 Open access peer-reviewed chapter
Open access peer-reviewed chapter
Abstract
In implementing Universal Health Coverage (UHC), public healthcare financing is the dependable mechanisms to ensure equity and to minimize catastrophic health spending. However, public financing often creates long queueing and low satisfaction of the community and is less responsive to the demand from the public. On the other hand, the private sector has advantages in responding to the demand of the patients, higher efficiencies, and having higher customer or patient satisfaction. The combination of the two sectors is the best in achieving UHC. The government must provide and regulate the room for the private sector. However, the private sector has limitations in developing services because of obstacles in providing appropriate healthcare for everyone without conflicting with the business goals. In general, there are three roles of the private sector to be adopted in the health system of countries to ensure equitable access to quality healthcare, provide options, facilitate higher satisfaction for patients, increase private sector opportunities to participate in providing health services, that potentially establish competition that will improve the quality of services.
Keywords
- health insurance
- private sector
- universal health coverage
- public-private mix
- public financing
1. Introduction
A country’s health system includes relevant organizations and resources, including personnel, funds, facilities, and technologies, among other things, to provide health services to its population. Currently, most people in developing countries face obstacles in obtaining access to appropriate and quality services, resulting in severe risk of illness. In general, all countries in the world provide public healthcare providers with free access or small user fees. Yet, many people in developing countries still rely on out-of-pocket payments, especially private providers or in rural areas where the public providers are unavailable [1, 2, 3, 4]. Private healthcare providers normally provide complement or supplement healthcare as options to public healthcare provision. In general, public providers or public health insurance has the advantage of ensuring equity in access to healthcare. But, often public provision or public health insurance is perceived as providing poor quality of care. Private providers or private health insurance are perceived better in providing perceived quality of services. Those who have health insurance or have access to public healthcare providers have a higher chance of receiving care [5, 6]. The right combination of public and private roles in ensuring access to healthcare and eliminating financial hardship in meeting healthcare needs is a big challenge to achieving universal health coverage (UHC) in many developing countries.
The World Health Organization (WHO) defines UHC as the ability of individuals to obtain health services they need without suffering financial hardship [7] as best achieved by Model 1 [8]. This supplemental or top-up option by the private sector is not well understood by many policymakers in developing countries. The balance roles between public and private insurance or providers must be thoroughly examined to ensure equity, efficiency, sustainability, and effectiveness of the health system [8]. The WHO’s 13th General Programme of Work has conducted a systematic analysis of barriers to service access, which provides evidence-based solutions for UHC [9]. The implementation of national (public) health insurance or publicly funded healthcare enables people to access the healthcare they need. However, many high-income people who perceive public provisions as poor quality prefer to use private insurance or high pay out of pocket in private healthcare providers [10, 11].
The private sector—including both insurance companies and healthcare providers—has an important role in ensuring access to health services. The private health sector provides health coverage to individuals or organizations that are neither owned nor directly controlled by the government in the distribution of health services. The private sector continues to improve in providing healthcare services, catering to more than a third of the total medical care needs in many developing nations. These developments are influenced by a growing middle class and an increasing demand for quality healthcare, macroeconomic stability and liberalization, poor public sector management, and operational practices [12, 13]. The development of private health insurance is determined by the variability in economic status (per capita expenditure) and education in society [14]. It should be noted that the private sector lags in ensuring equitable access for everyone. Because of market failure in healthcare services, the private sector’s role is limited to complementing the public sector, especially in health financing, such as in insurance.
In implementing UHC, the government must provide room for the private sector so that there is a healthcare option for higher-income groups [15]. In this regard, this study assesses the potential of the private sector and strengthens private role models to complement UHC in the health insurance system by considering the challenges faced and plans for improvement in this sector.
2. The private sector as an under-utilized entity
The private health sector is recognized as an important player in any health system, but many policymakers do not know the extent of its strengths and limitations. In some countries, efforts by the public sector to collaborate with private providers face political constraints, but there are many other opportunities for maximizing the sector to help improve public health [16]. Private insurance caters to several chronic diseases and can help to reduce the burden of personal medical expenses for policyholders [17]. Private health insurance has the potential to provide healthcare via good coordination with the public sector [18, 19].
The United Nations Sustainable Development Goals (SDGs) comprise 16 targets that are set to be achieved by 2030 and that are directly or indirectly related to health. Both the private and public sectors should work hand in hand to meet health-related SDG 3.8 on UHC and related goals, such as SDG 8 (decent work and economic growth) and SDG 9 (industry, innovation, and infrastructure) [20]. The participation of the private sector to achieve the SDG goals is strengthened by the following statement by Norimasa Shimomura, resident representative of the United Nations Development Programme Indonesia: “The SDGs cannot be achieved without contributions from the private sector, and vice versa, business actors cannot continue their business practices without the SDGs, where the SDGs can create a supportive environment for sustainable business” [21].
The government must determine the interrelationship between the roles of private health insurance and national (public) health insurance. Public–private partnerships have the potential to achieve the best health indicators for publicly funded health care. Public–private partnerships are a viable alternative, as the public sector faces constraints in meeting the growing need for quality health services by higher-income groups [22]. However, it must be acknowledged that private health insurance will not be able to provide coverage for low-income people, those who live in rural areas, and high-risk groups, such as the elderly and persons with disabilities.
3. The private sector as a partner in fostering innovation
Innovation often occurs in the private sector, as it must continue implementing changes to remain competitive. Private health insurance has developed 14 rules that are used as guidelines for evaluating insurance claims [23]. Internally, innovation in the private sector develops in relation to people, resources, and the vision and mission. Cultural innovation, organizational learning, and private organizational commitment have positive and significant effects on organizational performance. The factors that encourage the development of innovation are government policies, technological advances, and the emergence of other private companies [23]. Innovation pursued by the private sector in tackling societal problems in health and education can also benefit the public sector [24].
Despite some external environment-related challenges, such as in terms of infrastructure, operational costs, and customers or service users, private insurance has relied heavily on the use of telemedicine during the COVID-19 pandemic [25, 26]. In collaboration with the public, the private sector has succeeded in creating better services and developing business models in PHC [27]. To achieve the best results, public–private partnerships harness the strengths of the public and private sectors together, creating expanded access to health services for underserved communities. These partnerships can produce sustainable benefits for the private sector [28].
4. Partnering with the private sector as a path to universal health coverage
To achieve UHC, many state governments are engaging with the private sector to improve the public’s access to quality primary health services. Most countries generally award command and control to the private sector, rather than providing incentives or allowing self-regulation. The arrangement requires private facilities to have a minimum number of doctors with special qualifications and a minimum number of infrastructure and equipment to provide health services. National health insurance (NHI) can pay capitation with performance incentives to private facilities that provide services. Likewise, private facilities are given accreditation scores associated with reimbursement payments [29].
National health insurance schemes suggest an opportunity for accredited private healthcare providers to serve low-income populations, but this would entail strengthening monitoring and accountability to reduce costs and maintaining a certain quality level to continue receiving public financing. Private service providers consider accreditation to be important to the continuity of their businesses, even though they find lengthy and convoluted accreditation processes a major obstacle to their participation in the public health insurance system. Private service providers would like to comprehend NHI, and they see an opportunity to participate. They are ready to undergo the accreditation process and engage in payment arrangements that will complement the implementation of NHI and thus provide a higher level of patient satisfaction [30].
The private health sector supports the implementation of UHC, and in Indonesia, government assistance accounts for half of the growth of private hospitals, in line with good governance initiatives to achieve UHC; around 32.6% of hospitals are integrated with community-centered health services [31]. Thus, it is increasingly clear that private sector participation is an integral part of efforts to achieve UHC.
5. Challenges
A framework for determining strategies to engage the private sector has been introduced. However, the existence of the private sector is often not appreciated because of varied understandings of the sector. Public and private cooperation in health insurance shows that there are challenges and constraints posed by contextual conditions in designing contracts for financing and providing healthcare. The presence of health insurance systems that are integrated between government/public insurance and private insurance have resulted in disparities in access and inappropriate health service outcomes at the primary care level [32]. Governments seek to implement a combination of private and public health insurance systems to support equity and promote effective PHC services.
There are also differences in views when interpreting the quality of services between implementers (health service providers) and the beneficiary community, thus significantly affecting the quality of health services itself. Implementers feel that beneficiaries have good access to the service, but beneficiaries think otherwise. From an implementer perspective, quality is assessed based on ease of referral, effectiveness in monitoring, timeliness, efficiency, replacement, and compliance with healthcare standards, guidelines, and accreditation processes. On the other hand, community beneficiaries evaluate processes based on essential health services, including medical consultations; diagnostics services; and the provision of medicines [33]. The discrepancy in views on the role of the private sector is mainly driven by political factors, such as economic transition, decentralization of the health system, and increased costs. Future policies to increase the role of the private sector in achieving health development goals require data collection on the efficiency, quality, and equity of private services [34].
Private insurance schemes are not equitable to the public and are reserved only for those who can afford them as supplemental insurance, particularly those who live in urban areas, while NHI can cover all people to achieve UHC. The Public funding, both tax-funded and SHI scheme pools risk-sharing contributions on proportion or percentage of individual or family income. The SHI basically similar to income tax with the difference is that income tax is normally progressive while SHI contribution can be regressive, if there is a ceiling income such as implemented in Indonesia [8]. Yet, SHI implemented as a single-payer at the national level could result in long queue in healthcare providers. Complement and supplemental insurance by private insurance for higher income people or corporate paid supplemental insurance could offer some solution to cut off the line by offering executive clinics.
Various international initiatives have been made to involve the private sector in the efforts of countries to complement UHC for the higher-income population. A PHC global agreement expects UHC to operationalize the progressive realization of the PHC vision and the right to health. The WHO strongly supports mixed systems governance to ensure the optimal combination of the private and public sectors in achieving UHC, as public funding is optimal for equity while private providers are good on quality of care. Private insurance is not good to ensure access for everyone because in financial protection the private insurance will set premiums on a risk-base. The higher risk individuals such as the elderly and the low-income will not be able to afford the premiums [8, 19]. Underlining the operational understanding of the provision of health services to achieve UHC can divide the scope of the private sector in both insurance and healthcare delivery in public funding systems. Championing UHC requires a commitment to becoming the health anchor for all implementations in the country by involving civil society and communities in all relevant processes and by acting responsibly in relation to such a commitment [35].
6. Private role models to achieve universal health coverage
Understanding the relationships of the parties involved in the healthcare and health insurance systems could provide the role of the private sector in achieving UHC without jeopardizing access to low-income and high-health risk people. The following general three models of the roles of the private health sector could be used as general guidance for low- and middle-income countries (LMICs).
Model 1: The private sector as health service providers.
Model 2: The private sector as a supplemental health insurers.
Model 3: The private sector as a supplemental buyer of health services for the employees.
6.1 Model 1: private sector as healthcare providers
Facilitating the role of the private sector as a provider of health services by having annual pay performance with NHI or NHS requires legal reform. Private health services contract with national insurance administrator (s) to deliver the benefits covered for the NHI members or the population. To ensure the quality of services provided to meet the needs for healthcare, the private providers must meet the terms and conditions to ensure service quality. The regulations set by the NHI or NHS normally cover tariffs that can be fee for services, per procedures, per diagnosis, per diem rates, procedures, claim mechanisms, payment schedules, and liability reports.
The government sets standards related to the accreditation of healthcare providers to ensure service quality is provided at convenient office hours, reasonable queueing time, and competency of medical personnel. Hospital accreditation includes patient safety, access to hospitals and continuity, patient and family rights, anesthesia, surgical services, pharmaceutical services, communication, and education management. Primary healthcare accreditation includes administration and management, patient-oriented clinical services, clinical service support management, clinical quality improvement, patient safety, and clinical performance indicators. To be able to enter a contract with the NHI; private healthcare providers must fulfill varification process to reduce practices of moral hazards or fraudulence. In some countries, the NHI or NHS establishes strict referral health procedures for efficiency. In managing the balance between efficiency and quality of care, patient satisfaction survey should be conducted regularly.
It is inevitable that the NHI/NHS needs to prioritize contracts with healthcare providers accepting cheaper healthcare, both from public and private healthcare providers. In some countries, There are regulations that give government health facilities the authority to use their income directly without depositing it into the state treasury. Therefore, health facilities can use their income according to their plans and budgets. They can set competitive rates with private healthcare providers. In Indonesia, public healthcare providers (puskesmases) are given too large number of members while the puskesmases also must provide public health services. So, there are pressures to reduce the puskesmases burden for medical care to ensure that the staff could not deviate their attention too much on serving the NHI patients and neglecting their primary mandates of providing health promotion and prevention.
The advantage of model 1 is that the private sector contracted will ensure a sizable market. The best rule is the government should ensure that members of NHI or people under the NHS have the right to choose public or private healthcare providers, while the NHI or NHS will pay for healthcare consumed by members or people at reasonable rates. This money follows the patient principle and will provide fairness in financing and delivering care (Figure 1).
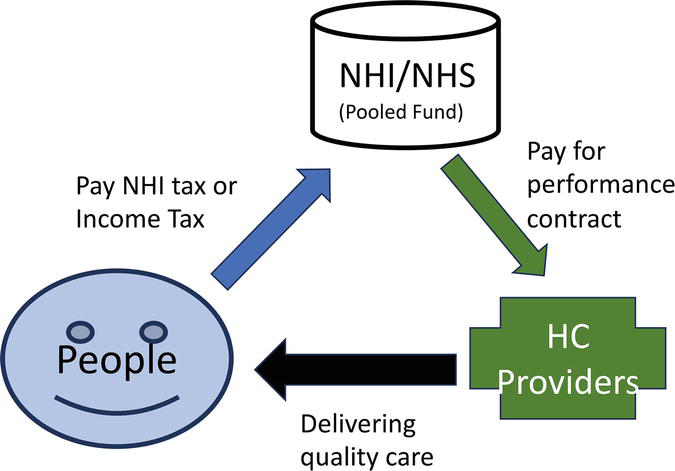
Figure 1.
Publicly funding and privately delivery healthcare.
6.2 Model 2: private sector as health insurers
Naturally, health insurance is the rational response to the uncertainty of the need for medical care, which results from uncertain risks of illnesses. The law of the large number allows an insurer to predict the amount of money needed to share among policyholders. The premiums are set based on the probability of a group to experience illhealth and the average claim costs once illhealth occurs by an insured. So, the premium is set on an expected risk-based. However, the risk-based premiums are not affordable by low-income or high-risk people, resulting in inequity and unacceptable reality by humanity’s norms. Therefore, the private health insurer’s roles are limited and cannot be the only funding mechanism for medical/healthcare.
The advantage of private health insurers is the responsiveness to the demand and the attractiveness to finance healthcare especially private healthcare providers. It is a good solution to offer as supplemental or complemental financing for high-income groups, mainly for corporations that want to attract high-competence employees. It could contribute to UHC by offering health benefits according to market demands, but not by the needs of the people. Certainly, private insurers are unable to reach the entire population of a country.
Expanding the roles of private health insurers needs strict licensing requirements because of a high information asymmetry between the insurers and the policyholders. They must be staffed with proven competent of human resources in managing health insurance and ensuring the insured gets healthcare fairly. Private health insurers may apply managed care techniques popular in the USA by applying prospective payment and rigid utilization reviews to contain costs. Private health insurers often conduct selective contracting to choose only credible healthcare providers to gain competitive advantages in attracting policyholders. In some countries where public healthcare providers are given autonomous status, private insurers can enter into a contract with them and receive competitive prices (Figure 2).
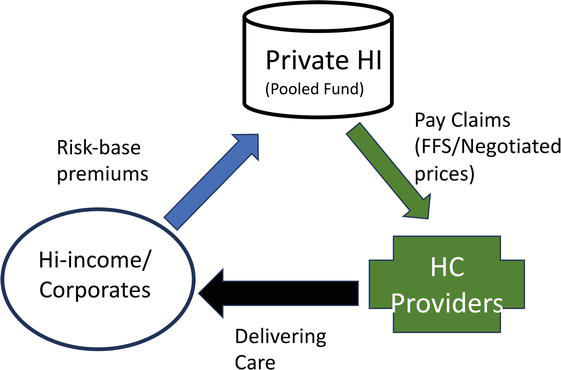
Figure 2.
Private sector as private insurers.
To attract qualified employees, private companies offer adequate healthcare coverage. In fact, many countries require that every company guarantees the health services of its employees through the insurance system. In this case, the company will consider the guaranteed benefits offered by health insurance, starting from benefits for top-level managers to ordinary employees. The advantage of model 3 is that companies that are aware of their participation in the health insurance system will likely support the achievement of UHC.
If the state implements a mandatory NHI policy, the company is faced with the choice of including or not including employees, with the consequence of violating mandatory laws. It is a reality that several private companies have not registered their employees as insurance participants, either because of the company’s income level or because the employee’s income is inadequate. This could also be due to the influence of private company labor unions that do not support insurance participation because they are not satisfied with the perceived benefits. Thus, private companies that have not yet registered their employees may look at the appropriateness of the benefits offered by insurance organizations. Good communication is needed to achieve UHC and bring together the interests of two parties in accordance with existing regulations.
In countries that implement a national health insurance system organized by the government, and provide space for private insurance organizations to develop, it could happen that private companies as participants can participate in two insurance systems at once with appropriate benefits. In double-insured conditions, this must be avoided so that there are no double payments so that financing efficiency is maintained. The health insurance system recognizes coordination of benefits, which is an agreement between insurance organizations as to who will pay first and who will pay the rest, so that no one is harmed by each other. Likewise, participating insurance companies can also experience the benefits of participating in more than one insurance company.
6.3 Model 3: private sector as buyer of healthcare for the employees
The private sector is normally aggressive and innovative in meeting their needs as the regulations allow them to do. In many countries where there is no NHI or NHS or even there is a public funding system for healthcare available, many employers could contract directly with healthcare providers to take care of their employees. Depending on the size of private employers, the size and the scope of contracting healthcare services vary widely. Large and reputable private employers need to attract competent or professional employees to boost productivity. Often, companies or private employers provide employment benefits (perks) such as healthcare, pension, family benefits, or even leisures for part or all employees. The perk can be sole benefits or supplemental benefits for the existing social security schemes.
The scheme can be delivered as service benefits in which private employers sign contracts with a single or a network providers or employees could pay directly the healthcare providers and get reimbursement from the department of human resources. The scheme could be very efficient and could also be expensive because the economic scale is small. Medium companies often have less power to contract with healthcare providers. For medium companies, insuring employees with or without immediate family members is more efficient and more convenient for the employees.
Other form of the private sector is individual person or family who may purchase healthcare and pay out of pocket or use public healthcare providers and pay small user charges. This form of the role of the private sector is the most regressive and can impoverish family or individual to pay high costs of inelastic healthcare. Often individual or family has no option and is imposed to pay high cost healthcare (Figure 3).
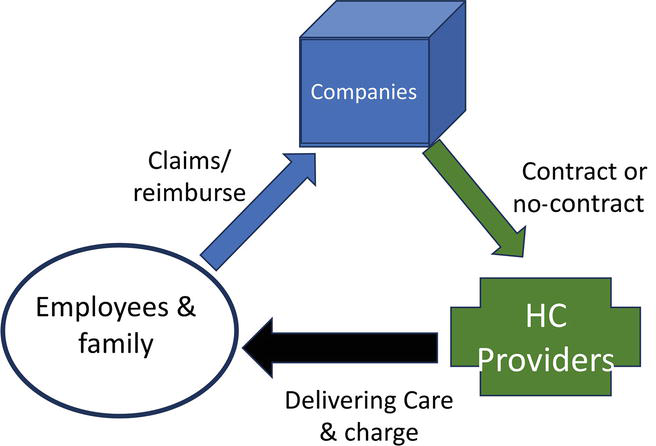
Figure 3.
Private sector as buyers of healthcare of employees.
7. Conclusion
Countries differ in their adoption and implementation of facilitating private sectors in the country’s health systems. In general public sector is superior in ensuring equity of healthcare, making low-income individuals could get access to healthcare with or without user fees or paying out of pocket. However, the public sector is often less responsive to the demand for quality of care, and often access to public healthcare providers requires long queueing. On the other hand, the private sector is not good to ensure equity as the private sector must ensure the return on investment and making profit or surplus for growth. The private sector is responsive to the demand from patients and is good at delivering quality care giving the patients have higher level of satisfaction. The combination of the public and the private sector could ensure equity, efficiency, and quality of healthcare. There are three models discussed in this chapter on the roles of the private sector to optimize UHC through supplemental health insurance, providing healthcare for the NHI members, or purchasing healthcare for employees when regulation allows. Private not-for-profit organizations and private for-profit entities could complement NHI or NHS to minimize catastrophic health spending of the people in a country. Countries could explore the roles of the private sector to ensure equitable access to quality healthcare, provide options, facilitate greater satisfaction for higher-income groups, expand private healthcare providers, and ensure that high-quality care is provided. Finally, the private sector is expected to participate in promoting UHC and reducing catastrophic health spending, and facilitate long-term investment in a country’s health system.
Conflict of interest
The authors declare that there is no conflict of interest in writing and publishing this chapter. None of the authors work or has a share in private health insurers or private healthcare providers.
References
- 1.
Campo-Arias A, Ceballos-Ospino GA, Herazo E. Barriers to access to mental health services among Colombia outpatients. International Journal of Social Psychiatry [Internet]. 2020; 66 (6):600-606. Available from:https://europepmc.org/article/MED/32466709 - 2.
Garnelo L, Parente RCP, Puchiarelli MLR, Correia PC, Torres MV, Herkrath FJ. Barriers to access and organization of primary health care services for rural riverside populations in the Amazon. International Journal for Equity in Health [Internet]. 2020; 19 (1):1-14. Available from:https://equityhealthj.biomedcentral.com/articles/10.1186/s12939-020-01171-x - 3.
World Health Organization. Assessment of Barriers to Accessing Health Services for Disadvantaged Adolescents in Nigeria [Internet]. Brazzaville: WHO; 2019. p. 80. Available from: file:///C:/Users/DELL/AppData/Local/Temp/9789290234319-eng.pdf - 4.
DeSa S, Gebremeskel AT, Omonaiye O, Yaya S. Barriers and facilitators to access mental health services among refugee women in high-income countries: A systematic review. Systematic Reviews [Internet]. 2022; 11 (1):186. Available from:https://pubmed.ncbi.nlm.nih.gov/35387680/ - 5.
Walker C, Peterson CL. Universal health coverage and primary health care: Their place in people’s health. Journal of Evaluation in Clinical Practice [Internet]. 2021; 27 (5):1027-1032. Available from:https://onlinelibrary.wiley.com/doi/full/10.1111/jep.13445 - 6.
Kumbeni MT, Apanga PA, Chanase MAW, Alem JN, Mireku-Gyimah N. The role of the public and private health sectors on factors associated with early essential newborn care practices among institutional deliveries in Ghana. BMC Health Services Research [Internet]. 2021;21(1):621. Available from: /pmc/articles/PMC8244223/ - 7.
World Health Organization. Universal Health Coverage (UHC) [Internet]. Geneva: World Health Report. 2010. Available from: https://www.who.int/news-room/fact-sheets/detail/universal-health-coverage- (uhc) - 8.
Thabarny and Sayekti. The advantage of a single payer health insurance. In: Travers, editor. Health Insurance. London, UK, London: Intech Open; 2022 - 9.
GPW-13 Team. Draft Thirteenth General Programme of Work, 2019-2023: Promote Health Keep the World Safe Serve the Vulnerable [Internet]. WHO Press; 2018. p. 50 Available from: https://www.who.int/publications/i/item/thirteenth-general-programme-of-work-2019-2023 - 10.
Sarkodie AO. Effect of the National Health Insurance Scheme on healthcare utilization and out-of-pocket payment: Evidence from GLSS 7. Humanities and Social Sciences Communications [Internet]. 2021; 8 (1):1-10. Available from:https://www.nature.com/articles/s41599-021-00984-7 - 11.
Nugraheni WP, Mubasyiroh R, Hartono RK. The influence of Jaminan Kesehatan Nasional (JKN) on the cost of delivery services in Indonesia. PLoS One [Internet]. 2020; 15 (7):e0235176. Available from:https://pubmed.ncbi.nlm.nih.gov/32614846/ - 12.
Rahman R. The privatization of health care system in Saudi Arabia. Health Services Insights [Internet]. 2020; 13 :3-6. Available from:https://journals.sagepub.com/doi/10.1177/1178632920934497 - 13.
Klinton J. The Private Health Sector: An Operational Definition [Internet]. Geneva: World Health Organization; 2020. pp. 1-5. Available from: https://www.who.int/docs/default-source/health-system-governance/private-health-sector-an-operational-definition.pdf - 14.
Hasan AR, Bachtiar A, Candi C. The potential of private health insurance ownership based on the 2018-2020 National Socioeconomic Survey Data. Kesmas. 2022; 17 (4):279-286 - 15.
Agbanyo R, Peprah JA. National health insurance and the choice of delivery facility among expectant mothers in Ghana. International Journal of Health Economics and Management [Internet]. 2021; 21 (1):27-49. Available from:https://link.springer.com/article/10.1007/s10754-020-09288-w - 16.
Abd Khalim MA, Sukeri S. Uptake and determinants of private health insurance enrollment in a country with heavily subsidised public healthcare: A cross-sectional survey in East Coast Malaysia. PLoS One [Internet]. 2023; 18 (1):e0278404 Available from:https://journals.plos.org/plosone/article?id=10.1371/journal.pone.0278404 - 17.
Yang JM, Bin LS, Kim YJ, Chon DY, Moon JY, Kim JH. Association between private health insurance and medical use by linking subjective health and chronic diseases. Medicine (Baltimore) [Internet]. 2022; 101 (32):E29865. Available from:https://pubmed.ncbi.nlm.nih.gov/35960073/ - 18.
Listya Dewi S, Setiyaningsih H, Kedokteran F, Dan Masyarakat Keperawatan K, Gadjah Mada U. Peran Sektor Swasta Dalam Respon Terhadap Covid-19: Studi Kasus Di Yogyakarta the role of private sector in response to covid-19: A study case of Di Yogyakarta. Jurnal Kebijakan Kesehatan Indonesia JKKI. 2020; 09 (04):218-224 - 19.
Engaging the private health service delivery sector through governance in mixed health systems: Strategy report of the WHO Advisory Group on the Governance of the Private Sector for Universal Health Coverage [Internet]. Available from: https://www.who.int/publications/i/item/9789240018327 [Accessed: August 31, 2023] - 20.
Theron GB. Sustainable development goals [Internet]. Obstetrics and Gynaecology Forum. 2016; 26 :1. Available from:https://www.who.int/data/gho/data/themes/sustainable-development-goals - 21.
Peran Swasta Wujudkan Pembangunan Berkelanjutan Perlu Diperkuat [Internet]. Available from: https://www.beritasatu.com/ekonomi/901523/peran-swasta-wujudkan-pembangunan-berkelanjutan-perlu-diperkuat [Accessed: August 31, 2023] - 22.
Nuhu S, Mpambije CJ, Ngussa K. Challenges in health service delivery under public-private partnership in Tanzania: Stakeholders’ views from Dar es Salaam region. BMC Health Services Research [Internet]. 2020; 20 (1):1-12 Available from:https://bmchealthservres.biomedcentral.com/articles/10.1186/s12913-020-05638-z - 23.
Ekaputrie AC, Fauzan A. Analysis of the character of the insured by policy holders of private insurance companies in Indonesia with the rough set method. Eksakta: Journal of Sciences and Data Analysis. 2023; 4 (2):8-14 - 24.
Pratama AB. The landscape of public service innovation in Indonesia: A comprehensive analysis of its characteristic and trend. Innovation & Management Review. 2020; 17 (1):25-40 - 25.
Whaley CM, Pera MF, Cantor J, Chang J, Velasco J, Hagg HK, et al. Changes in health services use among commercially insured US populations during the COVID-19 pandemic. JAMA Network Open [Internet]. 2020; 3 (11):e2024984 Available from:https://pubmed.ncbi.nlm.nih.gov/33151319/ - 26.
Scassa T. Pandemic innovation: The private sector and the development of contact-tracing and exposure notification apps. Business and Human Rights Journal [Internet]. 2021; 6 (2):352-359 Available from:https://www.cambridge.org/core/journals/business-and-human-rights-journal/article/pandemic-innovation-the-private-sector-and-the-development-of-contacttracing-and-exposure-notification-apps/78A78BE8922FD8512A93C6648B76C2CE - 27.
Srinivasan A, Garg A. Role of the private sector in supporting access to primary healthcare. The CSR Journal [Internet]. 10 Dec 2021. Available from: https://thecsrjournal.in/private-sector-primary-healthcare-meghalaya/ - 28.
Public-private partnerships can give more people better healthcare, World Economic Forum [Internet]. Available from: https://www.weforum.org/agenda/2021/12/how-public-private-partnerships-can-give-more-people-better-health/ [Accessed: August 31, 2023] - 29.
Wegewijs D. Engaging the private health service delivery sector through governance in mixed health systems: strategy report of the WHO Advisory Group on the Governance of the Private Sector for Universal Health Coverage 2020 [Internet]. 2020. Available from: https://www.who.int/publications/i/item/9789240018327 [Accessed: August 31, 2023] - 30.
Sinjela KM, Simangolwa WMW, Hehman L, Kamanga M, Mwambazi WK, Sundewall J. Exploring for-profit healthcare providers’ perceptions of inclusion in the Zambia National Health Insurance Scheme: A qualitative content analysis. PLoS One [Internet]. 2022; 17 (5):e0268940. Available from:https://journals.plos.org/plosone/article?id=10.1371/journal.pone.0268940 - 31.
Role of Private Sector in defence [Internet]. Available from: https://www.daily-sun.com/printversion/details/346764/Role-of-Private-Sector-in-Healthcare [Accessed: August 31, 2023] - 32.
Wu R, Li N, Ercia A. The effects of private health insurance on universal health coverage objectives in China: A systematic literature review. International Journal of Environmental Research and Public Health; Mar 2020; 17 (6):2049. Available from:https://www.mdpi.com/1660-4601/17/6/2049/htm - 33.
Role of the Private Sector in Health Care Research Paper—EssayEmpire [Internet]. Available from: https://research-paper.essayempire.com/examples/health/role-of-the-private-sector-in-health-care-research-paper/ [Accessed: August 31, 2023] - 34.
Fisher M, Freeman T, Mackean T, Friel S, Baum F. Universal health coverage for non-communicable diseases and health equity: Lessons from Australian primary healthcare. International Journal of Health Policy and Management [Internet]. 2022; 11 (5):690-700 Available from:https://www.ijhpm.com/article_3964.html - 35.
Espinosa MF, Andriukaitis VP, Kickbusch I, Nishtar S, Saiz E, Takemi K, et al. Realising the right to health for all people—UHC is the umbrella to deliver health for all. The Lancet Global Health [Internet]. 2023; 11 (8):e1160. Available from:http://www.thelancet.com/article/S2214109X23002024/fulltext