Open Access is an initiative that aims to make scientific research freely available to all. To date our community has made over 100 million downloads. It’s based on principles of collaboration, unobstructed discovery, and, most importantly, scientific progression. As PhD students, we found it difficult to access the research we needed, so we decided to create a new Open Access publisher that levels the playing field for scientists across the world. How? By making research easy to access, and puts the academic needs of the researchers before the business interests of publishers.
We are a community of more than 103,000 authors and editors from 3,291 institutions spanning 160 countries, including Nobel Prize winners and some of the world’s most-cited researchers. Publishing on IntechOpen allows authors to earn citations and find new collaborators, meaning more people see your work not only from your own field of study, but from other related fields too.
To purchase hard copies of this book, please contact the representative in India:
CBS Publishers & Distributors Pvt. Ltd.
www.cbspd.com
|
customercare@cbspd.com
Point-of-care ultrasound (PoCUS) has emerged as a valuable tool in regional anesthesia and airway management. The chapter begins with an overview of PoCUS and its relevance to anesthetic practice, highlighting its advantages and limitations, and emphasizing the potential benefits of PoCUS in improving the accuracy and safety of regional anesthesia procedures, leading to enhanced patient outcomes. Furthermore, the chapter explores the utility of PoCUS in airway management, including the assessment of the upper airway, identification of anatomical locations, and real-time visualization of needle placement during airway blocks. Additionally, the chapter addresses the practical aspects of incorporating PoCUS into the daily practice of anesthesiologists, including the necessary equipment, technique considerations, and training requirements. It emphasizes the importance of proper education and ongoing proficiency in PoCUS to optimize its clinical utility and ensure accurate interpretation of images, optimizing patient care. Overall, this book chapter provides a comprehensive overview of the integration of PoCUS with regional anesthesia techniques and airway management, serving as a valuable resource for anesthesiologists, trainees, and allied healthcare professionals interested in enhancing their knowledge and skills.
Alcorcón Foundation University Hospital, Madrid, Spain
*Address all correspondence to: eugeniodaniel.martinez@salud.madrid.org
1. Introduction
Up to 30% of adverse effects solely attributed to the anesthesia procedure are related to the airway pathway. The majority of these are due to the inability of orotracheal intubation (or errors in it) or difficulty in ventilation. The consequences are catastrophic, and although the more widespread use of capnography and pulse oximetry has reduced these adverse effects, patients can still experience irreversible brain damage or death in up to 85% of cases [1, 2, 3, 4].
Therefore, proper management of the airway constitutes one of the fundamental pillars of medical care in certain specialties (anesthesiology, intensive care, emergency medicine, or pulmonology). However, an inadequate approach still represents one of the leading causes of morbidity and mortality among patients, as well as demands in these specialty fields.
In order to approach an airway and to anticipate and manage both foreseeable and unexpected difficulties, different strategies need to be developed, starting with patient assessment, including medical history and specific physical examination.
When predictors suggest a difficult airway (DA) (either due to previous surgeries or highly indicative DA prediction tests), prioritizing oxygenation and ventilation while causing minimal damage to the airway pathway is crucial. In cases where DA is anticipated, the safest and standard technique is considered to be vigil intubation [5]. However, this approach to the airway pathway induces greater physical and psychological stress for the operator, which can lead to suboptimal execution of the technique, a higher number of complications, and even procedure failure. Moreover, certain patient characteristics such as obesity, prior cervical radiotherapy, presence of masses, and cervical scars or abscesses can hinder its proper execution.
With the patient awake, any airway device can be used, as long as proper preparation with local anesthesia and sedation is performed. Regional anesthesia (RA) of the airway pathway provides adequate anesthesia of all its structures, allowing intubation to be performed without sedation or with minimal doses, with very good tolerance and patient cooperation with spontaneous ventilation and preserved reflexes. Similarly, it can be useful in patients where we want to reduce the autonomic response to endotracheal intubation and minimize the doses of drugs used in anesthesia induction [6].
For awake intubation, there is no single method to approach the procedure. Different strategies of premedication, sedation, and topicalization can be employed to maintain a level of patient consciousness that ensures proper airway and spontaneous ventilation, with adequate anxiolysis to tolerate the procedure [7].
All physicians responsible for managing an advanced airway device (DA) should be trained in performing awake intubation. Whether through nasal or oral route, tracheostomy, or cricothyrotomy, awake intubation allows for maintaining airway patency, gas exchange, and protection against aspiration of gastric contents or blood.
The most common technique is performing awake intubation using a fiberoptic bronchoscope (FOB) or videoendoscope, but it can also be done with other devices such as videolaryngoscopes (VDL), optical stylets, lighted stylets, or supraglottic devices, which are used to pass the FOB through them [8, 9, 10, 11, 12, 13, 14].
The preferred technique for intubation in these cases remains the use of FOB, although there are increasing studies suggesting videolaryngoscopy as an alternative, with the patient awake or, if not feasible, in spontaneous ventilation (in case the patient refuses the awake procedure) [15]. Supporting the procedure with an inhalation induction technique and topical anesthesia of the airway can enhance its effectiveness [16].
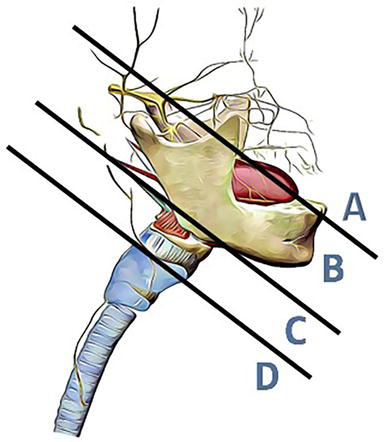
The upper airway is divided into four zones encompassing a total of five nerves, which provide sensory innervation to the airway (Figures 1 and 2, Table 1):
Nasal zone, innervated by the trigeminal nerve (anterior ethmoidal and maxillary/sphenopalatine branches).
Oral zone, innervated by the glossopharyngeal nerve.
Laryngeal zone, innervated by the vagus nerve through its superior laryngeal and recurrent branches.
Tracheal zone, innervated by the vagus nerve through the recurrent laryngeal branches.
Figure 1.
The upper airway sensory innervation division, by Fernandez-Vaquero [17].
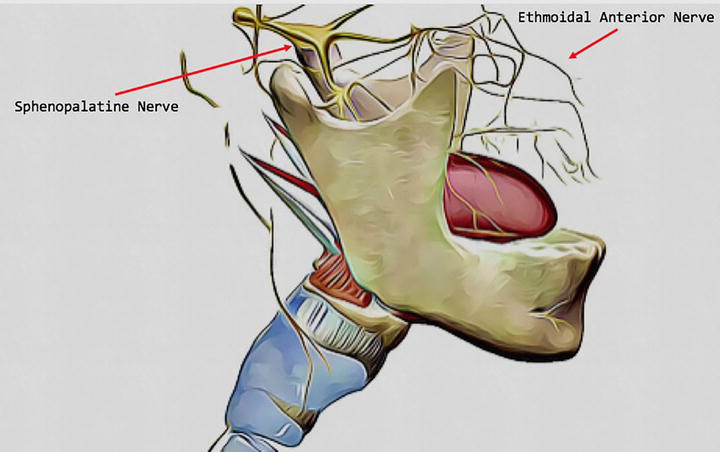
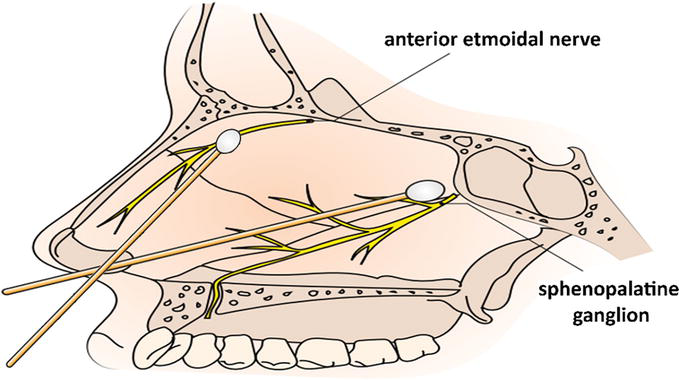
Figure 2.
Nasal innervation, by Fernandez-Vaquero [17].
Zone
Nerve
Branches and areas
Nasopharynx
Branches of the Trigeminal nerve (V cranial nerve)
Ophthalmic branch: anterior ethmoidal nerve.
Nasal cavity: anterior 1/3 of nostrils.
Maxillary branch: nasal cavity: nasal turbinates and posterior 2/3 of nasal septum.
Oropharynx
Glossopharyngeal nerve (IX cranial nerve)
Posterior 1/3 of tongue, anterior surface of epiglottis and vallecula (lingual branch), tonsils (tonsillar branch), pharyngeal walls, and tonsillar pillars (pharyngeal branch).
Nausea reflex.
Larynx
Vagus nerve (X cranial nerve)
Superior laryngeal nerve: base of tongue, posterior area of epiglottis, aryepiglottic folds, and arytenoids.
Recurrent laryngeal nerve: vocal cords and infraglottic region.
Trachea
Vagus nerve (X cranial nerve)
Recurrent laryngeal nerve: Abduction of vocal cords. Sensation in the infraglottic larynx and trachea.
Table 1.
Innervation of different regions of the airway. Nerve branches and areas.
3.1 Nasal innervation
It is primarily provided by two branches:
Anterior ethmoidal nerve. Located in the orbital cavity, is the sensory branch of the nasociliary nerve and, also, a branch of the ophthalmic nerve (one of the branches of the trigeminal [V PC]). It enters the nasal cavity through the anterior ethmoidal foramen. It innervates the anterior region and the nasal septum. It is not directly accessible for blocking (Figure 2).
Maxillary and sphenopalatine nerves. Located in the pterygopalatine fossa (posterior to the middle turbinate), these nerves form a triangular-shaped parasympathetic ganglion. It is composed of sensory branches from the maxillary nerve (a branch of the trigeminal nerve), sympathetic fibers from the carotid plexus (after reaching the ganglion through the vidian nerve, a branch of the greater petrosal nerve), and parasympathetic fibers from the communicating branches of the glossopharyngeal nerve. From it emerge the greater and lesser palatine nerves, which supply sensory innervation to the nasal cavity (nasal passages and posterior two-thirds of the nasal septum), the roof of the mouth, the soft palate, and the tonsils. Other important branches of the maxillary nerve that innervate the nasal cavity are the posterosuperior lateral and inferoposterior branches (Figure 2).
3.2 Innervation of the oropharyngeal zone is determined by the glossopharyngeal nerve
Glossopharyngeal nerve. A mixed nerve supplies sensory innervation to the posterior third of the tongue (gag reflex and the sense of taste), pharyngeal walls (pharyngeal branch), tonsils (tonsillar branch), and the anterior surface of the epiglottis (lingual branch) (Table 1).
3.3 Innervation of the laryngeal zone is determined by the vagus nerve through two of its branches
Superior laryngeal nerve (Table 1). It runs parallel to the superior thyroid vessels (branches of the external carotid artery), descends anterior to it to the greater horn of the hyoid bone, dividing into a mainly motor external branch (which innervates the cricothyroid and inferior pharyngeal constrictor muscle), and a sensitive internal branch (which innervates the base of the tongue, the epiglottis and the supraglottic mucosa of the larynx). The level of division into its terminal branches varies greatly. Its injury causes dysphonia.
The superior laryngeal nerve provides sensory innervation (internal branch) and motor innervation to the supraglottic portion of the larynx: cricothyroid muscle and the inferior constrictor of the pharynx. The level at which it divides into its internal and external terminal branches varies greatly.
Recurrent laryngeal nerve. It supplies sensory innervation to the infraglottic region and trachea and motor innervation by the external branch of the superior laryngeal nerve (except to the cricothyroid muscle, which is innervated by the external branch of the superior laryngeal nerve). It runs parallel to the inferior thyroid artery. Its injury causes inability to abduct the vocal cords (closed vocal cords) and secondary airway obstruction (Table 1).
3.4 Innervation of the tracheal zone is determined by the vagus nerve through its recurrent laryngeal branch
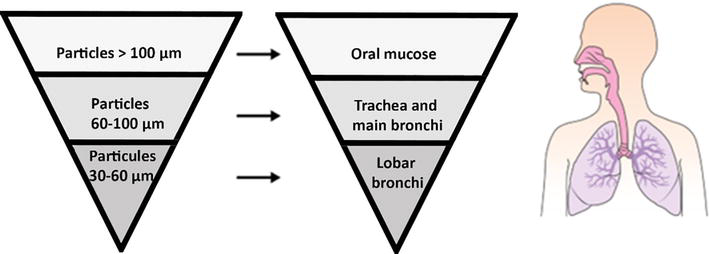
4.1.1 Nebulization (8–10 mL of 5% lidocaine with an oxygen flow of 8 L)
The respiratory tract can be anesthetized with lidocaine through a nebulizer. Particles larger than 100 μm will concentrate in the oral mucosa, those between 60 and 100 μm in the trachea and main bronchi, and those between 60 and 30 μm. in the larger bronchi. In the nebulizer, 8–10 mL of 5% lidocaine is placed, and oxygen is released with an 8 L/min flow.
This is an easy, safe, non-invasive, and comfortable technique for the patient. Coughing is minimal or absent. It requires 20 to 30 minutes to achieve adequate anesthesia. Absorption varies; therefore, high doses are sometimes used to compensate for this limitation (Figure 3).
Figure 3.
Airway nebulization, by Fernandez-Vaquero [17].
4.1.2 Direct application of lidocaine gel or spray
Currently, the atomizer spray (MADgic atomizer) is used, as it is the most effective, easiest to apply, and most commonly used. With gauze or swabs. This method is useful for applying lidocaine with vasoconstrictor in the nasal cavity. When performing nasal intubation, it is important to prepare the nasal mucosa with a vasoconstrictor to minimize the risk of bleeding. A rhinoscope and special otolaryngology forceps are used to introduce the swabs soaked with the anesthetic into the back of the nasal cavity (5% lidocaine with 0.5 mL. of oxymetazoline, 4% lidocaine with adrenaline 1,200,000 as the vasoconstrictor or 10 mg./ml. tetracaine with 0.1 mg./ml. epinephrine). The local anesthetic should be deposited in the space behind the inferior turbinate along the floor of the nose to the choana. This anesthetizes the nose and part of the oropharynx as the anesthetic falls by gravity toward these structures.
4.1.3 “Spray as you go” (SAYGo)
It consists of applying local anesthetic through the working channel of the Fiber-Optic Bronchoscope (FOB) to the mucosa of the airways as it is advanced.
If a small syringe is used for application, the local anesthetic may stay in the channel instead of reaching the mucous membrane of the respiratory tract. To prevent this, 2 mL. of 5% lidocaine is loaded into a 10 mL. syringe and the remaining space is filled with air. This creates a mixture of lidocaine and air. In this way, a greater force is created when the plunger is pressed, and the lidocaine falls to the distal part of the working channel almost like a jet.
The local anesthetic can also be instilled through an epidural catheter placed in the working channel. Normally, this maneuver should be performed by an assistant. It may cause coughing. If the anesthetic is introduced with less force, the risk of coughing is reduced. When the spray falls, the FOB’s vision will become blurry. It is necessary to administer O2 or ask the patient to take a deep breath to regain clear vision.
4.2 Regional nerve blocks providing sensation to the airways in their three regions
Blocks can be performed by locating anatomical structures or by using ultrasound, with the latter technique offering greater safety by avoiding accidental puncture of blood vessels or other structures adjacent to the airway, such as the thyroid gland. Additionally, it allows for the identification of structures even in patients with more complex anatomy (obese patients, previous surgeries, goiter, etc.) [19]. Ultrasound has become an essential tool in the daily practice of every physician, especially in anesthesiology, as it greatly enhances patient safety throughout the perioperative period, whether by performing nerve blocks, vascular access, intraoperative ultrasound for hemodynamic management, or any other use that improves the quality of care. It is a technique that offers many obvious advantages (safety, speed, repeatability, portability, wide availability, and real-time dynamic imaging). It has been demonstrated that even in expert hands, only three out of every 10 specialists are capable of locating the cricothyroid membrane based solely on anatomical references [6]. Tracheal structures can be identified by ultrasound, even when they are not palpable [20, 21].
Ultrasound of the airway has a steep learning curve and is operator-dependent, although basic structure identification can be acquired with just a few hours of training. For this purpose, a high-frequency linear probe (5–14 MHz.) is probably the most suitable since it deals with superficial structures (within 0–5 cm. below the skin surface) [22].
Regional blocks, ideally guided by ultrasound, are indicated in cases where topical anesthesia is contraindicated or not recommended, has been ineffective, or when the depth of the nerve prevents topical blockade. They involve the injection of a local anesthetic into the territory of a nerve to produce anesthesia in the area [19, 23, 24, 25].
Specific nerve blocks can be performed for the following nerves:
Palatine nerve (sphenopalatine ganglion)
Glossopharyngeal nerve
Superior laryngeal nerve
Inferior or recurrent laryngeal nerve
Regional/topical anesthesia of the airway provides adequate anesthesia of all its structures and allows for intubation (orotracheal or nasotracheal) without sedation or with minimal doses, with very good patient tolerance and cooperation, spontaneous ventilation, and preserved reflexes. In addition to patient tolerance, it can be useful to inhibit reflex responses provoked by intubation, such as coughing or laryngospasm [26, 27], as well as sympathetic nervous system-mediated cardiovascular responses [23, 28].
5. Applied anatomy for anesthetic management of the airway
Practically speaking, we will divide the innervation of the airway into the four previously mentioned zones: nasal, innervated by the trigeminal nerve; oral-pharyngeal, innervated by the glossopharyngeal nerve; laryngeal, innervated by the vagus nerve through its superior and recurrent laryngeal branches; and tracheal, innervated by the vagus nerve through its recurrent laryngeal branch.
5.1 Nasal zone
For this zone, topical anesthesia is commonly used due to its high efficacy and good patient tolerance, the high risk of vascular puncture in palatine nerve blocks, and the inaccessibility of the anterior ethmoidal nerve.
5.1.1 Topical anesthesia
By direct contact with swabs or pledgets (4 mL. of 5% lidocaine with 0.5 mL. of 0.5% oxymetazoline or 4% lidocaine with 1,200,000 adrenaline) on the posterior space behind the inferior turbinate (identified using a rhinoscope) (Figure 4).
Figure 4.
Direct contact block of the sphenopalatine and anterior ethmoid nerves, by Fernandez-Vaquero [17].
5.1.2 Sphenopalatine ganglion block
Blockade of the sphenopalatine ganglion, by blocking the greater and lesser palatine nerves, the nasociliary nerve, and the nasopalatine nerves, inhibits the sensitivity of the nasal cavity. Two approaches have been described: intraoral and nasal [19].
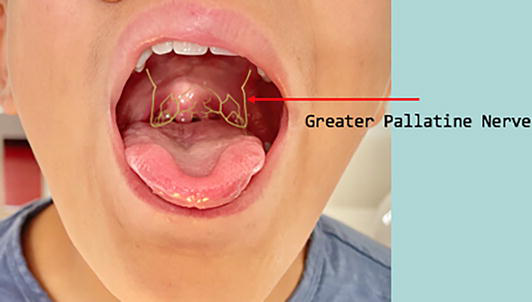
In order to visualize the blockage point of the greater palatine nerve and to perform the intraoral approach, the patient is placed in the supine position with a pillow under the shoulders, with the mouth open and the chin elevated (Figure 5). With the operator to the right of the patient, the right hand is placed at the 8 o’clock position and the left hand at 4 o’clock. The greater palatine foramen is identified with the aid of a swab, usually (in 50% of cases) 1 cm medial to the space between the second and third molars, or slightly anterior (39%) or posterior. At that level, pressure is applied with the swab on the palatogingival border until the depression caused by the foramen is felt.
Figure 5.
Intraoral major palatine nerve blockage, by Fernandez-Vaquero [17].
Once the foramen is located, a fine needle (25G or 27G spinal needle bent at approximately 120° about 2–3 cm. from the tip) is inserted 1–2 mm. anterior to the foramen, in a superior direction with a slight posterior inclination until bone contact is felt. Prior to aspiration in two planes (the original plane and rotating the needle 45°), 1–2 mL. of local anesthetic (2% lidocaine with 1,100,000 adrenaline) is injected at a very slow speed (approximately 1 minute) to avoid sympathetic stimulation. In 5–15% of cases, resistance may be encountered when inserting the needle into the canal, at which point the technique should be stopped and alternatives sought.
Complications include hemorrhage, infection, nerve injury, and intravascular injection of local anesthetic.
This technique is contraindicated in cases of acute inflammatory or infectious processes in the puncture area.
On the other hand, in the nasal approach to perform the nasopalatine nerve block, the anesthetic solution is applied with swabs on the upper edge of the middle turbinate (3 mL. of 4–5% lidocaine with 1 mL. of oxymetazoline). The swab shall be introduced at a 45° angle to the hard palate, directed posteriorly and inferiorly until it reaches the posterior wall of the nasopharynx. It can also be performed using a 20G catheter in the same location.
5.2 Oropharyngeal zone
The responsible nerve for the sensory innervation of the oropharynx is the glossopharyngeal nerve. Topical anesthesia is usually sufficient for upper airway instrumentation, although it must be accompanied by preventive measures for nausea and vomiting as it does not reach the receptors of the posterior third of the tongue. Glossopharyngeal nerve blockade, however, does inhibit the gag reflex as it is able to block the deep sensitivity of the posterior third of the tongue, so bilateral gag reflex blockade is used to abolish it.
5.2.1 Topical anesthesia
Topical anesthesia of the glossopharyngeal nerve is performed using swabs or cotton swabs. Swabs soaked in 5% lidocaine (mixed with 10 mL. of 5% lidocaine solution) are used. It is inserted into the channel between the teeth and the tongue until it reaches the palatoglossal arch. The swab is held in place for approximately 1 minute, repeating three or four times on each side. Always check that the topicalization is correct before inserting the device.
5.2.2 Glossopharyngeal block
Several approaches have been described using visualization and palpation of anatomical landmarks or ultrasound guidance (the latter being the preferred method). The most important risk to be taken into account is vascular puncture due to the proximity of the internal carotid artery and jugular vein, which will be avoided by aspirating before injecting the anesthetic [19]. Given the proximity to the carotid artery and jugular vein, injection of the anesthetic should be stopped in case of headache.
5.2.2.1 Glossopharyngeal block using anatomical landmarks
Intraoral or anterior approach (palatoglossal or anterior pillar). With the patient seated with the mouth open, the block is approached from the opposite side of the target nerve. Once appropriate topical anesthesia (lidocaine spray) has been administered, the tongue is pulled toward the midline using a laryngoscope blade or tongue depressor, while directing the 22-25G needle along the floor of the mouth down to the bottom of the pouch formed by the base of the palatoglossal arch. Once negative aspiration is confirmed, 2–5 mL. of 2% lidocaine is injected into the submucosa (Figure 6).
Posterior intraoral approach (palatopharyngeal or posterior tonsillar pillar). With the patient seated, the nerve is approached from the same side as the blockage by puncturing the palatopharyngeal cavity approximately 0.5 cm. lateral to the lateral edge of the tongue, where it joins the floor of the mouth, at the base of the posterior tonsillar pillar, blocking both the sensory and motor branches. A 22-23G needle is inserted up to 1 cm., and after aspiration, 3 mL. of 0.5–1% lidocaine (with a test dose of 0.5 mL.) are injected slowly, following verification through aspiration. Alternatively, an anesthetic-soaked pledget can be applied to the area to be blocked instead of puncture.
The injection is bilateral, blocking the sensory fibers (pharyngeal, lingual, and tonsillar) and the motor branch of the stylopharyngeus muscle, with a consequent increased risk of complications.
Peristyloid external approach. This approach is indicated when the patient cannot open their mouth wide enough to adequately expose the structures. The mastoid process and the angle of the mandible shall be located by placing the patient in the supine position with the head in a neutral position. The styloid process (next to the glossopharyngeal nerve, which runs adjacent to the internal carotid artery) is located by deep palpation or at the midpoint of the line drawn from the mastoid process to the mandibular angle. At this point, a 22G needle is inserted perpendicular to the skin until it comes into contact with the bone (1–2 cm), then angled to inject 5–7 mL of the anesthetic solution (2% lidocaine) after verification by aspiration. Peristyloid approach guided by ultrasound is recommended.
Figure 6.
Blockage of the glossopharyngeal nerve at the level of the palatoglossal archs, by Fernandez-Vaquero [17].
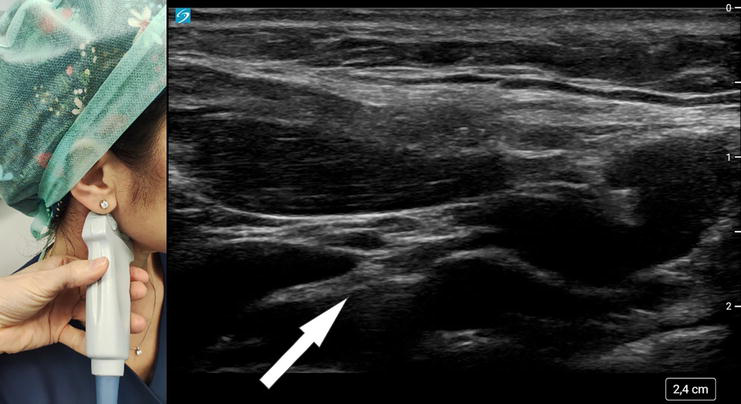
With the patient in the supine position and the head tilted to the contralateral side of the block, the cervical region shall be scanned with a high-frequency linear ultrasound transducer or a hockey stick probe to locate the mastoid process, mandibular angle, and styloid process at the midpoint, usually with the probe in an oblique transverse axis. At this point, the vessels (carotid artery and jugular vein) are identified using Doppler ultrasound, and the glossopharyngeal nerve is identified as a hyperechoic structure posterior and deeper to the styloid process and anterior to the carotid artery (Figure 7).
Figure 7.
Glossopharyngeal nerve block by ultrasound-guided peristylohyoid approach. The transducer is placed between the mandibular angle and the mastoid process and angled to locate the styloid process, carotid artery, and external jugular vein. The glossopharyngeal nerve is located posterior to the styloid process, by Fernandez-Vaquero [17].
The puncture is performed out of the plane until contacting the styloid process, and then the needle is redirected posteriorly to inject 3 mL of local anesthetic after aspiration to ensure that there is no blood or cerebrospinal fluid leakage.
Proper alignment of the transducer is crucial in Doppler effect usage: ideally, it should be positioned parallel to the blood flow (if not possible, at an angle of 0–60°). The Doppler effect can be enhanced by increasing the ultrasound frequency, increasing the flow velocity, or decreasing the transducer angle relative to the vessel or structure to be visualized.
Conventionally, blue represents the flow moving away from the transducer (longer wavelengths), and red represents the flow moving toward the transducer (shorter wavelengths).
5.3 Laryngeal region
5.3.1 Topical anesthesia
The larynx is innervated by branches of the vagus nerve (superior and recurrent laryngeal nerves). To anesthetize the supraglottic laryngeal region, topical anesthesia shall be applied in the piriform recess. This procedure requires proper oral opening, time, and prior preparation of the oropharynx, which is why it is infrequently used. If this is insufficient, the blockage of the superior laryngeal nerve can be performed, although it is less commonly used and has a higher number of complications (vascular injection, severe vagal reactions, etc.). The vocal cords are not completely paralyzed.
5.3.2 Superior laryngeal nerve block
Bilateral blockade of the superior laryngeal nerve results in anesthesia of the hypopharynx and upper glottis, including the vallecula and the posterior surface of the epiglottis. The main indication for this blockage is to facilitate the management of a difficult airway associated with local anesthetic nebulization in the oral/nasal and transtracheal cavities. Its blockage inhibits the gag reflex and coughing provides supraglottic anesthesia and minimizes the risk of laryngospasm by preventing the contraction of the cricothyroid muscle. It has been used in awake fiberoptic intubation and rigid bronchoscopy procedures (Table 2) [29, 30].
Topical anesthesia
Nerve block
Control of secretions
Atropine required
Not required
Anesthetic dose
10 mg./spray lidocaine 10%.
Lower dose (2 mL.)
Blocking duration
Lower
Longer
Need for repeat doses
More frequent
No
Table 2.
Comparison between topical anesthesia and upper laryngeal blockade.
Other indications include as an alternative to neuromuscular blockers in case of contraindication (myasthenia gravis, dystrophies, etc.) and the treatment of persistent headaches due to superior laryngeal nerve neuralgia [31]. Classically, it is located by palpation. With the patient in the supine position and the head extended and tilted laterally to the side opposite to the block, locate the greater horn of the hyoid bone or the thyroid cartilage (upper horn or midline prominence) [19].
A 25G needle is then inserted perpendicular to the plane of the skin to a depth of 1–2 cm until the bone is palpated, at which point it is redirected anteroinferiorly toward the midline to penetrate the thyrohyoid membrane at a depth of 2–3 mm. Using the superior horn of the thyroid cartilage as a reference, in this case, after inserting the needle and hitting the cartilage, it is angled anterosuperiorly to locate the thyrohyoid membrane, where a loss of resistance is felt (Figure 8).
Figure 8.
Superior laryngeal nerve block guided by anatomical references, by Fernandez-Vaquero [17].
Another possibility is to palpate the thyroid notch, puncturing at a suprathyroid level 2 cm. from the midline, and directing the needle cranially and posteriorly until the thyroid membrane is located at a depth of 1–2 cm.
Before injecting the anesthetic (2 mL. of 2% lidocaine with 1/200,000 adrenaline), negative aspiration should be checked (neither air, indicating excessive depth, nor blood should appear).
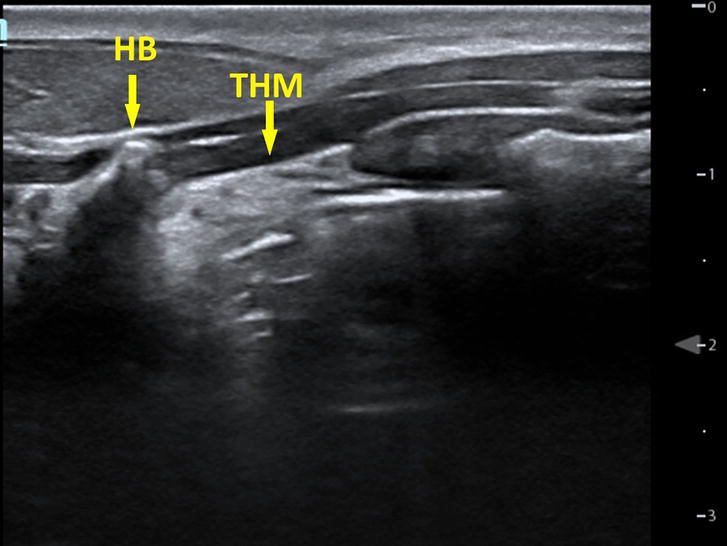
The use of ultrasound is recommended for the localization of the hyoid bone and the cricothyroid membrane (Figure 9), as the technique is safer with a lower risk of complications, such as vascular puncture, among others [32].
Figure 9.
HB: Hyoid bone; THM: Thyrohyoid membrane, by Fernandez-Vaquero [17].
Ideally, a hockey stick transducer is used, which provides higher resolution and smaller size, allowing for more maneuverability of the needle. However, a linear or convex probe is typically used. The in-plane approach is recommended to control the needle tip due to the limited space available and to avoid injury to adjacent structures.
Different approaches can be considered:
Barberet’s approach: a high-frequency linear transducer is placed in a parasagittal axis at the submandibular level. The hyoid bone, the upper edge of the thyroid cartilage, the muscles of the vocal cords (omohyoid, sternohyoid, and thyrohyoid), the artery, and the superior laryngeal nerve (between the muscles and the thyrohyoid membrane) are identified, as well as the internal laryngeal mucosa. The cartilage and bone are hyperechoic structures, among which the thyrohyoid membrane is located. At this level, local anesthetic is bilaterally injected. This technique has a success rate of 90% [33].
Manikandan’s approach: the submandibular region is explored to locate the external carotid artery and, following its branches, to visualize the superior laryngeal nerve [25].
Lida’s approach: the greater horn of the hyoid bone is identified without visualizing the superior laryngeal nerve [24].
Transverse axis approach with a probe, in case of technical impossibility or contraindication for the longitudinal approach or non-visualization of the nerve (<1 mm. diameter) [34].
An attempt should be made to avoid the potential risk of broncho-aspiration: it is necessary to observe the required fasting time, maintain an appropriate level of consciousness, and adopt an anti-Trendelenburg position upon awakening. The duration of supraglottic anesthesia will depend on the anesthetic used. The blockage of the superior laryngeal nerve should be complemented with topical anesthesia of the nasal and oral cavities, as well as transtracheal nebulization. The external branch of the superior laryngeal nerve can be injured during neck surgeries.
There are various degrees of injury, although clinically it is characterized by a slight deterioration in voice quality. Anesthesia of the superior laryngeal nerve can cause Wallerian degeneration with damage to the Schwann cell and axonal dystrophy, characterized by mild hoarseness. The use of a linear probe requires greater pressure on the neck, resulting in pain.
5.4 Tracheal zone
5.4.1 Blockage of the recurrent laryngeal nerve
The recurrent laryngeal nerve is a mixed nerve with intrinsically connected motor and sensory fibers. Blocking it would cause bilateral paralysis of the vocal cords and obstruction of the airway, so it is contraindicated.
However, it is necessary to block it to prevent coughing and allow the passage of the tracheal tube or fibroscope through the vocal cords. For this purpose, topical anesthesia of the mucosa is advised, using the “as you go” technique or through transtracheal or translaryngeal blockage.
5.4.2 Translaryngeal or transtracheal blockage
The patient is placed in a supine position with the neck extended (ideally with a pillow under the shoulders), which makes the laryngeal structures more prominent.
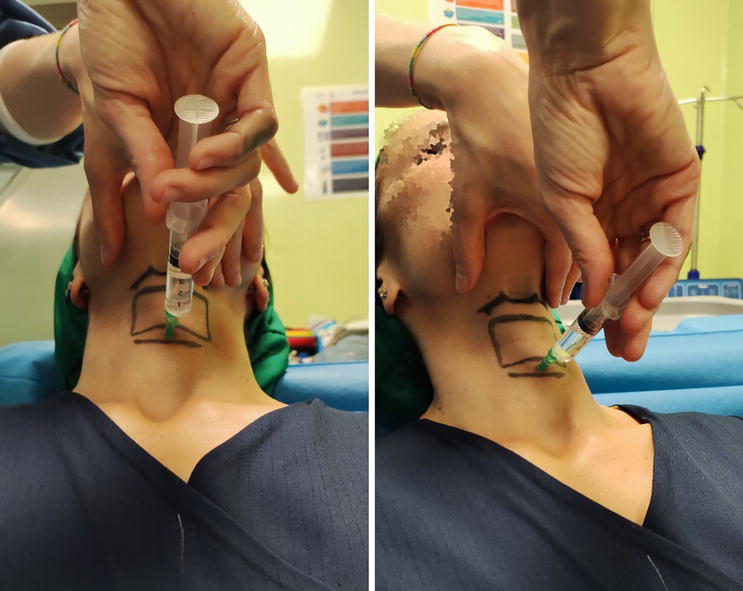
The classic approach is blindly performed by palpating the cricoid cartilage in the midline. The larynx is stabilized with the first and second fingers of one hand; after identifying the upper edge of the cartilage, a subcutaneous wheal is formed with the free hand, and a 20-22G needle is inserted perpendicularly to the skin until it traverses the cricothyroid membrane, which is confirmed by the continuous aspiration of air (bubbling). At that moment, the needle is secured to prevent puncturing the posterior wall, and 5 mL. of 4% lidocaine are rapidly injected. The injection of the anesthetic stimulates coughing, which nebulizes the anesthetic and blocks the recurrent laryngeal nerve (Figure 10). After the procedure, the needle is quickly withdrawn, and a catheter can be left in place if further doses are anticipated to prolong the blockade.
Figure 10.
Translaryngeal block through the cricothyroid membrane using anatomical landmarks, by Fernandez-Vaquero [17].
Ultrasound-guided approach facilitates the localization of the cricothyroid membrane between the thyroid and cricoid cartilages, as well as the control of needle tip placement into the laryngeal lumen, ensuring proper deposition of the anesthetic through translaryngeal blockade. Among the advantages of the ultrasound-guided approach are the more precise localization of blood vessels (avoiding the risk of bleeding and VA hematomas) and the possibility of confirming the correct placement of the tracheal tube [24, 32].
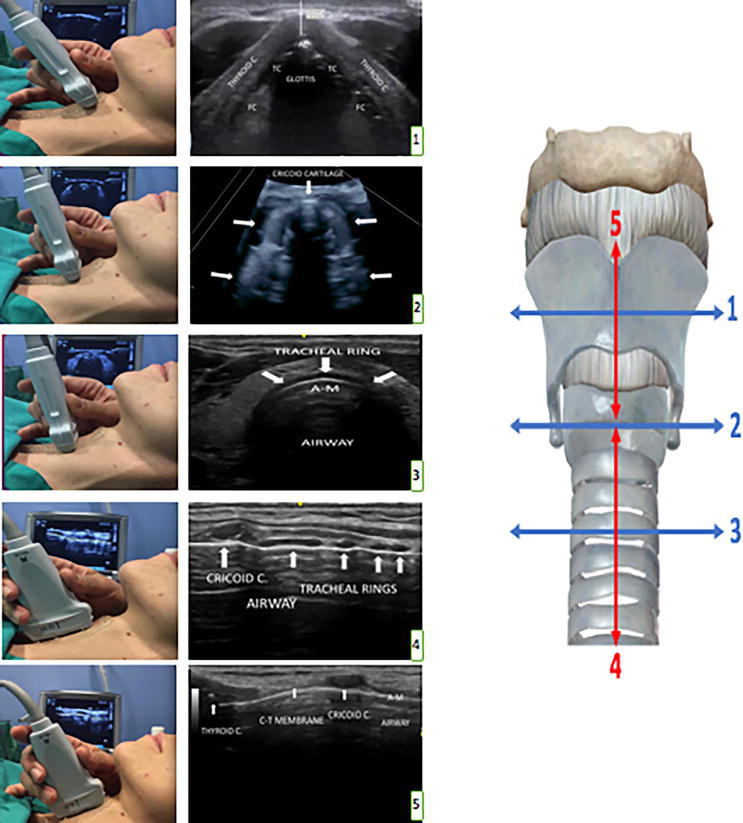
Caudocranial scanning of the neck allows differentiation of the tracheal cartilage, the cricoid cartilage, and the thyroid cartilage. The cricothyroid membrane is echogenic (white), although it may vary in appearance depending on the anatomy, and is located between the caudal edge of the thyroid cartilage (hypoechogenic or gray) and the cephalic boundary of the cricoid cartilage (hypoechogenic or gray) and the cricothyroid muscles. Ultrasound waves do not penetrate air, therefore the posterior wall of the larynx cannot be visualized.
Thyroid cartilage level: a triangular structure with a delta wing shape is observed. The vocal cords will appear inside with a triangular shape. (Requires angulation of the probe at 45–60° in a cephalic direction).
Cricoid cartilage level: for the second cut, slide the probe caudally until the next semicircular cartilaginous structure, which is the cricoid cartilage.
Tracheal rings level: for the third transverse cut, direct the probe caudally until it reaches the tracheal rings. At the level of the 6th or 7th tracheal ring, stop the probe and rotate it 90° on its own axis, thus achieving the change from transverse to longitudinal exploration.
Longitudinal Section:
Cricoid cartilage and tracheal rings: hypoechoic images in the form of “lentils” (tracheal rings) and a larger, rounder structure in a cephalic position resembling a “bean” (cricoid cartilage) are observed.
Thyroid-cricoid cartilage (cricothyroid membrane): in a cephalic direction, once the cricoid cartilage is identified, the tissue that appears just after it is the cricothyroid membrane, which inserts in a cephalic position on the thyroid cartilage (Figure 11).
Figure 11.
Ultrasound-guided approach for the localization of the cricothyroid membrane, by Fernandez-Vaquero [17].
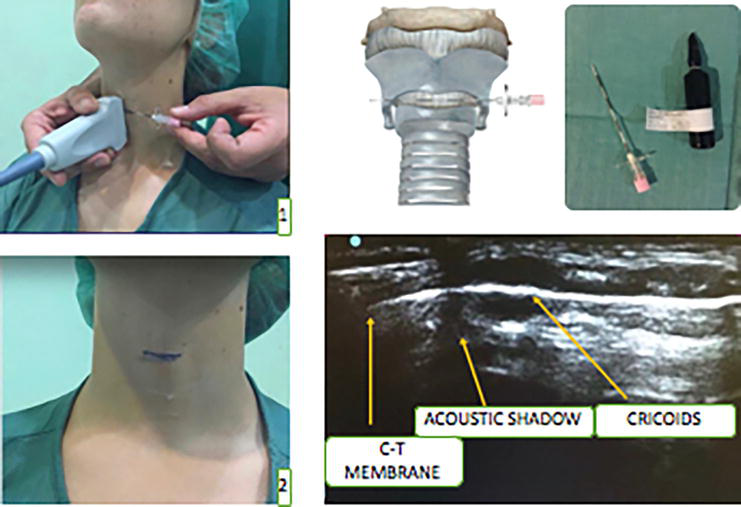
Cricothyroid Membrane Marking:
Preparation of marking kit and needle placement: a Tuohy needle or another guide needle can be used, along with a vial of methylene blue for coloring. Position the needle between the skin and probe, creating a hyperechoic image on the superficial part with subsequent acoustic shadowing. Then, move it to the upper edge of the cricoid cartilage.
Membrane marking: finally, upon needle removal, a mark will remain at the level of the lower border of the cricothyroid membrane. If measurements of the membrane have been taken, a millimeter ruler can be used to draw the entire thickness (Figure 12).
Figure 12.
Cricothyroid membrane marking, by Fernandez-Vaquero [17].
Maintaining the probe with the membrane in the center of the image, the exact location is marked with a pen or needle, or a subcutaneous wheal is created and the prelaryngeal space is measured to calculate the maximum needle insertion length, which is inserted in a caudal direction on a plane. Once air aspiration is confirmed, 4 mL of 2% lidocaine is injected. Ultrasound localization surpasses palpation and surface anatomical references (usual maneuver) in terms of time and effectiveness. Additionally, it allows for confirmation of the tracheal tube placement and identification of potential procedure-related complications.
Real-time visualization of laryngeal vessels is also facilitated. It is important not to lose sight of the superior and inferior laryngeal vessels or the needle tip. Since intralaryngeal air hinders visibility of the needle’s posterior part, it is recommended to measure the anteroposterior laryngeal diameter and clamp the needle to a length smaller than this diameter to prevent perforation of the vessels, mediastinitis, and/or laryngoesophageal fistula [35].
The following complications of translaryngeal block can occur: bleeding, infection, and tracheal perforation (secondary pneumomediastinum, subcutaneous emphysema, and esophageal perforation). This block should not be performed in patients at risk of aspiration, coagulation disorders, or cervical instability.
The main indication for regional anesthesia of the laryngeal vestibule (LV) is awake intubation in difficult airways. There is no single approach for the total LV block.
The most commonly used technique is topical anesthesia or direct application of local anesthetic (LA) to the LV. The least invasive technique should be chosen, with a preference for topical anesthesia over nerve blocks.
To select an appropriate regional anesthesia, it is crucial to individualize the technique based on the objectives, characteristics of the procedure, patient, and environment. Likewise, a comprehensive knowledge of the anatomy and physical principles of ultrasound equipment is essential.
The use of ultrasound is recommended to enhance the safety and efficiency of anesthesia, as well as to combine necessary blocks. Ultrasound minimizes complications, but in-depth anatomical knowledge of the blocking area is indispensable.
Regional techniques complement oxygenation, adequate sedation, and antiemetic measures, with proper patient information. Among the most commonly used techniques are anesthetic topicalization and blocks of the glossopharyngeal, superior laryngeal, and translaryngeal nerves.
Any instrumentation of the LV can cause trauma or adverse effects such as edema, hemorrhage, esophageal or tracheal perforation, pneumothorax, or bronchoaspiration.
Pediatric patients, polytraumatized patients, patients with full stomach or glottic/subglottic obstruction, and obstetric patients require special treatment.
1.Caplan RA, Posner KL, Ward RJ, Cheney FW. Adverse respiratory events in anesthesia: A closed claims analysis. Anesthesiology. 1990;72(5):828-833
2.Cheney FW, Posner KL, Lee LA, Caplan RA, Domino KB. Trends in anesthesia-related death and brain damage: A closed claims analysis. Anesthesiology. 2006;105(6):1081-1086
3.Li G, Warner M, Lang BH, Huang L, Sun LS. Epidemiology of anesthesia-related mortality in the United States, 1999-2005. Anesthesiology. 2009;110(4):759-765
4.Cook TM, Woodall N, Frerk C, Fourth National Audit Project. Major complications of airway management in the UK: Results of the fourth National Audit Project of the Royal College of Anaesthetists and the difficult airway society. Part 1: Anaesthesia. British Journal of Anaesthesia. 2011;106(5):617-631
5.Echevarría-Correas MA, González-Bada A, Rodrigo-Casanova MP, García-Peña JM, Aguilera-Celorrio L. Vía aérea difícil, detección preoperatoria y manejo en quirófano. Revista Mexicana de Anestesiología. 2015;38(2):85-90
6.Marisa Mariscal Flores, Eugenio Martínez Hurtado. Manual de manejo de la Vía Aérea Difícil [Internet]. Disponible en: https://shop.anestesiar.org/tienda/manual-vad-pdf/
7.Elliott DSJ, Baker PA, Scott MR, Birch CW, Thompson JMD. Accuracy of surface landmark identification for cannula cricothyroidotomy. Anaesthesia. 2010;65(9):889-894
8.Law JA, Duggan LV, Asselin M, Baker P, Crosby E, Downey A, et al. Canadian airway focus group updated consensus-based recommendations for management of the difficult airway: Part 2. Planning and implementing safe management of the patient with an anticipated difficult airway. Canadian Journal of Anaesthesia. 2021;68(9):1405-1436
9.Law JA, Duggan LV, Asselin M, Baker P, Crosby E, Downey A, et al. Canadian airway focus group updated consensus-based recommendations for management of the difficult airway: Part 1. Difficult airway management encountered in an unconscious patient. The Canadian Journal of Anesthesia. 2021;68(9):1373-1404
10.Hung O, Murphy M. Context-sensitive airway management. Anesthesia and Analgesia. 2010;110(4):982-983
11.Ahmad I, El-Boghdadly K, Bhagrath R, Hodzovic I, McNarry AF, Mir F, et al. Difficult airway society guidelines for awake tracheal intubation (ATI) in adults. Anaesthesia. 2019;75(5):688
12.Cabrini L, Baiardo Redaelli M, Ball L, Filippini M, Fominskiy E, Pintaudi M, et al. Awake Fiberoptic intubation protocols in the operating room for anticipated difficult airway: A systematic review and meta-analysis of randomized controlled trials. Anesthesia & Analgesia. 2019;128(5):971-980
13.Frerk C, Mitchell VS, McNarry AF, Mendonca C, Bhagrath R, Patel A, et al. Difficult airway society 2015 guidelines for management of unanticipated difficult intubation in adults. British Journal of Anaesthesia. 2015;115(6):827-848
14.Apfelbaum JL, Hagberg CA, Connis RT, Abdelmalak BB, Agarkar M, Dutton RP, et al. American Society of Anesthesiologists Practice Guidelines for management of the difficult airway. Anesthesiology. 2022, 2022;136(1):31-81
15.Murphy M, Hung O, Launcelott G, Law JA, Morris I. Predicting the difficult laryngoscopic intubation: Are we on the right track? Canadian Journal of Anesthesia. 2005;52(3):231-235
16.Galán Gutiérrez JC, Mora PC, Pestana AS. Inducción inhalatoria y anestesia tópica de la vía aérea guiada por videolaringoscopio C-MAC pala d-Blade en un paciente con miastenia gravis y vía aérea difícil. Revista Colombiana de Anestesiología [Internet]. 2023;41:287-290. Disponible en: https://www.elsevier.es/es-revista-revista-colombiana-anestesiologia-341-articulo-induccion-inhalatoria-anestesia-topica-via-S0120334713000397?referer=coleccion
17.Fernandez-Vaquero MA, Charco-Mora P, Garcia-Aroca MA, Greif R. Preoperative airway ultrasound assessment in the sniffing position: a prospective observational study. Brazilian Journal of Anesthesiology (English Edition). Jul 2022
18.Wieczorek PM, Backman SB. Airway topical anesthesia. Anesthesia and Analgesia. 2009;109(3):991; author reply 991-992
20.Novitch M, Prabhakar A, Siddaiah H, Sudbury AJ, Kaye RJ, Wilson KE, et al. Point of care ultrasound for the clinical anesthesiologist. Best Practice & Research. Clinical Anaesthesiology. 2019;33(4):433-446
21.Umobong EU, Mayo PH. Critical care airway management. Critical Care Clinics. 2018;34(3):313-324
22.Fernández-Vaquero MÁ, Carrillo-Esper R. Ecografía de vía aérea: en busca de la membrana cricotiroidea. Revista Mexicana de Anestesiología. 2021;44(2):116-122
23.Krause M, Khatibi B, Sztain JF, Rahman P, Shapiro AB, Sandhu NS. Ultrasound-guided airway blocks using a curvilinear probe. Journal of Clinical Anesthesia. 2016;33:408-412
24.Iida T, Suzuki A, Kunisawa T, Iwasaki H. Ultrasound-guided superior laryngeal nerve block and translaryngeal block for awake tracheal intubation in a patient with laryngeal abscess. Journal of Anesthesia. 2013;27(2):309-310
25.Manikandan S, Neema PK, Rathod RC. Ultrasound-guided bilateral superior laryngeal nerve block to aid awake endotracheal intubation in a patient with cervical spine disease for emergency surgery. Anaesthesia and Intensive Care. 2010;38(5):946-948
26.Minogue SC, Ralph J, Lampa MJ. Laryngotracheal topicalization with lidocaine before intubation decreases the incidence of coughing on emergence from general anesthesia. Anesthesia and Analgesia. 2004;99(4):1253-1257
27.Tanaka Y, Nakayama T, Nishimori M, Sato Y, Furuya H. Lidocaine for preventing postoperative sore throat. Cochrane Database of Systematic Reviews. 2009;3:CD004081
28.Tsui B, Ip V, Walji A. Airway sonography in live models and cadavers. Journal of Ultrasound in Medicine. 2013;32(6):1049-1058
29.Kaur B, Tang R, Sawka A, Krebs C, Vaghadia H. A method for ultrasonographic visualization and injection of the superior laryngeal nerve: Volunteer study and cadaver simulation. Anesthesia and Analgesia. 2012;115(5):1242-1245
30.Sawka A, Tang R, Vaghadia H. Sonographically guided superior laryngeal nerve block during awake fiberoptic intubation. A A Case Reports. 2015;4(8):107-110
31.Rodríguez-Martín C, de la Cruz RC, Ruiz Piñero M, Guerrero Peral ÁL. Refractory neuralgia of the superior laryngeal nerve: A case study. Neurología. 2016;31(5):344-345
32.Kristensen MS. Ultrasonography in the management of the airway. Acta Anaesthesiologica Scandinavica. 2011;55(10):1155-1173
33.Barberet G, Henry Y, Tatu L, Berthier F, Besch G, Pili-Floury S, et al. Ultrasound description of a superior laryngeal nerve space as an anatomical basis for echoguided regional anaesthesia. British Journal of Anaesthesia. 2012;109(1):126-128
34.Kumar A, Sinha C, Kumar A, Bhadani UK. Transverse approach for ultrasound-guided superior laryngeal nerve block for awake fiberoptic intubation. Saudi Journal of Anaesthesia. 2017;11(3):373-374
35.Simmons ST, Schleich AR. Airway regional anesthesia for awake fiberoptic intubation. Regional Anesthesia and Pain Medicine. 2002;27(2):180-192
Written By
Eugenio Daniel Martínez Hurtado, Nekari de Luis Cabezón, Miguel Ángel Fernández Vaquero and Míriam Sánchez Merchante
Submitted: 18 June 2023Reviewed: 09 November 2023Published: 03 April 2024
 Open access peer-reviewed chapter
Open access peer-reviewed chapter