This method uses analytical reasoning in a more planned way by sticking to a set of distinct steps: careful observation, data collection, a physical exam, coming up with hypotheses, and finally diagnostic testing to confirm these hypotheses [20]. Therapists who adopt a biomedical clinical reasoning approach in pediatric neurorehabilitation may prioritize the development of a recovery strategy and the attainment of a diagnosis as the ultimate objectives.
4.2 Nonanalytical clinical reasoning model
Nonanalytical clinical reasoning refers to a cognitive process when individuals are able to arrive at a conclusion without relying on formal analytical methods, instead drawing upon their past interactions and experiences [18, 21]. The automation of this process is frequently noted and seen as an indicator of heightened clinical proficiency. This phenomenon can be attributed to the disparity in prior clinical experience between novices and individuals with higher degrees of expertise, as supported by earlier research [21]. This methodology enables expeditious decision-making, although some scholars contend that it may engender erroneous inferences among less seasoned practitioners. This approach allows for quick decisions to be made by less experienced professionals, and there is a risk of inappropriate conclusions being drawn.
4.3 Hypothetico-deductive clinical reasoning model
The present paradigm is dependent upon the collection of data from the patient, which is then utilized to build a hypothesis. This hypothesis is initially developed by the therapist and then subjected to testing. The confirmation or rejection of the hypothesis depends on the patient’s response to treatment, necessitating the need for periodic examinations [22]. Practitioners across diverse therapeutic fields commonly employ this approach [19, 23]. The initial phase involves the therapist being equipped beforehand with a comprehensive and elaborate patient history, encompassing the patient’s motivations for seeking rehabilitation treatments. Subsequently, the therapist proceeds to administer an examination technique employing several tests and assessments. Following the conclusion of the examination, the therapist proceeds to formulate several hypotheses pertaining to “evaluation, diagnosis, and prognosis.” These hypotheses are developed by synthesizing and analyzing the data gathered throughout the examination, ultimately serving as a foundation for further assessment and prognostication. The therapist may employ a collaborative reasoning approach, drawing upon the patient’s knowledge base, in order to attain a comprehensive grasp of the issue during the therapeutic session. During the process of hypothesis formation, the therapist may introduce generic questions and afterward reflect on the issues expressed by the patient. Ultimately, the therapist arrives at a definitive diagnosis or formulates a comprehensive plan for implementing a specific intervention [23].
Empirical data support the paradigms in rehabilitative treatment. Doody and McAteer [18] employed a qualitative approach and utilized the hypothetico-deductive model to examine the clinical reasoning abilities of expert and novice physiotherapists in the context of outpatient orthopedic care. A group of 10 seasoned doctors and 10 students were observed and recorded via audio while they conducted a comprehensive examination and administered treatment to an actual patient who had not been encountered previously. The findings indicated that every participant employed a hypothetico-deductive reasoning process. However, both individuals with expertise in the field and those with limited experience extended their analysis beyond the first diagnostic phase to incorporate a thoughtful approach to treatment. Specifically, manual therapy treatment was employed as a means to conduct more hypothesis testing. Furthermore, alongside the application of hypothetico-deductive reasoning, the professionals also employed a nonanalytical model, as anticipated, due to their extensive clinical expertise [18].
This model demonstrates a high level of development and serves as a valuable tool in the field of pediatric neurorehabilitation. It effectively integrates decision-making processes with corresponding actions and closely monitors the dynamic changes that occur throughout the patient’s treatment journey. Kenyon [23] utilized this particular model as an instructional tool for providing clinical reasoning skills to students specializing in pediatric physiotherapy. However, it was noted that students exhibited a proclivity for providing an inaccurate portrayal of their actions and thoughts during the diagnostic procedure. However, the authors merely provided a reconstructed conceptualization of the appropriate approach to resolving the issue [23].
The therapists mostly based their decision-making process on subjective results obtained from physical examination rather than relying on objective testing. Consequently, they expressed a lack of confidence in the effectiveness of practical establishment testing. Hence, based on empirical observations, it appears that pediatric neurorehabilitation relies on a combination of analytical thinking, nonanalytical reasoning, and hypothetico-deductive reasoning, as indicated by previous studies [22, 23, 24, 25]. The clinical reasoning models in question likely originate from the framework of biomedical knowledge. Consequently, therapists in the field of pediatric neurorehabilitation often make the assumption that an intervention involving the manipulation of bodily functions will yield the intended outcomes in terms of the patient’s physical performance and ability to engage in activities [22]. For instance, there is a common assumption that enhancing the muscular strength of an ambulant child (body function) will influence the child’s capacity to walk with optimal efficiency (related to activity).
In the field of pediatric neurorehabilitation, it is crucial for therapists to apply a clinical reasoning model that acknowledges the significance of the biomedical model while also offering a structured approach to recognizing and addressing both biomedical and psychosocial factors. The ICF model facilitates the formulation of a hypothesis by taking into account the interplay between several aspects, such as bodily structure, function, activities, and participation, as well as environmental and personal factors, for every individual child.
5. Personal factors in the ICF framework
Personal factors (PFs), known as background knowledge about a person’s life and way of living, have not been categorized by the WHO. Examples of personal factors include assets, coping methods, education, and behavioral patterns [8]. The facilitation of comprehension about the cognitive processes of children and their parents, including their evaluation and understanding of their own situations, aspirations, and coping mechanisms in their everyday lives, can be enhanced by the identification of these factors pertaining to functioning. The decision-making process regarding the choice of rehabilitation programs, measures, and other forms of support is contingent upon the effect of PFs and their respective interpretations [24].
Numerous studies have consistently demonstrated the significant function and special significance of PFs in the context of rehabilitation processes. Patient- and family-centered care emphasizes the importance of prioritizing the needs and preferences of individuals and their families during various healthcare processes. Moreover, by comprehensively comprehending and incorporating PFs into the evaluation of a client’s functioning, professionals in neurorehabilitation can enhance their grasp of effective strategies to bolster child and parent commitment. PFs would enable therapists to engage in systematic documentation and optimize time management [24, 26]. In the meantime, it is advisable to utilize the ICF framework as a tool for organizing information and ideas associated with functioning, even in cases where PFs have not been officially defined within the categorical framework.
6. Roles of personal factors in pediatric neurorehabilitation
Personal factors (PFs) play an essential role in pediatric neurorehabilitation; asking and understanding about PFs promotes respect for values, beliefs, experience, and circumstances and the inclusion of client-defined families. PF assessment is crucial for pediatric neurorehabilitation planning and functioning documentation. Rehabilitation programs include multiple phases; motivation is personal, and it has been shown to predict exercise intervention adherence. Additionally, different clients value different things, which affect commitment. Considering how different PFs affect commitment might help professionals encourage empowerment and strengths [24, 26]. The rehabilitation process combines two theoretical frameworks: treatment theory shows how to change a factor, and enablement theory recognizes that functioning is complex and determined by multiple factors and models of these complex interrelationships. Understanding child PF variation is necessary to apply enabling theory to pediatric neurorehabilitation. The PFs provide crucial information on functioning throughout a child’s rehabilitation. In clinical practice, the ICF organizes and codes functioning, and environmental and child PFs can affect health, functioning, and the neurorehabilitation process [27, 28].
7. Environmental factors in the ICF framework
The classification of environmental factors was developed to include significant elements of the physical, social, and attitudinal environments in which individuals live and engage in their daily activities. The factors consisted of both immediate factors, such as products and technology for mobility, as well as more distant factors, such as societal attitudes, systems, and policies. These factors have the potential to influence an individual’s functioning. Additionally, there are factors that necessitate interventions targeted at the individual, such as the provision of accessible environments, as well as interventions aimed at society, such as the development and implementation of inclusive policies [8].
The term “disability” can be used to describe various situations. Firstly, it can refer to an individual who solely experiences a physical issue at the bodily level, known as an impairment, without any limitations in their activities or restrictions in their participation. For example, this could include a person with severe scarring on their face who does not encounter any difficulties in their daily activities or engagement in society. Secondly, disability can represent individuals who face challenges in functioning across all three levels: the body (impairments), the person (activity limitations), and society (participation restrictions). Thirdly, disability may involve individuals who have both an impairment and an activity limitation but do not experience any participation restrictions. Fourthly, disability can refer to individuals who encounter activity limitations and participation restrictions but do not have any impairments. Lastly, disability can also apply to individuals who do not have any impairments or activity limitations but face participation restrictions in their daily lives [29].
An illustrative case of an individual encountering impairments, limitations in activities, and restrictions in participation would involve a child with spina bifida. This child, regrettably, lacks access to essential services such as orthotic and prosthetic services, which are crucial for their well-being. Additionally, due to the absence of assistive technology in the form of an orthosis, the child faces difficulties in mobility. Furthermore, their ability to attend school is hindered by an inaccessible educational environment and the presence of negative attitudes toward their condition. To gain a comprehensive understanding of an individual’s experience of disability, it is necessary to delineate the various dimensions of functioning alongside an examination of the environmental and personal elements that contribute to this experience. The alteration of contextual elements might lead to a modification in the outcome, consequently impacting the experience of impairment. The ICF model offers a conceptual framework that enables the description of the various elements involved in an interaction.
8. Roles of environmental factors in pediatric neurorehabilitation
In the relationship between environmental factors and other components of functioning in the ICF model, disability arises from the interplay between an individual’s health condition and the surrounding contextual elements in which the individual is situated. This relationship is further analyzed in terms of the components of functioning and the three viewpoints of body, person, and society. At the social, bodily impairments, and individual activity restriction levels, it is clear that the consequences are influenced by the interaction of an individual’s health state and many contextual factors [30].
The child who utilizes a wheelchair and is currently not enrolled in an educational institution does not require any modifications to their physical condition in order to access educational opportunities. In order to enhance a child’s engagement in education, it is imperative to address both the accessibility of the school and the prevailing attitudes inside the education system. The education student diagnosed with epilepsy does not necessarily have to abandon their pursuit of training. It is imperative to critically examine the perspectives held by education authorities in order to identify a more efficacious strategy for effectively addressing the potential incidence of a seizure during instructional sessions.
The ICF model offers a comprehensive framework for categorizing environmental influences and their impact on individuals with health conditions. The ICF model serves as the initial step in advancing the comprehension of the influence of the environment on impairment. The application of the ICF model within the context of pediatric neurorehabilitation has the potential to facilitate the active involvement of families in the process of defining goals. This approach also enables therapists to be more adaptable to the specific requirements of the family and to effectively communicate information in a manner that is meaningful and beneficial to them. Moreover, applying the ICF model in the context of pediatric neurorehabilitation could enhance a therapist’s engagement with both the child and their family. It has the potential to facilitate the establishment of attainable objectives and facilitate progression from one level of care to another, taking into account the child’s level of functioning, disability, and health while also considering the child’s environment and personal factors.
9. Clinical reasoning in pediatric neurorehabilitation
The therapist’s level of knowledge, cognitive abilities, and metacognitive skills have a significant impact on the clinical reasoning process because they enable them to effectively recognize and resolve problems in situations that are ambiguous or uncertain [31].
The clinical reasoning process persists throughout the child’s neurorehabilitation course of continuing child management. Reassessment serves the purpose of either providing support for the hypotheses and chosen course of action or indicating the need for revision or production of hypotheses, as well as further data gathering and problem clarification. This may involve an additional examination or a referral for consultation with other specialists. During a therapeutic session, clinicians engage in the ongoing process of interpreting child and parent reactions in order to inform their clinical judgments. Additionally, therapists regularly evaluate treatment outcomes to assess the validity of their management hypotheses [32].
Child and parent thinking regarding their difficulties is of equal importance to the therapist’s thinking. Children and their families typically enter their interaction with a therapist with preconceived notions about the nature of their disorder, which are influenced by personal experiences and guidance from healthcare professionals, as well as input from their social network. Previous research has demonstrated that patients’ comprehension of their clinical condition has a significant influence on their pain tolerance, impairment levels, and ultimate outcome [32, 33]. The presence of a child’s or parent’s beliefs and emotions that hinder their management and recovery might have a detrimental impact on their engagement in the management process, their self-efficacy, and ultimately, their overall outcome. On the other hand, research has demonstrated that patients who are included in the decision-making process exhibit a higher level of accountability for their own treatment and are more likely to have improved outcomes. By engaging in a collaborative reasoning process with their therapists, patients can maximize their self-efficacy and level of responsibility for their management [34].
Therapists specializing in pediatric neurorehabilitation are required to thoroughly evaluate and take into account all conceivable aspects that may have an impact on a child’s overall well-being. Therapists are commonly associated with a primary emphasis on the physical aspects of health. However, in line with the modern biopsychosocial perspective on health and disability, it is essential for therapists to recognize that addressing a child’s well-being necessitates a comprehensive assessment of environmental and psychosocial factors that can impact health. This approach should be implemented within the boundaries of the therapists’ professional training and expertise. A successful approach to addressing this matter necessitates a comprehensive perspective on health and disability as well as a thorough understanding of evaluation and management principles, including knowledge of appropriate referral pathways. Additionally, it demands the acquisition of skills to effectively address all potential elements that may contribute to the issue at hand.
Furthermore, the ability to engage in clinical reasoning is essential in determining the relevance of these potential contributing factors to the specific patient, enabling the healthcare provider to make proper clinical judgments that would ultimately enhance the patient’s overall healthcare outcomes [35]. The ICF model offers a standardized language and framework that facilitates communication regarding health and healthcare across many professional disciplines and scientific fields. The conceptual framework of the ICF emphasizes the absence of a direct cause-and-effect relationship between a particular health condition and the resulting functional outcomes. Additionally, it recognizes contextual elements as significant determinants of outcomes. The ICF model offers a comprehensive framework and organizational system for gathering and categorizing clinical, behavioral, and contextual data. This framework has the potential to have a beneficial impact on the processes of assessment, intervention design, and outcome evaluation [36, 37]. This facilitates the establishment of a comprehensive clinical and contextual profile for a pediatric patient with a neurological health condition and offers systematic guidance for the integrated provision of services to children and their families who need to be included in their rehabilitation management.
Most common pediatric neurological disorders have a reciprocal relationship with their body functions and structures, their ability to conduct functional tasks, and their subsequent engagement in familial, occupational, and recreational responsibilities. The physical well-being, activities, participation, and health of individuals can be impacted in either a positive or negative manner by a range of factors. These factors encompass both environmental elements and various factors that contribute to the shaping of individuals’ behaviors and experiences. These factors include social attitudes, architectural characteristics, legal and social structures, climate, and terrain. Gender, age, psychological traits (e.g., thoughts, beliefs, and coping styles), health and illness behaviors, social circumstances, education, and past and present experiences are also playing a significant role [38].
10. Application of the ICF as clinical reasoning tool in pediatric neurorehabilitation
Therapists in pediatric neurorehabilitation typically use a degree of routine in their evaluation process. Based on their expertise in ICF knowledge and their clinical practice, the therapists have determined the specific categories of information that have been considered highly valuable for the identification of problems and the making of management decisions, as shown in Figure 2. These categories include environmental data, subjective and objective attributes of the patient’s impairments (such as location, behavior, and history of symptoms), as well as specific evaluations of functioning, structure, and cognition.
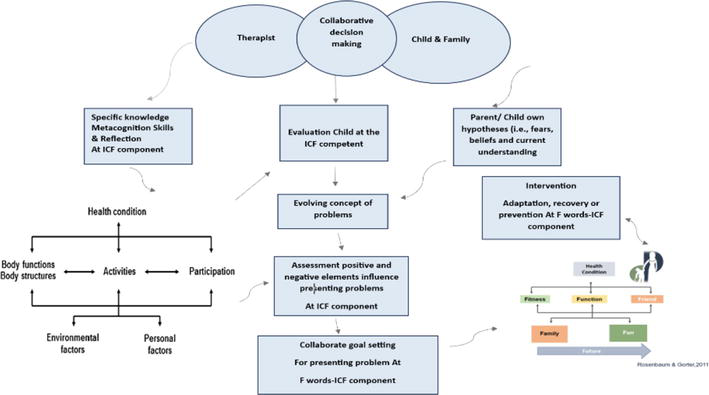
Figure 2.
ICF model of clinical reasoning as collaborative process between therapist in pediatric neurorehabilitation and child & family.
In addition to these established procedures, individualized investigations and examinations are customized to accommodate the individual manifestations of each child. The development of tailored inquiries and tests for each individual child is prompted by the formulation of first hypotheses. The cognitive process known as “hypothesis testing” ideally involves the systematic exploration of both confirming and disconfirming evidence. The obtained data are further analyzed to determine their alignment with previously collected data and relevant theories.
The interpretation of routine inquiries, tests, and spontaneous information provided by child/family will be conducted within the framework of initial hypotheses. Through this process, the therapist gains a progressive comprehension of the child’s neurological disorder. The initial hypothesis will undergo modifications, and further hypotheses will be taken into consideration. The process of generating and testing hypotheses persists until an adequate amount of information is acquired to enable a therapist to formulate a diagnosis pertaining to the physical and psychosocial manifestations. This diagnosis also considers the suitability of therapist involvement and/or referral to other healthcare professionals, as well as the implementation of rehabilitation management strategies.
The clinical reasoning involved in the assessment and management using the ICF component in child and family contexts necessitates the careful study of the cognitive processes employed by the therapist, child, and family, as well as the collaborative nature of decision-making among them. Figure 2 depicts an ICF model of clinical reasoning as a collaborative process involving patients, as proposed in Figure 2. Within the context of pediatric neurorehabilitation settings, the therapist’s cognitive processes are initiated by the initial data and cues acquired, such as the referral information and observations made of the patient. The initial data presented will elicit a variety of impressions or provisional judgments. Although not commonly recognized as such, these early interpretations can be regarded as hypotheses since they are not definitive or conclusive choices. However, these first impressions are evaluated in light of additional information (data) that may either corroborate or contradict them. While there are similarities between this procedure and hypothesis testing, it is important to note that not all therapists may possess a comprehensive understanding of the ICF model or be aware of this process or their thinking in general. The process of hypothesis formation encompasses the integration of specific data interpretations or inductions with the synthesis of many hints or deductions [36, 37, 38, 39].
The use of the six F-word concepts at the clinical level has the potential to enable service providers to effectively incorporate the ICF framework into the development of child-family-neurorehabilitation team goal setting (Figure 2). This approach would involve the inclusion of an individual’s strengths in order to customize interventions. There are six fundamental factors that play an important role in the goal-setting process in pediatric neurorehabilitation [1]:
By addressing function, fitness, family, fun, friends, and constantly reminding therapists in pediatric neurorehabilitation to be aware of the importance of children and families in rehabilitation services. It is crucial to involve child and their relatives in the decision-making process rather than making unilateral decisions on their behalf.
11. Conclusion
The International Classification of Functioning, Impairment, and Health (ICF) serves as a valuable instrument in enhancing comprehension of health and impairment within the context of pediatric neurorehabilitation. The utilization of this tool facilitates the enhancement of clinical reasoning among healthcare professionals by including a greater amount of information that surpasses the limitations of a mere list of diagnoses. Neurorehabilitation personnel must possess an awareness of and familiarity with the personal and environmental elements pertaining to their patients in order to have a comprehensive understanding of their values, desires, and objectives. The incorporation of this element is seen as crucial for the implementation of evidence-based practice within the field of pediatric neurorehabilitation.
The understanding of the impact of the environment and personal factors on disability has experienced a substantial transformation from the ICF framework in pediatric neurorehabilitation. The ICF recognizes the environment as a distinct and essential element within its framework. The ICF’s conceptual framework necessitates the inclusion and clarification of environmental elements in order to fully comprehend disability. The conceptualization of intervention has similarly seen a shift in focus. This paradigm shift includes interventions aimed at both individuals and society, with an emphasis on removing barriers and cultivating facilitators.
Conflict of interest
The author declares no conflict of interest.
References
- 1.
Rosenbaum P, Gorter JW. The ‘F-words’ in childhood disability: I swear this is how we should think! Child: Care, Health and Development (John Wiley & Sons Ltd). 2011; 38 (4):283-289 - 2.
Verschuren O, Ada L, Maltais DB, Gorter JW, Scianni A, Ketelaar M. Muscle strengthening in children and adolescents with spastic cerebral palsy: Considerations for future resistance training protocols. Physical Therapy. 2011; 91 :1130-1139 - 3.
Wright FV, Rosenbaum PL, Goldsmith CH, Law M, Fehlings DL. How do changes in body functions and structures, activity, and participation relate in children with cerebral palsy? Developmental Medicine and Child Neurology. 2008; 50 (4):283-289. DOI: 10.1111/j.1469-8749.2008.02037.x - 4.
Huber EO, Tobler A, Gloor-Juzi T, Grill E, Gubler-Gut B. The ICF as a way to specify goals and to assess the outcome of physiotherapeutic interventions in the acute hospital. Journal of Rehabilitation Medicine. 2011; 43 (2):174-177. DOI: 10.2340/16501977-0629 - 5.
World Health Organization. Towards a common language for functioning, disability and health ICF. In: International Classification. Vol. 1149. 2002. pp. 1-22. Available from: https://cdn.who.int/media/docs/default-source/classification/icf/icfbeginnersguide.pdf - 6.
Banning M. Clinical reasoning and its application to nursing: Concepts and research studies. Nurse Education in Practice. 2008; 8 (3):177-183. DOI: 10.1016/j.nepr.2007.06.004 - 7.
Kostanjsek N. Use of the international classification of functioning, disability and health (ICF) as a conceptual framework and common language for disability statistics and health information systems. BMC Public Health. 2011; 11 (Suppl. 4):S3. DOI: 10.1186/1471-2458-11-S4-S3 - 8.
Demyati H. Exploring the utility of the ICF-CY (international classification functioning disability and health children and youth version) framework as a clinical reasoning tool for physiotherapists who treat children with cerebral palsy [PhD thesis]. United Kingdom: Univerity of Strthclyde; 2017. Available from: https://stax.strath.ac.uk/concern/theses/g732d910q - 9.
World Health Organization. International Classification of Functioning, Disability and Health: Children & Youth Version. Vol. 1. Geneva: World Health Organization; 2007. DOI: 10.1017/CBO9781107415324.004 - 10.
World Health Organization. International Classification of Functioning, Disability and Health (ICF). Geneva: World Health Organization; 2001 - 11.
dos Santos AN, Neves A, Pavão SL, de Campos AC, Rocha NACF. International classification of functioning, disability and health in children with cerebral palsy. Disability and Rehabilitation. 2012; 34 (12):1053-1058. DOI: 10.3109/09638288.2011.631678 - 12.
Darrah J. Using the ICF as a framework for clinical decision making in pediatric physical therapy. Advances in Physiotherapy. 2008; 10 (3):146-151. DOI: 10.1080/14038190802242046 - 13.
Cruz EB, Moore A, Cross V. Clinical reasoning and patient-centred care in musculoskeletal physiotherapy in Portugal - A qualitative study. Manual Therapy. 2012; 17 (3):246-250. DOI: 10.1016/j.math.2012.02.007 - 14.
Jones M, Jensen GM, Edwards I. Clinical reasoning in physiotherapy. In: Higgs J, Jones M, Loftus S, editors. Clinical Reasoning in the Health Professionals. 3rd ed. Philadelphia: Elsevier; 2008. pp. 163-174 - 15.
Wade DT, Halligan PW. Do biomedical models of illness make for good healthcare systems? British Medical Journal. 2004; 329 (7479):1398-1401. DOI: 10.1136/bmj.329.7479.1398 - 16.
Marcum J. Biomechanical and phenomenological models of the body, the meaning of illness and quality of care. Medicine, Health Care and Philosophy. 2005; 7 (311e20):311-320. DOI: 10.1007/s11019-004-9033-0 - 17.
Eva KW, Hatala RM, LeBlanc VR, Brooks LR. Teaching from the clinical reasoning literature: Combined reasoning strategies help novice diagnosticians overcome misleading information. Medical Education. 2007; 41 (12):1152-1158. DOI: 10.1111/j.1365-2923.2007.02923.x - 18.
Doody C, McAteer M. Clinical reasoning of expert and novice physiotherapists in an outpatient orthopaedic setting. Physiotherapy. 2002; 88 (5):258-268. DOI: 10.1016/S0031-9406(05)61417-4 - 19.
Tan S, Ladyshewsky R, Gardner P. Using blogging to promote clinical reasoning and metacognition in undergraduate physiotherapy fieldwork programs. Australasian Journal of Educational Technology. 2010; 26 (3):355-368 [Cited 2023 August 2] - 20.
Carraccio CL, Benson BJ, Nixon LJ, Derstine PL. From the educational bench to the clinical bedside: Translating the Dreyfus developmental model to the learning of clinical skills. Academic Medicine. 2008; 83 (8):761-767 - 21.
Norman GR. Research in clinical reasoning: Past history and current trends. Medical Education. 2005; 39 (4):418-427 - 22.
Case K, Harrison K, Roskell C. Differences in the clinical reasoning process of expert and novice cardiorespiratory physiotherapists. Physiotherapy. 2000; 86 (1):14-21. DOI: 10.1016/S0031-9406(05)61321-1 [Cited 2023 August 2] - 23.
Kenyon LK. The hypothesis-oriented pediatric-focused algorithm: A framework for clinical reasoning in pediatric physical therapist practice. Physical Therapy. 2012; 93 (3):413-420. DOI: 10.2522/ptj.20120080 - 24.
Karhula M, Saukkonen S, et al. ICF personal factors strengthen commitment to person-centered rehabilitation - A scoping review. Frontiers in Rehabilitation Sciences. 2021; 2 (709682):1-11. Available from:www.frontiersin.org - 25.
May S, Withers S, Reeve S, Greasley A. Limited clinical reasoning skills used by novice physiotherapists when involved in the assessment and management of patients with shoulder problems: A qualitative study. The Journal of Manual & Manipulative Therapy. 2010; 18 (2):84-88. DOI: 10.1179/106698110X12640740712770 - 26.
Geyh S, Schwegler U, Peter C, Müller R. Representing and organizing information to describe the lived experience of health from a personal factors perspective in the light of the international classification of functioning, disability and health (ICF): A discussion paper. Disability and Rehabilitation. 2019; 41 :1727-1738. DOI: 10.1080/09638288.2018.1445302 - 27.
Lee JY, Ready EA, Davis EN, Doyle PC. Purposefulness as a critical factor in functioning, disability and health. Clinical Rehabilitation. 2017; 31 :1005-1018. DOI: 10.1177/0269215516672274 - 28.
Whyte J. Contributions of treatment theory and enablement theory to rehabilitation research and practice. Archives of Physical Medicine and Rehabilitation. 2014; 95 :S17-23.e2. DOI: 10.1016/j.apmr.2013.02.029 - 29.
Schneidet M, Hurst R, et al. The role of environment in the international classification of functioning, disability and health (ICF). Disability and Rehabilitation. 2003; 25 (11-12):588-595 - 30.
Arocha JF, Patel V. Methods in the study of clinical reasoning. In: Higgs J, Jones M, Loftus S, editors. Clinical Reasoning in the Health Professions. 3rd ed. Philadelphia: Elsevier; 2008 - 31.
Edwards I, Jones M. Movement in our thinking and our practice. Manual Therapy. 2013; 18 (2):93-95. DOI: 10.1016/j.math.2012.10.002 - 32.
Edwards I, Jones M, Hillier S. The interpretation of experience and its relationship to body movement: A clinical reasoning perspective. Manual Therapy. 2006; 11 (1):2-10. DOI: 10.1016/j.math.2005.10.0 - 33.
Edwards I, Jones M, Carr J, Jensen GM. Clinical reasoning strategies in physical therapy. Physical Therapy. 2004; 84 (4):312-330. DOI: 10.1093/ptj/84.4.312 - 34.
Rothstein JM, Echternach JL. Hypothesis-oriented algorithm for clinicians. A method for evaluation and treatment planning. Physical Therapy. 1986; 66 (9):1388-1394 - 35.
Jette AM, Haley SM, Kooyoomjian JT. Are the ICF activity and participation dimensions distinct? Journal of Rehabilitation Medicine. 2003; 35 :145-149 - 36.
Edwards I, Jones M, Higgs J, Trede F, Jensen G. What is collaborative reasoning? Advances in Physiotherapy. 2004; 6 (2):70-83. DOI: 10.1080/14038190410018938 - 37.
Bruyère SM, Peterson DB. The international classification of functioning, disability and health: Contemporary literature overview of literature. Rehabilitation Psychology. 2005; 50 (2):1-21 - 38.
Martinuzzi A, De Polo G, Bortolot S, Pradal M. Pediatric neurorehabilitation and the ICF. NeuroRehabilitation. 2015; 36 (1):31-36. DOI: 10.3233/NRE-141188 - 39.
Leonardi M, Bickenbach J, Raggi A, Sala M, Guzzon P, Valsecchi MR, et al. Training on the international classification of functioning, disability and health (ICF): The ICF-DIN basic and the ICF-DIN advanced course developed by the disability Italian network. Journal of Headache and Pain. 2005; 6 (3):159-164. DOI: 10.1007/s10194-005-0173-2