Open Access is an initiative that aims to make scientific research freely available to all. To date our community has made over 100 million downloads. It’s based on principles of collaboration, unobstructed discovery, and, most importantly, scientific progression. As PhD students, we found it difficult to access the research we needed, so we decided to create a new Open Access publisher that levels the playing field for scientists across the world. How? By making research easy to access, and puts the academic needs of the researchers before the business interests of publishers.
We are a community of more than 103,000 authors and editors from 3,291 institutions spanning 160 countries, including Nobel Prize winners and some of the world’s most-cited researchers. Publishing on IntechOpen allows authors to earn citations and find new collaborators, meaning more people see your work not only from your own field of study, but from other related fields too.
To purchase hard copies of this book, please contact the representative in India:
CBS Publishers & Distributors Pvt. Ltd.
www.cbspd.com
|
customercare@cbspd.com
Chronic kidney disease, defined as abnormal kidney function for more than 3 months, affects roughly 15% of the US, and approximately 40% of people with chronic kidney disease have type 2 diabetes. In the last decade, pharmacotherapies have been approved that may reduce chronic kidney disease progression and its complications. Sodium-glucose cotransporter-2 inhibitors (SGLT2Is) are recommended for diabetic kidney disease as they may reduce chronic kidney disease progression and cardiovascular events. Glucagon-like peptide 1 receptor agonists (GLP-1 RAs) are recommended for those with diabetic kidney disease who have not achieved glycemic targets with metformin and SGLT2Is. Finerenone (a nonsteroidal mineralocorticoid receptor antagonist [MRA]) may reduce chronic kidney disease progression and cardiovascular events. This chapter will review the evidence for these pharmacotherapies for diabetic kidney disease.
Internal Medicine Department, University of Texas at Austin Dell Medical School, Austin, TX, USA
Tessa K. Novick*
Internal Medicine Department, University of Texas at Austin Dell Medical School, Austin, TX, USA
*Address all correspondence to: tessa.novick@austin.utexas.edu
1. Introduction
Chronic kidney disease (CKD) is defined as the presence of an abnormality in kidney structure or function persisting for more than 3 months [1]. This includes one or more of the following: (1) estimated glomerular filtration rate (eGFR) less than 60 mL/min/1.73 m2; (2) urine albumin ≥30 mg per 24 h or urine albumin-to-creatinine ratio (UACR) ≥30 mg/g; (3) abnormalities in urine sediment, histology, or imaging suggestive of kidney damage; (4) renal tubular disorders; or (5) history of kidney transplantation [2]. Stages of CKD are based on UACR and eGFR and predict risk of progression to end-stage kidney disease (ESKD), defined as the requirement for renal replacement with chronic dialysis or kidney transplantation.
The prevalence of CKD in people with diabetes is approximately 20%, while it is 10% in those with prediabetes [1]. Because it is the leading cause of CKD, optimal screening and treatment of diabetes is essential in preventing CKD progression. This includes screening for proteinuria, optimizing glucose levels, and reducing cardiovascular morbidity and mortality [3].
Pharmacotherapy is a mainstay in the treatment of CKD for controlling blood pressure, glucose levels, and preventing CKD progression. Angiotensin converting enzyme inhibitors (ACEI) and angiotensin receptor blockers (ARB) demonstrated benefit for diabetic nephropathy decades ago. In 1993, The Collaborative Study Group Captopril Trial showed that in participants with insulin-dependent diabetes and proteinuria, captopril reduced the risk of serum creatinine doubling by 48%, and the composite risk of death, dialysis, and transplantation by 50% [4]. In 2001, The Irbesartan Diabetic Nephropathy Trial (IDNT) showed that irbesartan reduced disease progression in participants with diabetic nephropathy (32.6% vs. 39.0%; RR 0.8; p = 0.02), independent of its antihypertensive effects [5]. In 2001, The Reduction in End Points in NIDDM with the Angiotensin II Antagonist Losartan (RENAAL) study showed that losartan reduced progression to ESKD (19.6% vs. 25.5%; relative risk (RR) 0.72; p = 0.002) and serum creatinine doubling (21.6% vs. 26.0%; RR 0.75; p = 0.006) in participants with diabetic nephropathy [5].
Aside from ACEI/ARBs for CKD treatment, novel pharmacotherapies include sodium-glucose cotransporter-2 inhibitors (SGLT2Is), glucagon-like peptide 1 receptor agonists (GLP-1 RAs), and finerenone. SGLT2Is are recommended for diabetic kidney disease to prevent CKD progression and cardiovascular events [6]. GLP-1 RAs are recommended for those with diabetic kidney disease who have not achieved glycemic targets with metformin and SGLT2Is [7]. Finerenone (a nonsteroidal mineralocorticoid receptor antagonist [MRA]) has been shown to reduce CKD progression and cardiovascular events [8].
SGLT2Is reduce renal tubular glucose reabsorption, lowering blood glucose without stimulating insulin release. Several trials (CANVAS, CREDENCE, DAPA-CKD) have shown that SGLT2Is may reduce CKD progression (Table 1). The proposed mechanisms are: (1) reduction of glomerular hyperfiltration via increased delivery of sodium to the macula densa and afferent arteriolar constriction, which lowers intraglomerular pressure and reduces albuminuria, (2) reduction of tubular workload due to decreased SGLT2 co-transporter activity, and (3) reduced renal inflammation due to reduced albuminuria, tubular cell glucose, and induction of inflammatory cytokines and fibrotic mediators [9].
CANVAS
CREDENCE
DAPA-CKD
Study Design
Double-blind RCT
Double-blind RCT
Double-blind RCT
Participants
10,142
4401
4304
Inclusion Criteria
DM2, high CV risk
DM2, albuminuria
CKD, albuminuria, with or without DM2
Exclusion Criteria
DM1, DKA history
DM1, dialysis, transplant, non-DM kidney disease
DM1, PCKD, lupus nephritis, vasculitis, transplant history
Baseline Therapy
Antihyperglycemic agents or no therapy
ACEI/ARB therapy
Maximum ACEI/ARB therapy
Intervention
Canagliflozin (300 mg daily vs.100 mg daily) vs. placebo
Canagliflozin (100 mg daily) vs. placebo
Dapagliflozin (10 mg daily) vs. placebo
Outcomes
CV mortality, nonfatal MI, or nonfatal stroke: 26.9 vs. 31.5 participants per 1000 pt-yrs; HR 0.86; 95% CI 0.75–0.97
ESKD, Cr doubling, or renal/CV mortality: 43.2 vs. 61.2 events per 1000 pt-yrs; HR 0.70; 95% CI 0.59–0.82
Reduction in eGFR >50%, new ESKD, or renal/CV mortality: 9.2% vs. 14.5%; HR 0.61; 95% CI 0.51–0.72
Albuminuria increase >30%: 89.4 vs. 128.7 participants per 1000 pt-yrs; HR 0.73; 95% CI 0.67–0.79
Cr doubling: 20.7 vs. 33.8 events per 1000 pt-yrs; HR 0.60; 95% CI 0.48–0.76
Reduction in eGFR >50%: 5.2% vs. 9.3%; HR 0–53; 95% CI 0.42–0.67
Reduction in eGFR>40%, renal replacement or renal death: 5.5 vs. 9.0 participants per 1000 pt-yrs; HR 0.60; 95% CI 0.47–0.77
ESKD: 20.4 vs. 29.4 events per 1000 pt-yrs; HR 0.68; 95% CI 0.54–0.86
New ESKD: 5.1% vs. 7.5%; HR 0.64; 95% CI 0.50–0.82
Adverse Events
Mycotic genital infection, amputation risk (both higher in canagliflozin group)
Mycotic genital infection, DKA (higher in canagliflozin group).
Volume depletion (higher in dapagliflozin group)
Limitations
Few patients with baseline CKD
Statin use not controlled
Trial stopped early due to benefits; underpowering of less common endpoints
The CANagliflozin cardioVascular Assessment Study (CANVAS) involved two multicenter, randomized, placebo-controlled trials with 10,142 participants in 30 countries [10]. It was an intention-to-treat analysis that enrolled participants from 2009 to 2013 and followed participants for a median of 126 weeks, and it included those with type 2 diabetes with hemoglobin A1C (HbA1C) between 7% and 10.5% not currently on antihyperglycemic therapy. Progression of albuminuria, defined as >30% increase in UACR, and progression of CKD, defined as >40% reduction in eGFR, were lower in the canagliflozin group (hazard ratio [HR] 0.73; 95% confidence interval [CI] 0.67–0.79; and HR 0.60; 95% CI 0.47–0.77, respectively). Canagliflozin lowered the primary cardiovascular outcome, which included cardiovascular mortality, nonfatal myocardial infarction, and nonfatal stroke (HR 0.86, 95% CI 0.75–0.97) [10]. Significant adverse events included: risk of amputation, genital infections, and osmotic diuresis.
CANVAS has been criticized for having too few participants with baseline CKD, and so these results may not be generalizable to the population with CKD. Overall, these were novel results because previous medications such as insulin, sulfonylureas, and dipeptidyl peptidase-4 (DPP-4) inhibitors had not been associated with improvements in cardiovascular outcomes or survival. This study was the first to show that SLGT2Is may reduce kidney disease progression.
2.1.2 CREDENCE
The Canagliflozin and Renal Events in Diabetes with Established Nephropathy Clinical Evaluation (CREDENCE) trial was a prospective, double-blind randomized controlled trial with 4401 participants across 690 sites in 34 countries [11]. It was an intention-to-treat analysis that enrolled participants from 2014 to 2017, and followed them for a median of 2.6 years. The study included 4401 participants with type 2 diabetes (HbA1C 6.5–12.0%) and CKD stage G2-G3/A3 (baseline eGFR 30 to <90 mL/min/1.73m2 and UACR>300 to 5000 mg/24 h) taking ACEI or ARB therapy. Those randomized to canagliflozin had a lower risk of developing the primary composite kidney outcome of doubling of serum creatinine, ESKD, or death from a kidney or cardiovascular cause, compared with those randomized to placebo (HR 0.70; 95% CI 0.59–0.82; p < 0.01). Significant adverse events included genital mycotic infection and diabetic ketoacidosis. A criticism of this study was that statin use was not universal in this trial and could have confounding effects since statins have been shown to prevent cardiovascular events [12].
2.1.3 DAPA-CKD
The Dapagliflozin And Prevention of Adverse Outcomes in Chronic Kidney Disease (DAPA-CKD) trial was a multicenter, double-blind, randomized placebo controlled trial with 4304 participants enrolled from 2017 to 2018 in 450 sites from 20 countries [13]. It was an intention-to-treat analysis with a mean follow-up of 2.4 years. Participants had eGFR between 25 and 75 mL/min/1.73 m2, UACR between 200 and 5000 mg/g, and were already on maximum ACEI/ARB therapy. This study found reduced primary outcome of eGFR decline >50%, new ESKD, or kidney or CVD mortality in the dapagliflozin group (9.2% vs. 14.5%, HR 0.61, 95% CI 0.51–0.72). A subgroup analysis revealed that in participants without diabetes, dapagliflozin reduced the primary outcome (HR 0.50; CI 0.35–0.72).
2.1.4 EMPA-KIDNEY
The EMPAgliflozin Once Daily to Assess Cardiorenal Outcome in Patients with Chronic KIDNEY Disease (EMPA-KIDNEY) trial was designed to investigate the effect of empagliflozin on kidney outcomes and cardiovascular death in people with CKD [14]. It began in 2019 and is estimated to be completed near the end of 2022. This trial will shed light on whether SGLT2Is benefit people with proteinuria regardless of diabetes status.
2.2 Glucagon-like peptide-1 receptor agonists
Glucagon-like peptide-1 receptor agonists (GLP-1 RAs) stimulate glucose-dependent insulin secretion. They are thought of as a “satiety peptide” that promotes release of insulin when glucose is elevated, while also decreasing prandial glucagon and delaying gastric emptying. GLP-1 RAs have the added benefit of promoting weight loss. Because they have shown to improve cardiovascular outcomes in the LEADER and REWIND trials among others, the American Diabetes Association (ADA) recommends GLP-1 RAs in people with type 2 diabetes with cardiovascular disease (Table 2) [7]. However, in a meta-analysis, GLP-1 RAs did not significantly decrease the risk of kidney events (RR 0.86 [0.72–1.03]) [15]. There has not been substantial evidence to date that GLP-1 agonists slow CKD progression, as there has not been a published GLP-1 RA trial with primary endpoint of kidney events. Existing data on kidney outcomes have been provided by cardiovascular outcomes trials.
LEADER
REWIND
Study design
Double-blind RCT
Double-blind RCT
Participants
9340
9901
Inclusion Criteria
DM2
DM2, CV risk factors
Exclusion Criteria
DM1, previous use of GLP-1 RA, ESKD, prior transplant
eGFR<15 ml/min/1.73 m2, life expectancy<1 yr, severe hypoglycemia in previous yr
Baseline Therapy
Antihyperglycemic agents or no therapy
Antihyperglycemic agents or no therapy
Intervention
Liraglutide (1.8 mg daily) vs. placebo
Dulaglutide (1.5 mg daily) vs. placebo
Outcomes
Nonfatal MI, nonfatal stroke, or CV mortality: 13.0% vs. 14.9%; HR 0.87; 95% CI 0.78–0.97
Nonfatal MI, nonfatal stroke, or CV mortality: 12.0% vs. 13.4%; HR 0.88; 95% CI 0.79–0.99
All-cause mortality: 8.3% vs. 9.6%; HR 0.78; 95% CI 0.74–0.97
New albuminuria>300 mg/g, reduction in eGFR>30%, or need for renal replacement: 17.1% vs. 19.6%; HR 0.85; 95% CI 0.77–0.93
New or persistent albuminuria, Cr doubling, CRRT need, or renal death: 5.7% vs. 7.2%; HR 0.78; 95% CI 0.67–0.92
Adverse Events
Severe hypoglycemia (higher in placebo group), acute gallstone disease (higher in liraglutide group)
GI adverse events (higher in dulaglutide group)
Limitations
Unequal statin use between groups
>25% participants were not taking study drug at last visit
Table 2.
Clinical trials involving GLP-1 RAs.
Abbreviations: GLP-1 RAs—Glucagon-like peptide-1 receptor agonists; LEADER—Liraglutide Effect and Action in Diabetes: Evaluation of Cardiovascular Outcome Results; REWIND—Researching Cardiovascular Outcomes with a Weekly Incretin in Diabetes; RCT—randomized controlled trial; DM2—type 2 diabetes mellitus; CV—cardiovascular; DM1—type 1 diabetes mellitus; ESKD—end-stage kidney disease; eGFR—estimated glomerular filtration rate; yr.—year; mg—milligrams; MI—myocardial infarction; HR—hazard ratio; CI—confidence interval; Cr—creatinine; CRRT—continuous renal replacement therapy; mg/g—milligrams per gram; GI—gastrointestinal.
2.2.1 LEADER
In the Liraglutide Effect and Action in Diabetes: Evaluation of Cardiovascular Outcome Results (LEADER) trial, liraglutide was found to reduce cardiovascular events compared to placebo in participants with diabetes at risk for cardiovascular disease [16]. This study was a multicenter, randomized, controlled trial that evaluated 9340 participants with type 2 diabetes at 410 sites in 32 countries. Participants had diabetes and cardiovascular diseases, including peripheral vascular disease, CKD, symptomatic congestive heart failure, or hypertension with left ventricular hypertrophy, among others. This intention-to-treat analysis enrolled participants from 2010 to 2012 and followed them up for a median of 3.8 years. The primary outcome was a composite of nonfatal myocardial infarction, nonfatal stroke, and cardiovascular mortality. Those who received liraglutide had a lower primary outcome compared to placebo (13.0% vs. 14.9%, HR 0.87, 95% CI 0.78–0.97). Those in the liraglutide group also had lower all-cause mortality (8.2% vs. 9.6%, HR 0.78, 95% CI 0.74–0.97, p = 0.02), and a lower rate of the kidney composite endpoint of new or persistent UACR>300 mg/g, doubling of serum creatinine and eGFR<45 ml/min/1.73m2, need for continuous renal replacement therapy, or death due to kidney disease (5.7% vs. 7.2%, HR 0.78, 95% CI 0.67–0.92, p = 0.003).
2.2.2 REWIND
The Researching Cardiovascular Outcomes with a Weekly Incretin in Diabetes (REWIND) trial was a multicenter randomized, double-blind controlled trial spanning 371 sites in 24 countries [17, 18]. It examined participants with type 2 diabetes, cardiovascular risk factors, and eGFR>15. The primary composite outcome included non-fatal MI, non-fatal stroke, or death from cardiovascular causes. Compared to placebo, those in the dulaglutide group had fewer primary outcome events (12.0% vs. 13.4%, HR 0.88, 95% CI 0.79–0.99; p = 0.026). However, all-cause mortality was not significantly different between the groups (10.8% vs. 12.0%, HR 0.90, 95% CI 0.80–1.01; p = 0.067).
The kidney outcome evaluated was a composite of new albuminuria>300 mg/g, decline in eGFR 30% or more from baseline, or need for renal replacement therapy. Fewer in the dulaglutide group exhibited the composite kidney outcome (17.1% vs. 19.6%; HR 0.85; 95% CI 0.77–0.93; p = 0.0004). The most prominent effect was reduction of albuminuria (HR 0.77; 95% CI 0.68–0.87; p < 0.0001).
2.2.3 FLOW
The Effect of Semaglutide Versus Placebo on the Progression of Renal Impairment in Subjects With Type 2 Diabetes and Chronic Kidney Disease (FLOW) trial was the first kidney outcome trial involving GLP-1 RAs, and it sought to determine the effects of semaglutide on kidney outcomes in people with type 2 diabetes [19, 20]. It began in 2019 and is estimated to be completed in 2024.
2.3 Finerenone
Finerenone is a nonsteroidal, selective mineralocorticoid receptor antagonist. It has been studied recently in two trials (FIDELIO-DKD and FIGARO-DKD) to determine its effect on cardiovascular and kidney outcomes (Table 3). Its proposed mechanism is through decreased mineralocorticoid receptor activation, and subsequent reduction in inflammation, fibrosis, and reactive oxygen species [21].
FIDELIO-DKD
FIGARO-DKD
Study Design
Double-blind RCT
Double-blind RCT
Participants
5734
7437
Inclusion Criteria
DM2, CKD
DM2, CKD, albuminuria
Exclusion Criteria
Non-diabetic kidney disease, already on MRA, kidney transplant
Reduction in eGFR > 40%, kidney failure, or death from kidney causes: 17.8 vs. 21.1%; HR 0.82; 95% CI 0.73–0.93
CV death, nonfatal MI, nonfatal stroke, or heart failure hospitalization: 12.4% vs. 14.2%; HR 0.87; 95% CI 0.76–0.98
CV death, nonfatal myocardial infarction, nonfatal stroke, or heart failure hospitalization: 13.0% vs. 14.8%; HR 0.86; 95% CI 0.75–0.99
Reduction in eGFR>40%, kidney failure, or death from kidney causes: 9.5% vs. 10.8%; HR 0.87; 95% CI 0.76–1.01
Adverse Events
Hyperkalemia (higher in finerenone group)
Hyperkalemia (higher in finerenone group)
Limitations
Most patients had advanced CKD; only 4.7% Black patients
Only 3.5% Black patients
Table 3.
Clinical trials involving Finerenone.
Abbreviations: FIDELIO-DKD—FInerenone in reducing kiDnEy faiLure and dIsease prOgression in Diabetic Kidney Disease; FIGARO-DKD—Finerenone in Subjects With Type 2 Diabetes Mellitus and the Clinical Diagnosis of Diabetic Kidney Disease; RCT—randomized controlled trial; DM2—type 2 diabetes mellitus; CKD—chronic kidney disease; MRA—mineralocorticoid receptor antagonist; HFrEF—heart failure with reduced ejection fraction; UACR—urine albumin-creatinine ratio; mg/g—milligrams per gram; ACEI—angiotensin converting enzyme inhibitor; ARB—angiotensin receptor blocker; mg—milligrams; eGFR—estimated glomerular filtration rate; HR—hazard ratio; CI—confidence interval; CV—cardiovascular; MI—myocardial infarction; CKD—chronic kidney disease.
2.3.1 FIDELIO-DKD
The FInerenone in reducing kiDnEy faiLure and dIsease prOgression in Diabetic Kidney Disease (FIDELIO-DKD) trial was a double-blinded randomized trial that showed in participants with CKD and type 2 diabetes, finerenone may lower risk of CKD progression and cardiovascular events [22]. The primary outcome was a composite of a sustained decrease of >40% in eGFR from baseline over a period of >4 weeks, or death from kidney causes. The secondary outcome event was a composite of death from cardiovascular causes, nonfatal myocardial infarction, nonfatal stroke, or hospitalization for heart failure. The primary and secondary outcomes occurred less in the finerenone group (17.8% vs. 21.1%; HR 0.82; 95% CI 0.73–0.93 for the primary outcome; 13.0% vs. 14.8%; HR 0.86; 95% CI 0.75–0.99 for the secondary outcome). Hyperkalemia-related trial discontinuation was higher in the finerenone group vs. placebo (2.3% and 0.9%, respectively).
Finerenone may also reduce new-onset atrial fibrillation/flutter in people with CKD and type 2 diabetes [23]. In this study, new onset atrial fibrillation was lower in the finerenone group compared to placebo (3.2% vs. 4.5%, p = 0.016).
2.3.2 FIGARO-DKD
The Finerenone in Subjects With Type 2 Diabetes Mellitus and the Clinical Diagnosis of Diabetic Kidney Disease (FIGARO-DKD) trial was a double-blind randomized trial that finerenone may reduce new onset heart failure and heart failure hospitalization rate among people with CKD and type 2 diabetes [8]. In this study of 7437 participants, 3686 were given finerenone, while there were 3666 in the placebo group. The primary outcome was a composite of cardiovascular death, nonfatal MI, nonfatal stroke, or heart failure hospitalization. This primary outcome event occurred in 12.4% in the finerenone group, and in 14.2% of the placebo group (HR 0.87; 95% CI 0.76–0.98).
Most of the benefit of finerenone was found to be from heart failure hospitalization (HR 0.71). The secondary outcome was a composite of kidney failure, defined as a sustained decrease in eGFR from baseline of at least 40%, or death from kidney causes. This event occurred in 9.5% of the finerenone group and 10.8% of the placebo group (HR 0.87; 95% CI 0.76–1.01). Of note, hyperkalemia-related discontinuation of the trial regimen was higher in the finerenone group (1.2% vs. 0.4%).
In people with type 2 diabetes, canagliflozin may reduce albuminuria progression, and the composite outcome of doubling of serum creatinine, ESKD, or kidney or cardiovascular mortality [10, 11]. In people with CKD, dapagliflozin may reduce the composite outcome of eGFR decline >50%, new ESKD, or kidney or CVD mortality, independent of diabetes status [13]. In people with diabetes at risk for cardiovascular disease, liraglutide may reduce all-cause mortality, and the composite outcome of new or persistent albuminuria, doubling of serum creatinine and eGFR<45 ml/min/1.73 m2, need for continuous renal replacement therapy, or death due to kidney disease [16]. In people with diabetes and cardiovascular risk factors, dulaglutide may reduce the composite outcome of new albuminuria > 300 mg/g, decline in eGFR 30% or more from baseline, or need for renal replacement therapy [18]. In people with CKD and type 2 diabetes, finerenone may lower the composite outcome of sustained decrease of at least 40% in the eGFR, or death from kidney causes [8, 22].
3.2 Comparison of newer therapies to established therapies
It is important to note that the reduction in kidney events was higher in general for ACEI/ARBs compared to SGLT2Is or finerenone, although these therapies have not been directly compared [5, 10, 11, 22]. In the SGLT2I and finerenone trials, participants were also on ACEI/ARB therapies. Thus ACEI/ARB are still first line for treatment of kidney disease with albuminuria. Studies have not compared SGLT2Is to finerenone. The effects of combined SGLT2I and finerenone therapy on kidney outcomes are unknown. Both SGLT2Is and finerenone cause adverse events, which must also be considered along with their benefits [24].
3.3 Approach to therapy along the continuum of diabetic kidney disease
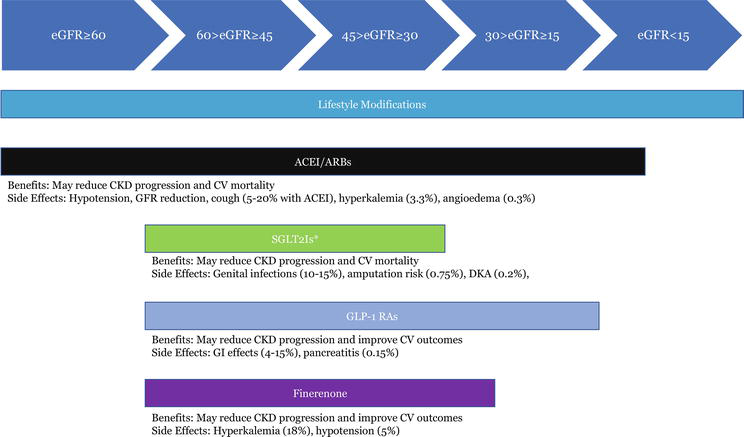
All people with CKD should follow lifestyle modifications (increased exercise, low sodium diet, protein restriction, and reduced dietary acid loads) to manage blood pressure and glucose levels, and to reduce cardiovascular risk (Figure 1).
Figure 1.
DKD treatment continuum. This illustrates therapeutic approaches that may reduce DKD progression, and the associated eGFRs for which they have been studied. Listed underneath each drug class are the benefits and side effects. Abbreviations: DKD—diabetic kidney disease; eGFR—estimated glomerular filtration rate; CKD—chronic kidney disease; ACEI—angiotensin converting enzyme inhibitor; ARB—angiotensin receptor blocker; CV—cardiovascular; GFR—glomerular filtration rate; SGLT2Is—sodium-glucose cotransporter-2 inhibitors; DKA—diabetic ketoacidosis; GLP-1 RAs—glucagon-like peptide-1 receptor agonists; GI—gastrointestinal.
*SGLT2Is may be continued for eGFR < 30 mL/min/1.73 m2 given that they were initiated when eGFR > 30 mL/min/1.73 m2, and they may be continued until a person is on dialysis.
ACEI/ARB therapy is recommended for treatment in people with CKD (diabetic or non-diabetic), with urine albumin excretion>30 mg/day. They can also be used as initial pharmacotherapy to treat hypertension. These medications should be held in the setting of acute kidney injury and should be discontinued if associated with hyperkalemia that cannot be controlled with dietary restriction or potassium binders [24].
SGLT2Is should be initiated in people with type 2 diabetes and CKD with eGFR≥30 mL/min/1.73 m2. They have not been studied in people with eGFR <30 ml/min/1.73 m2, thus they should not be initiated in people with CKD stages 4–5. Studies have shown that if they are started when eGFR is above 30 mL/min/1.73 m2, they can be continued until the individual is on dialysis and then stopped [25, 26]. However, they likely have benefit in people with eGFR<30 mL/min/1.73 m2 based on a pooled analysis of phase 3 randomized controlled trials [27]. Dapagliflozin may benefit people who have albuminuria who do not have diabetes [13]. The DAPA-CKD study excluded patients with type 1 diabetes and specific kidney conditions including polycystic kidney disease, lupus nephritis, vasculitis, and history of organ transplantation [13]. Therefore, outcomes of SGLT2Is in these specific populations are unknown. SGLT2Is should be used with caution in people with a prior lower extremity amputation or threat of amputation. Adverse effects include polyuria, hyperkalemia, a higher risk for genital mycotic infections, diabetic ketoacidosis, bony fractures, and the need for lower limb amputations.
GLP-1 RAs may be used in people with type 2 diabetes and diabetic kidney disease, after metformin and SGLT2Is have not shown improved glycemic control. Studies have shown that liraglutide and dulaglutide improved kidney outcomes, although most of the trials involving GLP-agonists focused on improved cardiovascular outcomes as the primary endpoint. In REWIND, dulaglutide was studied in people with eGFR>15 mL/min/1.73 m2, thus it may be used for Stage 4 CKD. Adverse effects include diarrhea, nausea, headache, and hypoglycemia.
Finerenone may be used in people with type 2 diabetes and diabetic kidney disease, with eGFR≥25 mL/min/1.73 m2. It has not been studied among people with eGFR<25 mL/min/1.73 m2. The risk of hyperkalemia may be higher among people on concurrent finerenone and ACEI/ARB therapy [28]. Caution is advised among people with hepatic impairment and those taking strong CYP3A4 inhibitors, because finerenone is a sensitive CPY3A4 substrate and its effects may be increased through CYP3A4 inhibition [29].
3.4 Approaches to develop therapeutics for CKD progression
The rising global burden of CKD requires comprehensive educational campaigns, screening for early CKD, and novel therapeutics to mitigate progression to ESKD and the need for dialysis [30]. Coordination between scientists, policymakers, physicians, pharmaceutical companies, insurance companies, governments, and other key players is paramount in advancing therapies from bench to bedside. The relationship between CVD and CKD is complex—it is known that CVD is a common complication in people with CKD, yet there are limited evidence and therapies to prevent CVD in people with CKD [31]. Blood pressure control, statin use, and renin-angiotensin-aldosterone axis blockade have improved cardiovascular outcomes, however excess mortality remains in people with CKD compared with the general population [3]. There is also an increasing incidence of CKD resulting from unknown causes in certain “hotspots” that exacerbates this problem [32].
Pollock et al. outlined four major goals towards establishing and validating novel therapeutic targets to reduce CKD progression [33]. The first goal is to improve identification of therapeutic targets. This requires use of biomarkers, −omics data, and cross-disciplinary research to identify pathophysiologic mechanisms. For example, what we learn about the physiological mechanism of kidney fibrosis may be useful in informing drug mechanistic approaches to prevent fibrosis leading to CKD. Acute kidney injury (AKI) is associated with CKD development, and understanding the multifactorial relationship between the two is crucial [34].
The second goal is to enhance preclinical and early clinical development. This requires improving clinical networks for CKD populations to facilitate trial recruitment, developing infrastructure to study human tissue to better understand CKD progression, improving collaboration between academic research scientists and the biotechnology company researchers, and rewarding academic career development when involved with industry to develop therapeutics.
The third goal is to increase availability of novel therapeutic approaches. This entails evaluating opportunities for repurposing drugs to find treatments for CKD and its complications, as well as improving access to costly drugs and biologics in low- and middle-income countries.
The fourth goal—encouraging investment in CKD therapeutics—is crucial to the overall global mission to reduce CKD progression. This includes marketing economic opportunity and developing business cases, lobbying for funding from governments and industry, and documenting differences in CKD treatment practice patterns and the therapeutic needs of different countries. Therapeutics in development for CKD include those mentioned in this article as well as drugs that reduce inflammation and mitigate oxidative injury [35].
ACEI/ARBs have been the mainstay for preventing CKD progression for the last several decades [36]. SGLT2Is and finerenone are newer therapies that may prevent disease progression in those with diabetic kidney disease, while GLP-1 RAs are useful in preventing cardiovascular disease in those with diabetes and cardiovascular risk factors. GLP-1 RAs have shown promise in preventing kidney outcomes through primary cardiovascular outcomes trials, but they have not directly been tested for kidney outcomes as a primary endpoint.
As the global burden of CKD rises, it is essential to improve the therapeutic development process from all perspectives, including academic research and industry. The scientific process of advancing basic and clinical biological research to identify therapeutic targets is just as critical as creating avenues for investment in CKD research, global collaboration in implementing clinical trials and information sharing, and improving access to costly drugs. To arrive at a comprehensive solution for CKD, many more advances in the basic science and genetics of kidney disease are essential. The increasing need to serve people with CKD will hopefully engender an era of evidence-based therapeutics that will revolutionize CKD care such that reaching ESKD will be a rarity.
No conflicts of interest or funding sources are reported.
References
1.CDC Surveillance System: CKD Prevalence by Diabetes Mellitus Status. 2022. Available from: https://nccd.cdc.gov/ckd/detail.aspx?Qnum=Q702
2.Chen TK, Knicely DH, Grams ME. Chronic kidney disease diagnosis and management. Journal of the American Medical Association. 2019;322:1294-1304
3.Kalantar-Zadeh K, Jafar TH, Nitsch D, Neuen BL, Perkovic V. Chronic kidney disease. The Lancet. 2021;398:786-802
4.Lewis EJ, Hunsicker LG, Bain RP, Rohde RD. The effect of angiotensin-converting-enzyme inhibition on diabetic nephropathy. The New England Journal of Medicine Massachusetts Medical Society. 1993;329:1456-1462
5.Sica DA, Bakris GL. Type 2 diabetes: RENAAL and IDNT—The emergence of new treatment options. Journal of Clinical Hypertension. 2007;4:52-57
6.Alicic RZ, Johnson EJ, Tuttle KR. SGLT2 inhibition for the prevention and treatment of diabetic kidney disease: A review. American Journal of Kidney Diseases is the official journal of the National Kidney Foundation. 2018;72:267-277
7.Li S, Vandvik PO, Lytvyn L, Guyatt GH, Palmer SC, Rodriguez-Gutierrez R, et al. SGLT-2 inhibitors or GLP-1 receptor agonists for adults with type 2 diabetes: A clinical practice guideline. BMJ. 2021;373:n1091
8.Pitt B, Filippatos G, Agarwal R, Anker SD, Bakris GL, Rossing P, et al. Cardiovascular events with Finerenone in kidney disease and type 2 diabetes. The New England Journal of Medicine. 2021;385:2252-2263
9.Wheeler DC, James J, Patel D, Viljoen A, Ali A, Evans M, et al. SGLT2 inhibitors: Slowing of chronic kidney disease progression in type 2 diabetes. Diabetes Therapy. 2020;11:2757-2774
10.Neal B, Perkovic V, Mahaffey KW, de Zeeuw D, Fulcher G, Erondu N, et al. Canagliflozin and cardiovascular and renal events in type 2 diabetes. The New England Journal of Medicine. 2017;377:644-657
11.Perkovic V, Jardine MJ, Neal B, Bompoint S, Heerspink HJL, Charytan DM, et al. Canagliflozin and renal outcomes in type 2 diabetes and nephropathy. The New England Journal of Medicine Massachusetts Medical Society. 2019;380:2295-2306
12.Ziaeian B, Fonarow GC. Statins and the prevention of heart disease. JAMA Cardiology. 2017;2:464
13.Heerspink HJL, Stefánsson BV, Correa-Rotter R, Chertow GM, Greene T, Hou F-F, et al. Dapagliflozin in patients with chronic kidney disease. The New England Journal of Medicine. 2020;383:1436-1446
14.B Ingelheim. A Multicentre International Randomized Parallel Group Double-blind Placebo-controlled Clinical Trial of EMPAgliflozin Once Daily to Assess Cardio-renal Outcomes in Patients With Chronic KIDNEY Disease. clinicaltrials.gov; 2022 Mar. Report No.: NCT03594110. Available from: https://clinicaltrials.gov/ct2/show/NCT03594110
15.Yamada T, Wakabayashi M, Bhalla A, Chopra N, Miyashita H, Mikami T, et al. Cardiovascular and renal outcomes with SGLT-2 inhibitors versus GLP-1 receptor agonists in patients with type 2 diabetes mellitus and chronic kidney disease: A systematic review and network meta-analysis. Cardiovascular Diabetology. 2021;20:14
16.Mann JFE, Ørsted DD, Brown-Frandsen K, Marso SP, Poulter NR, Rasmussen S, et al. Liraglutide and renal outcomes in type 2 diabetes. The New England Journal of Medicine Massachusetts Medical Society. 2017;377:839-848
17.Gerstein HC, Colhoun HM, Dagenais GR, Diaz R, Lakshmanan M, Pais P, et al. Dulaglutide and cardiovascular outcomes in type 2 diabetes (REWIND): A double-blind, randomised placebo-controlled trial. Lancet London England. 2019;394:121-130
18.Gerstein HC, Colhoun HM, Dagenais GR, Diaz R, Lakshmanan M, Pais P, et al. Dulaglutide and renal outcomes in type 2 diabetes: An exploratory analysis of the REWIND randomised, placebo-controlled trial. Lancet London England. 2019;394:131-138
19.Mosenzon O, Schechter M, Leibowitz G. Kidney outcomes with glucagon-like Peptide-1 receptor agonists in patients with type 2 diabetes. Advances in Chronic Kidney Disease. 2021;28:347-360
20.Novo Nordisk AS. Renal Mode of Action of Semaglutide in Patients With Type 2 Diabetes and Chronic Kidney Disease. clinicaltrials.gov; 2022 Mar. Report No.: NCT04865770. Available from: https://clinicaltrials.gov/ct2/show/NCT04865770
21.Agarwal R, Kolkhof P, Bakris G, Bauersachs J, Haller H, Wada T, et al. Steroidal and non-steroidal mineralocorticoid receptor antagonists in cardiorenal medicine. European Heart Journal. 2020;42:152-161
22.Bakris GL, Agarwal R, Anker SD, Pitt B, Ruilope LM, Rossing P, et al. Effect of Finerenone on chronic kidney disease outcomes in type 2 diabetes. The New England Journal of Medicine. 2020;383:2219-2229
23.Filippatos G, Bakris GL, Pitt B, Agarwal R, Rossing P, Ruilope LM, et al. Finerenone reduces new-onset atrial fibrillation in patients with chronic kidney disease and type 2 diabetes. Journal of the American College of Cardiology. 2021;78:142-152
24.KDIGO 2020 Clinical Practice Guideline for Diabete.pdf. 2022. Available from: https://kdigo.org/wp-content/uploads/2020/10/KDIGO-2020-Diabetes-in-CKD-GL.pdf
25.Chertow GM, Vart P, Jongs N, Toto RD, Gorriz JL, Hou FF, et al. Effects of dapagliflozin in stage 4 chronic kidney disease. Journal of American Society of Nephrology. 2021;32:2352-2361
26.Bakris G, Oshima M, Mahaffey KW, Agarwal R, Cannon CP, Capuano G, et al. Effects of Canagliflozin in Patients with Baseline eGFR <30 ml/min per 1.73 m2: Subgroup Analysis of the Randomized CREDENCE Trial. Clinical Journal of the American Society of Nephrology. American Society of Nephrology. 2020;15:1705-1714
27.Dekkers CCJ, Wheeler DC, Sjöström CD, Stefansson BV, Cain V, Heerspink HJL. Effects of the sodium-glucose co-transporter 2 inhibitor dapagliflozin in patients with type 2 diabetes and stages 3b-4 chronic kidney disease. Nephrology Dialysis Transplantation. 2018;33:2005-2011
28.Rakugi H, Yamakawa S, Sugimoto K. Management of hyperkalemia during treatment with mineralocorticoid receptor blockers: Findings from esaxerenone. Hypertension Research, Nature Publishing Group. 2021;44:371-385
29.Heinig R, Gerisch M, Engelen A, Nagelschmitz J, Loewen S. Pharmacokinetics of the novel, selective, non-steroidal mineralocorticoid receptor antagonist Finerenone in healthy volunteers: Results from an absolute bioavailability study and drug–drug interaction studies In vitro and In vivo. European Journal of Drug Metabolism and Pharmacokinetics. 2018;43:715-727
30.Alebiosu CO, Ayodele OE. The global burden of chronic kidney disease and the way forward. Ethnicity & Disease. 2005;15:418-423
31.Vallianou NG, Mitesh S, Gkogkou A, Geladari E. Chronic kidney disease and cardiovascular disease: Is there any relationship? Current Cardiology Reviews. 2019;15:55-63
32.Obrador GT, Levin A. CKD hotspots: Challenges and areas of opportunity. Seminars in Nephrology. 2019;39:308-314
33.Pollock C, Zuk A, Anders H-J, Ganji MR, Johnson DW, Kasiske B, et al. The establishment and validation of novel therapeutic targets to retard progression of chronic kidney disease. Kidney International. Supplement. 2017;7:130-137
34.Sato Y, Takahashi M, Yanagita M. Pathophysiology of AKI to CKD progression. Seminars in Nephrology. 2020;40:206-215
35.Breyer MD, Susztak K. Developing treatments for chronic kidney disease in the 21st century. Seminars in Nephrology. 2016;36:436-447
36.Murphy DP, Drawz PE, Foley RN. Trends in angiotensin-converting enzyme inhibitor and angiotensin II receptor blocker use among those with impaired kidney function in the United States. Journal of the American Society of Nephrology. 2019;30:1314-1321
Written By
Nidharshan S. Anandasivam and Tessa K. Novick
Submitted: 28 March 2022Reviewed: 31 March 2022Published: 24 June 2022
 Open access peer-reviewed chapter
Open access peer-reviewed chapter