 Open access peer-reviewed chapter
Open access peer-reviewed chapter
Abstract
Metabolic Bariatric Surgery (MBS) is increasingly gaining ground, given that it constitutes the most effective treatment of obesity and associated health problems, with enduring results and a well-documented safety profile. Nevertheless, certain issues may rise in the medium and long term. Among them, there is a heterogeneous group of complications under the umbrella term “post-bariatric hernia”, including internal hernias, abdominal wall hernias, and hiatal hernias. Internal hernias constitute the most studied category, but evidence on the other categories is not lacking. This chapter will attempt to cover diagnostic, treatment, and preventive aspects in the management of hernia post-MBS following a comprehensive, evidence-based approach. In brief, with regards to the prevention of internal hernias, suturing of all defects is strongly recommended for Roux-en-Y Gastric Bypass (RYGB), but the evidence is less clear when it comes to newer bypass procedures, such as One-Anastomosis/Mini Gastric Bypass (OAGB/MGB) and Single Anastomosis Duodenal-Ileal Bypass (SADI). As far as abdominal wall hernias are concerned, there is no clear evidence of the advantages of suture closure against non-closure. Finally, with respect to hiatal hernias post-MBS, the caveat rests in the documentation of de novo versus pre-existing hiatal hernia, which mandates meticulous preoperative evaluation of symptoms and potentially further endoscopic documentation.
Keywords
- bariatric surgery
- metabolic surgery
- internal hernia
- Petersen’s defect
- mesenteric defect
- Brolin’s space
- mesocolic defect
- trocar site hernia
- port site hernia
- incisional hernia
- hiatal hernia
- de novo hiatal hernia
1. Introduction
Metabolic bariatric surgery (MBS) is the most effective and sustainable treatment for obesity and associated health problems, such as type 2 diabetes mellitus [1, 2, 3, 4, 5, 6]. Most importantly, MBS has shown a favorable safety profile over time [7], even at the extremes of age [8, 9, 10], even during pandemic periods with high epidemiological burden [11], and even for patient groups that are traditionally considered as high perioperative risk [12].
Nevertheless, there is no surgery without complications, as such bariatric operations bear an overall mortality risk of 1% and are accompanied by a number of early and late complications [13, 14]. The most studied early complications are anastomotic or staple-line leaks and hemorrhage, whereas the most referenced medium-term and late complications are malnutrition following hypoabsorptive procedures, gastroesophageal reflux after sleeve gastrectomy, and anastomotic ulcers. Another cluster of complications following bariatric surgery falls into the umbrella term “hernia”. Hernia post-MBS can take several forms but may be summarized into three cardinal categories:
The pathophysiology underlying post-MBS hernia remains elusive, and only extrapolations can be made about this complex issue, including but not limited to factors such as disrupted healing; nutritional deficiencies; diabetes mellitus; chronic constipation; chronic or vigorous cough; tissue subluxation and connective tissue disorders; alterations in intra-abdominal pressure; creation of visceral space defects that naturally would not exist; altered peristalsis and disrupted bowel transit; neurohormonal, immunologic, and inflammatory mediators; genetic and epigenetic influences; and so forth [15].
Most importantly, patients with hernia post-MBS may present in acute distress and their condition may mandate immediate surgical exploration, with incarcerated internal hernia being the most striking example. Consequently, the subject of hernia post-MBS expands well beyond the scope of bariatric surgery and may concern the general surgeon [16, 17].
This chapter will attempt to clarify the diagnostic challenges, treatment modalities, and prevention strategies regarding hernia post-MBS in a comprehensive and evidence-based manner.
2. Internal hernia following metabolic bariatric surgery
Internal hernias constitute the most widely studied category of hernia post-MBS. Most surgeons are familiar with the term “Petersen’s defect”, but this constitutes only one of many potential sites of herniation following Roux-en-Y gastric bypass (RYGB) and bariatric surgery in general.
2.1 Epidemiology and pathophysiology of internal hernia post-RYGB
Beginning with the epidemiological features of Internal Hernia (IH) post-MBS, according to the literature 42–61% of all cases of Small Bowel Obstruction (SBO) after RYGB are due to IH. This may indicate a relative increase of small bowel obstruction with the establishment of laparoscopic versus open approach in bariatric surgery, which in turn leads to the formation of less adhesions and allows for greater mobility of the small bowel. The crude incidence of IH post-RYGB is 5%, ranging 0.3–6.2%, but the true incidence is hard to assess, for reasons of short-term follow-up and/or loss to follow-up. In a large review comprising 9527 patients after RYGB and covering a period of 8 years, Koppman et al. showed that the incidence of IH ranged from 0.3% for antecolic to 2.4% for retrocolic fashioning of the Roux limb [18]. Among them, there are two seminal studies with regards to sample size and study design. The first was authored by Higa et al. in 2003 and comprised 2000 RYGB patients over the period 1998–2001 [19]. There were 63 cases and 66 IH in total (3 cases had hernia in multiple sites), with the most common site of herniation being the transverse mesocolon (67%), followed by the jejunal mesentery (21%), and Petersen’s space (7.5%). The authors documented a progressive decline in the incidence of IH throughout the duration of this study. The second study by Paroz et al. included 607 patients who underwent RYGB between 1999 and 2006 [20]. There were 25 cases of IH, 2 immediate postoperative and 23 late. In contradistinction to the study of Higa et al., the authors of this study found a peak of IH incidence at 36 months and a mean time of presentation at 29 months postoperatively, followed by a progressive decline toward the end of the study at 72 months. Additionally, the most common site was the jejuno-jejunal window (56%), followed by Petersen’s space (27%), and mesocolic window (17%). By contrast to both of these studies, a more recent research showed that Petersen’s space is the most common site of IH (67.6%), followed by jejuno-jejunal window (24.3%), whereas multi-site hernia incidence was as high as 8.1% [21]. This indicates that not only is hernia post-MBS a heterogeneous topic, but there is inherent heterogeneity in the specific subcategories depending on each study period, which may reflect changes in surgical technique.
With regards to pathophysiology of IH, RYGB has been the most extensively studied bariatric operation because it entails a multitude of bowel loop mobilizations, dissections, and thus potential herniation sites, and also because it used to be the most commonly performed bariatric operation globally until recently [22]. The most common IH sites following RYGB include: 1) the
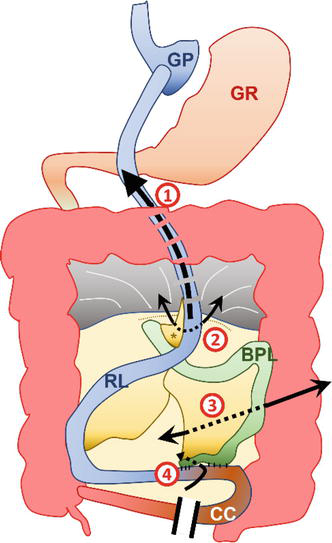
Figure 1.
Schematic representation of potential sites of internal herniation following Roux-en-Y gastric bypass. 1) Transmesocolic window. This potential site of internal herniation exists only if a transmesocolic Roux limb has been fashioned, which nowadays happens in the minority of the cases. 2) Petersen’s window (or retro-alimentary limb space) defined by the transverse mesocolon posteriorly (dotted line) and the mesojejunum (asterisk) of the Roux limb anteriorly. 3) Mesojejunal window (or Brolin’s space) defined by the mesojejunum of the biliopancreatic limb anteriorly and the mesojejunum of the Roux limb posteriorly. 4) Jejuno-jejunal window, between the Roux limb the biliopancreatic limb. For details, please refer to the text. GP – Gastric pouch; GR – Gastric remnant; RL – Roux limb; CC – Common channel. Vector graphic designed by Athanasios Pantelis.
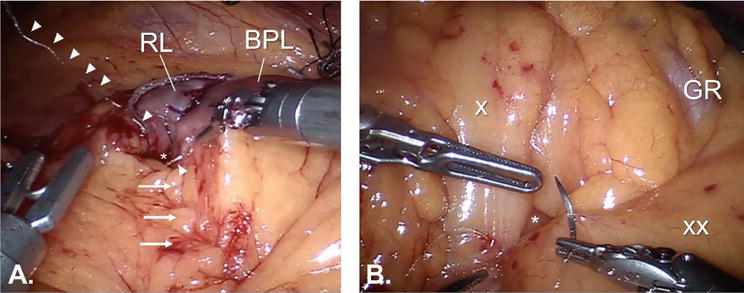
Figure 2.
Closure of internal defects in a case of robotic RYGB. A. Closure of the jejuno-jejunal defect (indicated by an asterisk), in continuity to closure of the mesojejunal defect (not clearly visible due to transparent suture material, trajectory indicated by arrows). The arrowheads indicate the course of the suture thread. RL – Roux limb; BPL – Biliopancreatic limb. B. Closure of Petersen’s defect (indicated by an asterisk). The symbol “x” indicates the mesentery of the Roux limb and the symbol “xx” indicates the transverse mesocolon. GR – Gastric remnant. Images courtesy of Dr. Mohit Bhandari, archives of Mohak bariatrics and robotics, Indore, MP, India.
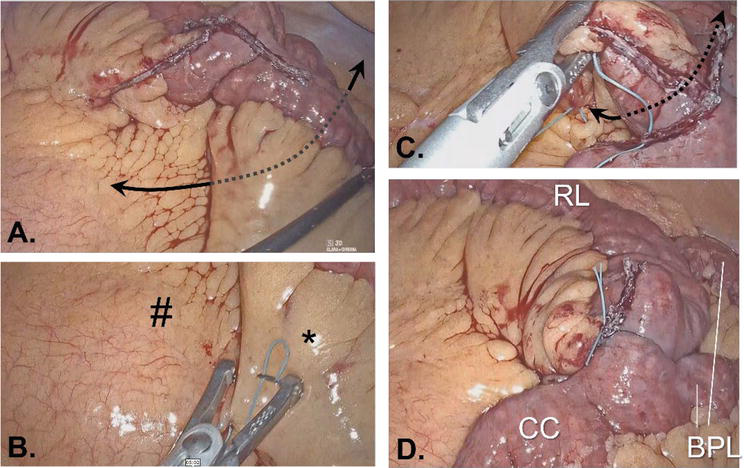
Figure 3.
The bariatric surgeon should be considerate of internal defects not only at primary operations, but also at reoperations. A case of type 1 biliopancreatic limb distalization due to weight regain following banded RYGB. A. the mesenteric defect. The principle of closing any potential site of internal herniation is common between primary and revisional bariatric surgery. B. the process of closing the defect with non-absorbable suture. The hashtag signifies the mesentery of the Roux limb, while the asterisk indicates the jejunal mesentery. C. the same suture is used in continuity in order to close the jejuno-jejunal defect created between the Roux limb and the biliopancreatic limb. D. the final picture after the closure of defects. RL – Roux limb; BPL – Biliopancreatic limb; CC – Common channel. Images courtesy of Dr. Mohit Bhandari, archives of Mohak bariatrics and robotics, Indore, MP, India.
2.2 Prevention of internal hernia following RYGB
Considering prevention, the two major areas of debate are the construction of the Roux limb in an antecolic versus retrocolic fashion, and the closure versus non-closure of the mesenteric defects. Currently, the trend is to create the Roux limb in an antecolic fashion and close all mesenteric defects. This was first supported in a meta-analysis of 45 articles by Geubbels et al., which included a cumulative number of 31,320 post-RYGB individuals [29]. IH with the antecolic approach without defect closure yielded a 95% CI of 0.02 [0.01–0.03] in the random-effects model (
The main advantages of an antecolic Roux (alimentary) limb are that there is one defect less in total and that the risk of mesocolic stenosis is non-existent. This comes at a cost of increased distance and increased tension at the gastro-jejunal anastomosis, which in turn may lead to a high incidence of leaks and strictures. However, fashioning an antecolic Roux limb may not be always technically feasible, especially in cases of short mesojejunum and thick mesocolon. In such cases, the creation of a transmesocolic window is mandatory and this essentially leads to one additional defect, which in turn potentially increases the relevant risks of IH and mesenteric stenosis [31]. Challenging this statement, in a large cohort of 1500 patients post-RYBG, Ribeiro-Parenti et al. compared antecolic versus retrocolic RYGB group and found that the latter had a significantly lower gastro-jejunal stricture rate, with no increased risk of IH, provided that the mesenteric defect was closed [32]. The risk for IH was greater for both groups in the first 4 postoperative months (maximum 4.5% in the antecolic group and < 1% in the retrocolic group), while the risk for gastro-jejunal stricture ranging approximately 25–35% for the antecolic group versus <15% in the retrocolic group, depending on the timing post-operatively. In total, there were 20 cases of IH in the antecolic group [12 without closure of defects (10.9%) and 8 with closure of all defects (1.7%)] and 11 cases in the retrocolic group (1.2%, all mesenteric defects closed in all cases). At a higher level of evidence, two meta-analyses have attempted to unravel the relationship between IH and positioning of the Roux limb. The first meta-analysis by Al Harakeh et al. included 4 studies in each group (antecolic vs. mesocolic), with 4805 vs. 2238 patients, respectively [31]. Mesenteric defects were closed in 45% of cases in each group. The antecolic group had an incidence of 1.4% regarding SBO vs. 5.2% in the retrocolic group (
The other hot topic on IH prevention is defect closure. In a recent study of 2093 RYGB cases, Amor et al. compared a cohort of 1676 patients who underwent defect closure (period: 2005–2013) with 421 historic controls without defect closure (period: 1998–2004) [34]. The former group comprised 13 IH cases versus 7 cases in the non-closure group (0.78% vs. 1.66%, respectively;
Given the variability of outcomes regarding IH post-RYGB, which is partly attributable to the large variation in IH definition, and in an attempt to homogenize data and reporting, two main classification systems have been developed [44]. The one is AMSTERDAM classification proposed by Geubbels et al. and is based on purely clinical criteria (presence of IH, presence of other pathology, remission of complains post-laparoscopy, etiology of symptoms) [45]. The other is the SDL (space - direction - limb) classification system, and, as indicated by the acronym, the criteria include predominantly anatomical definitions: P (Petersen’s) and/or B (Brolin’s) regarding space; L (right-to-left) or R (left-to-right) regarding direction; and A (alimentary), B (biliopancreatic), C (common channel), and/or E (entero-enterostomy/emergency), regarding limb [46]. A detailed analysis of these classification systems is beyond the scope of this chapter, nevertheless their implementation could benefit standardization and this in turn would result in research and practices of higher quality.
2.3 Diagnostic aspects
The diagnosis of IH post-RYGB is notoriously challenging, because the symptoms may be non-specific and the patient may have been experiencing them over a long period. A high index of suspicion should be kept in any post-bariatric patient, particularly during the first 1–3 years postoperatively and in cases of massive or excessive weight loss. Imaging studies may be helpful especially during exacerbations of symptoms. Even in this case, the differential between IH and adhesions may be difficult. Moreover, in up to 20% of patients with IH, imaging studies are non-diagnostic or even normal.
In the seminal study by Higa et al., the cases of frank bowel obstruction constituted 52.3% of IH cases, followed by non-specific abdominal pain (41.3%), whereas a striking 6.3% of patients were totally asymptomatic [19]. In the other seminal study by Paroz et al., all patients with IH had experienced colicky pains, both in the elective and in the acute setting, whereas only 20% had nausea and/or vomiting in the elective setting, in contrast to 50% of patients with IH presenting acutely [20]. In a more recent study, acute abdominal pain was the first manifestation of IH for 75.7% of patients, followed by chronic abdominal pain (16.2%), and ischemic bowel necrosis (8.1%) [21]. In a recent study by Tartamella et al., the clinical features that differed significantly between IH cases (IH) and positive controls (PC) were the quality of pain (colicky: IH 31%, PC 19%,
The clinician is advised to pay attention to details, as this may facilitate the origin of IH. Internal herniation of the biliopancreatic is expected to manifest as closed-loop syndrome, with a distended gastric remnant and possibly referred left shoulder pain secondary to irritation of the diaphragm, tachycardia, or eructation [44]. Conversely, obstruction of the alimentary (Roux) limb may lead to clinical presentation more typical of SBO (nausea, vomiting, retention of gas and feces). Laboratory tests should also be critically appraised, as an elevation of amylase or lipase (in the range of hundreds instead of thousands) may falsely direct diagnostic rationale toward pathologies of pancreatic or biliary origin [44].
Imaging with CT scan may be a useful adjunct in the diagnosis of IH. There is a constellation of eponymous and characteristic imaging findings:
Recently, a panel of experts issued a bundle of guidelines, based on the Operative management in Bariatric Acute Abdomen (OBA) Survey outcomes (the OBA guidelines) [48]. Most recommendations are based on low quality of evidence, nevertheless this is one of the first comprehensive attempts and could be utilized as a roadmap for future research and care pathways. According to the OBA guidelines, tachycardia ≥110 bpm, fever ≥38°C, hypotension, respiratory distress with tachypnea and hypoxia, and decreased urine output, altogether constitute alarming clinical signs in patients presenting with acute abdominal pain and a previous history of bariatric surgery. Additionally, persistent nausea and vomiting are alarming clinical signs for IH, volvulus, and gastrointestinal stenosis, among other entities. They also state that the most common clinical presentation of IH post-RYGB is acute onset, crampy/colicky epigastric pain. Besides, the triad of persistent epigastric pain, pregnancy, and a history of RYGB should prompt further evaluation for IH. Regarding lab investigations, there is no diagnostic biological marker, but high CRP and leukocytosis may serve as predictors of abdominal emergencies in general post-RYGB. Finally, the use of contrast-enhanced CT with oral contrast is strongly recommended, whenever possible and in suitable patients (i.e. non-pregnant, hemodynamically stable). Nevertheless, no investigation should delay surgical exploration in the presence of high index of suspicion and alarming clinical symptoms and signs, regardless of the findings of imaging studies.
2.4 Management
The cornerstones of treating IH after bariatric surgery are a high index of clinical suspicion based on a detailed history and prompt reduction of an incarcerated internal hernia before bowel ischemia settles in. It is also very important to determine which operation has been performed, because, for instance, RYGB is much more likely to be associated with IH as compared to sleeve gastrectomy.
A critical decision that the surgeon is called to make is the operative approach. In a cohort of 166 patients, Ianelli et al. reported laparoscopic access in 142 cases (85.5%) versus open in 24 cases (14.5%). Henceforth, the majority of published series of explorations for IH have implemented the laparoscopic approach. This is reflected in the recent OBA guidelines as well, which dictate exploratory laparoscopy in the first 24–48 hours in stable patients with abdominal pain and inconclusive clinical and radiological data [48]. Furthermore, exploration should proceed in a systematic distal-to-proximal fashion [ileo-cecal valve→ jejuno-jejunostomy→ mesojejunal space→ Petersen’s space→ transverse mesocolon (in cases of retrocolic RYGB)→ remnant stomach] [48]. If an IH is found, the next step should be the assessment of the viability of the involved bowel. In cases of ischemic necrosis, the least possible enterectomy should be undertaken, followed by anastomosis of well-perfused bowel ends. A useful adjunct for assessing the viability of the remnant bowel could be Indocyanine (ICG) Fluorescence Angiography, although the doses, timing, and routes of administration have not been standardized yet. Closure of all mesenteric defects with non-absorbable sutures (running or interrupted) is
The flowchart in Figure 4 summarizes the general principles of IH management following RYGB in the form of an algorithmic flowchart.
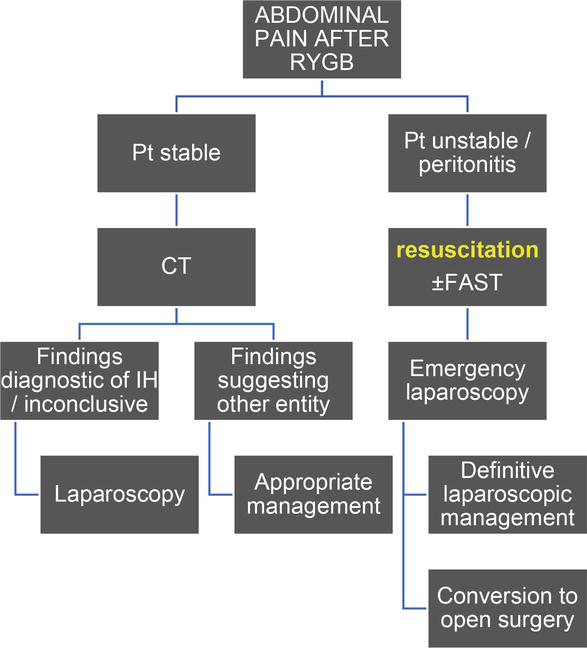
Figure 4.
A proposed algorithm outlining the principles for managing internal hernia after Roux-en-Y gastric bypass. Key: RYGB – Roux-en-Y gastric bypass; pt. – Patient; IH – Internal hernia; FAST – Focused assessment with sonography for trauma (bedside assessment for free intra-abdominal fluid).
2.5 Internal hernia following bariatric surgery other than RYGB
Although RYGB is the bariatric operation most associated with IH, it is not the only one. There have been reports of IH following Biliopancreatic Diversion with Duodenal Switch (BPD-DS), one-anastomosis/mini gastric bypass (OAGB/MGB), and single anastomosis duodeno-jejunostomy with sleeve (SADI-S). There have also been counter-intuitive associations of IH with bariatric operations such as Adjustable Gastric Band (LAGB) and Greater Curvature Plication (LGCP). Relevant reports are expected to multiply in the future, as new techniques arise and as the number of reoperations increases.
OAGB/MGB is a simplified version of RYGB, in the context of which one anastomosis (and consequently one defect) is spared. The first report of IH post-OAGB/MGB was published in 2016 [49]. In 2017, Carbajo, the inspirer of OAGB, reported an incidence of 0.26% regarding SBO and 0% regarding IH in his series of 1200 OAGB cases [50]. One year later, however, Kamal Mahawar stressed out that IH post-OAGB/MGB may be more common than previously reported [51]. Indeed, OAGB/MGB has less defects than RYGB, but Petersen’s hernia may occur. More recently, the analysis of a large series of 3368 consecutive OAGB patients yielded an incidence of IH as high as 2.8% [52]. This is particularly important, in view of the fact that OAGB/MGB is continuously gaining ground over RYGB as being technically more feasible, safer, and equally effective with regards to weight loss and remission of associated disease.
If OAGB is a simplified version of RYGB, then SADI-S is a simplified version of BPD-DS. Classical BPD-DS is nowadays performed rarely, because, despite its excellent bariatric outcomes, it was accompanied by a multitude of long-term complications principally owing to malabsorption and micronutrient deficiencies. However, it is not that rare for a surgeon to come across an old case of BPD-DS, or for a bariatric surgeon to implement BPD-DS as a revisional procedure for insufficient weight loss or weight regain. Summerhays et al. presented a case of IH after revisional laparoscopic loop DS [53]. The patient presented on the 64th postoperative day with mid- and left-sided abdominal pain and the CT scan revealed non-specific findings. Upon exploratory laparoscopy, the authors noted an 180o counterclockwise twist of the duodenal ileostomy, which caused rolling of the entire afferent limb underneath the anastomosis and over the right side of the abdominal cavity. More recently, Al-Tai et al. published a series of 121 DS operations (92 standard DS and 29 SADI-S) [54]. The incidence of IH was 5% (6 patients), all cases belonging to the group of standard DS with the mesenteric defects having been left open at the index operation.
IH after non-bypass procedures is even less common, but the incidence is not null. Hamed et al. gleaned the published literature of IH secondary to tubing problems, i.e. intestinal loops tangled around the gastric band, leading to IH, strangulation, and volvulus [55]. Besides, gastro-gastric herniation is a well-documented complication following LGCP [56, 57]. In this case, there is segmental herniation of the gastric wall between plication sutures secondary to increased intraluminal pressures. The take-home message is that IH may complicate any bariatric operation that may potentially lead to the creation of anatomic spaces.
3. Abdominal wall hernia complicating metabolic bariatric surgery
The main focus of this section shall be Trocar Site Hernias (TSH – Figure 5A). According to a meta-analysis of 22 studies, the pooled median prevalence of TSH after laparoscopic surgery is 0.5% (range 0–5.2%, 95% CI 0.3–0.9) [58]. Obesity itself is commonly considered a predisposing factor for TSH, but the evidence is conflicting [59, 60].
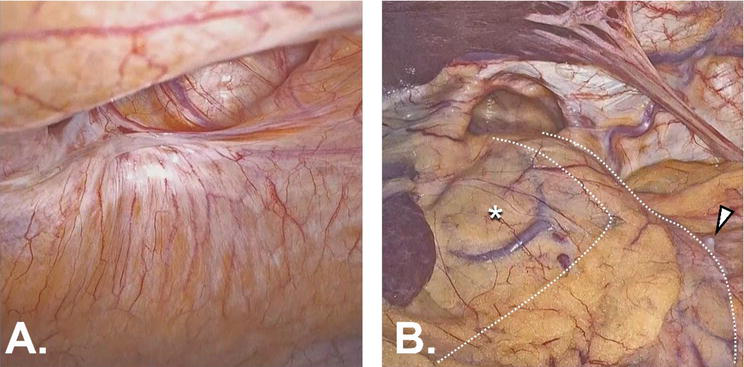
Figure 5.
A. a case of trocar site hernia (TSH) 1.5 year following single-incision sleeve gastrectomy (SILS-LSG). B. In the same patient, hiatal hernia (HH) was found incidentally during laparoscopy. This is considered a large defect of approximately 4 cm. Notably, the patient did not report any acid reflux symptoms preoperatively. Dashed lines indicate the contour of the gastric sleeve. The asterisk signifies the hepatogastric ligament, within which the course of left gastric vascular axis is clearly visible. The arrowhead points at a suture remnant that had been used to imbricate the staple line at the index operation.
TSH is a true yet underestimated complication after MBS, according to most authors. The first thing one needs to determine is the definition of TSH. Clinical symptoms may be feeble, vague, or even absent and clinical examination is notoriously misleading in post-bariatric individuals, for reasons of altered anatomical correlations, lipodystrophy of the subcutaneous adipose tissue, skin shagging, etc. In a recent study, Karampinis et al. attempted to systematize the diagnosis of TSH by means of Ultrasonography (USG), in a single-center cohort of 365 patients who had been operated over a 10-year period [61]. The incidence of TSH detected by USG in this series was 34%. Even though USG is a non-invasive, reproducible method without exposure to radiation, its implementation as a screening tool in this setting may lack cost-effectiveness and feasibility due to suboptimal adherence to follow-up on behalf of the patients. The same group of authors had performed a systematic review and meta-analysis one year earlier and found a pooled TSH incidence of 3.22% (range 0–39.2) among 68 studies that had met the inclusion criteria [62]. Overall, this evidence shows that THS may be much more common than originally thought.
Given the high incidence of TSH post-MBS and the sequelae this may potentially have, the area of debate that naturally follows is whether the trocar sites should be closed or not. Port site closure refers to fascial closure. In general, small port sizes are less likely to be associated with TSH. Conversely, according to a recent international Delphi consensus, the panel provided strong recommendation for closure of all 15 mm port sites and advised considering fascial closure for 10–12 mm ports [63]. Additionally, they recommended against drain placement through ≥10 mm sites, because this practice increases the risk of TSH after removal of the drain [63]. Beyond diameter, the type of trocars may also play its role. Bladeless trocars are thought to be associated with less risk of TSH compared to cutting ones, nevertheless there has been evidence that challenges this statement [64, 65]. Specifically regarding bariatric surgery, in a series of 624 procedures without fascial closure, Pilone et al. reported a TSH prevalence of 1.6% [66]. For LSG and BPD (totally 82 procedures) they used two 5 mm trocars and three 10–12 mm, whereas for LAGB (542 procedures) they used two 5 mm trocars, one 10–12 mm trocar, and one 15 mm trocar. Furthermore, in a meta-analysis of 36 relevant studies, the incidence for TSH after RYGB was 0.4% for fascial non-closure and 1.1% for closure (
Basta et al. developed a risk-stratification predictive model for TSH based upon 2161 bariatric operations with a total TSH incidence of 2.4% [68]. This study highlighted the following risk factors: open approach (hazard ratio [HR] = 10.3), malnutrition (HR = 3.10), prior abdominal surgery (HR = 2.89), and BMI >60 Kg/m2 (HR = 2.60). The patients were stratified into low-, moderate-, and high-risk accordingly. The incidence of TSH in the low-risk group was 0.6%, whereas the respective incidence in the high-risk group was 15.2%. Such models need further clinical validation, which will confirm their usefulness for preventing TSH as adjuncts in the decision-making process.
Among the factors predisposing to hernia, obesity has been recognized as one of the most consistent ones, resulting in an increased risk for both primary and incisional hernia [69]. A detailed reference to Abdominal Wall Hernia (AWH) repair in the context of MBS is beyond the scope of this chapter, nevertheless we shall provide a general outline for the purpose of comprehensively covering the topic of hernia post-MBS. According to a recent comprehensive review by Vilallonga et al., when obesity and AWH co-exist there are 3 options regarding operative strategy [70]:
First perform the MBS (with or without reduction of the hernia contents) and then proceed to AWH repair. Interestingly, the risk of SBO in case of reduction might be as high as 35.7% [71], whereas without reduction the respective risk is 0–5% [72].
First perform AWH repair and then proceed to MBS. Beyond the technical difficulties that this approach may present, there is also an increased risk of surgical site infection (2–26%) and recurrence (5.5–44.4%), depending on the timing of the bariatric operation.
Perform AWH repair and MBS simultaneously. The advantage of this single-stage approach is that the anesthetic risk is minimized. From a technical point of view, hernia repair in this context can be done in 3 different ways: If primary closure of the hernia defect is performed, the risk of SBO is 2.6%, while the risk of recurrence is as high as 25.7% [73]. If a synthetic mesh is applied, the risk of SBO minimizes to 0–0.6%, and this is also true regarding recurrence (0.6–6.6%) [74, 75]. Finally, if a biological mesh is implemented, the risk of SBO practically disappears, whereas the risk of recurrence is 14.3%.
According to a consensus joint statement issued by the American Society for Metabolic and Bariatric Surgery (ASMBS) and American Hernia Society (AHS) in 2018, management should depend on whether both obesity and AWH are amenable to laparoscopic repair [69]. If they are, then a combined approach is recommended, whereas if they are not, a staged approach is encouraged, where weight loss should take place before AWH repair, either surgically or non-operatively (very low/low-calorie diet, lifestyle modifications, pharmacotherapy, endoscopically). This will presumably render the patient fit for hernia repair surgery, while minimizing perioperative risk and optimizing postoperative outcomes at the same time. In any case, further research is necessary, given that relevant evidence is still weak, based primarily on retrospective study designs.
4. Hiatal hernia following metabolic bariatric surgery
Hiatal Hernia (HH) after MBS is the least studied category, and the main reason is the lack of concrete definition. One must be very careful when evaluating the incidence of HH after MBS, in that it should be clear whether HH pre-existed bariatric surgery or it is a true case of
4.1 Hiatal hernia and sleeve migration following sleeve gastrectomy
Saba et al. attempted to map the incidence of
An entity closely associated with HH, which is recognized with increasing frequency after LSG, is Intrathoracic (or trans-hiatal) Sleeve Migration (ITSM) [82, 83, 84]. Termine et al. published their experience with ITSM in a series of 1954 post-LSG patients with a minimum follow-up of 24 months [85]. The incidence of ITSM was 7% within a mean period of 24.16 ± 13.6 months. Patients with GERD due to ITSM who did not respond to conservative treatment were converted to RYGB with posterior cruroplasty (n = 15, 16%). Most importantly, surgeons are advised to keep a high index of suspicion, as this complication may present in the acute setting, in the immediate and short-term postoperative period (within 2 weeks of LSG) [84, 85, 86]. Clinical presentation may range from intolerance of oral intake, nausea, and vomiting to a dramatic symptomatology of gastric incarceration, with severe dehydration, electrolyte disturbances, and sepsis.
4.2 Hiatal hernia after Roux-en-Y gastric bypass
The evidence on HH post-RYGB is based on case reports and case series, among which the largest one includes 7 patients [87, 88, 89, 90]. In this context, HH constitutes a late complication, with patients presenting 2–14 years following the index RYGB procedure. Several mechanisms have been proposed to contribute to this condition, including rapid weight loss after MBS which is associated with relaxation of the phrenoesophageal ligament of Laimer and widening of the hiatus, creation of a large pouch with an ensuing higher intragastric pressure, extended dissection of the cardia and the left crus, or a small pre-existing hernia that enlarges over time [90, 91, 92].
4.3 Hiatal hernia after gastric banding
In the section of internal hernia (§ 2.5), we mentioned published cases of visceral entanglement around adjustable gastric bands. Another relevant complication of gastric banding is worth mentioning in this section, that of gastric necrosis due to paraesophageal (type II) hernia [93]. In this case report, it is not clear whether the gastric band was responsible for the herniation itself or contributed only to the inability of the stomach to resume its anatomical position within the abdominal cavity. In any case, no generalizations can be made on the basis of one case report. On the other hand, a high index of suspicion should be reserved in all post-bariatric patients, regardless of the specific type of operation.
5. Conclusions
Hernia after metabolic bariatric surgery is a heterogeneous group of complications. Based on bibliographic records, internal hernias are the most common. Regarding internal hernias, the closure of all defects after Roux-en-Y gastric bypass is highly recommended. With the advent of one-anastomosis gastric bypass the risk for internal herniation is lower but not null. For trocar site hernia prevention, fascial closure has not proven its advantage over non-closure. Lastly, regarding hiatal hernia, its documentation before any bariatric operation is of paramount importance, for this is the only way to distinguish between pre-existing and
Acknowledgments
Special thanks to Dr. Winnie Mathur for her valuable insight and for her suggestions regarding the Figures.
Special thanks to Ashish Rajvaidya for contributing substantially to this chapter with his skills in retrieval of cases and video editing.
References
- 1.
Martins C, Strømmen M, Stavne OA, Nossum R, Mårvik R, Kulseng B. Bariatric surgery versus lifestyle interventions for morbid obesity--changes in body weight, risk factors and comorbidities at 1 year. Obesity Surgery. 2011; 21 (7):841-849. DOI: 10.1007/s11695-010-0131-1 - 2.
Courcoulas AP et al. Three-year outcomes of bariatric surgery vs lifestyle intervention for type 2 diabetes mellitus treatment: A randomized clinical trial. JAMA Surgery. 2015; 150 (10):931-940. DOI: 10.1001/jamasurg.2015.1534 - 3.
Cummings DE et al. Gastric bypass surgery vs intensive lifestyle and medical intervention for type 2 diabetes: The CROSSROADS randomised controlled trial. Diabetologia. 2016; 59 (5):945-953. DOI: 10.1007/s00125-016-3903-x - 4.
Schauer PR et al. Bariatric surgery versus intensive medical therapy for diabetes — 5-year outcomes. The New England Journal of Medicine. 2017; 376 (7):641-651. DOI: 10.1056/NEJMoa1600869 - 5.
Courcoulas AP et al. Bariatric surgery vs lifestyle intervention for diabetes treatment: 5-year outcomes from a randomized trial. The Journal of Clinical Endocrinology and Metabolism. 2020; 105 (3):866-876. DOI: 10.1210/clinem/dgaa006 - 6.
Kirwan JP et al. Diabetes remission in the Alliance of randomized trials of medicine versus metabolic surgery in type 2 diabetes (ARMMS-T2D). Diabetes Care. 2022; 45 (7):1574-1583. DOI: 10.2337/dc21-2441 - 7.
Arterburn DE, Telem DA, Kushner RF, Courcoulas AP. Benefits and risks of bariatric surgery in adults: A review. JAMA. 2020; 324 (9):879-887. DOI: 10.1001/jama.2020.12567 - 8.
Goldberg I et al. Safety of bariatric surgery in patients older than 65 years. Surgery for Obesity and Related Diseases: Official Journal of the American Society for Metabolic and Bariatric Surgery. 2019; 15 (8):1380-1387. DOI: 10.1016/j.soard.2019.05.016 - 9.
Singhal R et al. 30-day morbidity and mortality of bariatric metabolic surgery in adolescence during the COVID-19 pandemic - the GENEVA study. Pediatric Obesity. 2021; 16 (12):e12832. DOI: 10.1111/ijpo.12832 - 10.
Singhal R et al. Safety of bariatric surgery in ≥ 65-year-old patients during the COVID-19 pandemic. Obesity Surgery. 2022; 32 (7):1-13. DOI: 10.1007/s11695-022-06067-z - 11.
Singhal R et al. 30-day morbidity and mortality of bariatric surgery during the COVID-19 pandemic: A multinational cohort study of 7704 patients from 42 countries. Obesity Surgery. 2021; 31 (10):4272-4288. DOI: 10.1007/s11695-021-05493-9 - 12.
Ruzieh M et al. Safety of bariatric surgery in patients with coronary artery disease. Surgery for Obesity and Related Diseases: Official Journal of the American Society for Metabolic and Bariatric Surgery. 2020; 16 (12):2031-2037. DOI: 10.1016/j.soard.2020.07.015 - 13.
Kassir R et al. Complications of bariatric surgery: Presentation and emergency management. International Journal of Surgery London England. 2016; 27 :77-81. DOI: 10.1016/j.ijsu.2016.01.067 - 14.
Chang S-H et al. Early major complications after bariatric surgery in the United States, 2003-2014: A systematic review and meta-analysis. Obesity Reviews: Official Journal of International Association Study Obesity. 2018; 19 (4):529-537. DOI: 10.1111/obr.12647 - 15.
Incisional Hernia: Pathogenesis and Clinical Findings | Calgary Guide. 2019. https://calgaryguide.ucalgary.ca/incisional-hernia-pathogenesis-and-clinical-findings/ [Accessed: February 14, 2023] - 16.
Healy P, Clarke C, Reynolds I, Arumugasamy M, McNamara D. ‘Complications of bariatric surgery- What the general surgeon needs to know’. The Surgeon: Journal of the Royal Colleges of Surgeons of Edinburgh. 2016; 14 (2):91-98. DOI: 10.1016/j. surge.2015.08.003 - 17.
Contival N, Menahem B, Gautier T, Le Roux Y, Alves A. Guiding the non-bariatric surgeon through complications of bariatric surgery. Journal of Visceral Surgery. 2018; 155 (1):27-40. DOI: 10.1016/j.jviscsurg.2017.10.012 - 18.
Koppman JS, Li C, Gandsas A. Small bowel obstruction after laparoscopic Roux-en-Y gastric bypass: A review of 9,527 patients. Journal of the American College of Surgeons. 2008; 206 (3):571-584. DOI: 10.1016/j.jamcollsurg.2007.10.008 - 19.
Higa KD, Ho T, Boone KB. Internal hernias after laparoscopic Roux-en-Y gastric bypass: Incidence, treatment and prevention. Obesity Surgery. 2003; 13 (3):350-354. DOI: 10.1381/096089203765887642 - 20.
Paroz A, Calmes JM, Giusti V, Suter M. Internal hernia after laparoscopic Roux-en-Y gastric bypass for morbid obesity: A continuous challenge in bariatric surgery. Obesity Surgery. 2006; 16 (11):1482-1487. DOI: 10.1381/096089206778870102 - 21.
Al-Mansour MR, Mundy R, Canoy JM, Dulaimy K, Kuhn JN, Romanelli J. Internal hernia after laparoscopic Antecolic Roux-en-Y gastric bypass. Obesity Surgery. 2015; 25 (11):2106-2111. DOI: 10.1007/s11695-015-1672-0 - 22.
Welbourn R et al. Bariatric-metabolic surgery utilisation in patients with and without diabetes: Data from the IFSO global registry 2015-2018. Obesity Surgery. 2021; 31 (6):2391-2400. DOI: 10.1007/s11695-021-05280-6 - 23.
O’Rourke RW. Management strategies for internal hernia after gastric bypass. Journal of Gastrointestinal Surgery: Official Journal of Society Surgery Alimentary Tract. 2011; 15 (6):1049-1054. DOI: 10.1007/s11605-010-1401-x - 24.
Kawkabani Marchini A et al. The four different types of internal hernia occurring after laparascopic Roux-en-Y gastric bypass performed for morbid obesity: Are there any multidetector computed tomography (MDCT) features permitting their distinction? Obesity Surgery. 2011; 21 (4):506-516. DOI: 10.1007/s11695-011-0364-7 - 25.
Paroz A, Calmes JM, Romy S, Giusti V, Suter M. A new type of internal hernia after laparoscopic Roux-en-Y gastric bypass. Obesity Surgery. 2009; 19 (4):527-530. DOI: 10.1007/s11695-008-9770-x - 26.
Dar R, Dola T, Sakran N. Biliopancreatic limb obstruction due to an unexpected variant of internal hernia after Roux-en-Y gastric bypass. Obesity Surgery. 2020; 30 (12):5184-5185. DOI: 10.1007/s11695-020-04992-5 - 27.
Elkbuli A, Santarone K, Kinslow K, McKenney M, Boneva D. A rare case of internal hernia, intussusception and volvulus following gastric bypass: A case report and literature review. International Journal of Surgery Case Reports. 2020; 67 :178-182. DOI: 10.1016/j.ijscr.2020.01.060 - 28.
Zheng X et al. Case report: An unusual complex internal hernia after Roux-en-Y gastric bypass. Obesity Surgery. 2021; 31 (4):1833-1835. DOI: 10.1007/s11695-020-05060-8 - 29.
Geubbels N, Lijftogt N, Fiocco M, van Leersum NJ, Wouters MWJM, de Brauw LM. Meta-analysis of internal herniation after gastric bypass surgery. The British Journal of Surgery. 2015; 102 (5):451-460. DOI: 10.1002/bjs.9738 - 30.
Vilallonga R. Internal hernia after bariatric surgery: A comprehensive review. Journal of Surgery Research and Practice. 2022; 3 (3):1-7. DOI: 10.46889/JSRP.2022.3302 - 31.
Al Harakeh AB, Kallies KJ, Borgert AJ, Kothari SN. Bowel obstruction rates in antecolic/antegastric versus retrocolic/retrogastric Roux limb gastric bypass: A meta-analysis. Surgery for Obesity and Related Diseases: Official Journal of the American Society for Metabolic and Bariatric Surgery. 2016; 12 (1):194-198. DOI: 10.1016/j.soard.2015.02.004 - 32.
Ribeiro-Parenti L, Arapis K, Chosidow D, Dumont J-L, Demetriou M, Marmuse J-P. Gastrojejunostomy stricture rate: Comparison between antecolic and retrocolic laparoscopic Roux-en-Y gastric bypass. Surgery for Obesity and Related Diseases: Official Journal of the American Society for Metabolic and Bariatric Surgery. 2015; 11 (5):1076-1084. DOI: 10.1016/j.soard.2015.01.019 - 33.
Rondelli F et al. Antecolic or Retrocolic alimentary limb in laparoscopic Roux-en-Y gastric bypass? A meta-analysis. Obesity Surgery. 2016; 26 (1):182-195. DOI: 10.1007/s11695-015-1918-x - 34.
Amor IB et al. Impact of mesenteric defect closure during laparoscopic Roux-en-Y gastric bypass (LRYGB): A retrospective study for a Total of 2093 LRYGB. Obesity Surgery. 2019; 29 (10):3342-3347. DOI: 10.1007/s11695-019-04000-5 - 35.
Blockhuys M, Gypen B, Heyman S, Valk J, van Sprundel F, Hendrickx L. Internal hernia after laparoscopic gastric bypass: Effect of closure of the Petersen defect - single-Center study. Obesity Surgery. 2019; 29 (1):70-75. DOI: 10.1007/s11695-018-3472-9 - 36.
Iannelli A, Sebastianelli L, Schneck A-S. Internal hernia and Roux-en-Y gastric bypass: Should the routine closure of defects still Be a matter of debate? Obesity Surgery. 2019; 29 (8):2614-2615. DOI: 10.1007/s11695-019-03846-z - 37.
Nuytens F et al. Closure of mesenteric defects is associated with a higher incidence of small bowel obstruction due to adhesions after laparoscopic antecolic Roux-en-y gastric bypass: A retrospective cohort study. International Journal of Surgery London England. 2019; 71 :149-155. DOI: 10.1016/j.ijsu.2019.09.017 - 38.
Al Motlaq AA, Al Saleh K. Commentary on: “Closure of mesenteric defects is associated with a higher incidence of small bowel obstruction due to adhesions after laparoscopic ante colic Roux-en-Y gastric bypass: A retrospective cohort study”. International Journal of Surgery London England. 2019; 72 :32-33. DOI: 10.1016/j.ijsu.2019.10.016 - 39.
Alkatary M. An invited commentary on “closure of mesenteric defects is associated with a higher incidence of small bowel obstruction due to adhesions after laparoscopic antecolic Roux-en-Y gastric bypass: A retrospective cohort study” (Int J Surg 2019; 17:149-155). International Journal of Surgery London England. 2020; 77 :119. DOI: 10.1016/j.ijsu.2020.03.011 - 40.
Gould L, Parmar C. A commentary on “closure of mesenteric defects is associated with a higher incidence of small bowel obstruction due to adhesions after laparoscopic antecolic Roux-en-y gastric bypass: A retrospective cohort study” (Int J Surg 2019 Oct. Epub ahead of print). International Journal of Surgery London England. 2019; 72 :55-56. DOI: 10.1016/j.ijsu.2019.10.011 - 41.
Sami S, Brown LR. Commentary: “Closure of mesenteric defects is associated with a higher incidence of small bowel obstruction due to adhesions after laparoscopic antecolic Roux-en-y gastric bypass”. International Journal of Surgery. 2019; 71 :174. DOI: 10.1016/j.ijsu.2019.10.005 - 42.
Lazaridis II, Köstler T, Kübler L, Zingg U, Delko T. Risk of reopening of the mesenteric defects after routine closure in laparoscopic Roux-en-Y gastric bypass: A single-Centre experience. Obesity Surgery. 2022; 32 (9):2853-2859. DOI: 10.1007/s11695-022-06179-6 - 43.
Aghajani E, Jacobsen HJ, Nergaard BJ, Hedenbro JL, Leifson BG, Gislason H. Internal hernia after gastric bypass: A new and simplified technique for laparoscopic primary closure of the mesenteric defects. Journal of Gastrointestinal Surgery. 2012; 16 (3):641-645. DOI: 10.1007/s11605-011-1790-5 - 44.
Pokala B, Giannopoulos S, Stefanidis D. Prevention and management of internal hernias after bariatric surgery: An expert review. Mini-Invasive Surgery. 2022; 6 :23. DOI: 10.20517/2574-1225.2021.136 - 45.
Geubbels N, Röell EA, Acherman YIZ, Bruin SC, van de Laar AWJM, de Brauw LM. Internal herniation after laparoscopic Roux-en-Y gastric bypass surgery: Pitfalls in diagnosing and the introduction of the AMSTERDAM classification. Obesity Surgery. 2016; 26 (8):1859-1866. DOI: 10.1007/s11695-015-2028-5 - 46.
Karcz WK et al. ‘Modification of internal hernia classification system after laparoscopic Roux-en-Y bariatric surgery’, Wideochirurgia Inne tech. Maloinwazyjne Videosurgery Miniinvasive Technology. 2015; 10 (2):197-204. DOI: 10.5114/wiitm.2015.52160 - 47.
Tartamella F et al. Abdominal pain and internal hernias after Roux-en-Y gastric bypass: Are we dealing with the tip of an iceberg? Acta Biomedica Atenei Parmensis. 2019; 90 (2):251-258. DOI: 10.23750/abm.v90i2.7145 - 48.
De Simone B et al. Operative management of acute abdomen after bariatric surgery in the emergency setting: The OBA guidelines. World Journal of Emerging Surgery WJES. 2022; 17 (1):51. DOI: 10.1186/s13017-022-00452-w - 49.
Kular KS et al. Petersen’s hernia after mini (one anastomosis) gastric bypass. Journal of Visceral Surgery. 2016; 153 (4):321. DOI: 10.1016/j.jviscsurg.2016.05.010 - 50.
Carbajo MA, Luque-de-León E, Jiménez JM, Ortiz-de-Solórzano J, Pérez-Miranda M, Castro-Alija MJ. Laparoscopic one-anastomosis gastric bypass: Technique, results, and long-term follow-up in 1200 patients. Obesity Surgery. 2017; 27 (5):1153-1167. DOI: 10.1007/s11695-016-2428-1 - 51.
Mahawar KK. Petersen’s hernia may be commoner after OAGB/MGB than previously reported. Obesity Surgery. 2018; 28 (1):257-258. DOI: 10.1007/s11695-017-3001-2 - 52.
Petrucciani N et al. Internal hernia after one anastomosis gastric bypass (OAGB): Lessons learned from a retrospective series of 3368 consecutive patients undergoing OAGB with a biliopancreatic limb of 150 cm. Obesity Surgery. 2021; 31 (6):2537-2544. DOI: 10.1007/s11695-021-05269-1 - 53.
Summerhays C, Cottam D, Cottam A. Internal hernia after revisional laparoscopic loop duodenal switch surgery. Surgery for Obesity and Related Diseases: Official Journal of the American Society for Metabolic and Bariatric Surgery. 2016; 12 (1):e13-e15. DOI: 10.1016/j.soard.2015.08.510 - 54.
Al-Tai SS, Axer SS, Hoffmann L. Internal hernia after duodenal switch. Surgery for Obesity and Related Diseases. 2018; 14 (11):S120. DOI: 10.1016/j.soard.2018.09.259 - 55.
Hamed OH, Simpson L, Lomenzo E, Kligman MD. Internal hernia due to adjustable gastric band tubing: Review of the literature and illustrative case video. Surgical Endoscopy. 2013; 27 (11):4378-4382. DOI: 10.1007/s00464-013-3024-2 - 56.
Hii M, Clarke N, Hopkins G. Gastrogastric herniation: An unusual complication following greater curve plication for the treatment of morbid obesity. Annals of the Royal College of Surgeons of England. 2012; 94 (2):e76-e78. DOI: 10.1308/003588412X13171221588695 - 57.
Chang P-C, Dev A, Katakwar A, Hsin M-C, Tai C-M, Huang C-K. Management of gastric fold herniation after laparoscopic adjustable gastric banded plication: A single-center experience. Surgery for Obesity and Related Diseases: Official Journal of the American Society for Metabolic and Bariatric Surgery. 2016; 12 (4):849-855. DOI: 10.1016/j.soard.2016.02.017 - 58.
Swank HA, Mulder IM, la Chapelle CF, Reitsma JB, Lange JF, Bemelman WA. Systematic review of trocar-site hernia. The British Journal of Surgery. 2012; 99 (3):315-323. DOI: 10.1002/bjs.7836 - 59.
Hy U et al. Trocar site hernia after laparoscopic cholecystectomy. Journal of Laparoendoscopic & Advanced Surgical Techniques. Part A. 2007; 17 (5):600-603. DOI: 10.1089/ lap.2006.0182 - 60.
Mayol J, Garcia-Aguilar J, Ortiz-Oshiro E, De-Diego Carmona JA, Fernandez-Represa JA. Risks of the minimal access approach for laparoscopic surgery: Multivariate analysis of morbidity related to umbilical trocar insertion. World Journal of Surgery. 1997; 21 (5):529-533. DOI: 10.1007/pl00012281 - 61.
Karampinis I et al. Trocar site HERnias after bariatric laparoscopic surgery (HERBALS): A prospective cohort study. Obesity Surgery. 2020; 30 (5):1820-1826. DOI: 10.1007/s11695-020-04400-y - 62.
Karampinis I et al. Trocar site hernias in bariatric surgery-an underestimated issue: A qualitative systematic review and meta-analysis. Obesity Surgery. 2019; 29 (3):1049-1057. DOI: 10.1007/s11695-018-03687-2 - 63.
Omar I et al. The first international Delphi consensus statement on laparoscopic gastrointestinal surgery. International Journal of Surgery London England. 2022; 104 :106766. DOI: 10.1016/j.ijsu.2022.106766 - 64.
Chiong E, Hegarty PK, Davis JW, Kamat AM, Pisters LL, Matin SF. Port-site hernias occurring after the use of bladeless radially expanding trocars. Urology. 2010; 75 (3):574-580. DOI: 10.1016/j.urology.2009.08.025 - 65.
Lee J, Zheng XJ, Ng CY. Trocar site hernias from using bladeless trocars: Should fascial closure be performed? Journal of Surgical Case Reports. 2014; 2014 (5):rju044. DOI: 10.1093/jscr/rju044 - 66.
Pilone V et al. Trocar site hernia after bariatric surgery: Our experience without fascial closure. International Journal of Surgery London England. 2014; 12 (Suppl 1):S83-S86. DOI: 10.1016/j.ijsu.2014.05.047 - 67.
Coblijn UK, de Raaff CAL, van Wagensveld BA, van Tets WF, de Castro SMM. Trocar port hernias after bariatric surgery. Obesity Surgery. 2016; 26 (3):546-551. DOI: 10.1007/s11695-015-1779-3 - 68.
Basta MN, Mirzabeigi MN, Shubinets V, Kelz RR, Williams NN, Fischer JP. Predicting incisional hernia after bariatric surgery: A risk stratification model based upon 2161 operations. Surgery for Obesity and Related Diseases: Official Journal of the American Society for Metabolic and Bariatric Surgery. 2016; 12 (8):1466-1473. DOI: 10.1016/j.soard.2016.03.022 - 69.
Menzo EL, Hinojosa M, Carbonell A, Krpata D, Carter J, Rogers AM. American Society for Metabolic and Bariatric Surgery and American hernia society consensus guideline on bariatric surgery and hernia surgery. Surgery for Obesity and Related Diseases: Official Journal of the American Society for Metabolic and Bariatric Surgery. 2018; 14 (9):1221-1232. DOI: 10.1016/j.soard.2018.07.005 - 70.
Vilallonga R et al. Abdominal Wall hernia and metabolic bariatric surgery. Journal of Laparoendoscopic & Advanced Surgical Techniques. Part A. 2020; 30 (8):891-895. DOI: 10.1089/lap.2020.0257 - 71.
Eid GM et al. Repair of ventral hernias in morbidly obese patients undergoing laparoscopic gastric bypass should not be deferred. Surgical Endoscopy. 2004; 18 (2):207-210. DOI: 10.1007/s00464-003-8915-1 - 72.
Datta T, Eid G, Nahmias N, Dallal RM. Management of ventral hernias during laparoscopic gastric bypass. Surgery for Obesity and Related Diseases: Official Journal of the American Society for Metabolic and Bariatric Surgery. 2008; 4 (6):754-757. DOI: 10.1016/j.soard.2008.03.246 - 73.
Lazzati A, Nassif GB, Paolino L. Concomitant ventral hernia repair and bariatric surgery: A systematic review. Obesity Surgery. 2018; 28 (9):2949-2955. DOI: 10.1007/s11695-018-3366-x - 74.
Praveen Raj P, Bhattacharya S, Saravana Kumar S, Parthasarathi R, Cumar B, Palanivelu C. Morbid obesity with ventral hernia: Is concomitant bariatric surgery with laparoscopic ventral hernia mesh repair the best approach? An experience of over 150 cases. Surgery for Obesity and Related Diseases: Official Journal of the American Society for Metabolic and Bariatric Surgery. 2019; 15 (7):1098-1103. DOI: 10.1016/j.soard.2019.04.027 - 75.
Marzouk AMSM, Ali HOE. Laparoscopic ventral hernia repair combined with sleeve gastrectomy in morbidly obese patients: Early outcomes. Surgery Journal (New York, N.Y.). 2019; 5 (3):e87-e91. DOI: 10.1055/s-0039-1694979 - 76.
Wilson LJ, Ma W, Hirschowitz BI. Association of obesity with hiatal hernia and esophagitis. The American Journal of Gastroenterology. 1999; 94 (10):2840-2844. DOI: 10.1111/j.1572-0241.1999.01426.x - 77.
Che F, Nguyen B, Cohen A, Nguyen NT. Prevalence of hiatal hernia in the morbidly obese. Surgery for Obesity and Related Diseases: Official Journal of the American Society for Metabolic and Bariatric Surgery. 2013; 9 (6):920-924. DOI: 10.1016/j.soard.2013.03.013 - 78.
Schneider R, Lazaridis I, Kraljević M, Beglinger C, Wölnerhanssen B, Peterli R. The impact of preoperative investigations on the management of bariatric patients; results of a cohort of more than 1200 cases. Surgery for Obesity and Related Diseases: Official Journal of the American Society for Metabolic and Bariatric Surgery. 2018; 14 (5):693-699. DOI: 10.1016/j.soard.2018.01.009 - 79.
Santonicola A et al. Hiatal hernia diagnosis prospectively assessed in obese patients before bariatric surgery: Accuracy of high-resolution manometry taking intraoperative diagnosis as reference standard. Surgical Endoscopy. 2020; 34 (3):1150-1156. DOI: 10.1007/s00464-019-06865-0 - 80.
Saba J, Bravo M, Rivas E, Fernández R, Pérez-Castilla A, Zajjur J. Incidence of de novo hiatal hernia after laparoscopic sleeve gastrectomy. Obesity Surgery. 2020; 30 (10):3730-3734. DOI: 10.1007/s11695-020-04742-7 - 81.
Almutairi BF, Aldulami AB, Yamani NM. Gastroesophageal reflux disease and hiatal hernia after laparoscopic sleeve gastrectomy: A retrospective cohort study. Cureus. 2022; 14 (3):e23024. DOI: 10.7759/cureus.23024 - 82.
Amor IB, Debs T, Kassir R, Anty R, Amor VB, Gugenheim J. De novo hiatal hernia of the gastric tube after sleeve gastrectomy. International Journal of Surgery Case Reports. 2015; 15 :78-80. DOI: 10.1016/j.ijscr.2015.08.029 - 83.
Alwatari Y, Roriz-Silva R, Bolckmans R, Campos GM. Intrathoracic sleeve gastrectomy migration with gastric volvulus treated with laparoscopic repair and conversion to gastric bypass. Journal of Surgical Case Reports. 2020; 2020 (8):rjaa234. DOI: 10.1093/jscr/rjaa234 - 84.
Meknat A, Fernandez-Ranvier G, Hariri K, Guevara DE, Beitner M, Herron DM. Intrathoracic sleeve migrations after sleeve gastrectomy: A compilation of case reports. Journal of Laparoendoscopic & Advanced Surgical Techniques. Part A. 2020; 30 (9):1013-1017. DOI: 10.1089/lap.2020.0237 - 85.
Termine P et al. Transhiatal migration after laparoscopic sleeve gastrectomy: Myth or reality? A Multicenter, retrospective study on the incidence and clinical impact. Obesity Surgery. 2021; 31 (8):3419-3426. DOI: 10.1007/s11695-021-05340-x - 86.
Pavelko Y, Bustos R, Gruessner S, Hassan C. Acute hiatal hernia with incarcerated proximal half of recent sleeve gastrectomy: Super rare complication. Obesity Surgery. 2021; 31 (1):469-471. DOI: 10.1007/s11695-020-05101-2 - 87.
Iannelli A, Kassir R, Schneck A-S, Martini F, Gugenheim J. Hiatal hernia of the Roux-en-Y gastric bypass pouch 8 years after surgery. Obesity Surgery. 2014; 24 (9):1494-1496. DOI: 10.1007/s11695-014-1360-5 - 88.
Clapp B et al. Late-term hiatal hernia after gastric bypass: An emerging problem. Surgery for Obesity and Related Diseases: Official Journal of the American Society for Metabolic and Bariatric Surgery. 2020; 16 (4):471-475. DOI: 10.1016/j.soard.2020.01.018 - 89.
Guglielmetti LC, Wyss R, Biraima M, Misirlic M, Peros G. Diaphragmatic hernia after laparoscopic gastric bypass surgery. Obesity Surgery. 2020; 30 (5):2069-2070. DOI: 10.1007/s11695-020-04495-3 - 90.
Thomopoulos T, FitzGerald M, Mantziari S, Demartines N, Suter M. Management of a Late-Term Hiatal Hernia with intrathoracic pouch migration after Roux-en-Y gastric bypass. Obesity Surgery. 2022; 32 (3):957-958. DOI: 10.1007/s11695-021-05881-1 - 91.
Griffith PS, Birch DW, Sharma AM, Karmali S. Managing complications associated with laparoscopic Roux-en-Y gastric bypass for morbid obesity. Canadian Journal of Surgery Journal of Canadian Chiropractic. 2012; 55 (5):329-336. DOI: 10.1503/cjs.002011 - 92.
Santonicola A, Angrisani L, Cutolo P, Formisano G, Iovino P. The effect of laparoscopic sleeve gastrectomy with or without hiatal hernia repair on gastroesophageal reflux disease in obese patients. Surgery for Obesity and Related Diseases: Official Journal of the American Society for Metabolic and Bariatric Surgery. 2014; 10 (2):250-255. DOI: 10.1016/j.soard.2013.09.006 - 93.
Oztürk A, Necati T, Faruk AÖ. Gastric necrosis due to type II paraesophageal hernia in obese patient with gastric band: Rescue sleeve gastrectomy. Surgery for Obesity and Related Diseases: Official Journal of the American Society for Metabolic and Bariatric Surgery. 2011; 7 (3):330-331. DOI: 10.1016/j.soard.2010.08.003