 Open access peer-reviewed chapter
Open access peer-reviewed chapter
Abstract
Current technology has improved the modalities of intra-corporeal lithotripsy, including: ultrasound and ballistic, combined with different laser energies useful in the most important procedures for resolving urinary system stones. Nowadays, the amount of lasers and their availability has grown considerably, lasers like Holmium:Yttrium-Aluminum-Garnet (Ho:YAG) and Thulium Fiber Laser (TFL) are the most effective and safest alternatives for lithotripsy in several types of endo urological strategies for lithotripsy. The selection of appropriate laser energy is crucial to optimize the usefulness in the management of urinary tract stones and it depends on the clinical indications validated for the International Urolithiasis Alliance based in technology but also in principles of management from the reported outcomes based in the expertise of several endo urological surgeons. Both, Ho:YAG laser and TFL are effective systems of fragmentation in retrograde intrarenal surgery (RIRS) and percutaneous nephrolitotomy (PNL), even in the miniaturized percutaneous tracts enhanced with suction. Comparative with other types of lithotripsy, they have the same stone-free rates, low complication indexes, and optimal surgical operative times. Urologists must be familiar of with the properties of each laser to get the best surgical outcomes for the benefits of their patients. The present chapter will describe the clinical indications and the adequate use of laser fibers.
Keywords
- lithotripsy
- laser
- holmium
- Thulium
- intra renal surgery
1. Introduction
Urolithiasis is the more often benign pathology in urology. Its incidence can be higher in some specific climes and countries. Nowadays there is an increase in innovations and technology for the treatment of kidney stones. Lithotripsy is a minimally invasive procedure used to treat calculi localized in the urinary tract like the kidney, the ureter, and the bladder, those stones need different management to be treated basically with some principles according to several factors like size, localization. Lithotripsy actually has some elements and different technical aspects, and technologies like the administration of energy directly to the stone in order to get fragmentation or dusting of the calculi to free the urinary tract from them [1, 2].
Urologists account for several modalities of intracorporeal lithotripsy, including: ultrasound, ballistic, combined, and laser energy useful in the most important treatments of stone diseases. Some approaches are percutaneous nephrolithotomy (PNL) and retrograde intrarenal surgery (RIRS). More recently, in the context of complex or Staghorn calculi, we have a new approach that mix both techniques named endoscopic combined intrarenal surgery (ECIRS) [3, 4].
However, this has been the most widely used option for intracorporeal management of urinary calculi due to its effectiveness regardless of the stone composition and its high lithiasic clearance capacity, therefore is a growing interest in the development of new laser energies [5, 6, 7, 8].
Laser energies in recent years have offerred very new modalities. Thulium laser which has exceptional results in stone fragmentation and seems to be promising given that it offers good clinical results compared to Ho:YAG laser [9, 10, 11].
2. Laser lithotripsy types
In the modern era of lithotripsy, we have two effective modalities for stone clearance. These are Holmium laser and Thulium laser, which are the result of technological development in order to improve efficiency and safety [9].
2.1 Holmium:YAG
The Holmium:YAG is the most used laser for lithotripsy. This conventional laser can be used for retrograde intrarenal surgery. When used as a high-power laser in RIRS could be associated with a decrease in the operating room time and a higher Stone Free Rate (SFR) specifically when compared to the lower-power devices.
When it is used with lower frequency and a combination of higher energy and shorter pulse duration again higher frequency, lower energy, and longer pulse duration, the improvement reflects an ability to generate dusting.
The Holmium laser is a well-defined and extensively source of energy for lithotripsy. It has an excellent capability of fragmentation instead of stone type and density, and its low tissue penetration allow a good safety margin for surrounding tissue and a low thermal effect for the contiguous epithelium. Several studies, including meta-analysis, had not demonstrated differences between stone-free rates compared with Thulium Fiber Laser and the postoperative complications between both groups are very similar [12, 13, 14].
2.2 Tulium
The Tulium laser has become a relative new but effective technology and safe. It allows the use of high frequencies and reduction in the retropulsion offering efficiency in ablation. Both lasers need the urologist consideration to be aware of their thermal effects, as they also have adequate irrigation and working space.
The Thulium Fiber Laser is a recent innovative laser technology that seems particularly promising in stone treatment. There is a necessity of more studies to define the future of lithotripsy through the good results TFL is achieving [15].
Ho:YAG laser lithotripsy offers the same stone-free rates compared to other fragmentation modalities (ultrasonic, pneumatic, and combined) as it is highly effective in terms of fragmentation regardless of stone composition. In contrast, it requires more surgery because the stone clearance time is longer compared to other modalities. In the literature, a lower rate of complications associated with bleeding is reported with laser lithotripsy (Ho:YAG) compared with other fragmentation modalities [16].
So, the election between laser modalities will depend on the surgeon’s expertise and clinical setting, the continuous development of those, will offer a broad spectrum of lithotripsy modalities which will be a milestone in stone management [13].
3. Current indications
Current indications for intracorporeal lithotripsy are indistinct between laser energy used (Ho:YAG vs. Thulium). Even, in the management of urinary stones in children we have the same indications and energy applications.
There exist a global effort to standardize the clinical diagnosis and management of urinary tract stones. Several organizations, including the American Urological Association (AUA), European Association of Urology (EAU), and National Institute for Health and Care Excellence (NICE) have worked to enhance clinical guidelines for a better approach to urolithiasis [2, 4, 17].
Consider for asymptomatic renal stones in adults and children, watchful waiting (WW) approach if the stones are smaller than 5 mm and if the stone is larger than 5 mm but the patient or their family carers agrees to watchful waiting (WW) [16, 18].
4. In the case of symptomatic stones, consider the following approaches
4.1 Retrograde intrarenal surgery (RIRS)
Retrograde intrarenal surgery has been a very useful minimally invasive approach for ureteral stones. Some of the following are clinical indications according to the size stone. The proximal ureteral calculi with a diameter less than 20 mm (LE:1, GR:A), intra-renal calculi with a diameter less than 20 mm (LE:1, GR:A), intra-renal or ureteral calculi in the proximal third of the ureter greater than 20 mm when there is a contraindication for percutaneous nephrolithotomy (*LE:2, GR:B).
Retrograde surgery for intra-renal or proximal ureteral calculi with a diameter less than 20 mm with laser fragmentation offers better success rates in a single procedure and lower rates of reoperation compared with extracorporeal lithotripsy [2, 18].
4.2 Percutaneous nephrolithotomy (PNL)
Since the percutaneous nephrolithotomy was born in 1979. It came as an innovative and precise minimally invasive procedure for greater stone diameter and at the beginning for lower calix localization. The main indications are in the kidney stones with a diameter greater than or equal to 20 mm in diameter (*LE:1, GR:A), and for difficult access upper urinary tract calculi (*LE: 2, GR: B), those can include inferior caliceal location, infundibular narrowing, narrow infundibulum-pelvic angle, and anatomical renal abnormalities.
Percutaneous nephrolithotomy (PNL) is the treatment modality for calculi larger than 20 mm or staghorn calculi. In those cases in which the PNL has a failure the use of extracorporeal lithotripsy or intrarenal retrograde surgery is recommended (LE: 2, GR: B).
4.3 Endoscopic combined intrarenal surgery (ECIRS)
There is always the possibility of performing a combined endoscopic procedure, is necessary to consider if we are facing a calculi with complex configuration, greater than 2 cm, when: (*LE: 2, GR: B), in those cases where the NLPC is not feasible, and if retrograde intrarenal surgery as monotherapy is not enough.
The need for re-intervention due to the high stone volume or the high probability of residual stones after a single procedure is an indication for a combined approach [18] (Figures 1–3).
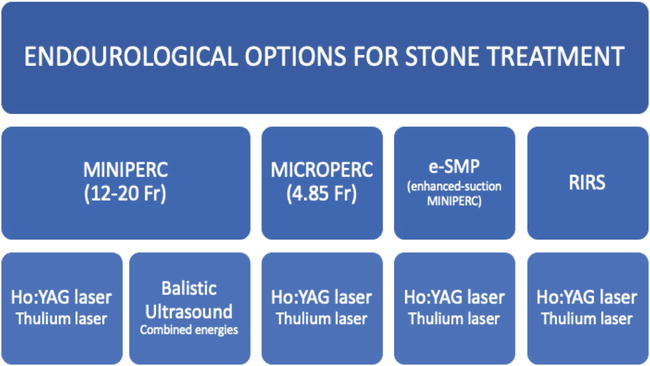
Figure 1.
Modalities of energy usefulness in different endourological approach to urinary tract stones. *LE, level of evidence; GR, grade recommendation.
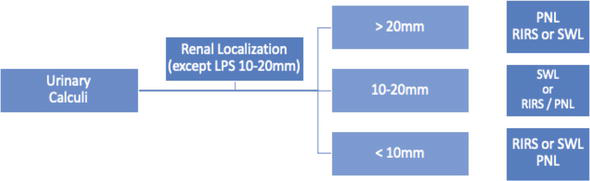
Figure 2.
Summary recommendations by international Urolithiasis Alliance for urinary tract stones considering size and location [
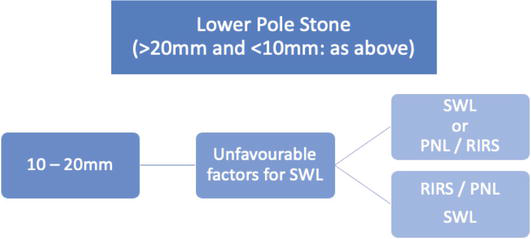
Figure 3.
Summary recommendations by international Urolithiasis Alliance for urinary tract stones considering size and location [
5. Complications
Associate complications to the RIRS procedures and to the use of lasers can be bleeding, ureteric perforation or avulsion, arterio-venous fistula, perirenal hematomas, infections.
The risk of bleeding when present is due to an injury generally self-limited or due to a perforation of the ureter or collecting system by insertion of fibers, guidewires, catheters creating a perforation or avulsion, special patient conditions like anticoagulation therapy or change in decompression after high intrarenal pressure.
Secondary to the use of energy lasers inadvertent thermal injury can also produce bleeding that generally is self-limited, however, wall injuries are properly described in the endoscopic classification system [19].
The main reasons to develop an infection are infection stone, size of burden stone, prolonged operating time, and forced irrigation, all of them can be prevented with adequate use of operative intrarenal pressure, shorter time of operation, proper antibiotic prophylaxis, and use of a Foley catheter.
Complications in PCNL have a bigger range in Clavien-Dindo classification, they are clearly lower with mini PCNL, the first is the bleeding present as hematuria according to not significant or even to avoid the proper view in the field, causing even incidence of transfusion or embolization can be required previous angiography control [16].
Describe risk factors for bleeding such as the urinary tract infection, infected stones, comorbidities as diabetes mellitus, associated to the puncture technique or anatomical aspects like lower kidneys or solitary kidney, and during the intervention as long operation time for the procedure.
Avoiding infections with adequate antibiotic previous therapy is required, in specific cases, a culture can be obtained intraoperative. The risk of a systemic inflammatory response syndrome (SIRS), urosepsis can be present, especially associated with the following risk factors preoperative positive urine test, recurrent infection, kind of stone as staghorn calculi, and during procedure associated to prolonged operative time and high renal pelvic pressure. Treatment must be implemented promptly and should be appropriate antibiotics, in some cases resuscitation support and intensive unit care maybe required.
Urinary extravasation occurs when a high intra-renal pressure is maintained, torquing the nephroscope, perforation of calyceal system clinically observed as abdominal distention, airway resistance and oxygen desaturation, considered to stop the procedure to place a nephrostomy and ureteral stent should be performed, an ultrasound evaluation to drain the peritoneal effusion by puncturing [16].
Injury to organs can be present according to the level of puncture, pleural, hydrothorax, hemothorax, pneumothorax a drainage tube could be necessary, liver or spleen are also probably present in supra-costal punctures, management can be conservative or urgent laparotomy’s.
Large bowel injury will be demonstrated by ultra-sonography guidance, CT scan or fistulography. The result will be an urgent laparotomy in front of an acute peritonitis, percutaneous colostomy, bowel rest, intravenous broad-spectrum, and parenteral nutrition will be recommended for the management [16].
6. Discussion
When and how to treat urinary stones depends on the size, location, and severity of the clinical manifestations.
It is important to remember that urinary calculi smaller than or equal to 4 mm with expulsive therapy in a period of 14–21 days, will achieve successful spontaneous passage in up to 80% of patients [2].
There are cases of asymptomatic renal ureteral lithiasis, according to current literature, up to 50% of them will develop some type of clinical manifestation within 5 years, so it is important to treat with the intention of preventing complications associated with them [1].
The need for intra-corporeal treatment has favored the development of laser technology for fragmentation or pulverization in situ. Over time, the modalities are becoming more efficient, safer, and accessible to the general population.
The advent of the Ho:YAG laser has favored better perioperative results in terms of stone-free rates and the number of procedures required for total stone clearance [7].
The characteristics of the laser fiber allow better synergy with flexible and semi-rigid ureteroscopes. The imminent need and trend for the miniaturization of percutaneous tracts will improve the development of better laser technologies to continue their usefulness in fragmentation matters [20, 21, 22].
Technology is now moving forward to develop laser innovations related to calculi fragmentation and pulverization: energy delivery systems, pulse and frequency applications, fiber quality and tip-shape novel designs, etc. Certainly, these innovations will contribute to the best endourological surgery performance to achieve better efficiency in the management of urinary tract stones [23].
The International Urolithiasis Alliance has a social commitment in order to create optimal clinical guidelines that will be actualized within an interval of two years because all the surgical systems, energies and devices development, etc. [16, 18].
7. Conclusions
We are in an era of a well-developed laser energies, which are capable of solving any kind of urinary stones. The clinical results demonstrate excellent stone-free rates after one procedure, a few necessities of re-intervention, safer procedures, and optimal operative times.
The selection of appropriate laser energy is crucial to optimize the efficiency and safety during endourological procedures.
The Ho:YAG laser is the most effective system for flexible ureteroscopic lithotripsy and the most useful for fragmentation through miniaturized percutaneous tracts with suction.
The Thulium laser is a new fragmentation modality. Its versatility (high frequencies and low retropulsion) seems to offer a promising outlook, but studies are needed to confirm these advantages in terms of lithotripsy.
Urologists must be acquainted with the properties of each laser to get the best surgical outcomes for the benefit of our patients.
Acknowledgments
Thanks to collaborative group and special thanks to them who provided linguistic revision.
Nomenclature
percutaneous nephrolithotomy | |
retrograde intrarenal surgery | |
endoscopic combined intrarenal surgery | |
Holmium:Yttrium-Aluminum-Garnet | |
American Urological Association | |
European Association of Urology | |
National Institute for Health and Care Excellence | |
International Urolithiasis Alliance | |
watchful waiting | |
level of evidence | |
grade of recommendation | |
lower pole stone | |
Thulium Fiber Laser | |
systemic inflammatory response syndrome |
References
- 1.
Hughes T, Ho HC, Pietropaolo A, Somani BK. Guideline of guidelines for kidney and bladder stones. Turkish Journal of Urology. 2020; 46 (Suppl 1):S104-S112 - 2.
Türk C, Petřík A, Sarica K, Seitz C, Skolarikos A, Straub M, et al. EAU guidelines on diagnosis and conservative management of urolithiasis. European Journal of Urology. 2016; 69 (3):468-474 - 3.
EAU Guidelines on Diagnosis and Conservative Management of Urolithiasis – PubMed [Internet]. [citado 1 de junio de 2023]. Disponible en: https://pubmed.ncbi.nlm.nih.gov/26318710/ - 4.
Kidney Stones: Surgical Management Guideline – American Urological Association [Internet]. [citado 1 de junio de 2023]. Disponible en: https://www.auanet.org/guidelines-and-quality/guidelines/kidney-stones-surgical-management-guideline - 5.
Ashmawy A, Khedr M, Saad IR, Zamel S, Kassem A. Laser lithotripsy using dusting technique (low energy, high frequency) for symptomatic upper urinary tract stones. African Journal of Urology. 2021; 27 (1):155 - 6.
Strittmatter F, Eisel M, Brinkmann R, Cordes J, Lange B, Sroka R. Laser-induced lithotripsy: A review, insight into laboratory work, and lessons learned. Transl Biophotonics. 2020; 2 (1-2):e201900029 - 7.
Tzelves L, Somani B, Berdempes M, Markopoulos T, Skolarikos A. Basic and advanced technological evolution of laser lithotripsy over the past decade: An educational review by the European Society of Urotechnology Section of the European Association of Urology. Turkish Journal of Urology. 2021; 47 (3):183-192 - 8.
Laser Lithotripsy – an overview | ScienceDirect Topics [Internet]. [citado 1 de junio de 2023]. Disponible en: https://www.sciencedirect.com/topics/medicine-and-dentistry/laser-lithotripsy - 9.
Denstedt J, Gabrigna Berto FC. Thulium fiber laser lithotripsy: Is it living up to the hype? Asian Journal of Urology. 2022; 2022 :S2214 - 10.
Gonzalez-Cuenca E, Razvi H. Thulium fiber laser: Game changer or marketing hype? Revista Mexicana de Urología. 2023; 2023 :83. Disponible en:https://revistamexicanadeurologia.org.mx/index.php/rmu/article/view/1013 - 11.
Ryan JR, Nguyen MH, Linscott JA, Nowicki SW, James E, Jumper BM, et al. Ureteroscopy with thulium fiber laser lithotripsy results in shorter operating times and large cost savings. World Journal of Urology. 2022; 40 (8):2077-2082 - 12.
Kim HJ, Ghani KR. Which is the best laser for lithotripsy? Holmium laser. European Journal of Urology Open Science. 2022; 44 :27-29 - 13.
Liang H, Liang L, Yu Y, Huang B, Chen J, Wang C, et al. Thermal effect of holmium laser during ureteroscopic lithotripsy. BMC Urology. 2020; 20 (1):69 - 14.
Chua ME, Bobrowski A, Ahmad I, Kim JK, Silangcruz JM, Rickard M, et al. Thulium fibre laser vs holmium: Yttrium-aluminium-garnet laser lithotripsy for urolithiasis: meta-analysis of clinical studies. BJU International. 2023; 131 (4):383-394 - 15.
Ulvik O, Aesoy MS, Juliebo-Jones P, Gjengsto P, Beisland C. Thulium fibre laser versus holmium:YAG for Ureteroscopic lithotripsy: Outcomes from a prospective randomised clinical trial. European Urology. 2022; 82 (1):73-79 - 16.
Zeng G, Zhong W, Mazzon G, Choong S, Pearle M, Agrawal M, et al. International Alliance of Urolithiasis (IAU) Guideline on percutaneous nephrolithotomy. Minerva Urology and Nephrology. December 2022; 74 (6):653-668. DOI: 10.23736/S2724-6051.22.04752-8 - 17.
Singh A, Shah M, Hameed BMZ, Singh A, Shah M, Hameed BMZ. Guideline Based Algorithmic Approach for the Management of Renal and Ureteric Calculi. IntechOpen; 2022. Disponible en: https://www.intechopen.com/online-first/84098 - 18.
Zeng G, Traxer O, Zhong W, Osther P, Pearle MS, Preminger GM, et al. International Alliance of Urolithiasis guideline on retrograde intrarenal surgery. BJU International. 2023; 131 (2):153-164 - 19.
Traxer O, Thomas A. Prospective evaluation and classification of ureteral wall injuries resulting from insertion of a ureteral access sheath during retrograde intrarenal surgery. The Journal of Urology. 2013; 189 (580):4 - 20.
Gao X, Wang W, Peng L, Di X, Xiao K, Chen J, et al. Comparison of micro-percutaneous and mini-percutaneous nephrolithotomy in the treatment of renal stones: A systematic review and meta-analysis. Frontier in Surgery. 2021; 8 :743017 - 21.
Zhu W, Huang Z, Zeng G. Miniaturization in percutaneous nephrolithotomy: What is new? Asian J Urol [Internet]. 7 de febrero de 2023 [citado 31 de mayo de 2023]. 2023. Disponible en: https://www.sciencedirect.com/science/article/pii/S2214388223000243 - 22.
Ganpule AP, Vijayakumar M, Malpani A, Desai MR. Percutaneous nephrolithotomy (PCNL) a critical review. International Journal of Surgery. 2016; 36 :660-664 - 23.
Sabler IM, Katafigiotis I, Gofrit ON, Duvdevani M. Present indications and techniques of percutaneous nephrolithotomy: What the future holds? Asian Journal of Urology. 2018; 5 (4):287-294