Open Access is an initiative that aims to make scientific research freely available to all. To date our community has made over 100 million downloads. It’s based on principles of collaboration, unobstructed discovery, and, most importantly, scientific progression. As PhD students, we found it difficult to access the research we needed, so we decided to create a new Open Access publisher that levels the playing field for scientists across the world. How? By making research easy to access, and puts the academic needs of the researchers before the business interests of publishers.
We are a community of more than 103,000 authors and editors from 3,291 institutions spanning 160 countries, including Nobel Prize winners and some of the world’s most-cited researchers. Publishing on IntechOpen allows authors to earn citations and find new collaborators, meaning more people see your work not only from your own field of study, but from other related fields too.
To purchase hard copies of this book, please contact the representative in India:
CBS Publishers & Distributors Pvt. Ltd.
www.cbspd.com
|
customercare@cbspd.com
Airway management is a fundamental skill for emergency medical professionals like paramedics, EMTs, and emergency physicians. It involves quickly evaluating and addressing airway obstructions or breathing difficulties, often in high-stress, life-threatening situations. Proficiency requires a deep understanding of airway anatomy, physiology, and interventions, along with adaptability and rapid decision-making. This chapter summarizes evidence on key aspects, including assessing difficult airways, positioning, oxygenation, intubation methods, medications, devices, and rescue strategies, across various patient groups. Effective airway management is crucial for enhancing patient outcomes and reducing mortality in emergencies.
Emergency Medicine, MNR Medical College, Telangana, India
Garima Jain
Fortis Hospital, Mohali, India
*Address all correspondence to: gauravdhir2003@gmail.com
1. Introduction
Emergency airway management is critical in emergency medicine, with securing the airway as the top priority for critically unstable patients. Around 0.5–1% of ED visitors require intubation due to conditions like respiratory failure, cardiac arrest, and altered mental state. ED intubation presents unique challenges, including vomiting, facial/neck injuries, cervical spine immobilization, and chest compressions. These factors impact intubation success, emphasizing the need for ED physicians to understand current evidence. Evidence underscores achieving first-pass intubation success, discouraging multiple attempts, which elevate risks like adverse events, higher failure rates, reduced chances of ROSC, and prolonged resuscitation times. Adequate preparation and assessing difficult airways are crucial for successful intubation. This chapter explores first-pass success, airway management algorithms, and systematic rescue intubation strategies.
The pharynx, connecting nasal and oral cavities to the larynx and esophagus, comprises the nasopharynx, oropharynx, and laryngopharynx. Obesity and a receding mandible can alter the airway, with excess fat affecting pharyngeal muscles and obstructing it. Enlarged tongues in obese individuals can pose challenges in mask ventilation. Negative intrathoracic pressure in obesity can further constrict the pharyngeal airway, worsening mask ventilation. The larynx, consisting of membranes, cartilage, and muscles, connects the respiratory and digestive tracts, safeguarding the airway and enabling speech. It includes nine cartilages, such as paired (arytenoid, corniculate, cuneiform) and unpaired (thyroid, cricoid, epiglottis). The thyroid cartilage forms the Adam’s apple, while the cricoid cartilage lies below it, both crucial for airway procedures and nerve blocks.
The cricothyroid membrane, located between the cricoid and thyroid cartilages in the neck, plays a significant role in anatomy and clinical practice. In emergencies with compromised upper airways, cricothyroidotomy becomes essential, involving an incision in the cricothyroid membrane to establish a temporary airway, serving as a life-saving intervention when conventional methods fail [1, 2, 3, 4, 5].
The tracheobronchial tree, responsible for gas transport from the trachea to the lung’s gas exchange units (acini), features a complex branching system. The trachea, extending from the C6 level to the carina, divides into the right and left main bronchi at the carina. The right main bronchus takes a more direct path and divides into smaller branches earlier, increasing the risk of inadvertent right endobronchial intubation during intubation.
A secured airway encompasses all necessary measures to establish and sustain an unobstructed air passage, ensure effective patient ventilation, and maintain oxygenation levels above 94%. This comprehensive approach encompasses the utilization of positioning techniques and a variety of airway adjunct tools, both basic and advanced, to ensure optimal patient respiratory function and safety (Figure 1) [6].
Figure 1.
Open airway vs. blocked airway.
3.1 Signs of blocked airway
Recognizing signs of a blocked airway is crucial for prompt intervention. These indicators include mild tachypnea, visible retractions in the suprasternal and supraclavicular areas, nasal flaring, alterations in voice such as hoarseness or a barking cough, the presence of inspiratory stridor, limited chest expansion, reduced air entry during auscultation, and the emergence of cyanosis, excessive drooling, or persistent coughing. Identifying these symptoms allows for timely action to ensure adequate airflow and prevent potentially life-threatening respiratory complications.
3.2 Techniques of securing an airway
Securing an airway aims to establish and maintain an open path for air to enter and exit the lungs. The approach varies based on severity and patient condition. Endotracheal intubation, inserting a tube into the trachea via mouth or nose, is a common method ensuring a protected airway with ventilation control. When intubation is not possible, supraglottic airway devices or bag-mask ventilation serve as viable alternatives.
3.3 Basic airway maneuvers
Basic airway maneuvers play a critical role in managing airway obstructions. The primary causes of blockage often involve the tongue or epiglottis displacement. Techniques like head tilt-chin lift and jaw thrust help establish a clear airway by repositioning the tongue and soft tissues. It’s essential to exercise caution when employing these maneuvers, especially if there’s a suspicion of cervical spine injury, as they can exacerbate the condition. For head tilt-chin lift, gently tilt the head back by pressing down on the forehead while lifting the chin with the index and middle fingers. For jaw thrust, place your palms on the temples, with fingers under the jaw, and lift the mandible upward to elevate the tongue. In children, a modified approach is used, with head tilt-chin lift without overextension and jaw thrust with just the index finger on the lower jaw. Combining head tilt, jaw thrust, and mouth opening creates the Triple airway maneuver, further enhancing airway clearance and maintenance.
3.4 Non definitive and definitive airway
The Non-Definitive airway category encompasses airway management techniques and devices that are positioned above the laryngeal inlet. Examples include oropharyngeal airways, nasopharyngeal airways, and supraglottic airway devices like the Combitube, Laryngeal tube, and LMA (Laryngeal Mask Airway). These tools and techniques are employed to establish and maintain a patent airway, particularly when definitive airway management may not be immediately necessary or feasible [7].
The Definitive airway category encompasses techniques and devices positioned below the laryngeal inlet, ensuring a secure and reliable airway. Examples include endotracheal tubes (both nasotracheal and orotracheal), tracheostomy, and cricothyroidotomy. These methods are utilized when there is a critical need to establish a secure and long-term airway, such as in cases of prolonged ventilation, surgical access, or severe upper airway obstruction.
3.5 Non definitive airway
3.5.1 Oropharyngeal airway (OPA, Guedel’s airway)
An oropharyngeal airway is an airway adjunct used to maintain or open the airway by stopping the tongue from covering the epiglottis. It can potentially bypass airway obstruction caused by any of the oral structures like tonsillar hypertrophy, or falling back of tongue into the posterior pharynx in the supine position. The tip of the OPA should lie just above the epiglottis at correct insertion depth.
Its primary indication lies in its use for unconscious patients who struggle to maintain an open airway despite attempted airway maneuvers. However, it’s essential to note that there are contraindications to its usage, namely conscious patients or those with an intact gag reflex, for whom alternative airway management methods should be considered. While the oropharyngeal airway can be lifesaving, it’s not without potential complications. If improperly sized, it may induce gagging, retching, or even laryngospasm. Moreover, using an OPA that is too small might exacerbate airway obstruction by pushing the tongue backward (Figure 2).
Figure 2.
Oropharyngeal and nasopharyngeal airway.
3.5.2 Nasopharyngeal airway (NPA)
Nasopharyngeal airways are plastic hollow or soft rubber tubes can be utilized to aid difficult bag valve mask ventilation. They are passed through the nose to the posterior pharynx. The direction of insertion should be straight back towards the occiput and along the nasal floor rather than cephalad, with the concave side facing down to allow it to pass into the posterior pharynx behind the tongue.
Nasopharyngeal airways are typically indicated for awake or semi-conscious patients who possess an intact gag reflex, individuals with limited mouth opening due to conditions like trismus or angioedema, and those with fragile dentition. However, there are clear contraindications that should be adhered to, including patients with basilar skull fractures, facial trauma, or disruption of the midface, nasopharynx, or roof of the mouth, as well as individuals with coagulopathies or those taking anticoagulants due to an elevated risk of bleeding. Large nasal polyps and a history of recent nasal surgery also stand as contraindications. As with any medical procedure, potential complications must be considered, which can encompass trauma to nasal mucosa or adenoids leading to epistaxis, as well as the risk of gastric distension and vomiting if an excessively long device is employed (Figures 3 and 4).
Figure 3.
Correct size assessment: The flange of the airway should be approximated,externally, to where it is abutting the lips, and the tip should be able to reach the angle of the mandible/ tragus of the ear.
Figure 4.
Correct size assessment can be done placing flange at nasal opening and orienting the device towards the angle of the mandible/tragus of the ear.
3.5.3 Supraglottic airway devices (also known as extraglottic or periglottic devices)
Supraglottic Airway Devices (SGD) are devices that ventilate patients by delivering oxygen above the level of the vocal cords. The chief advantage of the supraglottic airway devices in emergency airway management include ease of placement by both experienced and inexperienced personal and hands free airway. As a rescue airway in difficult airway, failed intubation and cannot ventilate cannot intubate (CVCI) situations. There are many ways to classify SGD and one of them is according to there sealing mechanism (functional classification) [8].
Cuffed perilaryngeal sealer
Non-directional non esophageal Sealers- cLMA, Flexible LMA, LMA unique.
With esophageal sealing: Combitube, Laryngeal tube, LTS.
Cuff less preshaped sealer
With esophageal sealing- Baska mask, i-gel.
Without esophageal sealing- SLIPA, AirQ-ILA.
This chapter will provide a brief description of the top five supraglottic devices commonly utilized in emergency departments: cLMA, LMA Fastrach, Air Q ILA, i-gel, and Esophageal Combitube.
3.5.3.1 LMA classic (cLMA)
The Classic Laryngeal Mask Airway (LMA) is a widely used medical device designed to establish a secure and effective airway during various surgical and medical procedures. It features an inflatable cuff that, when properly positioned, seals the laryngeal inlet, allowing for ventilation and oxygenation (Figure 5).
Figure 5.
Classic LMA.
3.5.3.2 Insertion technique
Inserting the Classic LMA is a relatively straightforward procedure. Hold the device like a pen, positioning your index finger at the junction of the cuff and airway tube. Gently press the cuff’s tip upward against the hard palate while maintaining visual guidance, ensuring it flattens against the palate. With your index finger, press the cuff backward towards the occiput, advancing the device into the hypopharynx. Continue the insertion until your finger reaches its fullest extent within the oral cavity, taking care to stop before encountering resistance.
3.5.3.3 LMA Fastrach
LMA Fastrach has proven to be an effective airway device both within and outside the emergency room. Effective ventilation is rapidly and successfully established in nearly all cases and blind intubation is possible in majority of cases if optimal technique is used. Adjunct such as fiber optic bronchoscope or light wand may be used occasionally (Figure 6).
Figure 6.
LMA Fastrach.
3.5.3.4 Insertion technique
Gently insert the LMA Fastrach into the patient’s mouth, following the natural curvature of the tongue. Avoid using excessive force, as this can cause trauma. As you insert the LMA Fastrach, advance it gently until resistance is felt. Then, slightly rotate it 90 degrees, which helps align the tip with the laryngeal inlet.
Chandy’s maneuver: It involves a series of precise steps for blind intubation via LMA Fastrach. The first step, the 1st Chandy’s maneuver, focuses on optimizing ventilation by directing the airway aperture towards the glottis, ensuring efficient airflow. Following this, the 2nd Chandy’s maneuver involves lifting the device vertically for proper positioning. Next, a well-lubricated wire-reinforced tube, with the black line oriented towards the patient’s nose, is passed through. The cuff is then inflated, and placement is confirmed by monitoring end-tidal CO2 levels. To secure the endotracheal tube (ETT), the obturator rod is used for stabilization. Finally, the Laryngeal Mask Airway (LMA) is deflated and carefully removed, completing the Chandy’s maneuver, a meticulous process critical for successful airway management [9].
3.5.3.5 Air-Q intubating laryngeal airway
Air -Q ILA was introduced by Daniel Cook in 2005 as an aid for airway maintenance and as a conduit for endotracheal intubation during general anesthesia. In case of intubation failure AirQ ILA can be used as a definitive airway (Figure 7).
Figure 7.
Air-Q ILA.
3.5.3.6 Insertion technique
Hold the Air-Q LMA like a pen, with your index finger at the junction of the cuff and airway tube. Gently insert the device into the patient’s mouth, following the natural curvature of the tongue. Aim to place the device so that the cuff sits within the hypopharynx and the airway tube is aligned with the laryngeal inlet.
To intubate via Air-Q LMA, first, disconnect the connector, and then introduce an appropriately sized and well-lubricated endotracheal tube (ETT). This can be accomplished either through blind insertion or with the assistance of a fiberoptic bronchoscope for precision. Once the ETT is securely in place, deflate the cuff of the Air-Q ILA, use the AIR-Q removal stylet to stabilize the ETT, and subsequently remove the AIR-Q ILA from the patient’s airway. This sequence of steps ensures a smooth and controlled transition from the Air-Q ILA to the ETT while maintaining optimal airway management.
3.5.3.7 I gel
I gel is made from a medical grade thermoelastic polymer, it has been designed to create a non inflatable anatomical seal of the pharyngeal, laryngeal and perilaryngeal structures while avoiding compression trauma. It houses separate airway tubing and gastric channels. The gastric channel allows suction of gastric contents and passage of a gastric tube (Figure 8).
Figure 8.
I-gel.
3.5.3.8 Insertion technique
Grasp the device along the integral bite block and introduce into the mouth towards the hard palate, gliding downwards and backwards along the palate until a definite resistance is felt.
3.5.3.9 Esophageal combitube
The combitube is now primarily used for emergency airway management in prehospital settings as well as in CVCI situations in the hospital setting. It differs from other supraglottic airway devices in being designed for blind placement in either the trachea or the esophagus. It is a double lumen tube with2 cuffs, with one lumen opening beyond the distal cuff, while the other ending between the 2 cuffs with only side openings. The proximal high volume (blue) pharyngeal cuff is inflated with 85-100 ml air while the distal (white) with12-15 ml. The proximal cuff occludes the hypopharynx while the distal occludes either the trachea or the esophagus (Figure 9).
Figure 9.
Esophageal Combitube.
3.5.3.10 Insertion technique
To ensure proper placement of the airway device, maintain the patient’s head in a neutral position and gently insert the device into the mouth in a downward curving motion until the teeth or gum line align with the two black lines on the device. Following insertion, inflate both cuffs with the appropriate volumes. Verify ventilation using the blue lumen: in the correct esophageal position, no gurgling should be audible over the epigastrium, and breath sounds should be detectable in the lung fields. If the distal cuff is in the trachea, gurgling will be heard in the epigastrium, and chest auscultation will reveal an absence of breath sounds. If neither breath sounds nor gurgling is present, it indicates that the tube has been inserted too far into the esophagus. To confirm tracheal placement, check ventilation using the clear lumen: if the distal cuff is in the trachea, there should be no gurgling, and breath sounds should be audible in the lung fields. Continue ventilation through the appropriate lumen that allows for effective ventilation.
3.6 Definitive airway
Endotracheal intubation is a common method used to create a definitive airway. This technique involves the insertion of a tube into the trachea, either through the mouth or nose, to maintain an open air passage. Intubation allows for precise control of ventilation and protects the airway from potential obstructions. Other approach to achieve a definitive airway in emergency care include cricothyroidotomy, which involves making an emergency incision in the cricothyroid membrane to access the airway. In the following discussion, we will explore various aids and techniques that assist in achieving a successful intubation procedure.
3.6.1 Endotracheal intubation aids
Endotracheal intubation may be achieved by any of the following airway aids depending upon the situation, device availability and operator expertise
Direct laryngoscopy and intubation
Bougie/Stylet guided intubation
Lightwand guided intubation
Video laryngoscopy and intubation
Fibreoptic bronchscope guided intubation
Supraglotic airway guided intubation
3.6.2 Direct laryngoscopy
Laryngoscope blades are essential instruments used during endotracheal intubation procedures to visualize the larynx and facilitate the insertion of an endotracheal tube. There are several different types of laryngoscope blades, each with its own unique design and purpose. The most commonly used blades include,
Macintosh: This curved blade is the traditional choice for laryngoscopy. It has a smooth, curved tip that allows the blade to lift the epiglottis and visualize the vocal cords.
Miller: The Miller blade is straight and has a flatter profile compared to the Macintosh blade. It is often used in pediatric cases or in patients with limited neck mobility. The straight design helps lift the epiglottis directly, providing a clear view of the vocal cords [10].
Mac Coy: Hinged tip helps in elevating the epiglottis leading to an increased increased view of the larynx, useful in patients with anterior larynx
Polio Blade: Very useful in intubating patients with breast hypertrophy, obese patients, patients with short neck and with restricted neck mobility [11].
Video Laryngoscope: Unlike traditional direct laryngoscopy, which relies on a direct line of sight, video laryngoscopes incorporate a small camera at the tip of the blade or handle. This camera captures a real-time video image of the airway, which is displayed on a screen, allowing direct visualization of the larynx and guide the insertion of the endotracheal tube (Figures 10–12).
Figure 10.
McCoy laryngoscope blade.
Figure 11.
Miller laryngoscope blade.
Figure 12.
Macintosh laryngoscope blade.
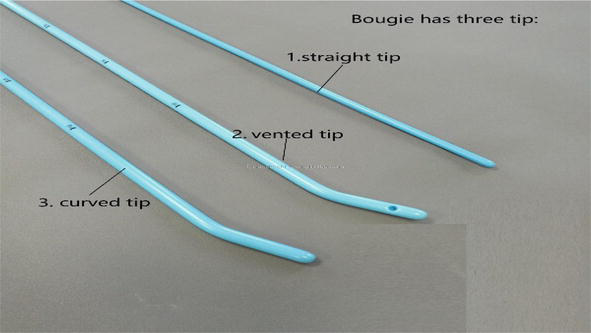
3.6.3 Bougie and stylets
When the larynx is only partially visualized or hidden behind the epiglottis at direct laryngoscopy, and may be difficult to reach with the normal curvature of an endotracheal tube, intubation may then be accomplished by either (Figures 13–16).
Altering the curvature of the ETT using a malleable plastic coated metal Stylet.
Inserting a long thin Gum Elastic Bougie (GEB) and using this as a guide over which the tube may be railroaded into the trachea.
Figure 13.
Polio Macintosh laryngoscope.
Figure 14.
Video laryngoscope.
Figure 15.
Intubating stylets of different sizes(Fr).
Figure 16.
Gum elastic Bougie.
3.6.4 Lightwand
It is an illuminated stylet which is introduced into the ETT and the tip of the tube is directed into the trachea guided by transillumination of neck tissues.
Lighwand tracheal intubation is a suitable method for difficult intubation in patients with
Restricted cervical spine movement
Limited mouth opening
Orofacial distortion
Unexpected failed intubation
3.6.5 Fibreoptic bronchoscope guided intubation
Fiberoptic bronchoscopes are currently used to facilitate endotracheal intubation via either the nasal or oral route (Figure 17). In clinical scenarios in which tracheal intubation is deemed necessary and mask or supraglottic ventilation (e.g., via a laryngeal mask airway [LMA]) is unlikely to be successful or poses an aspiration risk, awake FOI is a standard approach. FOI remains the accepted standard in emergency airway management of a patient with an anticipated difficult airway. FOI is ideally suited in such patients because intubation can be performed prior to the induction of anesthesia with its attendant risks of inadequate ventilation and oxygenation, loss of upper airway patency, and failed intubation. This FOI technique also safeguards against the risk of the cannot intubate/cannot ventilate scenario (Figure 18) [12].
Figure 17.
Lightwand.
Figure 18.
AMBU fiberoptic bronchoscope.
3.6.6 Supraglotic airway guided intubation
Supraglottic device aids intubation by establishing initial airway, then guides endotracheal tube. Ensures clear, protected ventilation passage. Useful in challenging laryngoscopy or difficult airways. Effective alternative for secure intubation in clinical scenarios (Figure 19) [13].
Figure 19.
Intubation via LMA Fastrach(above) and AIR-Q LMA(below).
Broadly, the indications for intubating a patient can be remembered and categorized by the mnemonic:
Airway Compromise. When other methods fail to maintain a clear airway, and there is a risk of airway obstruction or compromise. This may occur in cases of inhalation injury, facial fractures, or retropharyngeal haematoma. In cases of dynamic airway early intubation is the key point.
Bullets: Neck trauma
Bites: Anaphylaxis/Angioedema
Burns: Thermal and caustic airway injury
Breathing. Inadequate Oxygenation or Ventilation: When the patient cannot achieve sufficient oxygenation through the use of a face mask and supplemental oxygen, or when there is apnea (cessation of breathing).
Circulation. Inadequate Circulation & Cerebral Hypoperfusion: To enhance tissue oxygen delivery by relieving the respiratory muscles. This is necessary when the patient is experiencing decreased mental status or combativeness due to reduced blood flow to the brain.
Disability. CNS Depression due to any reason like Head Injury, CNS catastrophes, etc. In cases where the patient has a Glasgow Coma Scale (GCS) score of 8 or less, indicating severe obtundation resulting from a head injury. This may also be necessary in situations of prolonged seizure activity, neuromuscular weakness, or to protect the airway from aspiration of blood or vomit.
Expected course. Anticipated deterioration in the patient’s condition or transfer to radiology or another institution.
Feral. The need for immediate aggressive sedation to protect the patient/others.
Algorithms are there for managing the airway, they provide a basic pathway for different intubation scenarios. It is vital that all clinicians who attempt intubation be familiar with the equipment and techniques necessary for successful intubation (Figures 20–22).
It is a technique of intubation where in the airway is secured quickly and safely while reducing the risk of aspiration. Rapid sequence intubation is the standard method in emergency airway management for patients without an anticipated difficult airway.
Classic Rapid Sequence Intubation (RSI) and Modified RSI are two approaches to securing the airway in emergency and critical care settings. In Classic RSI, a standardized drug sequence, typically involving a rapid-acting induction agent followed by succinylcholine, is used, often with the application of cricoid pressure. In contrast, Modified RSI is more flexible, allowing for variations in drug choices and their order based on the patient’s condition and provider’s judgment. It may include positive pressure ventilation before paralysis and may avoid cricoid pressure. The choice of paralytic agents can also differ, with non-depolarizing agents like rocuronium sometimes preferred. Modified RSI emphasizes individualized care and adaptability to the clinical context, while Classic RSI follows a more standardized protocol. The approach chosen depends on factors such as patient condition, clinician expertise, and local protocols.
6.1 Conduct of RSI
Preparation
Pre oxygenation
Intravenous anesthesia induction
Cricoid pressure/Sellick’s maneuver (The esophagus is blocked in an extended neck by pressing the cricoid cartilage against the 5th cervical vertebra. Apply 10–40 N (1–4 kg) pressure using thumb and index finger post-induction until intubation and cuff inflation. Contraindicated in patients suspected with cervical spine injury or laryngeal injury [14]).
Laryngoscopy followed by intubation after the requisite time has elapsed or by observing fasciculations.
Confirmation of correct tube placement by 4 phase capnography waveform for at least 5 breaths or auscultation of chest.
Delayed Sequence Intubation (DSI) is a specialized airway management technique used in emergency medicine and critical care when traditional rapid sequence intubation (RSI) may not be immediately feasible or safe. DSI is employed to optimize the patient’s oxygenation and ventilation before initiating RSI. It is typically employed in cases where the patient presents with severe respiratory distress, hypoxemia, or impending respiratory failure. These situations may include agitated or combative patients who cannot cooperate with the standard RSI procedure (Figure 23) [15].
Crash airway refers to patients in cardiopulmonary arrest, deep coma or near death who cannot maintain their ventilation and oxygenation (Figures 24–26).
Before performing intubation, it is crucial to position your patient correctly. Unless your patient is undergoing chest compressions due to cardiac arrest, optimizing the positioning prior to intubation is essential. Improved positioning enhances your view and increases the likelihood of a successful intubation on the first attempt, minimizing the risk of complications. Elevate the patient to the operator’s xiphoid level for optimal positioning. While ventilation and intubation are typically done with the patient lying flat on their back, aligning the external ear with the sternal notch may enhance the visibility of the glottis. Avoid using padding under the shoulders or neck as this position is not ideal for facilitating emergency intubation. The goal of laryngoscopy is to align the oral, pharyngeal, and laryngeal axes to achieve a clear and unobstructed view of the glottis, enabling the passage of the endotracheal tube (ETT) between the vocal cords.
11.1 Scenario 1: Normal body position and the sniffing position
Positioning theory is centered on aligning three axes: the oral axis (OA), pharyngeal axis (PA), and laryngeal axis (LA). When a patient lies flat, their OA guides your line of sight to the oropharynx. In the sniffing position, achieved by using towels or blankets to flex the cervical spine and align the external auditory meatus with the sternal angle, these three axes come into alignment. This reduces the force needed to clear the glottis opening during intubation (Figure 27) [16].
Figure 27.
Normal body position and the sniffing position.
11.2 Scenario 2: the overweight patient and the ramp
Overweight patients need special positioning attention, especially for the sniffing position due to excessive force for pharyngeal tissue displacement. Their heavier chest wall poses ventilation challenges and shortens safe apnea time. Elevating the torso with a ramp, using linens or pillows, helps slide chest wall tissues, improving preoxygenation and extending desaturation time. The ramped position, with the head at a 30-degree angle and the ear canal level with the sternum, benefits obese patients during intubation, as research shows advantages regardless of body mass index (BMI) (Figure 28) [17].
Figure 28.
The ramp position.
12. Pre intubation optimisation of oxygenation
When oxygen falls below 70%, it raises risks like dysrhythmias, decompensation, and cardiac arrest (Table 1). Pre-oxygenation removes alveolar nitrogen, creating an oxygen reserve, preventing hypoxia. In healthy patients, it extends safe apnea time to 8 minutes, but it’s shorter for critically ill patients. Start preoxygenation before intubation, administering 100% oxygen for ≥3 mins at ≥15 L/min. Adjust the regulator to maximum “flush” for 90–97% oxygen at 40-60 L/min. Use tidal volume breathing with a proper seal. If >95% O2 is not achieved, consider bag-valve-mask ventilation, PEEP valves, or CPAP. Tilting the head 20–30 degrees upward enhances preoxygenation. For agitated patients, consider sedation or induction agents. During laryngoscopy, high-flow oxygen maintains airflow from the pharynx to the lungs [18].
Device
% Fio2 Obtained
Flow (L/min)
1
Nasal Cannula
24–40%
1–6
2
Face mask
35–60%
5–10
3
Oxymizer
24–45%
1–15
4
Venturi mask
24–50%
2–15
5
Non-rebreather mask
50–90%
10–15
6
High flow nasal cannula
30–100%
15–60
7
BIPAP
35–100%
8
Endotracheal Intubation
35–100%
Table 1.
Various oxygenation delivery devices.
12.1 Bag valve mask ventilation
Bag-valve mask ventilation is essential for airway management by various medical professionals. Techniques like denture retention, beard lubrication, and airway adjuncts aid in challenging situations. It delivers positive pressure ventilation to patients with inadequate breaths, excluding those with total airway obstruction or aspiration risk. Perform with the patient supine and the head in a sniffing position (except for cervical spine injury). Two techniques:
One-person: Seal the mask to the patient’s face using the E-C method.
Two-person: One squeezes the bag, and the other maintains the mask seal, avoiding neck compression and ensuring pressure on bony points. Proper positioning matters; larger masks improve the seal, while smaller ones may leak. Complications can include gastric insufflation leading to vomiting and aspiration (Figures 29 and 30).
Figure 29.
Single rescuer bag mask ventilation (E-C).
Figure 30.
Two rescuer bag mask ventilation.
13. Vortex approach
The Vortex approach to airway management has been designed to assist decision making during airway crisis (Figure 31). It follows the principle that if the non-surgical methods (tracheal intubation, SAD, and facemask ventilation) for achieving alveolar oxygenation fail, there is diminishing time and options available before critical hypoxaemia occurs. If a best effort at any of these is unsuccessful, the ‘CICO status’ is initiated and preparation for eFONA starts, and failure of the best effort in all three should initiate eFONA [19].
Figure 31.
Use of vortex during failed RSI.
14. Emergency front of neck access [eFONA]/surgical airway
About 3% of intubation attempts are challenging, necessitating consideration of a surgical airway when endotracheal intubation fails. In these emergencies, securing the airway is crucial for saving lives. Accessing the airway through the front of the neck typically involves cricothyrotomy (needle, scalpel-bougie, transtracheal catheter, or surgical) or tracheostomy (surgical or percutaneous), with an emphasis on the cricothyroid membrane. This approach is recommended and included in the difficult airway algorithm for situations where other airway management methods have failed, such as “can’t intubate, can’t oxygenate” (CICO) scenarios. It can also be performed electively before anesthesia induction in awake patients with upper airway obstruction, severe injuries, or high CICO risk (Figure 32) [19].
Figure 32.
Approaches for eFONA.
14.1 Scalpel cricothyroidotomy
Using a ‘scalpel-bougie-tube’ technique is recommended by Difficult Airway Society as the first line technique for eFONA and employs a number 10 blade scalpel, a size 6.0 mm cuffed tracheal tube and a bougie for the same. A ‘scalpel-bougie-tube’ technique with a horizontal stab incision of the CTM, followed by bougie insertion and rail roading of ETT through the CTM into the trachea is recommended if the CTM is palpable. If this fails, or the CTM is impalpable, then a 8–10 cm vertical incision followed by a ‘scalpel-finger-bougie-tube’ technique is recommended, wherein blunt dissection with fingers is carried out after skin incision until the CTM is reached, followed by bougie and ETT.
14.2 Needle/seldinger technique
In needle/seldinger technique the trachea is entered with a needle (from commercially available sets) connected to a 5 ml syringe containing 2 ml saline with continuous aspiration, a guidewire passed through it and the cricothyrotomy cannula with its dilator then railroaded over it.
14.3 Surgical technique
The surgical technique involves blunt or scalpel dissection till the CTM, followed by its horizontal incision and passage of the cricothyrotomy cannula (commercially available sets).
14.4 Transtracheal catheter technique
The transtracheal catheter technique similarly involves entering the cricothyroid membrane with a cannula and advancing the transtracheal catheter after needle removal.
Cannulas for these techniques can be narrow bore (ID ≤2 mm) or wide bore (ID ≥4 mm). Narrow bore cricothyroidotomy requires high-pressure ventilation for transtracheal jet ventilation (TTJV) and has drawbacks like misplacement, kinking, and barotrauma. It lacks a tracheal cuff and requires conversion to a definitive airway for aspiration protection and PEEP application. Wide bore cricothyroidotomy’s main advantage is enabling conventional ventilation. In the absence of commercial sets, a 14G cannula, a 2 cc syringe barrel, and an 8 mm ETT connector assembly can be used, which can be connected to a breathing circuit or TTJV (Figure 33).
Figure 33.
Transtracheal cricothyrotomy catheter using a 14G cannula,2 cc syringe and 8 mm ETT connector.
15. Airway pharmacology
Airway management, especially endotracheal intubation, requires a deep understanding of airway pharmacology. This procedure can provoke significant physiological responses, like hypertension, tachycardia, increased ICP, and bronchoconstriction. These reactions are usually short-lived but can harm certain patients, such as those with heart disease, cerebral aneurysms, aortic issues, or high blood pressure. Stimulation of the upper airway activates both branches of the autonomic nervous system. In adults, the sympathetic response dominates, increasing catecholamine levels. However, in young children and some adults, it may trigger a vagal response, causing bradycardia. Sedative and hypnotic agents are commonly used to achieve various levels of sedation or anesthesia based on the dose administered [20, 21, 22].
The pharmacology of drugs commonly used in emergency airway management are categorized as:
Sedative/Hypnotic/Induction agents
Muscle Relaxants (Depolarizing and Non-depolarizing Relaxants)
Adjunctive Agents
Rescue drugs (vasopressors and ionotropes)
Neuromuscular Blockade Reversal Agents
16. Post intubation assessment and endotracheal tube care
Confirming endotracheal tube placement traditionally relies on potentially unreliable methods like chest and stomach auscultation (Table 2). To ensure reliability, it’s recommended to use at least two confirmation methods. The primary choice is ETCO2 detectors, with anteroposterior chest radiography as another option. Fiberoptic bronchoscopy provides a “gold standard” view of tracheal rings, and ultrasound can detect tracheal placement and potential unilateral bronchial intubation. Proper endotracheal tube care involves securing it to prevent displacement, maintaining cuff pressure at 25–30 cm H2O to prevent aspiration and air leaks without injuring the airway mucosa, and regular or as-needed suctioning to prevent mucus blockage.
Hypotension, Myocardial depression, Bronchospasm, Avoid in porphyria
Status epilepticus, ↑ICP
Muscle relaxant/paralytic agents
Succinylcholine
1.5–2 mg/kg(i.v), 4–5 mg/kg (i.m)
30–60 sec
5–15 min
↑HR (Adults), ↓HR(Children, 2nd dose), ↑IOP
Rapid onset and offset, hence ideal for RSI.
Hyperkalemia,Precipitate malignant hyperthermia Fasciculations, Myalgia, Increase IOP, Bradycardia may occur after repeated doses
Essentially all patients except those with: Hyperkalaemia, Causes severe hyperkalaemia if used in patients presenting between 5 days-6 months after burns, de-nervation injury, spinal cord injury, stroke
Rocuronium bromide
0.6 mg/kg i.v(allows intubation in 90–120 sec) 1.2 mg/kg, i.v(allows intubation in 60 sec)
60–120 sec
45–70 min
↑HR (at high doses)
Does not have any active metabolites, so better choice for patients requiring prolonged infusions.
Long duration of action
RSI when succinylcholine contraindicated, Rapid reversal with suggamadex.
Atracurium besylate
0.5 mg/kg
90–120 sec
20–45 min
Histamine release can lead to ↓BP & bronchoconstriction
Not metabolized by liver or kidney
Histamine release, Long duration of action
Not recommended for RSI
Vecuronium bromide
0.1–0.3 mg/kg
90–120 sec
45–70 min
Cardiostable
Cardiostable
Long duration of action
Not recommended for RSI
Adjunctive agents
Lidocaine
1–1.5 mg/kg(i.v)
1–3 mins
∼20 mins
Lidocaine will help protect the patient from increases in intracranial pressure, pressor response or cough reflex to intubation
Local anesthetic systemic toxicity (if given in high dose)
Head injury, traumatic brain injury, elevated ICP, To be given 2–3 mins before intubation.
Fentanyl
0.5–2 mcg/kg
2–3 min
30–60 min
↓HR, ↓Ventilation
Blunt sympathetic response to intubation, Relatively cardio-stable, Analgesia, Cough suppression
Respiratory depression, chest wall rigidity at high doses
Fentanyl helps decrease catecholamine discharge secondary to intubation,to be given 2–3 mins before intubation.
Tachyphylaxis(usually seen after ∼30 mg given), C/I in the presence of MAO inhibitors
Hypotension
Phenylephrine
Given as boluses of 50–100 mcg i.v
<1 min
5–10 min
↑ BP, ↓HR (reflex)
Direct stimulation of α receptor, ↑coronary pressure without chronotropic effects(useful in cardiac patients)
Bradycardia
Hypotension
Atropine
0.2–0.6 mg i.v (adult), 20 mcg/kg(children)
<1 min
20–30 min
↑HR, Bronchodilation, miosis
Antiemetic, Antisialagogue
Crosses BBB causing central anticholinergic syndrome,
Bradycardia, Treatment of organophosphate poisoning.
Neuromuscular blockade reversal agents
Neostigmine
0.04–0.08 mg/kg i.v
1.5–3 min
4 hrs
↓HR, Bronchoconstriction, ↑ secretions, ↑ peristalsis (mixed with glycopyrolate(0.2 mg per mg of neostigmine) to negate the undesirable cholinergic effects)
Cholinesterase inhibitor
At high doses causes desensitization of post synaptic acetylcholine receptors l/t flaccid paralysis with respiratory failure
Reversal of neuromuscular blockade caused by non-depolarising muscle relaxants
Sugammadex
Moderate block: 2 mg/kg i.v, Deep block: 4 mg/kg i.v, Immediate reversal from RSI: 16 mg/kg i.v
Cardio stable
Reversal of neuromuscular blockade can be performed as quickly as 3 minutes of administration of rocuronium.
Anaphylaxis <1%
Reversal of neuromuscular blockade caused by rocuronium and vecuronium.
Table 2.
Airway pharmacology.
17. Post intubation hypotension (PIH)
Post-intubation hypotension (PIH) is defined as a decrease in systolic blood pressure (SBP) to ≤90 mmHg, a drop of ≥20% from baseline SBP, a decrease in mean arterial pressure (MAP) to ≤65 mmHg, or initiation of vasopressors within 30 minutes post-intubation. Risk factors for PIH include a high pre-intubation shock index, chronic renal disease history, intubation for acute respiratory failure, advanced age, lower MAP before intubation, neuromuscular blockers use, or complications during emergent intubation. To reduce PIH risk, preload with a fluid bolus pre-intubation, use hemodynamically stable drugs like ketamine or reduced-dose etomidate, avoid pretreatment drugs like fentanyl and lidocaine that blunt sympathetic tone, set tidal volume at 6–8 ml/kg with low PEEP, insert a nasogastric tube for stomach decompression, and administer vasopressors before intubation [23].
18. Post intubation cardiac arrest (PICA)
Cardiac arrest within 60 minutes of intubation is a severe complication, alongside failed intubation, esophageal intubation, aspiration, hypoxia, and post-intubation hypotension (PIH). It occurs in about 4% of ER cases with high in-hospital mortality, even after achieving spontaneous circulation. Risk factors include multiple intubation attempts, a high intubation-related shock index (>0.9), neuromuscular blockers use, and pre-intubation vasopressors. Patients may struggle with reduced preload and venous return due to increased intrathoracic pressure during positive pressure ventilation. Additionally, physiological changes in severe diseases like acidosis can worsen with intubation and positive pressure ventilation, while sedatives and neuromuscular blockers inhibit stress-induced catecholamine secretion [23].
19. Special circumstances
19.1 Children
Pediatric airways differ significantly from adults, being narrower, softer, and more prone to obstruction due to smaller anatomy and a different larynx position. Children have a higher risk of rapid desaturation and complications like laryngospasm. To manage their airways effectively, careful assessment, specialized equipment, and techniques are essential. Microcuff endotracheal tubes and length-based resuscitation tapes help determine proper equipment sizes. Children’s increased oxygen demand and lower reserve make them vulnerable to rapid hypoxia, especially the younger ones. Avoiding multiple intubation attempts is crucial, and while rapid sequence intubation is effective, awake intubation with retained spontaneous respiration is common in children [24].
19.2 Pregnancy
Airway management in pregnant women is complex due to physiological and anatomical changes that occur during pregnancy (Table 3). These changes affect both the technical and physiological aspects of airway management. Laryngoscopy becomes more challenging, and there may be a need for smaller-sized endotracheal tubes. The risks of airway bleeding, desaturation, and aspiration increase. It is crucial to optimize all factors involved to ensure success on the first attempt. The use of a short handle direct laryngoscope may be preferred, and the consideration of a bougie is recommended. Preoxygenation, positioning with a 20-to-30-degree head-up tilt, and apneic oxygenation can help further reduce the risk of desaturation. Additionally, uterine displacement through left lateral tilt can be beneficial in preventing supine hypotension syndrome [25].
Pediatric
Adult
Tongue
Relatively larger
Relatively smaller
Larynx
Opposite 2nd & 3rd cervical vertebrae
Opposite 4th & 5th cervical vertebrae
Epiglottis
“U” shaped and short
Spade shaped,flat,erect,flexible
Hyoid/ Thyroid sepration
Very close
Further apart
Glottis
½ cartilage
¼ cartilage
Arytenoids
Inclined inferiorly
Horizontal
Vocal cords
Concave
Horizontal
Cricoid
Plate forms funnel
Plate and vertical
Smaller diameter
Cricoid ring
Vocal cord aperture
Consistency of cartilage
Soft
Firm
Shape of head
Pronounced occiput
Flatter occiput
Table 3.
Differences between pediatric and adult airway.
19.3 Obesity
Obesity affects airway control by reducing space in the pharyngeal tissues and increasing upper airway resistance. It also leads to restrictive lung disease with decreased functional residual capacity (FRC), lung compliance, and alveolar hypoventilation. To manage obese patients’ airways effectively, it’s essential to position them with an elevated head before intubation, promoting lung expansion, increasing FRC, and oxygen reserve. For obese patients with obstructive sleep apnea undergoing bariatric surgery, the sitting position is recommended for preoxygenation. Due to their heightened risk of rapid desaturation after anesthesia induction, non-invasive positive pressure ventilation (NIPPV) can be used to enhance preoxygenation and extend desaturation time. Implementing head-elevated preoxygenation is crucial for optimal results [11].
19.4 Elevated intracranial pressure
In patients with suspected elevated intracranial pressure (ICP), improper airway management can lead to secondary brain injury and poor neurological outcomes. To mitigate ICP increase, rapid sequence intubation (RSI) should prioritize normocapnia, oxygenation, and blood pressure control. Proper choice of induction agents, sedatives, and analgesia is crucial. Maintain a target partial pressure of carbon dioxide (PaCO2) between 35 and 45 mmHg to avoid cerebral vasodilation and elevated ICP. End-tidal CO2 (ETCO2) can guide normocapnia and prevent hypo- or hyperventilation. Hyperventilation is a last resort for acute ICP rise. Preoxygenation and bag valve mask ventilation should aim for oxygen saturation above 94%. Lowering the bed’s head should be minimal and brief, with post-intubation elevation to at least 30° to aid cerebral venous drainage. Etomidate is suitable for brain injury due to minimal hemodynamic effects, and opioid fentanyl pretreatment helps prevent sympathetic responses. Propofol reduces ICP but can cause hypotension, while ketamine is now considered safe with favorable hemodynamics. Succinylcholine and rocuronium are common neuromuscular blockers; succinylcholine’s ICP increase is no longer significant, offering rapid onset and shorter duration, facilitating quicker neurological evaluation. Rocuronium, ideal in hyperkalemia risk, has no known ICP effects [26].
20. Role of ultrasound in airway management
Upper airway ultrasound, as a valuable and noninvasive point-of-care ultrasound (POCUS) technique, offers simplicity, portability, and usefulness in evaluating airway management, even in cases where the anatomy is distorted by pathology or trauma. By visualizing important structures such as the thyroid cartilage, epiglottis, cricoid cartilage, cricothyroid membrane, tracheal cartilages, and esophagus, clinicians gain a better understanding of the applied sonoanatomy. This empowers them to utilize ultrasound for various purposes, including assessing difficult intubation, determining appropriate depths for endotracheal tube (ETT) and laryngeal mask airway (LMA) placement, evaluating airway size, guiding invasive procedures like percutaneous needle cricothyroidotomy and tracheostomy, predicting postextubation stridor, determining the appropriate size for left double-lumen bronchial tubes, and detecting upper airway pathologies [27].
21. Conclusion
In conclusion, airway management is a vital aspect of emergency care that saves lives and minimizes complications. This chapter emphasized a systematic approach to assess airway issues through signs, symptoms, patient history, and examination. It highlighted various intervention techniques, from basic maneuvers to advanced procedures, ensuring a clear airway and adequate oxygenation. Equipment selection, including laryngoscopes, tubes, and adjuncts, was discussed with a focus on understanding their indications and limitations. Continuous training and practice are crucial for maintaining proficiency. This chapter offers a comprehensive overview, equipping professionals with the knowledge and skills to approach emergencies confidently. In summary, airway management is a dynamic field requiring a multidisciplinary approach and strong understanding of assessment, intervention techniques, and equipment use, ultimately improving emergency care and patient outcomes.
Acknowledgments
I express deep gratitude to those who significantly contributed to this chapter. First, I thank my father, Dinesh Kumar Dhir, for his unwavering support and belief in my abilities. To my mother, Neelam Dhir, I appreciate your strength and boundless love. My wife, Sonam Dhir, has been my anchor, and her encouragement fuels my drive for excellence. Dr. Susheela Taxak, my teacher, has been pivotal in my academic growth, and her mentorship is invaluable. I also thank my coauthors Dr. Mayank Dhir and Dr. Garima Jain for their support and feedback. Your contributions shaped my thoughts and ideas. I’m profoundly grateful to all of you for being integral to my journey.
1.Goto T, Goto Y, Hagiwara Y, Okamoto H, Watase H, Hasegawa K. Advancing emergency airway management practice and research. Acute Medicine & Surgery. 2019;6(4):336-351. DOI: 10.1002/ams2.428
2.Chou HC, Wu TL. Large hypopharyngeal tongue: A shared anatomic abnormality for difficult mask ventilation, difficult intubation, and obstructive sleep apnea? Anesthesiology. 2001;94:936-937
3.Benumof JL. Obstructive sleep apnea in the adult obese patient: Implications for airway management. Anesthesiology Clinics of North America. 2002;20:789-811
4.Isono S. Obesity and obstructive sleep apnoea: Mechanisms for increased collapsibility of the passive pharyngeal airway. Respirology. 2012;17:32-42
5.Weibel ER. Geometry and dimensions of airways of conductive and transitory zones. In: Morphometry of the Human Lung. Berlin, Heidelberg: Springer; 1963. pp. 110-135
6.Myatra SN, Shah A, Kundra P, Patwa A, Ramkumar V, Divatia JV, et al. All India difficult airway association 2016 guidelines for the management of unanticipated difficult tracheal intubation in adults. Indian Journal of Anaesthesia. 2016;60(12):885-898. DOI: 10.4103/0019-5049.195481
7.Khan RM, Sharma PK, Kaul N. Airway management in trauma. Indian Journal of Anaesthesia. 2011;55(5):463-469. DOI: 10.4103/0019-5049.89870
8.Rosenberg MB, Phero JC, Becker DE. Essentials of airway management, oxygenation, and ventilation: Part 2: Advanced airway devices: Supraglottic airways. Anesthesia Progress. 2014 Fall;61(3):113-118. DOI: 10.2344/0003-3006-61.3.113
9.Gerstein N, Braude D, Hung O, Sanders J, Murphy M. The Fastrach (TM) intubating laryngeal mask airway (R): An overview and update. Canadian Journal of Anaesthesia = Journal Canadien D’anesthésie. 2010;57:588-601. DOI: 10.1007/s12630-010-9272-x
10.Passi Y, Sathyamoorthy M, Lerman J, Heard C, Marino M. Comparison of the laryngoscopy views with the size 1 miller and Macintosh laryngoscope blades lifting the epiglottis or the base of the tongue in infants and children <2 yr of age†. British Journal of Anaesthesia. 2014;113:869-874. DOI: 10.1093/bja/aeu228
11.Lotia S, Bellamy MC. Anaesthesia and morbid obesity. Continuing Education in Anaesthesia Critical Care & Pain. 2008;8(5):151-156. DOI: 10.1093/bjaceaccp/mkn030
12.Ramkumar V. Preparation of the patient and the airway for awake intubation. Indian Journal of Anaesthesia. 2011;55(5):442-447. DOI: 10.4103/0019-5049.89863
13.Wong DT, Yang JJ, Mak HY, Jagannathan N. Use of intubation introducers through a supraglottic airway to facilitate tracheal intubation: A brief review. Canadian Journal of Anaesthesia. 2012;59(7):704-715. DOI: 10.1007/s12630-012-9714-8 Epub 2012 Jun 1
14.Ehrenfeld JM, Cassedy EA, Forbes VE, Mercaldo ND, Sandberg WS. Modified rapid sequence induction and intubation: A survey of United States current practice. Anesthesia and Analgesia. 2012;115(1):95-101. DOI: 10.1213/ANE.0b013e31822dac35 Epub 2011 Oct 24
15.Weingart SD. Preoxygenation, reoxygenation, and delayed sequence intubation in the emergency department. The Journal of Emergency Medicine. 2011;40(6):661-667. DOI: 10.1016/j.jemermed.2010.02.014 Epub 2010 Apr 8
16.Sahay N, Samaddar DP, Chatterjee A, Sahay A, Kant S, Ranjan A. Sniff to see. Comparing sniffing position versus simple head extension position for glottic exposure - a prospective, randomized cross over study. Journal of Health Specialties. 2016;4:212. DOI: 10.4103/2468-6360.186503
17.Hassan EA, Baraka AAE. The effect of reverse Trendelenburg position versus semi-recumbent position on respiratory parameters of obese critically ill patients: A randomised controlled trial. Journal of Clinical Nursing. 2021;30(7–8):995-1002. DOI: 10.1111/jocn.15645 Epub 2021 Jan 25
18.Chiang TL, Tam KW, Chen JT, et al. Non-invasive ventilation for preoxygenation before general anesthesia: A systematic review and meta-analysis of randomized controlled trials. BMC Anesthesiology. 2022;22:306. DOI: 10.1186/s12871-022-01842-y
19.Price TM, McCoy EP. Emergency front of neck access in airway management. BJA Education. 2019;19(8):246-253. DOI: 10.1016/j.bjae.2019.04.002 Epub 2019 Jun 14
20.Consilvio C, Kuschner W, Lighthall G. The pharmacology of airway management in critical care. Journal of Intensive Care Medicine. 2011;27:298-305. DOI: 10.1177/0885066611402154
21.Lindsay S, Benger J. Pharmacology of emergency airway drugs. In: Burtenshaw A, Benger J, Nolan J, editors. Emergency Airway Management. Cambridge: Cambridge University Press; 2015. pp. 63-79. DOI: 10.1017/CBO9781107707542.009
22.Ghatehorde NK, Regunath H. Intubation Endotracheal Tube Medications. Treasure Island (FL): StatPearls Publishing; 2023 Available from: https://www.ncbi.nlm.nih.gov/books/NBK459276/
23.Althunayyan SM. Shock index as a predictor of post-intubation hypotension and cardiac arrest; a review of the current evidence. Bull Emerg Trauma. 2019;7(1):21-27. DOI: 10.29252/beat-070103
24.Harless J, Ramaiah R, Bhananker SM. Pediatric airway management. International Journal of Critical Illness and Injury Science. 2014;4(1):65-70. DOI: 10.4103/2229-5151.128015
25.Tolga Saracoglu K, Cakmak G, Saracoglu A. Airway management during pregnancy and labor. In: Special Considerations in Human Airway Management. London, UK: IntechOpen; 2021. DOI: 10.5772/intechopen.96476
26.Khandelwal A, Bithal PK, Rath GP. Anesthetic considerations for extracranial injuries in patients with associated brain trauma. Journal of Anaesthesiology Clinical Pharmacology. 2019;35(3):302-311. DOI: 10.4103/joacp.JOACP_278_18
27.Osman A, Sum KM. Role of upper airway ultrasound in airway management. Journal of Intensive Care. 2016;4:52. DOI: 10.1186/s40560-016-0174-z
Written By
Gaurav Dhir, Mayank Dhir and Garima Jain
Submitted: 30 June 2023Reviewed: 05 July 2023Published: 09 November 2023
 Open access peer-reviewed chapter
Open access peer-reviewed chapter