Open Access is an initiative that aims to make scientific research freely available to all. To date our community has made over 100 million downloads. It’s based on principles of collaboration, unobstructed discovery, and, most importantly, scientific progression. As PhD students, we found it difficult to access the research we needed, so we decided to create a new Open Access publisher that levels the playing field for scientists across the world. How? By making research easy to access, and puts the academic needs of the researchers before the business interests of publishers.
We are a community of more than 103,000 authors and editors from 3,291 institutions spanning 160 countries, including Nobel Prize winners and some of the world’s most-cited researchers. Publishing on IntechOpen allows authors to earn citations and find new collaborators, meaning more people see your work not only from your own field of study, but from other related fields too.
To purchase hard copies of this book, please contact the representative in India:
CBS Publishers & Distributors Pvt. Ltd.
www.cbspd.com
|
customercare@cbspd.com
Age-related hearing loss (ARHL) is the most common sensory impairment. Older people with ARHL may vary in their profiles and usually manifest heterogeneous phenotypes, including in combination with presbyastasis, tinnitus, different frailty phenotypes, and multi-morbidity. Patients with these phenotypes generally have a decreased intrinsic capacity, high health burden, and poor prognosis, such as disability, fall, and other adverse events. However, the absence of an evidence-based guidance leads to a significant limitation of current approaches to ARHL care. Here, we present a framework for the rapid and in-depth geriatric assessment, and a recommendation for the coordinated and personalized management of older adults according to their etiology of hearing loss, imbalance, tinnitus, the status of frailty phenotype, and multi-morbidity. The main purpose is to recover functional health, reduce complications, and improve the quality of life for older people with ARHL and frailty phenotypes.
Laboratory of Aging, Anti-aging and Cognitive Performance, Shanghai Institute of Geriatrics and Gerontology, Huadong Hospital, Shanghai Medical College, Fudan University, Shanghai, China
Shanghai Key Laboratory of Clinical Geriatrics, Huadong Hospital, and Research Center of Aging and Medicine, Shanghai Medical College, Fudan University, Shanghai, China
Jian Ruan
Department of Otolaryngology, Huadong Hospital, Shanghai Medical College, Fudan University, Shanghai, China
Xiuhua Hu
Laboratory of Aging, Anti-aging and Cognitive Performance, Shanghai Institute of Geriatrics and Gerontology, Huadong Hospital, Shanghai Medical College, Fudan University, Shanghai, China
Shanghai Key Laboratory of Clinical Geriatrics, Huadong Hospital, and Research Center of Aging and Medicine, Shanghai Medical College, Fudan University, Shanghai, China
Aiguo Liu*
Department of Otolaryngology, Tongji Hospital, Tongji Medical College, Huazhong University of Science and Technology, Wuhan, China
Zhuowei Yu*
Laboratory of Aging, Anti-aging and Cognitive Performance, Shanghai Institute of Geriatrics and Gerontology, Huadong Hospital, Shanghai Medical College, Fudan University, Shanghai, China
Shanghai Key Laboratory of Clinical Geriatrics, Huadong Hospital, and Research Center of Aging and Medicine, Shanghai Medical College, Fudan University, Shanghai, China
*Address all correspondence to: 13661717346@163.com, aiguoliu309@163.com and hdyxyzw@163.com
1. Introduction
Age-related hearing loss (ARHL), or presbycusis, is highly prevalent in old age with the increase in life expectancy. It is estimated that 20–26% of adults aged 45 years and increasing to 63% in adults older than 70 years, and nearly 80% of people over 85 years have hearing loss [1, 2, 3]. ARHL is characterized by central auditory processing deficit (CAPD), including temporal processing and frequency resolution, and greater auditory speech perception challenges, apart from different degrees of peripheral hearing loss [4], and often associated with presbyastasis, subjective tinnitus or hyperacusis, and physical, cognitive, and psychological disorders [5, 6, 7, 8]. The interaction of aging and internal and external environment factors results in different pathological alterations and heterogeneous clinical phenotypes. Aging causes gradually increasing decline of multi-system physiological reserve [7]. Some external environmental factors, such as environmental enrichment, including educational, occupational, or leisure activities, are beneficial for the improvement of cognitive and auditory reserves, and active physical exercise for the improvement of multi-system physiological reserves. More environmental factors are harmful for health, referred as to stressors, including physical, physiological, psychosocial, and unhealthy lifestyles [7]. Local audiogenic stressors and otological diseases can cause auditory reserve decline, the imbalance of auditory system homeostasis, and hearing loss with tinnitus. Chronic physiological (functional reserve decline in metabolically active organs, polypharmacy) and psychological stresses (sleep problems and noise exposure), and unhealthy lifestyles (unhealthy diet, smoking, physical inactivity) might lead to the allostatic load and maladaptation in different physiological systems or organs, and multi-morbidities, such as cognitive impairment, cancer, cardiometabolic and affective disorders. In turn, the comorbidities can cause secondary hearing loss, presbyastasis, and tinnitus.
The age-related decline of functional reserve in multiple physiological systems, and following vulnerability increase of the body to minor stressor exposures, might cause the imbalance of homeostasis, allostatic load, and multi-system dysregulation. This condition is defined as frailty that could increase susceptibility to the occurrence of adverse consequences, such as disability, falls, dependence, and death risk [9]. Frailty could be classified into physical [9], cognitive [10], social [11], psychological [12], psychosocial [13], and nutritional [14] frailty phenotypes. Physical frailty rises with age and the prevalence greatly varies because of lack of standardization of concepts or measures. The prevalence of physical frailty is 8–15% in community-dwelling older people and is higher in women than in men [15, 16]. Our community population study (aged 60 years or older) indicated that the prevalence of pre-physical and physical frailty is 35.86 and 4.41% assessed by the FRAIL scale, respectively, and reversible and potential reversible cognitive frailty is 19.86 and 6.3% [17]. The prevalence of (pre-) physical frailty in otological outpatient is 25.5%, cognitive frailty is 32.17%, and cognitive impairment is 18.2% (pre-MCI 10% and MCI 8.2%) [18]. Moreover, patients with physical frailty had a lower risk for severe ARHL, tinnitus, and the presence of ARHL with tinnitus than those with cognitive frailty or cognitive impairment. Patients with the reversible cognitive frailty subtype had a lower risk for severe ARHL, tinnitus, and the presentation of ARHL with tinnitus than those with the potential reversible cognitive frailty subtype. ARHL severity was independently associated with overall cognition, and domain-specific cognition, including executive function, delayed memory, and language function [19]. Patients with ARHL, presbyastasis, and tinnitus had a high risk for cognitive impairment. Physical frailty and ARHL accompanying presbyastasis and/or tinnitus had significant impacts on the overall and domain-specific quality of life [20, 21]. Physical frailty had a stronger and more profound effect on the quality of life, particularly on independent living and pain in the physical dimension and happiness and coping in the psychosocial dimension.
Since ARHL is heterogeneous and usually accompanies high prevalent multi-morbidities, frailty phenotypes, the cooperation among audiologist, otologist, and geriatrician is required to face the aforementioned challenges. Frailty is a pre-disable status, and dynamic and potentially reversible. Apart from hearing and balance rehabilitation, to integrate person-centered geriatric assessment and personalized intervention into the diagnosis and management of ARHL could achieve healthy aging and reduce the risk of complications and adverse outcomes, including geriatric syndrome, functional disability, fall, dependence, and poor quality of life.
2. Early detection of presbycusis with different frailty phenotypes
There are guidelines for the etiological assessment of bilateral sensorineural hearing loss and comprehensive audiological management in children [22, 23]; and for the screening and management of ototoxic hearing loss [24]. There are also some protocols or proposals for the etiological assessment and management of presbyastasis [8, 21, 25] and tinnitus [26, 27]. Moreover, the United States Preventive Services Task Force concluded that the evidence is insufficient to assess the balance of benefits and harms for health outcomes of screening for hearing loss in asymptomatic adults 50 years or older (excluding conductive hearing loss, congenital hearing loss, sudden hearing loss, or hearing loss caused by recent noise exposure, or those reporting signs and symptoms of hearing loss) [28]. However, the international guideline for the screening and management of older adults with ARHL is limited. Notwithstanding, hearing loss has been considered as a critical component of sensory domain impairment of intrinsic capacity (IC) [29]. World Health Organization (WHO) proposed the guidance for the person-centered assessment of intrinsic capacity [30] and for systems and services of integrated care for older people (ICOPE) implementation framework [31]. For older people, several clinical practice guidelines for the screening, assessment, and management of frailty had been proposed by different organizations [32, 33, 34]. In order to reorient the disease-centered to function-centered care model and achieve healthy aging, we propose a coordinated care framework to optimize the early detection and management of ARHL according to the framework for integrated care for older people with intrinsic capacity decline and clinical practice guidelines for the management of frailty.
2.1. Rapid screening for the subject with presbycusis and different phenotypes in primary care
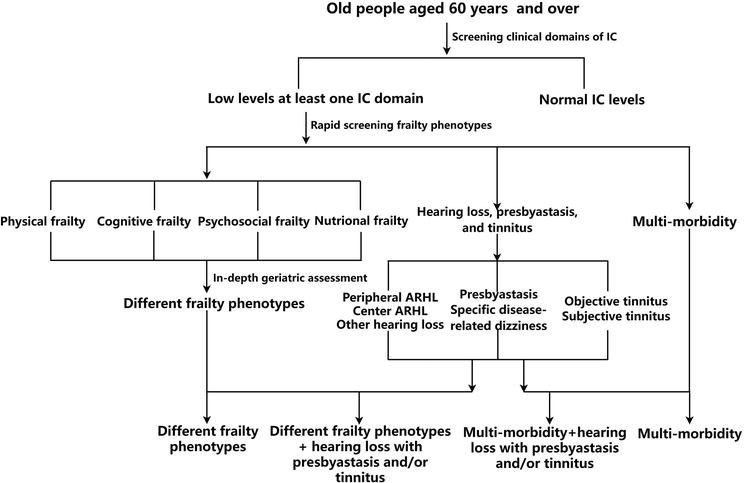
To capture the major clinical events, including declines in functions, onset of disability, frailty, and burdensome chronic diseases in older people aged 60 years and over, a general assessment approach for the subject with ARHL and different frailty phenotypes contains two steps outlined in Figure 1. The recommended step 1 is the rapid geriatric assessment, including rapid screening in primary care settings for the loss in IC and physical frailty phenotypes. Step 2 is the in-depth geriatric assessment in secondary care settings, including frailty phenotypes and the etiology of hearing loss, presbyastasis, and tinnitus.
Figure 1.
An approach to rapid screening and in-depth assessment of ARHL with presbyastasis, tinnitus, frailty phenotypes, and multi-morbidity.
For the beginning, the ICOPE step one is used to screen for loss of domain-specific IC (i.e., locomotion, cognition, vitality/nutrition, and psychological and sensorial capacities) by using a screening test (Table 1) [33, 35]. The screening test can be delivered by primary providers or by patient self-assessment using either a mobile application for a smartphone or an Internet conversational robot. The IC domains were monitored by a primary provider or nurse each 4 months [36].
Intrinsic capacity domains
Recommended screening tests
Cognitive decline
Remember three words: for example: flower, door, rice
Orientation in time and space, what is the full date today? Where are you now (home, clinic, etc.)
Recalls the three words
Limited mobility
Chair rise test, Rise from chair five times without using arms
Did the person complete five chair rises within 14 seconds?
Malnutrition (vitality impairment)
Weight loss: Have you unintentionally lost more than 3 kg over the last 3 months?
Appetite loss: Have you experienced loss of appetite?
Depressive systems (impairment in psychological domain)
Over the past 2 weeks, have you been bothered by: feeling down, depressed or hopeless: little interest or pleasure in doing things.
Visual impairment (sensory impairment)
Do you have any problems you are your eyes: difficulties in seeing far, reading, eye diseases or currently under medical treatment (e.g., diabetes, high blood pressure)?
Hearing loss (sensory impairment)
Hears whispers (whisper test) or screening audiometry result is 35 dB or less or passes automated app-based digits-in-noise test
Table 1.
The rapid screening for the loss in intrinsic capacity [33, 35].
About sensorial capacity domain, we proposed a preliminary presbyastasis and tinnitus screening also should be performed during hearing loss screening, since presbyastasis and tinnitus are the most related symptoms in older adults with hearing loss. Presbyastasis, or age-related degeneration of peripheral as well as the central part of the vestibular system, refers to dizziness and/or ataxia with apparent localizing signs and is typically attributed to the aging process [25, 37]. The clinical differentiation of presbyastasis from symptoms related to specific diseases or risk factors is required based on medical history. These diseases include specific or unilateral vestibular diseases, such as Meniere’s disease, visional impairment from various etiologies, muscle weakness, neurological lesions, diabetes-related neuropathy, cognitive impairment, arthritis, narrowing of the lumbar vertebral canal, and lumbago-sciatica [21, 25, 38]. The risk factors include polypharmacy, especially drugs for hypertension (e.g., diuretics), anxiety, or depression, excessive consumption of alcohol, and extrinsic environmental factors, such as stairs and other indoor obstacles [25]. ARHL and noise exposure are the most common causes of non-pulsatile tinnitus (subjective tinnitus) [5, 6]. Other etiologically differential diagnosis of tinnitus symptoms includes pulsatile or objective (pulsatile synchronous or vascular and asynchronous or mechanical) tinnitus, and more common subjective tinnitus accompanying unilateral or bilateral hearing loss [26, 27]. The screening also includes tinnitus-related systemic morbidities, such as cardiometabolic diseases, mental health disorders, neurological diseases (e.g., multiple sclerosis and head injury), tinnitus-related otological diseases, such as Meniere’s disease, middle ear infection, noise exposure, and tinnitus-related polypharmacy, such as diuretics for hypertension therapy [39], aspirin [40, 41], and other ototoxic medications [24]. Visual analog scales and questionnaires (e.g., Tinnitus handicap inventory and Tinnitus functional index) usually are used to assess tinnitus annoyance, distress, and severity [42].
Once IC decline was confirmed, individuals would have rapid physical frailty screening [33]. Although there are more than a dozen rapid frailty screening instruments, the FRAIL Scale is widely validated, simple, and rapid tool for the screening of physical frailty phenotype [32, 33, 34]. The FRAIL scale is a simple five-item questionnaire: Fatigue: Are you fatigued? Resistance: Cannot walk up one flight of stairs? Aerobic: Cannot walk one block? Illnesses: Do you have more than five illnesses? Loss of weight: Have you lost more than 5% of your weight in the last 6 months? Pre-physical frailty is defined as scoring 1 or 2; physical frailty is defined as scoring 3 or greater.
After IC and physical frailty screening, individuals were classified into with (pre-) physical frailty and without frailty. Among these with (pre-) physical frailty, individuals further were classified into psychological, nutritional, cognitive, and mixed frailty phenotypes according to the decline of domain-specific IC. The mixed frailty phenotype means accompanying a decline in two or more than two domains of IC. Individuals with cognitive frailty could be classified into reversible and potential reversible cognitive frailty [10, 17] using the rapid cognitive screening (RCS) tool [43] in combination with a pre-mild cognitive impairment (pre-MCI) questionnaire with two items [17]. The scores for dementia and MCI were ≤5 and 6-7, respectively. Individual with a score of 8-10 was considered to have pre-MCI when had a positive response to pre-MCI questionnaire. Individuals with (pre-) physical frailty and pre-MCI or MCI were defined as reversible or potentially reversible cognitive frailty.
Individuals without (pre-) physical frailty but with domain-specific decline of IC were referred to as psychological, cognitive, and sensory diseases, and other multi-morbidities (less than five chronic illnesses in the FRAIL questionnaire). These without domain-specific decline of IC and chronic diseases were considered as robust individuals. Thus, older people were classified into individuals having ARHL with different frailty phenotypes and multi-morbidity, individuals having ARHL with multi-morbidities (especially cardiometabolic morbidity), these with different frailty phenotypes, and robust individuals.
2.2. In-depth Assessment for the subject with presbycusis and different phenotypes in secondary care
Although rapid screening instruments for frailty phenotypes are sensitive, these tools often display low specificity [44]. In order to timely identify the causes of ARHL and tinnitus, individuals with ARHL and different frailty phenotypes by rapid geriatric assessment require referral to secondary care for in-depth IC-centered geriatric evaluation and frailty phenotype assessment by audiologist/geriatrician. The ICOPE care plan provides preliminary recommendations for in-depth geriatric assessment for the loss of IC [35].
Since individuals with ARHL usually accompany CAPD, presbyastasis, and subjective tinnitus, we proposed additional tests for the in-depth assessment of ARHL. For peripheral ARHL in-depth assessment, the results of audiometry should include pure-tone threshold average of the frequencies 0.5, 1.0, and 2.0 kHz (speech-frequency pure-tone average) and 4.0, 6.0, and 8.0 kHz (high-frequency pure-tone average). The word recognition (discrimination) scoring was determined by using the percentage of recognition of a list of monosyllabic phonetically balanced words at 30–40 dB above the PTA threshold for each ear. A score greater than 70% was considered normal to understand speech in a quiet environment [45, 46]. According to the WHO definition of disabling ARHL, peripheral ARHL was defined as a PTA threshold greater than 40 dB hearing level in the better ear [47].
For CAPD in-depth assessment, the eligible subject criteria for the central auditory tests include normal tympanogram, presenting ipsilateral acoustic reflexes, no history of ear surgery to exclude possible middle ear disease in the past or present, no history of hearing loss since childhood, and less than 21 dB difference among pure-tone averages (PTA) for 0.5, 1.0, and 2.0 kHz for the two ears to exclude otologic disorders (e.g., congenital or unilateral sudden deafness, tumor, or infection) other than aging [45, 46]. Moreover, individuals have no disabling peripheral ARHL (i.e., PTA threshold below 40 dB hearing level in the better ear, word recognition score at 30 dB over PTA threshold over 70%) [45, 46]. The test used to diagnose age-related CAPD includes the Synthetic Sentence Identification With Ipsilateral Competitive Message (SSI-ICM), Staggered Spondaic Word test, and other tests [48]. The SSI-ICM test consists of administering for each ear a primary signal of 10 short sentences against a background competition signal. The short sentences are presented at 50 dB over the PTA for each ear. The rate of identification of sentences is expressed as a percentage (0–100%) at various primary-competitive ratios (0, +5, +10 dB sound pressure level). Age-related CAPD was considered present when the patient scored less than 50% in the better ear with a 0-dB message-competition ratio [45, 46, 48].
Apart from medical history, the in-depth assessment for individuals with presbyastasis includes gait and stance assessment, such as “time up-and-go” test, standing on one leg, to differentiate dizziness from ataxia [25]. Hearing assessment, other accurate otoneurological evaluation, including Romberg, Unterberger, head-shaking, and Halmagyi tests, the Dix-Hallpike maneuver, and dynamic posturography; vestibular function assessment tests, such as rotational and caloric tests, videonystagmography or electronystagmography examination, and otolith function assessment usually were used to differentiate presbyastasis from disease-specific imbalance. [8, 25]. The video head impulse test was recently verified to be an effective test for the differentiation presbyastasis from Meniere’s disease [38] and the prediction of fall risk in elderly patients [21]. Computed tomography imaging, MRI scanning, and ultrasonography are important auxiliary examinations.
The in-depth assessment for referring people with tinnitus includes tinnitus with acute conditions, such as a crisis of mental health, significant neurological systems or signs, uncontrolled vestibular symptoms, suspected stroke [49], tinnitus disorder (associated with emotional distress, cognitive dysfunction, and/or autonomic arousal, leading to behavioral changes, and functional disability) [50], tinnitus with sudden hearing loss, objective tinnitus, and tinnitus with unilateral or asymmetric hearing loss [26, 27, 49]. The differential diagnosis of tinnitus symptoms could be conducted by in-depth assessment, including audiological testing, psychoacoustic tests (pitch, loudness, and matching), and imaging. Idiopathic intracranial hypertension, glomus tumors, and atherosclerosis of the carotid arteries are frequent causes of pulse synchronous tinnitus [51]. Eustachian tube contraction and middle ear muscle myoclonus might cause pulse asynchronous tinnitus [27]. Unilateral tinnitus, but normal otoscopy and positive neurologic signs might be caused by cerebellopontine angle tumor, brainstem infarction, and multiple sclerosis; and by noise exposure; and these with negative neurologic signs might be Meniere’s disease, semicircular canal dehiscence. Apart from ARHL and noise exposure, bilateral hearing loss and normal otoscopy findings might also be caused by acoustic trauma, otosclerosis, and ototoxic medication [26, 27].
To improve the specificity of (pre-) physical frailty, a cardiovascular health study frailty screening scale with more objective parameters (weight loss, exhaustion, low activity, slowness, and weakness) is used as an in-depth assessment instrument [9]. Individuals with a score of 1 or 2 is diagnosed as pre-physical frailty; and with a score of 3 or greater is diagnosed as physical frailty. Individuals, with (pre-) physical frailty simultaneously presenting impairment in the cognitive domain of IC, are classified as cognitive frailty. Cognitive performance could be thoroughly assessed by using demographically corrected normative z scores on the Neuropsychological Test Battery [52, 53, 54]. Reversible and potentially reversible cognitive frailty subtypes could be diagnosed according to the severity of cognitive impairment, including pre-MCI and MCI [18]. Social and psychological domains of IC are assessed by using the 21-item Social Dysfunction Rating Scale [55] and the 15-item short form of the Geriatric Depression Scale [56], respectively. Individuals with (pre-) physical frailty simultaneously presenting social or psychological dysfunction are classified as social or psychological frailty phenotype. Nutritional frailty phenotype could be diagnosed when individuals simultaneously present (pre-) physical frailty and nutritional imbalance [14]. Malnutrition also could be identified using a Mini nutritional assessment or malnutrition universal screening tool [35]. These in-depth geriatric assessments may uncover unrecognized problems following the rapid geriatric screening and provides the possibility for multi-disciplinary specialists to design and implement function-centered and personalized interventions, which can promote patient healthy aging.
3. The management of presbycusis with different frailty phenotypes
Multi-modality intervention is required for these ARHL with frailty phenotypes and/or multi-morbidity. An integrated and person-centered approach to the management of ARHL with frailty phenotypes and multi-morbidity is shown in Table 2.
Hearing loss
Presbyastasis
Tinnitus
Frailty phenotypes
Multi-morbidity
Stop noise and ototoxic medication exposure
Identify risk factors and exclude potential curable causes
Exclude polypharmacy-related subjective tinnitus
Multi-component physical activity programs (resistance and aerobic exercise, balance, or coordination training) to reverse or slow the progression of (pre-)physical frailty
Proactive personalized assessment and care plan
Prescribe hearing aid
Vestibular and balance rehabilitation
Optimal pre-operative risk and toxicity assessment of invasive therapies and thorough monitoring during the treatment period to these with tinnitus of definite cause
Adequate protein, energy, and micronutrient supplementation to these with malnutrition
Optimizing the management of multi-morbidity
Optimal pre-operative risk assessment and thorough monitoring during the treatment period to these considering cochlear implant for severe-to-profound sensorineural hearing loss with poor word recognization
Drug treatment (e.g., betahistine) to increase cerebral blood flow; Other vasodilator and antivertiginous drugs
Subjective tinnitus intervention: amplification, sound, and neuromodulation
Optimizing environment and the improvement of health behavior
Reduction of polypharmacy
Optimal pre-operative risk and toxicity assessment of other invasive therapies and thorough monitoring during the treatment period to these with hearing loss of definite cause
Fall prevention, including regular physical and intellectual activities, nutritional supplement
Cognitive behavioral or comprehensive therapy to these with tinnitus disorder
Optimizing psychosocial resources to these with low mood and affective problems
Reduction of treatment burden, adverse event, and uncoordinated care
Cognitive behavior training to these with cognitive decline
Table 2.
The coordinated and personalized management of hearing loss with frailty phenotypes and multi-morbidity.
3.1. Non-invasive treatment of ARHL with different frailty phenotypes
The integrated and person-centered management includes ARHL, presbyastasis, tinnitus, frailty phenotypes, and multi-morbidity. The primary management is to improve unfavorable lifestyles, including smoking, alcohol consumption, physical inactivity, improper nutrition, and poor social, economical, and environmental conditions, and reduction of polypharmacy, including the number and the dosage, and these increase the risk for presbyastasis, delirium, cardiovascular disease, kidney, and ototoxicity. The non-invasive intervention for ARHL is to prescribe a hearing aid, which could significantly slow short- and long-term cognitive decline [57]. The management of presbyastasis includes the identification of risk factors and potentially curable causes, vestibular and balance rehabilitation, and drug treatment, such as H1-receptor agonist and H3-receptor anti-agonist (e.g., betahistine) and Other vasodilator and antivertiginous drugs, and fall prevention, including regular physical and intellectual activities with gradually increasing difficulty and nutritional supplement [25, 37]. Amplification by hearing aids acting as a masker by introducing more ambient noise also is used to relieve subjective tinnitus symptoms in some patients. Other non-invasive subjective tinnitus interventions include sound therapy, psychological therapies, neuromodulation, and combined therapy of these interventions [26, 27, 49, 58]. Psychological therapies, such as cognitive behavioral therapy, have been shown to improve quality of life and decrease depression for these with persistent and bothersome tinnitus, or tinnitus disorder [24, 59].
The interventions recommended by different international organizations to reverse or slow the progression of frailty include multi-component physical activity programs, adequate nutrition supplementation, and cognitive behavior training to improve physiological, psychological, and cognitive reserves [31, 32, 33, 34, 60]. The decline of physiological, psychological, and cognitive reserves also causes multi-morbidity, and the complex overlap of frailty and morbidity, physical and mental health disorders, and frailty and polypharmacy [61]. The management of multi-morbidity includes a proactive personalized assessment and care plan, which improves the quality of life by reducing treatment burden, adverse events, and unplanned or uncoordinated care [61]. Recently, the holistic and patient-centered hearing healthcare had been proposed, including the integrated management of hearing loss with diabetes, dementia, and other comorbidities [62].
3.2. Invasive treatment in ARHL with different frailty phenotypes
Invasive treatment includes surgery, radiotherapy, chemotherapy, and multi-modal therapy. Individuals with ARHL and different frailty phenotypes may need a cochlear implant due to severe-to-profound sensorineural hearing loss with poor word recognition. Geriatric patients with dizziness-related specific diseases, or objective tinnitus-related diseases, such as idiopathic intracranial hypertension, vascular tumors, and these with subjective tinnitus-related diseases, including Meniere’s disease, cholesteatoma, and otosclerosis, require complex surgery, and tinnitus-related Cerebellopontine angle tumor, acoustic neuroma, and skull base tumors require multi-modal therapy. Compared with younger patients, older people have higher surgery risk and radio- and chemotherapy toxicity. The prevalence of physical frailty in geriatric patients for elective surgery is over 10%, and individuals with physical frailty have more than two times higher risk of postoperative complications [63]. The frequent postoperative complications include death, delirium, extending stay in hospital, falls, functional deterioration, and poorer quality of life, apart from complications resulting from existing diseases such as acute coronary syndromes, stroke, thromboembolism, pneumonia, or other infections. Multi-morbidity and functional limitations are also indicated to be the main predictors of adverse prognosis and poorer tolerance of multi-modality therapy in geriatric patients with head and neck cancer [64]. However, direct evidence of adverse prognosis of the above treatments for ARHL and tinnitus with frailty phenotypes is absent. Cochlear implantation had been validated to slow cognitive decline and the progression of dementia [57, 65]. A previous study indicated that cochlear implant for older patients with frailty does not cause additional complications from existing diseases [66].
To balance the risk and benefit, the cooperation between an otolaryngologist and a geriatrician had been recommended to identify these high-risk patients and optimize the treatment with special surveillance during the treatment period [67]. A guideline for pre-operative assessment of geriatric patients had been proposed that comprehensive geriatric assessment, such as physical and mental health, daily and social function, frailty, and poly-pharmacotherapy, should be implemented during the diagnostic and therapeutic, and post-operative process [68]. The guideline is similar to our in-depth assessment of IC and frailty phenotypes. Identification of deficits in IC and frailty phenotype, and multi-morbidity in pre-operative assessment not only are used to make surgical decisions, and choose anesthesia techniques, peri-operative care, and nursing plans to minimize complications, but also allow for the patient’s pre-operative preparation through nutritional support, functional improvement, and rehabilitation, and excluding surgical contraindications.
4. To prevent secondary presbycusis in subjects with different frailty phenotypes
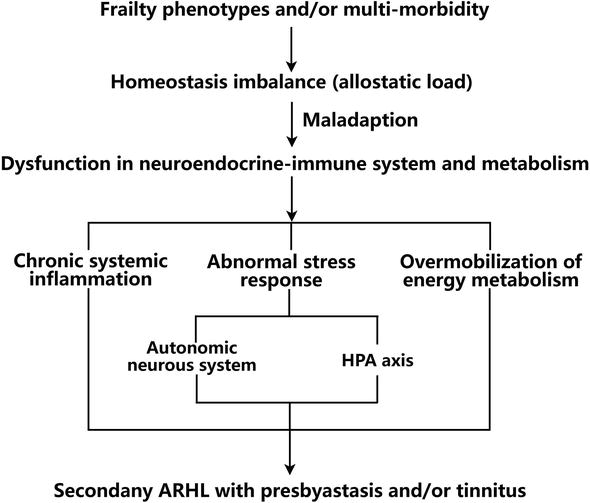
Individuals with frailty phenotypes, or more complex overlap of frailty, multi-morbidity, and polypharmacy, usually showed an imbalance of homeostasis to additional minor stressors. The long-term allostatic load results in dysfunction in the neuroendocrine-immune system and metabolism (Figure 2). The maladaptation of these regulation systems results in the decline of stress-responsive capacity of the HPA axis and autonomic nervous system, chronic systemic inflammation, and over mobilization of energy metabolism. All these systemic alterations might cause secondary ARHL, tinnitus, and other widespread functional impairment or health deficits [7].
Figure 2.
The secondary ARHL with presbyastasis and/or tinnitus in subjects with frailty phenotypes and multi-morbidity.
To improve IC capacity and decrease stress exposure are the basic principles for the management of these individuals. Multi-component physical activity programs, nutrition supplementation, and environmental enrichment can enhance the physical, cognitive [69], and auditory reserves [70]. The management of multi-morbidity and polypharmacy, optimal home, and psychosocial environment could slow the progress from frailty to disability, including secondary ARHL [32, 33, 34, 60].
5. Challenges of the detection and management of presbycusis with different frailty phenotypes
There are several critical challenges to optimize the diagnosis and management of presbycusis with different frailty phenotypes. One of the main challenges is frailty construct and screening instruments for clinical practice. Two well-validated and the most widely used models in clinical practice are variations of the frailty phenotype or frailty indexes based on the deficit accumulation approach [9]. However, most instruments lack extensive validation. Simple, rapid instruments for the assessment of frailty phenotypes based on physical frailty seem to meet the clinical translation demands. The evidence for frailty phenotypes, such as social frailty, nutritional frailty, and cognitive frailty, and subtypes, such as reversible and potential reversible cognitive frailty, is still limited.
Another main challenge is two parallel constructs with the same mission for healthy aging: IC and multi-morbidity. IC is endorsed by WHO but still lacks an operational definition, especially in the vitality domain [71]. Since many instruments are commonly used to diagnose frailty phenotypes and IC, it is necessary to integrate the two constructs and reduce confusion in clinical practice. Although frailty and multi-morbidity are different concepts, more than 16% of people have multi-morbidity with frailty and about three-quarters of people have frailty with multi-morbidity [72], it is difficult to separate different frailty phenotypes from comorbidities, such as cognitive frailty vs. cognitive impairment, and psychological frailty vs. psychological diseases.
There are similar challenges to differentiate peripheral from central ARHL, and tinnitus disorder from tinnitus with frailty phenotypes and multi-morbidity, especially with cognitive frailty or impairment, and psychological frailty or disorders. Therefore, further research is imperative to provide a more evidence-based proposal to improve the coordinated and personalized care to these with complex geriatric conditions.
The bidirectional association between ARHL and frailty phenotypes and multi-morbidity supports coordinated and personalized care for older people with ARHL and different frailty phenotypes. We proposed the rapid screening, in-depth assessment of IC, and frailty phenotypes as part of routine ARHL management. Albeit based predominantly on consensus and recommendation, we hope coordinated and personalized treatment strategies could be employed to reduce the complication and improve health and quality of life.
This work was supported by the Huadong Hospital project on intractable and complicated diseases (grant no. 20220101), the Medical Science and Technology Support Project of Shanghai Science, Technology Commission (grant No. 18411962200).
1.Agrawal Y, Platz EA, Niparko JK. Prevalence of hearing loss and differences by demographic characteristics among US adults: Data from the National Health and nutrition examination survey, 1999-2004. Archives of Internal Medicine. 2008;168(14):1522-1530. DOI: 10.1001/archinte.168.14.1522
2.Lin FR, Thorpe R, Gordon-Salant S, Ferrucci L. Hearing loss prevalence and risk factors among older aduStates. The Journals of Gerontology. Series A, Biological Sciences and Medical Sciences. 2011;66(5):582-590. DOI: 10.1093/gerona/glr002
3.Scholes S, Biddulph J, Davis A, Mindell JS. Socioeconomic differences in hearing among middle-aged and older adults: Cross-sectional analyses using the health survey for England. BMJ Open. 2018;8(2):e019615. DOI: 10.1136/bmjopen-2017-019615
4.Kricos PB. Audiologic management of older adults with hearing loss and compromised cognitive/psychoacoustic auditory processing capabilities. Trends in Amplification. 2006;10(1):1-28. DOI: 10.1177/108471380601000102
5.Jafari Z, Kolb BE, Mohajerani MH. Age-related hearing loss and tinnitus, dementia risk, and auditory amplification outcomes. Ageing Research Reviews. 2019;56:100963. DOI: 10.1016/j.arr.2019.100963
6.Knipper M, Van Dijk P, Nunes I, Rüttiger L, Zimmermann U. Advances in the neurobiology of hearing disorders: Recent developments regarding the basis of tinnitus and hyperacusis. Progress in Neurobiology. 2013;111:17-33. DOI: 10.1016/j.pneurobio.2013.08.002
7.Ruan J, Hu X, Liu Y, Han Z, Ruan Q. Vulnerability to chronic stress and the phenotypic heterogeneity of presbycusis with subjective tinnitus. Frontiers in Neuroscience. 2022;16:1046095. DOI: 10.3389/fnins.2022.1046095
8.Berge JE, Nordahl SHG, Aarstad HJ, Goplen FK. Hearing as an independent predictor of postural balance in 1075 patients evaluated for dizziness. Otolaryngology and Head and Neck Surgery. 2019;161(3):478-484
9.Hoogendijk EO, Afilalo J, Ensrud KE, Kowal P, Onder G, Fried LP. Frailty: Implications for clinical practice and public health. Lancet. 2019;394(10206):1365-1375. DOI: 10.1016/S0140-6736(19)31786-6
10.Ruan Q , Yu Z, Chen M, Bao Z, Li J, He W. Cognitive frailty, a novel target for the prevention of elderly dependency. Ageing Research Reviews. 2015;20:1-10. DOI: 10.1016/j.arr.2014.12.004
11.Tsutsumimoto K, Doi T, Makizako H, Hotta R, Nakakubo S, Makino K, et al. Association of social frailty with both cognitive and physical deficits among older people. Journal of the American Medical Directors Association. 2017;18(7):603-607. DOI: 10.1016/j.jamda.2017.02.004
12.Gobbens RJ, van Assen MA, Luijkx KG, Wijnen-Sponselee MT, Schols JM. The Tilburg frailty indicator: Psychometric properties. Journal of the American Medical Directors Association. 2010;11(5):344-355. DOI: 10.1016/j.jamda.2009.11.003
13.Solfrizzi V, Scafato E, Seripa D, Lozupone M, Imbimbo BP, D’Amato A, et al. Reversible cognitive frailty, dementia, and all-cause mortality. The Italian longitudinal study on aging. Journal of the American Medical Directors Association. 2017;18(1):89.e1-89.e8. DOI: 10.1016/j.jamda.2016.10.012
14.Zupo R, Castellana F, Guerra V, Donghia R, Bortone I, Griseta C, et al. Associations between nutritional frailty and 8-year all-cause mortality in older adults: The Salus in Apulia study. Journal of Internal Medicine. 2021;290(5):1071-1082. DOI: 10.1111/joim.13384
15.Collard RM, Boter H, Schoevers RA, Oude Voshaar RC. Prevalence of frailty in community-dwelling older persons: A systematic review. Journal of the American Geriatrics Society. 2012;60(8):1487-1492. DOI: 10.1111/j.1532-5415.2012.04054.x
16.Hoogendijk EO, Rijnhart JJM, Kowal P, Pérez-Zepeda MU, Cesari M, Abizanda P, et al. Socioeconomic inequalities in frailty among older adults in six low- and middle-income countries: Results from the WHO study on global ageing and adult health (SAGE). Maturitas. 2018;115:56-63. DOI: 10.1016/j.maturitas.2018.06.011
17.Ruan Q , Xiao F, Gong K, Zhang W, Zhang M, Ruan J, et al. Prevalence of cognitive frailty phenotypes and associated factors in a community-dwelling elderly population. The Journal of Nutrition, Health & Aging. 2020;24(2):172-180. DOI: 10.1007/s12603-019-1286-7
18.Ruan Q , Chen J, Zhang R, Zhang W, Ruan J, Zhang M, et al. Heterogeneous influence of frailty phenotypes in age-related hearing loss and tinnitus in Chinese older adults: An explorative study. Frontiers in Psychology. 2021;11:617610. DOI: 10.3389/fpsyg.2020.617610
19.Zhang W, Ruan J, Zhang R, Zhang M, Hu X, Han Z, et al. Association between age-related hearing loss with tinnitus and cognitive performance in older community-dwelling Chinese adults. Psychogeriatrics. 2022;22(6):822-832. DOI: 10.1111/psyg.12889
20.Zhang W, Ruan J, Zhang R, Zhang M, Hu X, Yu Z, et al. Age-related hearing loss with tinnitus and physical frailty influence the overall and domain-specific quality of life of Chinese community-dwelling older adults. Frontiers in Medicine (Lausanne). 2021;8:762556. DOI: 10.3389/fmed.2021.762556
21.Politi L, Salerni L, Bubbico L, Ferretti F, Carucci M, Rubegni G, et al. Risk of falls, vestibular multimodal processing, and multisensory integration decline in the elderly-predictive role of the functional head impulse test. Frontiers in Neurology. 2022;13:964017
22.McDermott JH, Molina-Ramírez LP, Bruce IA, Mahaveer A, Turner M, Miele G, et al. Diagnosing and preventing hearing loss in the genomic age. Trends in Hearing. 2019;23:2331216519878983. DOI: 10.1177/2331216519878983
23.Wiseman K, Sapp C, Walker E, McCreery R. Comprehensive audiological management of hearing loss in children, including mild and unilateral hearing loss. Otolaryngologic Clinics of North America. 2021;54(6):1171-1179. DOI: 10.1016/j.otc.2021.08.006
24.Lindeborg MM, Jung DH, Chan DK, Mitnick CD. Prevention and management of hearing loss in patients receiving ototoxic medications. Bulletin of the World Health Organization. 2022;100(12):789-796A. DOI: 10.2471/BLT.21.286823
25.Vaz GF. Disequilibrium and its management in elderly patients. The International Tinnitus Journal. 2009;15(1):83-90
26.Langguth B, Kreuzer PM, Kleinjung T, De Ridder D. Tinnitus: Causes and clinical management. Lancet Neurology. 2013;12(9):920-930. DOI: 10.1016/S1474-4422(13)70160-1
27.Wu V, Cooke B, Eitutis S, Simpson MTW, Beyea JA. Approach to tinnitus management. Canadian Family Physician. 2018;64(7):491-495
28.US Preventive Services Task Force, Krist AH, Davidson KW, Mangione CM, Cabana M, Caughey AB, et al. Screening for hearing loss in older adults: US preventive services task force recommendation statement. Journal of the American Medical Association. 2021;325(12):1196-1201. DOI: 10.1001/jama.2021.2566
29.Cesari M, Araujo de Carvalho I, Amuthavalli Thiyagarajan J, Cooper C, Martin FC, Reginster JY, et al. Evidence for the domains supporting the construct of intrinsic capacity. The Journals of Gerontology. Series A, Biological Sciences and Medical Sciences. 2018;73(12):1653-1660. DOI: 10.1093/gerona/gly011
30.WHO. Guidance for Person-Centred Assessment and Pathways in Primary Care. Geneva: World Health Organization; 2019
31.WHO. Integrated Care for Older People (ICOPE) Implementation Framework: Guidance for Systems and Services. Geneva: World Health Organization; 2019
32.Dent E, Lien C, Lim WS, Wong WC, Wong CH, Ng TP, et al. The Asia-Pacific clinical practice guidelines for the Management of Frailty. Journal of the American Medical Directors Association. 2017;18(7):564-575. DOI: 10.1016/j.jamda.2017.04.018
33.Ruiz JG, Dent E, Morley JE, Merchant RA, Beilby J, Beard J, et al. Screening for and managing the person with frailty in primary care: ICFSR consensus guidelines. The Journal of Nutrition, Health & Aging. 2020;24(9):920-927. DOI: 10.1007/s12603-020-1492-3
34.Dent E, Morley JE, Cruz-Jentoft AJ, Woodhouse L, Rodríguez-Mañas L, Fried LP, et al. Physical frailty: ICFSR international clinical practice guidelines for identification and management. The Journal of Nutrition, Health & Aging. 2019;23(9):771-787. DOI: 10.1007/s12603-019-1273-z
35.Chhetri JK, Harwood RH, Ma L, Michel JP, Chan P. Intrinsic capacity and healthy ageing. Age and Ageing. 2022;51(11):afac239. DOI: 10.1093/ageing/afac239
36.de Souto BP, Guyonnet S, Ader I, Andrieu S, Casteilla L, Davezac N, et al. The INSPIRE research initiative: A program for GeroScience and healthy aging research going from animal models to humans and the healthcare system. The Journal of Frailty & Aging. 2021;10(2):86-93. DOI: 10.14283/jfa.2020.18
37.Belal A Jr, Glorig A. Dysequilibrium of ageing (presbyastasis). The Journal of Laryngology and Otology. 1986;100(9):1037-1041
38.Lerchundi F, Laffue AH, Olivier M, Gualtieri FJ. Bilateral posterior semicircular canal dysfunction: A new finding with video head impulse test. Journal of Neurology. 2020;267(8):2347-2352
39.Borghi C, Brandolini C, Prandin MG, Dormi A, Modugno GC, Pirodda A. Prevalence of tinnitus in patients withhypertension and the impact of different anti hypertensive drugs on the incidence of tinnitus: A prospective, single-blind, observational study. Current Therapeutic Research, Clinical and Experimental. 2005;66(5):420-432. DOI: 10.1016/j.curtheres.2005.10.001
40.Salvi R, Radziwon K, Manohar S, Auerbach B, Ding D, Liu X, et al. Review: Neural mechanisms of tinnitus and Hyperacusis in acute drug-induced ototoxicity. American Journal of Audiology. 2021;30(3S):901-915. DOI: 10.1044/2020_AJA-20-00023
41.Sheppard A, Hayes SH, Chen GD, Ralli M, Salvi R. Review of salicylate-induced hearing loss, neurotoxicity, tinnitus and neuropathophysiology. Acta Otorhinolaryngologica Italica. 2014;34(2):79-93
42.National Guideline Centre (UK). Evidence Review for Questionnaires to Assess Tinnitus: Tinnitus: Assessment and Management: Evidence Review E. London: National Institute for Health and Care Excellence (NICE); 2020
43.Malmstrom TK, Voss VB, Cruz-Oliver DM, Cummings-Vaughn LA, Tumosa N, Grossberg GT, et al. The rapid cognitive screen (RCS): A point-of-care screening for dementia and mild cognitive impairment. The Journal of Nutrition, Health & Aging. 2015;19(7):741-744. DOI: 10.1007/s12603-015-0564-2
44.Clegg A, Rogers L, Young J. Diagnostic test accuracy of simple instruments for identifying frailty in community-dwelling older people: A systematic review. Age and Ageing. 2015;44(1):148-152. DOI: 10.1093/ageing/afu157
45.Gates GA, Beiser A, Rees TS, D'Agostino RB, Wolf PA. Central auditory dysfunction may precede the onset of clinical dementia in people with probable Alzheimer's disease. Journal of the American Geriatrics Society. 2002;50(3):482-488. DOI: 10.1046/j.1532-5415.2002.50114.x
46.Sardone R, Castellana F, Bortone I, Lampignano L, Zupo R, Lozupone M, et al. Association between central and peripheral age-related hearing loss and different frailty phenotypes in an older population in southern Italy. JAMA Otolaryngology. Head & Neck Surgery. 2021;147(6):561-571. DOI: 10.1001/jamaoto.2020.5334
47.World Health Organization. Global costs of unaddressed hearing loss and cost-effectiveness of interventions: a WHO report. 2017. [Accessed December 20, 2019]. Available from: https://apps.who.int/iris/bitstream/handle/10665/254659/9789241512046-eng.pdf
48.Cooper JC Jr, Gates GA. Hearing in the elderly--the Framingham cohort, 1983-1985: Part II. Prevalence of central auditory processing disorders. Ear and Hearing. 1991;12(5):304-311. DOI: 10.1097/00003446-199110000-00002
49.National Guideline Centre (UK). Tinnitus: Assessment and Management. London: National Institute for Health and Care Excellence (NICE); 2020
50.De Ridder D, Schlee W, Vanneste S, Londero A, Weisz N, et al. Tinnitus and tinnitus disorder: Theoretical and operational definitions (an international multidisciplinary proposal). Progress in Brain Research. 2021;260:1-25. DOI: 10.1016/bs.pbr.2020.12.002
51.Reiss M, Reiss G. Zur Problematik des pulsierenden Tinnitus [Pulsating tinnitus]. Wiener Klinische Wochenschrift. 2000;112(2):84-91
52.Thomas KR, Bangen KJ, Weigand AJ, Edmonds EC, Wong CG, Cooper S, et al. Alzheimer’s disease neuroimaging initiative. Objective subtle cognitive difficulties predict future amyloid accumulation and neurodegeneration. Neurology. 2020;94(4):e397-e406. DOI: 10.1212/WNL.0000000000008838
53.Ruan Q , Xiao F, Gong K, Zhang W, Zhang M, Ruan J, et al. Demographically corrected normative Z scores on the neuropsychological test battery in cognitively Normal older Chinese adults. Dementia and Geriatric Cognitive Disorders. 2020;49(4):375-383. DOI: 10.1159/000505618
54.Ruan Q , Zhang W, Ruan J, Chen J, Yu Z. Clinical and objective cognitive measures for the diagnosis of cognitive frailty subtypes: A comparative study. Frontiers in Psychology. 2021;12:603974. DOI: 10.3389/fpsyg.2021.603974
55.Linn MW, Sculthorpe WB, Evje M, Slater PH, Goodman SP. A social dysfunction rating scale. Journal of Psychiatric Research. 1969;6(4):299-306. DOI: 10.1016/0022-3956(69)90023-5
56.Chau J, Martin CR, Thompson DR, Chang AM, Woo J. Factor structure of the Chinese version of the geriatric depression scale. Psychology, Health & Medicine. 2006;11(1):48-59. DOI: 10.1080/13548500500093688
57.Yeo BSY, Song HJJMD, Toh EMS, Ng LS, Ho CSH, Ho R, et al. Association of Hearing Aids and Cochlear Implants with Cognitive Decline and dementia: A systematic review and meta-analysis. JAMA Neurology. 2023;80(2):134-141. DOI: 10.1001/jamaneurol.2022.4427
58.Ruan Q , Yu Z, Zhang W, Ruan J, Liu C, Zhang R. Cholinergic hypofunction in Presbycusis-related tinnitus with cognitive function impairment: Emerging hypotheses. Frontiers in Aging Neuroscience. 2018;10:98. DOI: 10.3389/fnagi.2018.00098
59.National Guideline Centre (UK). Evidence Review for Psychological Therapies: Tinnitus: Assessment and Management: Evidence Review L. London: National Institute for Health and Care Excellence (NICE); 2020 Mar
60.Dent E, Martin FC, Bergman H, Woo J, Romero-Ortuno R, Walston JD. Management of frailty: Opportunities, challenges, and future directions. Lancet. 2019;394(10206):1376-1386. DOI: 10.1016/S0140-6736(19)31785-4
61.Yarnall AJ, Sayer AA, Clegg A, Rockwood K, Parker S, Hindle JV. New horizons in multimorbidity in older adults. Age and Ageing. 2017;46(6):882-888. DOI: 10.1093/ageing/afx150
62.Maidment DW, Wallhagen MI, Dowd K, Mick P, Piker E, Spankovich C, et al. New horizons in holistic, person-centred health promotion for hearing healthcare. Age and Ageing. 2023;52(2):afad020. DOI: 10.1093/ageing/afad020
63.Makary MA, Segev DL, Pronovost PJ, Syin D, Bandeen-Roche K, Patel P, et al. Frailty as a predictor of surgical outcomes in older patients. Journal of the American College of Surgeons. 2010;210(6):901-908. DOI: 10.1016/j.jamcollsurg.2010.01.028
64.VanderWalde NA, Fleming M, Weiss J, Chera BS. Treatment of older patients with head and neck cancer: A review. The Oncologist. 2013;18(5):568-578. DOI: 10.1634/theoncologist.2012-0427 Epub 2013 May 1
65.Mosnier I, Vanier A, Bonnard D, Lina-Granade G, Truy E, Bordure P, et al. Long-term cognitive prognosis of profoundly deaf older adults after hearing rehabilitation using Cochlear implants. Journal of the American Geriatrics Society. 2018;66(8):1553-1561. DOI: 10.1111/jgs.15445
66.Gordon SA, Aylward A, Patel NS, Bowers C, Presson AP, Smith KR, et al. Does frailty or age increase the risk of postoperative complications following Cochlear implantation? OTO Open. 2021;5(3):2473974X211044084. DOI: 10.1177/2473974X211044084
67.Skalska A, Składzień J. Challenges of modern medicine - geriatric otolaryngology or the advantages of cooperation between an otolaryngologist and a geriatrician. Otolaryngologia Polska. 2018;73(1):1-5. DOI: 10.5604/01.3001.0012.7218
68.Chow WB, Rosenthal RA, Merkow RP, Ko CY, Esnaola NF, American College of Surgeons National Surgical Quality Improvement Program, et al. Optimal preoperative assessment of the geriatric surgical patient: A best practices guideline from the American College of Surgeons National Surgical Quality Improvement Program and the American Geriatrics Society. Journal of the American College of Surgeons. 2012;215(4):453-466. DOI: 10.1016/j.jamcollsurg
69.Leon M, Woo C. Environmental enrichment and successful aging. Frontiers in Behavioral Neuroscience. 2018;12:155. DOI: 10.3389/fnbeh.2018.00155
70.Skoe E, Kraus N. Musical training heightens auditory brainstem function during sensitive periods in development. Frontiers in Psychology. 2013;19(4):622. DOI: 10.3389/fpsyg.2013.00622
71.Bautmans I, Knoop V, Amuthavalli Thiyagarajan J, Maier AB, Beard JR, Freiberger E, et al. WHO working definition of vitality capacity for healthy longevity monitoring. The lancet. Healthy Longevity. 2022;3(11):e789-e796. DOI: 10.1016/S2666-7568(22)00200-8
72.Vetrano DL, Palmer K, Marengoni A, Marzetti E, Lattanzio F, Roller-Wirnsberger R, et al. Frailty and multimorbidity: A systematic review and meta-analysis. The Journals of Gerontology. Series A, Biological Sciences and Medical Sciences. 2019;74(5):659-666. DOI: 10.1093/gerona/gly110
Written By
Qingwei Ruan, Jian Ruan, Xiuhua Hu, Aiguo Liu and Zhuowei Yu
Submitted: 04 May 2023Reviewed: 11 June 2023Published: 04 July 2023
 Open access peer-reviewed chapter
Open access peer-reviewed chapter