Open Access is an initiative that aims to make scientific research freely available to all. To date our community has made over 100 million downloads. It’s based on principles of collaboration, unobstructed discovery, and, most importantly, scientific progression. As PhD students, we found it difficult to access the research we needed, so we decided to create a new Open Access publisher that levels the playing field for scientists across the world. How? By making research easy to access, and puts the academic needs of the researchers before the business interests of publishers.
We are a community of more than 103,000 authors and editors from 3,291 institutions spanning 160 countries, including Nobel Prize winners and some of the world’s most-cited researchers. Publishing on IntechOpen allows authors to earn citations and find new collaborators, meaning more people see your work not only from your own field of study, but from other related fields too.
To purchase hard copies of this book, please contact the representative in India:
CBS Publishers & Distributors Pvt. Ltd.
www.cbspd.com
|
customercare@cbspd.com
Large-scale chronic arsenic poisoning in several areas worldwide has not been eradicated. Adverse health effects of inorganic arsenic (iAs) exposure are associated with decreased arsenic methylation capacity (AMC). The AMC results from 21 children and 39 adults with acute arsenic poisoning support and effectively guide the analysis and evaluation of AMC in chronic arsenic poisoning. Results of the 65th-year follow-up for 6223 cases of infants, who survived subacute arsenic poisoning, contribute to future projections against health effects (cancer and cognitive dysfunction). Currently, arsenolipids from fish and shellfish are attracting attention because of their direct association with brain dysfunction. Accordingly, the European Food Safety Authority is considering legal restrictions on their dietary intake. Modern society overlooks the environmental contamination and health hazards caused by arsenic chemical weapons mainly produced during World War II. This review aims to evaluate the various health effects of AMC reduction in acute, subacute, and chronic arsenic poisoning, in addition to the methylarsenic compounds such as arsenolipids, arsenosugars, and arsenobetaine, as well as arsenic chemical weapons such as lewisite, diphenylchloroarsin, and diphenylcyanoarsine.
Department of Preventive Medicine, St. Marianna University School of Medicine, Kawasaki, Japan
Takahiko Yoshida
Department of Social Medicine, Asahikawa Medical University, Asahikawa, Japan
Ayako Takata
Department of Preventive Medicine, St. Marianna University School of Medicine, Kawasaki, Japan
*Address all correspondence to: hyama@marianna-u.ac.jp
1. Introduction
As a result of naturally occurring inorganic arsenic (iAs) leached into aquifers and polluted drinking water, large-scale chronic arsenic poisoning in various areas of the worldwide occurred and has not ended even today. As the source of iAs contamination cannot be fundamentally removed, chronic arsenic poisoning is difficult to eradicate. The adverse health effects of arsenic exposures observed on the general population from the fetus through maternal placenta to the elderly comprise lifestyle disorders and cognitive dysfunctions in addition to the conventional poisoning symptoms such as skin lesions and malignancy. The health effects of iAs exposure are expected to be strongly associated with a reduction in arsenic methylation capacity (AMC) [1, 2]. In general, various confounding factors can affect the AMC results obtained from urinary samples. Valid supportive information on this issue is based on the occurrence of acute arsenic poisoning in 61 patients [3]; however, it virtually included no confounding effect and was able to serve as a reference value in the AMC evaluation in chronic arsenic poisoning. The results of a survey of 6223 survivors at the time of 65 years of follow-up among the 12,131 subjects exposed to arsenic sub-acutely in infancy [4] provide important data in predicting effects on the future health outcomes of chronic arsenic exposure, especially on carcinogenesis and the cognitive impairment resulting from the damage to the brain and central nervous system.
Conventionally, the complications of arsenic exposure are attributed only to iAs. The seafood for daily consumption contains arsenolipids (AsLipids) with an estimated stronger toxicity than iAs [5, 6]. Accordingly, the European Food Safety Agency (EFSA) is preparing a legal regulation focusing on AsLipids ingested via seafood [7]. On the other hand, arsenic chemical weapons, largely produced during World War II, have been causing environmental contamination due to abandoned phenylarsenic chemical warfare agents in the Baltic Sea [8, 9, 10], Germany [11], China [12, 13, 14], and Japan [15]. The degradation product of phenylarsenic chemical warfare agents is diphenylarsinic acid (DPAA). In Japan, poisoning by DPAA has been confirmed in 157 patients [15]. The target organ of this DPAA is the brain, where it can infiltrate the blood-brain barrier (BBB) and cause cerebral central nervous system damage.
This review aims to outline the differences in health effects of acute, subacute, and chronic arsenic poisoning based on the results of the AMC. In addition, it presents the adverse effects of AsLipids and phenylarsenic chemical warfare agents, which are likely to be more toxic than iAs.
2. Factors affecting the occurrence and the symptoms of acute arsenic poisoning
2.1 Crystallized and dissolved arsenic trioxide (ATO)
Arsenic compounds have long been used in many countries for intentional suicide and homicide. The background of their utilization is related to their physical properties of being tasteless, odorless, and non-irritating. Powdered arsenic trioxide (ATO) has been used in many cases of suicide (Table 1) [16, 17, 18, 19, 20] and by some medical personnel with access to ATO [17]. Factors such as the arsenic dose ingested, the form of ATO (crystals or solution), and time to life-saving treatment play a key role in the development of acute arsenic poisoning. It should be noted that in case reports of acute arsenic poisoning, most references to ATO intake are in terms of the swallowed weight (g) rather than the actual amount absorbed into the body. ATO crystals do not rapidly dissolve in water, predicting their gradual dissolution in the gastrointestinal tract; this slow dissolution rate provides an opportunity for emergency treatment, such as washing the stomach and the intestines, and adsorption and removing ATO with activated carbon. As ATO is a metalloid with metallic properties, an abdominal X-ray of the patient should show a white shadow on the wall of the gastrointestinal tract [16, 19, 20], indicating the ingestion status. A critically ill patient who ingested a large amount of ATO (54 g) was successfully saved by surgically removing the ATO through an incision in the stomach [19]. In other words, in acute arsenic poisoning caused by crystalline ATO, the removal of ATO residues from the gastrointestinal tract has been shown to be extremely important for the patient’s survival.
An acute arsenic poisoning of 61 people, including children (n = 22) and adults (n = 39), in Wakayama, Japan, was caused by the intentional addition of industrial ATO to hot curry soup. Later investigations revealed that most of the ATO was dissolved (with small amounts of crystals) in the residual heat of the curry soup. The estimated arsenic intake amount (body absorption) was calculated using the arsenic in the patient’s urine. The arsenic doses in children and adults were 67.4 ± 29.5 mg and 78.3 ± 38.7 mg, respectively. Information on the lethal dose in humans is scarce; however, it is nearly 300 mg [21]. Four people (aged 10, 16, 53, and 64 years) died by approximately 12 h after ingesting ATO. Dissolved ATO is presumed to be absorbed faster and at a higher rate in the gastrointestinal tract than crystallized ATO. Adults with severe symptoms have taken 100–200 mg of ATO. In contrast, even when the ingested arsenic dose exceeded 100 mg, the children had mild symptoms and were discharged from the hospital after about 1 week. The differences in symptoms between children and adults are discussed in later chapters (see 2.3).
In all patients, the ingestion of dissolved ATO caused severe nausea and vomiting within approximately 5 min [3]. Gastrointestinal symptoms were observed even at the minimum body arsenic dose of 22 mg (1-year-old infant). Afterward, watery diarrhea developed in approximately 30% of the patients. Laboratory values showed an initial increase in white blood cell count, followed by a rapid decrease to reach a minimum on days 3–6. The liver dysfunction (abnormal increase of GOT and GPT) peaked at about 1 week and then slowly recovered. The prolongation of the Q–T interval was characteristic of the electrocardiogram and was also observed in children. In adults with severe disease, erythematous macule, without pain or itching, was found as skin lesions on the abdomen, armpits, and neck [22]. In addition, peripheral neuropathy (paresthesia and motor paralysis) was observed [23]. Patients showed white shadows on the wall of their gastrointestinal tract on the abdominal X-ray, consistent with the observations on the reported victims who ingested crystalline ATO [16, 19, 20]. Therefore, the symptoms of acute arsenic poisoning by dissolved ATO tend to develop quickly and severely ill, especially in adults.
2.2 Effects of chelating agent treatment
British Anti-Lewisite (BAL), initially developed against the arsenic chemical weapon-lewisite, was subsequently used to treat acute iAs poisoning. However, BAL has disadvantages, such as severe pain with muscle injection. The use of chelating agents in acute arsenic poisoning is to promote urinary excretion by binding iAsIII to SH groups. To achieve a high rate of this pharmacological reaction, iAsIII should be not oxidized or methylated to monomethylarsonic acid (MMA) or dimethylarsinic acid (DMA), and the chelating agent must be used as soon as possible after ATO ingestion. This mechanism of action is common to BAL, 2,3-dimercapto-1-propanesulfonic acid (DMPA) and 2, 3-dimercaptosuccinic acid (DMSA) [24, 25]. DMPA tends to be used orally or intramuscularly, depending on the patient’s symptoms [20].
On the other hand, DMPA or DMSA as a treatment for chronic arsenic poisoning due to iAs exposure has been tested in India and Bangladesh without efficacy [24, 25]. However, studies are still ongoing for the development of an effective therapeutic drug for chronic arsenic poisoning.
2.3 Differences in symptoms between children and adults: evaluation by AMC
Epidemiological studies of chronic arsenic poisoning have been attempted to elucidate the relationship between health effects and AMC. In summary, the studies suggested that any decrease in the metabolic efficiency of methylation to iAs can lead to health deterioration. The indicators of an AMC decrease are an increase in %MMA and a decrease in the second methylation ratio (DMA/MMA) or the secondary methylation index (SMI; DMA/MMA + DMA). Recent reports indicate a trend toward higher rates of AMC in children compared to adults [26, 27, 28]. Chronic arsenic poisoning occurs more often in economically developing countries, and the situation of poisoning has been related to the environment, diet, and hygienic conditions in which the subjects live. There are various confounding factors in the urinary arsenic results obtained from subjects, especially the influence of nutrients [29, 30].
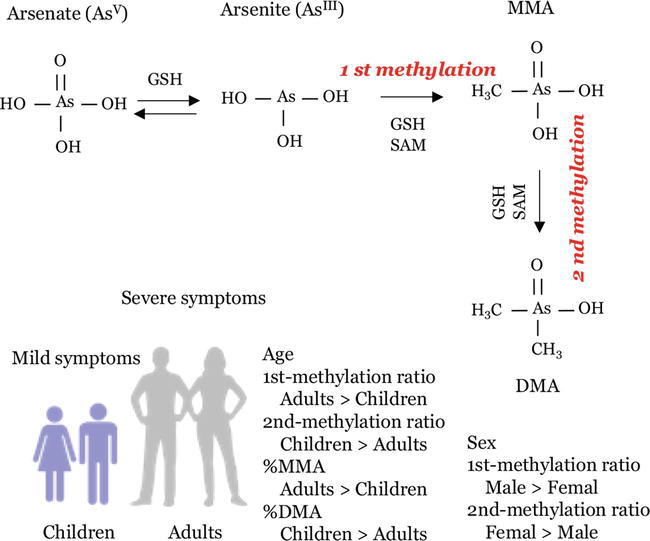
To our knowledge, there are no studies evaluating AMC in patients with acute arsenic poisoning, including ATO. The 61 patients with acute arsenic poisoning cases presented in this review did not have the opportunity for emergency treatment with chelating agents [3]. Therefore, their urinary arsenic results reflected only the observed results without confounding factors such as nutrients and arsenic species in the diet, which are usually noted in epidemiological studies of chronic arsenic poisoning. Although the estimated arsenic intake amount of ATO was similar among the patients (see section 2.1), the symptoms were milder in children and, conversely, more significant in adults [3]. The characteristics of AMC in children and adults are shown in Figure 1. Children had lower %MMA and higher second methylation ratio or SMI. In adults with severe symptoms, we observed a significant trend toward increased %MMA and decreased second methylation ratio or SMI. In acute and chronic arsenic poisoning [27], the data available to elucidate the cause of high AMC in younger children are limited. The mechanism that is currently receiving the most attention is its association with one-carbon metabolism (OCM). OCM is a biochemical pathway that provides methyl donor group S-adenosylmethionine (SAM) to methylate arsenic. It has been estimated that OCM is activated in younger children and degrades with age; there are several interesting reviews that have evaluated the link between OCM and arsenic methylation [1, 29, 31].
Figure 1.
Characteristics of arsenic methylation capacity (AMC) in children and adults with acute arsenic poisoning. Children are under 16 years old and adults are over 16 years old. Monomethylarsonic acid (MMA), dimethylarsinic acid (DMA), S-adenosylmethionine (SAM), reduced glutathione (GSH). First methylation ratio (MMA/inorganic arsenic (iAs)), second methylation ratio (DMA/MMA). Methylation efficiency was assessed by determining the relative amounts of total arsenic in urinary (%iAs, %MMA, and %DMA).
AMC findings from children and adults with acute arsenic poisoning may serve as a valid guideline for evaluating AMC in patients with chronic arsenic poisoning and those exposed to high concentrations of iAs.
3. After-effects of subacute arsenic poisoning in infants after 55–65 years
Subacute arsenic poisoning occurs under conditions of continuous intake of approximately 1/100th of the lethal dose of acute arsenic poisoning over several months. In 1955, out of 12,131 infants who developed subacute arsenic poisoning after ingesting the powdered Morinaga Milk contaminated with iAs (arsenate, iAsV), 130 died. The contaminated milk was consumed on an average of 3 months with an estimated daily arsenic intake of 1.3–3.6 mg, leading to a total accumulation of 90–140 mg. The major initial symptoms were fever, vomiting, diarrhea, abdominal distension, hepatomegaly, cough, nasal discharge, conjunctivitis, and melanoderma. Nevertheless, the neurological indices might not have been properly identified due to the age of the patients who were infants. The confirmed laboratory results comprised anemia, electrocardiographic abnormalities, and a radiographic band-like shadow of the epiphysis of the long bone [4, 32].
The acute arsenic poisoning patients in Wakayama included four 1-year-old infants (mean ATO intake; 44 (22–65) mg) with mild symptoms [3]. In contrast, 130 infants of the same age died from subacute arsenic poisoning [4]. To date, this question has not been resolved, but we can speculate on possible interpretations on the basis of differences in AMC affected by exposure situation of iAs. The continual ingestion of iAs is assumed to accelerate the deterioration of physical condition. The iAs methylation requires the supply of the methyl group donor SAM and reduced glutathione (GSH) by the OCM pathway. If deteriorating physical conditions persist, the supply of SAM decreases due to the reduced function of the OCM [1, 29, 31]. It is assumed that the deterioration of physical conditions led to the depletion of SAM and GSH due to the inability of the nutritional supply to function, and as a result, the detoxification mechanism of iAs was blocked, leading to severe illness and even death.
Results of a subsequent follow-up survey in the 15th year showed a delayed growth, intellectual disability, central nervous system disorders such as epilepsy and hearing loss, and skin conditions such as melanoderma and keratosis [32]. Another survey in the 55th year demonstrated carcinogenesis and cognitive dysfunctions, with a significantly higher risk of mortality from neurological diseases compared to the general population [33]. Recently, the results of the 65th-year follow-up study were reported [4]. In total, 6223 survivors of the iAs poisoning were enrolled in a prospective cohort study from 1982 to 2018. Using standardized mortality rates (SMRs), the subjects’ mortality and cancer incidence rates were compared to their respective Japanese population rates and 95% confidence intervals (95% CI) were calculated. A statistically significant increase in mortality ratio was observed for all causes (SMR, 1.15; 1.01–1.19), nervous system disease (2.83, 1.62–4.19), respiratory disease (2.02, 1.37–2.62), genitourinary systems disease (2.25, 1.10–3.73). It should be noted that epilepsy and cerebral palsy mainly contributed to the high mortality rate caused by the central nervous system disease. Therefore, it is suggested that subacute arsenic poisoning in infancy may cause permanent damage to the central nervous system. Furthermore, liver cancer showed a high mortality rate (SMR, 1.68, 1.06–2.31), whereas that of bladder cancer increased; however, no significant difference was detected. These findings are consistent with the epidemiological studies in Chile [34, 35] that suggested a link between exposure to high levels of iAs during infancy and the risk of developing bladder and lung cancers at an older age. Consequently, we consider that the results of the subsequent follow-up surveys applied to the subacute arsenic poisoning survivors are a warning sign against the risk of human exposure to iAs when the BBB is still not functional, such as in infants and fetuses.
4. Past, present, and expected future health effects from exposure to environmental iAs
In the early twentieth century, chronic arsenic poisoning was first discovered in Argentina, followed by large epidemics in Chile and Taiwan. Then, starting in the late 1970s, it was detected in India, Bangladesh, and China among Asian countries. Chronic arsenic poisoning occurred by consuming the provided drinking water without previous testing for the presence of toxic substances. Particularly well water triggered the outbreaks of serious poisoning. Because chronic arsenic poisoning is caused by naturally existing iAs and the source cannot be eliminated, the potential occurrence of epidemic to be continue in the future [32].
4.1 iAs exposure and skin lesions
Chronic arsenic poisoning generally develops from drinking well water contaminated with iAsIII or iAsV (approximately 50 μg/L) over a period of more than several years. However, even low concentrations (5–10 μg/L) have been associated with the development of skin lesions [36]. The most prominent symptom of chronic arsenic poisoning is skin lesions, characterized by hyperkeratosis of the palms and soles and hyperpigmentation and depigmentation (raindrops) particularly pronounced on the abdomen and trunk. Hyperkeratosis is painful and can affect daily routine activities and reduce the quality of life.
The iAs exposure dose is the primary factor in the development of skin lesions. Another possible factor suggested factor is the decrease in AMC, which raises %MMA and decreases SMI [2]. This factor is more significant in males compared with females. On the other hand, skin lesions in children are significantly milder than in adults, suggesting that AMC in children is higher than in adults [27]. This is consistent with the acute arsenic poisoning case, in which children had milder symptoms than adults [3]. The mechanism between the decrease in AMC and skin lesions has not been clearly elucidated, but the genetic polymorphism of methylation has been explored [37, 38].
4.1.1 AMC determined from blood arsenic and evaluation of skin lesions
For unknown reasons, epidemiological studies of chronic arsenic poisoning have not reported the profile of arsenic species in the blood. The difficulty in analyzing arsenic in blood by chemical form (its species) may be one of the reasons for the lack of reports. In 1999, we measured the urinary and blood arsenic in a small sample (n = 78) in Gangfangying village, Inner Mongolia, China, without publishing the results. In this review, we reanalyzed the relationship between the index of AMC determined from blood arsenic and skin lesions.
The determination of the chemical form of arsenic in blood is similar to the method of urine analysis [39].
Of the 78 subjects [14 children (7–17 years) and 64 adults (21–70 years)], 38 had skin lesions (dyspigmentation and hyperkeratosis). Table 2 shows the comparison of compares the urinary and blood arsenic concentrations and the index values of AMC (iAs, MMA, and DMA) in the subjects grouped by the presence and absence of skin lesions. Arsenic levels in urine and blood were significantly higher in the group with skin lesions (p < 0.001). However, urinary arsenic profile did not show any statistically significant difference in the AMC index, unlike blood arsenic profile (p < 0.001) (Table 2). In general, urinary arsenic is known to vary due to confounding factors. The urinary arsenic levels of the 78 subjects showed four cases of outliers for iAs, three for MMA, and another three for DMA, but no outliers for blood arsenic (results not shown in table). Tamayo et al. [40] noted that arsenic in blood has fewer outliers than arsenic in urine. The fact that AMC calculated based on blood arsenic is superior to that based on urinary arsenic in evaluation of the AMC of individual subjects is due to the result of the relatively stable of blood arsenic concentration.
Comparison of urinary and blood arsenic concentrations and AMC in 78 residents of Gangfangying village, China.
μg/l years. Urine, U; blood, B. Values are median (IQR). IMD, inorganic arsenic (iAs) + methylarsonic acid (MMA) + dimethylarsinic acid (DMA). First methylation ratio (MMA/iAs), second methylation ratio (DMA/MMA). Primary methylation index (PMI, MMA + DMA/IMD), secondary methylation index (SMI, DMA/MMA + DMA).
Mann-Whitney’s U test was used for continuous variables, and Chi-square test was used for categorical variables to compare two groups.
Table 3 shows the adjusted odds ratios (OR) for age and sex for each of the variables listed in Table 2. In the AMC determined from of blood, %MMA showed a significant association with the risk of developing skin lesions (OR = 1.12, 95%CI: 1.06–1.19, p < 0.001). AMC determined from blood arsenic profiles was validated in a small group of subjects; however, more studies reaching various research areas are needed.
OR and 95% CI for skin lesions by variable factors using arsenic methylation capacity calculated based on arsenic species in urine or blood.
μg/l years.
Adjusted for age and sex. OR, odds ratio; CI, confidence interval.
4.1.2 Improvement of skin lesions by reducing iAs exposure
We investigated through a one-year observation study whether the confirmed skin lesions of the 38 subjects could be ameliorated by reducing iAs doses from well water by changing water source. The average arsenic concentration in well water during iAs exposure was 0.13 ± 0.20 mg/l, while the one used for exposure reduction was 0.037 mg/l. The urinary IMD (iAs + MMA + DMA) concentration during iAs exposure was median (IQR) 200 (53.5–398) μg/g cr., while the IMD level at 1-year was median (IQR) 50.4 (33.3–83.0) μg/g cr. Dyspigmentation and hyperkeratosis changes are shown in Figure 2, where relative but insufficient improvement was observed. The AMC index determined from urinary arsenic in all 38 subjects did not significantly change. These patients were followed up for an additional 5, 10, and 15 years. A fast improvement in hyperkeratosis was observed in the first year, but, unexpectedly, successive improvement was found to be slow [41].
Figure 2.
Improvement of skin lesions by reducing iAs exposure for 1 year. Dyspigmentation at top, and hyperkeratosis at bottom.
A study in Bangladesh suggested that reducing iAs exposure from well water (from >50 μg/l to <50 μg/l) over a 2-year period not only increased the recovery rate of skin lesions, but also reduced the severity of skin lesions in patients over time [42]. A study in Inner Mongolia, China, tested whether skin lesions improved by reducing the arsenic concentrations in the well water from >200 μg/l (2004) to <5 μg/l (2017). The 119 subjects were compared for skin symptoms (hyperkeratosis), urinary arsenic levels, and AMC indices in 2004 and 2017. As a result, 25 subjects (21%) showed improvement of skin symptoms. However, recovery of skin symptoms showed an association between %iAs and %DMA, no association between %MMA due to its wide variable value [43]. Reduction of iAs exposure from drinking water may not be sufficient for improvement of hyperkeratosis.
4.2 iAs exposure and carcinogenesis
IARC has identified iAs as a Group 1 carcinogen that causes skin, lung, bladder, and liver cancers [44]. The latent period of arsenic carcinogenesis is generally estimated at 30–50 years. The data on carcinogenesis in patients with chronic arsenic poisoning recognize a trend toward reporting from countries with a relatively long history of iAs exposure. Evidence between iAs exposure and carcinogenesis has been reported from Taiwan for skin [45, 46, 47] and bladder cancers [48], and from Chile [49] and Argentina [50] for lung cancers. Previous reports have suggested a relationship between decreased AMC and carcinogenesis. Epidemiological studies in Chile [34, 35] have reported that exposure to high levels of iAs in infancy increased the risk of developing bladder and lung cancer in older age. Since the iAs exposure level in Asian countries had increased around 1980, a peak of carcinogenesis is expected around 2010–2030 if the incubation period for carcinogenesis is correct. Recently, reports of bladder cancer due to iAs exposure have increased [35, 48, 49]. On the other hand, some reports predicted a relatively low incidence of skin cancer in China [51].
Strangely, little progress has been made in elucidating the mechanism of arsenic carcinogenesis. Because the accumulation of knowledge that arsenic has none or weakly mutagenic property, researchers shifted their focus on the mechanisms involving epigenetic dysregulation in the carcinogenicity arsenic [52, 53].
4.3 iAs exposure and cognitive dysfunction
A growing number of studies on iAs exposure and health effects have focused on the cognitive abilities. A prospective study of subacute arsenic poisoning in infants led to find the cognitive dysfunction manifested in the elderly as a sequela of cerebral and central nervous system damage [4]. The outcomes are important as predictive data for cognitive dysfunction in chronic arsenic poisoning.
Studies in Bangladesh [54, 55], Taiwan [56], Mexico [57], Spain [58], and United States [59] confirmed cognitive abilities in children. Taiwanese studies reported that a lower AMC can lead to cognitive development [56]. The WHO (2018) raised the alarm about cognitive abilities from iAs exposure during fetal and infancy stages [60]. Recently, it has become known that rice accumulates arsenic in the soil at a high rate during cultivation. Since rice is a staple food in most Asian countries (which account for approximately 50% of the world’s population), it is likely that the discussion of the sources of iAs exposure would revolve around rice, rather than drinking water. In this regard, EFSA discusses the need for the legal regulation of iAs intake from rice and processed rice products for infants and children [61].
Although the effects on cognitive abilities have been studied mainly in children, an association between iAs exposure and cognitive dysfunction in adults has been suggested [62, 63, 64]. However, there is insufficient information on the mechanism of cognitive dysfunction, whether it is due to the exposure in infancy which was manifested in older age [4] or to direct exposure in adults. iAs exposure started to be among the stated causes of cognitive dysfunction.
4.4 iAs exposure and cardiovascular disease (CVD) and diabetes
Exposure to high concentrations of iAs has been associated with CVD. The relationship between iAs exposure and CVD has been attributed to carotid atherosclerosis [65, 66], with an increase in %MMA, suggesting an association with a decrease in AMC. Nevertheless, no significant association between hypertension and a decreased AMC has been observed. We were the first to discover that peripheral vascular damage in iAs-exposed humans is induced by nitric oxide (NO), an oxidative stress [67].
Exposure to high concentrations of iAs has been suggested to be associated with diabetes [68, 69]. However, the relationship between AMC and diabetes at low iAs exposures has been studied, but no clear association has been found. The relationship between iAs intake (mainly from rice) and lifestyle-related diseases (non-communicable diseases, NCDs) is expected to be the subject of much debate among most people living in non-arsenic-contaminated environments.
5. Health effects of organic arsenic compounds ingested from seafood and seaweeds
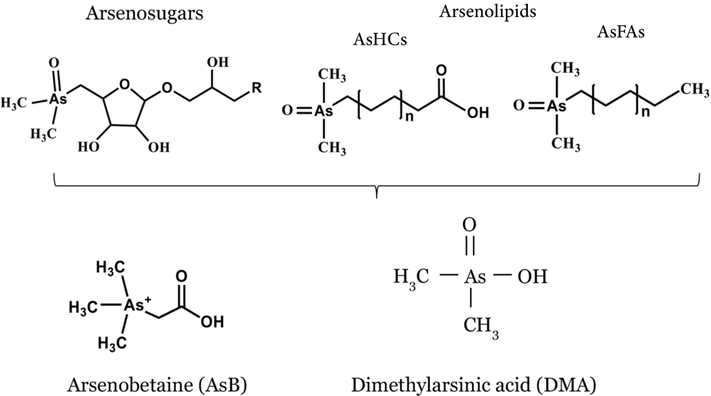
The demand for seafood is increasing internationally as the dietary intake of omega-3 fatty acids, mainly found in seafood, has been highly recommended for the prevention of NCDs. On the other hand, arsenolipids, arsenobetaine, and arsenosugars are found in fish and shellfish, and varying toxicity has been observed (Figure 3). In 2022, the EFSA started to adopt legal regulations for the dietary intake of AsLipids in fish and shellfish [7].
Figure 3.
Chemical structure of arsenolipids, arsenosugars, and arsenobetaine. Typical arsenolipids are known as arsenic-containing hydrocarbons (AsHCs) and arsenic-containing fatty acids (AsFAs). The major metabolite of arsenolipids and arsenosugars is DMA.
5.1 Arsenolipids (AsLipids)
Many types of AsLipids have been detected in marine organisms, among which four were identified, including arsenic-containing hydrocarbons (AsHCs), arsenic-containing fatty acids (AsFAs), arsenic-containing phospholipids, and arsenic-containing phosphatidyl-cholines. Of these, the first two are noted in this study [5, 6, 70].
One of the major adverse health effects of AsLipids concerns brain function. An experimental validation suggests that AsHCs can penetrate the BBB and migrate to the brain tissues. An in vitro model of the blood–cerebrospinal fluid barrier composed of porcine choroid plexus epithelial cells showed that AsHCs were 1.5-fold more potent than arsenite (iAsIII) in disrupting the barrier function. Consequently, it is suggested that being exposed to high levels of certain AsLipids may be harmful to the central nervous system [71]. In addition, AsHCs have been shown to accumulate in brain tissues when applied to drosophila [72]. The toxicity of AsHCs in brain cells has been shown to be 5–19 times greater than that of iAsIII when applied to human neuronal astrocytes [73]. In contrast, AsFAs tend to be less permeable to the BBB and less neurotoxic than AsHCs [74].
To our knowledge, there is insufficient information to evaluate the effects of AsLipids on the human brain. After 24 h of salmon ingestion containing AsHCs, approximately 3% was detected in breast milk [75], which could cross the BBB and migrate to the infant’s brain tissue. Alternatively, the strong brain cytotoxicity of AsHCs is also predicted to cause brain dysfunction.
Detailed studies on the biotransformation of AsLipids in animal studies are deemed difficult to conduct, due to the required large sample size. To search for AsLipid metabolites, the urinary arsenic was measured in two volunteers who took a single oral dose of test material prepared from cod liver oil. The major metabolites of AsLipids were DMA and small amounts of thio-dimethylarsenobutanoic acid (DMAB), oxo-DMAB, thio-dimethylarsenopropanoic acid (DMAPr), and oxo-DMAPr [76].
Studies predicting the daily intake of AsLipids are difficult and limited. However, a market basket survey estimated the daily intake of AsLipids from 152 food items, including seafood and algae. AsHCs and AsFAs were 4200 and 2100 ng As/person/day, respectively, as solely detected in seafood and algae [77]. Notably, AsLipid concentrations were measured in 18 samples of the purchased seafood, and AsHC values were 83 ± 73 ng As/g fresh-weight; this study revealed that consumed seafood contain toxic AsHC [78]. Seafood is commonly cooked by boiling or baking. The chemical structure of AsLipids, when heated in a microwave oven, was reported unchanged [79]. Therefore, toxic AsLipids are absorbed without loss due to cooking.
5.2 Arsenobetaine (AsB)
AsB in seawater is produced by the methylation of iAs by phytoplankton and zooplankton and is concentrated in fish or shellfish through the food chain. In mammals, AsB is not synthesized in the body; thus, it is entirely derived from seafood and is rapidly excreted in the urine, as verified in human [80] and animal [81, 82] studies. Its half lethal dose (LD50) is 10 g/kg, and AsB has been shown to be the least toxic of the arsenic compounds [5, 6].
5.3 Arsenosugars (AsSugars)
The structure of AsSugars was first elucidated from brown kelp (Ecklonia radiata) by Edmonds and Francesconi in 1981 [83]. It is presumed that AsSugars in seaweeds are originally biosynthesized by the direct absorption of iAs from seawater. Seaweed and kelp showed to contain large amounts of AsSugar-Gly and AsSugar-SO3, which are not degraded into iAs when treated with heat or stomach acid [6]. The metabolites of AsSugars, validated in humans, were DMA, thio-dimethylarsinoylacetate, thio-dimethylarsinoylethanol, and thio-dimethyl arsenate [84]. The last two seem to be the most toxic, and their cytotoxicity is suggested to be similar to that of iAsIII [85]. The major metabolite of AsSugars in human urine is DMA, which is less toxic than iAs. Further monitoring is needed due to the limited knowledge of the metabolism and toxicity of AsSugars.
6. Abandoned arsenic chemical weapons and health effects
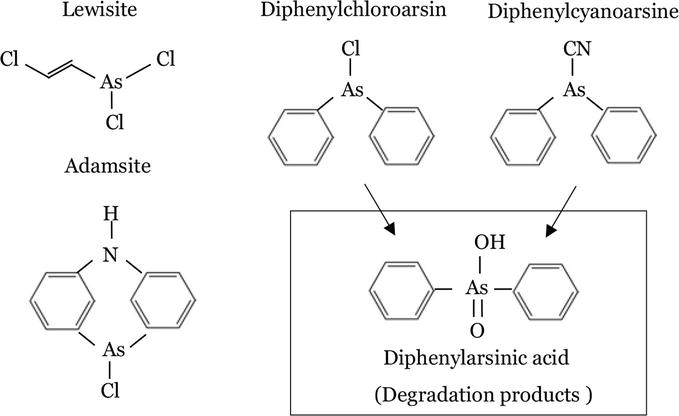
Chemical weapons (CW) were produced in large amounts by the countries that participated in World Wars I and II. In 1997, the Chemical Weapons Convention was signed by the international community, which now includes 192 countries. The Organization for the Prohibition of Chemical Weapons (OPCW, Hague, the Netherlands) oversees and operates the disposal of CW [86]. OPCW defines CW as any chemical substance used to intentionally cause death or harm by its toxicity. The most potent chemical warfare agents include the blister agents: sulfur or nitrogen mustards (yperite), and lewisite; the riot control (vomiting) agents: diphenylchloroarsine (DA, Clark I), diphenylcyanoarsine (DC, Clark II), and adamsite; the blood agents: hydrogen cyanide and arsine; the asphyxiants: chlorine and phosgene; and the nerve agents: sarin, soman, tabun, VX, and Novichok. The main arsenic CW (Figure 4) produced in World War II were the blister and the vomiting agents, which have been largely produced in Japan, Germany, the Soviet Union, and the United States [87].
Figure 4.
Chemical structure of arsenic chemical weapons. The degradation products of diphenylchloroarsin (DA, Clark I) and diphenylcyanoarsine (DC, Clark II) are diphenylarsinic acid (DPAA).
There are two types of CW: stockpile (available) and non-stockpile (abandoned). So far, the largest stockpiles have been held by the United States and Russia, both of which have approximately 30,000–40,000 tons. The United States declared that most of its stockpiled CW have been completely destroyed [87]; however, information about the destruction process in Russia is still not credible. The international community has major concerns related to the non-signatory countries that still possess CW, in addition to the fears of CW possession and use by terrorist organizations. After World War II, many countries dumped their CW in the sea as a cheap disposal method [87]. Approximately 50,000 tons of arsenic CW (including Clarks I and II and adamsite) are estimated to be left in the Baltic Sea [8], which has resulted in phenylarsenic chemical contamination of some seafood [8, 9, 10]. The former Japanese military buried large quantities of arsenic CW in various parts of China during its defeat in World War II. In particular, iAs and phenylarsenic chemical warfare agents derived from arsenic CW have been recently detected in agricultural soil in Jilin Province [12, 13, 14]. Alternatively, the arsenic contamination persists in Germany at the sites of the facilities where arsenic CW filling operations were conducted [11]. After more than 75 years of arsenic CW abandonment, the derived risk of health effects from arsenic still exists in soils and the seabed. Therefore, the international community is invited to recognize the current situation and take action accordingly.
6.1 Lewisite
The blister agents include mustard and lewisite. The former freezes in cold climates (≤ − 20°C) and loses its function as a weapon, while the latter, to which arsenic is added, does not freeze and is used in cold climates. Therefore, lewisite was manufactured in larger amounts by the former Japanese Army and the Soviet Union than in any other country. In 2003, 44 people at a construction site in Heilongjiang Province in China, suffered from severe skin damage due to exposure to containers filled with arsenical CWs (lewisite + mustard), believed to have been abandoned by the former Japanese army [88]. Consequently, this incident implies that the arsenic-containing CW, lewisite, has not been completely and safely removed from the environment.
Exposure to lewisite can cause rapid hydrolysis in the epidermis, resulting in severe skin blistering and inflammation, after which the arsenic is absorbed through the dermis [89]. The eyes are sensitive to lewisite exposure, which can cause edema, blepharospasm, and blindness [90]. Lewisite is absorbed transdermally and distributed throughout the body, causing multiple organ damage in the lungs [91] and kidneys [92], and increasing the likelihood of mortality. On the other hand, little is known about the sequelae following lewisite and mustard exposure. A > 10-year follow-up study on the 44 victims exposed at construction work sites revealed mental and cognitive dysfunctions as new arising health problems [88].
6.2 Diphenylchloroarsine (DA) and diphenylcyanoarsine (DC)
Arsenic CWs that are known as vomiting agents, include DA, DC, and adamsite (Figure 4) and were aimed to be used for disturbing combat abilities of the soldiers rather than for killing or wounding them. Exposure to DA or DC can cause a strong sneeze, nausea, and instant vomiting. However, their detailed toxic effect is still unclear. Diphenylarsinic acid (DPAA) is the raw material for the production of DA and DC and, conversely, their degrading substance in the human body. In 2003, poisoning from contaminated well water in Kamisu, Japan, was caused by DPAA that had been buried underground. The residents used this water for cooking and bathing, while some others used it to prepare infant formula. Ishii et al. (2004) reported that in 2000, the first victim was a junior high school student who had cerebellar ataxia, tremors, and myoclonus [15]. Subsequently, a population health survey led by medical professionals revealed the presence of a total of 157 victims in the surrounding area. Before this incident, there was no toxicological data on DPAA. DPAA can pass through the BBB in trace amounts and target the cerebellum, causing disruption of the glutamatergic system [93, 94]. A summary document published by the Japanese Ministry of the Environment [95] revealed that DPAA is mainly absorbed in the gastrointestinal tract, while a mere amount is absorbed through the skin. Additionally, DPAA is not metabolized in the body and is mainly excreted in the urine. The relative toxicity of DPAA deduced from cytotoxicity studies is 1/100th compared with ATO.
So far, information on DA and DC has been limited to their acute toxicity as vomiting agents, damaging the mucous membranes of the eyes and nasal passages. We did not envision a situation where DA and DC would be decomposed to product DPAA, which would then be ingested via drinking water. However, DPAA and related substances have been found to contaminate fish, shellfish, and soil [8, 9, 10, 11, 12, 13, 14]. The clinical findings in DPAA poisoning patients [15] and animal studies [93, 94, 95] are consistent with the brain being the target organ. Toxicological information on DPAA suggests that it may be the most dangerous of the arsenic compounds. In the future, the factual extent of contamination in seafood, agricultural products, and drinking water needs to be further investigated.
The AMC index determined from non-confounding urinary arsenic in patients with acute arsenic poisoning is expected to contribute to research investigations of chronic arsenic poisoning. The effects of acute and chronic arsenic poisoning on health are associated with decreased AMC. Children and adult females tend to have higher levels of AMC than adult males. However, iAs exposure in infancy increases cancer and cognitive dysfunction in old age. Furthermore, AsLipids ingested from seafood penetrate the BBB and accumulate in the brain, resulting in toxicity. DPAA, a degradant of DA and DC used in vomiting agents among the arsenic CWs used in World War II, is overlooked by the international community as a cause of cerebellar disorders. In the past, the effects of arsenic on health have been mostly concerned with carcinogenesis. However, the target organ for iAs, AsLipids, and DPAA is mainly the brain; therefore, a deeper understanding of brain dysfunction is needed. Scientific evidence has begun to confirm that exposure to iAs during infancy and conception (fetus) exacerbates carcinogenesis and cognitive dysfunction in old age.
1.Vahter ME. Interactions between arsenic-induced toxicity and nutrition in early life. Journal of Nutrition. 2007;137(12):2798-2804. DOI: 10.1093/jn/137.12.2798
2.Shen H, Niu O, Xu M, Rui D, Xu S, Feng G, et al. Factors affecting arsenic methylation in arsenic-exposed humans: A systematic review and meta-analysis. International Journal of Environmental Research and Public Health. 2016;13(2):205. DOI: 10.3390/ijerph13020205
3.Yamauchi H, Takata A. Arsenic metabolism differs between child and adult patients during acute arsenic poisoning. Toxicology and Applied Pharmacology. 2021;410:115352. DOI: 10.1016/j.taap.2020.115352
4.Liu R, tabuchi T, Kitamura T, Miyashiro I, Sobue T. Long-term observational study on 6223 survivors of arsenic poisoning due to contaminated milk powder during infancy. Cancer Science. 2020;111(10):3873-3880. DOI: 10.1111/cas.14623
5.Taylor V, Goodale B, Raab A, Schwerdtle T, Reimer K, Conklin S, et al. Human exposure to organic arsenic species from seafood. Science of the Total Environment. 2017;580:266-282. DOI: 10.1016/j.scitotenv.2016.12.113
6.Cao Y, Takata A, Hitomi T, Yamauchi H. Metabolism and toxicity of organic arsenic compounds in marine organisms. In: Yamauchi H, Sun G, editors. Arsenic Contamination in Asia. Current Topics in Environmental Health and Preventive Medicine. Singapore: Springer; 2018. pp. 119-136. DOI: 10.1007/978-981-13-2565-6_7
7.European Food Safety Authority (EFSA). Extensive literature search on organic arsenic in food. EFSA Journal. 2022;19(9):EN-7565. DOI: 10.2903/sp.efsa.2022.EN-7565
8.Vanninen P, Östin A, Bełdowski J, Pedersen EA, Söderström M, Szubska M, et al. Exposure status of sea-dumped chemical warfare agents in the Baltic Sea. Marine Environmental Research. 2020;161:105112. DOI: 10.1016/j.marenvres.2020.105112
9.Niemikoski H, Lehtonen KK, Ahvo A, Heiskanen I, Vanninen P. Metabolism and cytotoxicity of diphenylarsinic acid, a degradation product of sea-dumped chemical warfare agents, in a rainbow trout liver cell line RTL-W1. Aquatic Toxicology. 2021;241:105993. DOI: 10.1016/j.aquatox.2021.105993
10.Czub M, Nawała J, Popiel S, Brzeziński T, Maszczyk P, Sanderson H, et al. Acute aquatic toxicity of arsenic-based chemical warfare agents to Daphnia magna. Aquatic Toxicology. 2021;230:105693. DOI: 10.1016/j.aquatox.2020.105693
11.Daus B, Hempel M, Wennrich R, Weiss H. Concentrations and speciation of arsenic in groundwater polluted by warfare agents. Environmental Pollution. 2010;158:3439-3444. DOI: 10.1016/j.envpol.2010.06.029
12.Zhang Y, Xi H, Zhu Y, Zhao S, Ji C. Study on the composition and distribution characteristics of As in As-containing agent contaminated soil. Environmental Research. 2022;214(Pt 3):114039. DOI: 10.1016/j.envres.2022.114039
13.Zhang Y, Zhu Y, Zhao S, Li D, Xi H, Wang Y. Arsenic in soils contaminated by arsenic-containing chemical weapons in a site of Jilin, China: Fraction and bioaccessibility. Environmental Science and Pollution Research. 2022;29(19):28957-28972. DOI: 10.1007/s11356-021-18482-3
14.Ji C, Zhu Y, Zhao S, Zhang H, Wang S, Zhou J, et al. Arsenic and heavy metals at Japanese abandoned chemical weapons site in China: Distribution characterization, source identification and contamination risk assessment. Environmental Geochemistry and Health. 2022. DOI: 10.1007/s10653-022-01382-x
15.Ishii K, Tamaoka A, Otsuka F, Iwasaki N, Shin K, Matsui A, et al. Diphenylarsinic acid poisoning from chemical weapons in Kamisu, Japan. Annals of Neurology. 2004;56(5):741-745. DOI: 10.1002/ana.20290
17.Kamijo Y, Soma K, Asari Y, Ohwada T. Survival after massive arsenic poisoning self-treated by high fluid intake. Journal of Toxicology. Clinical Toxicology. 1998;36(1-2):27-29. DOI: 10.3109/15563659809162579
18.Heinrich-Ramm R, Schaller H, Horn J, Angerer J. Arsenic species excretion after dimercaptopropanesulfonic acid (DMPS) treatment of an acute arsenic trioxide poisoning. Archives of Toxicology. 2003;77:63-68. DOI: 10.1007/s00204-002-0413-z
19.Dueñas-Laita A, Pérez-Miranda M, González-López MA, Martín-Escudero JC, Ruiz Mambrilla M, Blanco-Varela J. Acute arsenic poisoning. Lancet. 2005;365(9475):1982. DOI: 10.1016/S0140-6736(05)66670-6
20.Lu PH, Tseng JC, Chen CK, Chen CH. Survival without peripheral neuropathy after massive acute arsenic poisoning: Treated by 2,3-dimercaptopropane-1-sulphonate. Journal of Clinical Pharmacy and Therapeutics. 2017;42(4):506-508. DOI: 10.1111/jcpt.12538
21.Vallee BL, Ulmer DD, Wacker WEC. Arsenic toxicology and biochemistry. Archives of Industrial Health. 1960;21:132-151
22.Uede K, Furukawa F. Skin manifestations in acute arsenic poisoning from the Wakayama curry-poisoning incident. British Journal of Dermatology. 2003;149:757-762. DOI: 10.1046/j.1365-2133.2003.05511.x
23.Kishi Y, Sasaki H, Yamasaki H, Ogawa K, Nishi M, Nanjo K. An epidemic of arsenic neuropathy from a spiked curry. Neurology. 2001;56(10):1417-1418. DOI: 10.1212/wnl.56.10.1417
24.Nurchi VN, Djordjevic AB, Crisponi G, Alexander J. Arsenic toxicity: Molecular targets and therapeutic agents. Biomolecules. 2020;10(2):235. DOI: 10.3390/biom10020235
25.Bjørklund G, Oliinyk P, Lysiuk R, Rahaman MS, Antonyak H, Lozynska I, et al. Arsenic intoxication: General aspects and chelating agents. Archives of Toxicology. 2020;94(6):1879-1897. DOI: 10.1007/s00204-020-02739-w
26.Waalkes MP, Liu J. Early-life arsenic exposure: Methylation capacity and beyond. Environmental Health Perspectives. 2008;116(3):A104. DOI: 10.1289/ehp.11276
27.Lindberg AL, Ekström EC, Nermell B, Rahman M, Lönnerdal B, Persson LA, et al. Genderand age differences in the metabolism of inorganic arsenic in a highly exposed population in Bangladesh. Environmental Research. 2008;106(1):110-120. DOI: 10.1016/j.envres.2007.08.011
28.Skröder Löveborn H, Kippler M, Lu Y, Ahmed S, Kuehnelt D, Raqib R, et al. Arsenic metabolism in children differs from that in adults. Toxicological Sciences. 2016;152(1):29-39. DOI: 10.1093/toxsci/kfw060
29.Vahter M. Effects of arsenic on maternal and fetal health. Annual Review of Nutrition. 2009;29:381-399. DOI: 10.1146/annurev-nutr-080508-141102
30.Desai G, Millen AE, Vahter M, Queirolo EI, Peregalli F, Mañay N, et al. Associations of dietary intakes and serum levels of folate and vitamin B-12 with methylation of inorganic arsenic in Uruguayan children: Comparison of findings and implications for future research. Environmental Research. 2020;189:109935. DOI: 10.1016/j.envres.2020.109935
31.Abuawad A, Bozack AK, Saxena R, Gamble MV. Nutrition, one-carbon metabolism and arsenic methylation. Toxicology. 2021;457:152803. DOI: 10.1016/j.tox.2021.152803
32.Yamauchi H, Takata A. Past and current arsenic poisonings. In: Yamauchi H, Sun G, editors. Arsenic Contamination in Asia, Biological Effects and Preventive Measures. Singapore: Springer; 2018. pp. 1-11. DOI: 10.1007/978-981-13-2565-6_1
33.Tanaka H, Tsukuma H, Oshima A. Long-term prospective study of 6104 survivors of arsenic poisoning during infancy due to contaminated milk powder in 1955. Journal of Epidemiology. 2010;20(6):439-445. DOI: 10.2188/jea.JE20090131
34.Roh T, Steinmaus C, Marshall G, Ferreccio C, Liaw J, Smith AH. Age at exposure to arsenic in water and mortality 30-40 years after exposure cessation. American Journal of Epidemiology. 2018;187(11):2297-2305. DOI: 10.1093/aje/kwy159
35.Smith AH, Marshall G, Roh T, Ferreccio C, Liaw J, Steinmaus C. Lung, bladder, and kidney cancer mortality 40 years after arsenic exposure reduction. Journal of the National Cancer Institute. 2018;110(3):241-249. DOI: 10.1093/jnci/djx201
36.Yoshida T, Yamauchi H, Fan SG. Chronic health effects in people exposed to arsenic via the drinking water: Dose-response relationships in review. Toxicology and Applied Pharmacology. 2004;198(3):243-252. DOI: 10.1016/j.taap.2003.10.022
37.De Loma J, Skröder H, Raqib R, Vahter M, Broberg K. Arsenite methyltransferase (AS3MT) polymorphisms and arsenic methylation in children in rural Bangladesh. Toxicology and Applied Pharmacology. 2018;357:80-87. DOI: 10.1016/j.taap.2018.08.020
38.De Loma J, Vicente M, Tirado N, Ascui F, Vahter M, Gardon J, et al. Human adaptation to arsenic in Bolivians living in the Andes. Chemosphere. 2022;301:134764. DOI: 10.1016/j.chemosphere.2022.134764
39.Yamauchi H, Yamamura Y. Metabolism and excretion of orally administered dimethylarsinic acid in the hamster. Toxicology and Applied Pharmacology. 1984;74(1):134-140. DOI: 10.1016/0041-008x(84)90279-5
40.Tamayo LI, Kumarasinghe Y, Tong L, Balac O, Ahsan H, Gamble M, et al. Inherited geneticneffects on arsenic metabolism: A comparison of effects on arsenic species measured in urine and in blood. Environmental Epidemiology. 2022;6(6):e230. DOI: 10.1097/EE9.0000000000000230
41.Yoshida T, Sun G, Pi J, Li X, Li B, Yamauchi H. Field research on chronical arsenic poisoning in Inner Mongolia, China. In: Yamauchi H, Sun G, editors. Arsenic Contamination in Asia, Biological Effects and Preventive Measures. Singapore: Springer; 2018. pp. 61-81. DOI: 10.1007/978-981-13-2565-6_5
42.Seow WJ, Pan WC, Kile ML, Baccarelli AA, Quamruzzaman Q , Rahman M, et al. Arsenic reduction in drinking water and improvement in skin lesions: A follow-up study in Bangladesh. Environmental Health Perspectives. 2012;120(12):1733-1738. DOI: 10.1289/ehp.1205381
43.Wei B, Yu J, Kong C, Li H, Yang L, Xia Y, et al. Effects of arsenic methylation and metabolism on the changes of arsenic-related skin lesions. Environmental Science and Pollution Research. 2018;25(24):24394-24402. DOI: 10.1007/s11356-018-2512-2
44.IARC, Arsenic, metals, fibres, and dusts. IARC Monographs on the Evaluation of Carcinogenic Risks to Humans. 100C. Lyon. 2012
45.Hsueh YM, Chiou HY, Huang YL, Wu WL, Huang CC, Yang MH, et al. Serum beta-carotene level, arsenic methylation capability, and incidence of skin cancer. Cancer Epidemiology Biomarkers and Prevention. 1997;6(8):589-596
46.Yu RC, Hsu KH, Chen CJ, Froines JR. Arsenic methylation capacity and skin cancer. Cancer Epidemiology Biomarkers and Prevention. 2000;9(11):1259-1262
47.Chen YC, Guo YL, Su HJ, Hsueh YM, Smith TJ, Ryan LM, et al. Arsenic methylation and skin cancer risk in southwestern Taiwan. Journal of Occupational and Environmental Medicine. 2003;45(3):241-248. DOI: 10.1097/01.jom.0000058336.05741.e8
48.Huang YK, Huang YL, Hsueh YM, Yang MH, Wu MM, Chen SY, et al. Arsenic exposure, urinary arsenic speciation, and the incidence of urothelial carcinoma: A twelve-year follow-up study. Cancer Causes & Control. 2008;19(8):829-839. DOI: 10.1007/s10552-008-9146-5
49.Melak D, Ferreccio C, Kalman D, Parra R, Acevedo J, Pérez L, et al. Arsenic methylation and lung and bladder cancer in a case-control study in northern Chile. Toxicology and Applied Pharmacology. 2014;274(2):225-231. DOI: 10.1016/j.taap.2013.11.014
50.Steinmaus C, Yuan Y, Kalman D, Rey OA, Skibola CF, Dauphine D, et al. Individual differences in arsenic metabolism and lung cancer in a case-control study in Cordoba. Argentina. Toxicology and Applied Pharmacology. 2010;247(2):138-145. DOI: 10.1016/j.taap.2010.06.006
51.Huang L, Wu H, van der Kuijp TJ. The health effects of exposure to arsenic-contaminated drinkingwater: A review by global geographical distribution. International journal of environmental health research. 2015;25(4):432-452. DOI: 10.1080/09603123.2014.958139
52.Saintilnord WN, Fondufe-Mittendorf Y. Arsenic-induced epigenetic changes in cancer development. Seminars in Cancer Biology. 2021;76:195-205. DOI: 10.1016/j.semcancer.2021.03.019
53.Islam R, Zhao L, Wang Y, Lu-Yao G, Liu LZ. Epigenetic dysregulations in arsenic-induce carcinogenesis. Cancers. 2022;14(18):4502. DOI: 10.3390/cancers14184502
54.Vahter M, Skröder H, Rahman SM, Levi M, Derakhshani Hamadani J, Kippler M. Prenatal and childhood arsenic exposure through drinking water and food and cognitive abilities at 10 years of age: A prospective cohort study. Environment International. 2020;139:105723. DOI: 10.1016/j.envint.2020.105723
55.Hamadani JD, Tofail F, Nermell B, Gardner R, Shiraji S, Bottai M, et al. Critical windows of exposure for arsenic-associated impairment of cognitive function in pre-school girls and boys: A population-based cohort study. International Journal of Epidemiology. 2011;40(6):1593-1604. DOI: 10.1093/ije/dyr176
56.Hsueh YM, Lin YC, Chung CJ, Huang YL, Hsieh RL, Huang PT, et al. Combined effect of polymorphisms of MTHFR and MTR and arsenic methylation capacity on developmental delay in preschool children in Taiwan. Archives of Toxicology. 2020;94(6):2027-2038. DOI: 10.1007/s00204-020-02745-y
57.Rosado JL, Ronquillo D, Kordas K, Rojas O, Alatorre J, Lopez P, et al. Arsenic exposure and cognitive performance in Mexican schoolchildren. Environmental Health Perspectives. 2007;115(9):1371-1375. DOI: 10.1289/ehp.9961
58.Soler-Blasco R, Murcia M, Lozano M, Sarzo B, Esplugues A, Riutort-Mayol G, et al. Prenatal arsenic exposure, arsenic methylation efficiency, and neuropsychological development among preschool children in a Spanish birth cohort. Environmental Research. 2022;207:112208. DOI: 10.1016/j.envres.2021.112208
59.Signes-Pastor AJ, Romano ME, Jackson B, Braun JM, Yolton K, Chen A, et al. Associations of maternal urinary arsenic concentrations during pregnancy with childhood cognitive abilities: The HOME study. International Journal of Hygiene and Environmental Health. 2022;245:114009. DOI: 10.1016/j.ijheh.2022.114009
60.WHO. Arsenic. Available from: https://www.who.int/news-room/fact-sheets/detail/arsenic [Accessed: March 8, 2023]
62.Liu J, Gao Y, Liu H, Sun J, Liu Y, Wu J, et al. Assessment of relationship on excess arsenic intake from drinking water and cognitive impairment in adults and elders in arsenicosis areas. International Journal of Hygiene and Environmental Health. 2017;220(2 Pt B):424-430. DOI: 10.1016/j.ijheh.2016
63.Karim Y, Siddique AE, Hossen F, Rahman M, Mondal V, Banna HU, et al. Dose-dependent relationships between chronic arsenic exposure and cognitive impairment and serum brain-derived neurotrophic factor. Environment International. 2019;131:105029. DOI: 10.1016/j.envint.2019.105029
64.Wang X, Huang X, Zhou L, Chen J, Zhang X, Xu K, et al. Association of arsenic exposure and cognitive impairment: A population-based cross-sectional study in China. Neurotoxicology. 2021;82:100-107. DOI: 10.1016/j.neuro.2020.11.009
65.Chen Y, Wu F, Liu M, Parvez F, Slavkovich V, Eunus M, et al. A prospective study of arsenic exposure, arsenic methylation capacity, and risk of cardiovascular disease in Bangladesh. Environmental Health Perspectives. 2013;121(7):832-838. DOI: 10.1289/ehp.1205797
66.Moon KA, Zhang Y, Guallar E, Francesconi KA, Goessler W, Umans JG, et al. Association of low-moderate urine arsenic and QT interval: Cross-sectional and longitudinal evidence from the strong heart study. Environmental pollution. 2018;240:894-902. DOI: 10.1016/j.envpol.2018.04.129
67.Pi J, Yamauchi H, Sun G, Yoshida T, Aikawa H, Fujimoto W, et al. Vascular dysfunction in patients with chronic arsenosis can be reversed by reduction of arsenic exposure. Environmental Health Perspectives. 2005;113(3):339-341. DOI: 10.1289/ehp.7471
68.Kuo CC, Moon KA, Wang SL, Silbergeld E, Navas-Acien A. The association of arsenic metabolism with cancer, cardiovascular disease, and diabetes: A systematic review of the epidemiological evidence. Environmental Health Perspectives. 2017;125(8):087001. DOI: 10.1289/EHP577
69.Farkhondeh T, Samarghandian S, Azimi-Nezhad M. The role of arsenic in obesity and diabetes. Journal of Cellular Physiology. 2019;234(8):12516-12529. DOI: 10.1002/jcp.28112
70.Luvonga C, Rimmer CA, Yu LL, Lee SB. Organoarsenicals in seafood: Occurrence, dietary exposure, toxicity, and risk assessment considerations - a review. Journal of Agricultural and Food Chemistry. 2020;68(4):943-960. DOI: 10.1021/acs.jafc.9b07532
71.Müller SM, Ebert F, Bornhorst J, Galla HJ, Francesconi KA, Schwerdtle T. Arsenic-containing hydrocarbons disrupt a model in vitro blood-cerebrospinal fluid barrier. Journal of Trace Elements in Medicine and Biology. 2018;49:171-177. DOI: 10.1016/j.jtemb.2018.01.020
72.Niehoff AC, Schulz J, Soltwisch J, Meyer S, Kettling H, Sperling M, et al. Imaging by elemental and molecular mass spectrometry reveals the uptake of an arsenolipid in the brain of drosophila melanogaster. Analytical Chemistry. 2016;88(10):5258-5263. DOI: 10.1021/acs.analchem.6b00333
73.Witt B, Bornhorst J, Mitze H, Ebert F, Meyer S, Francesconi KA, et al. Arsenolipids exert less toxicity in a human neuron astrocyte co-culture as compared to the respective monocultures. Metallomics. 2017;9(5):442-446. DOI: 10.1039/c7mt00036g
74.Meyer S, Raber G, Ebert F, Leffers L, Müller SM, Taleshi MS, et al. In vitro toxicological characterisation of arsenic-containing fatty acids and three of their metabolites. Toxicology Research. 2015;4(5):1289-1296. DOI: 10.1039/c5tx00122f
75.Xiong C, Stiboller M, Glabonjat RA, Rieger J, Paton L, Francesconi KA. Transport of arsenolipids to the milk of a nursing mother after consuming salmon fish. Journal of Trace Elements in Medicine and Biology. 2020;61:126502. DOI: 10.1016/j.jtemb.2020.126502
76.Amayo KO, Raab A, Krupp EM, Feldmann J. Identification of arsenolipids and their degradation products in cod-liver oil. Talanta. 2014;118:217-223. DOI: 10.1016/j.talanta.2013.-09.056
77.Amin MHA, Xiong C, Glabonjat RA, Francesconi KA, Oguri T, Yoshinaga J. Estimation of daily intake of arsenolipids in Japan based on a market basket survey. Food and Chemical Toxicology. 2018;118:245-251. DOI: 10.1016/j.fct.2018.05.019
78.Amin MH, Xiong C, Francesconi KA, Itahashi Y, Yoneda M, Yoshinaga J. Variation in arsenolipid concentrations in seafood consumed in Japan. Chemosphere. 2020;239:124781. DOI: 10.1016/j.chemosphere.2019.124781
79.Xiong C, Glabonjat RA, Al Amin MH, Stiboller M, Yoshinaga J, Francesconi KA. Arsenolipids in salmon are partly converted to thioxo analogs during cooking. Journal of Trace Elements in Medicine and Biology. 2022;69:126892. DOI: 10.1016/j.jtemb.2021.126892
80.Yamauchi H, Yamamura Y. Metabolism and excretion of orally ingested trimethylarsenic in man. Bulletin of Environmental Contamination and Toxicology. 1984;32(6):682-687. DOI: 10.1007/BF01607556
81.Vahter M, Marafante E, Dencker L. Metabolism of arsenobetaine in mice, rats and rabbits. Science of the Total Environment. 1983;30:197-211. DOI: 10.1016/0048-9697(83)90012-8
82.Yamauchi H, Kaise T, Yamamura Y. Metabolism and excretion of orally administered in the hamster. Bulletin of Environmental Contamination and Toxicology. 1984;36(3):350-355. DOI: 10.1007/BF01623519
83.Edmonds JS, Francesconi KA. Arseno-sugars from brown kelp (Ecklonia radiata) as intermediates in cycling of arsenic in a marine. Nature. 1981;289:602-604. DOI: 10.1038/289602a0
84.Francesconi KA, Tanggaar R, McKenzie CJ, Goessler W. Arsenic metabolites in human urine after ingestion of an arsenosugar. Clinical Chemistry. 2002;48(1):92-101. DOI: 10.1093/clinchem/48.1.92
85.Leffers L, Ebert F, Taleshi MS, Francesconi KA, Schwerdtle T. In vitro toxicological characterization of two arsenosugars and their metabolites. Molecular Nutrition & Food Research. 2013;57(7):1270-1282. DOI: 10.1002/mnfr.201200821
86.Organisation for the Prohibition of Chemical Weapons (OPCW). Available from: https://www.opcw.org/about-us [Accessed: March 8, 2023]
87.Muzaffar S, Khan J, Srivastava R, Gorbatyuk MS, Athar M. Mechanistic understanding of the toxic effects of arsenic and warfare arsenicals on human health and environment. Cell Biology and Toxicology. 2023;39(1):85-110. DOI: 10.1007/s10565-022-09710-8
88.Isono O, Kituda A, Fujii M, Yoshinaka T, Nakagawa G, Suzuki Y. Long-term neurological and neuropsychological complications of sulfur mustard and lewisite mixture poisoning in Chinese victims exposed to chemical warfare agents abandoned at the end of WWII. Toxicology Letters. 2018;293:9-15. DOI: 10.1016/j.toxlet.2018.04.017
89.Li C, Srivastava RK, Athar M. Biological and environmental hazards associated with exposure to chemical warfare agents: Arsenicals. Annals of the New York Academy of Sciences. 2016;1378(1):143-157. DOI: 10.1111/nyas.13214
90.Tewari-Singh N, Croutch CR, Tuttle R, Goswami DG, Kant R, Peters E, et al. Clinical progression of ocular injury following arsenical vesicant lewisite exposure. Cutaneous and Ocular Toxicology. 2016;35(4):319-328. DOI: 10.3109/15569527.2015.1127255
91.Manzoor S, Mariappan N, Zafar I, Wei CC, Ahmad A, Surolia R, et al. Cutaneous lewisite exposure causes acute lung injury. Annals of the New York Academy of Sciences. 2020;1479(1):210-222. DOI: 10.1111/nyas.14346
92.Srivastava RK, Traylor AM, Li C, Feng W, Guo L, Antony VB, et al. Cutaneous exposure to lewisite causes acute kidney injury by invoking DNA damage and autophagic response. American Journal of Physiology. 2018;314(6):F1166-F1176. DOI: 10.1152/ajprenal.-00277.2017
93.Negishi T, Matsunaga Y, Kobayashi Y, Hirano S, Tashiro T. Developmental subchronic exposure to diphenylarsinic acid induced increased exploratory behavior, impaired learning behavior, and decreased cerebellar glutathione concentration in rats. Toxicological Sciences. 2013;136(2):478-486. DOI: 10.1093/toxsci/kft200
94.Sasaki S, Negishi T, Tsuzuki T, Yukawa K. Diphenylarsinic acid induced activation of MAP kinases, transcription factors, and oxidative stress-responsive factors and hypersecretion of cytokines in cultured normal human cerebellar astrocytes. Neurotoxicology. 2022;88:196-207. DOI: 10.1016/j.neuro.2021.12.002
95.Ministry of the Environment, Japan. Health Effects from diphenylarsinic Acid (Japanese report, translated by author). 2008. pp. 1-20
Written By
Hiroshi Yamauchi, Takahiko Yoshida and Ayako Takata
Submitted: 20 March 2023Reviewed: 23 March 2023Published: 10 May 2023
 Open access peer-reviewed chapter
Open access peer-reviewed chapter