Open Access is an initiative that aims to make scientific research freely available to all. To date our community has made over 100 million downloads. It’s based on principles of collaboration, unobstructed discovery, and, most importantly, scientific progression. As PhD students, we found it difficult to access the research we needed, so we decided to create a new Open Access publisher that levels the playing field for scientists across the world. How? By making research easy to access, and puts the academic needs of the researchers before the business interests of publishers.
We are a community of more than 103,000 authors and editors from 3,291 institutions spanning 160 countries, including Nobel Prize winners and some of the world’s most-cited researchers. Publishing on IntechOpen allows authors to earn citations and find new collaborators, meaning more people see your work not only from your own field of study, but from other related fields too.
To purchase hard copies of this book, please contact the representative in India:
CBS Publishers & Distributors Pvt. Ltd.
www.cbspd.com
|
customercare@cbspd.com
Peritonsillar and intratonsillar abscesses are one of the not too frequent emergencies encountered by the ENT fraternity. Tonsillitis refers to inflammation of the tonsils, whereas peritonsillitis refers to cellulitis with or without an abscess collection within the surrounding soft tissue of the tonsils. Peritonsillar abscess is often unilateral, while peritonsillitis may be bilateral in 20% of cases, whereas intratonsillar abscess is rare with an incidence of 7%. The shared symptoms of peritonsillitis and intratonsillar abscess include fever, trismus, deviation of uvula and referred pain. These shared symptoms have placed many physicians in a dilemma, resulting in an intratonsillar abscess to be missed. The medical therapy consists of intravenous antibiotics and intravenous fluids. A needle aspiration is useful when a diagnosis is uncertain. Aspiration of pus is diagnostic confirming a peritonsillar abscess from a peritonsillar cellulitis. Incision and drainage can be performed for intratonsillar abscess not responding to treatment or a failed needle aspiration, which is preferably performed under general anesthesia for children. Elective tonsillectomy should be indicated for patients with recurrent peritonsillar abscess. CT contrast is useful to identify complications arising mainly in retropharyngeal or parapharyngeal abscess and to know its extension, spread and drainage approaches.
Department of Otorhinolaryngology, Head and Neck Surgery, Universiti Kebangsaan Malaysia Medical Center, Malaysia
Balwant Singh Gendeh
Department of Otorhinolaryngology, Head and Neck Surgery, Universiti Kebangsaan Malaysia Medical Center, Malaysia
Pantai Hospital Kuala Lumpur, Malaysia
*Address all correspondence to: hardip88@gmail.com
1. Introduction
The tonsils are oval shaped lymphoid tissues situated at the oropharynx between the anterior and posterior pillars. Its boundaries are the soft palate superiorly, base of tongue inferiorly, palatoglossal arch anteriorly and palatopharyngeous arch posteriorly. It is part of the Waldeyer’s ring, named after Heinrich Wilhelm Gottfried von Waldeyer-Hartz who described the incomplete ring of lymphoid tissue within the nasopharynx and oropharynx in 1884 [1]. The ring consists of the pharyngeal tonsils (adenoids), tubal tonsils (tonsils of the torus tuberous), palatine tonsils and lingual tonsils. The earlier two are covered by stratified columnar epithelium while the latter two are lined by stratified non-keratinized squamous epithelium [1]. It is the palatine tonsils that are commonly referred to as tonsils by the lay person. Tonsils are involved in immunity as it is a form of lymphoid tissue rich in B cells that stimulates plasma cells and production of antibodies. It is most active within 4 to 10 years of age and in most individuals, undergoes involution after puberty.
Tonsillitis, peritonsillitis and intratonsillar abscess are pathology associated with inflammation of the tonsils and its surrounding soft tissues. Tonsillitis refers to inflammation of the tonsils. Peritonsillitis on the other hand refers to cellulitis with or without an abscess collection within the surrounding soft tissue (soft palate) of the tonsils. They are at different stages to the disease process, differentiated only by the presence of pus from the peritonsillar space. The peritonsillar space is essentially the loose connective tissue that separates the tonsils or its capsule which itself is part of the pharyngobasilar fascia. A peritonsillar abscess may be localized or occur within many small locules of the peritonsillar space [2]. This may cause aspiration of an abscess difficult, hence such cases are treated as a cellulitis. If abscess is evident and or drained within the peritonsillar space, then it is termed a peritonsillar abscess. Without imaging a peritonsillar abscess may be missed especially when there is no yield on aspiration or incision and drainage due to multiple small locules that are being missed. Peritonsillar abscess is often unilateral while peritonsillitis may be bilateral in 20% of cases [2].
An intratonsillar abscess occurs when the abscess is situated within the tonsillar parenchyma. It is rare and literature remains scarce with an incidence is 7%. Its presentation and appearance may be similar to peritonsillitis, thus making it difficult to be diagnosed and easily missed. For these reasons, the authors have chosen to discuss peritonsillitis and intratonsillar abscess, its presentation, diagnosis, and treatment.
Earlier understanding is that peritonsillitis occurs secondary to acute exudative tonsillitis. After all one may argue that it is the inflammation of the tonsils due to infection which is not resolving that may develop into a surrounding soft tissue infection or abscess collections [3]. The pathogenesis of tonsillitis will not be discussed in detail within this chapter. Acute exudative tonsillitis is commonly caused by group A beta hemolytic streptococcus which appears to be seasonal in certain countries [3]. However, literature has shown that the incidence of peritonsillitis does not coincide with that of an acute upper respiratory infection and acute tonsillitis. Kordeluk at al 2011 showed that the incidence of peritonsillitis was consistent all year round compared to acute tonsillitis and upper respiratory tract infections that were seasonal, which was commoner in the first two months of the year [4]. However, the study also found a significant relationship between acute tonsillitis and peritonsillitis occurring within the same week, indicating that peritonsillitis may be caused by the same pathogen as acute tonsillitis rather than being a sequela of it.
The presence of minor salivary glands termed Weber’s gland may be the culprit for infection resulting in peritonsillitis. These glands are concentrated at the upper region of the peritonsillar space at the soft palate superiorly and some may be found at the middle and inferior sections. These glands have ducts that open onto the surface of the tonsils inferiorly. Production of secretions is thought to aid cleaning of the tonsillar surface from food debris and digesting trapped food within the crypts. Tonsillitis or its inflammation causes obstructions of these ducts leading to abscess formation within the gland. These abscesses form the peritonsillar abscess superior to the tonsils at the soft palate [4, 5]. This may explain why patients post tonsillectomy do not develop peritonsillar abscess. There are two possible explanations to this, either the glands are taken out together with the tonsils during dissection or tonsillectomy has freed the obstruction from the ducts draining the Weber’s glands [4, 5, 6].
2.2 Intratonsillar abscess
Unlike peritonsillitis, the occurrence of intratonsillar abscess is believed to be a sequela of acute tonsillitis. There are two postulations to the occurrence of an intratonsillar abscess. Firstly, obstruction of the tonsillar crypts and secondly delay in lymphatic flow within the tonsils. In the earlier, tonsillar inflammation may cause direct extension to the crypts, causing it to be inflamed and obstructed. Presence of debris and localized infection results in multiple abscesses with the crypts. Furthermore, failure of contraction of the tonsillopharyngeous muscle prevents expulsion of debris within these crypts.
In the second cause, the tonsils are rich in blood supply and lymphatics. They may carry bacteria to the tonsils via hematologic or lymphatic route, resulting in a localized infection. Inflammation causes reduction in lymphatic flow, leading to stasis allowing the formation of a nidus of infection within the tonsils. Inflammation intensifies leading to necrosis and abscess formation. Combination of multiple small locules of abscess may form a large abscess collection within the tonsils. This may extend into the parenchyma. Therefore, intratonsillar abscess may occur concurrently with peritonsilitis [7].
Histopathology findings suggest that bacteria travel from the surface to the crypts and underlying parenchyma via valveless lymphatic flow. Lymphatic valves are thought to be present within the capsule and absent within the parenchyma. In healthy tonsils, lymphatic clearance occurs between 10 to 30 minutes, often too short for bacteria to proliferate. However, inflammation reduces these transit times allowing a medium and environment for bacterial proliferation [7, 8].
It is important to note that with the lack of imaging years ago, earlier intratonsillar abscesses were found incidentally from histopathological examination of the tonsils post tonsillectomy among patients with peritonsillitis undergoing a hot tonsillectomy [9]. Histology revealed abscesses within crypts extending to the parenchyma, presence of necrosis within the tonsils and microabscesses [9]. Table 1 below describes the differences in histology among tonsillitis, peritonsillitis and intratonsillar abscess [7].
Tonsillitis
Peritonsillitis
Intratonsillar abscess
Ulceration on squamous surface epithelium with neutrophils invasion
Ulceration on squamous surface epithelium with localized infiltration by neutrophils. Normal tonsillar parenchyma. Presence of neutrophils at peritonsillar space
ulceration of squamous surface epithelium. Localized infiltration of neutrophils extending into crypts. Abscess within parenchyma.
Table 1.
Differences in histology between tonsillitis, peritonsillitis and intratonsillar abscess.
2.3 Other causes
Dehydration has a role to play in peritonsillitis and intratonsillar abscess. One must not overlook other adjacent sources which are dental hygiene and sinus infections. Dental caries may be the source of infection more so in children. The authors have seen many children with recurrent tonsillitis, only to have their frequency improved by identifying and managing their oral hygiene. Furthermore, poorly controlled sinus related infections may be a culprit. Patients with allergic rhinitis may be predisposed to chronic rhinosinusitis and recurrent upper respiratory tract infection. This acts as a nidus of infection which may easily spread to the pharynx via a postnasal drip.
Similar to tonsillitis, common symptoms of peritonsillitis and intratonsillar abscess are sore, throat, odynophagia and referred otalgia. Referred otalgia also known as secondary otalgia is a referred pain due to the glossopharyngeal nerve innervation of the tonsils and pharynx. This pain is then referred to the medial aspect of the tympanic membrane via the Jacobson’s nerve [10, 11]. In tonsillitis the tonsils are erythematous and often bilateral.
In a peritonsillar abscess the soft palate is often inflamed with uvula deviation (Figure 1). This is often referred to as a curtain sign. This may easily be mistaken by medialization of the tonsils due to a space occupying lesion within the paraphryngeal space or deep neck abscess pushing the ipsilateral tonsils and lateral pharyngeal wall medially. Voice change or a hot potato voice is commoner in peritonsillitis as the edematous soft palate does not assist with phonation [6, 9]. Fever is common due to systemic infection [9]. Trismus may occur too especially when there is spread of abscess of cellulitis involving the pterygoids.
Figure 1.
Inflamed right peritonsillar region (PT) with inflamed soft palate touching the uvula (u). The tonsils were not inflamed. Image curtesy of HS Gendeh.
In intratonsillar abscess the tonsils may be inflamed with a unilateral enlargement. Uvula deviation is unlikely for an intratonsillar abscess. Furthermore, the soft palate may or may not be oedematous depending on the presence of a concomitant peritonsillitis [6, 9]. Like peritonsillitis, trismus may occur too.
Therefore, many signs and symptoms are shared between peritonsillitis and intratonsillar abscess with no clear demarcation. For these reasons, a CT neck is always recommended when an intratonsillar abscess is suspected. Surprisingly, symptom progression is faster among patients with peritonsillar abscess compared to intratonsillar abscess [12]. Recent publication by Ahmed Ali et al. 2019 had attempted to shed some light in differentiating the symptomatology of peritonsillar abscess and intratonsillar abscess. They found that patients with peritonsillar abscess are more likely to complain of otalgia, trismus and voice change compared to neck pain which was commoner in the intratonsillar abscess group. The latter may experience higher rates of cervical lymphadenopathy due to longer presentation of symptoms; contributing to neck pain [12]. Trismus should be less among the intratonsillar abscess as the abscess should lie within the tonsillar parenchyma and not spreading to the masseteric space. Shall an intratonsillar abscess present with trismus this could be due to complication due to disease extension of soft tissue oedema to these surrounding vital structures (Table 2).
Fever Trismus Deviation of uvula Referred pain
Table 2.
Shared symptoms of peritonsillitis and intratonsillar abscess [9].
The management of a patient with peritonsillitis or intratonsillar abscess ranges from bedside examination to a hot tonsillectomy. It is vital to differentiate the two due to their different management.
4.1 Clinical examination
Clinical examination is vital. A good oral examination with a headlight or adequate light source will allow the doctor to evaluate if there is any tonsillar swelling. Kindly lookout for a unilateral or bilateral swelling (Figure 2). Bilateral tonsils may be inflamed, enlarged with or without exudates in cases of tonsillitis. The oral cavity is examined for soft palate inflammation and/or uvula deviation. Dentition is assessed for caries which may be a source of infection especially for children. Some patients may have halitosis due to salivary stasis from reduced swallowing. If there are rhinitis symptoms, a nasal endoscopy will be useful to rule or rhinosinusitis. Examination of the neck may reveal lymphadenitis. Large swelling may suggest a deep space collection.
Figure 2.
An elderly lady presented with odynophagia for 3 months. Examination revealed an enlarged right tonsil with smooth surface. She had no history or indications of an infective process and malignancy should be suspected. Right tonsillar biopsy revealed a right tonsillar malignancy. Picture curtesy of HS Gendeh.
4.2 Bedside needle aspiration
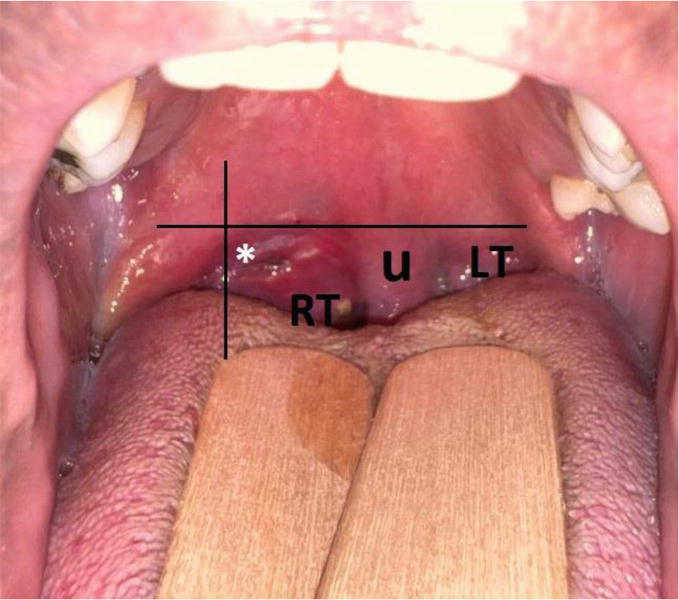
When there is swelling and erythema of the soft palate and a peritonsillar abscess is suspected, a needle aspiration can be attempted as both diagnostic and therapeutic. Drainage is the gold standard for peritonsillar abscess. The area of aspiration should be that of the most fluctuant below the horizontal imaginary line of the soft palate and medial to the vertical imaginary line of the anterior pillar. The needle should be inserted straight and not laterally whereby the carotid artery is located (Figure 3). Depth should not be beyond 0.8 cm [13]. In order to prevent further insertion, the proximal two thirds of the needle may be lined with tape, or some have suggested the use of a needle guard whereby its distal third has been trimmed [13]. If the initial aspiration has failed, this can be tried again at lower levels above the tonsils. If successful, pus will be aspirated into the syringe, which can be sent for culture and sensitivity.
Figure 3.
The area for needle aspiration for left tonsillar abscess should be at the area of most fluctuant below the horizontal imaginary line of the soft palate and medial to the vertical imaginary line of the anterior pillar labeled *. U: Uvula; RT: Right tonsils; LT: Left tonsils. Picture curtesy of HS Gendeh.
A needle aspiration is also useful when a diagnosis is uncertain. Aspiration of pus is both diagnostics confirming a peritonsillar abscess from a peritonsillar cellulitis and therapeutic. A needle aspiration is also useful when a Computed Tomography (CT) scan is hard to come by for confirmation of a peritonsillar collection. However, a needle aspiration may miss a collection with a false negative rate of 10 to 24% [14]. In such cases, if still in doubt it is wise to admit the patient and treat the patient with antibiotics or consider imaging shall the patients symptoms worsen or not respond to antibiotics. Ophir et al. suggested that all patients with peritonsillar swelling, should undergo a needle aspiration. Shall there be no yield on three sides, thus a diagnosis of peritonsillar cellulitis is made [15].
Many have advocated needle aspiration for an intratonsillar abscess with or without imaging guidance. Without imaging guidance, the needle shall be placed at the medial border of the tonsils and directed laterally without crossing the lateral border of the tonsils. Approximately 63% of patients with intratonsillar abscess received needle aspiration with a 15% success rate [12].
4.3 Incision and drainage
For an incision and drainage, the patient should be seated to prevent aspiration of pus. A suction is handy to aspirate the pus. A 11-size blade is prepared. The authors prefer securing the proximal end of the blade with tape exposing the distal 5 mm of the blade [16]. This is to ensure that the blade does not penetrate too deep beyond the abscess. Local anesthesia may be injected or applied topically with a spray. Similarly, a small incision is made at the most fluctuant are below the horizontal imaginary line of the soft palate and medial to the vertical imaginary line of the anterior pillar. Alternatively, if a needle aspiration was successful prior, the incision should be made at the site of aspiration. A sinus forceps can be used to widen and break the loci. The patient is then required to gargle his or her oral cavity. Bear in mind that the incision site may close and will be required to be reopened from time to time to allow complete drainage and prevent re-accumulation of pus. Some have suggested flushing the cavity with a bactericidal solution using a syringe and cannula void of its inner needle. However, the authors do not recommend it nor is it recommended to insert a ribbon gauze to keep the cavity open.
What happens if both needle aspiration and incision and drainage fail to yield any pus collection? There are three possibilities being site of aspiration and incision did not target the loci of collection, the patient has peritonsillitis rather than a peritonsillar abscess, the patient may be suffering from an intratonsillar abscess. At this conjecture, one may consider giving some time for intravenous antibiotics to work. Should the swelling not reduce, or symptoms worsen, imaging should be considered to rule out the possibilities. The evidence of when to perform imaging is still lacking and it is not wrong to perform imaging earlier when no yield is obtained.
Incision and drainage can be performed for intratonsillar abscess not responding to treatment or failed a needle aspiration. Th incision should be made at the medial surface of the tonsils directed towards its center avoiding its lateral border.
Contraindications to a needle aspiration and incision and drainage are a severe trismus. The above two can be done under local anesthesia for an adult. However, for children, it is certainly recommended to be performed under general anesthesia.
4.4 Imaging
In the earlier years, imaging used to be reserved for peritonsillitis not responding to treatment or if there are suspicions of complication a deep neck abscess. However, the improved and easier access to CT imaging in tertiary referral centers have resulted in imaging to be performed even before treatment is initiated with antimicrobial therapy or needle aspiration. Clinical diagnosis of peritonsillitis has a sensitivity of 78% and specificity of 50% when compared to CT imaging [17]. The authors would reserve imaging where a peritonsillitis is not resolving or worsening with antibiotics despite negative aspiration. In other words, when a peritonsillar cellulitis diagnosis is in doubt. Contrast CT of the head and neck may indicate a rim enhancing collection superior to the tonsil in a peritonsillar abscess or within the tonsils in an intratonsillar abscess (Figure 4). There may be surrounding soft tissue oedema and cervical lymphadenopathy. On the other hand, intra tonsillar abscess diagnosis often requires imaging for confirmation [12]. This may explain the underdiagnosing and under reporting of intratonsillar abscess prior to this due to the more cautious use of imaging.
Figure 4.
Contrasted axial CT neck showing a rim enhancing hypodence collection of the left palatine tonsil (orange arrow) representing a left intratonsillar abscess. Note the lateral calcification (yellow arrow) representing a tonsilolith. A tonsilolith may cause obstruction to the lymphatic outflow of the tonsils resulting in an intratonsillar abscess. Image curtesy of HS Gendeh.
Neck radiographs have little value in diagnosing peritonsillitis or intratonsillar abscess. It may be useful to identify a retropharyngeal abscess as a complication. Shall there be a retropharyngeal abscess, a CT is often required to identify extension, spread and drainage approach [18, 19].
Ultrasonography on the other hand has proven to be effective in differentiating a peritonsillar cellulitis and abscess in the emergency department upon presentation [17]. Presence of fluid within the posterior pharynx can be identified/It is also handy to guide a needle aspiration of a peritonsillar abscess which is both diagnostic and therapeutic, more so for smaller loci. Some have even reported the use of ultrasonography in the emergency department to drain the abscess and discharge the patient with antibiotics without further complications [14]. The downside of ultrasonography is it is operator dependent and ENT surgeons may not be trained in using them.
4.5 Intravenous antibiotics
Among 48 aspirations of peritonsillar abscess, there were 58 anaerobic and 49 aerobic bacteria isolated. Among the aerobic group, streptococcus group, Haemophilus group and staph aureus are the organisms isolated. Anaerobes are common owing to their presence in the oral cavity. Many patients had a combination of aerobes and anaerobes. Moreover, more than half of the specimens had B lactamase producing organisms resistant to penicillin [20]. Klung et al. revealed that the most common bacteria were streptococcus viridans, Group A beta haemolytic streptococcus, F necrophorum and staph aureus [21]. Co-amoxiclav is the most prescribed antibiotic followed by clindamycin. Duration of antibiotics ranged from five to fourteen days with 10 days being most popular [22]. Many authors have recommended a broad-spectrum antibiotic with or without metronidazole or penicillin with a second antibiotic with b lactamase activity. Certainly, due to its rarity there has yet to be recommendations for intratonsillar abscess [20].
Patients presenting with a peritonsillar cellulitis or peritonsillar abscess may be septic. They may have odynophagia with a decrease in oral intake. Therefore, hydration assessment is important and do not hesitate to convene intravenous fluids as appropriately.
5.1 Tonsillectomy
A tonsillectomy performed during an ongoing infection of a peritonsillitis or intratonsillar abscess is term an immediate or hot tonsillectomy. Earlier literature recommended a hot tonsillectomy as a treatment of the above two [23]. However, recent evidence suggests that adequate drainage of collection of a peritonsillitis or intratonsillar abscess with systemic antibiotics is sufficient to resolve infection. Therefore, the authors have never required to perform a hot tonsillectomy for the above two indications in their institution. Only once a hot tonsillectomy had to be performed for a non-resolving tonsillitis with pyrexia despite being on prolonged intravenous antibiotics. The risk of a hot tonsillectomy is bleeding due to ongoing inflammation and infection. Certainly, the availability of powered instruments such as an ultrasonic scalpel does reduce this risk.
An elective tonsillectomy should be considered among patients with recurrent peritonsillar abscess or recurrent peritonsillar abscess twice or more. Some authors have suggested that a single episode is sufficient to warrant an elective tonsillectomy. This is because 90% of patients with peritonsillar abscess do not have recurrence [24]. In summary, Figure 5 depicts a flow chart on the management in identifying a peritonsillar abscess and an intratonsillar abscess.
Figure 5.
A suggested flow chart on the management in identifying a peritonsillar abscess and an intratonsillar abscess. I&D; incision and drainage.
A large collection has a potential to cause upper airway obstruction, more so if it is complicated with a retropharyngeal abscess. This is an emergency, and the airway must be secured first.
A retropharyngeal lymph node drains lymphatics from the posterior part of the nose, nasopharynx, and adenoids. Therefore, infection from the palatine tonsils may spread retrogradely to the retropharyngeal lymph nodes. Suppuration of these lymph nodes results in a retropharyngeal abscess [25]. The left and right retropharyngeal spaces are in communication; thus, the patient may have a bulge in the posterior pharyngeal wall (Figure 6). Airway compromise may occur if severe enough.
Figure 6.
Lateral neck radiograph of a child with retropharyngeal abscess. Appreciate the increase in horizontal distance between the pharynx anteriorly and vertebrae posteriorly. The posterior pharyngeal wall is pushed anteriorly. Picture curtesy of HS Gendeh.
The retropharyngeal space spreads from the skull base cranially to the posterior mediastinum caudally. Therefore, if severe enough it may be a pathway to mediastinitis [25]. Buccopharyngeal fascia forms the anterior boundary while the prevertebral fascia forms the posterior boundary.
The retropharyngeal space connects directly to the parapharyngeal space. The Parapharyngeal space is a potential space containing lymph nodes that may undergo suppuration. It is not surprised that peritonsillar retropharyngeal and parapharyngeal infections are termed deep neck infections.
6.3 Intracranial involvement
Very rarely would a patient present with intracranial complications. However, local spread of infection may result in cavernous sinus thrombosis, brain abscess, meningitis, or osteomyelitis of the sella turcica.
6.4 Recurrent abscess
Recurrent abscess is reported to be in 15% and 7% for peritonsillar abscess and intratonsillar abscess respectively. Limited case reports of ipsilateral brain abscess and peritonsillar abscess [26].
The presence of minor salivary glands termed Weber’s gland may be the culprit for infection resulting in peritonsillitis. An intratonsillar abscess occurs when the abscess is situated within the tonsillar parenchyma and may occur concurrently with peritonsilitis. Dehydration has a role to play in peritonsillitis and intratonsillar abscess and the medical therapy consists of intravenous antibiotics and intravenous fluids. Poor management can result in complications like retropharyngeal abscess, parapharyngeal abscess, mediastinitis and upper airway obstruction and CT scan with contrast is essential to know its extension, spread and drainage approaches. Aspiration of pus is diagnostic confirming a peritonsillar abscess from a peritonsillar cellulitis. Incision and drainage can be performed for intratonsillar abscess not responding to treatment or a failed needle aspiration which is preferably performed under general anesthesia for children. Elective tonsillectomy should be indicated for patients with recurrent peritonsillar abscess. Thus, a clear understanding of peritonsillitis and intratonsillar abscess, its presentation, diagnosis and treatment is of outmost importance to physicians dealing with the airway and food passageway.
References
1.Crumbie L, Chaves C. Waldeyer Ring. Available from: https://www.kenhub.com/en/library/anatomy/waldeyers-ring [Accessed: March 6, 2023]
2.Fried MP, Forrest JL. Peritonsillitis: Evaluation of current therapy. Archives of Otolaryngology. 1981;107(5):283-286. DOI: 10.1001/archotol.1981.00790410021004
3.Woolley BJWAL. Cummings Otolaryngology Head & Neck Surgery. St Louis, MO: Mosby; 2005
4.Kordeluk S, Novack L, Puterman M, Kraus M, Joshua BZ. Relation between peritonsillar infection and acute tonsillitis: Myth or reality? Otolaryngology and Head and Neck Surgery. 2011;145(6):940-945
5.Galioto JN. Peritonsillar Abscess. American Family Physician. 2017;95(8):501-506
6.Powell EL, Powell J, Samuel JR, Wilson JA. A review of the pathogenesis of adult peritonsillar abscess: Time for a re-evaluation. The Journal of Antimicrobial Chemotherapy. 2013;68(9):1941-1950
7.Blair AB, Booth R, Baugh R. A unifying theory of tonsillitis, intratonsillar abscess and peritonsillar abscess. American Journal of Otolaryngology. 2015;36(4):517-520
8.Loo BW Jr, Draney MT, Sivanandan R, Ruehm SG, Pawlicki T, Xing L, et al. Indirect MR lymphangiography of the head and neck using conventional gadolinium contrast: A pilot study in humans. International Journal of Radiation Oncology, Biology, Physics. 2006;66(2):462-468
9.Childs EW, Baugh RF, Diaz JA. Tonsillar abscess. Journal of the National Medical Association. 1991;83(4):333-336
10.Chen RC, Khorsandi AS, Shatzkes DR, Holliday RA. The radiology of referred otalgia. AJNR. American Journal of Neuroradiology. 2009;30(10):1817-1823
11.Greenhall CJ, Rhys R. The radiology of referred otalgia. American Journal of Neuroradiology. 2014;23(2):1817-1823
12.Ali SA, Kovatch KJ, Smith J, Bellile EL, Hanks JE, Truesdale CM, et al. Predictors of intratonsillar versus peritonsillar abscess: A case-control series. The Laryngoscope. 2019;129(6):1354-1359
13.Roberts JRMD. InFocus: Mastering aspiration for Peritonsillar abscess. Emergency Medicine News. 2018;40(12):8-9
14.Lyon M, Blaivas M. Intraoral ultrasound in the diagnosis and treatment of suspected peritonsillar abscess in the emergency department. Academic Emergency Medicine. 2005;12:85Y88
15.Ophir D, Bawnik J, Poria Y, Porat M, Marshak G. Peritonsillar abscess. A prospective evaluation of outpatient management by needle aspiration. Archives of Otolaryngology, Head and Neck Surgery. 1988;114:661-663
17.Scott PM, Loftus WK, Kew J, et al. Diagnosis of peritonsillar infections: A prospective study of ultrasound, computerized tomography and clinical diagnosis. The Journal of Laryngology and Otology. 1999;113:229Y232
18.Honnegowda T, Silvia WD, Babu VS. Clinical evaluation and management of deep neck space infections. International Journal of Head and Neck Surgery. 2017;8(3):102-106
19.Sakaguchi M, Sato S, Asawa S, Taguchi K. Computed tomographic findings in peritonsillar abscess and cellulitis. The Journal of Laryngology & Otology. 1995;109(5):449-451
20.Brook I, Frazier EH, Thompson DH. Aerobic and anaerobic microbiology of peritonsillar abscess. The Laryngoscope. 1991;101(3):289-292
21.Klug TE, Greve T, Hentze M. Complications of peritonsillar abscess. Annals of Clinical Microbiology and Antimicrobials. 2020;19(1):32
22.Wu V, Manojlovic Kolarski M, Kandel CE, Monteiro E, Chan Y. Current trend of antibiotic prescription and management for peritonsillar abscess: A cross-sectional study. Laryngoscope Investigative Otolaryngology. 2021;6(2):183-187
23.Hsu C-H, Lin Y-S, Lee J-C. Intratonsillar abscess. Otolaryngology-Head and Neck Surgery. 2008;139(6):861-862
24.Powell J, Wilson JA. An evidence-based review of peritonsillar abscess. Clinical Otolaryngology. 2012;37:136-145. DOI: 10.1111/j.1749-4486.2012.02452.x
25.Esposito S, De Guido C, Pappalardo M, Laudisio S, Meccariello G, Capoferri G, et al. Retropharyngeal, Parapharyngeal and Peritonsillar abscesses. Children (Basel). 2022;9(5):618
26.Sankararaman S, Riel-Romero RM, Gonzalez-Toledo E. Brain abscess from a peritonsillar abscess in an immunocompetent child: A case report and review of the literature. Pediatric Neurology. 2012;47(6):451-454
Written By
Hardip Singh Gendeh and Balwant Singh Gendeh
Submitted: 31 March 2023Reviewed: 29 May 2023Published: 16 June 2023
 Open access peer-reviewed chapter
Open access peer-reviewed chapter