 Open access peer-reviewed chapter
Open access peer-reviewed chapter
Abstract
This chapter describes increasing and sustaining environmental health literacy (EHL) within the less disadvantaged and minority communities in third-world countries. People from developing countries experience systemic barriers to quality and affordable health due to economic disadvantages and lower educational attainment levels. Traditional cultural practices in developing economies reflect values and beliefs held by members for periods spanning generations. However, harmful conventional methods include female genital mutilation (FGM), forced feeding of women, early marriages, taboos, and religious beliefs that prevent women from controlling their fertility, nutritional taboos and traditional birth practices, early pregnancy, and bride price, among others. These undesirable practices affect public health negatively and increase the risk of otherwise preventable diseases. This chapter discusses community-based education approaches to promote healthy living styles and improve attitudes toward clinical interventions and treatments. The chapter contains examples of community-engaged education initiatives to promote EHL in various contexts, like community-initiated training that creates public awareness. Community-based education systems can contribute to building and sustaining equitable access to professional health and partnership between communities and stakeholders in the health sectors, emphasizing mutual co-learning and knowledge co-creation to meet unique existing and emerging needs.
Keywords
- environmental health literacy
- developing countries
- sustainability
- public education
- and harmful cultural practices
1. Introduction
Communicable diseases refer to transferable diseases transmissible by contact with infected individuals, bodily discharge, fluids like respiratory droplets, blood or semen, and contaminated surfaces. The World Health Organization (WHO) defines communicable diseases as infectious conditions, including HIV/AIDS, tuberculosis (TB), malaria, viral hepatitis, sexually transmitted infections (STIs), and neglected tropical diseases (NTDs) [1]. Despite the success of vaccination programs worldwide, some infectious diseases like polio, malaria, TB, HIV/AIDS, and others constitute a significant health burden in most African countries [2].
Undesirable cultural practices, low levels of education, low income, and ignorance are among the key factors contributing to the spread of infectious diseases in African countries. WHO estimated that contagious diseases caused 14.7 million deaths in 2001, which accounted for approximately 26% of all global deaths [3]. However, WHO reports indicate that existing drugs and vaccines could have prevented these deaths [3]. Besides, food access and drinking water free from fecal contamination could have prevented approximately 2 million communicable disease-related deaths [3]. These challenges continue to undermine the quality of public health in developing countries despite the observed progress in controlling infectious diseases in developed nations. Low-income and lower-middle-income countries continue to experience the poorest overall health outcomes despite the progress achieved in fighting contagious diseases worldwide [4]. Although global interventions against infectious diseases have led to a two-fold reduction in HIV incidence between 2000 and 2018, the observed change is inadequate to reach the sustainable development goals (SDG) target to end the HIV/AIDs epidemic by 2030 [4]. Lack of focus on the cultural and social factors that increase the risk of infectious diseases in developing countries contributes to these slowed rates in reducing infectious diseases.
2. Burden and impact of communicable diseases in developing countries
Communicable diseases are infectious and preventable through appropriate lifestyles and sustainable health policies. Developed countries have made significant progress in eradicating infectious diseases from their populations. However, developing countries lag in eradicating infectious diseases. The situation increases the burden on public health. Failure to manage infectious diseases increases the burden of non-communicable diseases.
2.1 The burden of communicable diseases in developing countries
The burden of infectious diseases in developing countries remains a significant issue in health. Contagious diseases like respiratory infections, HIV/AIDS, diarrhea, Malaria, and tuberculosis claimed approximately 12 million lives annually [2] in developing countries in the past two decades. Infectious diseases contribute nearly 80% [2] of the disease burden in developing countries. The disease burden continues to increase despite the implementation of vaccination programs. Sub-Saharan Africa has the highest number of HIV/AIDS infections, which accounts for approximately two-thirds of the global population living with HIV [5]. Research findings from recent studies indicated that the cervical cancer burden caused by HPV infection was highest in Sub-Saharan African regions and Oceania, with more than 250 disability-adjusted life-years (DALYs) per 100,000 population in each area [6]. Due to undesirable cultural practices, the level of new infections in developing countries in Oceania and Sub-Saharan regions is higher than in developed countries.
Sub-Saharan countries continue to experience an epidemic of infectious diseases. Sub-Saharan Africa has approximately 37 million people living with HIV/AIDS, where groups with specific high-risk behaviors contribute to about 47% of new infections [7]. Some groups with high-risk behaviors, which contribute to the rise of new diseases, include LGBTQs, prisoners, drug addicts, and sex workers.
The ongoing interventions to reduce and combat the rise of infectious diseases fail to yield desirable outcomes. Figure 1 shows HIV prevalence and antiretroviral therapy (ART) in some African countries. Countries like Eswatini, Lesotho, and Botswana have high levels of HIV infections and ART uptake. These outcomes suggest that the availability and use of ART interventions may contribute to the rising of new HIV infections. Despite ongoing interventions, cultural and social values are possible causes of the rising infectious diseases in developing countries.
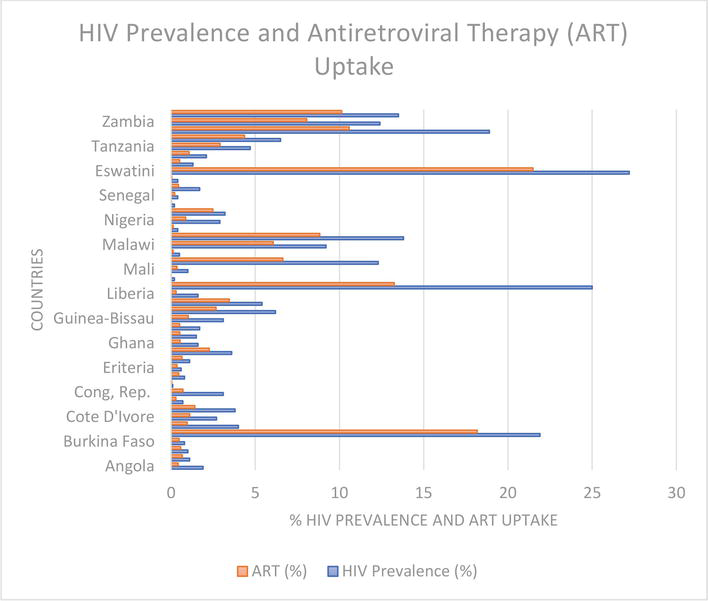
Figure 1.
HIV prevalence and ART uptake in different African countries. The data presented in this figure is a summary of the findings presented in Coetzee et al. ([
2.2 Impacts of communicable diseases in developing countries
The lack of effective methods to manage infectious diseases in developing countries increases the overall public health burden. Okongo et al. developed a mathematical model indicating that TB and malaria treatment has an insignificant effect on HIV/AIDS prevalence [8]. The presence of HIV/AIDS increases the burden of diseases among high-risk populations. However, the mathematical models developed by Okongo et al. revealed that effective management of HIV/AIDS could lower the risk of developing other infectious diseases [8]. Ineffective ways to manage HIV/AIDS as an infectious disease in developing countries increase the burden of public health. The HIV/AIDS crisis at the end of the twentieth century and the resulting high burden of infectious diseases in low- and middle-income countries made managing infectious diseases a high-priority initiative [9]. Despite such intentions, ongoing interventions on infectious diseases are less effective because of low community engagement. Lack of public awareness in Sub-Saharan African countries leads to a situation where malaria and HIV/AIDS continue to drive substantial public health loss at higher rates than those recorded in the twentieth century [9]. Some risk factors for declining public health due to infectious diseases include inadequate knowledge and undesirable cultures that compel people to engage in unsafe lifestyles.
The ongoing epidemic of infectious diseases in developing countries increases the risk of non-communicable diseases. Sub-Saharan Africa faces a double burden of communicable and non-communicable diseases due to the adopted health systems and policies [10], which hinder the effectiveness of the adopted intervention. Sub-Saharan African countries lack robust health systems that can satisfy the needs of a population. Robust health systems integrate personal and public health care services, teaching and research, and health insurance [10]. The absence of practical research and health insurance policies in developing countries undermines the efforts to manage communicable and non-communicable diseases. The inevitable results include an increased burden in managing non-communicable conditions that people may fail to prioritize. Case study 1 presents a unique scenario of a woman struggling with non-communicable illnesses due to a lack of effective government measures to manage infectious diseases. Lack of adequate knowledge or access to appropriate preventive measures and ARVs contributes to Joan’s deteriorating health. Joan’s HPV and HIV/AIDS infections were the primary causes of cervical cancer. The increasing burden of infectious diseases exposes low-income earners in developing countries to higher risks of developing non-communicable conditions. HIV/AIDS infections increase the risk of developing specific malignancies [11, 12], which contributes to an emerging epidemic in Sub-Saharan Africa [13]. The less effective health interventions in developing countries are unsustainable because they increase the burden of sickness and the cost of treatment. For instance, failure to manage HIV/AIDS and HPV infections increases cancer risk in developing countries.
Case Study 1
Joan (anonymous name) is 48 years old and a single mother of two teenage girls. Joan is a sex worker in the City of Nakuru in Kenya, with an average monthly income of $300. Joan lives with HIV/AIDS and developed respiratory complications due to her working conditions. In addition, Joan developed cervical cancer due to a possible HPV infection. Neither she nor the two girls have received an HPV vaccine.
Joan did not have prior knowledge about HPV or effective prevention methods. Her income is inadequate to cater for reliable health insurance coverage. She cannot afford the required treatments for cancer and respiratory complications. The inaccessibility of Antiretroviral drugs (ARVs) exposes Joan to higher risks of deteriorating health. Joan struggles to raise her children and provide them with access to quality education. Her current health state leaves the two teenage girls to seek unreliable part-time jobs to sustain their needs.
Joan experiences familial rejection and social stigma as a sex worker. The African culture requires women to have and support a family. Unmarried women, especially sex workers, experience social and cultural stigma. The current social and cultural challenges discourage Joan from seeking assistance from non-governmental organizations.
The rising epidemic of HPV in Sub-Saharan African countries increases the burden of cancer cases. Various studies have reported a high prevalence of HPV infections in Sub-Saharan African countries [14, 15, 16, 17], with high rates among men ranging between 19% and 100% [14]. These prevalence levels in Sub-Saharan African countries are higher than the global average, ranging between 1.3% and 72.9% [14]. The prevalence of HPV infections among African men contributes to higher infection rates among women. Results from a study, which comprised 1846 participants, indicated an average prevalence of 29.07% for women over 25 years, with the highest rate being 42.2% among women aged between 25 and 29 years [15]. Poor HPV management practices in developing countries contribute to the rising level of HPV infections and related cancer cases. Some barriers to effective HPV vaccination include limited health system capacities, socio-economic status, stigma, fear, and cost of vaccines [17]. These barriers lead to low levels of HPV vaccination among young girls and high cancer related cases at later ages. Figure 2 shows data on cancer patients treated between January 2002 and May 2023 at Moi Teaching and Referral Hospital (MTRH), a radiotherapy center in Kenya. There were 279 cases of cervical cancer out of 1090 cancer patients treated at the facility within the stipulated period. Approximately 26% of all cancer cases treated at MTRH are cervical cancers, mainly caused by HPV infections. This data indicates the current scenario in Sub-Saharan countries where the lack of effective ways to manage infectious diseases increases the risk of non-communicable diseases. In addition, undesirable cultural and social practices are a significant factor that increases contagious diseases in developing countries.
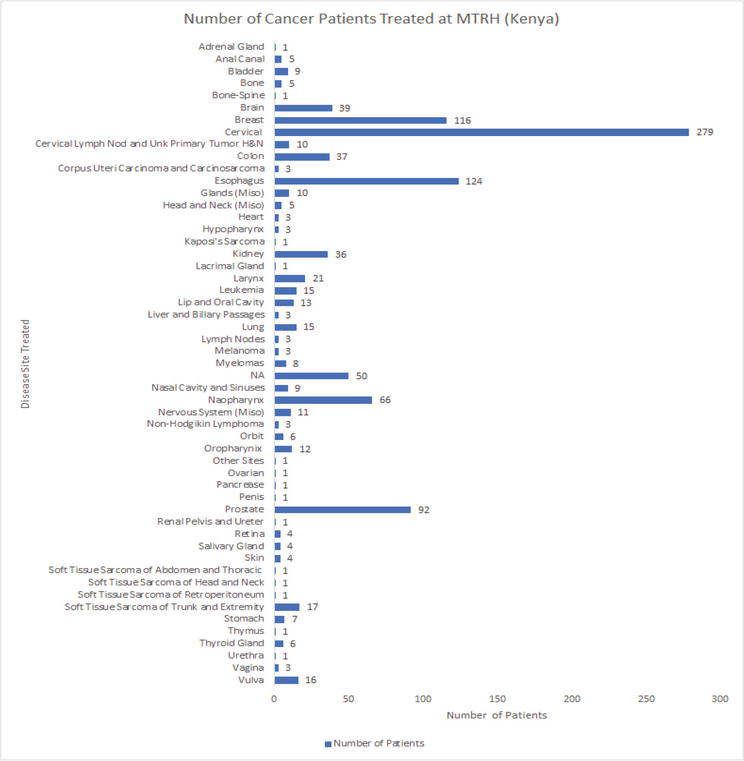
Figure 2.
Different cancer cases were treated at Moi Teaching and Referral Hospital between 1/1/2022 and 6/23/2023.
3. Cultural factors that increase the risk of communicable diseases
Sab-Saharan African countries struggle with infectious diseases like malaria, HIV/AIDS, acute respiratory infections, cholera, tuberculosis, hepatitis B, Ebola, and COVID-19 [10]. Some of these infectious diseases occur due to specific cultural and social practices, which escalates the burden of public health. This section focuses on three contagious diseases and how cultural factors increase their risk in developing countries. Failure to align health interventions with socio-cultural values and practices through effective community engagement undermines their effectiveness.
3.1 Hepatitis
The prevalence of hepatitis infections occurs due to socio-cultural barriers to the utilization of appropriate sexual health services [18]. Cultural norms that influence people to underestimate preventative health, gender norms, and help-seeking behaviors increase the risk of hepatitis infections [18]. For instance, some cultural norms that promote male chauvinism may encourage men to engage in unhealthy sexual practices that increase their risk of hepatitis infections. Besides, the desire to fulfill specific cultural roles and values increases the prevalence of infectious diseases. Cultural and lifestyle practices that may include but are not limited to circumcision, female genital mutilation, tattooing, ear piercing, and unprotected sexual [19] activities increase the risk of hepatitis B virus (HBV) infections among teenagers. Some cultural practices dictate that people must engage in practices like traditional circumcision, which increases the risk of contracting HBV. Although Hepatitis B is a vaccine-preventable condition, its prevalence remains high in Ghana despite the introduction of vaccines [19]. Some religious and cultural practices discourage people from using pharmaceutical medications and vaccines, increasing the risk of infectious infections. Hepatitis B and C are significant public health problems in developing countries where between 40% and 80% of people ignorantly live with chronic hepatitis B and C [20]. Lack of knowledge of serostatus causes many infectious people to spread the virus to others. Inadequate public awareness of the importance of conducting regular health checkups and seeking timely treatment leads to a situation where contagious people spread the virus unknowingly.
3.2 HIV/AIDS
Social and cultural factors increase the prevalence level of HIV/AIDS in developing countries. Some undesirable cultural practices such as child marriage, socio-cultural gender, power, economic disparities, and sex at an earlier age [21, 22, 23] increase the prevalence of HIV/AIDS. The patriarchal culture in most African communities denies women equal opportunities for education, power, and employment and exposes them to early marriages. Several factors, including incentives to marry out young women to lessen the financial burden on low-income African families, contribute to child marriage [23]. Power disparities between men and women deny girls an opportunity to influence the decisions regarding their marriages. Besides, economic differences affect many girls to get married at an early age. These factors contribute to an increasing rate of HIV/AIDS infections. Some scholars [23] have found that the need to reinforce social ties, protect daughters from sexual adversity, and improve social status by marrying girls to well-off families is standard in African cultures. The lack of proper public awareness of how such practices impact health by increasing the risk of contracting HIV/AIDS is a significant problem in African countries.
Inadequate sexual and reproductive health and rights (SRHR) undermines the nature and responses to challenges that increase the risk of HIV/AIDS in African settings. Effective SRHR strategies require an extensive understanding of the socio-cultural and spatial settings where people live [24]. The relevant stakeholders can improve the quality of public health by engaging members of the target group to incorporate their cultural and social values. For instance, mitigating sexually transmitted infections (STIs) remains a significant challenge in Sub-Saharan Africa due to harmful cultural practices, illiteracy, and lack of access to screening services [25]. Most African women lack adequate knowledge of the impact of negative cultures on their overall health or the availability of appropriate health interventions. In addition, the fear of expressing pressing health concerns due to the imposed cultural values increases the risk of health burdens in African women.
3.3 COVID-19
COVID-19 represents a unique, infectious disease whose impact on Africans was influenced by socio-cultural values and norms. Mitigating the effects of the COVID-19 pandemic in a nonhomogeneous continent like Africa requires adopting locally relevant and culturally appropriate interventions [26]. Africans have unique and diverse cultures that influence their behaviors and attitudes toward health outcomes. The strategies used to contain COVID-19 in developed countries were less effective in Sub-Saharan communities depending on the targeted communities’ cultural, social, and economic conditions. Failure to engage local communities leads to weak adoption of public health measures irrelevant to a cultural context [27]. These challenges became evident during the COVID-19 pandemic. For example, vaccine uptake hesitancy was a significant problem in Africa, which undermined the effectiveness of containing the pandemic [28, 29, 30, 31, 32, 33]. Vaccine acceptance depended on people’s interest in protecting against COVID-19, and concerns about possible side effects were the leading cause of hesitancy [31]. Lack of adequate education on the effectiveness of vaccines in containing a pandemic influences people to disregard the containment measures taken by governments and healthcare institutions. Positioning vaccines to reflect equitable access and benefits to the targeted population effectively reduces possible resistance [28]. Failure to engage community leaders and local healthcare providers in rolling out vaccination programs contributed to the hesitancy observed across developing countries. For instance, some Africans regarded compulsory isolation and vaccination as violating their fundamental rights to association, religion, and freedom of choice. The hesitancy to uptake COVID-19 indicated people’s desire to safeguard their independence and participate fully in deciding the right health interventions that align with their needs.
The case study of Tanzania in managing COVID-19 reveals the impact of cultural practices in increasing the risk of infectious diseases. The negative perception toward foreign COVID-19 vaccines compelled Tanzanians to use plant products like eucalyptus species, pepper, berries, ginger, garlic, and onions, among others, to manage the pandemic [34]. Although the natural products may have had positive outcomes in containing the pandemic, the desire to safeguard cultural independence compelled Tanzanians to reject pharmaceutical vaccines. Figure 3 shows some methods used to control the COVID-19 pandemic in Tanzania, despite the need for adequate scientific evidence regarding their effectiveness.
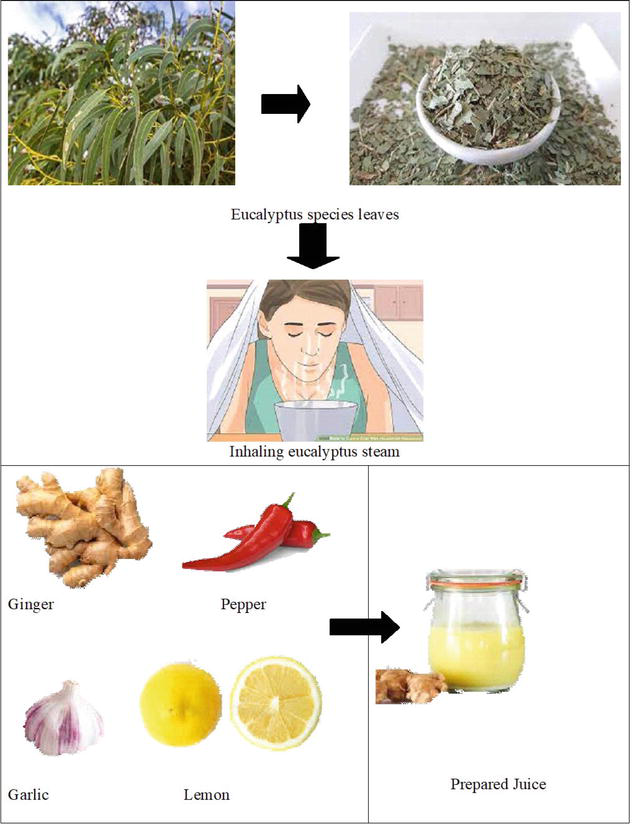
Figure 3.
Natural products used to control the COVID-19 pandemic in Tanzania. Modification of a chart presented in Mlozi ([
Women from North-West Tanzania gave accounts of how they used cultural-based containment measures to control the COVID-19 pandemic. Some of their interventions included biomedical solutions, cultural and religious frames, traditional practices, and spiritual interventions alongside public health recommendations [35]. Such patterns reveal the importance of cultural and religious values in promoting public health. Excluding important socio-cultural values in the adopted interventions may result in hesitancy to adopt recommended public health interventions. The introduction of various concoctions to curb the COVID-19 pandemic in Tanzania resulted from the experience of using medicinal herbs to prevent, treat, and cure epidemics in the past [36]. Traditional medicine practices and interventions are crucial in enhancing and promoting public health. In addition, religious and spiritual practices accompanying such conventional health interventions are essential in promoting public acceptance of proposed medications. Although extensive use of scientifically unproved interventions may increase the prevalence level of infectious diseases, the case study of Tanzania provides a renewed perception of managing communicable diseases.
4. The role of community education in minimizing the risk of communicable diseases
Community education is essential in promoting health sustainability by minimizing the risk of infectious diseases. Educational instructions through face-to-face or online approaches were critical to promoting public health during the COVID-19 pandemic [37]. Engaging people through relevant education and instructions can allow them to understand the importance of embracing scientifically proven health interventions. Such practices promote sustainability by ensuring the effective use of available resources for prompting public health due to reduced hesitancy in adopting pharmaceutical medications. Education allows people to develop a wide range of skills and behaviors that can predispose them toward improved health and well-being [38]. Public health education must motivate people to change their lifestyles and behaviors to promote health outcomes. Effective community education programs should focus on addressing the existing gaps in a specific community. For instance, a general lack of knowledge and misconceptions about the transmission of infectious diseases is a current problem [39]. Healthcare workers should strive to understand people’s misconceptions about a particularly contagious disease. The designed learning interventions should incorporate adequate knowledge to allow people to embrace preventive measures for infectious diseases and their valued socio-cultural practices and beliefs. Healthcare providers should understand the importance of socio-cultural values in a community to avoid people resisting the appropriate ways of controlling infectious diseases. Effective community education should involve collaboration between primary care providers (PCPs) and patients. Some elderly HIV/AIDS patients expressed their concerns that PCPs lack an understanding of their sexual needs [39]. Taking time to understand the factors that affect health perceptions among specific groups can reduce resistance and negligence among the target groups.
Community education programs should align with the local socio-cultural needs of the targeted communities. Most developing countries have cultural diversity, influencing people’s behaviors and attitudes toward infectious diseases. For example, outreach programs in Vietnam effectively reduced risky sexual behaviors and increased HIV-testing services among the targeted high-risk groups [40]. Aligning communicable disease intervention programs with local community cultures can produce positive reception. People can appreciate the importance of various mitigations and embrace them as effective living methods to lower their risk of contracting infectious diseases. This intervention is applicable in communities where people engage in health-risk cultural practices like traditional circumcision, FGM, early marriages, and polygamous marriages. Engaging people in learning the health risks associated with valued cultural practices that promote infectious diseases can influence them to adopt healthy ways of living that lower the burden of infectious diseases.
Community education programs should incorporate cultural and social beliefs in the target population. The case of Tanzania reveals the need to allow people to combine their cultural values into the health interventions used to control infectious diseases. People attach more significant meaning to traditional, religious, and spiritual practices, influencing their overall health outcomes. Healthcare providers should engage community members in developing countries in developing community engagement health programs.
5. Conclusion
Communicable diseases continue to impose a significant health burden on public health systems in developing countries. Lack of effective community education increases the risk of communicable diseases in developing countries. Community education is essential in promoting health sustainability by reducing the risk of infectious diseases. Effective community education programs should align with the local socio-cultural needs of the targeted communities. Such interventions should integrate cultural diversity, influencing people’s behaviors and attitudes toward infectious diseases.
Acknowledgments
I acknowledge my dear wife Vivian Wanjiru and children, Dan Ndashi, Ann Muthoni, Ruth Waithera, Joseph Mwangi, Naomi Wanjiru for their support throughout this project. I also acknowledge their moral support and their willingness to give me ample time.
Acronyms and abbreviations
environmental health literacy | |
female genital mutilation | |
World Health Organization | |
tuberculosis | |
sexually transmitted infections | |
neglected tropical diseases | |
sustainable development goals | |
disability-adjusted life-years | |
antiretroviral therapy | |
Moi Teaching and Referral Hospital | |
hepatitis B virus | |
sexual and reproductive health and rights | |
primary care providers |
References
- 1.
World Health Organization. Our Work: Communicable and Non-communicable Diseases, and Mental Health. Geneva, Switzerland: WHO; 2023. Available from: https://www.who.int/our-work/communicable-and-noncommunicable-diseases-and-mental-health - 2.
Boutayeb A, Boutayeb S. The burden of non-communicable diseases in developing countries. International Journal for Equity in Health. 2005; 4 (1):532-544. DOI: 10.1186/1475-9276-4-2 - 3.
Kindhauser MK. Global Defence against the Infectious Disease Threat. Geneva, Switzerland: World Health Organization; 2003 - 4.
World Health Organization. World Health Statistics 2020: Monitoring Health SDGs. Baltimore, Maryland; 2020 - 5.
Coetzee L, Bogler L, De Neve J, Bärnighausen T, Geldsetzer P, Vollmer S. HIV antiretroviral therapy and non-communicable diseases in sub-Saharan Africa: Empirical evidence from 44 countries over the period 2000 to 2016. Journal of the International AIDS Society. 2019; 22 (7):1-7. DOI: 10.1002/jia2.25364 - 6.
Coates MM et al. Burden of non-communicable diseases from infectious causes in 2017: A modelling study. The Lancet Global Health. 2020; 8 :e1489-e1498. DOI: 10.1016/S2214-109X(20)30358-2 - 7.
Achwoka D, Mutave R, Oyugi JO, Achia T. Tackling an emerging epidemic: The burden of non-communicable diseases among people living with HIV/AIDS in sub-Saharan Africa. Pan African Medical Journal. 2020; 36 (271):1-9. DOI: 10.11604/pamj.2020.36.271.22810 - 8.
Okongo MO, Lunani MA, Menge BK, Ochwach JO. The impact of HIV/AIDS treatment and counseling on the prevalence of tuberculosis and malaria Co-infections. International Journal of Mathematical Analysis. 2023; 17 (2):51-67. DOI: 10.12988/ijma.2023.511270 - 9.
Zeltner T, Riahi F, Huber J. Acute and chronic health challenges in sub-Saharan Africa: An unfinished agenda. In: Africa’s Population: In Search of a Demographic Dividend. 2017. pp. 283-297. DOI: 10.1007/978-3-319-46889-1_18 - 10.
Sarpong E et al. Zero malaria: A mirage or reality for populations of sub-Saharan Africa in health transition. Malaria Journal. 2022; 21 (1):1-12. DOI: 10.1186/s12936-022-04340-1 - 11.
National Cancer Institute. HIV Infection and Cancer Risk. Bethesda, Maryland: National Cancer Institute; 2017. Available from: https://www.cancer.gov/about-cancer/causes-prevention/risk/infectious-agents/hiv-fact-sheet - 12.
Oliver NT, Chiao EY. Malignancies in women with HIV infection. Current Opinion in HIV and AIDS. 2017; 12 (1):69-76. DOI: 10.1097/coh.0000000000000332 - 13.
Sasco AJ et al. The challenge of AIDS-related malignancies in sub-Saharan Africa. PLoS One. 2010; 5 (1):1-10. DOI: 10.1371/journal.pone.0008621 - 14.
Olesen TB, Munk C, Christensen J, Andersen KK, Kjaer SK. Human papillomavirus prevalence among men in sub-Saharan Africa: A systematic review and meta-analysis. Sexually Transmitted Infections. 2014; 90 (6):455-462. DOI: 10.1136/sextrans-2013-051456 - 15.
Mutombo AB, Benoy I, Tozin R, Bogers J, Van geertruyden J-P, Jacquemyn Y. Prevalence and distribution of human papillomavirus genotypes among women in Kinshasa, the Democratic Republic of the Congo. Journal of Global Oncology. 2019; 5 :1-9. DOI: 10.1200/jgo.19.00110 - 16.
Okoye JO, Ofodile CA, Adeleke OK, Obioma O. Prevalence of high-risk HPV genotypes in sub-Saharan Africa according to HIV status: A 20-year systematic review. Epidemiology and Health. 2021; 43 :1-11. DOI: 10.4178/epih.e2021039 - 17.
Kutz J-M, Rausche P, Gheit T, Puradiredja DI, Fusco D. Barriers and facilitators of HPV vaccination in sub-Saharan Africa: A systematic review. BMC Public Health. 2023; 23 (1):1-13. DOI: 10.1186/s12889-023-15842-1 - 18.
Ghimire S, Hallett J, Gray C, Lobo R, Crawford G. What works? Prevention and control of sexually transmitted infections and blood-borne viruses in migrants from sub-Saharan Africa, Northeast Asia and Southeast Asia living in high-income countries: A systematic review. International Journal of Environmental Research and Public Health. 2019; 16 (7):1-17. DOI: 10.3390/ijerph16071287 - 19.
Nyambah PK, Adjei R, Sarfo B. Seroprevalence of hepatitis B virus infection is associated with male circumcision among senior high school students in the Krachi Nchumuru District in the Oti region of Ghana: A cross-sectional study. Research Square. 2023:1-22. DOI: 10.21203/rs.3.rs-2845421/v1 [Pre-print] - 20.
Ayele A, Abera D, Hailu M, Birhanu M, Desta K. Prevalence and associated risk factors for hepatitis B and C viruses among refugees in Gambella, Ethiopia. BMC Public Health. 2020; 20 (1):1-10. DOI: 10.1186/s12889-020-08893-1 - 21.
Obeagu EI, Alum EU, Obeagu GU. Factors associated with prevalence of HIV among youths: A review of Africa perspective. Madonna University Journal of Medicine and Health Sciences. 2023; 3 (1):13-18 - 22.
Mhungu A, Sixsmith J, Burnett E. Adolescent girls and young Women’s experiences of living with HIV in the context of patriarchal culture in sub-Saharan Africa: A scoping review. AIDS and Behavior. 2022; 27 :1365-1379. DOI: 10.1007/s10461-022-03872-6 - 23.
Yaya S, Odusina EK, Bishwajit G. Prevalence of child marriage and its impact on fertility outcomes in 34 sub-Saharan African countries. BMC International Health and Human Rights. 2019; 19 (1):1-11. DOI: 10.1186/s12914-019-0219-1 - 24.
Wado YD, Bangha M, Kabiru CW, Feyissa GT. Nature of, and responses to key sexual and reproductive health challenges for adolescents in urban slums in sub-Saharan Africa: A scoping review. Reproductive Health. 2020; 17 (1):1-14. DOI: 10.1186/s12978-020-00998-5 - 25.
Armstrong-Mensah EA, Ebiringa D-P, Whitfield K, Coldiron J. Genital chlamydia trachomatis infection: Prevalence, risk factors and adverse pregnancy and birth outcomes in children and women in sub-Saharan Africa. International Journal of Maternal and Child Health and AIDS (IJMA). 2021; 10 (2):251-257. DOI: 10.21106/ijma.523 - 26.
Renzaho AMN. The need for the right socio-economic and cultural fit in the COVID-19 response in sub-Saharan Africa: Examining demographic, economic political, health, and socio-cultural differentials in COVID-19 morbidity and mortality. International Journal of Environmental Research and Public Health. 2020; 17 (10):1-14. DOI: 10.3390/ijerph17103445 - 27.
Aduh U et al. Risk perception, public health interventions, and Covid-19 pandemic control in sub-Saharan Africa. Journal of Public Health in Africa. 2020; 21 (1562):1-16. DOI: 10.4081/jphia.2021.1622 - 28.
Mutombo PN et al. COVID-19 vaccine hesitancy in Africa: A call to action. The Lancet Global Health. 2021; 10 (3):e320-e321. DOI: 10.1016/s2214-109x(21)00563-5 - 29.
Sallam M. COVID-19 vaccine hesitancy worldwide: A concise systematic review of vaccine acceptance rates. Vaccine. 2021; 9 (2):1-14. DOI: 10.3390/vaccines9020160 - 30.
Aborode AT et al. Vaccine hesitancy in Africa: Causes and strategies to the rescue. Therapeutic Advances in Vaccines and Immunotherapy. 2021; 9 :1-5. DOI: 10.1177/25151355211047514 - 31.
Machingaidze S, Wiysonge CS. Understanding COVID-19 vaccine hesitancy. Nature Medicine. 2021; 27 (27):1338-1339. DOI: 10.1038/s41591-021-01459-7 - 32.
Afolabi AA, Ilesanmi OS. Dealing with vaccine hesitancy in Africa: The prospective COVID-19 vaccine context. Pan African Medical Journal. 2021; 38 :1-7. DOI: 10.11604/pamj.2021.38.3.27401 - 33.
Cooper S, van Rooyen H, Wiysonge CS. COVID-19 vaccine hesitancy in South Africa: How can we maximize uptake of COVID-19 vaccines? Expert Review of Vaccines. 2021; 20 (8):1-13. DOI: 10.1080/14760584.2021.1949291 - 34.
Mlozi SH. The role of natural products from medicinal plants against COVID-19: Traditional medicine practice in Tanzania. Heliyon. 2022; 8 (6):1-6. DOI: 10.1016/j.heliyon.2022.e09739 - 35.
Mchome Z, Mshana G, Peter E, Aloyce D, Kapiga S, Stöckl H. Women’s narratives about COVID-19, preventive practices and sources of information in northwestern Tanzania. International Journal of Environmental Research and Public Health. 2021; 18 (10):1-13. DOI: 10.3390/ijerph18105261 - 36.
Kamazima SR, Kakoko DCV, Kazaura M. “Manifold tactics are used to control and prevent pandemics in contemporary Africa”: A case of Tanzania’s fight against COVID-19. International Journal of Advanced Scientific Research and Management. 2020; 5 (11):20-33. DOI: 10.36282/ijasrm/5.11.2020.1770 - 37.
Honein MA. Summary of guidance for public health strategies to address high levels of community transmission of SARS-CoV-2 and related deaths, December 2020. MMWR. Morbidity and Mortality Weekly Report. 2020; 69 :1860-1867. DOI: 10.15585/mmwr.mm6949e2 - 38.
Raghupathi V, Raghupathi W. The influence of education on health: An empirical assessment of OECD countries for the period 1995-2015. Archives of Public Health. 2020; 78 (1):1-18. DOI: 10.1186/s13690-020-00402-5 - 39.
Davis TEK, Elder MA. HIV knowledge and preferences for HIV prevention among older adults living in the community. Gerontology and Geriatric Medicine. 2020; 6 :1-10. DOI: 10.1177/2333721420927948 - 40.
Sabin LL et al. Effectiveness of community outreach HIV prevention programs in Vietnam: A mixed methods evaluation. BMC Public Health. 2019; 19 (1):1-17. DOI: 10.1186/s12889-019-7418-5