 Open access peer-reviewed chapter
Open access peer-reviewed chapter
Abstract
The psychodynamic therapy technique is used in addressing a variety of mental health concerns, including behaviors that are considered criminal. In this chapter, the implementation of psychodynamic short-term therapy (PSTT) for people who engage in criminal behavior will be examined. Psychodynamic short-term therapy (PSTT) can be conceptualized as a brief therapy that helps individuals to gain awareness of unconscious factors that play a role in shaping their behaviors. It is based on the idea that criminal behaviors are associated with the trauma and unresolved conflicts from the past experiences repressed into the unconscious. This therapy technique, which leads to the discovery of these unconscious factors, provides tools for individuals to better understand and change their behavior. In this chapter, the theoretical basis of psychodynamic therapy, including its key concepts such as the unconscious, transference, and defense mechanisms, will be explored. Then, specific approaches and strategies such as identification of maladaptive coping mechanisms and the impact of trauma on individual’s criminal behavior will be discussed with case examples from the literature. At the end, the empirical evidence supporting the effectiveness of psychodynamic short-term therapy for criminal behavior and its limitations will be examined. The findings of the literature and recommendations will be offered to expedite forthcoming research in this domain.
Keywords
- criminal behavior
- psychoanalysis
- psychodynamic short-term therapy
- psychodynamics
- psychotherapy
1. Introduction
Within the context of criminal behaviors and efforts toward preventative measures and rehabilitation, psychodynamic short-term therapy emerges as an effective method for addressing the underlying psychological elements that may lead to criminal behaviors. In the scope of this chapter, the theoretical framework and techniques behind psychodynamic therapies and how it is integrated into a short-term form will be explained in relation to criminal behaviors. Lastly, the effectiveness of short-term psychodynamic therapy in terms of a rehabilitation tool for criminal behaviors will be discussed.
2. Psychodynamic short-term therapy: understanding the theory and techniques
A very important perspective on human behavior to discuss is Freud’s argument that psychological disturbances are caused by unconscious conflicts rather than organic causes [1]. Calling his theory psychoanalysis, Freud stated that the inner conflicts caused by past experiences of early relationships in early childhood are suppressed to the unconscious. Therefore, it is possible for these suppressed notions to lead to anxiety and other psychological problems in adulthood [2]. From Freud to other theorists who studied psychoanalysis, a broad range of therapies were developed. Psychodynamic therapy is one of the therapy techniques that emerged from the psychoanalytic theory. In Webster’s Third New International Dictionary, the term psychodynamic is defined as the study of the driving factors that influence behavior and mental states, particularly those that are unconscious or related to emotions, and their development during early childhood and subsequent impact [3]. The goal of psychodynamic therapy is to assist the progress of emotional experience and increase one’s understanding of their own by using various techniques such as transference, countertransference, and defense mechanisms [4].
The psychodynamic approach, while making use of the basic propositions and concepts of psychoanalysis and different theories and schools, has become a holistic perspective [5]. Moreover, the term psychodynamic is used because it is inclusive enough to cover any theory addressing psychological forces that operate beneath conscious awareness and form the basis of the majority of human behavior [6]. Commonly, psychodynamic therapies are long term, and they necessitate a higher frequency of sessions. However, the theory and techniques of psychodynamic therapies could be applied to short-term therapy. Therefore, short-term psychodynamic therapies emerged in line with needs.
Short-term dynamic therapy is an intervention that utilizes the concepts and techniques of psychoanalytic theory to address specific disorders usually within a timeframe of 10–25 sessions [7]. It is used for having the patient gain insight into the underlying causes of their specific problems [8]. As mentioned, psychodynamic therapies are usually long term, so why should there be a need for the use of short-term psychodynamic therapies? Firstly, long-term therapies are costly and require a commitment for a long time. In that sense, short-term therapies are more accessible. As there is a higher demand for short-term therapies, research on the effectiveness of short-term psychodynamic therapy showed that there is an increase in the number of studies that are challenging the assumption of needing long-term therapies [9].
Before starting to explain the theory and techniques used in short-term psychodynamic therapy, how it can be used in a criminal setting will be discussed. Forensic psychotherapy mainly originates from psychoanalytical and psychodynamic foundations. The insightful comprehension offered by forensic psychotherapy with regard to the patient’s previous encounters and present psychological condition can contribute to decision making. In this context, the psychotherapists who work with forensic patients not only offer therapy but also employ psychodynamic reasoning to understand the intricacies and dynamics among staff teams and institutions when treating this particular group of patients [10]. Dynamic therapy aims to uncover unconscious thoughts, impulses, and defense mechanisms. Gaining insight into one’s own unconscious motivation behind their actions provides individuals the chance to understand the underlying reasons behind a specific focal problem. By gaining such insight, an inmate or a criminal would gain comprehension in terms of recognizing and handling their recurrent patterns of criminal behavior. This insight would help to resolve the internal conflicts they experience, leading to a more realistic perception of the outside world. This is an important point in distinguishing short-term psychodynamic therapies from other time-limited therapies. For example, while cognitive behavioral therapy (CBT) has proven its effects on modifying behavior and thinking, it does not aim to consider the root cause of behaviors. Therefore, short-term psychodynamic therapy can not only become an effective tool for one to understand the root reason behind their criminal behavior and let them be active agents in terms of dealing with certain impulses but also is cost and time efficient as it is limited with a certain number of sessions [11].
Gaining insight about oneself is not an easy task, especially in a short-term period; however, it is possible under some criteria and using some techniques. To be able to explain them, first, it is necessary to talk about the theoretical background of short-term psychodynamic therapy. In this context, the terms unconscious, Oedipal relationships, transference, and defense mechanisms will be discussed. Starting with the term unconscious will be important for grasping other concepts. The term unconscious has been used before; however, with Freud’s use the term gained an original meaning that puts it in the position of the most important concept in psychoanalytic theory. In his structural/topographical theory, Freud explains the unconscious as not being limited to what is outside of conscious awareness, but rather comprises thoughts and memories that have been deeply separated from consciousness through repression. Without undergoing distortion, these thoughts or memories cannot enter the conscious or preconscious [12]. If the premise is bringing unconscious material into consciousness for healing, how can this be made possible? Psychoanalyst and theorist Jacques Lacan, who is known for the “return to Freud” movement, states that “the unconscious is structured like language” [13]. This means that our understanding of the unconscious only becomes clear when it is articulated and expressed through words. In psychoanalysis, the free associations, dreams, and the way the patient tells these, such as hesitations, pausing, forgetting, repetition, ambiguity in the language (equivoques), and slips of the tongue make up the foundation [14].
The therapeutic relationship is formed between the therapist and the patient. In essence, the therapist relies on the therapeutic relationship as the primary catalyst for facilitating transformation. The patient’s learning and the factors that lead to therapeutic progress primarily occur within the dynamics of this relationship. A significant part of therapeutic change is likely achieved through identifying the childhood origins of present psychological conflicts, along with the unconscious fantasies and emotions connected to the enduring impact of these early experiences [15]. The term transference was used by Freud first in his work called The Interpretation of Dreams [16]. The term indicates the displacement of affect from one idea to another. In a therapeutic setting, however, transference refers to the, whether positive or negative, affects placed on the therapist as a figure that is unconsciously put in a position of a familiar person by the patient [17]. The familiar person/s that are meant here are usually the patient’s parents or parental figures. The unconscious feelings of love and hostility that an individual experience toward their parents is called the Oedipus complex. It involves the desire for one parent, leading to a sense of competition or rivalry with the other parent. In that sense, it can be said that what is transferred by the patient onto the therapist is the Oedipal relations. This phenomenon is conceptualized by Malan [18] with his triangular models (see Figure 1).
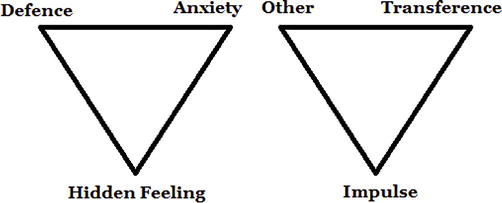
Figure 1.
The two triangles.
The first one is called the triangle of conflict. The corners consist of defense, anxiety, and hidden feelings. The first triangle is connected to the second one in the sense that the hidden feelings one has are directed toward specific categories of individuals. These categories are represented by the Other, Parent, and Transference. The corner the triangles stand on means that element is foundational for the other two. In the second triangle, the three categories of the person also signify three potential connections. They include the Other and Parent link, where emotions toward the Other are derived from emotions toward the Parent; the Other and Transference link, where similar emotions are directed toward the Other and the Therapist; and the Transference and Parent link, where Transference feelings originate from feelings associated with the Parents. The apex that the triangles stand on symbolizes the goal of dynamic psychotherapy to delve beneath defenses and anxiety to uncover hidden emotions. The process involves tracing these emotions back to their origins in the past, which is typically related to parents. These two triangles are crucial as they encompass nearly every intervention made by a therapist. A therapist’s skill lies in knowing which components of the triangles to incorporate into interpretations at any given moment.
In psychodynamic short-term therapy, the therapeutic focus is on the triangular interpersonal or Oedipal relationships as the underlying factor of psychological conflicts [19]. As alterations occur in the types of defenses and desires and that they are more suitably fulfilled, the patient is no longer going to be fixated on their drives at an early stage of development. The therapist helps the patient to have a conscious recognition of the aspects within these triangles that operate in the unconscious. By recognizing this process in their unconscious, the patient can prevent the confusion of past conflicts with the present relationships [20]. However, this recognition may not come easy due to the factor called defense. Being reluctant to talk about certain things and to freely associate indicates resistance as an integral part of treatment. Rather than an obstacle, resistance has an adaptive goal of conserving the patient from material that could be agonizing to be experienced in consciousness. Resistance is used by repressing distressing information, which involves blocking one’s own awareness of it.
While paying attention to the defenses of the patient, as the unconscious conflicts surface and the patient’s unconscious anxieties reduce, the therapist also undergoes emotional and impulsive fluctuations, known as the countertransference experience. The term countertransference was framed to indicate the unconscious feelings of the therapist for the patient. Lacan stated that countertransference is a handicap that hampers the treatment process and it is a resistance that belongs to the therapist. Many analysts stated that manifestations of countertransference occur when the analyst has not completed their own analysis.
In psychodynamic understanding, therapy can be applied to forensic patients with regard to the patient’s unconscious beliefs and impulses, previous encounters, and present psychological condition. The question arises, how does the theory see crime? Psychodynamic theories have a maladaptive childhood as the subject matter in relation to crime. From the point of view of Freud’s structural theory, it can be said that a frail superego, or conscience, is lacking in terms of keeping the powerful id under control. Therefore crime-related behavior arises accompanied by Oedipal conflicts that are unresolved as a product of insufficient psychosexual development. On the other hand, Kleinian theory explains criminal tendencies with guilt, stating that the origin of crime could be attributed to an abundance of guilt rather than a deficiency in having a conscience. This theory suggests that instead of a feeble conscience, disturbances in behavior may stem from a persecutory conscience [21]. Theoretically, many psychodynamic and psychoanalytic theorists bring crime explanations from somewhat different perspectives. However, they all emphasize the experiences from childhood. Each and every subject’s experience can only be unique to themselves. This uniqueness brings about different unconscious processes. Therefore, it can be said that subjectivity is at the very center of psychoanalysis and psychodynamic therapies.
3. Practical application: treatment plan
In the literature, the treatment plan is described in terms of three phases that are the beginning phase, middle phase, and ending phase [22]. Beginning phase includes evaluation, relationship building, goal, and parameter setting. The aim of the evaluation part is to determine appropriate or inappropriate candidates for short-term psychodynamic therapy with comprehensive assessment. For this purpose, the therapist receives the main complaint; evaluates mental status, intelligence, and psychological mindedness; and gathers information such as personal, social, and significant early life experiences with various techniques such as interviews, questionnaires, or projective tests. The intended parameters to be measured are the ability to identify or clearly define a main complaint for the focus of therapy, history of a meaningful relationship during childhood, the capacity to express feelings freely and relate flexibly with the therapist, intelligence, psychological sophistication, and motivation for change. Alongside these criteria, ego strength is another essential feature that a patient needs to benefit from short-term psychodynamic therapy (to tolerate and benefit from anxiety-provoking techniques such as interpretation and confrontation). Considering all the information provided, it can be said that due to its time-limited nature, this psychodynamic therapy approach generally operates with strict and careful selection criteria in order to be beneficial.
Within the context of PSTT, it often is believed that patients with unresolved Oedipal issues are the most appropriate candidates for short-term psychodynamic therapy. There is a general emphasis on the investigation of interpersonal interactions and transference in therapy, with a focus on unresolved Oedipal issues originating from the patient’s history. In other words, PSTT investigates the connection between the patient’s relationship with past parental figures and the conflict in the therapist-patient relationship. It is also shown that the selection of patients in PSTT can go beyond Oedipal problems like separation anxiety or loss experience. It can be said, however, that there is a common belief that neurotic patients should be chosen over those with severe psychiatric issues because they are unable to handle the insight they would encounter in therapy [23].
Trial interpretation or trial therapy is one of the methods used for testing a patient’s appropriateness for short-term psychodynamic therapy. The aim of the trial interpretation or therapy is to see if the patient was able to respond appropriately to the new insights presented by the therapist [24]. The focus of the therapy is determined and worked upon directly in connection with the patient’s openness to new insights. When a patient starts therapy with a particular complaint, the complaint is reformulated by the therapist considering early life experiences. In this process, the therapist creates a psychodynamic hypothesis by combining the patient’s complaint and history information. This hypothesis helps to explain the nature of the patient’s presented problem such as criminal behavior and lays the groundwork for the resolution process. The formulation is presented to the patient and the patient is expected to be open to interpretation and agreement on this matter. The patient’s responsiveness to interpretation and willingness for agreement are crucial factors in focalization of the therapy.
Setting treatment goals with a central focus is a required part considering the aim of achievement in a limited time. Determining clinical priorities is done to ensure the most efficient use of available time. In accordance with this trajectory, potentially achievable goals are set. Such goals may include gaining greater understanding of interpersonal conflicts, greater access to repressed emotions, emotional maturity, capacity for intimacy in relationships, reduction of anxiety and depression, and so on. Goals are set for an individual patient and address the issues that are of most immediate concern.
Setting boundaries and explaining them clearly to the patient are another required part in psychodynamic short-term therapy. It includes specification of time and place to conduct therapy. To exemplify, sessions can be done face-to-face once a week, at a specific time, for about 45 minutes. A clear explanation of goals and boundaries in this manner is important for establishing a solid therapeutic relationship and a ground for a successful therapeutic process. However, it should be added at this point that setting clear and firm boundaries may be of extra importance in order to achieve a successful therapeutic process with criminal patients who have problems with legal boundaries.
The middle phase is an essential stage in which the therapeutic process starts to concentrate on certain aspects such as work focus, curative factors, and goal achievement. In this phase, the therapist actively exposes the patient’s conscious ego to the repressed thoughts and emotions originating from the unconscious, which are the source of underlying conflicts, and helps the patient in readjustment. By investigating these repressed aspects, the therapist addresses the underlying psychological factors that can contribute to the criminal behavior to give an example. To facilitate this process in the short term, the therapist uses anxiety provoking questions, confrontations, and interpretations with the aim of increasing awareness and acceptance. However, it is crucial to note that these therapeutic interventions can be wounding since they create high anxiety. Although patients with criminal behavior may have ego strength against anxiety-provoking statements, it should be kept in mind that individuals who exhibit criminal behavior tend to resist acceptance, in other words, use the defense mechanism called denial.
Miller states that defense mechanisms have the function of keeping one’s consciousness away from unconscious conflicts. He adds that the threat of punishment in the face of unconscious thoughts and emotions may lead to the use of defense mechanisms to escape from unwanted thoughts and emotions. This phenomenon is specifically relevant for patients with criminal behavior given the legal aspect of their behavior and the possibility of punishment. Miller also proposed the idea that a therapist offers interpretations so that a patient can use insight to become aware of internal conflicts, thereby replacing awareness with defense mechanisms used [25]. Nevertheless, Molnos claimed that it is more favorable in the long term for patients to explore their unconscious processes rather than be readily given them by the therapist [26]. At this point, it can be suggested that resistance is one of the factors indicating the need for long-term psychodynamic therapy. However, it can also be said that in the short term, the therapist may play a crucial role creating an appropriate medium to surmount or handle with resistance. Taking the limitedness of the time into consideration, the therapist should confront the patient with their defensive strategies or resistant attitudes by recognizing them from the very first session. The therapist should confront the patient with a clear and understandable use of language to improve trust in the relationship. Moreover, the therapist should create a safe environment for communication without the fear of judgment and foster a therapeutic alliance that is characterized by a clear framework, rules, and goals to reduce resistance while increasing tolerance for interpretations.
One of the fundamental techniques employed in PSTT is the utilization of transference in therapeutic relationships. It is based on the idea of connecting the current therapeutic relationship between therapist and patient with past relationships. The advantage of establishing these connections is obvious since it brings old Oedipal issues and all associated emotions into the therapeutic relationship. At this phase of the therapy, the therapeutic atmosphere is established to allow the patient to experience those repressed issues and emotions through a transference relationship. The role of the therapist is to show the patient how these issues and emotions have shaped their current relationships in a repetitive manner. When the therapist facilitates the individual’s awareness of their here-and-now transferential reactions and facilitates their experience of connections with current and past relationships, insight follows producing powerful meaning. At this point, the therapist should reduce the patient’s internal psychological tension by providing a supportive environment. Through this attitude, the therapist can make the patient realize how these transference reactions may have been adaptive in the past, but are now expressed unconsciously, maladaptive in the present. In this way, the possibilities for the development of new learning and new behavioral patterns can be presented to the patient. In the final analysis, the resolution of core Oedipal issues depends on new learning and cognitive understanding, successful utilization of gained insights, and the experiential activation of emotions with the help of transference interpretations during therapy.
During this process, the therapist also experiences emotional and impulsive fluctuations, known as the countertransference reactions, as the unconscious conflicts surface and the patient’s unconscious anxieties decrease. The term countertransference basically refers to unconscious thoughts and emotions of the therapist for the patient. It can be stated that the therapist’s countertransference responses can be used as a powerful tool for therapeutic change when they arise in response to the patient’s transference. However, these reactions may not always occur as expected. The therapist’s own unconscious processes and conflicts may come to light in the patient’s presence and negatively impact the therapeutic process. Studies examining the experiences of therapists working with criminals have revealed that the therapist’s encounter with the patient’s criminal history, feelings, and behaviors related to crime can lead to deep emotional and cognitive conflicts in the therapeutic process. These studies reported a variety of countertransference responses that may hinder the therapeutic process [27, 28]. According to Lacanian psychoanalytic theory, on the other hand, there is no concept called countertransference. Instead, there is the transference of the therapist. This transference has the potential to influence the healthy functioning of the therapeutic process. Awareness of the therapist’s own internal processes and conflicts, making sense of these responses and managing them appropriately, can improve the quality of the therapeutic relationship. Therefore, therapists’ participation in the supervision process and personal analysis is a critical step for the healthy functioning of the therapeutic process. These platforms can help the therapist make sense of their own transference, explore their blind spots, and contribute to the therapeutic process with deeper understanding and awareness [29].
The last phase of PSTT is called the ending phase. At this phase, the evidence the therapist should be looking for is improved problem-solving skills, changes in attitudes, behavioral patterns, and overall changes in the patient. Once the therapist is convinced that these are taking place, he or she must understand that treatment must end soon.
At this point, some questions arise. What should be the evidence of change? What should the therapist look for to be convinced that it is really taking place? The first and most important thing is to demonstrate a change in the patient’s attitude toward the fundamental psychological problem and their attitude toward the Oedipal foundation that therapy focuses on. The therapist may use a variety of ways to test whether this is happening. One of these ways is for the therapist to carefully examine the transference relationship. Elements such as progressive independence, increased self-confidence, improved self-esteem, and reduced dependence on the therapist are indicators of important steps in the right direction. Another way the therapist can resort to is to ask the patient to explain his or her understanding of his or her psychodynamic roots of psychological problems. In PSTT, it is extremely important at the end of treatment that the therapist and patient have a clear understanding of the psychodynamics roots of the psychological problems. Moreover, the therapist should ask the patient to give instances of situations where their attitudes and behavioral patterns have changed and inquire about the differences in how they engage with significant people around them. Finally, information should be gathered about the development of new relationships and the emergence of new ways of dealing with old problems. The reduction or disappearance of past neurotic patterns should provide tangible evidence that fundamental changes have indeed occurred, and that some insight has been gained.
4. Fictional case example
Due to his persistent issues with criminal activity, John, a 35-year-old man, seeks out psychodynamic short-term therapy. His judicial troubles in the past have included stealing and substance abuse. John wants to understand the underlying reasons for his behavior because he recognizes the damaging effects it has had on his life and personal relationships.
John and his therapist conduct a thorough evaluation of his psychological background and criminal activities throughout the evaluation phase. The therapist investigates John’s early life, family relationships, and any traumatic situations that might have affected his development. They explore the idea of the Oedipal complex, which contends that early life experiences have a major impact on a person’s conduct and personality. John reveals that he was raised in a low-income area with a history of high crime, little prospects, and exposure to drug usage. Due to his father’s frequent absences and involvement in illegal enterprises, their relationship was strained. During this process, the therapist discovers unresolved issues related to the Oedipal conflict, where John has experienced feelings of rivalry and jealousy toward his father’s criminal lifestyle.
As the therapeutic relationship is formed, the therapist provides John with a secure and accepting environment in which to examine his feelings and thoughts, including his encounters with the Oedipal dynamic. John displays a range of contradictory feelings, such as resentment, a yearning for parental guidance, and a desire to forge his own identity. The therapist fosters trust and fosters an atmosphere that is conducive to self-reflection by actively listening and exhibiting empathy.
Setting therapy objectives while taking into consideration the Oedipal theme is a joint effort between John and his therapist. They list a number of particular objectives, such as comprehending how the Oedipal conflict affects John’s criminal behavior, resolving unresolved feelings related to his father-son relationship, creating healthier coping mechanisms, and strengthening decision-making abilities. John says he wants to develop a secure profession, mend his relationships, and release himself from the Oedipal dilemma.
John and the therapist also talk about how long therapy will last, with the therapist highlighting how short-term psychodynamic therapy is time limited. With the understanding that the emphasis will be on accomplishing specific goals connected to the Oedipal theme within this timeframe, they agree on the specification of the time and location to conduct treatment. This conversation makes sure that John and the therapist are on the same page on the goals and framework of the therapy, with a focus on addressing the Oedipal issues.
In the middle phase of the treatment, the emphasis shifts toward resolving the Oedipal conflicts and unconscious forces that underlie John’s criminal behavior. As John projects his unresolved thoughts and emotions related to his criminal tendencies onto the therapist, transference becomes a critical component of the therapeutic process. John starts to project his unresolved issues with his father and his criminal behavior onto the therapist as their therapy relationship develops. He views the therapist as an authoritative figure or perhaps a “criminal accomplice,” causing him to experience strong emotions and unresolved problems related to his illegal behavior. John’s emotions alternate between wanting approval for his actions and carrying around guilt or shame. The therapist is aware of this transference and accepts it, giving John a secure and compassionate environment in which to explore and express these difficult feelings. The therapist urges John to consider how his prior experiences might be influencing his present criminal behavior and decisions by assisting him in seeing that his feelings toward the therapist are a mirror of those events.
John has used defense mechanisms such as denial or rationalization to lessen the gravity of his conduct within the framework of the Oedipal conflicts and his criminal tendencies. But as therapy goes on, these protective mechanisms progressively give way to new and more beneficial coping strategies. John learns to accept responsibility for his criminal actions while also addressing the underlying psychological issues with the help of the therapist. A supportive and nonjudgmental environment is established by the therapist in order to address these defense mechanisms. The therapist offers John empathy and understanding as he explores and processes his feelings and thoughts in relation to his criminal actions. The therapist supports John’s personal development and a change to a law-abiding lifestyle by encouraging him to test out better alternatives to his old coping mechanisms.
To address the transference and direct John toward healthy coping strategies tailored to his criminal behavior, the therapist employs a variety of techniques. The therapist assists John in making the connection between his present encounters with the therapist and his unresolved conflicts over his criminal behavior through interpretation and confrontation. The therapist draws comparisons between John’s unconscious wishes for authority or recognition in relation to the Oedipal conflicts and his craving for power or control inside his criminal activity.
The therapist keeps track of and controls their own countertransference reactions throughout this stage. The therapist maintains a professional demeanor while acknowledging any emotional reactions brought on by John’s views on his illegal activities. The therapist makes sure that their own unresolved issues or emotional reactions associated with crime do not interfere with the therapeutic process by using supervision and personal therapy to address any potential biases or blind spots that may occur.
John’s therapist helps him gain a deeper awareness of the psychological elements influencing his conduct by addressing the transference and working through the defense mechanisms connected to his criminal behavior. Together, they elucidate the hidden motives, unsolved issues, and unfulfilled needs that underpin his criminal propensities. John learns new techniques for managing his emotions, making wise judgments, and encouraging positive behavioral changes
In the ending phase of the treatment, the therapist wants to evaluate the progress made. They pay close attention to how John’s projections onto the therapist have greatly lessened. John no longer views the therapist as an authority figure or an accomplice, but rather as a reliable mentor on his road to recovery. John demonstrates a profound awareness of the psychological causes that motivated his illegal activity during their genuine conversations. He discusses how his behaviors are related to his unmet emotional demands after learning how his prior experiences shaped his decisions. This new perspective illuminates the path to recovery and personal development.
At this process, the therapist observes that John has adapted new coping mechanisms. John shares stories of how he now controls his rage and impulsivity using mindfulness practices, which helps him respond instead of reacting negatively. He has the capability to deal with challenging circumstances thanks to the learned tools. With a transformed mindset and improved coping mechanisms, John begins to mend his connections. In an effort to put things right and forge stronger bonds, he contacts his family and friends. He has meaningful interactions with his loved ones thanks to his increased communication abilities and his newly discovered capacity for understanding others. He expresses guilt for his prior deeds and demonstrates empathy for their perspectives.
The therapist witnesses John’s remarkable changes as therapy comes to an end. His attitudes, actions, and coping techniques have undergone a profound transformation. Although John’s path to recovery has not been simple, he has become stronger and more resilient and is now prepared to embrace a law-abiding and fulfilling life.
5. Effectiveness of PSTT on criminal behavior
There are plenty of studies in the literature that compares the effectiveness of both psychodynamic therapy and short-term psychodynamic therapy specifically with other therapy schools. A meta-analysis article that integrated 17 studies reported that short-term psychodynamic therapies generated large effect sizes for different variables such as target problems and social functioning [30]. According to a study of university counseling services including both psychodynamic and CBT approaches, significant improvements were seen after both therapy and at the 6-month follow-up, compared to before treatment [31]. Short-term psychodynamic therapy is found to be more effective than psychoanalysis in the initial year in terms of improvement in work ability and functional capacity for anxiety and depression patients, whereas in 5-year follow-up psychoanalysis showed better improvement [32]. Long-term psychodynamic therapy is also found to be more effective in terms of elimination of psychiatric symptoms and working ability compared to PSTT and solution-focused therapy, which were classified as “short-term” therapy approaches with no significant difference among them [33]. There are also studies showing that there is no significant difference between cognitive therapy and PSTT in terms of defensive functioning of Cluster C personality disorder patients [34]. In light of such findings, long-term psychodynamic approaches seem to be more effective for long-term results. However, PSTT shows promising efficacy similarly with other short-term therapy methods, such as CBT.
The effectiveness of PSTT on different types of psychiatric conditions was proven within the literature as well. For personality disorders, it is shown that Intensive Short-Term Dynamic Psychotherapy-treated individuals achieved better results compared to the control group across all outcome measures. Furthermore, the improvements in both functionality and reduction of symptoms were maintained during the long-term follow-up period [35]. Psychodynamic short-term therapy (PSTT) has been discovered to be a successful therapy for individuals experiencing depression, regardless of whether they also have a concurrent borderline personality disorder [36]. For various types of psychiatric symptomatology, PSTT was found to be significantly effective to reduce symptoms [37]. Related to personality disorders, a review paper revealed that PSTT offers efficient improvement as compared to control groups [38]. Same paper suggests that Cluster C personality traits are the most proper for PSTT as compared to Clusters A and B, since they are seen as less vulnerable, which will be discussed later on.
Therapies conducted on crime in the literature generally appear to adopt the cognitive behavioral therapy approach. On the other hand, some studies reported use of psychodynamic approaches toward domestic violence perpetrators [39], sexual offenders [40, 41], violent individuals [42], and offenders who self-harm [43]. Although such studies report promising use of PSTT, there are a limited number of studies showing the use of PSTT on crime behavior. The possible reasons for that will be discussed in the following parts.
There are some case reports that summarize psychodynamic therapy processes with criminals. Such studies would be a good investigation method for effectiveness of PSTT, since psychoanalytic point of view notices the importance of subjectivity of each individual. As one of those case reports, Marriott described a detailed case of a teenager murder convict and his one-year long psychodynamic psychotherapy process [44]. In this report, the use of transference and countertransference concepts within the sessions and how these were worked in therapy were well described. Moreover, it is stated that through therapy, the subject began to establish more internal attributions for his acts and became more remorseful, which may reduce the risk of reoffending.
5.1 Why PSTT would be a good therapy alternative for criminal behavior?
There are numerous theoretical explanations stating that the roots of criminal behavior stem from unconscious conflicts. Moreover, although limited, a number of studies succeed to empirically present such connections. For instance, Brody and Rosenfeld’s study showed that there is a significant relationship between object relation dimensions and psychopathy [45]. Object relation theory proposes that interpersonal behavior is driven, in part, by internalized and unconscious mental representations of oneself and others. These representations are formed as a result of early experiences, specifically going back to mother-child unity, which takes roots from psychoanalytic theory. As findings supported as well, work with criminal behavior requires unconscious study. Although not detailed as psychoanalysis, PSTT would be considered as a shortcut alternative to interpret unconscious processes. As described in previous chapters, theories emphasizing the dynamic nature of criminal personality based on early childhood conflicts, PSTT would be the best way to refer to those issues in a limited time.
When working with criminal behavior, one aim is to help the client in taking accountability for their offense. By recognizing their role and ownership in the crime, the goal is to decrease the likelihood of future acts of violence [46]. As other psychoanalytically oriented therapies, PSTT also favors subjectivity of the client by pursuing the unconscious conflicts that are idiopathic to the client. Therefore, PSTT is a good method specifically for criminals, since it may help take and accept the responsibility of their acts.
6. Limitations
As reviewed in the previous section, there is a limited amount of research, which was able to investigate the effectiveness of PSTT for criminal behaviors empirically. The first reason for that would be that most studies about criminal behavior for therapy setting have samples from convict individuals. For offenders staying in an institute, hope for reduction in the sentence was a common characteristic for psychotherapy motivation [47]. Considering the strict election criteria for PSTT, such individuals might be considered to be not eligible for psychodynamic treatment. Moreover, due to the scarce resources in prison settings, group psychodynamic therapies seem to be preferred over individual psychotherapy, as a more cost-efficient alternative. Overall, this scarcity of data makes it challenging to measure its efficacy. The overall discussion on efficacy of PSTT focuses on psychodynamic theory in general, rather than focusing on PSTT specifically due to the lack of empirical effectiveness studies in the literature. Although using similar concepts and methods, PSTT needs to be assessed in terms of its efficacy on criminal behavior.
The duration for “short-term” psychodynamic therapy is not consistent within the literature. In the review paper investigating the effectiveness of PSTT, a maximum of 40 sessions and a minimum of seven sessions were included [48]. Moreover, some PSTT procedures include no time limit at all. Since there is a discrepancy between durations among studies, it becomes harder to define “short-term” or “brief” psychodynamic therapy within the literature in the beginning. Moreover, since criminal behavior is characterized with resistance and denial, obtaining successful results through short-term therapy approaches can be challenging.
One final limitation regarding the issue is the relation of criminal behavior with specific personality traits. Considering personality disorders, criminal and violent behaviors are more prominent among Clusters A and B personality types as plenty of studies in literature suggested [49, 50]. As noted previously, however, Cluster C personality traits are the most proper characteristics to benefit from PSTT. Considering such differences among subtypes of personality disorders, it becomes harder to reach a general conclusion about the effectiveness.
7. Conclusion
In this chapter, theoretical background, treatment plan, and effectiveness of PSTT on criminal behavior were discussed. Despite the theoretical underpinning of crime and psychoanalytical theory, there are a limited number of studies examining the usage of psychodynamically oriented treatment plans on criminals. More case studies are needed to illustrate the relationship among unconscious conflicts with such behavior. Further studies would also focus to demonstrate the practical outcomes such as symptom or criminal attempt reduction of PSTT.
References
- 1.
Balkaya D. Özerk dil dizgesinden lacan’ın simgesel düzenine. Konya: Çizgi Kitabevi; 2013 - 2.
Kesken J. Örgütsel İşlev Bozukluklarına Psikodinamik Yaklaşım Ve Niteliksel Bir Araştırma Yöntemi Olarak Psikanaliz. Yaşar Üniversitesi E-Dergisi. 2011; 6 (21):3499-3514. DOI: 10.19168/jyu.45839 - 3.
Gove PB, editor. Webster’s Third New International Dictionary. Springfield, MA: Merriam-Webster; 2002. p. 2816 - 4.
Summers RF, Barber JP. Psychodynamic Therapy: A Guide to Evidence-Based Practice. New York: Guildford Press; 2010. p. 355 - 5.
Yıldırım O, Kumcağız H. Psikodinamik Yaklaşıma Göre İnsan Davranışının İncelenmesi. Adıyaman Üniversitesi Sosyal Bilimler Enstitüsü Dergisi. 2022; 40 :103-132. DOI: 20.500.12414/3194 - 6.
Berzoff J, Flanagan LM, Hertz P. Why psychodynamic theories? Why a biopsychosocial context? In: Inside Out and Outside In: Psychodynamic Clinical Theory and Psychopathology in Contemporary Multicultural Contexts. 4th ed. Maryland: Rowman & Littlefield; 2016. pp. 1-13 - 7.
Messer SB. What makes brief psychodynamic therapy time efficient. Clinical Psychology: Science and Practice. 2001; 8 (1):5-22. DOI: 10.1093/clipsy.8.1.5 - 8.
Lanza ML, Anderson J, Boisvert CM. Assaultive behavior intervention in the veterans administration: Psychodynamic group psychotherapy compared to cognitive behavior therapy. Perspectives in Psychiatric Care. 2002; 38 (3):89-97. DOI: 10.1111/j.1744-6163.2002.tb00662.x - 9.
Huprich SK. Psychodynamic Therapy: Conceptual and Empirical Foundations. 1st ed. New York: Routledge; 2009. p. 273 - 10.
McGauley G, Humphrey M. Contribution of forensic psychotherapy to the care of forensic patients. Advances in Psychiatric Treatment. 2003; 9 (2):117-124. DOI: 10.1192/apt.9.2.117 - 11.
Mcleary J. Theoretical review of principle concepts in brief psychodynamic therapy applied in a model for treatment of adult incarcerated males [thesis]. Michigan: UMI Dissertation Publishing; 2009 - 12.
Evans D. An Introductory Dictionary of Lacanian Psychoanalysis. 1st ed. London: Routledge; 1996. p. 241. DOI: 10.4324/9780203135570 - 13.
Lacan J. The Seminar of Jacques Lacan: Book XX: Encore: 1972-1973. New York: W. W. Norton & Company; 2011. p. 242 - 14.
Gençöz T, Özbek-Şimşek D. Psikanalitik psikoterapiler. In: Eskin M, Dereboy ÇG, Karancı N, editors. Klinik Psikoloji: Bilim ve Uygulama. 1st ed. Ankara: Türk Psikologlar Derneği Yayınları; 2020. pp. 379-408 - 15.
Binder JL, Strupp HH. The Vanderbilt approach to time-limited dynamic psychotherapy. In: Crits-Christoph P, Barber JP, editors. Handbook of Short-Term Dynamic Psychotherapy. New York: Basic Books; 1991. pp. 137-165 - 16.
Freud S. The Interpretation of Dreams. Reprint ed. New York: Basic Books; 1900 - 17.
Cléro JP. Lacan Sözlüğü. 1st ed. İstanbul: Say Yay; 2011. p. 22 - 18.
Malan DH. Individual Psychotherapy and the Science of Psychodynamics. London: Butterworth; 1990. p. 74. DOI: 10.1201/b13307 - 19.
Sifneos PE. Short-Term Dynamic Psychotherapy: Evaluation and Technique. 2nd ed. New York: Springer Science & Business Media; 2013. p. 324 - 20.
Fialkow NJ, Muslin HL. Working through: A cornerstone of psychotherapy. American Journal of Psychotherapy. 1987; 41 (3):443-452. DOI: 10.1176/appi.psychotherapy.1987.41.3.443 - 21.
Brown AP. From individual to social defenses in psychosocial criminology. Theoretical Criminology. 2003; 7 (4):421-437. DOI: 10.1177/13624806030074002 - 22.
Mann J. Time-Limited Psychotherapy. Cambridge: Harvard University Press; 1973. p. 218 - 23.
Peake TH, Meyers TL, Duenke ST. Options for brief psychotherapy: Cognitive and psychodynamic variations. Journal of Mental Health. 1997; 6 (3):217-236.DOI: 10.1080/09638239718761 - 24.
Davanloo H. Principles and Techniques of Short-Term Dynamic Psychotherapy. New York: Spectrum Press; 1979 - 25.
Miller SJ. Analytic gains and anxiety tolerance: Punishment fantasies and the analysis of superego resistance revisited. Psychoanalytic Psychology. 2003; 20 (1):4-17. DOI: 10.1037/0736-9735.20.1.4 - 26.
Molnos A. A Question of Time Essentials of Brief Dynamic Psychotherapy. 1st ed. London: Karnac Books; 1995. p. 152. DOI: 10.4324/9780429471476 - 27.
Cartwright AD, Stark MD, Mountain J. The countertransference experiences of pregnant counselors working with sex offenders. Journal of Addictions & Offender Counseling. 2018; 39 (1):31-45.DOI: 10.1002/jaoc.12039 - 28.
Bach MH, Demuth C. Therapists’ personal experiences in their work with clients who have sexually offended against children: A phenomenological study. Journal of Child Sexual Abuse. 2019; 28 (7):799-818. DOI: 10.1080/10538712.2019.1592273 - 29.
Necef I. Aktarımın ve bilinçdışının rosetta taşı: Anna O. vakası. In: Gençöz T, editor. Freud’dan Lacan’a Vaka İncelemeleri. 1st ed. Ankara: Nobel Publishing Group; 2021. pp. 1-33 - 30.
Leichsenring F, Rabung S, Leibing E. The efficacy of short-term psychodynamic psychotherapy in specific psychiatric disorders: A meta-analysis. Archives of General Psychiatry. 2004; 61 (12):1208-1216 - 31.
Monti F, Tonetti L, Ricci Bitti PE. Short-term effectiveness of psychotherapy treatments delivered at a university counselling service. British Journal of Guidance & Counselling. 2016; 44 (4):414-422. DOI: 10.1080/03069885.2015.1119233 - 32.
Knekt P, Lindfors O, Laaksonen MA, Renlund C, Haaramo P, Härkänen T, et al. Quasi-experimental study on the effectiveness of psychoanalysis, long-term and short-term psychotherapy on psychiatric symptoms, work ability and functional capacity during a 5-year follow-up. Journal of Affective Disorders. 2011; 132 (1-2):37-47. DOI: 10.1016/j.jad.2011.01.014 - 33.
Knekt P, Lindfors O, Sares-Jäske L, Virtala E, Härkänen T. Randomized trial on the effectiveness of long- and short-term psychotherapy on psychiatric symptoms and working ability during a 5-year follow-up. Nordic Journal of Psychiatry. 2013; 67 (1):59-68. DOI: 10.3109/08039488.2012.680910 - 34.
Johansen P-Ø, Krebs TS, Svartberg M, Stiles TC, Holen A. Change in defense mechanisms during short-term dynamic and cognitive therapy in patients with cluster C personality disorders. The Journal of Nervous and Mental Disease. 2011; 199 (9):712-715. DOI: 10.1097/NMD.0b013e318229d6a7 - 35.
Abbass A, Sheldon A, Gyra J, Kalpin A. Intensive short-term dynamic psychotherapy for DSM-IV personality disorders: A randomized controlled trial: A randomized controlled trial. The Journal of Nervous and Mental Disease. 2008; 196 (3):211-216. DOI: 10.1097/NMD.0b013e3181662ff0 - 36.
Hilsenroth MJ, Defife JA, Blake MM, Cromer TD. The effects of borderline pathology on short-term psychodynamic psychotherapy for depression. Psychotherapy Research: Journal of the Society for Psychotherapy Research. 2007; 17 (2):172-184. DOI: 10.1080/10503300600786748 - 37.
Tanzilli A, Majorana M, Fonzi L, Pallagrosi M, Picardi A, Coccanari de’ Fornari MA, … Lingiardi V. Relational variables in short-term psychodynamic psychotherapy: An effectiveness study. Research in Psychotherapy: Psychopathology, Process and Outcome. 2018; 21 (3):190-200. DOI: 10.4081/ripppo.2018.327 - 38.
Town JM, Abbass A, Hardy G. Short-term psychodynamic psychotherapy for personality disorders: A critical review of randomized controlled trials. Journal of Personality Disorders. 2011; 25 (6):723-740 - 39.
Hamilton L, Koehler JA, Lösel FA. Domestic violence perpetrator programs in Europe, part I: A survey of current practice: A survey of current practice. International Journal of Offender Therapy and Comparative Criminology. 2012; 57 (10):1189-1205. DOI: 10.1177/0306624X12469506 - 40.
Romero JJ, Williams LM. Recidivism among convicted sex offenders: A 10-year follow-up study. Federal Probation. 1985; 49 :58-64 - 41.
Weiss P. Assessment and treatment of sex offenders in the Czech Republic and Eastern Europe. Journal of Interpersonal Violence. 1999; 14 (4):411-421 - 42.
Yakeley J. Psychodynamic approaches to violence. BJPsych Advances. 2018; 24 (2):83-92. DOI: 10.1192/bja.2017.23 - 43.
Walker T, Shaw J, Turpin C, Reid C, Abel K. The WORSHIP II study: A pilot of psychodynamic interpersonal therapy with women offenders who self-harm. The Journal of Forensic Psychiatry & Psychology. 2017; 28 (2):158-171. DOI: 10.1080/14789949.2017.1301529 - 44.
Marriott S. Applying a psychodynamic treatment model to support an adolescent sentenced for murder to confront and manage feelings of shame and remorse. The Journal of Forensic Psychiatry & Psychology. 2007; 18 (2):248-260. DOI: 10.1080/14789940601116366 - 45.
Brody Y, Rosenfeld B. Object relations in criminal psychopaths. International Journal of Offender Therapy and Comparative Criminology. 2002; 46 (4):400-411 - 46.
Yakeley J, Adshead G. Locks, keys, and security of mind: Psychodynamic approaches to forensic psychiatry. The Journal of the American Academy of Psychiatry and the Law. 2013; 41 :38-45 - 47.
Drapeau M, Korner CA, Brunet L, Granger L. Treatment at La Macaza clinic: A qualitative study of the sexual offenders' perspective. Canadian Journal of Criminology and Criminal Justice. 2004; 46 (1):27-44. DOI: 10.3138/cjccj.46.1.27 - 48.
Lewis AJ, Dennerstein M, Gibbs PM. Short-term psychodynamic psychotherapy: Review of recent process and outcome studies. The Australian and New Zealand Journal of Psychiatry. 2008; 42 (6):445-455. DOI: 10.1080/00048670802050520 - 49.
Greeven PGJ, De Ruiter C. Personality disorders in a Dutch forensic psychiatric sample: Changes with treatment. Criminal Behavior and Mental Health. 2004; 14 :280-290 - 50.
de Barros DM, de Pádua SA. Association between personality disorder and violent behavior pattern. Forensic Science International. 2008; 179 (1):19-22. DOI: 10.1016/j.forsciint.2008.04.013