Open Access is an initiative that aims to make scientific research freely available to all. To date our community has made over 100 million downloads. It’s based on principles of collaboration, unobstructed discovery, and, most importantly, scientific progression. As PhD students, we found it difficult to access the research we needed, so we decided to create a new Open Access publisher that levels the playing field for scientists across the world. How? By making research easy to access, and puts the academic needs of the researchers before the business interests of publishers.
We are a community of more than 103,000 authors and editors from 3,291 institutions spanning 160 countries, including Nobel Prize winners and some of the world’s most-cited researchers. Publishing on IntechOpen allows authors to earn citations and find new collaborators, meaning more people see your work not only from your own field of study, but from other related fields too.
To purchase hard copies of this book, please contact the representative in India:
CBS Publishers & Distributors Pvt. Ltd.
www.cbspd.com
|
customercare@cbspd.com
The higher annual growth rate of kidney stone disease occurrence and the lower annual growth rate of practicing urologists require more efficient treatment tools. This chapter’s research explores ways to increase laser lithotripsy stone ablation efficiency while reducing the stone retropulsion so that the stone procedure time can be effectively shortened. It covers the investigation of laser stone ablation threshold, ablation efficiency, retropulsion control, and the optimal dusting mode of a concept Holmium-doped yttrium aluminum garnet (Ho:YAG) laser with advanced tailored pulse technology to produce a high ablation rate and low retropulsion. Ho:YAG laser stone damage and recoil movement were investigated in vitro utilizing a tabletop model in a highly reproducible manner while evaluating the effects of several laser mode pulses. A thorough evaluation of the pseudo-optimal dusting mode’s behavior (dusting rate and recoil movement) against a standard laser dusting mode was performed. The optimal dusting mode in this benchtop test model maintained a modest level of retropulsion while having a somewhat quick ablation rate. The transient pressure field measurement results of the standard and custom laser modes of a concept Ho: YAG laser are also included.
Boston Scientific Corporation, Marlborough, MA, USA
*Address all correspondence to: james.zhang@bsci.com
1. Introduction
1.1 Kidney stones diseases
The kidney stone disease occurrence rate is 8.8% in the United States, with an annual growth rate of 5.5% [1]. However, according to the annual census of the American Urological Association (AUA), the annual growth rate of practicing urologists is 2.2%, and of the ratio of urologist-to-population is 1.8% [2]. The gap between disease treatment and the available physician requires efficient treatment tools.
The prevalence of kidney stone disease, urolithiasis, which is the production of hard tissue (stones) in the urinary tract as a result of oversaturated bodily fluids, has progressively increased in recent years. A decrease in urine volume (or water consumption), an increase in calcium oxalate/calcium phosphate secretion, a change in urine pH, and/or urinary tract infections (bacteria that produce urease) are the main reasons for stone formation [3, 4, 5, 6]. According to estimates, 10–15% of cases occur in Western nations, and the recurrence rate can reach 50% [7, 8, 9]. And from 1995 to 2012, around 17 years, kidney stone prevalence increased by almost half, according to Charles D. Scales [10]. Due to factors such as population expansion, anticipated trends in obesity, and projected rises in diabetes, to name a few, the prevalence of urolithiasis has been increasing globally over the past few decades. By 2030, the annual cost of treating stone disease in the United States could exceed $5 billion (at 2014 pricing) [11, 12].
1.2 Advancement of treatment methods for urolithiasis
Even though percutaneous nephrolithotomy (PCNL) is also a “minimally invasive” procedure, the two treatments that are most frequently used in the US to treat patients with urinary calculi are shockwave lithotripsy (SWL) and ureteroscopic laser lithotripsy (URSL) [13, 14]. Due to a slightly faster recovery period and a higher stone-free percentage, URSL is currently the preferred urolithiasis treatment method [3].
Inspired by the theoretical research of Townes and Schawlow, Maiman [15] created the first laser device in 1960. In 1968, Mulvaney et al. [16] used quartz rods to carry the laser emission to the treatment target and documented the first disintegration of kidney calculus using a pulsed ruby laser (694 nm) in an in vitro experiment. After that, the pulsing second harmonic Nd:YAG laser (FREDDY), the pulsing dye-laser, and the triple doped yttrium aluminum garnet flash-lamp-pumped Ho:YAG laser were the three laser lithotripters that were clinically available [17, 18, 19]. Additionally, among all the commercially available lasers for lithotripsy, the flash-lamp-pumped Ho:YAG laser is the most effective and adaptable device when compared to nanosecond Nd:YAG lasers. All calculus compositions can be disintegrated by the Ho:YAG laser, and when compared to short-pulsed lasers, it causes less calculus recoil-movement (retropulsion) [20, 21, 22, 23, 24]. The Ho:YAG laser has long been the go-to lithotripter for the treatment of urinary calculus, having been developed in the 1990s. At a wavelength of 2.1 μm, it is a solid-state pulsed laser. Its broad margin of safety makes it perfect for lithotripsy in the urinary system because it is easily absorbed by water (26 cm-1 [25]) [26, 27, 28]. In addition to treating stone disease, it can be applied to soft tissue conditions such as removing urothelial tumors and curing urinary strictures. The prostate can be surgically removed using the high-powered variation (HoLEP). Thulium fiber laser technology has recently been investigated for future state of art laser lithotripsy [29, 30]. This cutting-edge method has a number of benefits that could push the limits of laser lithotripsy.
1.3 Challenges of laser lithotripsy (URSL)
Intracorporeal lithotripsy has been transformed by the use of medical lasers. The Ho:YAG laser and the more contemporary thulium fiber laser (TFL) are the main players of today, and pulse-modulation technologies can further modify how each of these lasers interacts with stones as well as the intermediary liquid medium. Ho:YAG laser lithotripsy primarily uses photothermal energy, with sonic emission having a minimal impact [31]. In other words, the Ho:YAG laser is photo-thermally restricted because its thermal diffusion time in water throughout its light propagation length is 286 ms [32], which is significantly longer than the laser pulse width (which is often less than a few milliseconds to a few hundred microseconds). Additionally, the Ho:YAG laser is neither photomechanically nor stress-confined in water due to the fact that the sonic diffusion time over the light propagation length is substantially shorter (0.267 μs) than the laser pulse width. Water strongly absorbs at the Ho:YAG 2.1 μm wavelength; hence, the amount of water in the calculus phantom was a factor in its ability to be removed from the sample [33, 34].
The stone disintegration speed, or ablation rate, is one of the essential factors determining laser effectiveness. A higher ablation rate can speed up the procedure, which means a shorter procedure time. And shorter procedure time is linked to less complication [35]. To reduce laser energy attenuation, the laser fiber should, in theory, be in direct contact with the stone. However, in fact, this is frequently not maintained consistently, and half or more of the pulsed laser energy may be transmitted while the fiber is more than 0.5 mm from the stone [36]. Ablation effectiveness is greatly affected if the fiber is not in contact with the stone.
Since its introduction into clinical practice, stone retropulsion has been a factor in intracorporeal laser lithotripsy. Early lasers, like the pulsed dye laser, functioned primarily by photoacoustic means by creating shockwaves that mechanically crushed stones [37, 38]. Stone retropulsion into the kidney increased risk and complexity via nephrostomy and antegrade ureteroscopy [39] and even signaled the end of the procedure due to the enormous quantities of kinetic energy involved and the lack of steerable flexible ureteroscopes [40]. As a result, retropulsion was often seen as a wholly negative phenomenon—a viewpoint that is still common today [41, 42, 43].
Urinary calculi absorb direct light, which raises the temperature of the exposed area above the ablation threshold and prompts the release of fragmented breakdown products. In addition, the creation of vapor bubbles and their subsequent collapse with shock-wave generation is caused by the absorption of laser energy by water between the fiber tip and calculus. The ablation threshold is one of the key variables in laser stone contact. According to the laser energy density, Richard L. Blackmon et al. [44] have investigated the ablation threshold for Ho: YAG and thulium fiber lasers (TFL). However, laser energy itself does not include the temporal information of the laser pulse. The peak power defines how fast the laser energy is delivered. Hence, a peak power density ablation threshold would be more broadly applicable.
Therefore, there are a few gaps in knowledge to be addressed, including peak power density ablation threshold, the transient pressure field of standard and advanced laser modes, and optimum laser dusting setting. In this chapter, we first measured the laser ablation threshold in terms of peak power density for the Bego stone phantom (15:3) with a fixed fiber and stone phantom setup [45]. Bego Stone is a reliable and consistent phantom material for lithotripsy study since it has physical properties matched with those of natural kidney stones of various chemical compositions [46]. The ablation volume is evaluated with direct laser-created crater measurement within the number of laser pulses below the crater volume saturation point. Then, we studied the transient pressure by the laser pulse in water by two types of hydrophones, optical and mechanical. The optimal dusting setting with the custom pulse modulation technology, developed considering the efficient use of laser energy to improve ablation efficiency with less retropulsion, is tested in a benchtop test model.
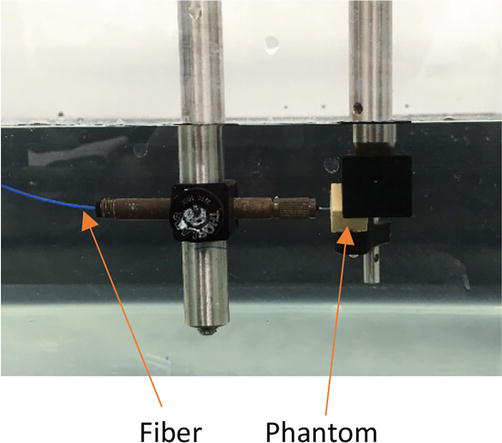
In order to maintain consistency without human factor, the fiber and the stone phantom are fixed inside a water tank with the fiber tip in contact with the phantom as illustrated in Figure 1.
Figure 1.
The picture of the test setup.
Two Ho: YAG lasers that are readily accessible on the market were employed in this work as the laser pulse source. SureFlex™ fibers, Models S-LLF273 and S-LLF365, having core diameters of 273 and 365 μm, respectively, are the fibers employed in the experiment. The substance of the Bego stone (15:3) was used to create the calculus phantoms in the shape of a 10 mm cube. The Bego Stone was prepared with the lowest powder-to-water ratio 15:3 to simulate a natural kidney stone with the highest tensile strength [46]. The Ho: YAG lasers were used to ablate these stone phantoms at various peak power densities. The laser-induced crater volumes were assessed using a 3-D digital microscope (Keyence VHX-900F, Elmwood Park, NJ, USA), and the laser pulse width was determined using a 2 μm photodiode (Thorlabs DET10D). Since the pulse shape is not regular, we use the full width of 10% max as the pulse width definition. This allowed us to calculate the Bego stone phantoms’ ablation threshold as a function of peak power density.
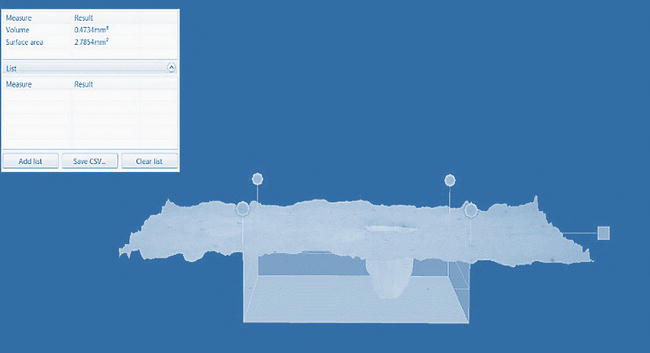
Figure 2 is a screenshot of the laser-induced crater by the 3-D digital microscope.
Figure 2.
A screenshot of the laser-induced crater by the 3-D digital microscope.
2.2 Transient pressure field measurement and retropulsion control
A prototype laser is used for the measurement, which can generate standard short pulse and two custom modes. SureFlex™ fiber, Model S-LLF365, having a core diameter of 365 μm, is the fiber employed in the experiment.
At the energies listed in Table 1, the prototype laser’s three modes were tested using the default pulse width.
Laser mode
0.5 J
1 J
2 J
3 J
Standard-short
X
X
X
X
Fragmenting
—
X
X
X
Dusting
—
X
X
X
Table 1.
The list of energy settings of different laser modes.
At least 40 pulses were included to produce every experimental data point, and the output is the highest hydrophone voltage signal. The largest standard deviation among the data gathered with the mechanical hydrophones was used in a 1-sample t-test. The estimated difference was 31%. The required sample size was determined to be n = 15 for the power of 95% at a significance level of = 0.05. For each of the 40 pulses, we record the highest voltage spike possible and also give the average of the Max.
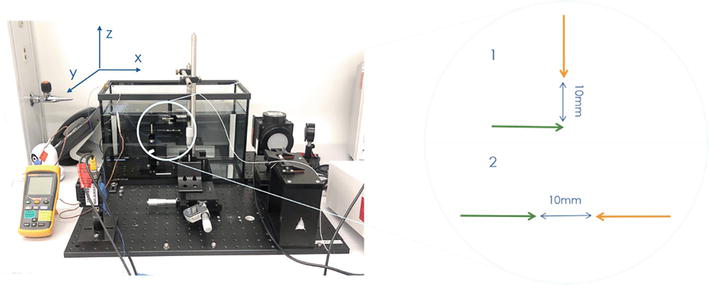
Since the vapor bubble generated by the laser pulse is typically like an ellipsoid, we expect the transient pressure field to have a similar shape. Due to the fact that an ellipse is entirely determined by its major and minor axes, two measurement orientations—parallel and perpendicular—were investigated. The fiber and sensor tips were positioned in both cases (See Figure 3) 10 mm apart. The action center of the vapor bubble collapse, which normally takes place about 0.5 mm distant from the laser fiber tip, was aligned with the sensor at this distance, which reduced damage to the sensor tip from the incident shockwave.
Figure 3.
Sensor to fiber orientation for the transient pressure field measurements.
2.3 The optimal dusting mode
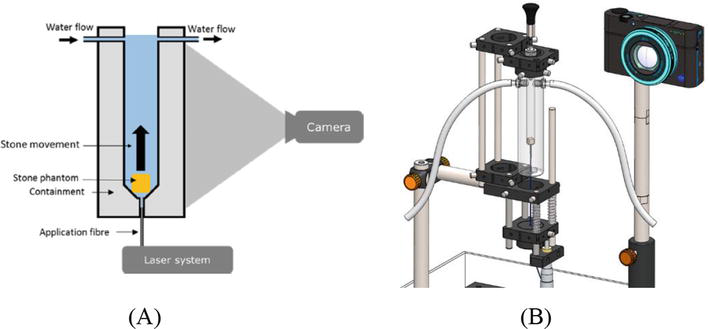
Particularly when measuring retropulsion, it can be difficult to characterize the URS performance (ablation and retropulsion) in a single setup that can simulate the clinical condition [47, 48, 49, 50, 51, 52, 53]. Typically, the laser fiber is fixed during the test [4, 47, 54]. With a benchtop model previously developed by Sroka’s group [4, 47], in vitro tests of Ho:YAG laser-induced stone ablation and retropulsion were carried out in this study. With the use of a hands-free setup and the measurement of the effects of several pulses that simulate a clinical setting, this test is extremely reproducible. Despite the fact that the stone moves during the test, causing the distance between the fiber tip and the stone to change and resulting in a decreased ablation rate being reported, this method is still effective for producing useful data about ablation and retropulsion for contrasting various laser modes. The list of elements in the experimental setup is described in Table 2. In Figure 4, the setup is shown. The composition of the Bego stone is 15:3 [46].
Item
Description
Laser-1
Prototype Ho:YAG laser
Laser-2
Reference Ho:YAG laser
Laser fiber
365-μm S-LLF365 SureFlex™ Fiber (American Medical Systems, San Jose, CA, USA)
Stone phantom
BeGo (BEGO GmbH & Co. KG, Bremen, Germany)
Camera
Sony RX100 IV (Sony Corporation of America, NY, USA)
Experimental setup (A) schematic diagram; (B) 3D rendering of the setup.
The speed at which the phantom moves vertically during the laser stone encounter is used to calculate the retropulsion. The setup’s camera is a Sony RX100 IV, which can record the laser stone interaction video at 1000 frames per second. A MATLAB software is then used to process the footage.
Design-Expert® created the experiment with laser pulse energies of 0.2, 0.4, 0.6, 0.8, 1.2, and 1.5 J with frequencies of 5, 10, 15, 20, 30, and 40 Hz. with two replicate points, two lack-of-fit points, and randomized optimal (custom). The laser stone interaction test had a sample size of 14 and lasted 15 seconds for each laser setting. A P-value of 5% or less was regarded as statistically significant for all paired t-tests, which were all two-tailed tests.
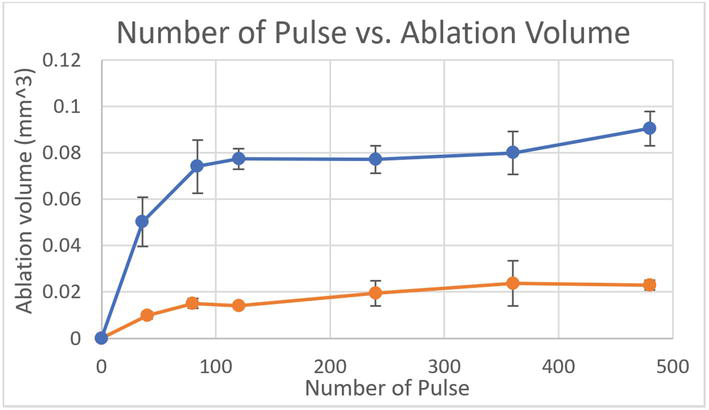
With fixed fiber and stone phantom, the laser-induced crater size will saturate after certain numbers of laser pulses due to the rapid decrease of laser ablation efficiency when the gap between the fiber tip and the stone increases. Figure 5 is the crater volume saturation curve by two laser settings; each data point is the average of three measurements. The saturation happens after ~80 pulses.
Figure 5.
Saturation point evaluation by laser 1 at 0.2 J 10 Hz (orange color curve) and laser 2 at 0.3 J 12 Hz (blue color curve).
3.1.2 Laser stone ablation threshold analysis
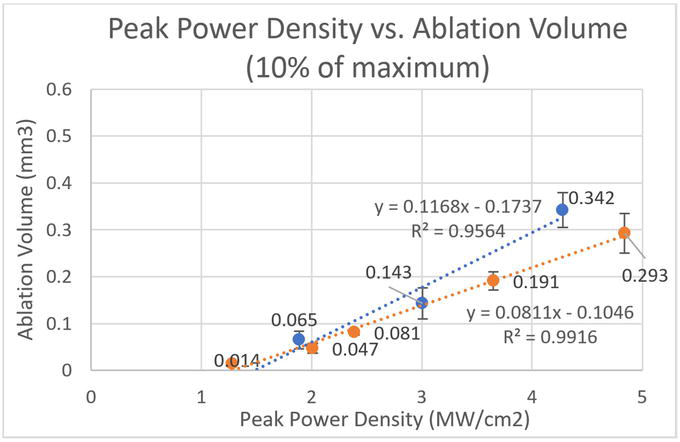
Figure 6 is laser stone ablation volume analysis curve by two laser types verses laser peak power density using pulse width definition of full width and 10% maximum (FW10%M). From the curves, we can calculate the laser ablation threshold in terms of peak power density is ~1.3 MW/cm2 for laser 1, and ~ 1.5 MW/cm2 for laser 2.
Figure 6.
The laser stone ablation volume analysis curve by two laser types (laser 1 in orange, and laser 2 in blue) versus laser peak power density using pulse width definition of full width and 10% maximum (FW10%M).
3.2 Transient pressure field measurement
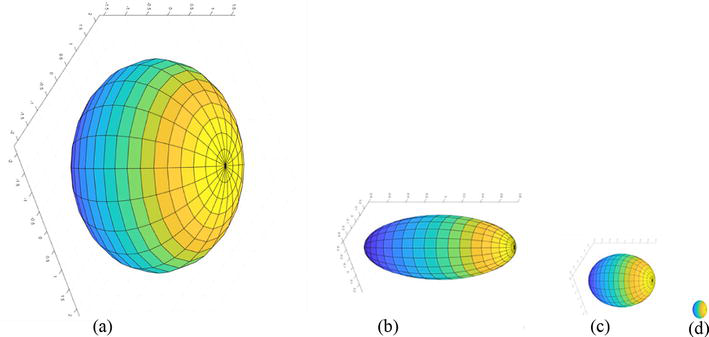
For all of the measurements of transient pressure spikes, we employed the HNR-0500 hydrophone (the optical hydrophone was not suitable for this laser generated bubble transient measurement due to the optical effect of the bubble and its relative lower sensitivity). The majority of the spectral content is anticipated to be contained within 1 MHz, according to the Fourier Transform Analysis. The peak spectrum value can be used to calibrate the hydrophone’s sensitivity. The measurement findings in terms of MPa are shown in Tables 3 and 4. Examples of the Transient Pressure Field Ellipsoids are shown in Figure 7.
Analysis of variance (ANOVA) of the tested data points, each of which represents the average of 14 measurements, is used by Design-Expert® to produce the response surfaces [55, 56]. The precise analytical formula for retropulsion and ablation in the optimal dusting mode is:
The laser ablation threshold in terms of peak power density is a critical reference for laser lithotripsy efficacy. The lithotripsy laser peak power density needs to be more than the laser ablation threshold. Since it is a parameter of density, the laser delivery fiber also has a play. For a 365 μm core fiber, the laser peak power threshold is ~1.3 kW, and for a 230 μm core fiber, the peak power density threshold is ~0.5 kW, which is around the max peak power level of a commercially available Thulium fiber laser on the current market. Therefore, the current commercially available Thulium fiber laser may have a hard time breaking harder stones like brushite or calcium oxalate. And it can be mitigated by using a smaller core laser beam delivery fiber.
4.2 Transient pressure field measurement and retropulsion control
For stone retropulsion, peak power has a greater impact coefficient [58]. We must limit the transient pressure by lowering the peak power in order to reduce retropulsion while still exceeding the ablation threshold. The prototype Smart Modes’ pulse modulation already contributes to this in several ways.
Our comprehension of the dynamic laser stone interaction during surgery is improved by bubble dynamics. A commercial Ho:YAG laser’s bubble dynamics, including bubble size, shape, and energy delivery distance, were previously compared to those of the prototype laser. Table 5 presents an overview of the information.
Power (W)
10
20
30
40
Optimal dusting mode
1 J 10 Hz
1 J 20 Hz
1 J 30 Hz
1 J 40 Hz
Referene dusting mode
0.25 J 40 Hz
0.5 J 40 Hz
0.6 J 50 Hz
0.8 J 50 Hz
Table 5.
The laser settings between the optimal dusting mode and dusting mode of the reference laser.
The speed of the laser energy injection is controlled by the laser pulse packet width. Except for the 0.5 J pulse, the prototype laser-generated bubble typically has an elongated form and is significantly smaller in height than the reference laser [59]. The lower transient pressure measurement result can be explained by the lesser height at 3 J compared to 2 J.
The spherical form of the 0.5 J bubble can be used to explain why the transient pressure value of the prototype laser’s standard short mode at 0.5 J is greater than those of 1–3 J pulses. Due to its omnidirectional structure, the pressure peak at the bubble’s collapse is very high. The vapor bubble’s elongated/elliptical/rod shape at 1–3 J (caused by pulse modulation) disrupts the bubble’s symmetry and lowers the transient peak pressure at the collapse.
A commercial Ho:YAG laser produces correspondingly huge vapor bubbles thanks to its high peak power and high energy pulses. Due to the omnidirectional nature of the vapor bubbles, a large portion of the energy injected is lost and not used for stone ablation. Longer water penetration tunnels and more focused vapor bubbles are produced by the prototype laser’s Smart Modes. In non-contact laser lithotripsy treatments, dusting with a narrow and lengthy vapor bubble has the potential to increase efficiency by delivering the laser pulse farther.
4.3 The optimal dusting mode
The majority (>75%) of urinary tract calculi are thought to be calcium oxalate or mixed forms with calcium phosphate nuclei [60]. These most frequent stones are mostly caused by Randall plaques, which act as accretion sites and, thus, as a favored accumulation zone (seed) for precipitated solutes [61, 62, 63, 64, 65, 66]. Urinary stones are known to have 100 different chemical components [5, 67]. The optimal lithotripsy laser dosimetry (setting), according to Sea J et al., relies on the particular case circumstance (calculus type, size, location, etc.), as well as the desired result [68]. There is not “one” optimal laser setting for URS, for this reason.
We must first specify the common laser parameters (power, energy, and frequency) used for URS in order to do our data analysis. Lower pulse energy (as low as 0.2 J) with a higher frequency is ideal for dusting needs since it produces significantly less retropulsion and smaller debris/remains [69]. High-power holmium settings (up to 40 W) fired in prolonged bursts with insufficient irrigation flow rates can result in high fluid temperatures in a laboratory “caliceal” model, despite the fact that higher power Ho:YAG lasers of up to 120 W are available for URS and the ablation rate is proportional to the laser power [70]. Higher irrigation flow rates, intermittent laser activation, and possibly chilled irrigation fluid are just a few of the ways urologists can control and reduce thermal effects now that they are aware of this risk [70].
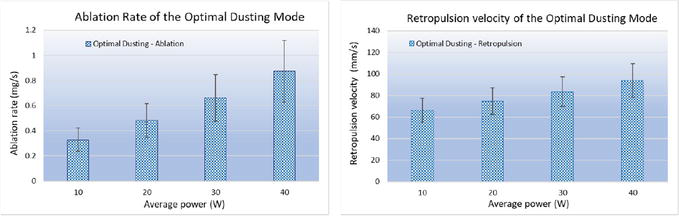
The laser settings for the optimal dusting mode and the reference laser’s dusting mode are listed in Table 5. The optimal dusting mode has a frequency range of 10–40 Hz and an energy level of 1 J. Use 40 or 50 Hz and low energy to calculate the average power level for the reference dusting mode.
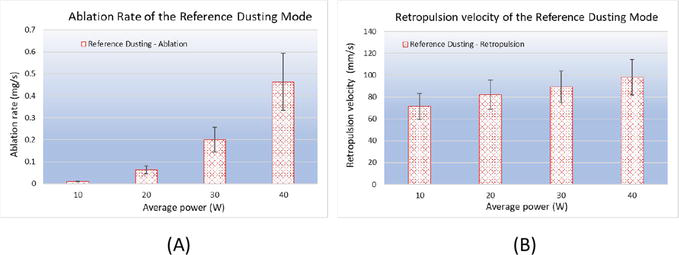
The dusting modes of the reference laser and the prototype laser’s ablation rate and retropulsion velocity are summarized in Figures 8 and 9. The average laser power is inversely correlated with the retropulsion velocity and ablation rate. The retropulsion velocity is more variable than the ablation rate, with a standard deviation that is 28% higher. The absolute value of the ablation rate will be lower than in studies with fixed fiber to stone distance [43, 54, 71, 72] since the stone phantom was not fixed during the test. Despite the drawbacks of (1) a reduced ablation rate due to stone movement; (2) retropulsion is a velocity that depends on the size of the phantom; the relative differences of the ablation rate and retropulsion velocity between the various laser modes are comparable. The optimal dusting setting in this benchtop test model maintains a modest retropulsion while having a somewhat quick ablation rate.
Figure 8.
Laser stone interaction results of the reference laser dusting mode. (A) Ablation rate vs. power; (B) retropulsion velocity vs. power.
Figure 9.
Laser stone interaction results of the prototype laser dusting mode. (A) Ablation rate vs. power; (B) retropulsion velocity vs. power.
In this chapter, we first measured the laser ablation threshold in terms of peak power density for the Bego stone phantom (15:3) was ~1.3 MW/cm2. This is a critical reference for laser lithotripsy efficacy. Then we studied the transient pressure of the laser pulse in water. The study showed that the optical hydrophone’s reduced sensitivity and distorted signal caused by the laser’s generated vapor bubble make it ineffective for sensing laser-induced transient pressure in water. Mechanical hydrophones were used to measure and create the transient pressure field profiles. With the hydrophone ~10 mm away from the fiber tip, the reference laser’s maximum transient pressure was 5.4 MPa and the prototype laser’s was 2.9 MPa. The Standard mode of the prototype laser has the highest transient pressure, which is followed by the Fragmenting and Dusting modes.
In order to efficiently use laser energy to improve ablation efficiency with less retropulsion, we consider the ablation efficiency related to the laser ablation threshold and lower the transient pressure for retropulsion control. The optimal dusting setting with the custom pulse modulation technology in the benchtop test model maintains a modest retropulsion while having a quick ablation rate. All these studies’ findings provide insights into future laser design to improve the efficiency, quality, and safety of lithotripsy procedures.
The authors thank the colleagues of Boston Scientific Corporation: Caroline Brial, Manjula Patel, John Goncalves, John Subasic, Jim Sarna, and Manuel Teixeira, Dongyul Chai, Gitanjali Multani, Brian Cheng, Xirong Yang, Baocheng Yang, David Jebbens, Ari Schwartz, Tram Vo, Trinh Pham, and Jasmine Cancino for laser test data gathering; Sean Curran, and Nicholas Nimchuk for their help on getting the software license of the Design-Expert® (DX10), as well as experimental data analysis, fitting, and optimization; and Sam Howard of Onda Corp. for setup and calibration of the hydrophones.
The opinions expressed in this book chapter are solely those of the author and not necessarily those of Boston Scientific Corporation (BSC). BSC does not guarantee the accuracy or reliability of the information provided herein.
References
1.Scales CD Jr, Smith AC, Hanley JM, Saigal CS. Urologic diseases in America project. Prevalence of kidney stones in the United States. European Urology. 2012;62(1):160-165. DOI: 10.1016/j.eururo.2012.03.052
2.AUA annual census. Practicing Urologists in the United States 2022 [Internet]. 2023. Available from: https://www.AUAnet.org/common/pdf/research/census/State-Urology-Workforce-Practice-US.pdf [Accessed: August 31, 2023]
3.Yang C, Li S, Cui Y. Comparison of YAG laser lithotripsy and extracorporeal shock wave lithotripsy in treatment of ureteral calculi: A meta-analysis. Urologia Internationalis. 2017;98:373-381
4.Bader MJ, Pongratz T, Khoder W, Stief CG, Herrmann T, Nagele U, et al. Impact of pulse duration on Ho:YAG laser lithotripsy: Fragmentation and dusting performance. World Journal of Urology. 2015;33:471-477
5.Graham A, Luber S, Wolfson AB. Urolithiasis in the emergency department. Emergency Medicine Clinics of North America. 2011;29(3):519-538
6.Türk C, Neisius A, Petřík A, Seitz C, Thomas K, Skolarikos A. EAU guidelines on urolithiasis 2018. In: European Association of Urology Guidelines. Presented at the EAU Annual Congress, Copenhagen. 2018th ed. Arnhem, The Netherlands: The European Association of Urology Guidelines Office; 2018
7.Matlaga BR, Jansen JP, Meckley LM, Byrne TW, Lingeman JE. Economic outcomes of treatment for ureteral and renal stones: A systematic literature review. The Journal of Urology. 2012;188(8):449-454
8.Rizvi SAH, Naqvi SAA, Hussain Z, Hashmi A, Hussain M, Zafar MN, et al. The management of stone disease. BJU International. 2002;89(Suppl. 1):62-68
9.Tiselius HG. Epidemiology and medical management of stone disease. BJU International. 2003;91:758-767
10.Scales CD Jr. Practice patterns in the management of urinary lithiasis. Current Urology Reports. 2013;14:154-157
11.Turney BW, Reynard JM. The cost of stone surgery. European Urology. 2014;66:730-731
12.Antonelli JA, Maalouf NM, Pearle MS, Lotan Y. Use of the National Health and Nutrition Examination Survey to calculate the impact of obesity and diabetes on cost and prevalence of urolithiasis in 2030. European Urology. 2014;66:724-729
13.Pearle MS, Calhoun EA, Curhan GC. Urologic diseases of America project. Urologic diseases in America project: Urolithiasis. The Journal of Urology. 2005;173(3):848-857
14.Seklehner S, Laudano MA, del Pizzo J, Chughtai B, Lee RK. Renal calculi: Trends in the utilization of shock-wave lithotripsy and ureteroscopy. The Canadian Journal of Urology. 2015;22(1):7627-7634
15.Maiman TH. Ruby Laser Systems. US Patent 3,353,115. 1967
16.Mulvaney WP, Beck CW. The laser beam in urology. The Journal of Urology. 1968;99:112-115
17.Watson G, Smith N. Comparison of the pulsed dye and holmium lasers for stone fragmentation: In-vitro studies and clinical experience. Proceedings of SPIE. 1993;1879:139-142
18.Tischer C, Koort HJ, Bazo A, Rasch R, Thiede C. Clinical experiences with a new frequency-doubled doublepulse Nd:YAG laser (FREDDY) for the treatment of urolithiasis. Proceedings of SPIE. 2002;4609:128-135
19.Sayer J, Johnson DE, Price RE, Cromeens DM. Endoscopic laser fragmentation of ureteral calculi using the holmium:YAG. Proceedings of SPIE. 1993;1879:143-148
20.Grasso M, Chalik Y. Principles and applications of laser lithotripsy: Experience with the holmium laser lithotrite. Journal of Clinical Laser Medicine & Surgery. 1998;16(1):3-7
21.Marguet CG, Sung JC, Springhart WP, L’esperance JO, Zhou SL, Zhong P, et al. In vitro comparison of stone retropulsion and fragmentation of the frequency doubled, double pulse Nd:YAG laser and the holmium:YAG laser. The Journal of Urology. 2005;173(5):1797-1800
22.Marks AJ, Teichman JMH. Lasers in clinical urology: State of the art and new horizons. World Journal of Urology. 2007;25(3):227-233
23.Jansen ED, van Leeuwen TG, Motamedi M, Borst C, Welch AJ. Temperature dependence of the absorption coefficient of water for midinfrared laser radiation. Lasers in Surgery and Medicine. 1994;14(3):258-268
24.Teichman JMH, Vassar GJ, Glickman RD. Holmium: Yttrium-aluminum-garnet lithotripsy efficiency varies with stone composition. Urology. 1998;52(3):392-397
25.Grasso M. Experience with the holmium laser as an endoscopic lithotrite. Urology. 1996;48(2):199-206
26.Chan KF, Vassar GJ, Pfefer TJ, et al. Holmium:YAG laser lithotripsy: A dominant photothermal ablative mechanism with chemical decomposition of urinary calculi. Lasers in Surgery and Medicine. 1999;25(1):22-37
27.Pierre S, Preminger GM. Holmium laser for stone management. World Journal of Urology. 2007;25(3):235-239
28.Teichman JMH, Rogenes VJ, McIver BJ, Harris JM. Holmium:Yttrium-aluminum-garnet laser cystolithotripsy of large bladder calculi. Urology. 1997;50(1):44-48
29.Fried NM, Irby PB. Advances in laser technology and fiberoptic delivery systems in lithotripsy. Nature Reviews Urology. 2018;15:563-573
30.Traxer O, Keller EX. Thulium fiber laser: The new player for kidney stone treatment? A comparison with holmium:YAG laser. World Journal of Urology. 2020;38(8):1883-1894
31.Frenz M, Zweig AD, Romano V, Weber HP. Dynamics in laser cutting of soft media. Proceedings of SPIE. 1990;1202:22-33
32.Niemz M. Laser-Tissue Interactions–Fundamentals and Applications. 2nd ed. Leipzig, Germany: Springer; 2002. p. 72. ISSN 1618-7210. ISBN 3-540-42763-5
33.Rajabhandharaks D, Zhang JJ, Wang H, Xuan JR, Chia RWJ, Hasenberg T, et al. Dependence of water content in calculus phantom during Q-switched Tm:YAG laser lithotripsy. In: Proc. SPIE 8565, Photonic Therapeutics and Diagnostics IX. 2013. 856519. Available from: SPIEDigitalLibrary.org
34.Rajabhandharaks D, Zhang JJ, Wang H, Xuan JR, Chia RWJ, Hasenberg T, et al. Water content contribution in calculus phantomablation during Q-switched Tm:YAG laser lithotripsy. Journal of Biomedical Optics. 2015;20(12):128001
35.Knipper S, Tiburtius C, Gross AJ, Netsch C. Is prolonged operation time a predictor for the occurrence of complications in ureteroscopy? Urologia Internationalis. 2015;95:33-37
36.Aldoukhi AH, Hall TL, Ghani KR, Roberts WW. Strike rate: Analysis of laser fiber to stone distance during different modes of laser lithotripsy. Journal of Endourology. 2021;35:355-359
37.Teng P, Nishioka N, Anderson RR, et al. Mechanisms of Laser-Induced Stone Ablation. In: Proc. SPIE 0712, Lasers in Medicine; 1987. p. 5. Available from: SPIEDigitalLibrary.org
38.Thomas S, Pensel J, Engelhardt R, et al. The pulsed dye laser versus the Q-switched Nd:YAG laser in laser-induced shock-wave lithotripsy. Lasers in Surgery and Medicine. 1988;8(4):363-370. DOI: 10.1002/lsm.1900080405
39.Grasso M, Shalaby M, el Akkad M, et al. Techniques in endoscopic lithotripsy using pulsed dye laser. Urology. 1991;37(2):138-144. DOI: 10.1016/0090-4295(91)80210-X
40.Bolton DM, Peters JS, Costello AJ. Experience with the pulsed dye laser in management of ureteric calculi. The Australian and New Zealand Journal of Surgery. 1992;62(10):788-790. DOI: 10.1111/j.1445-2197.1992.tb06919.x
41.Finley DS, Petersen J, Abdelshehid C, et al. Effect of holmium:YAG laser pulse width on lithotripsy retropulsion in vitro. Journal of Endourology. 2005;19(8):1041-1044. DOI: 10.1089/end.2005.19.1041
42.Kamal W, Kallidonis P, Koukiou G, et al. Stone retropulsion with Ho: YAG and Tm: YAG lasers: A clinical practice-oriented experimental study. Journal of Endourology. 2016;30(11):1145-1149. DOI: 10.1089/end.2016.0212
43.Wollin DA, Ackerman A, Yang C, et al. Variable pulse duration from a new holmium:YAG laser: The effect on stone comminution, fiber tip degradation, and retropulsion in a dusting model. Urology. 2017;103:47-51. DOI: 10.1016/j.urology.2017.01.007
45.Chai DY, Zhang JJ, Podana N, Xuan RJ, Hasenberg T, Harrah T. The study of Ho: YAG laser ablation thresholds of calculus phantom in terms of peak power density. In: Proc. SPIE 10852, Therapeutics and Diagnostics in Urology. 2019. 108520D. Available from: SPIEDigitalLibrary.org
46.Esch E, Simmons WN, Sankin G, Cocks HF, Preminger GM, Zhong P. A simple method for fabricating artificial kidney stones of different physical properties. Urological Research. 2010;38(4):315-319
47.Eisel M, Strobl S, Pongratz T, Strittmatter F, Sroka R. In vitro investigations of propulsion during laser lithotripsy using video tracking. Lasers in Surgery and Medicine. 2018;50:333-339
48.Eisel M, Strobl S, Pongratz T, Strittmatter F, Sroka R. Holmium:Yttrium-aluminum-garnet laser induced lithotripsy: In-vitro investigations on fragmentation, dusting, propulsion and fluorescence. Biomedical Optics Express. 2018;9(11):5115
49.Zhang JJ, Rajabhandharaks D, Xuan RJ, Chia RWJ, Hasenberg TC. Characterization of calculus migration during Ho:YAG laser lithotripsy by high speed camera using suspended pendulum method. In: Proc. SPIE 8926, Photonic Therapeutics and Diagnostics X. 2014. 89261I-1-7. Available from: SPIEDigitalLibrary.org
50.Kronenberg P, Traxer O. Update on lasers in urology 2014: Current assessment on holmium:Yttrium–aluminum–garnet (Ho:YAG) laser lithotripter settings and laser fibers. World Journal of Urology. 2015;33:463-469
51.Hutchens TC, Gonzalez DA, Irby PB, Fried NM. Fiber optic muzzle brake tip for reducing fiber burnback and stone retropulsion during thulium fiber laser lithotripsy. Journal of Biomedical Optics. 2017;22(1):18001
52.Sroka R, Haseke N, Pongratz T, Hecht V, Tilki D, Stief CG, et al. In vitro investigations of repulsion during laser lithotripsy using a pendulum setup. Lasers in Medical Science. 2012;27:637
53.Zhang JJ, Rajabhandharaks D, Xuan RJ, Chia RWJ, Hasenberg TC. Calculus migration characterization during Ho:YAG laser lithotripsy by high-speed camera using suspended pendulum method. Lasers in Medical Science. 2017;32:1017-1021
54.Kronenberg P, Traxer O. In vitro fragmentation efficiency of holmium: Yttrium–aluminum–garnet (YAG) laser lithotripsy: A comprehensive study encompassing different frequencies, pulse energies, total power levels and laser fibre diameters. BJU International. 2014;114(2):261-267
55.Zhang JJ, Rutherford J, Solomon M, Cheng B, Xuan RJ, Gong J, et al. Numerical response surfaces of volume of ablation and retropulsion amplitude by settings of Ho:YAG laser lithotripter. Journal of Healthcare Engineering. 2018;2018:8261801. DOI: 10.1155/2018/8261801, 11 pages
56.Zhang JJ, Rutherford J, Solomon M, Cheng B, Xuan JR, Gong J, et al. The study of laser pulse width on efficiency of Ho:YAG laser lithotripsy. In: Proc. SPIE 10038, Photonic Therapeutics and Diagnostics XIII. 2017. pp. 1-7. Available from: SPIEDigitalLibrary.org
57.Zhang JJ, Chai D, Xuan RJ, Ray A, Hasenberg TC, Harrah T. In search of optimal settings for Ho:YAG laser lithotripsy to maximize the ablation rate, while minimizing the retropulsion. In: Proc. SPIE 11212, Therapeutics and Diagnostics in Urology. 2020. 1121204. Available from: SPIEDigitalLibrary.org
58.Zhang JJ. In search of optimal laser settings for lithotripsy by numerical response surfaces of ablation and retropulsion. In: Kayaroganam P, editor. Response Surface Methodology in Engineering Science. London, United Kingdom. 2021. Online ISBN: 978-1-83968-918-5, Print ISBN: 978-953-51 3459 6 (Aug 23, 2021). DOI: 10.5772/intechopen.96271
59.Zhang JJ, Xuan JR, Yu H, Devincentis D. Study of cavitation bubble dynamics during Ho:YAG laser lithotripsy by high-speed camera. Proceedings of SPIE. 2016;9689:E-1-E-7
60.Chan KF, Pfefer TJ, Teichman JMH, Welch AJ. A perspective on laser lithotripsy: The fragmentation processes. Journal of Endourology. 2001;15(3):257-273
61.Coe FL, Evan AP, Worcester EM, Lingeman JE. Three pathways for human kidney stone formation. Urological Research. 2010;38:147-160
62.Kuo RL, Lingeman JE, Evan AP, Paterson RF, Parks JH, Bledsoe SB, et al. Urine calcium and volume predict coverage of renal papilla by Randall's plaque. Kidney International. 2003;64:2150-2154
63.Kim SC, Coe FL, Tinmouth WW, Kuo RL, Paterson RF, Parks JH, et al. Stone formation is proportional to papillary surface coverage by Randall's plaque. The Journal of Urology. 2005;173:117-119
64.Miller NL, Gillen DL, Williams JC Jr, Evan AP, Bledsoe SB, Coe FL, et al. A formal test of the hypothesis that idiopathic calcium oxalate stones grow on Randall's plaque. BJU International. 2009;103:966-971
65.Miller NL, Williams JC Jr, Evan AP, Bledsoe SB, Coe FL, Worcester EM, et al. In idiopathic calcium oxalate stone-formers, unattached stones show evidence of having originated as attached stones on Randall's plaque. BJU International. 2010;105:242-245
66.Low RK, Stoller ML. Endoscopic mapping of renal papillae for Randall's plaques in patients with urinary stone disease. The Journal of Urology. 1997;158:2062-2064
67.Khan A. Prevalence, pathophysiological mechanisms and factors affecting urolithiasis. International Urology and Nephrology. 2018;50:799-806
68.Sea J, Jonat LM, Chew BH, et al. Optimal power settings for holmium:YAG lithotripsy. The Journal of Urology. 2012;187(3):914-919
69.Aldoukhi AH, Roberts WW, Hall TL, Ghani KR. Holmium laser lithotripsy in the new stone age: Dust or bust? Frontiers in Surgery. 2017;4:57
70.Aldoukhi AH, Ghani KR, Hall TL, Roberts WW. Thermal response to high-power holmium laser lithotripsy. Journal of Endourology. 2017;31(12):1308-1312
71.Aldoukhi AH, Roberts WW, Hall TL, Ghani KR. Watch your distance: The role of laser fiber working distance on fragmentation when altering pulse width or modulation. Journal of Endourology. 2019;33(2):120-126. DOI: 10.1089/end.2018.0572
72.Elhilali MM, Badaan S, Ibrahim A, Andonian S. Use of the Moses technology to improve holmium laser lithotripsy outcomes: A preclinical study. Journal of Endourology. 2017;31(6):598-604
Written By
Jian James Zhang
Submitted: 14 July 2023Reviewed: 29 August 2023Published: 15 November 2023
 Open access peer-reviewed chapter
Open access peer-reviewed chapter