 Open access peer-reviewed chapter
Open access peer-reviewed chapter
Abstract
Airway management is an essential skill that is relevant to the practice of medicine especially with regards specialties such as anesthesia, intensive care and emergency medicine. This vital skill can be made more challenging in an austere environment with limited facilities and equipment. Being pre-informed on the peculiarity of each patient, developing and mastering necessary skills through regular trainings and having a pre- outlined care plan based on available resources in the immediate environment can mitigate against some of the possible challenges in such environment. Hence, the pre-operative assessment of a patient with a difficult airway is an integral part of the peri-operative workup that helps to predict potential problems, develop a management plan thereby avoiding an unanticipated difficult airway as much as possible and inadvertently preparing for an unanticipated difficult airway in rare instances.
Keywords
- difficult airway
- limited resources
- anticipated difficult airway
- airway equipment
- supraglottic devices
- advanced airway equipment
1. Introduction
Airway management hazards are common causes of morbidity and mortality in the peri-operative period especially in a resource limited environment. Adequate airway assessment is essential in the care of all patients requiring advanced airway management. The goal of airway assessment is to identify patients who may have difficult airway and develop practical management options depending on the cause of the difficult airway, the patient’s condition, skill of the attending airway manager and the available equipment in the immediate environment. There are two major focus areas in the management of a difficult airway:
Laryngoscopy and intubation
Ventilation (oxygenation)
Although protocols are available to guide the management of difficult airways, but these protocols can only help each team or unit to develop guidelines that are convenient and peculiar to them based on available equipment, skill of attending airway managers and the cause of difficulty in airway. The aim is to prevent critical airway outcomes such as hypoxic brain injury, cardiac arrest, oropharyngeal trauma and death. Predicting problems with ventilation and oxygenation supersedes predicting difficulties with laryngoscopy or intubation as failed laryngoscopy is not as dangerous as a situation of failed oxygenation. Airway assessment to predict a difficult airway will entail history taking, examination and investigations. For patients who have never been intubated, airway difficulty can only be suspected from review [1].
According to the American Society of Anaesthesiologists Task Force definitions [1]:
The difficult airway occurs when a conventionally trained Anesthetist has difficulty with either facemask or laryngeal mask airway ventilation, tracheal intubation or all the three clinical scenarios.
Problem with facemask ventilation is when the conventional anesthetist cannot maintain oxygen saturation on at least 92% as measured by a pulse oximeter or prevent clinical evidence of deficient ventilation during advanced airway management. With difficult laryngoscopy, a conventional anesthetist has a problem visualizing the vocal cords. This usually corresponds to a Cormack and Lehane Grade IV laryngoscopy view [1, 2].
A difficult intubation occurs when a conventional laryngoscopy requires more than three attempts or more than 10 minutes to introduce an endotracheal tube by a conventionally trained anesthetist.
The prevalence of difficult airways varies widely and changes with the environment, situation and type of patient. It is approximately1 in 1–2000 in the elective setting, 1 in 300 during rapid sequence intubation in the obstetric setting and 1 in 50–100 in the emergency department, intensive care unit, and pre-hospital settings [1, 3].
2. Identifying a Difficult Airway
The management of a difficult airway begins with the anticipation of a difficult airway and developing a plan to avert critical incidents due to a difficult airway encounter. The prediction of a difficult airway is heralded by a proper pre- operative assessment [1].
2.1 Pre-operative airway evaluation
This involves history taking, examination, investigation, familiarization with the work environment and available instruments to maneuver the airway, identifying the strength of each team member and assigning roles, identifying shortfalls and developing care plans that fits the immediate environment while not deviating from acceptable world standards [1, 3].
2.2 History
History that may suggest difficult airway management includes: The Reason for airway management, obesity, history suggestive of obstructive sleep apnea, exercise intolerance, smoking, change in voice, difficulty swallowing, burns affecting the airway, poor mouth opening, poor neck mobility, large mammary glands, Infections of the oropharynx and neck, previous surgery or radiotherapy to neck, difficult dentition, pregnancy, recent intubation (swelling, trauma), previous anesthetics and operations, previous difficulties with mask ventilation or laryngoscopy [4, 5].
2.3 Examination
The level of consciousness and co-operation, Body Mass Index, Beard, craniofacial deformity, Mallampati grade I to IV, Mouth opening, Inter-incisor gap distance (> 3 cm = good, < 3 cm = bad), Shape of palate, Jaw protrusion, Teeth, Edentuous, Teeth prominence (upper incisors) and condition, Relation of maxillary to mandibular incisors during normal jaw closure, dentures/ caps/ crowns/ loose teeth, Range of motion of head and neck, thyro-mental distance <6 cm, Neck length and circumference/ thickness, Compliance of mandibular space, Sternomental distance, upper lip bite test, Mallampati Classification [4, 5].
2.4 Investigations
Nasal endoscopy, awake laryngoscopy, Lateral neck xray, Chest Xray, CT neck
2.5 Modified Mallampati score
Class I: the soft palate, the uvula, fauces and pillars are seen easily [4]
Class II: the soft palate, the uvula and the fauces are seen
Class III: only the Soft palate and the base of the uvula can be seen
Class IV: Only the hard palate can be seen
Class III/IV predicts a difficult airway. The mallampattit scoring system can not be used alone to predict difficulty [6, 7].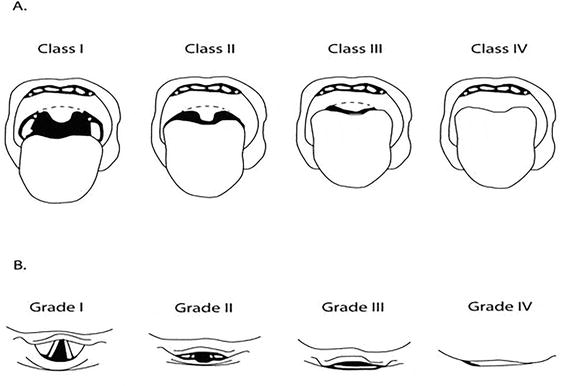
2.6 Cormack-Lehane classification
Grade 1: The full glottis is seen
Grade 2a: The glottis is partially seen
Grade 2b: Only the posterior aspect of the glottis is seen
Grade 3: Only epiglottis seen, no part of the glottis is sighted
Grade 4: No part of the glottis or the epiglottis is seen
A difficult intubation is suggested with a Grade 2b view or more [2].
Grade 1: the upper lip can be fully covered by the lower incisors
Grade 2: the upper lip can be partially covered with the lower incisors
Grade 3: the lower teeth cannot reach the upper lip [8]
3. Acronyms for difficult airway predictions
3.1 The acronym for difficult laryngoscopy and intubation is the LEMON SCORE
Look externally for facial anomaly, bleeding, small mouth [9]
Evaluate 3-3-2 rule
Mallampati score
Obstruction/ Obesity
Neck Mobility for trauma, arthritis, spondylosis and consider the use of video laryngoscopy
3.2 The acronym for the Difficult Bag Valve Mask (BVM) ventilation is BONES
The difficult BVM is described according to the American Society of Anesthesiologists (ASA) as a situation in which it is impossible to provide adequate ventilation due to poor mask seal, excessive gas leak or excess resistance to gas inflow or outflow [9].
Beard
Obese
No teeth
Elderly
Sleep Apnea / Snoring
3.3 The mnemonic for difficulty using a supra glottic device such as the laryngeal mask airway, LMA = RODS
Restricted mouth opening [9]
Obstruction
Distorted or disrupted airway
Stiff lungs or cervical-spine
3.4 The acronym for Difficult surgical airway (difficult cricothyrotomy) is SHORT
Surgery or other airway obstruction [9]
Hematoma, Infection or abcess
Obesity
Radiation distortion or other deformity
Tumor
4. Strategy for managing a predicted difficult airway: A pre planned pre-induction strategy includes:
4.1 Familiarization with the procedural environment
Is the anesthetic team conversant with the procedural environment? Is it the regular theater. Emergency room, the intensive care unit or a totally strange environment like an accident point, a catheterization laboratory? Do they have all needed equipment and resuscitatory drugs available? Do they have adequate support staff? Do they need to move needed equipment such as back up laryngoscopes, difficult airway trolleys and others to augment the facilities where the procedure will take place [1].
4.2 Selection of equipment
The choice of appropriate airway device is essential for effective airway management. The use of the facemask, oropharyngeal airway, curved and straight-blade laryngoscopes, different sizes of endotracheal tubes with adequate airway training skills were the mainstay of endotracheal intubation and airway management. The facemask is a basic airway device for providing ventilation during airway management. This then led to the introduction of the gum-elastic bougie for accessing minimally visible laryngeal inlets even after applying significant externally applied downward and upward laryngeal pressure. The bougie is then serving as a guide for advancing the endotracheal tube. Endotracheal tubes are devices inserted through the nose or mouth to provide oxygenation and ventilation. The distal end of the tube is located at the mid-trachea [1, 8, 10].
When the facemask fails to provide adequate ventilation/oxygenation in some situations (such as craniofacial deformities, edentulousness) which may require filling the defect with gauzes to support holding the facemask or handling the facemask with special techniques and the larynx cannot be accessed with the external maneuver or a gum elastic bougie, the use of supra glottic airway adjuncts may be necessary. Supraglottic airways devices ventilate from above the glottis. A common supraglottic device used in airway management is the Laryngeal Mask Airway, LMA. LMAs are used during difficult facemask ventilation and they can be used during difficult intubation as conduits for introducing the endotracheal tube [8, 11].
The LMAs can be used for noninvasive positive-pressure ventilation to provide positive-pressure airway support. Patients can be placed on a continuous positive airway pressure (CPAP) device or a bilevel positive airway pressure (BIPAP) device. The noninvasive positive-pressure ventilation is ideal in conscious patients with ventilatory efforts. However, patient should be closely monitored for a decline in consciousness or depreciating respiratory effort or exhaustion so that endotracheal intubation is established if needed [12].
A supraglottic device may be considered in difficult mask ventilation or difficult intubation .cases, or when a rescue device or conduit is required for endotracheal tube introduction during difficult intubation. For a difficult intubation, the use of a gum elastic bougie, the intubating LMA, a video laryngoscope or awake fibreoptic intubation are the various options.
When a difficult airway is encountered, the downward and upward laryngeal pressure maneuver is performed to attempt to bring the laryngeal inlet into better view. The gum elastic bougie is used for accessing minimally visible laryngeal inlets after the above maneuver fails. The bougie serves as a guide to advance the endotracheal tube.
It is important to note that, the patient, the cause of difficulty, the skill of the anesthetist and the available equipment are all determinants of the choice of equipment and technique of airway management. The Intubating Laryngeal Mask Airway, ILMA is a special type of LMA that is recommended in the management of a difficult airway. It is said to have about 94% success rate [11].
The awake fibreoptic intubation is another option for managing a difficult airway. These are not readily available in resource limited facilities. Although studies have recorded 88–100% success rate in their use for managing difficult airways. The ILMA and the awake fibreoptic intubation are said to have comparable success rate [12].
The video laryngoscope is a choice equipment for managing a difficult airway. It enables smooth and safe introduction of eitheran endotracheal tube, an endotracheal tube introducer, or fiber optic scopes in the care of both an anatomically normal upper airways and also those with a difficult upper airway. The video laryngoscope has an in built camera that allows the process of airway management to be watched on a screen that is either attached to the handle of the laryngoscope itself or is freestanding. There are various types of video laryngoscopes offering different designs of laryngoscope blades such as the straight, curved or hyper-angulated blades [13, 14]. It is advisable that the managing anesthetist uses the equipment they are familiar with and they have available on their airway trolley arranged with available resuscitatory drugs. With a failed attempt at intubation despite the use of the LMA, fibreoptic and videolaryngoscope and patient cannot be ventilated using the LMA or facemask, a surgical airway is indicated. Hence, the difficult airway tray should always include a cricothyroidotomy kit.
Assessment of equipment: It is vital to check the functionality of all equipment to be used for the procedure and carefully arrange them. From the oxygen source, to the sunction machine to the laryngoscopes must be checked. Backup equipment like extra tubes of various sizes, different types of laryngoscopes and sizes of blades, different types and sizes of LMA must be available. Equipment failure is a known cause of critical airway incidents. In the case report by Fagbohun et al. [15], they experienced laryngoscope light source failure after an initial check of the said laryngoscope prior to commencing the procedure. However, they were able to seamlessly maneuver around the incident as there was a back up laryngoscope on their airway trolley.
Skills, Strategy and positioning: The airway managers must collaborate with other theater professionals to ensure a smooth and supportive inter personal relationship. The choice of airway management in patients should not only consider the anesthetists and patient but also consider the surgical access/field for the surgeons and adherence to established airway guidelines to facilitate effective airway management.
Air way managers have emphasized that proper positioning of the patient by maintaining jaw-lift, good neck positioning, use of continuous positive airway pressure, identifying a potential difficult airway before a procedure and outlining a care-plan based on the accepted difficult airway algorithm will reduce the risk of critical incidents during airway management especially in an environment where resources are scarce
It is appropriate to ensure adequate debriefing between all members of the peri-operative care team regarding the observed peculiarity of the patient, potential difficulties envisaged and possible resolution plans associated with the airway assessment.
4.3 Ethics and team members’ roles/specification
Obtaining thorough and comprehensive informed consent from patients or their authorized legal care givers or decision makers is crucial before administering anesthesia and conducting an airway assessment. All team members should freely air their opinions and views to ensure patient has optimal care. All issues of concern should be discussed and resolved before the procedure begins. The role of each team member should be clearly specified during debriefing to ensure proper coordination [17, 18].
4.4 Preparation for extubation
The anaesthesiologist should consider the benefit of awake extubation to extubation while patient is still unconscious. The patient should be well ventilated to avoid critical incidents from hypoxia. Until the patient is fully recovered, the difficult airway tray should be maintained and within reach.
4.5 Follow up care
It is necessary that all difficult airway management experiences and how they were managed are properly documented. Detailed information should be given to the patient or responsible adult in the case of children or the incapacitated patient to guide future airway management. (Preferably as a document)The patient should also be evaluated for possible complications from the difficult airway management experienced [1, 17, 18].
5. Conclusion
Working in a resource scarce environment is challenging to the airway manager. It is important that these specialists working in these unique environments are constantly engaged in refresher courses to update their knowledge and skills on current standard practices and constant drills should be organized to put the knowledge acquired to test and use so that they do not forget the skills acquired. It is important to note that the best airway plan for the patient is dependent on the patient, the skill of the attending airway manager and the available equipment at the time of intervention and not just the availability of advanced airway equipment.
References
- 1.
American Society of Anesthesiologists Task Force on Management of the Difficult Airway. Practice guidelines for management of the difficult airway: an updated report by the American Society of Anesthesiologists Task Force on Management of the Difficult Airway. Anaesthesiology. 2003; 98 (5):1269-1277. Erratum in: Anesthesiology. 2004 Aug;101(2):565 - 2.
Cormack RS, Lehane J. Difficult tracheal intubation in obstetrics. Anaesthesia. 1984; 39 (11):1105-1111 - 3.
Cook TM, MacDougall-Davis SR. Complications and failure of airway management. British Journal of Anaesthesiology. 2012; 109 (1):68-85. DOI: 10.1093/bja/aes393 - 4.
Mallampati SR, Gatt SP, Gugino LD, Desai SP, Waraksa B, Freiberger D, et al. A clinical sign to predict difficult tracheal intubation: A prospective study. Canadian Anaesthetists' Society Journal. 1985; 32 (4):429-434 - 5.
Nørskov AK, Rosenstock CV, Wetterslev J, Astrup G, Afshari A, Lundstrøm LH. Diagnostic accuracy of anaesthesiologists’ prediction of difficult airway management in daily clinical practice: a cohort study of 188 064 patients registered in the Danish Anaesthesia Database. Anaesthesia. 2015; 70 (3):272-281 - 6.
Bair AE, Caravelli R, Tyler K, Laurin EG. Feasibility of the preoperative Mallampati airway assessment in emergency department patients. The Journal of Emergency Medicine. 2010; 38 (5):677-680. DOI: 10.1016/j.jemermed.2008.12.019 - 7.
Kar S, Senapati LK, Samanta P, Satapathy GC. Predictive value of modified Mallampati Test and Upper Lip Bite Test Concerning Cormack and Lehane’s Laryngoscopy Grading in the Anticipation of Difficult Intubation: A Cross-Sectional Study at a Tertiary Care Hospital, Bhubaneswar, India. Cureus. 2022; 14 (9):e28754 - 8.
Brain AI. The laryngeal mask – A new concept in airway management. British Journal of Anaesthesia. 1983; 55 :801-805 - 9.
Rachel M, Jarrod M, Darren B, Calvin A, Fred E. Crash a mnemonic for the physiological difficult airway. NRP. 2020; 2020 :1 - 10.
Rich JM. Recognition and management of the difficult airway with special emphasis on the intubating LMA-Fastrach/whistle technique: a brief review with case reports. Proceedings (Bayl Univ Med Cent). 2005; 18 (3):220-227 - 11.
Onyekwulu FA, Nwosu A. Emergency airway management with laryngeal mask airway. Nigerian Journal of Clinical Practice. 2011; 14 :95-97 - 12.
Chalam KS, Gupta J. Comparison of intubating laryngeal mask airway and fibreoptic bronchoscopy for endotracheal intubation in patients undergoing cervical discectomy. Journal of Anaesthesiology Clinical Pharmacology. 2016; 32 (4):515-518 - 13.
Yumul R, Elvir-Lazo OL, White PF, Sloninsky A, Kaplan M, Kariger R, et al. Comparison of three video laryngoscopy devices to direct laryngoscopy for intubating obese patients: A randomized controlled trial. Journal of Clinical Anesthesia. 2016; 31 :71-77 - 14.
Boehringer B, Choate M, Hurwitz S, Tilney PV, Judge T. Impact of video laryngoscopy on advanced airway management by critical care transport paramedics and nurses using the CMAC pocket monitor. BioMed Research International. 2015; 2015 :821302 - 15.
Fagbohun O, Ibifuro D, Olugbusi S, Oresanwo T. Anaesthesia for reconstruction surgery post mandibulectomy in a patient with a predicted difficult airway: A case sreport. Integrated Journal of Medical Science. 2021; 8 :1-3 - 16.
American Society of Anesthesiologists Task Force on Management of the Difficult Airway. Practice guidelines for management of the difficult airway: An updated report by the American Society of Anesthesiologists Task Force on Management of the Difficult Airway. Anesthesiology. 2003; 98 :1269-1277 - 17.
Frerk C, Mitchell VS, McNarry AF, Mendonca C, Bhagrath R, Patel A, et al. Difficult Airway Society 2015 guidelines for management of unanticipated difficult intubation in adults. British Journal of Anaesthesia. 2015; 115 :827-848 - 18.
Nickson C. Airway assessment. In: LITFL – Life in the FastLane. Available from: https://litfl.com/airway-assessment/ [Accessed June 8, 2023]