Open Access is an initiative that aims to make scientific research freely available to all. To date our community has made over 100 million downloads. It’s based on principles of collaboration, unobstructed discovery, and, most importantly, scientific progression. As PhD students, we found it difficult to access the research we needed, so we decided to create a new Open Access publisher that levels the playing field for scientists across the world. How? By making research easy to access, and puts the academic needs of the researchers before the business interests of publishers.
We are a community of more than 103,000 authors and editors from 3,291 institutions spanning 160 countries, including Nobel Prize winners and some of the world’s most-cited researchers. Publishing on IntechOpen allows authors to earn citations and find new collaborators, meaning more people see your work not only from your own field of study, but from other related fields too.
To purchase hard copies of this book, please contact the representative in India:
CBS Publishers & Distributors Pvt. Ltd.
www.cbspd.com
|
customercare@cbspd.com
Each physiotherapist carries the ethical duty to practice in a holistic manner, ensuring that treatment approaches are firmly grounded in the most up-to-date evidence. Consequently, the primary objective of this chapter is to provide a comprehensive exposition of the essential stages that physiotherapists ought to adhere to when addressing patients with deformities. Additionally, it seeks to empower physiotherapists by offering practical insights into formulating precise and pertinent queries during patient interactions. This includes effective strategies for sourcing and evaluating evidence, which can then be judiciously applied to inform optimal decisions regarding patient care and treatment strategies. Throughout the course of this chapter, I will illustrate these concepts through the lens of a stroke patient scenario, facilitating a more accessible grasp of the material. However, it is crucial to note that the insights and instances presented within this chapter possess applicability that extends to various other neurological conditions within the domain of physiotherapy.
Federal Medical Centre, Nguru, Yobe State, Nigeria
*Address all correspondence to: ibrahimcsskd@gmail.com
1. Introduction
1.1 Meaning of evidence based practice
Evidence-based practice (EBP) holds a crucial role in the fields of rehabilitation and physiotherapy, progressively gaining significance. EBP is defined as the dedicated use of the most reliable evidence available to guide decisions regarding individual management, involving a fusion of clinical expertise, professional judgment, and systematic research [1]. Sackett et al. [2] further refined the concept, describing it as the fusion of top-tier research evidence, clinical proficiency, and patient preferences. The National Institute of Public Health (NIPH) in 1996 characterized evidence-based as the latest credible facts derived from pertinent, valid research. These encompass the effects of healthcare approaches, potential treatment risks, diagnostic precision, and prognostic foresight [3].
In essence, evidence-based practice in physiotherapy encompasses a methodical process of locating, evaluating, and applying current preeminent evidence to guide clinical actions. Practicing evidence-based physiotherapy involves integrating contemporary research findings with clinical skill and patient values, resulting in the most pertinent and effective care [4]. Despite its evident benefits in physiotherapy and broader healthcare, the adoption of EBP remains inconsistent in terms of quality [5]. Researchers and clinicians have voiced concerns about the compatibility of EBP elements and the scarcity of relevant, substantiated research [6, 7]. Bridging the gap between research and clinical insights can heighten the competence of physiotherapists’ practice [8], guarding against inappropriate healthcare utilization [9].
Given the rising accountability of healthcare professionals, including physiotherapists, this framework gains significance as a guiding principle. Some argue that a moral obligation exists for practitioners to base decisions on research findings [7]. Physiotherapists can enhance patient management outcomes by integrating three distinct forms of evidence into their decision-making process.
1.1.1 Scientific research
Scientific research stems from rigorous hypothesis testing and observation, providing valuable experiential insights. When communicating research evidence to patients, it’s essential to use clear and straightforward language and encourage open-ended questions to ensure patient comprehension. Physiotherapists are responsible for identifying, evaluating, and summarizing research evidence pertinent to patient care.
1.1.2 Clinical expertise
Clinical expertise encompasses both implicit and explicit knowledge gained from experience in diagnosing, intervening, preventing, and predicting outcomes for patients with physical conditions. This knowledge is accumulated over time and contributes to refining patient care.
1.1.3 Patient values
The foundation of decision-making and management lies within the caregivers, patient relatives, and the patients themselves. Patient values can be categorized as values and circumstances. Values include the patient’s beliefs, preferences, expectations, and cultural identity, which significantly influence their life choices and decisions [10].
In the original framework (depicted in Figure 1 above), to summarize, the most reliable evidence often emerges from clinically significant research carried out with robust methodological procedures. Clinical expertise encompasses the amassed knowledge, experience, and clinical skills of the Physiotherapist. Patient values encompass the distinct preferences, concerns, and expectations that each patient brings when engaging in a clinical interaction. The integration of these three elements constitutes the foundation of making evidence-based clinical decisions [11].
The primary goal is to empower healthcare professionals, including Physiotherapists, to make well-considered choices regarding clinical practice by employing the ‘thoughtful, clear, and prudent utilization of the most current and reliable evidence within the healthcare system’ [11].
In their work [12], a set of six stages outlining evidence-based practice was delineated. Physiotherapists are advised to adhere to these stages in order to provide optimal care for their patients (Figure 2).
Figure 2.
Stages of EBP.
3.1 How to formulate a clear and answerable clinical question
The time allocated for assessment and diagnosis in a clinic is often limited for a Physiotherapist. As a result, efficiently searching for the most suitable available evidence requires mastering the skill of formulating well-structured questions within a short timeframe. Questions posed by a Physiotherapist to their patients can be categorized into these groups [11]:
Etiology: How can I identify potential causes of a problem? For instance, what leads to limited shoulder range of motion among stroke survivors?
Assessment/Diagnosis: What crucial information should I collect? How can I obtain that information and correctly interpret the results? For example, what’s the optimal method for evaluating balance in stroke patients?
Treatment: Which intervention or procedure will be most beneficial for my patient? For instance, what are the outcomes of applying the Proprioception Neuromuscular Facilitation concept in post-stroke patients compared to other physiotherapy approaches?
Prognosis: What’s the recovery pattern over time and what potential complications might arise? As an illustration, if my patient had a stroke two months ago, when can they expect to regain independent walking ability?
Prevention: How can I avert emerging problems and enhance my patient’s well-being? As an example, what’s the most effective approach to prevent shoulder pain in post-stroke patients?
Differential diagnosis: When symptoms point to various potential diagnoses, how do I determine the most probable one? For example, in a young man with knee swelling, stiffness, pain, crepitus, quadriceps atrophy on examination, pain on palpation, and resistance during extension, what’s the likely underlying cause?
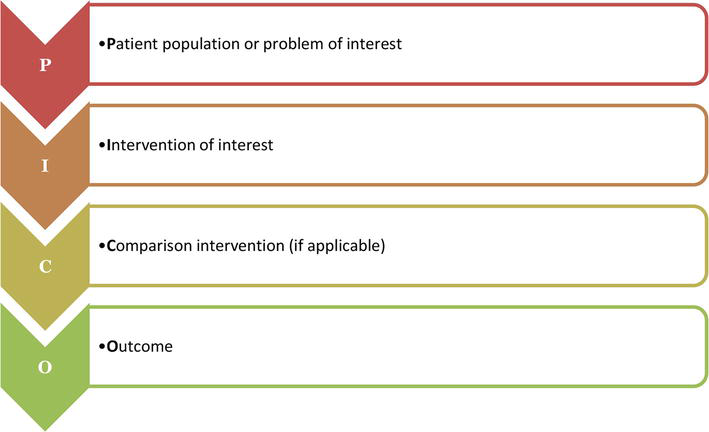
3.1.1 PICO framework
The PICO framework holds great importance in shaping a precise question. This framework identifies and outlines the crucial components of a well-organized question. It’s important to remember that a focused question should address a single issue at a time (Figure 3 and Table 1).
Figure 3.
PICO framework.
Example
Patient population or relevant issue
What is the specific disease or condition under consideration?
A 60-year-old woman dealing with shoulder pain post-stroke
Intervention
What particular treatment, modality, or procedure is being focused on?
What is the alternative to the current treatment being administered? For instance, placebo or medication.
Non-steroidal anti-inflammatory drugs
Outcome
What are the goals in terms of measurement, enhancement, or impact?
Reduction in the level of experienced pain
Table 1.
Using the PICO framework to develop a clear question.
An example of clinical question from the above table could be ‘Is TENS better than non-steroidal anti-inflammatory drugs at reducing the intensity of post stroke shoulder pain?’
3.2 Searching and finding the best evidence
Once you have carefully formulated a precise clinical question addressing the disease or condition presented by your patient, your next step involves sourcing the most reliable evidence to address this query. A range of resources exists to aid your quest for answers. These encompass personal experience, logical reasoning, and intuition, inquiring with a fellow practitioner, referring to textbooks, accessing pertinent scientific papers from your personal collection, utilizing bibliographic databases such as Medline or Embase, and consulting literature that’s clinically assessed or grounded in evidence, along with established healthcare guidelines.
However, a caveat exists when relying on personal experience and subjective opinions. Such an approach might not yield the most efficient, effective, and economically viable treatment pathways. Conversely, seeking advice from a seasoned colleague can be an expedient approach, especially when grappling with unique or infrequent scenarios. It’s worth noting that textbooks, while informative, often become outdated even before their publication, necessitating a cautious approach when consulting them.
The specific type of evidence you seek hinges on your question’s scope. Navigating the different types of research available will direct you toward attaining the utmost level of evidence relevant to your specific clinical inquiry. By discerning the nature of your question, you can methodically select the research avenue that aligns with your inquiry, leading you to the most robust evidence available to inform your clinical decisions effectively and accurately.
3.2.1 Levels of evidence
‘Levels of evidence’ refer to frameworks for categorizing research designs. These systems rank research designs based on intervention assessment, evaluating their reliability, validity (protection against bias and error), and truthfulness. Systematic reviews, meta-analyses of randomized controlled trials, and evidence-based clinical practice guidelines hold the highest status on the evidence hierarchy (illustratedas a pyramid in Figure 4), forming a robust foundation for treatment decisions. Conversely, expert opinion is widely considered the least robust evidence category in this hierarchy.
Figure 4.
Level of evidence pyramid.
3.2.2 Observational studies: Understanding research design
Research design encompasses two main approaches: qualitative and quantitative. Both methods, if properly executed, are rigorous and valuable for addressing significant clinical inquiries [13, 14]. Employing both designs within a single study is especially advantageous for extensive trials assessing clinical practices. This comprehensive approach is particularly beneficial for large-scale trials aimed at evaluating clinical practice.
3.2.3 Quantitative design
The quantitative design focuses on robustly examining hypotheses related to predefined variables. Examples of such designs encompass clinical trials, comparative studies, and epidemiological investigations. These studies primarily address queries like “whether” (evaluating whether Physiotherapy treatment yields more benefits than harm) and “how much” (measuring the strength of the correlation between a specific risk factor, like hypertension, and the occurrence of a particular disease or condition, such as stroke) [15].
3.2.4 Qualitative design
Qualitative studies delve into inquiries involving “how,” “what,” and “why” [15]. These studies often employ detailed interviews and focus group interactions to investigate and gain insight into “social, emotional, and experiential phenomena” within healthcare contexts. Examples encompass exploring the significance of the stroke experience for survivors and their families, offering a deeper understanding of these individuals’ perspectives.
Critical appraisal constitutes a crucial aspect of evidence-based practice (EBP), involving the meticulous and systematic evaluation of research evidence to gauge its credibility, significance, and relevance to clinical application [16]. It’s pivotal to recognize that diverse research designs entail distinct methodological procedures and levels of validity. This distinction underscores the significance of comprehending how findings can be translated into practical use within specific clinical contexts.
5. Implementing evidence-based into clinical practice
Incorporating optimal evidence-based practices into your daily routine as a Physiotherapist is challenging. However, identifying barriers specific to your setting can aid in devising a more efficient strategy, enhancing the likelihood of successful patient management [17].
Barriers to evidence-based Physiotherapy can impede optimal patient care. The challenges of a busy clinical setting may make accessing current, relevant evidence difficult [18]. Reluctance to alter established practices in light of new evidence can impede progress. Limited familiarity with research resources and a lack of confidence in interpreting findings are common obstacles [19]. Moreover, the absence of conclusive evidence might discourage practitioners, though it should not deter them from engaging in evidence-based processes [20]. Overcoming these barriers through education, enhanced resource accessibility, and fostering adaptability is vital for advancing evidence-based Physiotherapy and ensuring informed, effective patient management (Table 2).
Barriers
Example
Structural
Policies and Financial disincentives
Organizational
Lack of staff skills, poor working environment or lack of equipment/diagnostic tools
Peer group
Local standard of care not standard
Individual
inadequate knowledge, quackery, attitudes or skills
Professional-patient interaction
Problems with information processing, lack of communication skills
Consumers
Wrong information and illiteracy
Table 2.
Barriers to implementing evidence-based practice [21].
Embracing evidence-based practice within Physiotherapy necessitates a resolute commitment to furnishing optimal care for patients. Amid the bustling hospital milieu, the initial stride toward effective evidence-based practice in Physiotherapy lies in discerning where to access the most current, fitting, and superior evidence, ideally in a readily accessible format. Equally vital is the determination and self-assuredness to recalibrate practices in light of evidence.
Occasionally, the sought-after answers to inform clinical practice may remain elusive. It’s essential to internalize that the absence of evidence does not imply an absence of impact. The absence of conclusive evidence should not hinder Physiotherapists from participating in the evidence-based process; instead, it should fuel the impetus to galvanize fresh research endeavors in pursuit of the requisite evidence within the domain of Physiotherapy. This resilience underscores the dynamic nature of evidence-based practice as a driver for continuous improvement and growth in the field.
References
1.World Confederation for Physical Therapy—European Region. Evidence Based Physiotherapy. Brussels: The Confederation; 2015. Available from: http://www.erwcpt.eu/education/evidence_based_physiotherapy_evidence_and_research
2.Sackett DL, Strauss SE, Richardson WS. Evidence-Based Medicine: How to Practice and Teach EBM. London: Churchill-Livingstone; 2000
3.National Institute of Public Health (NIPH). First Annual Nordic Workshop on How to Critically Appraise and Use Evidence in Decisions about Healthcare. Oslo, Norway: NIPH; 1996
4.Haynes RB, Devereaux PT, Guyatt GH. Clinical expertise in the era of evidence based medicine and patient choice. Evidence-Based Medicine. 2002;7:36-38
5.Caldwell K, Coleman K, Copp G, Bell L, Ghazi F. Preparing for professional practice: How well does professional training equip health and social care practitioners to engage in evidence-based practice. Nurse Education Today. 2007;27:518-528
6.Chan S, Clough A. A critical evaluation of evidence-based practices of physiotherapy in musculoskeletal medicine. IMM. 2010;32:163-166
7.Dannapfel P, Peolsson A, Nilsen P. What Supports Physiotherapists’ Use of Research in Clinical Practice? A Qualitative Study in Sweden Implementation Science. 2013. p. 8. Available at: http://www.implementationscience.com/content/8/1/31/prepub [Accessed: January 31, 2012]
8.Bello A. Utilizing research findings in physiotherapy: A call for gap bridging. Nigerian Postgraduate Medicine. 2011;18(19):54-58
9.Kumar S, Grimmer-Somers K, Hughes B. The ethics of evidence implementation in health care. Physiotherapy Research International. 2010;15:96-102
10.Linda F, Julie T. Evidence Based Physical Therapy. FA Davis; 2008
11.Sackett DL, Rosenberg WMC, Gray JAM, Haynes RB, Richardson WS. Evidence based medicine: What it is and what it isn’t. BMJ. 1996;312:71-72
12.Greenhalgh T, Toon P, Russell J, et al. Transferability of principles of evidence based medicine to improve educational quality: Systematic review and case study of an online course in primary health care. BMJ. 2003;326:142-145
14.Portney LG, Watkins MP. Foundations of Clinical Research: Applications to Practice. 2nd ed. London: Prentice-Hall Health; 2000
15.Giacomini M, Cook DJ. Users’ guides to the medical literature: XXIII. Qualitative research in health care. Are the results of the study valid? JAMA. 2000;284:357-362
16.Greenhalgh T. How to read a paper: Papers that summarise other papers (systematic reviews and meta-analyses). BMJ. 1997;315:672-675
17.Grimshaw JM, Shirran L, Thomas R, et al. Changing provider behaviour: An overview of systematic reviews of interventions. Medical Care. 2001;39(8):II-2-II-45
18.Smith A, Johnson B, Williams C. Challenges in evidence-based practice for physiotherapists. Physical Therapy Reviews. 2019;24(4):203-208
19.Jones R, Davies D, Green J. Barriers and facilitators to evidence-based practice in physiotherapy. Physiotherapy. 2020;106:e134-e135
20.Brown L, Green J. Challenges and barriers to implementing evidence-based practice in physiotherapy. International Journal of Physiotherapy and Research. 2018;6(1):2677-2680
21.Grimshaw JM. Changing Professional Behaviour: Empirical, Theoretical and Pragmantic Perspectives. Sydney, Australia: Australasian Cochrane Collaboration Course; 2003
Written By
Ibrahim Ahmad Abubakar
Submitted: 17 July 2023Reviewed: 23 July 2023Published: 28 February 2024
 Open access peer-reviewed chapter
Open access peer-reviewed chapter