Open Access is an initiative that aims to make scientific research freely available to all. To date our community has made over 100 million downloads. It’s based on principles of collaboration, unobstructed discovery, and, most importantly, scientific progression. As PhD students, we found it difficult to access the research we needed, so we decided to create a new Open Access publisher that levels the playing field for scientists across the world. How? By making research easy to access, and puts the academic needs of the researchers before the business interests of publishers.
We are a community of more than 103,000 authors and editors from 3,291 institutions spanning 160 countries, including Nobel Prize winners and some of the world’s most-cited researchers. Publishing on IntechOpen allows authors to earn citations and find new collaborators, meaning more people see your work not only from your own field of study, but from other related fields too.
To purchase hard copies of this book, please contact the representative in India:
CBS Publishers & Distributors Pvt. Ltd.
www.cbspd.com
|
customercare@cbspd.com
The major objective of any pharmacotherapeutic activity is to achieve an effective concentration of drug at a particular site of action for a sufficient period of time to produce a desired response or effect. The eye is a very important organ of the body because of its use in vision as well as its easy accessibility. Though solution-type drug delivery to the eye records high patient adherence but it is limited by poor ocular bioavailability due to certain pre-corneal physiological and anatomical obstacles. Hydrogels are important self-assembly nanoformulations that serve as alternatives to solution-type eye preparations with good potential to produce enhanced local absorption and bioavailability in the treatment of eye disorders that may be vision-threatening. This chapter will present an overview of the eye anatomy, ocular barriers, hydrogels and their classes, applications in ocular diseases, and future prospects of hydrogels in ophthalmic therapeutics.
Department of Pharmaceutical Sciences and Technology, Institute of Chemical Technology, Mumbai, India
Department of Pharmaceutics and Pharmaceutical Technology, Faculty of Pharmaceutical Sciences, Nnamdi Azikiwe University, Awka, Anambra State, Nigeria
Emmanuel Uronnachi
Department of Pharmaceutics and Pharmaceutical Technology, Faculty of Pharmaceutical Sciences, Nnamdi Azikiwe University, Awka, Anambra State, Nigeria
Drug Delivery System Excellence Centre, Faculty of Pharmaceutical Sciences, Prince of Songkhla University, Thailand
Abhit Nayak
Department of Pharmaceutical Sciences and Technology, Institute of Chemical Technology, Mumbai, India
Tochukwu Okeke
Department of Pharmaceutics and Pharmaceutical Technology, Faculty of Pharmaceutical Sciences, Nnamdi Azikiwe University, Awka, Anambra State, Nigeria
Purav Shah
Thoroughbred Remedies Manufacturing, TRM, Industrial Estate, Newbridge, Co Kildare, Ireland
Vandana Patravale*
Department of Pharmaceutical Sciences and Technology, Institute of Chemical Technology, Mumbai, India
*Address all correspondence to: ec.umeyor@unizik.edu.ng and vb.patravale@ictmumbai.edu.in
1. Introduction
The eye is an important organ of the body due to its prominent role as the centre of vision which helps to keep the body safe from physical injury and harm. Sometimes, the visual functions of this vital organ is compromised by a variety of pathologic conditions and injuries such as bacterial or fungal infections, vascular diseases of the retina, inflammatory diseases, tumors, glaucomatous neuropathies, cataract, dry eye, and macular degeneration, which may lead to impaired or total loss of vision [1]. Various ophthalmic interventions including solutions, drops, emulsions, gels, lubricants, ointments, films, and implants incorporating small drug molecules and peptides have been designed, developed, and applied for the clinical management of these ocular pathologies [2]. The pros and cons of these treatment strategies have been reviewed and discussed in several reports. The major concern raised in these reports is the negative impact of the lacrimal drainage and tear dilution system of the eye on drug delivery because they facilitate rapid clearance of applied therapeutics resulting in decreased pre-corneal retention time, low bioavailability, and poor therapeutic outcome [3]. To advance efficient ocular drug delivery for alleviation or elimination of these conditions, researchers have focused their interests in the fabrication of bioinspired delivery systems using materials that have the ability to maintain prolonged contact with the compromised visual architecture of the eye. This would ensure that the long term treatment goals of topical drug administration to the eye are realized. The topical route is one of the easiest and commonest routes of drug administration. However, topical ocular delivery mostly favors the anterior segment of the eye with little or no impact felt in the posterior eye due to poor accessibility and the complexities of the physiological and anatomical structures of the eye. In addition, increasing the dose by intravitreal or intravenous administration will increase toxicity risks due to the possibility of drug uptake in the conjuctiva and systemic dose dumping through the nasolacrimal pathway [4]. Therefore, the ultimate objective of innovative biomimetic delivery systems like liposomes, nanotubes, nanoparticles, micelles, contact devices, hydrogels, and dendrimers, is to improve permeation, surface contact, pre-corneal retention time, and deposition of encapsulated payloads to both the anterior and posterior segments of the eye.
Hydrogel is a hydrophilic drug delivery platform fabricated into a three-dimensional array using swellable polymers which possess excellent water absorption and retention capacity. The concept of hydrogel was first hinted in the late nineteenth century while an attempt to formerly describe it was made in the early twentieth century using a ternary system comprising water, alcohol, and gelatin [5]. With recent advances in the chemistry of polymer synthesis, smart and stimuli-reactive hydrogels have been synthesized incorporating drugs, genes, biologics, and other small molecules for targeted ophthalmic therapy by enhanced co-administration of drugs, prolonged contact and residence times at the target site, and controlled drug release in the ocular tissue [6]. Often, hydrogels have been synthesized to serve as the core carrier system for other nanoparticulate systems like solid lipid nanoparticles, lipid nanoemulsions, liposomes, or nanostructured lipid carriers for therapeutic purposes. Their properties could be tuned by covalent or physical crosslinking of ligands and molecules to improve their surface, mechanical, retention, safety, stimuli-responsive, and targeting profiles [7]. This chapter will present an overview of the eye anatomy, ocular barriers to drug delivery, discuss different classes of hydrogels and their fabrication techniques, explore mechanisms of drug entrapment in hydrogels and their biocompatibility with the eye, applications of hydrogels in ocular diseases, challenges in hydrogels translation for ocular application, and future prospects of hydrogels in ophthalmic therapeutics.
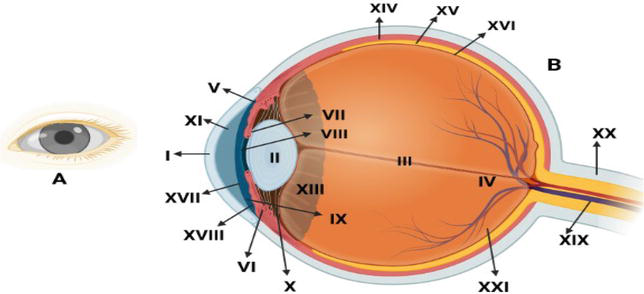
The eye is structured into two distinct parts: the anterior and posterior parts of the eye. The anterior eye comprises the cornea, iris, conjuctiva, crystalline lens, aqueous humor, and ciliary body, whereas the posterior portion of the eye is made up of the neural retina, choroid, retinal pigment epithelium, vitreous humor, and the sclera. The accessory structures of the eye include the eyelids, eyelashes, eyebrows, the lacrimal (tear-producing) apparatus, and extraocular muscles. The eyeball is rooted into the cranium and its movement is regulated by the extraocular muscles (Figure 1) [8, 9].
Figure 1.
(A) Frontal view of the human eye. (B) Illustration of the anatomical structures of the eye: I—cornea; II—lens; III—vitreous body; IV—optic disc; V—conjunctival fornix; VI—sclera; VII—iris; VIII—anterior chamber; IX—iridocorneal angle; X—ciliary body; XI—meibomian glands; XII—posterior chamber; XIII—suspensory ligament; XIV—choroid; XV—retinal pigmented epithelium; XVI—retina; XVII—palpebral conjuctiva; XVIII—bulbar conjunctiva; XIX—central artery and vein of the retina; XX—optic nerve; XXI—fovea.
2.1 Anterior eye
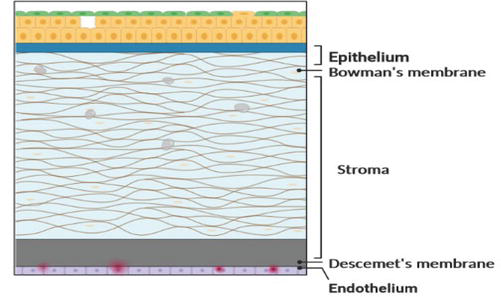
The cornea is the most sensitive, highly specialized, and innervated tissue of the anterior eye which measures 10.5 by 11.5 mm in a normal healthy adult. The cornea is stratified into the epithelium, lamellar stroma, Bowman’s layer, Desçemet’s membrane, and endothelium. The stroma supports the mechanical structure of the cornea. The epithelium serves as a barrier to the permeation of toxins into the ocular intracellular chamber. The Bowman’s layer or membrane lack cells, does not regenerate and forms scars when damaged. The Desçemet’s membrane is usually produced by endothelial cells in utero during which it is banded or after birth when it is amorphous or unbanded. The endothelium maintains corneal transparency, dehydration, and clarity necessary for enhanced vision [10]. The conjuctiva has three components with distinct functions—palpebral, forniceal, and bulbar conjunctiva. Forniceal forms a barrier to the exposed eye, and the palpebral conjunctiva holds the eyelids in position. The conjunctiva is responsible for ocular immunity (provided through the conjunctiva-associated lymphoid tissue), motion due to its elastic nature, protection, and lubrication [8]. Conjuctiva epithelium contains Manz glands, mucous glands, Henle crypts, and goblet cells which produce mucin, and electrolytic fluids components of tear film. The cells are present in the palpebral, forniceal, and bulbar conjunctiva [11]. The iris is a brightly colored layer which regulates the amount of light that enters the eye. It serves as the root of formation of the ciliary body, and it makes a spherical impression on the lens, referred to as the pupil, which adjusts its size according to available light, controls light penetration through the retina, and maintains visual acuity [12]. The ciliary body is very closely localized with the iris. The capillaries of the ciliary body facilitates exchange of impulses and sensory information between the anterior and posterior eye. The ciliary body is involved in aqueous humor secretion, and assists the lens to adjust its focus on objects [13]. The aqueous humor is secreted from plasma in the ciliary body at the rate of about 2.5 μL/min through active production, ultrafiltration, and diffusion which ensures effective distribution and draining. The average period of turnover for aqueous humor is about 100 minutes. It is a rich source of glucose, ascorbic acid, globulins, albumin, oxygen, and other essential nutrients for the cornea and crystalline lens, and also evacuates debris, wastes materials, and toxins from these non-vascularized tissues. It is also responsible for the maintenance of intraocular pressure (IOP) and shape of the eye [8]. Crystalline lens is a biconvex, non-innervated ocular tissue that is held in position by the zonula fibers of the ciliary body. The lens controls the transfer of waste products and metabolic materials through diffusion. It is compartmentalized into the nucleus, epithelium, capsule, and cortex [14].
2.2 Posterior eye
The choroid is a vascularized layer located between the sclera and retina which contains mucinated extracellular fluid and melanocytes. The choroid receives a high amount of vascular supply compared to the brain and other parts of the eye. The high blood supply is responsible for excellent supply of nutrients and oxygen to the retina, the removal of metabolic wastes and maintenance of IOP [13]. The normal human eye contains about 3.5 million retinal pigment epithelial cells which converge into a tight junction called zonulae occludentes. These cells proliferate in disease conditions because they produce large amount of growth factors including ciliary neurotropic, vascular endothelial, and platelet-derived growth factors. The cells secrete catalase, melanin pigment, superoxide dismutase, and immunomodulatory enzymes which protect the eye against oxidative damages. It supports the photoreceptor cells (amacrine, rod, cone, bipolar, horizontal, ganglion, interplexiform, and glia cells) to maintain effective vision cycle and control of chemical components of the retina [15]. The sclera (white eye) is a mesh-like continuation of the corneal tissue which contains mucopolysaccharides, fibroblasts, and collagen fibers from the central nervous system. It gives shape to the eyeball, makes it more rigid, protects its inner parts, and serves as a site of attachment for the extrinsic eye muscles [13, 16]. The neural retina is made up of millions of photoreceptor cells mainly rod and cone cells, and facilitates the exchange of sensory information between the brain and the ocular exterior. The rod and cone cells trap visual nerve information which is relayed to the brain through bipolar cells, and support differentiation of colored objects in low and bright light. The vitreous humor (or vitreous body) is rich with water and has negligible amounts of hyaluronic acid and ions, and collagen fibers. The quality of the vitreous body deteriorates with age [13, 15].
Generally, topical drug transport into the cornea is influenced by the pH and degree of ionization of the drug molecules. The cornea presents sufficient permeation obstacle to topical dosage forms due to its physiomechanical features especially its content of epithelial cells [17]. The epithelial cells hinder drug absorption due to their tight adherence to ocular proteins like occludens (Zonula occludens-1 and Zonula occludens-2), and cingulin, forming tight junctions which decrease paracellular transportation of hydrophilic or ionic drugs into the cornea while transcellular-mediated diffusion propels the permeation of hydrophobic drugs. The corneal stroma acts as a barrier to the deep absorption of lipophilic and modest hydrophilic drugs by trapping the molecules as a reservoir. The stroma forms a barrier with endothelium but this obstacle possesses leaky structures which permits the passage of macromolecules. The barrier function of epithelial cells or tight junctions of the cornea is lost in pathologic conditions such as vernal keratoconjuctivitis (Figure 2) [18].
Figure 2.
Ocular drug delivery barriers of the cornea (reproduced from [18] under the terms and conditions of the creative commons attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
3.2 Blood aqueous barrier
This barrier comprises the ciliary epithelium, blood vessels of the ciliary body, and epithelial cells of the iris. These ocular factors form junctions which limit or regulate the access of non-targeted drug molecules to the deep tissues of the eye. Through this mechanism, the tight junctions assist the eye to maintain its homeostatic chemical components and visual clarity [19].
3.3 Conjunctival barrier
Drug uptake through the conjunctiva following topical application is implemented through the transcellular, endocytic, paracellular, and active routes of absorption. However, the transepithelial electrical resistance acts a barrier to drug uptake across the conjunctiva. The paracellular pathway is decorated with tight junctions which act as obstacle to drug absorption. Drug absorption in the conjunctival tissue is also negatively impacted by secretory cells in the tissue. Tear film acts as a barrier to the concentration and bioavailability of drug molecules absorbed in the conjunctiva. Generally, molecular weight and aqueous solubility are two vital determinants of drug uptake in the conjunctiva. Water-soluble drugs with molecular weight < 20 kDa are more likely to be absorbed than molecules with higher molecular weight. Further, conjunctiva is a centre of excellence for the absorption of proteins and peptides such as insulin. Its uptake is facilitated by paracellular mechanism of drug transport due to the leaky microstructure and large surface area of the conjunctiva [19].
3.4 Barrier due to efflux proteins
Efflux proteins located in the lateral or apical region of the cell membrane act as barriers to drug absorption. Two prominent examples include a member of the ABC (ATP-binding cassette) protein known as multi-drug resistant protein, which acts as a barrier to the transport of conjugated and organic molecules, and p-glycoprotein which hinders the absorption of amphipathic drugs. P-glycoprotein 1 has an approximate molar weight of 170 kDa found in polarized cells and it decreases drug permeation in multi-drug resistant cells. It is secreted by ciliary-iris muscles, ciliary epithelium, epithelial cells of the conjunctiva, capillary endothelial cells of the retina, and cornea. Multi-drug resistant protein is an efflux protein with an approximate molar weight of 190 kDa that is prominently found in the kidney, liver, and intestines. Its transporter efficiency is improved when it is conjugated with glucuronides, bile salts, glutathione, sulphate, and cysteinyl leukotrienes [20].
3.5 Nasolacrimal production and drainage
Tear film is made up of mineral salts, lysozymes, water, and antibodies. It aids the eye to produce clear vision, wash off irritants from the eye, lubricates the eye, maintain a strong immune response, and healthy ocular epithelial cells [21]. Topical drops which are instilled to the eye are docked in the cul-de-sac of the conjunctiva and most of them are eliminated into the nasolacrimal ducts through precorneal tear drainage system due to prior adherence of drug to tear proteins, tear dilution, and accelerated drug clearance process. The lacrimal system is the pathway through which tear produced in the eye flow into the nasal cavity, and the system is made up of lacrimal sac, canaliculi, nasolacrimal duct, and puncta. Tear drainage due to reflex blinking (about 6 blinks/min) restricts drug permeation and acts as a barrier to overall drug available for absorption and therapeutic effect. Drug drainage from the precorneal ducts occur within 2 minutes resulting in decreased ocular contact time and low bioavailability of absorbed drug [8].
3.6 Aqueous humor barrier
The flow of aqueous humor in opposite direction to that of drugs instilled topically to the ocular tissue acts as an obstacle to its absolute absorption. In addition, there is increased drainage of hydrophilic drugs into the Schlemm canal through the trabecular mesh. This barrier function which results in the bioavailability of sub-therapeutic concentrations of instilled drugs could be limited by pathologic conditions like pathogenic inflammation of the ocular tissue due to decreased drainage of topically administered drugs. However, this condition restricts the permeation and absorption of drugs administered to the eye through intravitreal injection as already demonstrated in a report using fluorescence-labeled albumin [22].
3.7 Scleral barrier
Sclera barrier is one of the prominent static barriers of the posterior eye. Due to its protective functions, drug transport across the sclera depends on the physicochemical profile, water solubility, molecular weight, and surface charge of the drug molecules. Thus, poor aqueous solubility and increased molecular weight of drug molecules results in limited delivery across the scleral pores and low absorption. Also, drug molecules with opposite surface charge to the negative charge on the scleral pores experience decreased permeation and are entrapped in the pores [23].
3.8 Blood retinal barrier
The blood retinal barrier selectively regulates the transport of drug molecules following periocular or systemic administration to the retina. The barrier has two layers—the outer layer comprising the retinal pigment epithelium (or epithelial cells), and the inner layer which houses the endothelial cells. These layers possess tight junctions (supported by Müller cells and astrocytes) which selectively control the transverse of biomolecules present in the blood into and out of the vitreous environment mainly through a passive transcellular transport system. In this system, permeability of drug molecules is inversely related to the molecular weight of drug as reported in a study using bovine retina. The efficiency of the retinal transport mechanism is maintained by transporter moieties such as organic anion polypeptides, and organic cation and anion transporters, and these transporters play prominent roles in the ocular distribution of proteins, peptides, biologics, and hormones in the retinal milieu [24].
3.9 Hydrogels for ocular therapeutics
Conventional methods of ocular drug delivery which include the use of drops and ointments have faced numerous challenges ranging from poor ocular bioavailability to rapid clearance from administration site. These hindrances are the result of unique physiological features inherent to the eye anatomy. Hydrogels in ocular therapeutics tend to provide cogent solutions to the problems encountered by conventional ocular drug delivery systems. Their ability to attain high biocompatibility, drug loading and bioavailability in the eye make them an ideal choice for ocular drug delivery [25]. Hydrogels are made up of three dimensional polymeric chain networks which have the ability to swell in aqueous solvents and hold other substances such as drugs, proteins, and other molecules. They are so versatile and can be specifically designed to exploit environmental physiological conditions to illicit a predetermined characteristic behavior at the administration site. Hydrogels which possess such ability are called “stimuli-sensitive” hydrogels because they detect physical, chemical or biological changes in physiological conditions and react by altering swelling capacity. This allows for both sustained and controlled release as well as optimal ocular bioavailability [26]. Changes in pH and ion concentrations of the physiological environment make up the chemical factors that influence hydrogel behavior. Other factors such as light pressure, sound and temperature are often referred to as physical stimuli. Hydrogels can also be designed as in situ gelling systems where the hydrogel is liquid before administration and turns to a gel after administration, thus undergoing a sol-gel transition. This involves stimuli sensitivity; therefore, gelation post-administration can occur as a result of changes in pH, temperature, or ion concentration. Fabrication of hydrogels with hydrophobic molecules can be a bit challenging because of the incompatibility existing between the molecules and aqueous contents of hydrogels. However, methods have been developed to integrate such drugs into hydrogels for ocular delivery. Hydrogels for ocular drug delivery are already in use, one of which is the soft disposable contact lens. Soft contact lenses (SCLs) are hydrogels that can increase corneal residence time of ophthalmic drugs thus increasing bioavailability [27]. These lenses are usually made from conventional polymers such as poly-(2-hydroxyethylmethacrylate) (pHEMA), silicone, gelatin, chitosan, hyaluronic acid, alginate, methylcellulose and collagen. Silicone SCLs can be employed for extended use due to increased oxygen permeability. Unlike hydrophobic drugs, hydrophilic drugs can be easily incorporated into SCLs by soaking the already formed SCLs in a solution of such drug. The use of organic solvents to dissolve hydrophobic drugs has been mentioned by some researchers as an effective method to incorporate hydrophobic drugs in SCLs. Latanoprost was loaded in silicone SCLs by soaking the lenses in a solution of latanoprost in n-propanol [28]. Other methods which include the use of colloidal systems such as micelles and microemulsions have also been employed to counteract the solubility challenges of hydrophobic drugs. This, however, may reduce the average light transmission of the hydrogel depending on the globule sizes of the colloidal system [29]. Bimatoprost was loaded in pHEMA SCLs by soaking in drug loaded microemulsion. In vitro release profile of this SCLs showed an extended drug release of up to 48–96 hours which is greater than the release observed in SCLs without microemulsion [30]. Other methods employed to improve drug loading and release form SCLs include molecular imprinting with hydrogels and supercritical solvent impregnation [27]. Molecular imprinting involves the introduction of artificial receptors for the target drug to be loaded on the hydrogels. Hydrophobic drugs like bimatoprost and prednisolone loaded in SCLs with this method have shown increased drug loading capacity and release durations [31]. Supercritical solvent impregnation relies on the unique properties of supercritical fluids to improve the perfusion of the dissolved hydrophobic drug into SCLs. Acetazolamide, an anti-glaucoma drug was incorporated in SCLs using this technique and a drug release duration of 450 minutes was reported [32]. Polymers employed in the fabrication of hydrogels for ocular delivery are biodegradable and do not cause inflammations during use. Chitosan, a cationic polysaccharide derived from chitin possesses mucoadhesive properties as a result of the interaction between its positive charge and the negatively charged mucin [33]. This enables drug permeation and controlled release of drug into the ocular tissues. However, due to its poor alkaline solubility, it is usually modified through PEGylation or carboxymethylation [34]. It can also be combined with other natural or synthetic polymers to optimize ocular drug permeability and release. Hyaluronic acid is another polymer which has shown immense potential in ocular drug delivery because it is a component of the vitreous humor of the eye [35]. It is highly biocompatible and non-immunogenic due to its natural occurrence in the body. However, it cannot form a gel on its own; so for it to be used for hydrogels, it must be either chemically modified or combined with a gelling agent. Gelatin polymeric platforms have also been explored in ocular drug delivery. Timolol hydrogels fabricated with gelatin and chitosan in a study by Song et al. [32] showed greater reduction in intraocular pressure and longer duration of action than the commercially available product. Alginate polymers undergo ion-responsive gelation. They are also biocompatible, biodegradable and not toxic to human tissues. Methylcellulose is also vastly used majorly as a viscosity enhancer in ocular delivery systems and more importantly, it is employed in in situ gelling hydrogel systems because of its heat-induced reversible sol-gel transition property [36].
Hydrogels are formulated by the crosslinking of polymers mainly initiated by physical or chemical means. The different methods for fabrication of hydrogels are discussed below.
4.1 Physical crosslinking
This involves the fabrication of hydrogels through the formation of non-covalent interactions along the polymer chains. These interactions can be as a result of electrostatic interactions, hydrogen bonding, and hydrophobic forces. These hydrogels are called physical gels because their formation was initiated by physical factors; thus, are reversible. They are highly sensitive to water and temperature [37]. They have a short lifespan in the physiological media and are therefore used for short term delivery of drugs. They do not contain toxic chemicals and are quite safe to use. Polymers are mixed together in appropriate conditions and interactions between polymer molecules are initiated. Hydrogels based on polysaccharide polymers such as chitosan are prepared using this method. Chitosan interacts with anionic molecules such as phosphates and sulfates to form physical hydrogels. These anions interact with chitosan through a protonated amino group. The concentration of chitosan as well as its degree of interactions with available anion molecules determine the properties of the hydrogel formed. Other naturally occurring polymers such as alginate and pectin also undergo ionic interactions to form physical hydrogels. Alginate can interact with Ca2+ ions while carrageenan interacts with K+ ions to form physical hydrogels. Melded non-ionic polymers undergoing freeze-thaw cycles can also produce physical hydrogels. The hydrogel is formed possibly as a result of crystallization reaction occurring via hydrogen bonding within the molecules. Polyvinyl alcohol (PVA) aqueous solution transformed into hydrogel after several freeze-thaw cycles and the hydrogel properties were determined by the concentration of the PVA and number of freeze-thaw cycles [38].
4.2 Chemical crosslinking
Unlike physically crosslinked hydrogels, chemically cross linked hydrogels can be easily manipulated to exhibit a pre-determined behavior. They are irreversible because they are formed by covalent interactions between polymer molecules. Physical properties of the chemical hydrogels such as mechanical strength and swelling capacity can be altered to achieve desired results [38]. There are different methods employed in the preparation of hydrogels through chemical cross-linking and they are as follows:
4.2.1 Use of chemical crosslinker
This involves covalent bonds mediated by hydrophilic groups. A schiff base is usually formed indicative of the covalent complexation between polymer chains. These hydrophilic groups usually include the hydroxyl, carboxylic, and amino groups [39].
4.2.2 Crosslinking by addition reaction
This is the reaction of hydrophilic polymers with higher functional crosslinkers to form larger polymer with longer chain length. These crosslinkers, some of which include 1,6-hexamethylenediisocyanate and 1,6-hexanedibromide have been used to crosslink polysaccharides producing hydrogels [40].
4.2.3 Crosslinking with aldehydes
This involves the use of aldehydes to crosslink hydrophilic polymers containing hydroxyl groups. This usually occurs at high temperature and acidic pH with methanol added to quench the reaction. This is observed in the crosslinking of polyvinyl alcohol with glutaraldehyde [41].
4.2.4 Crosslinking by condensation reaction
Reactions between amino or hydroxyl group with derivatives of the carboxylic group have been reported to produce hydrogels. Gelatin hydrogel was prepared using 1-ethyl-3-(3-dimethylaminopropyl)carbodiimide, a good cross-linking reagent for amide groups [42].
4.2.5 Crosslinking through ionizing radiation
Hydrogels can be chemically crosslinked using ionizing radiation. Radiation sources that emit high energy such as electron beam and gamma rays have been reported to polymerize unsaturated substances. Recently, a superabsorbent hydrogel was prepared using gamma radiation and a combination of N, N-dimethylenebisacrylamide, poly(vinylacetate-co-acrylic acid) and gelatin as crosslinking agent [43].
4.2.6 Crosslinking by free radical polymerization
Monomers with low molecular weights can be crosslinked with free radicals. However, crosslinking agents such as ethylenedimethacrylate, N, N′-methylenedi(prop-2-enamide) and melamine triacrylamide still play a role in this process [38]. Hydrogels can also be prepared with the aid of UV polymerization. This technique can be used to create a photoreversible system which allows hydrogels to degrade on exposure to UV light, thus enabling drug release [44].
4.2.7 Crosslinking using enzymes
Enzymes catalyze a number of natural crosslinking reactions resulting in stability in the extracellular matrix (ECM) of human tissue structures. The assemblage of collagen or elastin is catalyzed by lysyl oxidase which enables the formation of aldehydes from lysine present in elastin and collagen molecules. Therefore, the fabrication of hydrogels with the aid of enzyme catalysts have been under continuous study with increasing positive prospects. One of its advantages is that it has the ability to maintain substrate specificity hence reducing the possibility of unwanted side effects. Enzymes which are usually used to crosslink polymers include, tyrosinase, transglutaminase, peroxidase and sortase [45].
4.2.8 Crosslinking by grafting
Some hydrogels possess fragile physical characteristics mostly due to their method of preparation. These hydrogels may be grafted onto strong support structures to improve some of their physical properties. This is common for hydrogels prepared by bulk polymerization. Starch has been grafted with a number of vinyl monomers such as acrylic acid to increase its scope of use. This was achieved by co-polymerization of vinyl monomers with free radicals generated on the surface of starch granules [46].
Hydrogels can be classified in several ways. Some classifications are based on molecular types e.g. natural and synthetic, while others are classified on the basis of composition and function. Based on this latter classification, they can be grouped into nanogels, multifunctional hydrogels, DNA-based hydrogels, stimuli-dependent hydrogels, and hydrogels based on supramolecular systems.
5.1 Nanogels
These are polymeric nanoparticles that are made of crosslinked polymer networks with nanometer sized particulate constituents that swell upon solvent penetration. They consist of polymers of natural origin, synthetic polymers or could be derived from both classes of polymers. They are tunable systems whose characteristics like charge, size, porosity, softness and amphiphilicity can be altered by varying their chemical composition. Nanogels upon swelling, exhibit matrix properties that hold absorbed liquid, and facilitate the diffusion of entrapped solutes into a bulk exterior. They are utilized in the delivery of hydrophobic and hydrophilic drugs, as well as drugs with low and high molecular weights [47]. This is due to their amphiphilic nature in addition to other characteristics of the polymer system like temperature, density of crosslinked gels, concentration of surfactants, and the type of linkage existing in the polymer system. The presence of hydrophobic groups like hydroxyl, amide, and sulphate in their structure, helps to preserve the arrangement of the polymer system upon hydration. The synthesis of nanogels usually proceeds via polymer precursors or polymerization reactions involving monomers. One unique feature of nanogels is their ability to encapsulate more than one bioactive agent in the same carrier. This is due to their hydrophilic characteristic and excellent biocompatibility. Nanogels can be classified using several parameters like responsive behavior: stimuli-responsive and non-responsive; crosslinking: physically crosslinked and chemically crosslinked; and structure: simple, hollow, functionalized, multi-layered, hairy crosslinked, and crosslinked core shell nanogels [48].
5.2 Multifunctional hydrogels
These are composites of hydrogels and other substances like nanomaterials aimed at improving the characteristics of the hydrogel for biomedical usage. Several approaches have been employed in their production including incorporation of nanoparticles into hydrogel matrix, and the addition of a second polymer network to form an interpenetrating network, or double network. Several nanomaterials are utilized in hydrogel synthesis to enhance their mechanical properties. These include: clays, metals, metal oxides, and polymers. These combinations have found uses in different aspects of biomedicine like tissue engineering, drug delivery, wound healing, bioprinting, ocular delivery, and dental therapy [49, 50].
5.3 DNA-based hydrogels
Their pure forms are derived completely from deoxyribonucleotides. Their formation is based on interchain reactions like physical entanglement, enzymatic reactions or hydrogen bonding. Specific features of tunability, specialized responsiveness, and biodegradability make them applicable in drug delivery, biosensing, and biomedical uses. Their hydrophilicity allows the interaction with water molecules to form gel-like DNA-based materials. These DNA-based hydrogels exhibit chemical properties attributable to DNA alongside the physicochemical properties of hydrogels. DNA-based hydrogels can be functionalized with structures like i-motifs, aptamers, and G-quadruplex. DNA-based hydrogels are similar in physical nature to natural substances like chitosan, polyethylene glycols (PEGs) and extracellular matrix. This enables them to be used in several biological applications like scaffolding in tissue engineering, targeted therapy of drugs, and phase separation processes. Due to its chemical robustness, DNA-based hydrogel can be combined with other polymers like chitosan, PEG, poly(lactic-co-glycolic acid) (PLGA), acrylamide and poly(N-Isopropylacrylamide) (PNIPA) to yield hybrid DNA-based hydrogels with desirable properties. Hybrid forms of these hydrogels can be derived from crosslinking which could be physical or chemical in nature. The concentration of the crosslinker and concentration of ions in solution determine the swelling capability of DNA-based hydrogels [51].
5.4 Smart hydrogels
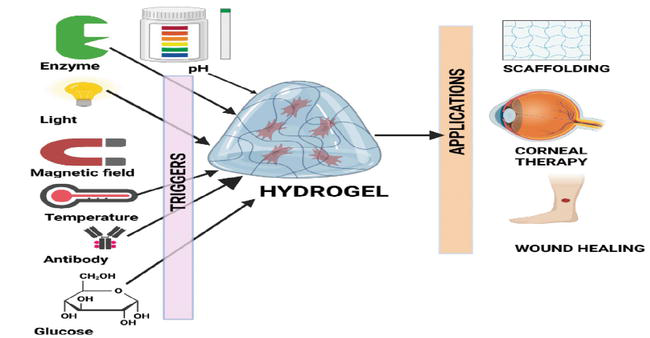
The capacity of hydrogels to respond to external triggers gives rise to the class of hydrogels termed smart hydrogels. These triggers can be physical, chemical or biochemical in nature. Triggers like light, temperature, pressure, electrical, and magnetic fields are physical stimuli. Factors like pH, ionic strength, and chemical agents are chemical stimulants. Biochemical/biomolecular stimuli include glucose, antigens, enzymes, and ligands [52].
5.4.1 Temperature-sensitive hydrogels
These absorb or release water according to the temperature of its environment. The degree of volume change with temperature depends on the relative proportions of their hydrophilic and hydrophobic moieties. These changes are facilitated by alterations in the crosslinking force, hydrogen bonding, and hydrophobic interactions in response to temperature changes. Thermosensitive polymers include: chitosan, agarose and hyaluronic acid which are natural polymers, and synthetic polymers like the poly(N-Isopropylacrylamide) family. They can be classified as positive or negative temperature hydrogels based on their critical solution temperature (CST) [52]. Temperature-sensitive hydrogels have been employed in wound healing [53], tissue regeneration [54], and tumor treatment [55].
5.4.2 Photosensitive hydrogels
These are attractive in biomedicine due to their ability to form hydrogels in situ via polymerization. Photodynamic moieties are inserted into the hydrogel structure to enable tunability. These photodynamic moieties/chromophores trap optical signals and convert them to chemical signals via photoreactions like cleavage, dimerization, and isomerization. Photosensitive hydrogels have been extensively applied in tissue engineering processes [52].
5.4.3 Pressure-responsive hydrogels
These are usually temperature or pH-sensitive. They respond to changes in the ionic concentration of a solution or its pressure to release entrapped drug molecules [56].
5.4.4 Magnetic field-sensitive hydrogels
These can be referred to as ferrogels. They possess polymer networks that are chemically crosslinked and contain fine suspensions of magnetic nanoparticles. Their volume contraction can occur at sufficient external magnetic stimuli or field strength. They have been employed in cancer diagnostics and targeted drug delivery [52].
5.5 pH-responsive hydrogels
These comprise hydrogels that contain ionizable basic or acidic groups. They are cationic when possessing amine groups, while carboxylic and sulphonic groups are present in anionic hydrogels. For anionic hydrogels, when the surrounding pH is above its pKa, deprotonation occurs. Conversely, for cationic hydrogels, when the surrounding pH is below its pKa, ionization occurs. This ionization process causes them to swell as a result of electrostatic repulsion. Examples of polymers that exhibit this behavior are chitosan, DNA, cellulose, hyaluronic acid, guar gum and poly(methacrylic acid) (PMAA). They have been applied in cell encapsulation, drug delivery, and biomedicine [52].
5.5.1 Ionic strength-sensitive hydrogels
These contain ionic monomers on a polymeric chain which respond to the ionic effects of the surrounding solution. Polyelectrolyte gels are classified in this category. Their volume changes arise from a combination of the elasticity of the hydrogel network and its ionization degree. Soluble monomers like acrylic acid and [3-(methacryloylamino) propyl] trimethylammonium chloride (MAPTEC) are used to synthesize these polymers [52]. These monomers dissociate to yield charged molecules upon immersing the hydrogels in a solution. The interaction between the ionic composition of the solution and the counterions in the hydrogel creates an electrostatic gradient that facilitates osmosis leading to swelling or shrinking of the hydrogel. Factors such as binding constant of the hydrogel monomers and their intrinsic dissociation, hydrogel polymer structure, the ionic composition of the solution, and the ionic species present influence sol-gel transitions in these hydrogels [57].
5.5.2 Biomolecule-responsive hydrogels
Glucose-responsive hydrogels are responsive to glucose concentrations in the body leading to insulin release. A novel glucose-responsive peptide hydrogel that is biocompatible and loaded with catalase, glucose oxidase, and insulin for treating diabetes has been designed [58]. Under physiologic conditions, the peptide self-assembles into a hydrogel while the formation of gluconic acid from glucose triggers insulin release from the gel matrix. This idea has also been employed in continuous glucose monitoring where an injectable fluorescent hydrogel microbead was injected under the dermis using a needle. When the concentration of glucose increases, the fluorescent intensity of the microbeads will increase [52]. Enzyme-sensitive hydrogels respond to specific enzymes which serve as biomarkers for certain disease conditions like cancer, neurodegenerative diseases, inflammatory and cardiovascular diseases [52]. For instance, hydrogels have been designed to release encapsulated drugs when exposed to high concentrations of metalloproteinases in diseased cells. Enzyme-sensitive hydrogels are capable of the instantaneous release of drugs to the target sites [59]. Antigen-responsive hydrogels utilize the antigen-antibody reaction mechanism in the body. Semi-interpenetrating network (semi-IPN) hydrogels have been formed which were impregnated with an antibody to target an antigen. Conformational changes will occur upon binding of the antigen to the antibody present on the hydrogel leading to the release of its drug content [60]. DNA-responsive hydrogels undergo sol-gel transitions in response to the presence of DNA aptamers. Conjugating hydrogels with DNA has been employed in sensing systems and targeted drug delivery [61]. Reactive oxygen species-sensitive hydrogels are synthesized through modifications with ROS-responsive moieties either by merging them into the polymer backbone, or incorporating their side chains into the hydrogels (Figure 3) [62].
Figure 3.
Smart hydrogel system and some applications
5.6 Supramolecular systems
The formation of supramolecular hydrogel systems involves non-covalent molecular bonds like π-π bonds, hydrogen bonding, van der Waals forces, host-guest combinations and metal-ligand binding. These supramolecular systems have enabled the development of injectable hydrogels. This is achieved by providing temporary interactions in designing polymer materials with reversible mechanical features and tunability. These supramolecular hydrogels are able to self-assemble, self-heal and respond to stimuli. In ophthalmic delivery, supramolecular hydrogels have been employed. Conventional ophthalmic delivery systems have limitations of poor adhesion and poor penetration in the aqueous humor, giving rise to sub-therapeutic concentrations in ocular tissues. Fernandes-Cunha et al. [63] designed a supramolecular hydrogel composed of adamantane in combination with hyaluronic acid or cyclodextrin for corneal wound healing. Other forms of supramolecular hydrogel systems like adhesive hydrogels, self-healing hydrogels, electrically-conducting hydrogels, and metallo-supramolecular hydrogels have been highlighted elsewhere [64].
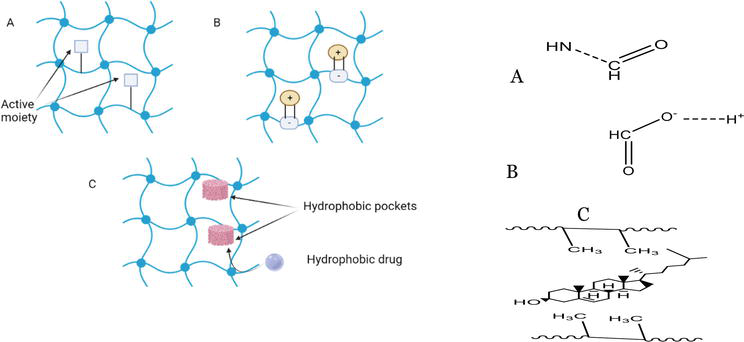
Drug loaded hydrogels are a group of crosslinked polymers into which one or more drugs are entrapped. During synthesis of these hydrogels, crosslinking happens either physically or chemically. The corresponding hydrogels synthesized could be termed as reversible or irreversible depending on their stability. The physical process involves weak binding interactions such as ionic bonds, hydrogen bonds and complexation. The hydrogels synthesized by this process generally have a much higher probability of deformation or degradation by changes in external parameters such as temperature, pH or physical stress while hydrogels synthesized by chemical processes are quite stable due to the strong covalent bonds holding the individual monomer units together [65]. Thus, they need to be formulated accordingly ensuring significant entrapment of the drug in the matrix. Effect of drug for a longer period of time, better bioavailability, targeting efficiency and higher contact time are some of the common advantages of hydrogel delivery systems over conventional formulations such as eye drops or other oral medications. Drugs are generally loaded in the polymer matrix either simultaneously during (in-situ encapsulation) or after crosslinking of the polymer/s. The former method encapsulates a much larger quantity of drug but there are more compatibility issues encountered due to reaction between the drug and the polymerizing monomers [65]. Drug entrapment occurs by formation of physical or chemical linkages with the polymer chains. These interactions can be classified into three types i.e. covalent, electrostatic and hydrophobic [66]. Schematic representation of these interactions are shown in Figure 4.
Figure 4.
Entrapment strategies (A) covalent linkage, (B) electrostatic linkage and (C) hydrophobic interactions. Linkages in the form of bonds shown by dashed lines (right).
Covalent interactions are those which lead to the formation of strong chemical bonds between the drug and the polymer chain. These can either form a cleavage which on external stimulus leads to bond dissociation or remain stable which would require degradation of entire polymer matrix for release of drug [66]. Amide bonds are the most common type of highly stable covalent interactions. Ester, disulphide and peptide linkages are examples of cleavable interactions [67]. Covalent bonds are formed as a result of affinity of an electron deficient molecule towards an electron rich molecule leading to mutual sharing of electrons and bond formation. In case of amide bonds, the carboxylic group of the polymer chain is the electron deficient molecule and the amine group of the drug is the electron rich molecule. Electrostatic/ionic interactions are formed as a result of attraction of molecules having opposite charge. Unlike covalent interactions, these are non-specific and hence could be used for delivery of multiple ionic active moieties simultaneously from a single system. The intensity of these interactions controls the release rate of drug. These interactions happen by transfer of electron from one molecule to another leading to formation of charge on the participating molecules. Thus, there is no electron sharing unlike covalent interactions thus, the bonds formed are much weaker. Alginate polymers containing anionic groups have been used to deliver vascular endothelial growth factor (VEGF). Sulfonate functional groups have found to improve the affinity of amino acids towards alginate polymers by improving the intensity of ionic interactions [68].
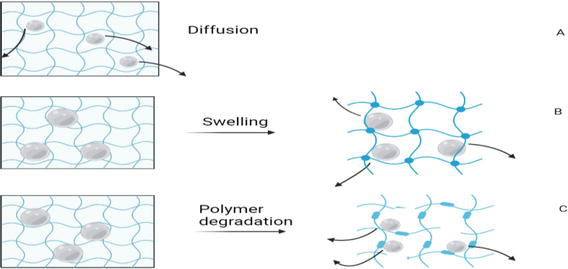
Due to the hydrophilic nature of hydrogels, incorporation of lipophilic moieties becomes very difficult. Stability and incompatibility issues such as phase separation, drug leaching during storage, degradation and erratic release profile are very common in such circumstances. Thus, there is a need for incorporation of hydrophobic functional groups into the hydrogel structures. But these hydrophobic functional groups increase the overall hydrophobicity of the hydrogel leading to hydrogel condensation thus, hampering release of drug. Cyclodextrins (CDs) are those compounds which when incorporated do not alter the hydrophilicity of hydrogels. These contain two phases- outer hydrophilic body and inner hydrophobic pocket. The active moieties bind inside the hydrophobic pocket. This facilitates efficient loading and controlled release of lipophilic moieties embedded into hydrophilic polymers [69]. Drug release rate is governed by various factors such as molecular weight of the drug, drug-polymer affinity, concentration of the polymer blend, degree of crosslinking of the polymers and the degradation rate. Three major mechanisms cater to the release of drug from the polymer. They are diffusion, swelling and degradation [66]. An appropriate polymer-polymer blend should be chosen for a particular drug of interest considering what type of release is desired. For drugs with sizes smaller than the mesh size of the hydrogel, drug release is majorly diffusion-oriented and hence would be more of an immediate release formulation but if its size exceeds the mesh size, then stearic interferences play a role in drug release. The diffusion path length also significantly increases [70] and hence drug release is sustained. In order to enable the release of such drugs through the smaller matrices, two mechanisms could be applied—swelling leading to increase in matrix size or degradation leading to breakdown of matrix network. The three drug release mechanisms are explained in Figure 5.
Figure 5.
Mechanisms of drug release from hydrogel matrix. (A) Simple diffusion, (B) swelling and (C) degradation.
7. Biocompatibility of hydrogels for ophthalmic application
Biocompatibility of implants or delivery systems is necessary to enable appropriate activity of the substance without any local or systemic adverse events. For this, the substance needs to be compatible with the tissues to which it is going to be in contact with. Hydrogels for ocular drug delivery should be transparent, mucoadhesive, flexible and should have the ability to retain water once administered. For administration into the aqueous chamber, the viscosity should be kept low but the viscosity should match that of vitreous fluids while administering intravitreally. The two major characteristics to consider during the development of any ocular formulation is pH and osmolality. The pH and the osmolality range for ocular drug delivery are 6.5–8.5 and 100–640 mOsm/Kg respectively [71]. Any formulation not complying with these values generally cause irritation to the eye. HET-CAM and Draize eye irritation tests are the most common tests which are carried out to evaluate the biocompatibility of ocular formulations. Both these tests give a prior idea about degree of irritation of the formulation after administration in the human eye [15]. The HET-CAM test measures the degree of hemorrhage, lysis, and coagulation on the chorioallantoic membrane of the fertilized egg of hens. The Draize test measures the degree of redness of formulation administered in the eye of rabbits, thus directly correlating to the irritation potential of the formulation. Excipients for the development of ocular formulations should be chosen in a manner that they do not cause any adverse reactions in the eye and also enable efficient activity of the API at the desired site. Choosing the appropriate excipients and also incorporating them in the right quantities in the formulation such that they cause no harm is the key. Reference to the Inactive Ingredient Guide (IIG) is done to get an idea of the upper limits of the excipients to be added into ocular formulations.
8. Modification of hydrogels for active ocular targeting
Hydrogels have found its application for both anterior and posterior segments of the eye. The anterior segment application is by soft contact lens (SCLs) for vision correction and to elute drugs, corneal wound healing, and as intraocular lenses (IOLs), whereas the posterior segment research has been as vitreous substitutes and intravitreal drug loading [72]. Vision correcting SCLs, being the most common application, generally use non-therapeutic payload on PHEMA polymer. However, evolution in the use of SCLs, hydrophilic/hydrophobic monomer hybrids of PHEMA and poly(dimethylsiloxane) to provide comfort and better structural flexibility for corneal fit and enable greater oxygen and gas permeability respectively has been achieved [73]. In an in vitro study by Wang et al. single protein adsorption on PEGMA—a methyl ether acrylate of poly(ethylene glycol) modified silicone hydrogel was decreased on the lens surface. This provided ophthalmic distinctness and further lowered the chances of infections [74]. Hydrogels have become a promising tool as post-surgery and ocular trauma wound closing sealant over the conventional nylon sutures. These novel ophthalmic adhesive systems have overcome the issues of ocular surface fluid leak leading to infection, anterior chamber collapse due to oozing of anterior aqueous humor and lens rotation, post IOL fitting through an incision through the cornea. ReSure® sealant is the only FDA-approved ocular healing hydrogel currently on the market, although researchers have also investigated using DuraSeal®, a formulation that is approved for cranial adhesion, to seal ocular wounds [75]. These hydrogels, which are predominantly crosslinked with PEG on trilysine amine groups, quadruple-armed with NHS capping, are shed off the eye’s surface during regeneration and structurization of tissue. While the use of hydrogel based-sealants in wound healing is upsurging, researchers have been successful in loading drugs in order to enhance the healing process. Anumolu et al. designed an in situ forming PEGylated hydrogel loaded with doxycycline and the results ensured an accelerated healing of vesicant-induced corneal wounds [76]. Similarly, the addition of epithelial growth factors (EGF) from hydrogel formulation concluded that the released protein showed therapeutic effect in rabbit corneal ocular trauma model [77]. Hydrogel-based intraocular lenses (IOLs) have found its application in replacing the altered natural crystalline lens of the eye in cataract and even restoring the axial length of the eye in myopia. While the poly(methylmethacrylate) (PMMA) is a gold standard polymer for IOLs, the next generation silicone-based and hydrophilic/hydrophobic acrylate polymer provide greater flexibility of insertion. Other major issue with IOLs have been the posterior capsule opacification (PCO), resulting from wearing of cells from the natural lens epithelium adhering to the IOL on the posterior end. In order to avoid this issue, Bozukova et al. chemically surface-PEGylated the IOL with PEG-chains varying in molecular weights [78]. In a similar manner, Lin et al. modified the silicone hydrogel used for IOL using multilayers of hyaluronic acid and chitosan [79]. Conventionally used gases (sulphurhexafloride, perfluoropropane) and liquids (semiflourinated alkanes, silicone oils) as vitreous substitutes, though with satisfying optical and biocompatible properties, possess threats of increased intraocular pressure, choroidal thinning, inflammation, and cataracts and require a face down position for few days making it less consumer acceptable. Various hydrogel polymers concentrates have been used to replace vitreous fluid. However, their immune response, quick absorption/degradation, and inability to form tamponade, have opened the avenue for researchers to explore further modifications approaches in hydrogels as vitreous substitutes [80]. A zwitterionic in situ hydrogel crosslinked with α-PEGMA on a acryloyl cystamine and sulfobetaine methacrylamide copolymer, poly(MPDSA-co-AC), in a thiol-ene Michael addition reaction showed appropriate physical and rheological properties with no postoperative inflammation and remained optically acceptable in vivo [81].
9. Therapeutic applications of hydrogels for ocular delivery
Hydrogels have been tested for the treatment of various conditions such as macular degeneration, diabetic retinopathy, conjunctivitis, glaucoma, etc. [15, 82]. Apart from delivery systems, hydrogels in the form of drug-eluting contact lenses, intraocular lenses, tissue adhesives as wound dressings and vitreous substitutes are alternative uses of hydrogels [72]. List of a few ocular hydrogel products in the market and their clinical uses is presented in Table 1.
10. Challenges and opportunities in the translation of hydrogel technology
The field of hydrogels for ocular therapy has enormously made advancement in the last few decades with multidimensional research in the field of SCLs, ocular dressings, contact lenses and smart drug delivery for ocular conditions and diseases. Though clinical translations of hydrogel technology can be seen through commercialized products for drug-free (majorly for dry-eyes syndrome) and drug-loaded hydrogel matrices, challenges are still persistent with intravitreal hydrogel-based drug delivery. Table 2 summarizes hydrogel-based products in the market [82].
Drug-free hydrogel-based products for ocular delivery [82].
Apart from the list above, a few of them are still in various clinical trial phases before commercial approvals will be granted [82]. The difficulty of widely utilizing hydrogel inventions in the clinic for intravitreal therapy is still evident, given the challenges in the need for sterilization, scale up, cost, shelf-life, and compliance for both medical practitioners and patients. The only contender for treating AMD after intravitreal injection is OTX-TKI, a PEG hydrogel containing axitinib microcrystals—a tyrosine kinase inhibitor, with clinical studies currently in Phase 1 (NCT03630315). A sustained release variant of aflibercept called OTX-IVT, is currently being developed in the preclinical stage to bind to the circulating VEGFs and reducing the intravitreal injection frequency to once in every 4–6 months [83]. The above moieties are also being evaluated for retinal vein occlusion and diabetic macular oedema. The Japanese health authorities have recently certified ACUVUE® Theravision™ containing Ketotifen by Johnson & Johnson, the world’s first drug-eluting contact lens for vision rectification and irritation of the eye due to allergic conjunctivitis for people who wear contact lenses [84].
11. Conclusion and future directions
This chapter attempted a discussion of the anatomy and physiology of the eye as an essential organ of vision. It discussed how light trapped into the ocular tissues are conveyed, relayed and processed into vision to aid physiological functions. It also exposed the various barriers which influence the circulation of molecules in the ocular architecture and what they portend for ophthalmic drug delivery. Indeed, the fabrication and use of hydrogel as an important device in the delivery of ocular therapeutics was considered in this chapter. Beyond discussions on the functionalities of smart and stimuli-responsive hydrogels presented in this chapter, it is imperative to deposit that hydrogels can be used to effect controlled drug delivery in the ocular tissue, improve topical corneal drug administration, promote prolonged corneal surface residence time, and enhance co-formulation and administration of biomacromolecules. Despite the marked successes achieved in ocular delivery using hydrogels, challenges inherent in in vivo delivery of biologics using hydrogels such as short half-life and poor stability, need to be tackled in order to enhance their clinical translation opportunities. Further researches are also needed to address the overwhelming influence of ocular barriers especially the anterior corneal and posterior blood retinal barriers for decreased pre-corneal clearance and improved corneal residence time, and increased transport of drug molecules into the retina. Therefore, hydrogel delivery system has vital roles to play in the future fabrication and utility of ocular therapeutics for the treatment of ophthalmic pathologies especially diseases of the posterior eye.
1.Alvarez-Lorenzo C, Anguiano-Igea S, Varela-García A, Vivero-Lopez M, Concheiro A. Bioinspired hydrogels for drug-eluting contact lenses. Acta Biomaterialia. 2019;84:49-62. DOI: 10.1016/j.actbio.2018.11.020
2.Novack GD, Robin AL. Ocular pharmacology. Journal of Clinical Pharmacology. 2016;56:517-527. DOI: 10.1002/jcph.634
3.Chen X, Wu J, Lin X, Wu X, Yu X, Wang B, et al. Tacrolimus loaded cationic liposomes for dry eye treatment. Frontiers in Pharmacology. 2022;13:838168. DOI: 10.3389/fphar.2022.838168
4.Muller L, Jensen BP, Bachmann LM, Wong D, Wells AP. New technique to reduce systemic side effects of timolol eye drops: The tissue press method-cross-over clinical trial. Clinical & Experimental Ophthalmology. 2020;48:24-30. DOI: 10.1111/ceo.13642
5.Buwalda SJ, Boere KW, Dijkstra PJ, Feijen J, Vermonden T, Hennink WE. Hydrogels in a historical perspective: From simple networks to smart materials. Journal of Controlled Release. 2014;190:254-273. DOI: 10.1016/j.jconrel.2014.03.052
6.Chang D, Park K, Famili A. Hydrogels for sustained delivery of biologics to the back of the eye. Drug Discovery Today. 2019;24(8):1470-1482. DOI: 10.1016/j.drudis.2019.05.037
7.Li Q , Cao Y, Wang P. Recent advances in hydrogels for the diagnosis and treatment of dry eye disease. Gels. 2022;8:816. DOI: 10.3390/gels8120816
8.Cholkar K, Dasari SR, Pal D, Mitra AK. Eye: Anatomy, physiology, and barriers to drug delivery. In: Mitra AK, editor. Ocular Transporters and Receptors. Sawston: Woodhead Publishing; 2013. pp. 1-36. DOI: 10.1533/9781908818317.1
9.Lynch CR, Kondiah PPD, Choonara YE, du Toit LC, Ally N, Pillay V. Hydrogel biomaterials for application in ocular drug delivery. Frontiers in Bioengineering and Biotechnology. 2020;8:228. DOI: 10.3389/fbioe.2020.00228
10.Gorantla S, Rapalli VK, Waghule T, Singh PP, Dubey SK, Saha RN, et al. Nanocarriers for ocular drug delivery: Current status and translational opportunity. RSC Advances. 2020;10:27835. DOI: 10.1039/d0ra04971a
11.DelMonte DW, Kim T. Anatomy and physiology of the cornea. Journal of Cataract and Refractive Surgery. 2011;37(3):588-598. DOI: 10.1016/j.jcrs.2010.12.037
12.Willoughby CE, Ponzin D, Ferrari S, Lobo A, Landau K, Omidi Y. Anatomy and physiology of the human eye: Effects of mucopolysaccharidoses disease on structure and function—A review. Clinical & Experimental Ophthalmology. 2010;38:2-11. DOI: 10.1111/j.1442-9071.2010.02363.x
13.Harvey TM, Fernandez AGA, Patel R, Goldman D, Ciralsky J. Conjunctival anatomy and physiology. In: Holland E, Mannis M, Lee WB, editors. Ocular Surface Disease: Cornea, Conjunctiva and Tear Film. 1st ed. Philadelphia: WB Saunders; 2013. pp. 23-27
14.Dartt DA. Regulation of mucin and fluid secretion by conjunctival epithelial cells. Progress in Retinal and Eye Research. 2002;21(6):555-576. DOI: 10.1016/s1350-9462(02)00038-1
15.Ahmed S, Amin MM, Sayed S. Ocular drug delivery: A comprehensive review. AAPS PharmSciTech. 2023;24(2):66. DOI: 10.1208/s12249023-02516-9
16.Maulvi FA, Shetty KH, Desai DT, Shah DO, Willcox MDP. Recent advances in ophthalmic preparations: Ocular barriers, dosage forms and routes of administration. International Journal of Pharmaceutics. 2021;608:121105. DOI: 10.1016/j.ijpharm.2021.121105
18.Dosmar E, Walsh J, Doyel M, Bussett K, Oladipupo A, Amer S, et al. Targeting ocular drug delivery: An examination of local anatomy and current approaches. Bioengineering. 2022;9(1):41. DOI: 10.3390/bioengineering9010041
19.Norman RE, Flanagan JG, Rausch SM, Sigal IA, Tertinegg I, Eilaghi A, et al. Dimensions of the human sclera: Thickness measurement and regional changes with axial length. Experimental Eye Research. 2010;90(2):277-284. DOI: 10.1016/j.exer.2009.11.001
20.Yi X, Wang Y, Yu FS. Corneal epithelial tight junctions and their response to lipopolysaccharide challenge. Investigative Ophthalmology & Visual Science;41(13):4093-4100
21.Ono SJ, Abelson MB. Allergic conjunctivitis: Update on pathophysiology and prospects for future treatment. The Journal of Allergy and Clinical Immunology. 2005;115(1):118-122. DOI: 10.1016/j.jaci.2004.10.042
22.Urtti A. Challenges and obstacles of ocular pharmacokinetics and drug delivery. Advanced Drug Delivery Reviews. 2006;58(11):1131-1135. DOI: 10.1016/j.addr.2006.07.027
23.Mannermaa E, Vellonen KS, Urtti A. Drug transport in corneal epithelium and blood-retina barrier: Emerging role of transporters in ocular pharmacokinetics. Advanced Drug Delivery Reviews. 2006;58(11):1136-1163. DOI: 10.1016/j.addr.2006.07.024
24.Kong X, Liu X, Huang X, Mao Z, Zhong Y, Chi W. Damage to the blood-aqueous barrier in eyes with primary angle closure glaucoma. Molecular Vision. 2010;16:2026-2032
25.Fujiwara T, Imamura Y, Margolis R, Slakter JS, Spaide RF. Enhanced depth imaging optical coherence tomography of the choroid in highly myopic eyes. American Journal of Ophthalmology. 2009;148(3):445-450. DOI: 10.1016/j.ajo.2009.04.029
26.Torres-Luna C, Fan X, Domszy R, Hu N, Wang NS, Yang A. Hydrogel-based ocular drug delivery systems for hydrophobic drugs. European Journal of Pharmaceutical Sciences. 2020;154:0928-0987. DOI: 10.1016/j.ejps.2020.105503
27.Kushwaha SK, Saxena P, Rai A. Stimuli sensitive hydrogels for ophthalmic drug delivery: A review. International Journal of Pharmaceutical Investigation. 2012;2(2):54-60. DOI: 10.4103/2230-973X.100036
28.Byrne ME, Park K, Peppas NA. Molecular imprinting within hydrogels. Advanced Drug Delivery Reviews. 2002;54(1):149-161. DOI: 10.1016/s0169-409x(01)00246-0
29.Horne RR, Judd KE, Pitt WG. Rapid loading and prolonged release of latanoprost from a silicone hydrogel contact lens. Journal of Drug Delivery Science and Technology. 2017;41:410-418. DOI: 10.1016/j.jddst.2017.08.011
30.Maulvi FA, Desai AR, Choksi HH, Patil RJ, Ranch KM, Vyas BA, et al. Effect of surfactant chain length on drug release kinetics from microemulsion-laden contact lenses. International Journal of Pharmaceutics. 2017;524(1-2):193-204. DOI: 10.1016/j.ijpharm.2017.03.083
31.Xu W, Jiao W, Li S, Tao X, Mu G. Bimatoprost-loaded microemulsion laden contact lens to treat glaucoma. Journal of Drug Delivery Science and Technology. 2019;54:101330. DOI: 10.1016/j.jddst.2019.101330
32.Song Y, Nagai N, Saijo S, Kaji H, Nishizawa M, Abe T. In situ formation of injectable chitosan-gelatin hydrogels through double crosslinking for sustained intraocular drug delivery. Materials Science & Engineering. C, Materials for Biological Applications. 2018;88:1-12. DOI: 10.1016/j.msec.2018.02.022
33.Costa VP, Braga MEM, Duarte CMM, Alvarez-Lorenzo C, Concheiro A, Gil MH, et al. Anti-glaucoma drug-loaded contact lenses prepared using supercritical solvent impregnation. Journal of Supercritical Fluids. 2010;53(1-3):165-173. DOI: 10.1016/j.supflu.2010.02.007
34.Malaekeh-Nikouei B, Ghaeni FA, Motamedshariaty VS, Mohajeri SA. Controlled release of prednisolone acetate from molecularly imprinted hydrogel contact lenses. Journal of Applied Polymer Science. 2012;126(1):387-394. DOI: 10.1002/app.36625
35.Fulgencio GO, Viana FA, Ribeiro RR, Yoshida MI, Faraco AG, Cunha-Junior AS. New mucoadhesive chitosan film for ophthalmic drug delivery of timolol maleate: In vivo evaluation. Journal of Ocular Pharmacology and Therapeutics. 2012;28:350-358. DOI: 10.1089/jop.2011.0174
36.Xu X, Weng Y, Xu L, Chen H. Sustained release of Avastin from polysaccharides cross-linked hydrogels for ocular drug delivery. International Journal of Biological Macromolecules. 2013;60:272-276. DOI: 10.1016/j.ijbiomac.2013.05.034
37.Martens TF, Remaut K, Deschout H, Engbersen JF, Hennink WE, van Steenbergen MJ, et al. Coating nanocarriers with hyaluronic acid facilitates intravitreal drug delivery for retinal gene therapy. Journal of Controlled Release. 2015;202:83-92. DOI: 10.1016/j.jconrel.2015.01.030
38.Lin J, Zheng SY, Xiao R, Yin J, Wu ZL, Zheng Q , et al. Constitutive behaviors of tough physical hydrogels with dynamic metal-coordinated bonds. Journal of the Mechanics and Physics of Solids. 2020;139:103935. DOI: 10.1016/j.jmps.2020.103935
39.Yokoyama F, Masada I, Shimamura K, Ikawa T, Monobe K. Morphology and structure of highly elastic poly (vinyl alcohol) hydrogel prepared by repeated freezing-and-melting. Colloid & Polymer Science. 1986;264:595-601. DOI: 10.1007/BF01412597
40.Bashir S, Hina M, Iqbal J, Rajpar AH, Mujtaba MA, Alghamdi NA, et al. Fundamental concepts of hydrogels: Synthesis, properties, and their applications. Polymers. 2020;12(11):2702. DOI: 10.3390/polym12112702
41.Ali F, Khan I, Chen J, Akhtar K, Bakhsh EM, Khan SB. Emerging fabrication strategies of hydrogels and its applications. Gels. 2022;8:205. DOI: 10.3390/gels8040205
42.Coviello T, Grassi M, Rambone G, Santucci E, Carafa M, Murtas E, et al. Novel hydrogel system from scleroglucan: Synthesis and characterization. Journal of Controlled Release. 1999;60(2-3):367-378. DOI: 10.1016/s0168-3659(99)00091-7
43.Zu Y, Zhang Y, Zhao X, Shan C, Zu S, Wang K, et al. Preparation and characterization of chitosan-polyvinyl alcohol blend hydrogels for the controlled release of nano-insulin. International Journal of Biological Macromolecules. 2012;50(1):82-87. DOI: 10.1016/j.ijbiomac.2011.10.006
44.Alla ASG, Sen M, El-Naggar AW. Swelling and mechanical properties of superabsorbent hydrogels based on Tara gum/acrylic acid synthesized by gamma radiation. Carbohydrate Polymers. 2012;89(2):478-485. DOI: 10.1016/j.carbpol.2012.03.031
45.Andreopoulos FM, Beckman EJ, Russell AJ. Light-induced tailoring of PEG-hydrogel properties. Biomaterials. 1998;9(15):1343-1352. DOI: 10.1016/s0142-9612(97)00219-6
46.Song W, Ko J, Choi YH, Hwang NS. Recent advancements in enzyme-mediated crosslinkable hydrogels: In vivo-mimicking strategies. APL Bioengineering. 2021;5(2):021502. DOI: 10.1063/5.0037793
47.Ahmed EM. Hydrogel: Preparation, characterization, and applications: A review. Journal of Advanced Research. 2015;6(2):105-121. DOI: 10.1016/j.jare.2013.07.006
48.Suhail M, Rosenholm JM, Minhas MU, Badshah SF, Naeem A, Khan KU, et al. Nanogels as drug-delivery systems: A comprehensive overview. Therapeutic Delivery. 2019;10(11):697-717. DOI: 10.4155/tde-2019-0010
49.Barrett-Catton E, Ross ML, Asuri P. Multifunctional hydrogel nanocomposites for biomedical applications. Polymers. 2021;13:856. DOI: 10.3390/polym13060856
50.Patel R, Purwada A, Cherchietti L, Inghirami G, Melnick A, Gaharwar AK, et al. Microscale bioadhesive hydrogel arrays for cell engineering applications. Cellular and Molecular Bioengineering. 2014;7:394-408. DOI: 10.1007/s12195-014-0353-8
51.Morya V, Walia S, Mandal BB, Ghoroi C, Bhatia D. Functional DNA based hydrogels: Development, properties and biological applications. ACS Biomaterials Science & Engineering. 2020;6:6021-6035. DOI: 10.1021/acsbiomaterials.0c01125
52.Merati AA, Hemmatinejad N, Shakeri M, Bashari A. Advances in research and applications of smart hydrogels part I: Preparation methods and classification. Journal of Textiles and Polymers. 2018;6(2):97-105
53.Yan X, Fang WW, Xue J, Sun TC, Dong L, Zha Z, et al. Thermoresponsive in situ forming hydrogel with sol-gel irreversibility for effective methicillin-resistant Staphylococcus aureus infected wound healing. ACS Nano. 2019;13:10074-10084. DOI: 10.1021/acsnano.9b02845
54.Zhao C, Tian S, Liu QH, Xiu KM, Lei IL, Wang Z, et al. Biodegradable nanofibrous temperature-responsive gelling microspheres for heart regeneration. Advanced Functional Materials. 2020;30:2000776. DOI: 10.1002/adfm.202000776
55.Jia YP, Shi K, Yang F, Liao JF, Han RX, Yuan LP, et al. Multifunctional nanoparticle loaded injectable thermos-responsive hydrogel as NIR controlled release platform for local photothermal immunotherapy to prevent breast cancer postoperative recurrence and metastases. Advanced Functional Materials. 2020;30:2001059. DOI: 10.1002/adfm.202001059
56.Shimoboji T, Larenas E, Fowler T, Kulkarni S, Hoffman AS, Stayton PS. Photoresponsive polymer–enzyme switches. Proceedings of the National Academy of Sciences. 2002;99(26):16592-16596. DOI: 10.1073/pnas.262427799
57.Li H, Lai F, Luo R. Analysis of responsive characteristics of ionic-strength-sensitive hydrogel with consideration of effect of equilibrium constant by a chemo-electro-mechanical model. Langmuir. 2009;25(22):13142-13150. DOI: 10.1021/la901833m
58.Li X, Fu M, Wu J, Zhang C, Deng X, Dhinakar A, et al. pH-sensitive peptide hydrogel for glucose-responsive insulin delivery. Acta Biomaterialia. 2017;51:294-303. DOI: 10.1016/j.actbio.2017.01.016
59.Zhao L, Wang J, Su D, Zhang Y, Lu H, Yan X, et al. The DNA controllable peroxidase mimetic activity of MoS2 nanosheets for constructing a robust colorimetric biosensor. Nanoscale. 2020;12:19420-19428. DOI: 10.1039/d0nr05649a
60.Miyata T, Asami N, Uragami T. A reversibly antigen-responsive hydrogel. Nature. 1999;399(6738):766-769. DOI: 10.1038/21619
61.Yang H, Liu H, Kang H, Tan W. Engineering target-responsive hydrogels based on aptamer–target interactions. Journal of the American Chemical Society. 2008;130(20):6320-6321. DOI: 10.1021/ja801339w
63.Fernandes-Cunha GM, Jeong SH, Logan CM, Le P, Mundy D, Chen F, et al. Supramolecular host-guest hyaluronic acid hydrogels enhance corneal wound healing through dynamic spatiotemporal effects. The Ocular Surface. 2022;23:148-161. DOI: 10.1016/j.jtos.2021.09.002
64.Sánchez-Fernández JA. Structural strategies for supramolecular hydrogels and their applications. Polymers. 2023;15:1365. DOI: 10.3390/polym15061365
65.Kirchhof S, Goepferich AM, Brandl FP. Hydrogels in ophthalmic applications. European Journal of Pharmaceutics and Biopharmaceutics. 2015;95:227-238. DOI: 10.1016/j.ejpb.2015.05.016
66.Li J, Mooney DJ. Designing hydrogels for controlled drug delivery. Nature Reviews Materials. 2016;1:16071. DOI: 10.1038/natrevmats.2016.71
67.Deepthi S, Jose J. Novel hydrogel-based ocular drug delivery system for the treatment of conjunctivitis. International Ophthalmology. 2019;39(6):1355-1366. DOI: 10.1007/s10792-018-0955-6
68.van Hove AH, Beltejar MJ, Benoit DS. Development and in vitro assessment of enzymatically-responsive poly(ethylene glycol) hydrogels for the delivery of therapeutic peptides. Biomaterials. 2014;35(36):9719-9730. DOI: 10.1016/j.biomaterials.2014.08.019
69.Freeman I, Kedem A, Cohen S. The effect of sulfation of alginate hydrogels on the specific binding and controlled release of heparin-binding proteins. Biomaterials. 2008;29(22):3260-3268. DOI: 10.1016/j.biomaterials.2008.04.025
70.Mateen R, Hoare T. Injectable, in situ gelling, cyclodextrin-dextran hydrogels for the partitioning-driven release of hydrophobic drugs. Journal of Materials Chemistry B. 2014;2(32):5157-5167. DOI: 10.1039/C4TB00631C
71.Amsden B. Solute diffusion within hydrogels. Mechanisms and models. Macromolecules. 1998;31(23):8382-8395. DOI: 10.1021/ma980765f
72.Cooper RC, Yang H. Hydrogel-based ocular drug delivery systems: Emerging fabrication strategies, applications, and bench-to-bedside manufacturing considerations. Journal of Controlled Release. 2019;306:29-39. DOI: 10.1016/j.jconrel.2019.05.034
73.Lin HC, Yeh YH, Lin WC, Yang MC. Novel silicone hydrogel based on PDMS and PEGMA for contact lens application. Colloids and Surfaces B: Biointerfaces. 2014;123:986-994. DOI: 10.1016/j.colsurfb.2014.10.053
74.Wang JJ, Liu F. Imparting antifouling properties of silicone hydrogels by grafting poly(ethylene glycol) methyl ether acrylate initiated by UV light. Journal of Applied Polymer Science. 2012;125(1):548-554. DOI: 10.1002/app.35687
75.Ghobril C, Grinstaff MW. The chemistry and engineering of polymeric hydrogel adhesives for wound closure: A tutorial. Chemical Society Reviews. 2015;44(7):1820-1835. DOI: 10.1039/c4cs00332b
76.Anumolu SNS, DeSantis AS, Menjoge AR, Hahn RA, Beloni JA, Gordon MK, et al. Doxycycline loaded poly(ethylene glycol) hydrogels for healing vesicant-induced ocular wounds. Biomaterials. 2010;31(5):964-974. DOI: 10.1016/j.biomaterials.2009.10.010
77.Schultz CL, Morck DW. Contact lenses as a drug delivery device for epidermal growth factor in the treatment of ocular wounds. Clinical & Experimental Optometry. 2010;93(2):61-65. DOI: 10.1111/j.1444-0938.2010.00459.x
78.Bozukova D, Pagnoulle C, De Pauw-Gillet MC, Desbief S, Lazzaroni R, Ruth N, et al. Improved performances of intraocular lenses by poly(ethylene glycol) chemical coatings. Biomacromolecules. 2007;8(8):2379-2387. DOI: 10.1021/bm0701649
79.Lin Q , Xu X, Wang B, Shen C, Tang J, Han Y, et al. Hydrated polysaccharide multilayer as an intraocular lens surface coating for biocompatibility improvements. Journal of Materials Chemistry B. 2015;3(18):3695-3703. DOI: 10.1039/c5tb00111k
80.Lin Q , Lim JYC, Xue K, Su X, Loh XJ. Polymeric hydrogels as a vitreous replacement strategy in the eye. Biomaterials. 2021;268:120547. DOI: 10.1016/j.biomaterials.2020.120547
81.Chang J, Tao Y, Wang B, Bao-hua G, Hong X, Jiang Y, et al. An in situ-forming zwitterionic hydrogel as vitreous substitute. Journal of Materials Chemistry B. 2015;3(6):1097-1105. DOI: 10.1039/c4tb01775g
82.Fang G, Yang X, Wang Q , Zhang A, Tang B. Hydrogels-based ophthalmic drug delivery systems for treatment of ocular diseases. Materials Science and Engineering: C. 2021;127:112212. DOI: 10.1016/j.msec.2021.112212
83.Pipeline—Ocular Therapeutix. Available from: https://www.ocutx.com/research/pipeline/ [Accessed: May 14, 2023]
84.Approval of Drug-Releasing Combination Contact Lens for Vision Correction and Allergic Eye Itch. Available from: https://www.jjvision.com/press-release/johnson-johnson-vision-receives-approval-worlds-first-and-only-drug-releasing [Accessed: May 14, 2023]
Written By
Chukwuebuka Umeyor, Emmanuel Uronnachi, Abhit Nayak, Tochukwu Okeke, Purav Shah and Vandana Patravale
Submitted: 31 May 2023Reviewed: 11 July 2023Published: 02 August 2023
 Open access peer-reviewed chapter
Open access peer-reviewed chapter