 Open access peer-reviewed chapter
Open access peer-reviewed chapter
Abstract
Venous thromboembolism (VTE) imposes a significant health care burden. Anticoagulation remains the mainstay of treatment for VTE. For decades, warfarin has been the oral anticoagulant of choice for the medical management of VTE; however, the scope and options for managing VTE have been gradually expanding. The coagulation cascade is a complex sequence of steps, and newer agents that act at different levels on this coagulation cascade have been developed. In the past decade, direct oral anticoagulants (DOACs) have proven to be the up-and-coming alternatives as oral agents in the medical management of VTE and have gradually become the first-line agents. Understanding their mechanism of action, uses, advantages, and disadvantages over other anticoagulants will be discussed in the scope of this chapter.
Keywords
- direct oral anticoagulant
- venous thromboembolism
- direct thrombin inhibitor
- factor Xa inhibitor
- DOAC
- VTE
- DTI
1. Introduction
Venous thromboembolism (VTE) refers to a thrombus or blood clot in the veins. It is a preventable and treatable medical condition but is often underdiagnosed. It includes deep venous thrombosis (DVT) and pulmonary embolism (PE) [1]. VTE has an estimated incidence rate of 1–2 per 1000 persons every year and is one of the leading causes of disability-adjusted life years (DALYs) lost and associated with significant healthcare costs [2].
Anticoagulation is a mainstay of treatment for the prevention and management of VTE. Unfractionated heparin (UFH) and vitamin K antagonist (VKA) warfarin have been the treatment of choice for the medical management of VTE for several years. These had several limitations, which had to be accepted, as there were no other options. Some of these limitations could be overcome with the advent of various low molecular heparins (LMWHs) and parenteral indirect thrombin inhibitors like fondaparinux. Despite all the progress in the field of anticoagulation for the management of VTE, there was still an unmet need for safe, efficient anticoagulants, particularly those that can be taken orally. Understanding the mechanism of action of heparin, researchers have realized that factor X and factor II in the coagulation cascade can be potential targets for therapeutic anticoagulation. This led to extensive research and the development of a newer generation of anticoagulants, now called the direct acting oral anticoagulants (DOACs). The discovery of these newer antithrombotic agents that act at different levels in the coagulation cascade has helped to further the management of VTE.
2. The nomenclature
Considering they are new compared to the conventional anticoagulants, they were initially called the NOACs, which stands for novel oral anticoagulants [3]. They were sometimes also called non-vitamin K antagonist oral anticoagulants, which also can be abbreviated as NOAC. Another name given to them was target-specific oral anticoagulants (TSOACs). However, as years passed, international societies have reassessed the name and considering their broad mechanism of action, the name DOAC is given [3]. DOACs include both direct thrombin inhibitors (DTIs) and factor Xa inhibitors—these names are given based on the specific step at which they act on the coagulation cascade (see Figure 1).
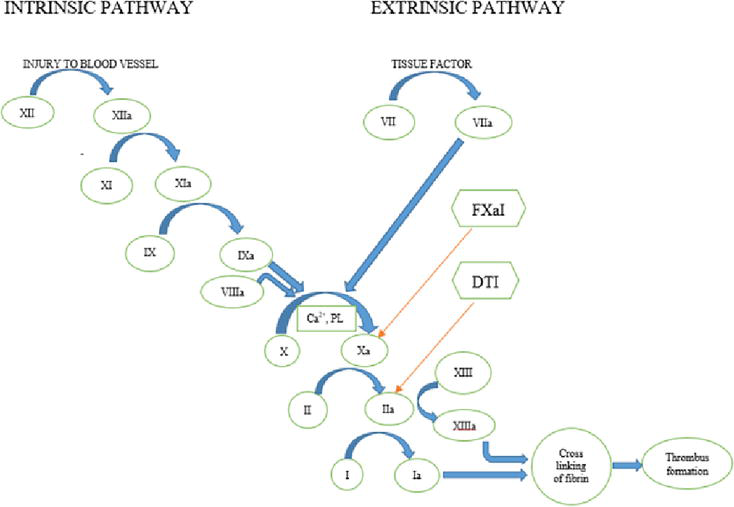
Figure 1.
Coagulation cascade showing intrinsic and extrinsic pathways and the site of action of the direct oral anticoagulants (DOACs). FXaI—factor Xa inhibitor; DTI—direct thrombin inhibitor; PL—platelet membrane phospholipid; Ca2+—calcium ions; II—prothrombin; IIa—thrombin; I—fibrinogen; Ia—fibrin; a—active form of the factor;
3. Types of DOACs
3.1 Direct thrombin inhibitors
Direct thrombin inhibitors act on activated factor II, also called thrombin (Figure 1). Thrombin plays a significant role in the coagulation cascade by helping convert factor I to activated factor I (factor Ia) or fibrin, which further helps form a clot [4]. Investigators working on novel anticoagulants targeted thrombin and designed a new structural class of nonpeptide inhibitors employing 1,2,5-trisubstituted benzimidazole as the central scaffold [5]. Using X-ray structure analysis, they further modified and developed a product named BIBR 1048, which was later named dabigatran, a direct thrombin inhibitor [5]. After initial studies showed the benefit, a larger randomized controlled trial called RE-COVER (Dabigatran vs. Warfarin for the Treatment of Acute Venous Thromboembolism) was conducted and concluded that a fixed dose of dabigatran is as effective as warfarin in treating VTE [6], and later approved for use in VTE. While there are parenteral DTIs like lepirudin, desirudin, bivalirudin, and argatroban, the only oral DTI is dabigatran.
3.2 Activated factor Xa inhibitors
Activated factor X (factor Xa) also plays a critical role in the coagulation cascade as both intrinsic and extrinsic pathways activate it (Figure 1). It acts as a catalyst for converting prothrombin to thrombin through the prothrombinase complex, which has factor Xa, activated factor V, Ca2+, and prothrombin on a phospholipid surface. Inhibition of factor Xa can decrease the generation of thrombin, thus decreasing the thrombin-mediated activation of coagulation. Research on factor Xa inhibitors led to the discovery of oxazolidinone derivatives, identified as potent factor Xa inhibitors [7]. This led to the discovery of BAY 59-7939, later named rivaroxaban, a potent and selective direct factor Xa inhibitor with excellent in vivo antithrombotic activity [7]. Other oral factor Xa inhibitors include apixaban, edoxaban, and betrixaban. As one may notice, these generic names end with Xa-ban, highlighting their role as factor Xa inhibitors.
4. Advantages of DOACs over VKA
VKAs like warfarin have been in use for several decades as the anticoagulants of choice; however, they have several limitations. Warfarin requires frequent monitoring to ensure that anticoagulation is within the therapeutic range. This would necessitate the use of additional healthcare resources and carries additional costs. DOACs do not require routine anticoagulation monitoring. Dosing of VKAs is affected by diet, medication interactions, etc., while DOAC dosing is not significantly affected by diet, and they have relatively fewer medication interactions. Warfarin has a long half-life of 35 h, and it takes a few days to reach therapeutic levels, while DOACs have a rapid onset of action. The dosage of warfarin needs to be adjusted regularly based on levels of anticoagulation; on the other hand, DOACs carry a convenient fixed-dose treatment. All these advantages have made DOACs popular and the anticoagulants of choice.
5. Direct oral anticoagulants (DOACs)
DOACs differ in their pharmacokinetic and pharmacodynamic profiles, and it is essential to understand them to select the right drug for the right patient. Here we review the commonly used DOACs and their specific characteristics.
5.1 Oral direct thrombin inhibitors
5.1.1 Dabigatran
Dabigatran was the first DOAC approved by the food and drug administration (FDA). The landmark study that investigated the role of dabigatran on venous thromboembolism is the RE-COVER trial [6]. It was a clinical study that investigated the efficacy and safety of dabigatran for treating acute VTE compared to warfarin. The study was conducted by Boehringer Ingelheim, the manufacturer of dabigatran, and was published in the New England Journal of Medicine in 2009.
The trial enrolled 2564 patients with acute VTE who were randomized to receive either dabigatran or warfarin for 6 months. The primary endpoint was the recurrence of VTE or related death within six months of treatment. It showed that dabigatran was non-inferior to warfarin in preventing recurrent VTE or related death, with 2.4% of patients in the dabigatran group experienced recurrent VTE or related death, compared to 2.1% in the warfarin group [6]. The bleeding rates were similar, with 16.1% of patients in the dabigatran group and 21.9% in the warfarin group [6].
The downsides of this trial include its industry funding, non-inferiority design, the short follow-up period of 6 months, limited generalizability (as this trial excluded those with severe renal impairment, bleeding disorders, etc.), and lack of head-to-head comparison with other novel oral anticoagulants. The follow-up period of 6 months may not be enough and might not capture long-term risks and benefits. Despite these limitations, it was a robust study and showed the benefits of dabigatran.
5.1.1.1 Mechanism of action and pharmacokinetics
It acts as a direct thrombin inhibitor and inhibits free and fibrin-bound thrombin. The prodrug dabigatran etexilate is metabolized to the active drug dabigatran in the liver. It has a bioavailability of 3–7% and a half-life of 12–17 h [8]. It reaches peak plasma levels in 1–2 h and is excreted predominantly in urine [8].
5.1.1.2 Dosage
DVT and PE treatment: the dosage of dabigatran in patients with venous thromboembolism is mainly determined by the results of the RE-COVER trial [6]. Based on the results of this trial, FDA approved this drug, and accordingly, the dosage recommended for VTE treatment is:
In hemodynamically stable patients—initial five days of therapeutic anticoagulation with a parenteral anticoagulant and then transition to dabigatran at a dosage of 150 mg oral capsule twice daily
VTE prophylaxis in total hip arthroplasty (THA) and total knee arthroplasty (TKA): RE-MODEL [9] and RE-NOVATE [10] and RE-NOVATE II [11] trials looked at the effect of dabigatran in knee and hip surgery thromboprophylaxis. A meta-analysis of these trials showed that though both 150 mg and 220 mg can be used for thromboprophylaxis, the higher dose of 220 mg daily is consistently non-inferior to enoxaparin when the surrogate venographic data on major and total venous thromboembolism are evaluated [12]. Hence the following dose is approved and indicated for VTE prophylaxis:
First dose—110 mg 1–4 h after surgery completion and hemostasis establishment. If not given on the day of surgery, 220 mg can be given after hemostasis is achieved. Maintenance doses 220 mg once daily for 10–14 days.
5.1.1.3 Caution with usage
No large-scale studies compare dabigatran with LMWH in treating malignancy-associated VTE [13]; hence, it is not recommended for treating malignancy-associated VTE. Its use is not recommended in pregnancy and in patients who are breastfeeding. It is not indicated in thrombosis associated with triple-positive antiphospholipid antibody syndrome (APS) [14]. It is mainly eliminated renally (80%); hence, we should be cautious in patients with renal failure. While the recommendation is that no dosage adjustment is required for CrCl > 30, no dosage recommendations are provided, and usage should be avoided in patients with chronic kidney disease with creatinine clearance (CrCl) < or = 30 mL/min or in hemodialysis patients [15]. Premature discontinuation can result in thrombotic events.
5.1.1.4 Adverse reactions
The most common side effect is bleeding, including life-threatening hemorrhage. Other side effects include gastrointestinal like dyspepsia, abdominal discomfort/pain, gastritis, esophagitis, and gastroesophageal reflux disease (GERD). Hypersensitivity reactions like angioedema and anaphylaxis are rare. Agranulocytosis, neutropenia, and thrombocytopenia are also recorded.
5.1.1.5 Specific benefit
While it is better to avoid all DOACs in severe hepatic impairment (transaminases > three times the upper limit of normal or Child-Pugh Class C), dabigatran is preferred to other DOACs in patients with moderate hepatic impairment, however should be used with caution [16].
6. Oral factor Xa inhibitors
6.1 Rivaroxaban
Rivaroxaban is the first factor Xa inhibitor approved for use in VTE. EINSTEIN-VTE study investigators looked at the role of rivaroxaban on VTE [17]. It was a large, randomized, multicenter trial that evaluated the efficacy and safety of oral rivaroxaban compared to standard therapy for treating acute VTE. The study included 4832 patients, randomized to receive either rivaroxaban (15 mg twice daily for three weeks followed by 20 mg once daily) or standard therapy, which consisted of enoxaparin followed by a VKA. The primary efficacy outcome was the composite of symptomatic recurrent VTE or death from any cause during the 3, 6, or 12-month follow-up period. The primary safety outcome was major bleeding. The study found that rivaroxaban was non-inferior to standard therapy for the primary efficacy outcome, with similar rates of recurrent VTE or death from any cause in the rivaroxaban and standard therapy groups (2.1% vs. 3.0%, respectively) [17]. Rivaroxaban was also associated with a significantly lower risk of major bleeding than standard therapy (1.1% vs. 2.2%, respectively) [17]. The study also found that rivaroxaban was associated with a lower risk of clinically relevant non-major bleeding.
The downsides of the Einstein VTE study include lack of blinding as it is an open-labeled study that could lead to reporting bias and a relatively short follow-up period of 12 months. Despite these concerns, the Einstein VTE study is generally regarded as a well-designed and carefully executed trial.
6.1.1 Mechanism of action and pharmacokinetics
It acts by inhibiting factor Xa, thus decreasing the conversion of prothrombin to thrombin. It reaches peak plasma levels in 2–4 h [18]. It is metabolized in the liver and primarily excreted through urine [19]. It has a bioavailability of 66–100% and a half-life of 5–9 h, with a longer half-life in the elderly.
6.1.2 Dosage
For VTE treatment: The EINSTEIN VTE study [17] and the study by Buller et al. [20] investigated the dosing of rivaroxaban and as per the results of these studies, the dosage recommended for VTE treatment is:
15 mg twice daily for 21 days, followed by 20 mg once daily.
For VTE prophylaxis: Studies by Lassen et al. [21], Turpie et al. [22], and Eriksson et al. [23] studied the dosing of rivaroxaban for hip and knee joint surgery thromboprophylaxis. Based on these studies:
In THA and total knee arthroplasty (TKA) patients and in acutely ill hospitalized patients, the dose of rivaroxaban for thromboprophylaxis is 10 mg once daily.
6.1.3 Caution with usage
Rivaroxaban is not recommended with pregnancy or with breastfeeding. As it is primarily excreted in the urine, it is not recommended with CrCl <30 ml/min and should be avoided in CrCl <15 ml/min, in hemodialysis, and peritoneal dialysis patients [19]. Usage should be avoided in moderate to severe hepatic impairment (Child-Pugh Class B or C). It is not recommended for patients with triple-positive APS [14]. Premature discontinuation can result in thrombotic events.
6.1.4 Adverse reactions
Bleeding, including life-threatening hemorrhage, can occur. Other side effects include abdominal pain, cholestasis, increased transaminases, skin rash, Stevens-Johnson syndrome (SJS), hypersensitivity, and anaphylaxis.
6.2 Apixaban
One of the breakthroughs was the AMPLIFY (Apixaban for the Initial Management of Pulmonary Embolism and Deep-Vein Thrombosis as First-Line Therapy) study by Angelli et al., which was a large, randomized, double-blind, non-inferiority trial that compared apixaban to conventional therapy (enoxaparin and warfarin) in the treatment of acute VTE [25]. The study enrolled over 5000 patients from 358 centers in 28 countries and found that apixaban was non-inferior to conventional therapy in preventing recurrent VTE and resulted in significantly less major bleeding. Patients were randomized to receive either apixaban 10 mg twice daily for seven days, followed by 5 mg twice daily for six months, or conventional therapy with enoxaparin followed by warfarin for six months. The results of the study showed that the incidence of recurrent VTE or death related to VTE was significantly lower in the apixaban group compared to the conventional therapy group (2.3% vs. 2.7%), and the incidence of major bleeding was significantly lower in the apixaban group (0.6% vs. 1.8%) [25]. The study concluded that apixaban was non-inferior to conventional therapy for treating acute VTE, with significantly less major bleeding.
Some limitations of this study include the use of a non-inferiority design instead of a superiority design, the fixed-dose regimen used in the study, which may not be optimal for all patients, and the fact that the study was funded by the manufacturer of apixaban, which may raise concerns about potential bias. However, the study followed rigorous scientific standards and was published in the New England Journal of Medicine (NEJM) in 2013.
6.2.1 Mechanism of action and pharmacokinetics
It inhibits factor Xa, thus decreasing the conversion of prothrombin to thrombin. It has an oral bioavailability of approximately 50%. It is metabolized by the liver primarily; excretion is through urine (approximately 27%) and gastrointestinal (GI) tract (biliary and direct intestinal excretion). It has a half-life of approximately 12 h and reaches peak plasma levels in 3–4 h [26].
6.2.2 Dosage
For VTE treatment: as per the results of the AMPLIFY study [25], the dosage that is recommended and approved for VTE treatment is:
Oral 10 mg twice daily for seven days, followed by 5 mg twice daily.
For VTE prophylaxis: the studies by Lassen et al. [27, 28] investigated apixaban for VTE prophylaxis in patients with THA and TKA. Based on these studies, the dosage that is approved and indicated is:
In THA and TKA patients: 2.5 mg twice daily for 10–14 days, which can be extended up to 35 days.
6.2.3 Caution with usage
It is not recommended with pregnancy or with breastfeeding. In case of renal impairment, the manufacturer recommends no dosage adjustment. A retrospective cohort study showed that it is safe and effective in patients on dialysis [29]. However, experts advise caution if CrCl < 25%. It should be used cautiously in moderate hepatic impairment (Child-Pugh Class B). Usage must be avoided in severe hepatic impairment (Child-Pugh Class C). It is not recommended for patients with triple-positive APS [14]. As with other DOACs, premature discontinuation can result in thrombotic events.
6.2.4 Adverse reactions
Bleeding, including life-threatening hemorrhage, can occur. Other side effects include nausea, increased transaminases, skin rash, hypersensitivity, and anaphylaxis.
6.2.5 Specific benefit
It may be used in patients with active cancer [30]. It can be used in obesity [24]. Concerning the side effect of bleeding, apixaban carries an advantage over other DOACs because the risk of major or clinically relevant non-major bleeding was less with apixaban than with other DOACs [31].
6.3 Edoxaban
A study by Hokusai—VTE investigators is the landmark trial investigating the role of edoxaban in VTE. It is a randomized, double blind, non-inferiority trial that compared the efficacy and safety of edoxaban versus warfarin in patients with VTE for the initial and extended treatment periods [32]. The study enrolled 8292 patients with acute symptomatic or incidental VTE, and patients were randomized to receive either edoxaban (60 mg once daily or 30 mg once daily in selected patients) or warfarin. The study consisted of two treatment periods: an initial treatment period of 5–10 days and an extended treatment period of up to 12 months. The primary efficacy endpoint was the composite of recurrent symptomatic VTE and VTE-related death during the entire study period. The primary safety endpoint was major bleeding. The study found that edoxaban was non-inferior to warfarin for the primary efficacy endpoint, with a significantly lower rate of major bleeding in the edoxaban group. The 12-month cumulative incidence of the primary efficacy endpoint was 3.2% in the edoxaban group and 3.5% in the warfarin group [32]. The incidence of major bleeding was 1.4% in the edoxaban group and 1.6% in the warfarin group [32]. The study thus showed the beneficial effects of edoxaban for VTE treatment.
The study has limitations as it does not include patients with CrCl less than 30 mL/min. This raises concerns about the generalizability of the results to patients with severe renal impairment or end-stage renal disease, who are at increased risk of bleeding and thromboembolic events. As the manufacturer of edoxaban sponsored the study, it may have introduced bias into the study design and analysis. Despite these shortfalls, it is a significant study that showed the benefits of edoxaban.
6.3.1 Mechanism of action and pharmacokinetics:
It acts by inhibiting factor Xa, thus decreasing the conversion of prothrombin to thrombin. Its bioavailability is approximately 62%. It has a half-life of 10–14 h and reaches peak plasma levels in 1–2 h. It is excreted through urine, with renal clearance being almost 50% of total clearance [33].
6.3.2 Dosage
The dosage recommended and approved for edoxaban is mainly derived from the results of the Honkusai study [32]. After five days of initial therapy with parenteral anticoagulation, we can transition to edoxaban if the patient is hemodynamically stable—60 mg once daily (if patient weight > 60 kg) or 30 mg daily (if patient weight < or = 60 kg). If CrCl 30–50 ml/min—30 mg orally once daily and if the CrCl < 30 ml/min—use is not recommended.
6.3.3 Caution with usage
It is not recommended with pregnancy or with breastfeeding. In renal impairment, it is not recommended if CrCl <30 ml/min [15]. Usage should be avoided in moderate and severe hepatic impairment (Child-Pugh Class B and C). It is not recommended for patients with triple-positive APS [14]. Premature discontinuation can result in ischemic events.
6.3.4 Adverse reactions
Bleeding, including life-threatening hemorrhage. Other side effects include abdominal pain, increased transaminases, skin rash, headache, thrombocytopenia, hypersensitivity, and anaphylaxis.
6.3.5 Specific benefit
Edoxaban can be taken independently of food. It can be given to patients with cancer, except those with GI tract cancers [16].
6.4 Betrixaban
Betrixaban is another factor Xa inhibitor approved by the FDA for VTE prophylaxis in adults hospitalized with acute medical illness [34]. However, it was discontinued in the US in 2020 for business reasons and is not marketed in other countries. Hence, this drug is not extensively discussed here.
7. Proximal vs. distal DVT
The DVTs in the lower extremities can be divided into proximal and distal DVTs. Proximal DVT in the lower extremities is located in the popliteal, femoral, or iliac veins, while distal DVT is usually confined to the calf veins, below the knee, in the anterior tibial, posterior tibial, peroneal and muscular veins.
Whether to treat a distal DVT is controversial, with practices differing from center to center [35]. The consensus is that typically, patients with distal DVT do not need the treatment with anticoagulation and can be followed up with surveillance venous doppler studies. However, factors that favor anticoagulation in cases of distal DVT include the presence of major symptoms, thrombus extension close to the popliteal vein, extensive thrombosis involving multiple veins, unprovoked DVT, presence of persistent risk factors, previous DVT or PE, Corona virus disease 2019 (COVID-19) and patient preference.
8. Duration of treatment for VTE
The decision on the duration of treatment of VTE is complicated and we have to consider various factors. These factors include: the kind of VTE, whether it is provoked or unprovoked, the risk factors—whether they are weak, moderate, or strong risk factors, and whether these risk factors are transient or persistent, and the risk of bleeding associated with anticoagulation. The benefits and risks should be discussed with the patient, and there should be informed decision-making in determining the anticoagulant and treatment duration.
VTEs can be divided into provoked VTEs and unprovoked VTEs. Provoked VTEs occur in the presence of transient or persistent risk factors. The risk factors for VTE can be divided into weak risk factors (odd’s ratio (OR) less than two), moderate risk factors (OR 2-9), and strong risk factors (OR more than 10) [36]. Weak risk factors include bed rest over three days, arterial hypertension, type 2 diabetes mellitus, immobility due to sitting, obesity, pregnancy, and varicose veins [36]. Moderate risk factors include arthroscopic knee surgery, autoimmune disease, blood transfusion, central venous lines, intravenous catheters and leads, chemotherapy, congestive heart failure or respiratory failure, hormone replacement therapy, oral contraceptive therapy, postpartum period, infection such as pneumonia, urinary tract infection, inflammatory bowel disease, cancer, stroke, superficial venous thrombosis, and thrombophilia [36]. Strong risk factors include fracture of the lower limb, hospitalization for heart failure or atrial fibrillation, hip or knee replacement, major trauma, myocardial infraction, previous VTE, and spinal cord injury [36].
Usually, if someone has a VTE with a transient risk factor, the duration of treatment is three to six months, and in the presence of VTE which is unprovoked, or in the presence of persistent risk factors, the duration of treatment is longer, possibly lifelong [37].
However, whether to treat those with weak but persistent risk factors with long-term anticoagulation is a matter of debate. There is concern that exposure to long-term anticoagulation may increase the risk of bleeding, particularly in the vulnerable population like the elderly, low body weight, etc. Some experts suggest that in these cases, we can consider reduced dose long-term anticoagulation based on certain studies [38, 39, 40].
The AMPLIFY-EXT trial is a study that looked at the effect of reduced-dose apixaban for long-term anticoagulation [38]. It was a randomized, double-blind, placebo-controlled trial that evaluated the efficacy and safety of extended treatment with apixaban in patients who had completed 6–12 months of anticoagulation therapy for VTE. The trial enrolled 2486 patients who were randomly assigned to receive either apixaban 2.5 mg twice daily or a placebo for an additional 12 months of treatment. The trial results showed that extended treatment with apixaban significantly reduced the risk of recurrent VTE or death from any cause, compared to placebo. The incidence of the primary efficacy outcome was 3.8% in the apixaban group and 11.6% in the placebo group, with a hazard ratio of 0.33 (95% confidence interval, 0.22–0.48; P < 0.001) [38]. The incidence of major bleeding was low in both treatment groups, with no significant difference. The incidence of clinically relevant non-major bleeding was higher in the apixaban group than in the placebo group, but this difference was not statistically significant.
The EINSTEIN CHOICE trial looked at the effect of a reduced dose of rivaroxaban for long-term anticoagulation [39]. It was a randomized, double blind, multinational trial that compared the efficacy and safety of rivaroxaban with aspirin for the extended treatment of VTE. The trial enrolled 3365 patients who had completed 6–12 months of anticoagulation therapy for VTE. These patients were randomly assigned to receive one of three regimens for an additional 12 months: rivaroxaban 20 mg once daily, rivaroxaban 10 mg once daily, or aspirin 100 mg once daily. The trial showed that both doses of rivaroxaban were more effective than aspirin for preventing recurrent VTE or VTE-related death. The incidence of the primary efficacy outcome was 1.5% in the rivaroxaban 20 mg group, 1.2% in the rivaroxaban 10 mg group, and 4.4% in the aspirin group, with hazard ratios of 0.34 (95% CI, 0.20–0.59; P < 0.001) and 0.26 (95% CI, 0.14–0.47; P < 0.001), respectively [39]. The incidence of major bleeding was low in all three treatment groups, with no significant differences. The incidence of clinically relevant non-major bleeding was higher in the rivaroxaban group than in the aspirin group.
Based on the results of the above studies, some experts suggest reduced dosing (apixaban 2.5 mg twice daily, rivaroxaban of 10 mg daily) for the maintenance therapy for long-term anticoagulation in patients with weak/mild persistent risk factors and with concerns of bleeding complications.
9. Reversal of the anticoagulation effect of DOACS
There are certain reversal agents that should be considered in case of severe or life-threatening bleeding with DOAC use. These include idarucizumab for dabigatran and andexanet alfa for rivaroxaban, apixaban and edoxaban. It is worth noting that these reversal agents are specific to the respective DOACs, and the effectiveness of reversal may depend on the timing of administration and the severity of the bleeding event. There is some role of prothrombin complex concentrate (PCC) as well, particularly if these first line agents are not available.
9.1 Idarucizumab
It is a reversal agent for dabigatran. It is a monoclonal antibody fragment that binds specifically to dabigatran and neutralizes its anticoagulant effect by forming inactive complexes that are rapidly cleared from the circulation. The RE-VERSE AD study is a phase III, prospective, open-label, multicenter study that evaluated the safety and efficacy of idarucizumab in reversing the anticoagulant effect of dabigatran in patients with uncontrolled bleeding or who required urgent surgery or intervention [41]. The study found that idarucizumab rapidly and effectively reversed the anticoagulant effect of dabigatran in the majority of patients, with a low rate of thrombotic events [41]. The recommended dosage is 5 grams, which is administered as two consecutive 2.5 gm intravenous (IV) bolus injections, given minutes apart [41]. The dose may be repeated if the patient’s anticoagulation is not adequately reversed. Though the risk of thrombotic events is low with idarucizumab, we have to carefully monitor the patient for such events.
9.2 Andexanet alfa
Andexanet alfa is a recombinant protein that acts as a decoy receptor for factor Xa inhibitors, such as apixaban, rivaroxaban, and edoxaban. It binds to these anticoagulants in the bloodstream, sequestering them and preventing them from inhibiting the clotting factor Xa. This restores the activity of factor Xa and allows the clotting process to proceed. ANNEXA studies [42, 43] have demonstrated the efficacy and safety of andexanet alfa in reversing the anticoagulant effects of these factor Xa inhibitors in patients experiencing bleeding or requiring urgent surgery or procedures. The recommended dosing for andexanet alfa as per these studies is:
Apixaban: bolus dose of 400 mg over 2 min, followed by a continuous infusion of 4 mg/min for up to 120 min, rivaroxaban: bolus dose of 800 mg over 30 min, followed by a continuous infusion of 8 mg/min for up to 120 min, edoxaban: bolus dose of 800 mg over 30 min, followed by a continuous infusion of 8 mg/min for up to 120 min.
9.3 PCC
Both unactivated prothrombin complex concentrate (uPCC) and activated prothrombin complex concentrate (aPCC) have therapeutic implications and can be used for the reversal of DOACs. The main difference between them is that aPCC contains activated factor VII (FVIIa), while uPCC does not. FVIIa can bypass the normal clotting pathway and activate factor X directly, leading to thrombin generation and clot formation. This makes aPCC a more potent clotting agent compared to uPCC. uPCC is generally preferred for the reversal of factor Xa inhibitors (e.g., apixaban, rivaroxaban, edoxaban) whereas aPCC may be more effective for the reversal of dabigatran [44].
Though there are case reports and case series on the benefits of aPCC in DOAC associated bleeding, there are no high-quality studies to support this. They can be considered if the first line agents are not available. If idarucizumab is not available for reversal of dabigatran, aPCC such as factor eight inhibitor bypassing activity (FEIBA), unactivated 4-factor PCC (contains factors II, VII, IX and X) or 3-factor PCC (contains factors II, IX and X) would be reasonable alternative [44]. If Andexanet alfa is not available for reversal of factor Xa inhibitors, 4-factor PCC is an alternative [44]. If neither is available, 3-factor PCC is the next option.
9.4 Other agents
In case of severe bleeding, in addition to the above reversal agents, antifibrinolytic agents like tranexamic acid, epsilon-aminocaproic acid can be used [44].
10. DOACs for VTE in specific conditions
It is crucial to appropriately dose and be aware of underlying conditions when prescribing DOACs. Some studies suggested that up to 32% of patients experience inappropriate dosing with DOACs [45]. Subtherapeutic and supratherapeutic dosing can expose the patient to the risks of thrombotic or bleeding consequences [46]. Collaboration with pharmacists is critical for evidence-based anticoagulant use and can help avoid inappropriate dosing. Although explained above, under each DOAC, we briefly review some of the special conditions or comorbidities that can influence the selection and dosage of DOACs.
10.1 DOACs for VTE in cancer
Patients with cancer are at an increased risk of VTE. Treating VTE in patients with cancer is complicated due to associated comorbidities like renal failure, being underweight, malabsorption, bleeding risks, etc. Historically LMWHs have been the treatments of choice in cancer VTE. The HOKUSAI -VTE cancer trial demonstrated that edoxaban is non-inferior to dalteparin (LMWH) in preventing recurrent VTE, but there was some increased risk of major bleeding [47]. Select D trial compared rivaroxaban to dalteparin, and there was a decreased risk of VTE and some increased risk of major bleeding [48]. ADAM VTE [49] and Caravaggio trial [50] have demonstrated the benefits of apixaban in cancer VTE patients with comparable major bleeding compared with LMWH. As a deduction from all these studies, evidence and guidelines suggest that edoxaban and rivaroxaban can be used for VTE in cancer patients except those with GI cancers, where there is an increased risk of bleeding with these agents. Apixaban, due to its relatively better major bleeding risk, is preferable to other DOACs in treating VTE in cancer patients [15].
10.2 DOACs for VTE associated with obesity
The large randomized controlled trials investigating different DOACs did not have patient weight as a significant factor in deciding the dosage. In addition, extreme-body weight populations (overweight or underweight) are severely under-represented in these trials [51]. Hence, it was unclear if the same dosages were sufficient for the drug to be effective or to avoid the side effects. The International Society of Thrombosis and Hemostasis analyzed these trials and the sub-group analysis and suggested that DOACs are safe in patients ≤120 kg (BMI ≤ 40 kg/m2) at standard dosing [15]. For patients with weight > 120 kg or BMI > 40 kg/m2, it is recommended to avoid dabigatran and edoxaban and can use apixaban and rivaroxaban [24].
10.3 DOACs for VTE associated with low body weight
In patients with low body weight (<60 kg), creatinine clearance is commonly overestimated as the muscle mass is less. In addition, patients with low-body weight can have associated comorbidities like renal impairment, elderly age, etc. Hence, choosing the appropriate DOAC and the correct dosage is crucial to avoid side effects. As there is increased systemic exposure, the dosage of apixaban and edoxaban should be reduced in low-body weight patients (<60 kg), while dabigatran and rivaroxaban should be better avoided [15].
10.4 DOACs for VTE in renal failure
Chronic kidney disease (CKD) patients have an increased risk for thromboembolic and bleeding events. One should be cautious of dosing DOACs appropriately in patients with renal insufficiency. Renal function is one of the most critical determinants of the dosage of DOACs, and renal insufficiency is one of the important factors associated with the inappropriate dosing of DOACs [52]. Among the DOACs, dabigatran is most renally eliminated at 80%, followed by edoxaban (50%), rivaroxaban (35%), and apixaban (27%) [53]. Hence, dabigatran, edoxaban, and rivaroxaban need dosage adjustment with renal impairment and should be avoided in severe renal impairment (CrCl < 30 mL/min). Apixaban undergoes the least renal clearance and is considered the DOAC of choice in severe renal impairment—even in patients with dialysis [29]; however, experts advise caution.
10.5 DOACs for VTE in hepatic failure
DOACs rely on hepatic metabolism for drug clearance, with apixaban accounting for 75%, followed by rivaroxaban (65%), edoxaban (50%), and dabigatran (20%) [54]. Anticoagulation management in patients with advanced chronic liver disease (ACLD) is complicated, particularly as they tend to have bleeding tendencies [55]. They also have an increased risk of thrombosis [55]; a meta-analysis showed a 1.7-fold increase in the risk of thrombosis in patients with cirrhosis compared to the general population [56]. As the large, randomized studies on DOACs have excluded patients with advanced liver failure, we have to rely on small retrospective studies for suggesting the DOACs for patients with advanced liver failure. Liver failure is classified based on the Child-Pugh classification system as Class A, B, and C, and recommendations for DOACs are based on that [55]. While all DOACs can be considered for mild hepatic impairment (Child-Pugh Class A) without dosage adjustment, they should be avoided in severe hepatic impairment (Child-Pugh Class C) [57]. Dabigatran can be considered in patients with moderate hepatic impairment (Child-Pugh Class B), while apixaban, rivaroxaban, and edoxaban should be used with caution [57]. Some guidelines recommend that apixaban and edoxaban should be avoided if transaminases are more than two times the upper limit of normal (ULN), while dabigatran and rivaroxaban should be avoided if transaminases are more than three times ULN [16].
10.6 DOACs for VTE in heart failure
While no specific dosage adjustments are needed for DOACs in heart failure for managing VTE, the presence of heart failure itself is considered a moderate risk factor for venous thromboembolism [36], and heart failure requiring hospitalization is considered a major risk factor for VTE [36]. A study by Fanola et al. showed that the presence of heart failure increased the risk of short-term and long-term VTE, regardless of the presence of other risk factors, and this risk persisted for the 22-year duration of the study in both heart failure with reduced ejection fraction (HFrEF) and heart failure with preserved ejection fraction (HFpEF) [58]. Hence, chronic heart failure would indicate a persistent risk factor, and as discussed earlier in the duration of treatment section, we may have to consider long-term anticoagulation for managing VTE in this population group.
10.7 DOACs for VTE in the elderly
No specific dosage corrections are needed for age in the adult population in managing VTE. The elderly population is at risk of VTE; however, age also is a strong risk factor for anticoagulation-associated bleeding, particularly in those >75 years [59]. Hence, when treating VTE in the elderly, if long-term anticoagulation is considered (based on unprovoked VTE or persistent risk factors), after the initial 3 to 6 months of treatment, we have to look at the benefits and risks closely. We may have to avoid long-term anticoagulation or consider dose reduction in this population group due to their increased risk of bleeding [59].
10.8 DOACs for VTE in COVID-19
COVID-19 is a prothrombotic, hypercoagulable condition. The prevalence of VTE in COVID-19 ranges from 2.6% to 35.3% [60]. The role of DOACs is not clearly defined in patients with COVID-19. There is evolving evidence on the role of DOACs concerning VTE prophylaxis and treatment in patients with COVID-19. Current guidelines do not recommend DOACs for treating hospitalized patients with acute VTE associated with COVID-19 infection or thromboprophylaxis in acutely ill patients with COVID-19 infection. In both these cases, guidelines recommend using LMWH or UFH [60, 61]. Aslan et al. [62] conducted a study on patients already using DOACs, which did not show any additional benefit of prior DOAC use against intensive care unit (ICU) need or in-hospital mortality. The ACTIV-4B trial by Connors et al. showed that among symptomatic and stable outpatients with COVID-19, thromboprophylaxis with apixaban did not show benefit against all-cause mortality, and venous thrombosis among other parameters studied [63]. In stable patients who are discharged and would benefit from extended prophylaxis, DOACs can be considered [61]. They can also be considered for outpatient management of VTE patients with COVID-19 [61].
11. Future directions
The role of DOACs, which took a boost a decade ago, continues to expand. There are several ongoing trials on the role of DOACs in VTEs. For example—DOAC’s role in VTE in patients with ESRD (ClinicalTrials.gov Identifier: NCT04818151), in cancer (ClinicalTrials.gov Identifier: NCT02744092), etc. LEAVE safe with DOACs (ClinicalTrials.gov Identifier: NCT04068727) is a study looking at Clinical Pharmacist intervention to avoid medication errors, which are relatively common with DOACs. Various studies are also in progress looking at the role of DOACs in thromboprophylaxis.
Researchers and scientists continue to explore various other targets in the coagulation cascade to address VTE. Factor XI, a vital component of the intrinsic pathway of the coagulation cascade, is another potential target, as inhibiting factor XI can attenuate thrombosis with little disruption of hemostasis [64]. Recently a study by Verhamme et al. investigated the role of Abelacimab [64]. This monoclonal antibody binds to factor XI and found that it was effective in preventing VTE after TKA [64]. Another agent called Asundexian, a factor XIa inhibitor, is in the investigational stages [65]. Another monoclonal antibody against factor XI, REGN9933, is also in the investigational stages (ClinicalTrials.gov Identifier: NCT05102136).
12. Conclusion
VTE is a relatively common but underdiagnosed healthcare burden. In the past decade, DOACs have revolutionized the management of VTE, overcoming several of the shortcomings of conventional therapies like UFH, LMWH, and VKAs. The oral route of administration, relatively easy dosing, and the lack of need for routine monitoring have made them favorites and preferred anticoagulants of choice in managing VTEs. However, to avoid inadvertent complications like bleeding or worsening of thrombosis and select the appropriate DOAC, dosage, and treatment duration, it is essential to understand their pharmacokinetic properties and be aware of underlying comorbidities and risk factors. With further research on the existing DOACs and prospects of discovering newer anticoagulants, there is hope that the medical management of VTE will be more efficient in the coming times.
References
- 1.
Tritschler T, Kraaijpoel N, Gal GL, et al. Venous thromboembolism advances in diagnosis and treatment. Journal of the American Medical Association. 2018; 320 (15):1583-1594. DOI: 10.1001/jama.2018.14346 - 2.
Scheres LJJ, Lijfering WM, Cannegieter SC. Current and future burden of venous thrombosis: Not simply predictable. Research and Practice in Thrombosis and Haemostasis. 2018; 2 (2):199-208. Published online 2018 Apr 17. DOI: 10.1002/rth2.12101 - 3.
Barnes GD, Ageno W, Ansell J, et al. Recommendation on the nomenclature for oral anticoagulants: Communication from the SSC of the ISTH. Journal of Thrombosis and Haemostasis. Jun 2015; 13 (6):1154-1156. DOI: 10.1111/jth.12969 - 4.
Lee CJ, Ansell JE. Direct thrombin inhibitors. British Journal of Clinical Pharmacology. 2011; 72 (4):581-592. DOI: 10.1111/j.1365-2125.2011.03916.x - 5.
Hauel NH, Nar H, Priepke H. Structure-based design of novel potent nonpeptide thrombin inhibitors. Journal of Medicinal Chemistry. 2002; 45 (9):1757-1766. DOI: 10.1021/jm0109513 - 6.
Schulman S, Kearon C, Kakkar AK, et al. Dabigatran versus warfarin in the treatment of acute venous thromboembolism. RE-COVER study group. The New England Journal of Medicine. 2009; 361 :2342-2352. DOI: 10.1056/NEJMoa0906598 - 7.
Roehrig S, Straub A, Pohlmann J, et al. Discovery of the novel antithrombotic agent 5-chloro-N-({(5S)-2-oxo-3- [4-(3-oxomorpholin-4-yl)phenyl]-1,3-oxazolidin-5-yl}methyl)thiophene2-carboxamide (BAY 59-7939): An oral, direct factor Xa inhibitor. Journal of Medicinal Chemistry. 2005; 48 :5900-5908. DOI: 10.1021/jm050101d - 8.
Stangier J. Clinical pharmacokinetics and pharmacodynamics of the oral direct thrombin inhibitor dabigatran etexilate. Clinical Pharmacokinetics. 2008; 2012 (47):285-295. DOI: 10.2165/00003088-200847050-00001 - 9.
Eriksson BI, Dahl OE, Rosencher N, et al. Oral dabigatran etexilate vs. subcutaneous enoxaparin for the prevention of venous thromboembolism after total knee replacement: The RE-MODEL randomized trial. Journal of Thrombosis and Haemostasis. 2007; 5 (11):2178-2185. DOI: 10.1111/j.1538-7836.2007.02748.x - 10.
Eriksson BI, Dahl OE, Rosencher N, et al. Dabigatran etexilate versus enoxaparin for prevention of venous thromboembolism after total hip replacement: A randomised, double-blind, non-inferiority trial. Lancet. 2007; 370 (9591):949-956. DOI: 10.1016/S0140-6736(07)61445-7 - 11.
Eriksson BI, Dahl OE, Huo MH, et al. Oral dabigatran versus enoxaparin for thromboprophylaxis after primary total hip arthroplasty (RE-NOVATE II). A randomised, double-blind, non-inferiority trial. Thrombosis and Haemostasis. 2011; 105 (4):721-729. DOI: 10.1160/TH10-10-0679 - 12.
Gómez-Outes A, Terleira-Fernández AI, Suárez-Gea ML, et al. Dabigatran, rivaroxaban, or apixaban versus enoxaparin for thromboprophylaxis after total hip or knee replacement: Systematic review, meta-analysis, and indirect treatment comparisons. BMJ. 2012; 344 :e3675. DOI: 10.1136/bmj.e3675 - 13.
Schulman S, Goldhaber SZ, Kearon C, et al. Treatment with dabigatran or warfarin in patients with venous thromboembolism and cancer. Thrombosis and Haemostasis. 2015; 114 (1):150-157. DOI: 10.1160/TH14-11-0977 - 14.
Pastori D, Menichelli D, Cammisotto V, et al. Use of direct oral anticoagulants in patients with antiphospholipid syndrome: A systematic review and comparison of the international guidelines. Frontiers in Cardiovascular Medicine. 2021; 8 :715878. DOI: 10.3389/fcvm.2021.715878 - 15.
Chen A, Stecker E, Warden BA. Direct oral anticoagulant use: A practical guide to common clinical challenges. Journal of the American Heart Association. 2020; 9 (13):e017559. DOI: 10.1161/JAHA.120.017559 - 16.
Streiff MB, Abutalib SA, Farge D, et al. Special series: Approach to the patient with cancer and thrombosis. Update on guidelines for the management of cancer-associated thrombosis. The Oncologist. 2021; 26 (1):e24-e40. DOI: 10.1002/onco.13596 - 17.
Prins MH, Lensing AW, Bauersachs R, et al. Oral rivaroxaban versus standard therapy for the treatment of symptomatic venous thromboembolism: A pooled analysis of the EINSTEIN-DVT and PE randomized studies. Thrombosis Journal. 2013; 11 (1):21. DOI: 10.1186/1477-9560-11-21 - 18.
Mueck W, Stampfuss J, Kubitza D, et al. Clinical pharmacokinetic and pharmacodynamic profile of rivaroxaban. Clinical Pharmacokinetics. 2014; 53 (1):1-1. DOI: 10.1007/s40262-013-0100-7 - 19.
Kumar S, Lim E, Covic A, et al. Anticoagulation in concomitant chronic kidney disease and atrial fibrillation: JACC review topic of the week. Journal of the American College of Cardiology. 2019; 74 :2204-2215. DOI: 10.1016/j.jacc.2019.08.1031 - 20.
Buller HR, Lensing AWA, Prins MH, et al. A dose-ranging study evaluating once-daily oral administration of the factor Xa inhibitor rivaroxaban in the treatment of patients with acute symptomatic deep vein thrombosis: The Einstein–DVT dose-ranging study. Clinical Trials & Observations. Blood. 2008; 112 (6):2242-2247. DOI: 10.1182/blood-2008-05-160143 - 21.
Lassen MR, Ageno W, Borris LC, et al. Rivaroxaban versus enoxaparin for thromboprophylaxis after total knee arthroplasty. The New England Journal of Medicine. 2008; 358 (26):2776-2786. DOI: 10.1056/NEJMoa076016 - 22.
Turpie AG, Lassen MR, Davidson BL, et al. Rivaroxaban versus enoxaparin for thromboprophylaxis after total knee arthroplasty (RECORD4): A randomized trial. Lancet. 2009; 373 (9676):1673-1680. DOI: 10.1016/S0140-6736(09)60734-0 - 23.
Eriksson BI, Borris LC, Friedman RJ, et al. Rivaroxaban versus enoxaparin for thromboprophylaxis after hip arthroplasty. The New England Journal of Medicine. 2008; 358 (26):2765-2775. DOI: 10.1056/NEJMoa0800374 - 24.
Sebaaly J, Kelley D. Direct oral anticoagulants in obesity: An updated literature review. The Annals of Pharmacotherapy. 2020; 54 (11):1144-1158. DOI: 10.1177/1060028020923584 - 25.
Agnelli G, Buller HR, Cohen A, et al. Oral apixaban for the treatment of acute venous thromboembolism. New England Journal of Medicine. 2013; 369 :799-808. DOI: 10.1056/NEJMoa1302507 - 26.
Byon W, Garonzik S, Boyd RA, et al. Apixaban: A clinical pharmacokinetic and pharmacodynamic review. Clinical Pharmacokinetics. 2019; 58 (10):1265-1279. DOI: 10.1007/s40262-019-00775-z - 27.
Lassen MR, Raskob GE, Gallus A, et al. Apixaban or enoxaparin for thromboprophylaxis after knee replacement. The New England Journal of Medicine. 2009; 361 (6):594-604. DOI: 10.1056/NEJMoa0810773 - 28.
Lassen MR, Gallus A, Raskob GE, et al. Apixaban versus enoxaparin for thromboprophylaxis after hip replacement. The New England Journal of Medicine. 2010; 363 (26):2487-2498. DOI: 10.1056/NEJMoa1006885 - 29.
Wetmore JB, Herzog CA, Yan H, et al. Apixaban versus warfarin for treatment of venous thromboembolism in patients receiving long-term dialysis. Clinical Journal of the American Society of Nephrology. 2022; 17 (5):693-702. DOI: 10.2215/CJN.14021021 - 30.
Agnelli G, Becattini C, Meyer G, et al. Apixaban for the treatment of venous thromboembolism associated with cancer. The New England Journal of Medicine. 2020; 382 (17):1599-1607. DOI: 10.1056/NEJMoa1915103 - 31.
Cohen AT, Hamilton M, Mitchell SA, et al. Comparison of the novel oral anticoagulants apixaban, dabigatran, edoxaban, and rivaroxaban in the initial and long-term treatment and prevention of venous thromboembolism: Systematic review and network meta-analysis. PLoS One. 2015; 10 (12):e0144856. DOI: 10.1371/journal.pone.0144856. eCollection 2015 - 32.
The Hokusai-VTE Investigators. Edoxaban versus warfarin for the treatment of symptomatic venous thromboembolism. The New England Journal of Medicine. 2013; 369 :1406-1415. DOI: 10.1056/NEJMoa1306638 - 33.
Parasrampuria DA, Truitt KE. Pharmacokinetics and pharmacodynamics of edoxaban, a non-vitamin K antagonist oral anticoagulant that inhibits clotting factor Xa. Clinical Pharmacokinetics. 2016; 55 :641-655. DOI: 10.1007/s40262-015-0342-7 - 34.
FDA Approves Betrixaban for Venous Thromboembolism. Available from: https://ashpublications.org/ashclinicalnews/news/3299/FDA-Approves-Betrixaban-for-Venous-Thromboembolism - 35.
Stevens SM, Woller SC, Kreuziger LB, et al. Antithrombotic therapy for VTE disease: Second update of the CHEST guideline and expert panel report. Chest. 2021; 160 (6):e545-e608. DOI: 10.1016/j.chest.2021.07.055 - 36.
Konstantinides SV, Meyer G, Becattini C, et al. 2019 ESC guidelines for the diagnosis and management of acute pulmonary embolism developed in collaboration with the European Respiratory Society (ERS). European Heart Journal. 2020; 41 (4):543-603. DOI: 10.1093/eurheartj/ehz405 - 37.
Ortel TL, Neumann I, Ageno W, et al. American Society of Hematology 2020 guidelines for management of venous thromboembolism: Treatment of deep vein thrombosis and pulmonary embolism. Blood Advances. 2020; 4 (19):4693-4738. DOI: 10.1182/bloodadvances.2020001830 - 38.
Agnelli G, Buller HR, Cohen A, et al. Apixaban for extended treatment of venous thromboembolism. The New England Journal of Medicine. 2013; 368 :699-708. DOI: 10.1056/NEJMoa1207541 - 39.
Weitz JI, Lensing AWA, Prins MH, et al. Rivaroxaban or aspirin for extended treatment of venous thromboembolism. The New England Journal of Medicine. 2017; 376 :1211-1222. DOI: 10.1056/NEJMoa1700518 - 40.
Vasanthamohan L, Boonyawat K, Chai-Adisaksopha C, et al. Reduced-dose direct oral anticoagulants in the extended treatment of venous thromboembolism: A systematic review and meta-analysis. Journal of Thrombosis and Haemostasis. 2018; 16 (7):1288-1295. DOI: 10.1111/jth.14156. Epub 2018 Jun 17 - 41.
Pollack CV, Reilly PA, Eikelboom J, et al. Idarucizumab for dabigatran reversal. The New England Journal of Medicine. 2015; 373 :511-520. DOI: 10.1056/NEJMoa1502000 - 42.
Siegal DM, Curnutte JT, Connolly SJ, et al. Andexanet alfa for the reversal of factor Xa inhibitor activity. The New England Journal of Medicine. 2015; 373 :2413-2424. DOI: 10.1056/NEJMoa1510991 - 43.
Connolly SJ, Crowther M, Eikelboom JW, et al. Full study report of andexanet alfa for bleeding associated with factor Xa inhibitors. The New England Journal of Medicine. 2019; 380 :1326-1335. DOI: 10.1056/NEJMoa1814051 - 44.
Tomaselli GF, Mahaffey KW, Cuker A, et al. 2020 ACC expert consensus decision pathway on management of bleeding in patients on oral anticoagulants. Journal of the American College of Cardiology. 2020; 76 (5):594-622. DOI: 10.1016/j.jacc.2020.04.053 - 45.
Ruiz Ortiz M, Muniz J, Rana Miguez P, et al. Inappropriate doses of direct oral anticoagulants in real-world clinical practice: Prevalence and associated factors. A subanalysis of the FANTASIIA registry. Europace. 2018; 20 (10):1577-1583. DOI: 10.1093/europace/eux316 - 46.
Yao X, Shah ND, Sangaralingham LR, et al. Non-vitamin K antagonist oral anticoagulant dosing in patients with atrial fibrillation and renal dysfunction. Journal of the American College of Cardiology. 2017; 69 :2779-2790. DOI: 10.1016/j.jacc.2017.03.600 - 47.
Raskob GE, Nv E, Verhamme P, et al. Edoxaban for the treatment of cancer-associated venous thromboembolism. The New England Journal of Medicine. 2018; 378 :615-624. DOI: 10.1056/NEJMoa1711948 - 48.
Young AM, Marshall A, Thirlwall J, et al. Comparison of an oral factor Xa inhibitor with low molecular weight heparin in patients with cancer with venous thromboembolism: Results of a randomized trial (SELECT-D). Journal of Clinical Oncology. 2018; 36 (20):2017-2023. DOI: 10.1200/JCO.2018.78.8034 - 49.
McBane RD, Wysokinski WE, Le-Rademacher JG, et al. Apixaban and dalteparin in active malignancy-associated venous thromboembolism: The ADAM VTE trial. Journal of Thrombosis and Haemostasis. 2020; 18 (2):411-421. DOI: 10.1111/jth.14662. Epub 2019 Nov 28 - 50.
Ageno W, Vedovati MC, Cohen A. Bleeding with apixaban and dalteparin in patients with cancer-associated venous thromboembolism: Results from the Caravaggio study. Thrombosis and Haemostasis. 2021; 121 (5):616-624. DOI: 10.1055/s-0040-1720975 - 51.
Boonyawat K, Caron F, Li A, et al. Association of body weight with efficacy and safety outcomes in phase III randomized controlled trials of direct oral anticoagulants: A systematic review and meta-analysis. Journal of Thrombosis and Haemostasis. 2017; 15 :1322-1333. DOI: 10.1111/jth.13701 - 52.
Sanghai S, Wong C, Wang Z, et al. Rates of potentially inappropriate dosing of direct-acting oral anticoagulants and associations with geriatric conditions among older patients with atrial fibrillation: The SAGE-AF study. Journal of the American Heart Association. 2020; 9 :e014108. DOI: 10.1161/JAHA.119.014108 - 53.
Steffel J, Verhamme P, Potpara TS, et al. The 2018 European heart rhythm association practical guide on the use of non-vitamin K antagonist oral anticoagulants in patients with atrial fibrillation. European Heart Journal. 2018; 39 :1330-1393. DOI: 10.1093/eurheartj/ehy136 - 54.
Qamar A, Vaduganathan M, Greenberger NJ, et al. Oral anticoagulation in patients with liver disease. Journal of the American College of Cardiology. 2018; 71 :2162-2175. DOI: 10.1016/j.jacc.2018.03.023 - 55.
Semmler G, Pomej K, Bauer DJM, et al. Safety of direct oral anticoagulants in patients with advanced liver disease. Liver International. 2021; 41 (9):2159-2170. DOI: 10.1111/liv.14992 - 56.
Ambrosino P, Tarantino L, Di Minno G, et al. The risk of venous thromboembolism in patients with cirrhosis. A systematic review and meta-analysis. Thrombosis and Haemostasis. 2017; 117 (1):139-148. DOI: 10.1160/TH16-06-0450 - 57.
Ballestri S, Capitelli M, Fontana MC, et al. Direct oral anticoagulants in patients with liver disease in the era of non-alcoholic fatty liver disease global epidemic: A narrative review. Advances in Therapy. 2020; 37 :1910-1932. DOI: 10.1007/s12325-020-01307-z - 58.
Fanola CL, Norby FL, Shah AM, et al. Incident heart failure and long-term risk for venous thromboembolism. Journal of the American College of Cardiology. 2020; 75 (2):148-158. DOI: 10.1016/j.jacc.2019.10.058 - 59.
Gross PL, Chan NC. Thromboembolism in older adults. Frontiers in Medicine. 2021; 7 :470016. DOI: 10.3389/fmed.2020.470016 - 60.
Schutgens RE. DOAC in COVID-19: Yes or no? Hema. 2021; 5 (1):e526. DOI: 10.1097/HS9.0000000000000526 - 61.
Flaczyk A, Rosovsky RP, Reed CT, et al. Comparison of published guidelines for management of coagulopathy and thrombosis in critically ill patients with COVID 19: Implications for clinical practice and future investigations. Critical Care. 2020; 24 :559. DOI: 10.1186/s13054-020-03273-y - 62.
Aslan B, Akyüz A, Işık F, et al. The effect of chronic DOAC treatment on clinical outcomes of hospitalized patients with COVID-19. International Journal of Clinical Practice. 2021; 75 (9):e14467. DOI: 10.1111/ijcp.14467 - 63.
Connors JM, Brooks MM, Sciurba FC, et al. Effect of antithrombotic therapy on clinical outcomes in outpatients with clinically stable symptomatic COVID-19. The ACTIV-4B randomized clinical trial. Journal of the American Medical Association. 2021; 326 (17):1703-1712. DOI: 10.1001/jama.2021.17272 - 64.
Verhamme P, Yi AB, Segers A, et al. Abelacimab for prevention of venous thromboembolism august 12, 2021. The New England Journal of Medicine. 2021; 385 :609-617. DOI: 10.1056/NEJMoa2105872 - 65.
First patients enrolled in Bayer's Phase III trial for FXIa inhibitor asundexian - Clinical Trials Arena. Comment. February 10, 2023. Available from: www.clinicaltrialsarena.com/comment/bayer-trial-asundexian/