 Open access peer-reviewed chapter
Open access peer-reviewed chapter
Abstract
Inguinal hernias are a common clinical condition that is present to the surgical clinic and open inguinal hernias repairs are one of the most common operations that are performed by general surgeons. Open inguinal hernia repairs have evolved from tension repairs like the Bassini and darning repair to the shouldice repair. As these procedures were under tension and hence the recurrence rates were high. The Lichtenstein repair was a tension free repair that uses mesh, revolutionized hernia repair as the procedure was simple and the recurrence rates were low whether the procedure was performed by a junior or senior surgeon. The Lichtenstein repair is now the most popular repair for inguinal hernias. Variants to this include the plug and patch repair and the prolene hernia system, which uses various types of tension free mesh repairs. This chapter investigates the various open hernia techniques with emphasis on the tension free repairs which involve the use of mesh (Lichtenstein) and not the use of mesh (Desarda). The older tension repairs like the Shouldice and Bassini repairs are also reviewed.
Keywords
- open hernia repair
- Lichtenstein repair
- Desarda repair
- Shouldice repair
- Bassini repair
1. Introduction
Inguinal hernias are protrusions that occur through the inguinal canal, and they are classified as direct and indirect inguinal hernias. They are far more common in males than females. They can also be classified as reducible or irreducible inguinal hernias [1].
The treatment of inguinal hernias has always been surgical repair and they can be divided into open and laparoscopic repair. The open inguinal hernia repairs are further classified into (1) Tension free repair and (2) Tissue-suture repair [2].
The tension free repair operations are Lichtenstein’s tension free repair, the prolene hernia system repair and the plug, patch technique and the desarda technique. The tissue suture repair includes the Bassini’s repair, The Mcvay’s repair and the Shouldice repair [3].
The Lichtenstien tension free repair is the most common open hernia operation that is performed as it is associated with low recurrence rate, and it is reproducible by all non-specialist surgeons [4].
In choosing the technique of hernia repair will depend on the patient characteristics and the experience of the surgeon as well as understanding the evidence that is available to achieve the best outcome for the patient [5].
1.1 Lichtenstein tension free repair
This technique was introduced by lichtenstein in 1984 and it is the most popular open hernia technique because it does not require a long learning curve and it has a low recurrence and complication rate [6].
The Lichtenstein procedure involves the placement of a prolene mesh over the posterior wall of the inguinal canal and anchoring it to the inguinal ligament with non-absorbable sutures and slit is made to accommodate the cord and the upper edge of the mesh is anchored with non-absorbable sutures. Sakorafas et al. conducted a retrospective study on 540 patients who underwent the Lichtenstein procedure for hernia repair and there were no complications like wound infection and the recurrence rate was 0.2% [7].
The advantage of this procedure is that it can be performed under local anesthesia and hence it is cost effective. The placement of the mesh over the posterior wall of the inguinal canal and adjustments to the size of the mesh and suture technique has been associated with the reduced rates of post operative complications. Just et al. in their prospective study in 1592 patients who underwent the Lichtenstein repair confirmed this [8].
The prospective study by Yamamoto et al. which performed this repair on 314 patients and the results showed no mortality and decreased wound infection rate and they concluded that the lichtenstein repair can be safely performed by trainee surgeons with minimal complications [9].
Praviz et al. performed the lichtenstein hernia repair on 3480 patients with inguinal hernia and they were performed under local anesthesia. The postoperative wound infection rate was low, and the postoperative analgesia and recurrence was low and the stay in hospital and cost were low [10].
The Hernia surge group guidelines also concluded that the Lichtenstein tension free hernia repair is the preferred method of open hernia repair due to its low complications and recurrence rate [11].
Metzger et al. conducted a retrospective study on 440 patients who underwent inguinal hernia repair of which the Lichtenstein repair was the predominant repair, and the results showed this repair can be conducted as a daycare procedure as it is associated with reduced cost and post operative complications [12].
Alabi et al. conducted a systemic review on mesh fixation techniques in inguinal hernia. Twenty systemic reviews were included in the study and the conclusion was that glue fixation and non-suture fixation was associated with better outcomes with regards to recurrence and chronic pain when compared to suture fixation of mesh. Further randomized control trials with large sample sizes may be needed to further evaluate this [13].
Ladwa et al. also conducted a systemic review and meta-analysis comparing suture mesh fixation to glue mesh fixation. Seven trials including 1259 patients of which 628 underwent suture mesh repair and 653 underwent glue mesh fixation. The results showed there were no differences with regards to recurrence rates and chronic pain, but further randomized trials may be needed to further evaluate the effectiveness of glue mesh fixation [14].
The Lichtenstein repair was also compared with the plug mesh repair by Wilasrusmee et al. who performed at study on 94 patients with inguinal hernias of which 25 underwent the plug mesh repair, 26 underwent the Lichtenstein repair and 36 underwent the Bassani repair. There were no complication or recurrence rates in the plug mesh and Lichtenstein repair groups. This concluded that both the plug mesh and Lichtenstein repair were effective in the management of inguinal hernias [15].
Singh et al. also compared the Lichtenstein repair with the plug and patch mesh repair on 200 patients who underwent primary hernia repair. There were no differences in the duration of surgery, post operative infection rates and chronic pain, hence it concluded that both procedures were effective in the treatment of primary inguinal hernias [16].
The prolene hernia system uses a special mesh with a three-dimensional theoretical effect of strengthening and maintaining the anterior and posterior wall of the inguinal canal without tension. It consists of an underlay patch and overlay patch with an intervening connector. This procedure was associated with a shorter hospital stay and reduced post operative pain and is a viable alternative to the Lichtenstein procedure [17].
The use of the prolene hernia system in a regional hospital as demonstrated by Berende et al. in their retrospective study on 193 patients who underwent this type of hernia repair. The patients were followed up and the wound infection rates and recurrence rates were low demonstrating its use in non-hernia specific centers [18].
The Lichtenstein, prolene hernia system and the ultrapro hernia system were compared by a prospective randomized trial by Magnusson et al. in the management of primary inguinal hernias. Three hundred nine patients were involved in the study and the conclusion was that recurrence rates and chronic pain rates were the same in all the groups hence the Lichtenstein repair should be the first choice in the management of primary inguinal hernias [19].
The Plug and Patch technique which was popularized by Rudkow and Robbins involves a cone shaped plug made of polypropylene that is inserted into the inguinal canal in an indirect hernia and followed by placement of a mesh patch that is sewn over the spermatic cord and laid on top of the posterior wall. This repair was prospectively studied by Bringman et al. and it was associated with a recurrence rate that is equivalent to the Lichtenstein repair [20].
The conclusion from these studies is that the Lichtenstein hernia repair is a safe and effective treatment option for inguinal hernia (Figure 1).
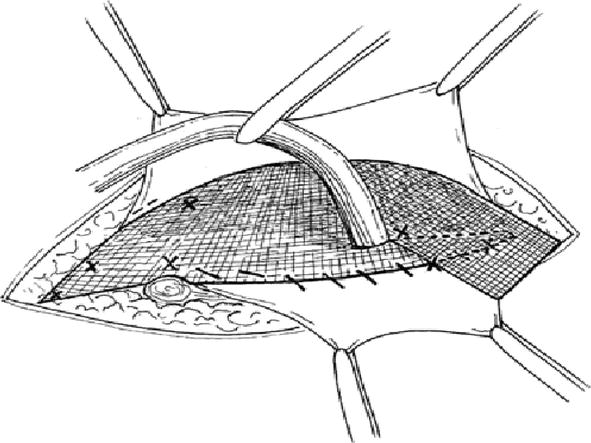
Figure 1.
The Lichtenstein repairs.
1.2 Desarda hernia repair
This procedure was introduced by Dr. M.P. Desarda in 2001 and he performed a hernia repair by strengthening the posterior wall by incising the external oblique aponeurosis and the undetached strip is sutured to the inguinal ligament to form a new posterior wall. This procedure does not use any foreign material like mesh and hence it has a decreased risk of wound infection and chronic pain. Desarda et al. performed a prospective study on 860 patients with inguinal hernias and all the patients underwent this type of hernia repair. The patients were followed up and there were no reported wound infection rates, and no recurrence were observed [21].
Desarda performed a further prospective study on 229 patients with this hernia repair and they were followed up and there were no reported recurrence or chronic groin pain with this hernia repair [22].
Gurgenidze et al. also performed a prospective study on 118 patients who underwent a desarda hernia repair for inguinal hernia. The patients were followed up and the wound infection rates were low and there was no recurrence. This showed that the Desarda hernia repair was good in the management of inguinal hernias [23].
Khairy et al. performed the desarda hernia repair on 100 patients with inguinal hernias. All the procedures were done under spinal anesthesia and there were no post operative complications like wound infection and seroma formation. There was also no recorded recurrence on follow up of these patients. This study showed the advantage of using the desarda hernia repair technique in the management of inguinal hernias [24].
Bashir et al. performed the desarda hernia technique on 50 patients with inguinal hernias. This was a prospective study, and the patients were followed up and there were no wound infection rates and there were also no recurrence rates. The conclusion from this study was that the desarda hernia repair was a safe and effective hernia repair technique [25].
Ge Hua et al. conducted a systemic review to compare the surgical outcomes of both the desarda repair and the Lichtenstein repair. Eight articles which included 4 randomized control trials and 4 nonrandomized control trials were included in the study. A total of 1014 patients of which 500 underwent the desarda repair and 514 underwent the Lichtenstein repair. The conclusion of this systemic review was that there was no difference in the surgical outcomes post operative wound infection, chronic pain, and recurrence rates. The limitation of this study was the small sample size and limited randomized control trials [26].
Pereira et al. also conducted a systematic review and meta-analysis on the desarda technique versus the Lichtenstein repair in the treatment of primary inguinal hernias, comparing both outcomes. Five randomized control trials including 536 patients were included in the study, 310 underwent the desarda repair and 226 underwent the Lichtenstein repair. The conclusion from this study showed that both procedures were comparable in terms of post operative infection rates and recurrence rates, but larger randomized control trials will be needed to evaluate the long-term outcomes of the desarda technique [27].
The conclusion from these studies is that the desarda technique is a good technique but further trials may be needed for further evaluation (Figure 2).
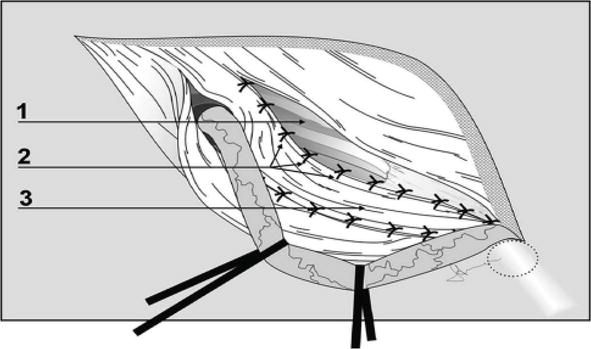
Figure 2.
Desarda hernia repair.
1.3 The shouldice repair
This repair was performed at the shouldice hospital, and it involves the division of the fascia transversalis and reconstruction of the posterior wall of the inguinal canal done with continuous stainless-steel sutures. Two continuous suture lines are used starting from the pubic crest and extending up to the transversalis fascia, transverses abdominus and internal oblique muscle. These sutures start from the pubic crest and advance towards the internal ring and the same sutures are reversed back towards the pubic crest including the shelving edge of the inguinal ligament. The second suture line begins laterally including the internal oblique and transversus muscle, extending medially, and including the inner line of the external oblique muscle and extending towards the pubic tubercle and then reverses back to the internal ring while picking up the inner aspect of the external oblique aponeurosis [28].
Amato et al. conducted a review to evaluate the efficacy of the shouldice repair against other open techniques of open repair. Sixteen trials were reviewed with 2566 shouldice repairs were done against 1121 mesh repairs and 1608 non mesh repairs. The conclusion of this review was that the shouldice repair was the best non mesh hernia repair, but recurrence rates were much lower in the mesh hernia repair group. Hence if mesh is not available, the shouldice repair is the best alternative for hernia repair [29].
Bracale et al. conducted a systemic review and network meta-analysis comparing the shouldice and desarda hernia repair in the treatment of primary hernia repairs. Fourteen randomized control trials involving 2791 patients and the conclusion of this study was that the recurrence rates were similar but the total operative time was reduced in the desarda group, hence the shouldice repair is still considered the best non-mesh hernia repair but the desarda repair is slowly emerging as an alternative non-mesh hernia repair [30].
Hay et al. conducted a multicentric trial on 1578 patients who underwent the shouldice repair for primary inguinal hernias. The patients were followed up to 5 years and the mean recurrence rate was 5% and the post operative infection rates were negligible. This showed that the shouldice repair is considered the best non mesh inguinal hernia repair (Figure 3) [31].
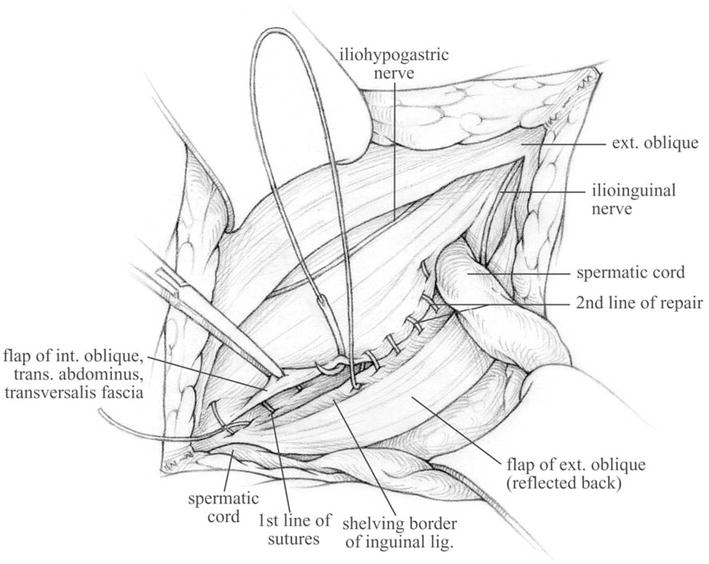
Figure 3.
The shouldice repair.
1.4 Other hernia repairs
The Bassini hernia repair has long been regarded as the first inguinal hernia repair, it involves suturing the transversalis fascia and conjoint tendon to the inguinal ligament behind the spermatic cord and is frequently associated with a tanner slide (vertical relaxing incisions over the anterior rectus sheath). This procedure was the most popular procedure before the introduction of tension free repair with mesh. Its main indication now is for primary inguinal hernia repair in patients who do not want to use mesh. Wayne et al. in their study on the use of the bassini repair in the treatment of inguinal hernias showed a recurrence rate of 3.7% to 4.8%, but they are much higher than the Lichtenstein repair. Another downside of this procedure is the need to avoid excessive tension over the inguinal region by not lifting heavy objects [32, 33].
The darning technique is another operation that is performed for primary inguinal hernias, and it involves the approximation of the conjoint tendon to the inguinal ligament with monofilament nylon from the pubic tubercle to the internal ring and back to the pubicle tubercle with forcibly bringing the tissues together. This procedure is relative tension free tissue repair with studies done by Olalekan et al. which showed a recurrence rate of 1.5% [34].
The advantage of the darning technique is the cost and early recovery, but the recurrence rate is still higher when compared with the Lichtenstein repair as demonstrated by the prospective clinical trial that was conducted by boonnithi et al. [35].
The Lotheissen/McVay repair is a tissue repair which is complex and rarely performed nowadays. The repair involves the splitting of the transversalis fascia and dissecting the cooper ligament. The hernia is repaired by suturing the transversalis fascia, transverses abdominus and internal oblique to the pectineal ligament (Figure 4) [36].
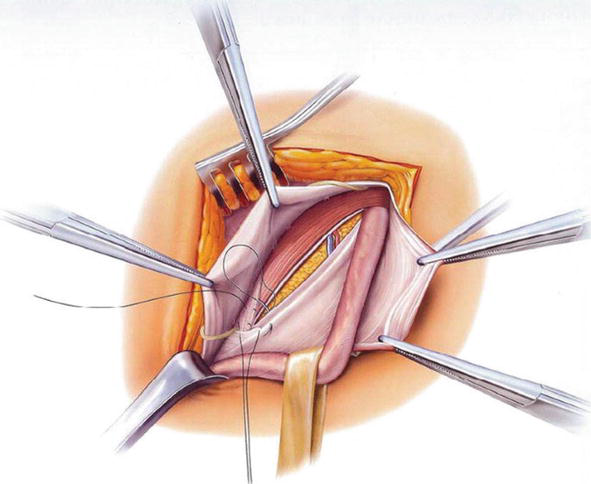
Figure 4.
The Bassini inguinal hernia repair.
2. Conclusion
Open inguinal hernia repair has evolved over time from pure tissue-based repair to mesh repair. The introduction of the tension free Lichtenstein repair with its low recurrence rate and low cost of operation has revolutionized the management of inguinal hernia repair and has become the most common open inguinal hernia repair. The Lichtenstein repair is easy to learn for junior surgeons and can be applied in various settings. It has replaced all tissue-based repair. The shouldice repair is the open tissue based inguinal hernia repair that is associated with the lowest recurrence rate and is indicated in patients where insertion of mesh is contraindicated. The Desarda repair is slowly emerging as an alternative for tension free inguinal hernia repair, but more studies are required to evaluate its recurrence rate. The Lichtenstein repair continues to be the most popular open inguinal hernia operation that is being performed worldwide as it can be performed under local anesthesia and hence be able to reduce the cost of the procedure. It is for this reason that open inguinal hernia repairs will continue to be a common surgical procedure that is being performed by general surgeons.
References
- 1.
Wib O, Ge N. Inguinal hernia. A review. Journal of Surgery and Operative Care. 2016; 1 (2):1-10 - 2.
Kulacoglu H. Current options in inguinal hernia repair in adult patients. Hippokratia. 2011; 15 (3):223-231 - 3.
Ismaila BO, Alayande BT, Ojo EO, Sule AZ. Inguinal hernia repair in Nigeria: A survey of surgical trainees. Hernia. 2019; 23 (3):625-629. DOI: 10.1007/s10029-019-01885-0. Epub 2019 Jan 17 - 4.
Jenkins JT, O’Dwyer PJ. Inguinal hernias. BMJ. 2008; 336 :269-272 - 5.
Kah, Heng Chiow A, Keong Chong C, Tan SM. Inguinal hernias: A current review of an old problem. Proceedings of Singapore Healthcare. 2010; 19 :202-211 - 6.
Campanelli G, Canziani M, Frattini F, Cavalli M, Agrusti S. Inguinal hernia: State of the art. International Journal of Surgery. 2008; 6 (Suppl. 1):526-528 - 7.
Sakorafas GH, Halikias I, Nissotakis C, Kotsifopoulos N, Stavrou A, Antonopoulos C, et al. Open tension free repair of inguinal hernias; the Lichtenstein technique [Internet]. 2001. Available from: http://www.biomedcentral.com/1471-2482/1/3 - 8.
Just E, Botet X, Martínez S, Escolà D, Moreno I, Duque E. Reduction of the complication rate in Liechtenstein hernia repair. International Journal of Surgery. 2010; 8 (6):462-465 - 9.
Yamamoto S, Maeda T, Uchida Y, Yabe SI, Nakano M, Sakano S, et al. Open tension-free mesh repair for adult inguinal hernia: Eight years of experience in a community hospital. Asian Journal of Surgery. 2002; 25 (2):121-125 - 10.
Amid PK. Lichtenstein tension-free hernioplasty: Its inception, evolution, and principles. Hernia. 2004; 8 (1):1-7. DOI: 10.1007/s10029-003-0160-y. Epub 2003 Sep 20 - 11.
Tran H. Endorsement of the HerniaSurge guidelines by the Australasian hernia society. In: Hernia. Vol. 22. France: Springer-Verlag; 2018. p. 177 - 12.
Metzger J, Lutz N, Laidlaw I. Guidelines for inguinal hernia repair in everyday practice. Annals of the Royal College of Surgeons of England. 2001; 83 :209-212 - 13.
Alabi A, Haladu N, Scott NW, Imamura M, Ahmed I, Ramsay G, et al. Mesh fixation techniques for inguinal hernia repair: An overview of systematic reviews of randomised controlled trials. Hernia. Springer-Verlag Italia s.r.l. Aug 2022; 26 (4):973-987 - 14.
Ladwa N, Sajid MS, Sains P, Baig MK. Suture mesh fixation versus glue mesh fixation in open inguinal hernia repair: A systematic review and meta-analysis. International Journal of Surgery. 2013; 11 :128-135 - 15.
Horharin P, Wilasrusmee C, Cherudchayaporn K, Pinyaku N, Phanpradi O, Phromsopha N. Comparative study of tailor-made mesh plug herniorrhaphy versus lichtenstein herniorrhaphy versus bassini operation: A prospective clinical trial. Asian Journal of Surgery. 2006; 29 (2):74-78 - 16.
Singh R, Gupta A, Shah A, Singh A. A study about inguinal hernia mesh repairs: Plug and patch versus lichtenstein mesh repair technique. International Surgery Journal. Nov 2016; 3 (4):1967-1974 - 17.
Gilbert AI, Graham MF, Voigt WJ. A bilayer patch device for inguinal hernia repair. Hernia. 1999; 3 (3):161-166 - 18.
Berende CAS, Ruurda JP, Hazenberg CEVB, Olsman JG, Geffen HJAA. Inguinal hernia treatment with the Prolene hernia system in a Dutch regional training hospital. Hernia. 2007; 11 (4):303-306 - 19.
Magnusson J, Nygren J, Thorell A. Lichtenstein, Prolene hernia system, and UltraPro hernia system for primary inguinal hernia repair: One-year outcome of a prospective randomized controlled trial. Hernia. 2012; 16 (3):277-285 - 20.
Bringman S, Ramel S, Nyberg B, Anderberg B. Introduction of Herniorraphy with Mesh Plug and Patch [Internet]. 2000. Available from: https://academic.oup.com/ejs/article/166/4/310/6040444 - 21.
Desarda MP. Physiological repair of inguinal hernia: A new technique (study of 860 patients). Hernia. 2006; 10 (2):143-146. DOI: 10.1007/s10029-005-0039-1. Epub 2005 Dec 9 - 22.
Desarda MP. No-mesh inguinal hernia repair with continuous absorbable sutures: A dream or reality? (a study of 229 patients). Saudi Journal of Gastroenterology. 2008; 14 (3):122-127. DOI: 10.4103/1319-3767.41730 - 23.
Gurgenidze M, Datuashvili G. Desarda technique for inguinal hernia repair. Georgian Medical News. Jul-Aug 2018; 280-281 :7-10 - 24.
Khairy M, Madbouly AEW, Sharaf M. Evaluation of Desarda technique in inguinal Herniorrhaphy. Al-Azhar International Medical Journal. 2020; 1 (2):193-197 - 25.
Bashir S, Afzal MO, Rafi Y. Desarda Technique for Inguinal Hernia Repair, a multicenter experience. 2016; 9 :311-313 - 26.
Ge H, Liang C, Xu Y, Ren S, Wu J. Desarda versus Lichtenstein technique for the treatment of primary inguinal hernia: A systematic review. International Journal of Surgery. Elsevier Ltd. 2018; 50 :22-27 - 27.
Pereira C, Varghese B. Desarda non-mesh technique versus Lichtenstein technique for the treatment of primary inguinal hernias: A systematic review and meta-analysis. Pereira Cureus. 18 Nov 2022; 14 (11) - 28.
Bendavid R. The Shouldice technique: A canon in hernia repair. Canadian Journal of Surgery. 1997; 40 (3):199-205 207 - 29.
Amato B, Moja L, Panico S, Persico G, Rispoli C, Rocco N, et al. Shouldice technique versus other open techniques for inguinal hernia repair. Cochrane Database of Systemic Reviews. 18 Apr 2012; 2012 (4):CD001543 - 30.
Bracale U, Melillo P, Piaggio D, Pecchia L, Cuccurullo D, Milone M, et al. Is Shouldice the best NON-MESH inguinal hernia repair technique? A systematic review and network metanalysis of randomized controlled trials comparing Shouldice and Desarda. International Journal of Surgery. 2019; 62 :12-21 - 31.
Hay JM, Boudet MJ, Fingerhut A, Pourcher J, Hennet H, Habib E, et al. S L E N Shouldice inguinal hernia repair in the male adult: The gold standard? A multicenter controlled trial in 1578 patients. Annals of Surgery. Dec 1995; 222 (6):719-727 - 32.
Naveen N, Srinath R. A comparative study between modified bassini’s repair and lichtenstein mesh repair of inguinal hernias in rural population. Journal of Clinical and Diagnostic Research. 2014; 8 (2):88-91 - 33.
Tse W, Johns W, Maher J, Rivers J, Miller T. Bassini inguinal hernia repair: Obsolete or still a viable surgical option? A single center cohort study. International Journal of Surgery Open. 2021:36 - 34.
Oo O, Oa A, Aa E, Ce A, Ak O, Om A. A 5-year review of darning technique of inguinal hernia repair. Nigerian Journal of Surgery. 2015; 21 (1):52 - 35.
Boonnithi N, Kongkham K. A prospective clinical trial comparing darn vs Bassini vs Lichtenstein inguinal Herniorrhaphy. The Thai Journal of Surgery. 2010; 31 :125-129 - 36.
Junge K. Lotheissen/McVay Repair [Internet]. 2019. Available from: https://www.ebsco.com/terms-of-use