 Open access peer-reviewed chapter
Open access peer-reviewed chapter
Abstract
The skin, the body’s largest organ, acts as a shield against infections and injuries. The skin has an inherent ability to autoregulate its blood flow, which depends on extrinsic/intrinsic factors. This function is facilitated by a complex regulatory system that includes local regulation of cutanemicrocirculation involving sensory and autonomic fibres. These play important roles in thermoregulation, maintenance of homeostasis, defence, inflammatory response and nutrition. Any structural or functional damage to the microvasculature can lead to an incongruity in the demand and supply either due to physiological or pathological reasons. Besides, the small fibre nerves supplied by the microvessels can suffer from hypoxia, which in turn can cause problems. By understanding these functional aspects and applying this knowledge for assessment, the complex pathophysiological mechanisms of diseases like Raynaud’s and diabetic-foot complications can be better understood. Moreover, microcirculation is crucial for wound healing in both diabetic foot and in pressure ulcers. This chapter aims to discuss the anatomy and physiology of foot microcirculation and its involvement in the pathobiology of certain diseases. Furthermore, various microcirculatory assessment tools and methods are discussed. Acquiring this knowledge can be helpful in providing more effective prevention, diagnosis, and treatment of microcirculatory diseases of the foot.
Keywords
- microcirculation
- foot
- microvessels
- skin
- perfusion
- foot disease
1. Introduction
The microcirculation of the human body plays an important role in the supply of nutrients, protection, elimination of waste products, defence mechanisms and maintaining homeostasis. The skin is the largest and most accessible organ to study microcirculation. The functional aspects of microcirculation are an important factor for foot health for maintaining tissue integrity, responding to noxious and non-noxious stimuli and thermoregulating. There are several pathological conditions in which the foot is adversely affected when the cutaneous microcirculation is compromised. Although microangiopathy, or small vessel disease, is not recognised as a disease in its own right, its involvement in the pathogenesis of diseases such as diabetic foot cannot be denied [1]. An understanding of the structural and functional aspects of microcirculation and the structures, such as small fibre nerves that interact with them, help identify mechanisms through which foot health can be improved. Also, the lack of understanding of complications in the presence of complex diseases such as diabetes can be bridged. This, in turn, will help identify diagnostic tools to assess the foot at risk and develop solutions to treat the foot. This chapter aims to provide an overview of the skin of the foot and the neurovascular interactions in the foot. Additionally, it intends to lay a foundation on the microcirculation of the foot, its assessments and applications in understanding the pathological conditions of the foot using selected diseases as an example.
2. The skin of the foot
The skin is the largest organ of the human body measuring about 2 metres in length. The skin can be either glabrous without hair such as in palmar or plantar surfaces or it can be non-glabrous with hair as found in the hand, feet or other regions of the body. Glabrous skin has highly innervated arteriovenous shunts and plays a major role in thermoregulation [2]. In contrast, non-glabrous hairy skin has fewer arteriovenous shunts and is primarily involved in defence and nutrition [2]. Therefore, the skin has both thermoregulatory and non-thermoregulatory roles to maintain homeostasis and preserve human health. Sweating helps to eliminate waste products and toxins. The different types of sweat glands in the skin aid to hydrate and moisturise the skin by the transportation of water; natural moisturising factors such as lactate, urea, sodium and potassium and antimicrobial peptides to the skin surface [3]. The human skin also contains a rich and diverse population of microbial organisms. Many of these microbes inhabit the follicular structures of the skin and their interactions with host cells lead to changes in cell function [4]. At the same time, the skin acts as a physical barrier to prevent injuries and infections due to external stimuli such as chemicals, water, dust, heat, adverse temperature and microorganisms [5]. Lastly, the skin has an intrinsic ability to auto-regulate its blood flow, which depends on some external or internal factors. Such functions are facilitated by a complex regulatory system that includes local regulation of cutaneous microcirculation involving sensory and autonomic fibres [2].
The skin is highly vascular and it is richly supplied by small blood vessels, which are known as microvessels or microvasculature that are a part of the microcirculatory system. The microvasculature is the network of finer arteries, arterioles, capillaries and venules that supply and drain blood from every tissue and organ in the body (Figure 1). These microvessels lack a muscular layer and their diameter ranges from 5 to 200 μm [6]. Cutaneous microcirculation plays an important role in the exchange of nutrients in the tissue, in the removal of waste products and last but not least in thermoregulation [7]. Cutaneous blood flow can be substantially altered in response to thermal stress. Vasodilation and increased skin blood flow are essential for heat dissipation during exposure to heat and exercise [8]. Similarly, vasoconstriction and decreased skin blood flow to prevent heat loss to protect against hypothermia during exposure to cold are necessary [8]. These skin blood flow mechanisms both local and reflex are controlled by nerves, endothelial derivatives and metabolic factors [8]. Such responses are a vital aspect of normal thermoregulation. These observations demonstrate that skin blood flow is affected by skin temperature and neurovascular interactions [9]. Hence, it could conceivably be hypothesised that vascular changes due to abnormal neuronal control are reflected in the cutaneous thermal changes. Prior studies have noted that the skin temperature on the feet increases in the presence of complications [10, 11]. This may be key to assessing neurovascular deficits and impairment in microcirculation, which will be discussed later in this chapter.
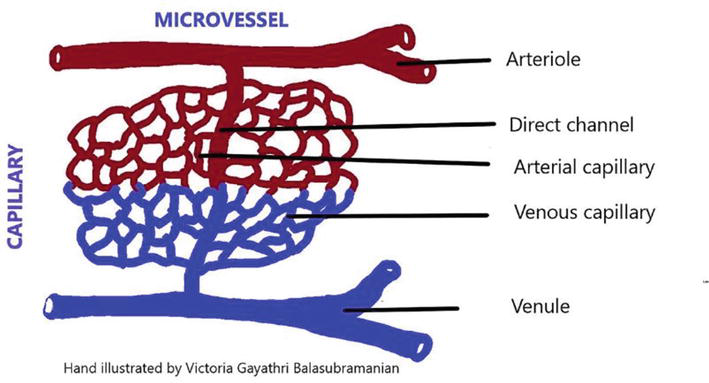
Figure 1.
The microvasculature structure including arterioles, venules and the interconnecting capillaries.
The skin is supplied with both large (>5 μm in diameter) and small fibre nerves (<5 μm in diameter) [12]. The skin’s somatosensory system has three basic types of sensory receptors that respond to external stimuli. First, there are mechanoreceptors that respond to mechanical stimuli such as light touch, vibration, pressure and texture. The commonly known mechanoreceptors are Merkel cells or disks, Meissner corpuscles, Ruffini endings and Pacinian corpuscles [13]. These entities are designed to respond to a specific type of mechanical stimuli. For instance, Meissner corpuscles are large, myelinated fibres that detect low-frequency vibration and are present in glabrous (smooth, hairless) skin on fingertips [13]. Pacinian corpuscles contain A-beta fibres, which are rapidly adapting and are present in the deeper layers of skin, ligaments and joints that respond to high-frequency vibration and deep pressure [13]. The Ruffini endings are slow-adapting, encapsulated receptors present in both the glabrous and hairy skin that responds to skin stretch [14, 15]. Finally, Merkel cells, also known as ‘touch cells’ found in the epidermis of mainly non-glabrous and tactile areas of glabrous skin respond to light touch sensation [16, 17]. Generally, they are low-threshold mechanoreceptors, whilst nociceptors respond to high-threshold stimuli. Second, there are nociceptors found in the skin, joints and viscera that respond to pain induced by a range of factors. Most nociceptors are either C fibres with small diameter unmyelinated axons or A fibres whose axons are myelinated [18, 19, 20]. Nociceptors are sensitive to a noxious (harmful) stimulus or a prolonged stimulus that eventually becomes noxious [19, 20, 21]. There are different types of nociceptors that respond to chemical, thermal and mechanical stimuli and polymodal that respond to all three [19, 20, 22]. Pain medicated by cutaneous nociceptors can be protective in nature. Stimulation and activation of the terminal branches of the sympathetic and nociceptor fibres result in axon reflex-mediated neurogenic inflammatory reaction, sweating and vasodilation [20, 23]. Third, thermoreceptors respond to thermal stimuli. The Krause end bulbs, Ruffini endings and free nerve endings (the warmth sensation has been attributed to C fibres, whereas cold detection is a function of Aδ fibres) are thermoreceptors [24]. These structures help with thermoregulation and offer protection by sensing harmful thermal stimuli.
As discussed above, the skin is richly supplied by microvessels and nerves. The small fibre nerves supply the microvessels. Therefore, the cutaneous microcirculation is regulated according to the responses of the small fibre nerves to various stimuli. For instance, vasodilation and vasoconstriction to thermoregulate based on temperature are mediated by the small fibres that perceive the signal. Likewise, the small fibre nerves are supplied by the microvessels that are essential for nutrition supply. Any damage to these microvessels results in endoneurial hypoxia, which is attributed to the pathogenesis of diabetic neuropathy [25]. Therefore, the small fibres and the microvasculature are in a mutual relationship in which damage to one or the other has serious consequences, such as loss of a protective sensation or failure of thermoregulation. Thus, in the presence of increased physiological stress from physical stress such as injury or infection and chemical stress, any neurovascular dysfunction impairs microcirculation and loss of tissue integrity [26].
3. Assessment of cutaneous microcirculation of the foot
In recent times, the field of medical research has seen a great deal of innovation in technology to facilitate research, diagnosis, and treatment. This also extends to the area of microcirculation and these microcirculation assessment methods can be categorised into Non-imaging and imaging techniques (Figure 2).
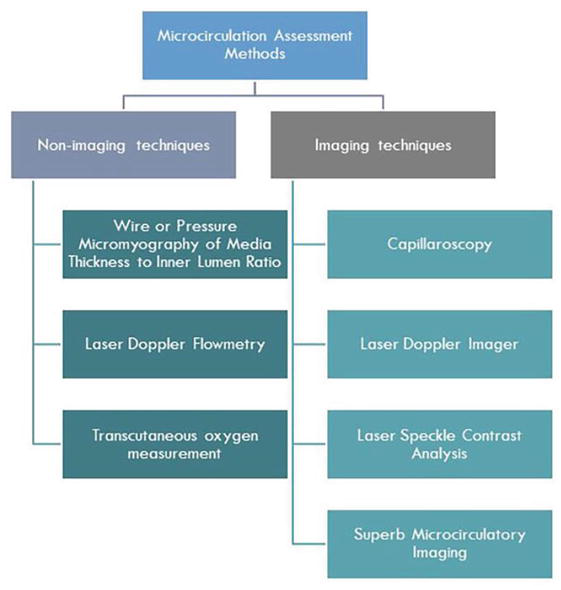
Figure 2.
Microcirculation assessment methods and the two categories of imaging and non-imaging techniques.
Previously, the gold standard method for assessing microcirculation was wire or pressure micromyography of the media thickness to inner lumen ratio (MLR) of subcutaneous small resistance arteries obtained from local biopsies [27]. There is evidence that increased MLR is associated with a poorer prognosis for conditions such as diabetes and hypertension. A reduction in the vascular density in the most distal part of the microcirculation, namely arterioles (100 μm to 7 μm in diameter) and capillaries (around 7 μm in diameter), has been observed in hypertension, diabetes and obesity [27, 28, 29, 30, 31]. Conventionally Ankle Brachial Index (ABI) and Toe Brachial Index (TBI) have been used for the diagnosis of peripheral arterial disease (PAD) related to the foot. ABI is an objective diagnostic method but it is considered to be less reliable in cases where the arteries may be calcified as in diabetes, therefore, it is resistant to compression [32, 33]. In such cases, TBI may be used [33, 34, 35]. Segmental blood pressure (SEGP) measurements taken at the thigh, calf and ankle are also used to assess PAD, but there are conflicting opinions about its utility [36, 37, 38]. However, both ABI and TBI are microcirculatory measurements and do not help to assess the microcirculatory issues. However, recently there are many advanced technologies for non-invasive assessment of microcirculation and neurovascular responses.
3.1 Technologies to assess skin microcirculation
There are currently different devices available to assess microcirculation non-invasively such as laser Doppler flowmetry or fluxmetry (LDF) system, laser Doppler imager (LDI) or laser Doppler perfusion imager (LDPI), laser speckle contrast imager (LSCI) or laser speckle contrast analysis (LASCA), superb microcirculatory imaging (SMI) and transcutaneous oxygen measurement (tcpO2).
3.1.1 Laser Doppler flowmetry or fluxmetry system
An LDF is a device that allows a non-invasive method to monitor changes in the cutaneous peripheral microcirculation [39]. It uses a monochromatic low-energy laser beam penetrating the tissue [39]. The LDF then detects the movement of the red blood cells (RBCs) in the peripheral microcirculation. Despite the depth to which the laser penetrates being relatively shallow (∼1 mm), it is a useful tool for assessing cutaneous microcirculation and its related disorders [40, 41]. However, there are a few disadvantages. Firstly, there may be high spatial variability in the perfusion values because of the regional heterogeneity of skin perfusion and the small measurement area that depends on the contact surface area of single-point LDF probes. This gives a relatively poor reproducibility of the single-point LDF technique [42, 43, 44]. Secondly, there may be movement-related artefacts from the attached probes or participants that interfere with the measurements [45, 46]. Thirdly, it is a contact technique and therefore requires the positioning of a probe on the tissues that limit perfusion monitoring of injuries such as an ulcer [42].
3.1.2 Laser Doppler Imager or Laser Doppler Perfusion Imager
The LDI or LDPI uses a contactless imaging technique. LDPI uses a special scanner head and a coherent laser light hits the tissue surface from a distance of about 15 cm [44]. A perfusion image is a collection of LDF points (pixels) arranged on a colour-coded map showing areas of low and high perfusion [42, 44]. The LDPI is useful to monitor perfusion changes for a variety of conditions in dermatology, ulcers, burns, skin grafts, Raynaud’s syndrome, and cerebral measurements [44, 47, 48, 49, 50, 51, 52]. Nevertheless, there are some limitations to the technique. For instance, LDPI requires long acquisition periods, which prevents the study of rapid changes in perfusion when the surface area to scan is large [42].
3.1.3 Laser speckle contrast imager or laser speckle contrast analysis
LSCI is a technique based on the dynamic changes that occur when a tissue is illuminated with coherent light, forming a speckle pattern at the detector, which is the backscattered light as a result of its interaction with RBCs [41, 53]. It can be used as a tool to capture high-resolution blood flow images, visualise perfusion in various tissues and has a wide range of applications, including both non-real-time investigations and real-time intraoperative perfusion monitoring [53, 54]. A limitation of the LSCI is that it is extremely sensitive to motion, and it can detect the minute movements of RBCs. However, different technical and environmental conditions may interfere with microvascular recordings [42]. When there is external noise, the unwanted motion artefacts are inherent in the measured signal and cannot be easily separated [53]. A simple precautionary step against motion artefacts might be able to create a distraction-free and quiet environment for the patient and overcome the challenge of movement artefacts [42]. Based on the consideration that the speckle contrast of the opaque surface only contains information about unwanted movement and not about perfusion, researchers Mahé et al. [42] added an adhesive opaque patch within the field of view. The contrast measured on the exposed skin contains information about both the blood flow and unwanted movement and when the opaque surface contrast is subtracted, with the addition of a linearity correction, only perfusion remains [53].
3.1.4 Superb Microcirculatory Imaging
More recently, there is an SMI ultrasound technique that expands the range of visible blood flow and allows visualization of low microvascular flow. Compared to traditional Doppler technologies, the advantages of SMI are known for providing high frame rates, resolution and sensitivity with fewer motion artefacts [55, 56]. Unlike traditional colour and power Doppler technologies, which eliminate clutter by suppressing low-velocity components, resulting in data loss and consequently reduced visibility of blood flow in smaller vessels, SMI separates these flow signals from overlying tissue motion artefacts while components with low flow rate and provide detail and definition [55]. Also, it uses clutter motion and uses an adaptive algorithm to identify and remove tissue motion and show a more accurate representation of blood flow. This results in a high-resolution ultrasound image in which minute vessels and low-velocity flows can be demonstrated [55, 56]. The device appears to have applications where visualization of the smallest vessels is required such as when evaluating lesions, cysts, inflammatory diseases, tumours, PAD and foot diseases [55, 56, 57].
3.1.5 Transcutaneous oxygen measurement
Apart from the above techniques, transcutaneous oxygen measurement (tcpO2) is a simple, non-invasive method that allows the assessment of the amount of oxygen that diffuses from the capillaries through the epidermis to the electrode and thus provides an estimate of the functional ability of the microvessels to deliver oxygen to the tissue and understand the ischaemic status [58]. Measurement of TcPO2 allows the determination of tissue oxygen tension and can help understand tissue perfusion as it can be performed in people with arterial calcification and no pedal pulse [59, 60]. Therefore, TcPO2 measurement can be useful in evaluating wound healing, especially in people with ulcers in relation to diabetic foot disease [58].
3.2 Tests to assess the skin microcirculation capacity
The different devices and techniques available for monitoring and imaging microcirculation were discussed above. In addition to this, it is important to note that there is a range of provocation tests used to study microcirculation. Some of the commonly used stimuli are pressure, heat stress, cold stress, chemicals (iontophoresis) and postural changes. There is usually a before and after measurement whilst using these stimuli to understand the microcirculatory changes that have occurred. Based on the outcome of interest and the physiological or pathological condition under study, these measurements may help to gain an understanding of the microcirculatory aspects at the region of interest. A select few of these tests are briefly discussed below.
3.2.1 Post-occlusive reactive hyperemia
Post-occlusive reactive hyperemia (PORH) uses occlusion as a stimulus and it is known to be primarily an endothelial-dependent process, however, it involves both endothelial-dependent and independent mechanisms [61, 62]. It helps to assess reperfusion after an occlusion, which is a testing of the tissue’s intrinsic ability. The hyperemic response is generated because of shear stress, the tangential frictional force acting at the endothelial cell surface caused by arterial occlusion [63]. The endothelium releases vasodilating substances in response to the mechanical stimulus, which in this case is occlusive pressure [61]. Several factors are known to contribute to vasodilation, which are myogenic, neurogenic, humoral and other local factors such as potassium ions, hydrogen ions, carbon dioxide, catecholamines, prostaglandins and adenosine [61, 62]. It is well known that endothelial nitric oxide and other endothelium-derived agents such as prostaglandins and endothelium-derived hyperpolarising factors play a role in the mechanism of PORH [63]. Apart from these substances, the sensory nerves contribute to the PORH mechanism, which makes this test suitable to assess neurovascular responses [20, 62, 63, 64, 65, 66, 67]. The test involves recording a baseline reading, followed by an occlusion using supra systolic pressure (~180 to 220 mmHg) for a certain period and release of pressure. The protocols widely vary depending on various factors such as region of interest, pre-existing complications and outcomes of interest [63]. However, the more recent literature suggests that PORH can be measured reliably using an occlusion time of as little as 30 seconds [63]. PORH is a quick, easy and useful method to assess microcirculation in the arms and feet. PORH is known to be an indicator of cardiovascular risks and foot complications [62, 68, 69]. Therefore, its potential applications could be in the area of risk assessment, which needs further research.
3.2.2 Laser Doppler Imager Flare
Thermal stress tests can be useful to assess microcirculation. The LDI flare test induces nociceptive stimuli-mediated vasodilation and a neurogenic flare through an axon reflex response involving the C-fibres [20]. The LDI flare area, or the size of the area with a hyperemic response, is known to reflect C-fibre function, and the cutaneous perfusion changes immediately below the heating probe reflect the non-neurogenic components involved and can reflect endothelial function in response to heat [20, 70, 71, 72]. The test involves heating the local area of the skin to 44°C for 20 minutes or 6 minutes in a stepwise fashion (44°C for 2 minutes, 46°C for 1 minute and finally 47°C for 3 minutes) in a temperature-controlled environment to evoke the flare, followed by scanning of the site using an LDI to measure the area [38, 39, 54]. The 6 minutes protocol is known to produce a significantly larger and more consistent response [72, 73]. The test can be used to assess microcirculatory impairments. Evidence suggests that reduced neurogenic flare along with microcirculatory dysfunction is observed when assessing using the LDI flare test in people with diabetes [70, 72, 74].
3.2.3 Cold stress test
Similar to heat stress, cold stress can also be used to assess microcirculation. The afferent nerves that mediate pain and thermal perception in the skin and the sympathetic efferent vasoconstrictor aspect are involved in the response. The microcirculatory response to a cold stress test might reflect a sympathetic vasoconstrictor and protective vasodilator events [75, 76]. Initial exposure to cold induces cutaneous vasoconstriction, manifested by reduced cutaneous perfusion, but prolonged exposure to cold increases the perfusion, which is a protective hyperemic vasodilator mechanism [8, 76, 77]. The test usually involves a baseline period, followed by exposure to cold (~8°C) for a specified time, followed by a time taken for the temperature to return to room temperature for 20 minutes [75]. The protocols widely vary based on the region of interest, the purpose of the study and the outcomes measured. The cold provocation test is commonly used to study Raynaud’s phenomenon, systematic sclerosis, neurovascular changes in diabetes and other conditions [20, 78, 79, 80]. The microcirculatory response to cold stress is known to be impaired in people with diabetes [20, 81, 82].
3.2.4 Skin perfusion pressure
The skin perfusion pressure (SPP) is the blood pressure required to restore microcirculatory or capillary flow after controlled occlusion and subsequent flow return. SPP is measured by gradually reducing the inflation cuff pressure and observing isotope washout, the reappearance of pulsatile flow or the movement of RBCs at the measurement site [83, 84]. The minimum external counter pressure exerted by the pressure cuff on the underlying skin is the SPP, above which skin perfusion ceases [83, 84]. It is measured using various techniques but if using LDF the laser Doppler probe is placed beneath a 5.8-cm-wide blood pressure cuff [83]. However, revascularization to restore perfusion is critical for the treatment and prevention of ischemic ulcers in different clinical guidelines. Studies have shown that the test is beneficial for the diagnosis of critical limb ischemia [85, 86, 87]. It also helps to assess the limbs for revascularisation procedures to restore perfusion for the treatment and prevention of ischemic ulcers [84]. In addition, SPP is known to serve as an effective guide for amputation-level decisions and for assessing wound healing [83, 84, 88]. However, since there is no consensus in the existing literature, the cut-off value for the diagnosis of various vascular conditions and the potential of SPP as a screening and diagnostic tool in routine practice need to be determined.
4. Microcirculation and select pathological conditions
Assessing the microcirculation of the foot can be helpful in various pathological conditions. Microcirculation plays an important role not only in maintaining homeostasis and tissue integrity but also in tissue injury and response [41]. Acquiring in-depth knowledge of microcirculatory mechanisms can help to explore core issues in various pathological mechanisms. Microcirculatory aspects may be a missing link in understanding complex cutaneous problems and forging solutions. Especially with developing technologies as discussed above, microcirculatory investigations are more accessible. In this chapter, two pathological conditions are discussed briefly in relation to microcirculation.
4.1 Microcirculation in Raynaud’s phenomenon
Raynaud’s phenomenon is a functional vascular disease presenting with recurrent episodes of limb ischemia in response to cold and emotional stress [89]. Normally, in response to cold temperatures, the body adapts by restricting blood flow to the skin, through a thermoregulatory mechanism to prevent further loss of body heat and maintain core body temperature [90, 91]. However, in Raynaud’s phenomenon, a restriction in blood flow, an increase in alpha-2 adrenergic sensitivity in the digital and cutaneous vessel and vasoconstriction of the arteries of the fingers and skin arterioles occur during cold temperatures and emotional stress [89, 90]. Raynaud’s phenomenon can be primary or secondary. While the Raynaud’s primary phenomenon is idiopathic, the secondary phenomenon is associated with different aetiologies like connective tissue disorders, such as scleroderma, systemic lupus erythematosus, Sjogren syndrome, drugs antimigraine medications, interferon alpha and beta, cyclosporine, and nonselective beta-blockers, and infections, such as parvovirus B19, cytomegalovirus, hepatitis B, and hepatitis C [89, 90]. The investigation of the cutaneous microcirculation can be an important tool for understanding the complex neuro-immunovascular interactions involving both the autonomic and sensory nervous systems in Raynaud’s phenomenon [89]. Early diagnosis can help with planning treatment for a better prognosis. There are studies that utilised non-invasive techniques such as LDF and LASCA to understand the underlying pathophysiological mechanisms in Raynaud’s phenomenon in order to develop management strategies [89, 92].
4.2 Microcirculation and diabetic foot disease
Diabetes is a chronic disease that leads to various microcirculatory complications in the eyes, kidneys and feet. Diabetic foot syndrome is one of the most common complications of diabetes. Damage to the soft tissue structure is one of the main causes of diabetic foot ulcers, which can be caused by the interaction of several factors such as vascular disease, neuropathy and trauma [41, 93]. Both structural and functional damages to the microvasculature have been linked to diabetes [62, 94]. This can lead to complications in microcirculation, which plays an important role in tissue injury and inflammation [41]. Previous research suggested that certain microcirculatory responses like pressure-induced vasodilation protect the skin and their impairment may contribute to an increased risk of occlusive and ischemic foot injuries [20, 95, 96]. Understanding and studying complex neurovascular responses in the foot can aid in the prevention and early detection of diabetic foot disease and prevent adverse complications such as ulcers and amputations.
5. Conclusion
This chapter provided an overview of the microcirculation of the foot, the structural and functional aspects. Key concepts for understanding microcirculatory functions such as neurovascular interactions were discussed. The chapter also gave a brief overview of different technologies and methods to assess microcirculation, especially in the foot. A selected number of pathological conditions and the relevance of understanding the microcirculation in these conditions were also highlighted. In summary, microvasculature fulfils various roles and forms an important aspect of maintaining skin integrity and homeostasis. It also forms a major part of thermoregulation and tissue injury response mechanisms. Therefore, the growing body of knowledge in the field of microcirculation can offer not only diagnostic but also prognostic solutions for foot health.
Acknowledgments
The authors would like to acknowledge the Staffordshire University Research studentship obtained by the first author, which supported this study.
Conflict of interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Thanks
The authors would like to thank the Centre for Biomechanics and Rehabilitation Technologies, Staffordshire University for the support.
References
- 1.
Tesfaye S, Gill G. v. Small vessel disease: A cause of foot ulceration in the neuropathic foot? Practical Diabetes International. 1997; 14 (3):78-79 - 2.
Stirban A. Microvascular dysfunction in the context of diabetic neuropathy. Current Diabetes Reports. 2014; 14 (11):1-9 - 3.
Baker LB. Physiology of sweat gland function: The roles of sweating and sweat composition in human health. Temperature: Multidisciplinary Biomedical Journal. 2019; 6 (3):211. Available from:/pmc/articles/PMC6773238/ - 4.
Gallo RL. Human skin is the largest epithelial surface for interaction with microbes. Journal of Investigative Dermatology. 2017; 137 (6):1213. Available from:/pmc/articles/PMC5814118/ - 5.
Natsuga K. Epidermal barriers. Cold Spring Harbor Perspective Medicine. 2014; 4 (4). Available from:/pmc/articles/PMC3968788/ - 6.
Yamaguchi T, Ishikawa T, Imai Y. Integrated Nano-biomechanics. New York, USA: Elsevier; 2018. pp. 1-297 - 7.
Boulton AJ, Cavanagh PR, Rayman G, Wukich DK. The Foot in Diabetes. Newark: John. In: Boulton AJ, Cavanagh PR, Rayman G, editors. 5th ed. Newark: John Wiley & Sons, Incorporated; 2020. pp. 89-138 - 8.
Charkoudian N. Skin Blood Flow in Adult Human Thermoregulation: How It Works, When It Does Not, and Why. Mayo Clinic Proceedings. 2003; 78 (5):603-612 Available from:https://www.sciencedirect.com/science/article/abs/pii/S0025619611619307 - 9.
Fromy B, Abraham P, Bouvet C, Bouhanick B, Fressinaud P, Saumet JL. Early decrease of skin blood flow in response to locally applied pressure in diabetic subjects. Diabetes. 2002; 51 (4):1214-1217 Available from:http://ezproxy.staffs.ac.uk/login?url=http://search.ebscohost.com/login.aspx?direct=true&db=cmedm&AN=11916947&site=ehost-live - 10.
Bharara M, Cobb JE, Claremont DJ. Thermography and Thermometry in the Assessment of Diabetic Neuropathic Foot: A Case for Furthering the Role of Thermal Techniques. The International Journal of Lower Extremity Wounds. 2006; 5 (4):250-260 Available from:http://journals.sagepub.com/doi/10.1177/1534734606293481 - 11.
Gatt A, Falzon O, Cassar K, Ellul C, Camilleri KP, Gauci J, et al. Establishing differences in thermographic patterns between the various complications in diabetic foot disease. International Journal of Endocrinology. 2018; 2018 :1-7 Available from:https://www.hindawi.com/journals/ije/2018/9808295/ - 12.
Agostini T, de Scisciolo G, Lazzeri D, Almesberger D, Mori A, Cassardo A, et al. Laser-evoked potentials as a novel tool for sensibility assessment following inferior pedicle breast reduction. European Journal of Plastic Surgery. 2013; 36 (7):423-430 - 13.
Bajwa a KY. Physiology, Vibratory Sense. StatPearls; 2019 Available from: https://www.statpearls.com/ArticleLibrary/viewarticle/31519 - 14.
Maeda T, Ochi K, Nakakura-Ohshima K, Youn SH, Wakisaka S. The Ruffini ending as the primary mechanoreceptor in the periodontal ligament: Its morphology, cytochemical features, regeneration, and development. Critical Reviews in Oral Biology and Medicine. 1999; 10 (3):307-327 Available from:https://pubmed.ncbi.nlm.nih.gov/10759411/ - 15.
Cobo R, García-Piqueras J, Cobo J, Vega JA. The Human Cutaneous Sensory Corpuscles: An Update. Journal of Clinical Medicine. 2021; 10 (2):227 Available from:https://www.mdpi.com/2077-0383/10/2/227/htm - 16.
Barbieri JS, Wanat K, Seykora J. Skin: Basic structure and function. Pathobiology of Human Disease: A Dynamic Encyclopedia of Disease Mechanisms. 2014; 2014 :1134-1144 - 17.
Eduardo CJ, Thomas B, Alexander JL, Steven B. McKee’s Pathology of the Skin. 5th ed. Vol. 51. New York: Elsevier; 2019. Available from: https://www.us.elsevierhealth.com/mckees-pathology-of-the-skin-9780702069833.html - 18.
Djouhri L, Lawson SN. Aβ-fiber nociceptive primary afferent neurons: A review of incidence and properties in relation to other afferent A-fiber neurons in mammals. In: Brain Research Reviews. 2004. pp. 131-145 - 19.
Dubin AE. Patapoutian A. Nociceptors: The sensors of the pain pathway. Journal of Clinical Investigation. 2010; 120 :3760-3772 - 20.
Balasubramanian G, Vas P, Chockalingam N, Naemi R. A synoptic overview of neurovascular interactions in the foot. Frontiers in Endocrinology (Lausanne). 2010; 11 :308 Available from:https://www.frontiersin.org/article/10.3389/fendo.2020.00308/full - 21.
Gangadharan V, Kuner R. Pain hypersensitivity mechanisms at a glance. Vol. 6. DMM Disease Models and Mechanisms. In: Company of Biologists. 2013. pp. 889-895 - 22.
Pinho-Ribeiro FA, Verri WA, Chiu IM. Nociceptor Sensory Neuron–Immune Interactions in Pain and Inflammation. Trends Immunol. Elsevier Ltd; Jan 2017; 38 (1):5-19. DOI: 10.1016/j.it.2016.10.001. Epub 2016 Oct 25. PMID: 27793571; PMCID: PMC5205568 - 23.
Gibbons CH, Wang N, Freeman R. Capsaicin induces degeneration of cutaneous autonomic nerve fibers. Annals of Neurology. 2010; 68 (6):888-898 - 24.
Torebjörk E, Schmelz M. Chapter 38 single-unit recordings of afferent human peripheral nerves by microneurography. In: Dyck PJ, Thomas PK, editors. Peripheral Neuropathy. 4th ed. Pennsylvania, USA: W.B. Elsevier Saunders; 2005. pp. 1003-1014 - 25.
Körei AE, Istenes I, Papanas N, Kempler P. Small-fiber neuropathy: A diabetic microvascular complication of special clinical, diagnostic, and prognostic importance. Angiology. 2016; 67 (1):49-57 Available from:http://journals.sagepub.com/doi/10.1177/0003319715583595 - 26.
Levy BI, Schiffrin EL, Mourad JJ, Agostini D, Vicaut E, Safar ME, et al. Impaired tissue perfusion: A pathology common to hypertension, obesity, and diabetes mellitus. Circulation. 2008; 118 (9):968-976 Available from:https://pubmed.ncbi.nlm.nih.gov/18725503/ - 27.
Rizzoni D, Mengozzi A, Masi S, Rosei CA, de Ciuceis C, Virdis A. New noninvasive methods to evaluate microvascular structure and function. Hypertension. 2022; 79 (5):874-886 Available from:https://www.ahajournals.org/doi/abs/10.1161/HYPERTENSIONAHA.121.17954 - 28.
Agabiti-Rosei E, Rizzoni D. Microvascular structure as a prognostically relevant endpoint. Journal of Hypertension. 2017; 35 (5):914-921 Available from:https://pubmed.ncbi.nlm.nih.gov/28355167/ - 29.
Agabiti-Rosei R, Rizzoni D. The effects of hypertension on the structure of human resistance arteries. In: Lip GY, Hall JE, editors. Comprehensive Hypertension. Philadelphia: Elsevier Mosby; 2007. pp. 579-570 - 30.
Rizzoni D, Rosei EA. Small artery remodeling in diabetes mellitus. Nutrition, Metabolism, and Cardiovascular Diseases. 2009; 19 (8):587-592 Available from:https://pubmed.ncbi.nlm.nih.gov/19481431/ - 31.
de Ciuceis C, Rossini C, Porteri E, la Boria E, Corbellini C, Mittempergher F, et al. Circulating endothelial progenitor cells, microvascular density and fibrosis in obesity before and after bariatric surgery. Blood Pressure. 2013; 22 (3):165-172. Available from:https://pubmed.ncbi.nlm.nih.gov/23286244/ - 32.
Suominen V, Rantanen T, Venermo M, Saarinen J, Salenius J. Prevalence and risk factors of PAD among patients with elevated ABI. European Journal of Vascular and Endovascular Surgery. 2008; 35 (6):709-714 Available from:https://pubmed.ncbi.nlm.nih.gov/18313338/ - 33.
Park SC, Choi CY, Ha YI, Yang HE. Utility of Toe-brachial index for diagnosis of peripheral artery disease. Archieves in Plastic Surgery. 2012; 39 (3):227. Available from:/pmc/articles/PMC3385338/ - 34.
Hyun S, Forbang NI, Allison MA, Denenberg JO, Criqui MH, Ix JH. Ankle Brachial Index, Toe Brachial Index, and cardiovascular mortality in participants with and without diabetes mellitus. Journal of Vascular Surgery. 2014; 60 (2):390. Available from:/pmc/articles/PMC4112146/ - 35.
Høyer C, Sandermann J, Petersen LJ. The toe-brachial index in the diagnosis of peripheral arterial disease. Journal of Vascular Surgery. 2013; 58 (1):231-238 Available from:https://www.sciencedirect.com/science/article/pii/S0741521413007106 - 36.
Gale SS, Scissons RP, Salles-Cunha SX, Dosick SM, Whalen RC, Pigott JP, et al. Lower extremity arterial evaluation: Are segmental arterial blood pressures worthwhile? Journal of Vascular Surgery. 1998; 27 (5):831-839 Available from:http://www.jvascsurg.org/article/S0741521498702629/fulltext - 37.
Hirai M, Shionoya S. Segmental blood pressure of the leg and its clinical use. The Japanese Journal of Surgery. 1978; 8 (2):102-110 Available from:https://pubmed.ncbi.nlm.nih.gov/682389/ - 38.
Gebuhr P, Soelberg M, Henriksen JH. Segmental blood pressure after total hip replacement. Orthopedics. 1992; 15 (4):488-490 - 39.
Sarnik S, Hofirek I, Sochor O. Laser Doppler fluxmetry. Biomedical Papers of the Medical Faculty of the University Palacky, Olomouc, Czech Republic. 2007; 151 (1):143-146 Available from:https://pubmed.ncbi.nlm.nih.gov/17690759/ - 40.
Mrowietz C, Franke RP, Pindur G, Sternitzky R, Jung F, Wolf U. Evaluation of Laser-Doppler-Fluxmetry for the diagnosis of microcirculatory disorders. Clinical Hemorheological Microcirculation. 2019; 71 (2):129-135. Available from:https://pubmed.ncbi.nlm.nih.gov/30584124/ - 41.
Balasubramanian G, Chockalingam N, Naemi R. The role of cutaneous microcirculatory responses in tissue injury, inflammation and repair at the foot in diabetes. Frontiers in Bioengineering and Biotechnology. 14 Sep 2021; 9 :732-753. DOI: 10.3389/fbioe.2021.732753. Available from:https://www.frontiersin.org/articles/10.3389/fbioe.2021.732753/full - 42.
Mahé G, Durand S, Humeau-Heurtier A, Leftheriotis G, Abraham P. Impact of experimental conditions on noncontact laser recordings in microvascular studies. Microcirculation. 2012; 19 (8):669-675 Available from:https://onlinelibrary.wiley.com/doi/full/10.1111/j.1549-8719.2012.00205.x ;https://pubmed.ncbi.nlm.nih.gov/22708898/ - 43.
Tenland T, Salerud EG, Nilsson GE, Oberg PA. Spatial and temporal variations in human skin blood flow. International Journal of Microcirculation, Clinical and Experimental. 1983; 2 (2):81-90 - 44.
O’Doherty J, McNamara P, Clancy NT, Enfield JG, Leahy MJ. Comparison of instruments for investigation of microcirculatory blood flow and red blood cell concentration. 2009; 14 (3):4025. Available from:https://www.spiedigitallibrary.org/journals/journal-of-biomedical-optics/volume-14/issue-3/034025/Comparison-of-instruments-for-investigation-of-microcirculatory-blood-flow-and/10.1117/1.3149863.full - 45.
Välisuo PO. Optical methods for assessing skin flap survival. In: Meglinski I, editor. Biophotonics for Medical Applications. Sawston, Cambridge: Woodhead Publishing; 2015; pp. 331-346 - 46.
Gupta AK, Gelb AW. Essentials of neuroanesthesia and neurointensive care: A volume in essentials of anesthesia and critical care. Essentials of Neuroanesthesia and Neurointensive Care: A Volume in Essentials of Anesthesia and Critical Care. 2008; 2008 :1-344 Available from:http://www.sciencedirect.com:5070/book/9781416046530/essentials-of-neuroanesthesia-and-neurointensive-care - 47.
Raabe A, van de Ville D, Leutenegger M, Szelényi A, Hattingen E, Gerlach R, et al. Laser Doppler imaging for intraoperative human brain mapping. Neuroimage. 2022; 44 (4):1284-1289. Available from:https://pubmed.ncbi.nlm.nih.gov/19049824/ - 48.
Kanetaka T, Komiyama T, Onozuka A. Laser Doppler skin perfusion pressure in the assessment of Raynaud’s phenomenon. TME Journal. 2023:414-416. Available from: https://www.sciencedirect.com/science/article/pii/S1078588403005963 - 49.
Jeng J, Bridgeman A, Shivnan L, Burns PT. Laser Doppler Imaging Determines need for Excision and Grafting in Advance of Clinical Judgment: A Prospective Blinded Trial. Burns. Elsevier; Nov 2003; 29 (7):665-670. DOI: 10.1016/s0305-4179(03)00078-0. PMID: 14556723. Available from:https://www.sciencedirect.com/science/article/pii/S0305417903000780?casa_token=hGw2dMJWBT8AAAAA:Br747hbuISSvzOnk8CE7kl1RMqs8NUa1j9TEAHPpotgMyWHmlyYR6sIYkw4xfd0OwkD-iJhd - 50.
Malanin K, Havu VK, Kolari PJ. Dynamics of cutaneous laser doppler flux with concentration of moving blood cells and blood cell velocity in legs with venous ulcers and in healthy legs. Angiology. 2004; 55 (1):37-42 - 51.
Stü M, Springer C, Paech V, Hermes N, Hoffmann M, Altmeyer P. Increased laser Doppler flow in skin tumors corresponds to elevated vessel density and reactive hyperemia. Wiley Online Library. 2006; 12 (1):1-6. Available from:https://onlinelibrary.wiley.com/doi/abs/10.1111/j.0909-725X.2006.00139.x?casa_token=mIam84FT4SAAAAAA:SfKLNIp_Tfc0g9x8Xhw2N7WEjeCgCZJRGipZvpdtk1u1wf6CLYfRHAT9JYTuxKgLYq7eEpiVSah - 52.
Ilias MA, Wårdell K, Stü Cker M, Anderson C, Salerud EG. Assessment of pigmented skin lesions in terms of blood perfusion estimates. Wiley Online Library. 2004; 10 (1):43-49 Available from:https://onlinelibrary.wiley.com/doi/abs/10.1111/j.1600-0846.2004.00052.x?casa_token=6Lu8iDg4PYwAAAAA:n89b1sZ0rEAthgxB5seLVXrlBxYXzgDr6r3yyCojuhGuy4nSOXTxmOMJTndIFctylF6EtChOMFrV - 53.
Heeman W, Steenbergen W, van Dam GM, Boerma EC, Heeman W. Clinical applications of laser speckle contrast imaging: A review. Journal of Biomedical Optics. 2019; 24 (8):080901 Available from:https://www.spiedigitallibrary.org/journals/journal-of-biomedical-optics/volume-24/issue-8/080901/Clinical-applications-of-laser-speckle-contrast-imaging-a-review/10.1117/1.JBO.24.8.080901.full - 54.
Mangraviti A, Volpin F, Cha J, Cunningham SI, Raje K, Brooke MJ, et al. Intraoperative laser speckle contrast imaging for real-time visualization of cerebral blood flow in cerebrovascular surgery: Results from pre-clinical studies. Scientific Reports. 2020; 10 (1):1-13 Available from:https://www.nature.com/articles/s41598-020-64492-5 - 55.
Toshiba America Medical Systems. Superb Microvascular Imaging. Tustin: Toshiba America Medical Systems; 2017 Available from: http://www.medical.toshiba.com/ - 56.
Fu Z, Zhang J, Lu Y, Wang S, Mo X, He Y, et al. Clinical applications of superb microvascular imaging in the superficial tissues and organs: A systematic review. Academic Radiology. 2021; 28 (5):694-703 Available from:http://www.academicradiology.org/article/S1076633220301781/fulltext - 57.
Suto Y, Sato W, Yamanaka T, Unuma M, Kobayashi Y, Aokawa M, et al. Utility of superb microvascular imaging in the assessment of foot perfusion in patients with critical limb ischemia. Diagnostics. 2022; 12 (11) - 58.
Yip WL. Evaluation of the clinimetrics of transcutaneous oxygen measurement and its application in wound care. International Wound Journal. 2015; 12 (6):625. Available from:http://pmc/articles/PMC7950484/ - 59.
Allen PI, Goldman M. Skin blood flow: A comparison of transcutaneous oximetry and laser Doppler flowmetry. European Journal of Vascular Surgery. 1987; 1 (5):315-318 Available from:http://ezproxy.staffs.ac.uk/login?url=http://search.ebscohost.com/login.aspx?direct=true&db=cmedm&AN=2971577&site=ehost-live - 60.
Cooper K, Majdalany BS, Kalva SP, Chandra A, Collins JD, Francois CJ, et al. ACR Appropriateness Criteria ® Lower Extremity Arterial Revascularization—Post-Therapy Imaging. Journal of the American College of Radiology. 2018; 15 (5):S104-S115. DOI: 10.1016/j.jacr.2018.03.011 - 61.
Wierzbowska J, Wojtkiewicz S, Zbieć A, Wierzbowski R, Liebert A, Maniewski R. Prolonged postocclusive hyperemia response in patients with normal-tension glaucoma. Medical Science Monitor. 2014; 20 :2607-2616 Available from:http://ezproxy.staffs.ac.uk/login?url=http://search.ebscohost.com/login.aspx?direct=true&db=cmedm&AN=25502623&site=ehost-live - 62.
Lanting SM, Barwick AL, Twigg SM, Johnson NA, Baker MK, Chiu SK, et al. Post-occlusive reactive hyperaemia of skin microvasculature and foot complications in type 2 diabetes. Journal of Diabetes and its Complications. 2017; 31 (8):1305-1310. DOI: 10.1016/j.jdiacomp.2017.05.005 - 63.
Balasubramanian G, Chockalingam N, Naemi R. A systematic evaluation of cutaneous microcirculation in the foot using post-occlusive reactive hyperemia. Microcirculation. 2021; 28 (5):e12692. Available from:http://www.ncbi.nlm.nih.gov/pubmed/33655651 - 64.
Lorenzo S, Minson CT. Human cutaneous reactive hyperaemia: Role of BKCa channels and sensory nerves. Journal of Physiology. 2007; 585 (Pt 1):295-303. Available from:http://www.ncbi.nlm.nih.gov/pubmed/17901123 - 65.
Marche P, Dubois S, Abraham P, Parot-Schinkel E, Gascoin L, Humeau-Heurtier A, et al. Neurovascular microcirculatory vasodilation mediated by C-fibers and Transient receptor potential vanilloid-type-1 channels (TRPV 1) is impaired in type 1 diabetes. Scientific Reports. 2017; 7 (1). Available from:http://www.nature.com/articles/srep44322 - 66.
Larkin SW, Williams TJ. Evidence for sensory nerve involvement in cutaneous reactive hyperemia in humans. Circulation Research. 1993; 73 (1):147-154 Available from:https://www.ahajournals.org/doi/10.1161/01.RES.73.1.147 - 67.
Barwick AL, Tessier JW, de Jonge X, Ivers JR, Chuter VH. Peripheral sensory neuropathy is associated with altered postocclusive reactive hyperemia in the diabetic foot. BMJ Open Diabetes Research & Care. 2016; 4 (1):e000235-e000235 Available from:http://drc.bmj.com/lookup/doi/10.1136/bmjdrc-2016-000235 - 68.
Bittner HB, Diemel KD, Friedel N, Stengele B, Hetzer R. Skin microcirculation and Laser Doppler blood flow in patients supported by the Berlin heart biventricular assist device. Vasa - Journal of Vascular Diseases. 1992; 21 (2):149-153 - 69.
Yamamoto-Suganuma R, Aso Y. Relationship between post-occlusive forearm skin reactive hyperaemia and vascular disease in patients with Type 2 diabetes-a novel index for detecting micro- and macrovascular dysfunction using laser Doppler flowmetry. Diabetic Medicine. 2009; 26 (1):83-88. Available from:http://doi.wiley.com/10.1111/j.1464-5491.2008.02609.x - 70.
Green AQ , Krishnan S, Finucane FM, Rayman G. Altered C-fiber function as an indicator of early peripheral neuropathy in individuals with impaired glucose tolerance. Diabetes Care. 2010; 33 (1):174-176 - 71.
Vas PRJ, Rayman G. The rate of decline in small fibre function assessed using axon reflex-mediated neurogenic vasodilatation and the importance of age related centile values to improve the detection of clinical neuropathy. PLoS One. 2013; 8 (7):e69920 Available from:https://dx.plos.org/10.1371/journal.pone.0069920 - 72.
Vas PRJ, Green AQ , Gerry R. Small fibre dysfunction, microvascular complications and glycaemic control in type 1 diabetes: A case–control study. Diabetologia. 2012; 55 (3):795-800 Available from:http://link.springer.com/10.1007/s00125-011-2417-9 - 73.
Vas PRJ, Rayman G. Validation of the modified LDIFlare technique: A simple and quick method to assess C-fiber function. Muscle & Nerve. 2013; 47 (3):351-356 - 74.
Nouri MN, Ahmed A, Bril V, Orszag A, Ng E, Nwe P, et al. Diabetic neuropathy and axon reflex-mediated neurogenic vasodilatation in type 1 diabetes. PLoS One. 2012; 7 (4). Available from:https://pubmed.ncbi.nlm.nih.gov/22529938/ - 75.
Edward PF, Andrew KL, Smith BP, Holden M, Russell GB, Poehling GG. Measurement of hand microvascular blood flow with isolated cold stress testing and laser Doppler fluxmetry. Journal of Hand Surgery. 1993; 18 (1):143-150. Available from:http://www.ncbi.nlm.nih.gov/pubmed/8423302 - 76.
van den Brande P, de Coninck A, Lievens P. Skin microcirculation responses to severe local cooling. International Journal of Microcirculation Clinical Experiment. 2019; 17 (2):55-60. Available from:http://www.ncbi.nlm.nih.gov/pubmed/9253681 - 77.
Cheung SS, Daanen HAM. Dynamic Adaptation of the Peripheral Circulation to Cold Exposure: Microcirculation. John Wiley & Sons, Ltd; Jan 2012; 19 (1):65-77. DOI: 10.1111/j.1549-8719.2011.00126.x. PMID: 21851473. Available from:http://doi.wiley.com/10.1111/j.1549-8719.2011.00126.x - 78.
Dinsdale G, Herrick A. Vascular diagnostics for Raynaud phenomenon. Journal of Vascular Diagnostic. 2014; 2 :127. Available from:http://www.dovepress.com/vascular-diagnostics-for-raynaud39s-phenomenon-peer-reviewed-article-JVD - 79.
Murray AK, Herrick AL, King TA. Laser Doppler imaging: A developing technique for application in the rheumatic diseases. Rheumatology. 2004; 43 (10):1210-1218. Available from:https://academic.oup.com/rheumatology/article-lookup/doi/10.1093/rheumatology/keh275 - 80.
Waszczykowska A, Goś R, Waszczykowska E, Dziankowska-Bartkowiak B, Jurowski P. Assessment of skin microcirculation by laser Doppler flowmetry in systemic sclerosis patients. Postepy Dermatological Alergology. 2014; 31 (1):6-11. Available from:http://www.ncbi.nlm.nih.gov/pubmed/24683391 - 81.
Wilson SB, Jennings PE, Belch JJ. Detection of microvascular impairment in type I diabetics by laser Doppler flowmetry. Clinical Physiology. 1992; 12 (2):195-208. Available from:http://www.ncbi.nlm.nih.gov/pubmed/1533824 - 82.
Chen YJ, Wang CL, Lo SK. Cutaneous microcirculation of diabetic foot: combined isolated cold stress testing and laser Doppler flowmetry study. Journal of Formos Medical Association. 1997; 96 (8):606-612. Available from:http://www.ncbi.nlm.nih.gov/pubmed/9290270 - 83.
Yamada T, Ohta T, Ishibashi H, Sugimoto I, Iwata H, Takahashi M, et al. Clinical reliability and utility of skin perfusion pressure measurement in ischemic limbs-Comparison with other noninvasive diagnostic methods. Journal of Vascular Surgery. 2008; 47 (2):318-323 - 84.
Pan X, Chen G, Wu P, Han C, Ho JK. Skin perfusion pressure as a predictor of ischemic wound healing potential (Review). Biomedical Reports. 2018; 8 :330-334 - 85.
Castronuovo JJ, Adera HM, Smiell JM, Price RM. Skin perfusion pressure measurement is valuable in the diagnosis of critical limb ischemia. Journal of Vascular Surgery. 1997; 26 (4):629-637. Available from:http://ezproxy.staffs.ac.uk/login?url=http://search.ebscohost.com/login.aspx?direct=true&db=cmedm&AN=9357464&site=ehost-live - 86.
Pitts J. Skin perfusion pressure: A case study demonstrating microcirculatory blood flow. Journal of Diagnostic Medical Sonography. 2014; 30 (4):213-216 - 87.
Tsai FW, Tulsyan N, Jones DN, Abdel-Al N, Castronuovo JJ, Carter SA. Skin perfusion pressure of the foot is a good substitute for toe pressure in the assessment of limb ischemia. Journal of Vascular Surgery. 2000; 32 (1):32-36 Available from:http://linkinghub.elsevier.com/retrieve/pii/S0741521400644841 - 88.
Urabe G, Yamamoto K, Onozuka A, Miyata T, Nagawa H. Skin perfusion pressure is a useful tool for evaluating outcome of ischemic foot ulcers with conservative therapy. Annals of Vascular Diseases. 2009; 2 (1):21-216 - 89.
Mosdósi B, Bölcskei K, Helyes Z. Impairment of microcirculation and vascular responsiveness in adolescents with primary Raynaud phenomenon. Pediatric Rheumatology Online Journal. 23 Mar 2018; 16 (1):20. DOI: 10.1186/s12969-018-0237-x - 90.
Musa R, Qurie A. Raynaud Disease. StatPearls. 2022. Available from: https://www.ncbi.nlm.nih.gov/books/NBK499833/ - 91.
Charkoudian N. Mechanisms and modifiers of reflex induced cutaneous vasodilation and vasoconstriction in humans. Journal of Applied Physiology. 1985; 109 (4):1221-1228. Available from:http://www.ncbi.nlm.nih.gov/pubmed/20448028 - 92.
Rossa A et al. Alteration of microcirculation is a hallmark of very early systemic sclerosis patients: A laser speckle contrast analysis. Clinical Experimental in Rheumatology. 2013; 31 (Suppl 76):109-114. Available from:https://www.clinexprheumatol.org/abstract.asp?a=6441 - 93.
Armstrong DG, Boulton AJM, Bus SA. Diabetic Foot Ulcers and Their Recurrence. The New England Journal of Medicine. 2017; 376 (24):2367-2375. Available from:https://www.nejm.org/doi/10.1056/NEJMra1615439 - 94.
Flynn MD, Tooke JE, Michael D. Microcirculation and the diabetic foot. Vascular Medicine Review. 1990; 1 (2):121-138. Available from:http://journals.sagepub.com/doi/10.1177/1358836X9000100204 - 95.
Koïtka A, Abraham P, Bouhanick B, Sigaudo-Roussel D, Demiot C, Saumet JL. Impaired pressure-induced vasodilation at the foot in young adults with type 1 diabetes. Diabetes. 2004; 53 (3):721-725. Available from:http://ezproxy.staffs.ac.uk/login?url=http://search.ebscohost.com/login.aspx?direct=true&db=cmedm&AN=14988257&site=ehost-live - 96.
Vouillarmet J, Josset-Lamaugarny A, Michon P, Saumet JL, Koitka-Weber A, Henni S, et al. Neurovascular response to pressure in patients with diabetic foot ulcer. Diabetes. 2019; 2019 :db180694. Available from:https://diabetes.diabetesjournals.org/content/early/2018/12/20/db18-0694