Open Access is an initiative that aims to make scientific research freely available to all. To date our community has made over 100 million downloads. It’s based on principles of collaboration, unobstructed discovery, and, most importantly, scientific progression. As PhD students, we found it difficult to access the research we needed, so we decided to create a new Open Access publisher that levels the playing field for scientists across the world. How? By making research easy to access, and puts the academic needs of the researchers before the business interests of publishers.
We are a community of more than 103,000 authors and editors from 3,291 institutions spanning 160 countries, including Nobel Prize winners and some of the world’s most-cited researchers. Publishing on IntechOpen allows authors to earn citations and find new collaborators, meaning more people see your work not only from your own field of study, but from other related fields too.
For people with schizophrenia, home environments that are readily understandable, easily managed, provide opportunities for self-expression and support psycho-social needs can enhance their wellbeing. Importantly, symptoms of schizophrenia (including agitation, anxiety, helplessness, perceptual distortion) can potentially be reduced through responsive accommodation design. The embedded potential of design of homes to offer support or create hindrances for people with schizophrenia has been poorly explored. Cues as to what things are and how to function in a space can be designed to provide support. This chapter records a multi-prong action research approach to develop a resource to assist designers and service providers create responsive residential environments for people with impeded cognitive functioning. Research from such fields as environmental psychology, sociology and design, together with discussions with people with schizophrenia, indicates that quality of life for people with schizophrenia can be enhanced through design. A key outcome is a Framework that enables the user to both understand the reason why a person with schizophrenia may respond to the environment in a particular way and how to design to acknowledge that potential response.
DEKS Design and Research Consultancy, Curtin University, Perth, West Australia
Elizabeth Karol*
DEKS Design and Research Consultancy, Curtin University, Perth, West Australia
*Address all correspondence to: elizabeth@deksdesignresearch.com.au
1. Introduction
Placed within a collection of chapters that cover a broad field of topics connected to schizophrenia, our work is a nonmedical approach to the subject of schizophrenia. Our backgrounds, based in architecture, interiors, building science, art therapy as well as research, influence this approach. Over our careers we have become intensely aware that environments can assist or inhibit the way people live; and consequently, that those responsible for the commissioning, design, construction, and management of accommodation have a responsibility to attend to these potential environmental influences through the projects they undertake. Our work has evolved to study home environments for those who live with schizophrenia.
When seeking insights into issues such as poor mental health, cognitive impairment or schizophrenia, people naturally are drawn to medical sources. The role of the creative arts, such as building design, does not immediately come to mind as a source of insight. However, as practitioners in this field we have come to realise the embedded potential in this area. By drawing on the theories of the sociologist, Bourdieu [1], it is evident that the body of knowledge from architecture and design can broaden and enrich the discussion and encourage new knowledge to emerge [2].
Consequently, we have taken a place ‘on the field’ as we join ‘the game’. Bourdieu’s concepts of ‘field’ and ‘habitus’ can inform propositions about design that can complement medical disciplines in achieving a common goal of improving quality of life for people with schizophrenia. In a ‘field’, disciplines have practices of thoughts and modes of operating that those within understand (initially through education and the like). However, these areas can become ‘struggles for legitimisation’ of one’s knowledge and practices in relation to its distinctiveness from other disciplines [1]. In this chapter, we present building design as a discipline that can potentially impact on the symptoms associated with cognitive difficulties (including poor mental health, cognitive impairment (CI) or schizophrenia) through responsive accommodation design.
Bourdieu referenced our unconscious perception of our position or place in the world as our ‘habitus’; and it is this which influences our actions and relations [3]. At an individual level, the habitus exists and provides the ‘sense’ of what action we are inclined to take; and we use the symbols available to us according to our habitus [1, 4]. The environment then not only provides the context, it holds ‘implicit rules that regulate transactions’ [5]; and are integral to the cultural system [6].
This is linked to discrimination, as ‘field’ and ‘habitus’ underpin meaning-making in respect to ‘discriminatory practices’ that may be embedded in our interpretations of others [7]. In the general community, people with impeded cognitive functioning (ICF)1 are often regarded as distinct from others. In the context of Bourdieu, this raises the notions of social capital and symbolic capital. Both reflect how people accidently or deliberately project their value or role on to the community; it is a means to identify distinction and differences [8]. It is acknowledged that architecture creates a field laden with social values [9] with symbols embedded within an environment. These symbols reflect societal standards, attitudes toward occupants, as well as economic, political, and educative values and associated worth (or not). This raises three questions. Does accommodation for those with ICF reflect a common understanding held by the society it is embedded in? Does the architectural profession apply the same common understanding? Is accommodation having a high social standing or rich social capital available to people with ICF?
In Australia, although many people with mental illnesses reside with family or in group houses, others (including those with schizophrenia) are dependent on social housing or low-cost housing [10]. This accommodation is often basic compared to the surrounding housing stock. Thus designers ‘create the aesthetics and the ideas that reinforce distinctions between groups’ [11]. Judgements are, in turn, made by and about the occupant of the accommodation. There is a social cost in making these judgements: firstly, for the resident and secondly, for families, organisations and/or society through the costs of care.
Having established the place of design in this conversation, we will describe our research in developing a Practice Document that can guide the development of good quality accommodation that potentially improves the quality of life for people with ICF. The core of the Practice Document is a Framework that informs the practice of responsive accommodation design for people with ICF.
This chapter outlines a series of projects that enabled us to achieve this end. Our process reflects both action research and design practice, where a situation is diagnosed to reveal the issue or problem; staged research carried out; actions proposed, undertaken, monitored, and evaluated prior to commencing the next stage of research. This continues until reaching a potential resolution; with each step bringing new understandings as well as cautionary notes.
In 2015, a provider of services and accommodation for people with disability, poor mental health and/or who were homeless in Perth, Western Australia approached us (as architects and academics). They requested our expertise to help them better understand the impact of accommodation design on their clients: an increasing number of whom had impaired cognitive abilities. The provider was expressly interested in aspects of design that reduce the amount of building damage wrought by clients when they were agitated, frustrated or generally unwell because of poor mental health. At that time therapeutic design in accommodation largely referred to universal design principles, which made accommodation accessible and manageable for those with mobility issues.
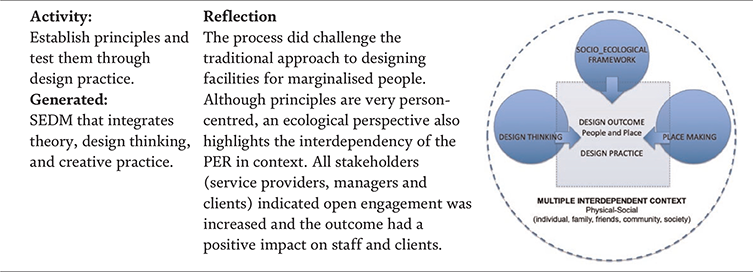
Our initial research showed that there were additional aspects of design that played a part in improving wellbeing for everyone, but particularly for those who are marginalised with ICF. These additional aspects revolved around what Pallasmaa, a highly acclaimed Finnish architect/academic referred to as “the process of living” [12]. He argued that for people to care about their accommodation they needed to think of it as ‘home’. Our research showed that for accommodation to become home it must allow for individualised expression of personality, patterns of life, rituals and routines. Ioannidou, an architectural researcher and designer, refers to “home as an intangible concept. It is the emotional and meaningful relationship between people and their familiar environment” [13].
We adapted this idea of intangibles to identify such aspects of the home environment that subtly create opportunities for wellbeing through opportunities for self-determination, a setting for personal possessions, spatial diversity and spatial delight. Thus, started our journey to discover how designers (including architects, interior designers, landscape architects) and service providers could commission, design, construct and manage accommodation for people with ICF, so it was better able to support this growing sector of our community.
By using design thinking as a reflective and evolutionary process over a series of projects we developed a generic Framework for designers and service providers. One that would help them foster health and wellbeing in the home for people with ICF. We used the generic Framework to establish design details for one particular condition, schizophrenia, thereby providing a demonstration case for how some symptoms of a mental health condition could be addressed through integration of certain design considerations. These design considerations are regarded as part of a package of support for people with schizophrenia.
In order to clarify the field of this study—particularly for those with limited knowledge of architectural and design theory—an overview is provided of three areas: the person-environment relationship (PER), accommodation design for people with ICF and action research.
2.1 Person-environment relationship
Many authors across environmental psychology and sociology as well as the design fields have described the impact of the person-environment relationship (PER) including how people feel and behave: see [14, 15, 16]. PER is well documented and various forms have been identified. Three forms of PER were described by Smith [7]. These ranged from a relationship where the environment was completely separate to the person to those where the environment and person were completely interdependent. Returning to Bourdieu’s concept of habitus, a person is said to have a ‘sense of the game’; knowing what is happening, what is expected and what to do [1]. That person may develop a strong sense of control, sense of identity or self-worth as the environmental setting reflects who they are and fosters self-expression as part everyday living.
So functional, emotional, psychological, and social aspects of a person’s life are all impacted by how they feel about their accommodation [17]. When translated to people with ICF, including those with schizophrenia, it is noted that a person may not be able to overcome negative environmental aspects, due to their cognitive attributes [17], and consequently may have their quality of life severely and detrimentally impacted. Although there is a broad and growing cross section of literature that relates physical places with impacts on people with ICF, in-depth knowledge of how this occurs and how design facilitates positive impacts is still scarce. Our work sought to navigate this field and explore the PER for people with schizophrenia.
2.2 Accommodation design for people with impeded cognitive functioning
The aim of architects and designers should be to not cause harm to the occupants of the buildings they design [18]. Our literature review [17] showed that the majority of houses designed and built in Australia meet functional needs. However, the intangible qualities of a home environment that address emotional, psychological, and/or social needs are rarely addressed. The building itself was generally considered as a ‘disembodied commodity’ [19], with no recognition that it is in fact “at the helm of a major force of neural functional dynamics” [20].
From the review of psychology and environmental psychology sources [15, 16, 21, 22, 23, 24, 25] the possible human responses which would indicate that a person at home felt emotionally, psychologically, and/or socially supported were identified. These responses included:
emotional and spiritual enhancement (including delight),
sense of belonging and control (including connectedness and privacy),
sense of self, self-esteem, and identity,
sense of dignity, homeliness, comfort, and affordance.
Sociologist and academic, Aaron Antonovsky [26] posited the concept of a sense of coherence. He identified physical, soulful, and spiritual coherence as being fundamental to health and wellbeing. Further to coherence, Lockard [25] references engagement with both space and community as being critical for well-being.
However, current housing stock in Western Australia shows little attention to the needs of people with an ongoing impairment in comprehension, reason, adaptive functioning, judgement, learning, or memory. There is little indication that designers are aware that by treating the home as a ‘disembodied commodity’ it may trigger significant responses and curtail a sense of wellbeing for people with ICF. From the literature there is minimal evidence, even from designers who professionally claim this space in their expertise, that detailed knowledge of how to incorporate appropriate intangible characteristics in a design is available.
For a person with ICF and limited choice in where they live, it seems to be particularly important that the home environment is designed to be both functionally and emotionally enabling. What is unclear is how designer-controlled elements can be extended to include intangible characteristics, so that a person with ICF feels nurtured and supported at home. We identified a need for evidence-based qualitative design research at the individual level and at a group level. Firstly, this was to analyse affordable home designs occupied by people with ICF in order to identify specifically what emotionally, psychologically and socially enabling intangible aspects exist. Secondly, to identify what people with CI value in their homes and what gives them a sense of well-being and emotional, psychological and social support.
An integrated approach is needed for holistic understanding of what it is to be at home as a person with ICF. This is complex, as people who have ICF have a wide variety of needs and are implicitly or explicitly conceptualised by researchers in each discipline in a variety of ways.
2.3 Action research
The Practice Document has been built from an ongoing process that involved continuous reflection and extrapolation to generate each subsequent step. This process is captured by an action research approach [27]. Such an approach is not linear, rather it is dynamic ‘where research, action, participation and evaluation interact’ [27] and strives to link practice and theory. Action research has traditionally been described as a repeated cycle involving planning, acting, observing and reflecting; and as such, mirrors the design process where the outcome emerges from a series of propositions, creations, tests against emergent criteria and reflection cycles toward each consequent proposition.
The involvement of those implicated is also part of action research – in this case accommodation providers, people from the target resident group, and researchers. The driver of action research is to generate change. In this case we aimed to challenge the accepted accommodation generated through current design practice and typical procurement strategies. It was recognised that this sector often has restricted budgets and opportunities to experiment with new ways of ‘doing architecture’. The involvement of a breadth of committees and funding bodies may mean that challenging everyday ways of doing is put to one side. However, improvement to accommodation design was worth exploring to ameliorate costs in terms of quality of life for residents, and financially for the providers and support workers.
The markers of success of an action research program are described by McTaggart [28] as being defensible, educative, politically effectual, and morally appropriate. The main aspects of action research that are common across the breadth of the various approaches described in the literature [29] are captured in Table 1. The seven aspects, summarised in Table 1, have been addressed in the development of the Practice Document.
Aspect of Action Research
Application to development of the Practice Document
Addressed real life issues and explored the need for change through literature reviews, conversations with providers, and interviews with people with schizophrenia.
Change intervention (change experiment)
A wide cross section of strategies of research were involved that led to a range of actions and propositions
Aims toward improvement
Improvement is targeted toward improved quality of life and wellbeing for future occupants with schizophrenia.
Cyclical process
Each step revealed relevant aspects that were then considered as part of the subsequent step/s.
Research relationship
Researchers are also designers, who developed a relationship with provider organisations, who in turn, provided access to properties and/or residents with ICF.
Educative
Designers, service providers, people with schizophrenia educated the researchers and will have open access to the findings.
Individuals are seen as members of social group
Service providers and accommodation providers for people with schizophrenia participated. People with schizophrenia are potential residents.
Table 1.
Summary of use of action research to develop practice document.
A multi-prong approach was required to develop a resource, a Practice Document, to assist designers and providers to create suitable environments for people with ICF. This approach evolved through a series of projects over many years. Each project arose through observations and reflections on the preceding activities. Collectively, they provide a pluralistic interrogation of what is going on.
3.1 Action research
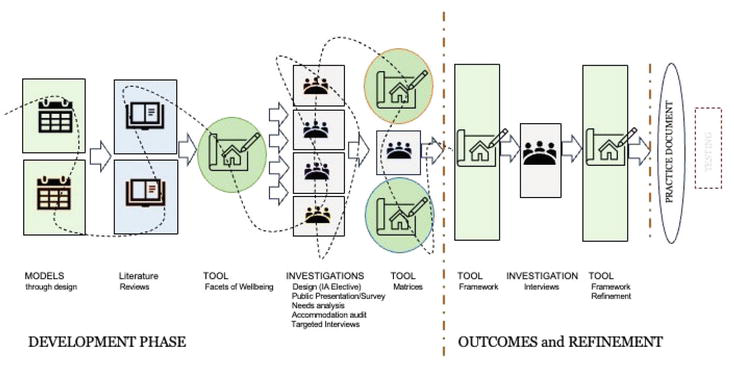
Figure 1 depicts the cycles of research over the decade. Each adds to providing an overall sense of the systematic expansion of our understanding. We also have noted any articles or reports produced en route and publicly available so that readers can explore the process and outcomes identified. The cycles did not necessarily occur in a neat linear manner as some investigations overlapped at times.
Figure 1.
Action embedded in research.
As noted in Figure 1 the process can be divided into two overarching phases: The Development Phase and the Outcomes and Refinement phase. The tool that emerged, called a Framework, is a comprehensive way of capturing the cycles of research and presenting the parameters that may influence design practice whilst including reference to the user’s (resident) condition (such as schizophrenia). The Framework was then contextualised within a Practice Document for those designing and investing in affordable housing for people with ICF. The hope is that others will build on this research by applying the Practice Document to the construction of accommodation for people with schizophrenia.
3.2 Cycles of research
Each cycle in the Development Phase is summarised in Tables 2–14. To succinctly explain the research, the activity and the outcome generated are stated, as well as a summary of our reflections. The Outcomes and Refinement Phase is then summarised.
3.2.1 The development phase
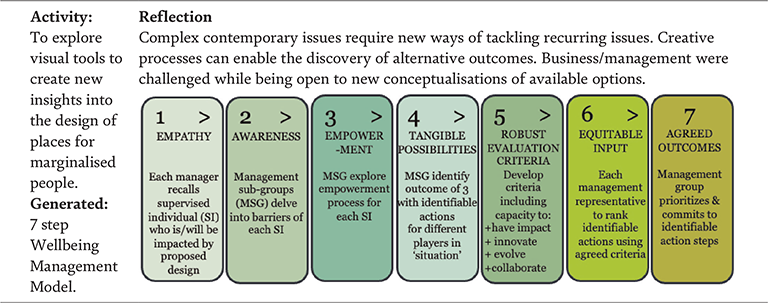
There were 13 cycles of research in the development phase, culminating in the Framework and Practice Document. We started by using design thinking to assist service provider managers to rethink ways of looking at the design of a day facility for homeless people (Table 2). We went on to develop a model that enabled better collaboration between all stakeholders when designing for marginalised people (Table 3). This was followed by literature reviews (Tables 4 and 5), creative design practice (Table 6), and an examination of language that captured the essence of the impact of intangible qualities of space (Table 9). Eventually we developed a design tool matrix that could assist designers and service providers to improve the PER in accommodation for people with ICF (Table 14).
Initially we were approached by a service provider to assist in the design of a day centre for homeless people. To achieve the best results within a very limited budget it was necessary to reframe the thinking of the service provider staff and collaboratively reconceptualize the situation and explore ways of tackling it. Table 2 summarises the project.
The proposed action resulting from the first project was to utilise creative practice processes on future projects at the brief and design development phases. We set out to apply this when considering alternative ways of approaching design for a supportive day centre for homeless people that integrates end-users as collaborators (Table 3).
It was recognised that design solutions to cater for people with ICF was needed. To start this process we initially needed to identify what was already known about the characteristics of domestic settings that support well-being for those with ICF. A literature review was carried out as summarised in Table 4.
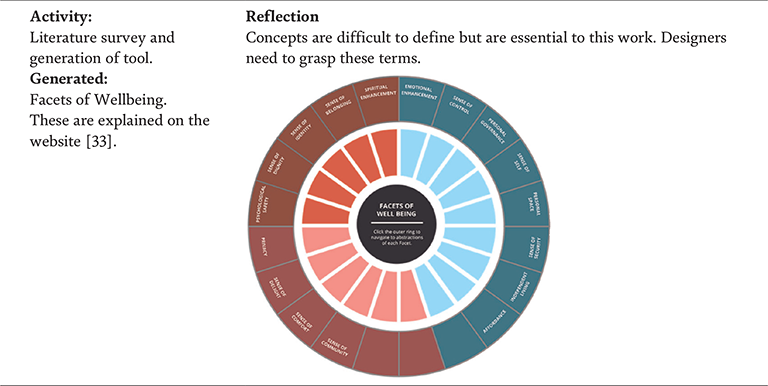
Activity: Literature review: home design and its impact on emotional, psychological, or social well-being for people with CI. Generated: Six Implications for Practice.
Reflection Researchers understand that pragmatic design inputs alone may not be sufficient. Others have shown or surmise that there are other “intangible” designer-controlled elements that have beneficial impacts. Information is sparse, and the degree of quality of life improvement for a person with CIP is not well understood. Identified aspects of the environment: (FE) Functionally enabling (FS) Functionally supportive (EPSE) Emotionally, psychologically, and/or socially enabling (EPSS) Emotionally, psychologically, and/or socially supportive (PER) Aspects of environment combined with resident’s particular attributes.
Table 4.
Literature review: Round 1.
The initial literature review identified an absence of research involving the nuanced qualities of the physical environment. We, therefore, proposed to revisit the literature to target these intangible qualities. In addition, we proposed it would also be of value to analyse affordable home designs to identify what emotionally, psychologically, and/or socially enabling intangible aspects exist; identify what people with CI value in their homes; and what gives them a sense of wellbeing and being emotionally, psychologically, and/or socially supportive (Table 5).
Activity: Literature Review Generated: An understanding of intangible qualities and their impacts.
Reflection Addressing intangible qualities has the potential to change the approach to environmental design and the user-experiences.
By identifying what the intangible qualities could be and their potential link to the built environment, we proposed that intangible qualities could be integrated into environmental design strategies to support the end users (in this case, residents).
To explore this proposal a project was developed for a small group of interior architecture students. Three university students were each to redesign an existing house for one of three hypothetical clients who each had ICF. They utilised the knowledge gained from the literature reviews but were not limited by what already existed as we aimed to generate ideas to stimulate new or alternative ways of looking at current design practice.
Table 6.
Design schemes suggested by interior architecture students.
The resultant designs proved very useful in exploring intangible qualities and extending accommodation design ideas. The ideas were presented to the accommodation provider and their affiliates (Table 7) to educate them on future possibilities and to gain feedback on feasibilities of the ideas generated. In addition, we hoped to generate further discussion and stimulate new ideas to share.
Activity: A public presentation of design schemes. Attendees and post-presentation visitors were surveyed. Generated: A public forum. A random sample of visitors commented via the survey.
Reflection 15 areas where ideas for improvements of existing accommodation were identified. Response was positive to the process and ideas at the forum. As only a small number responded to the survey further investigation is required.
Table 7.
Assessment by service provider and affiliates.
Through the discussions, we identified several ideas to explore further, particularly in the details embedded in suggestions. This also reinforced the value of integrating the intangible aspects in future designs. We, therefore, targeted those constructed architectural projects, noted as best-practice, to ascertain if intangible qualities were noted and considered. This was done via a desktop audit (Table 8).
Activity: A desk-top search to identify recognised projects where the designers /clients/stakeholders claiming to cater for users’ needs/aspirations beyond pragmatic requirements. Generated: Realisation that the impact of intangible design elements are not well understood.
Reflection The most informative projects state and depict significant intangibles as contributing to mental health of the occupants. Intangible features mentioned:
supporting dignity
quality of light
the views and connectedness to outside.
social dignity and socialising
a sense of comfort
Only three of the projects clearly included an element of delight.
As a result of the audit and our previous work, we identified there was a need to develop a common language to identify the intangible features. In addition, we aimed to include the intangibles into all housing experimentation to improve wellbeing for occupants’ with ICF.
It was proposed that local accommodation, controlled by the provider, would be audited to gain an in-depth knowledge of the physical environment of the accommodation. Eight single homes plus one group home for 12 people were audited (Table 10). This involved mapping the current design attributes, identifying those attributes that target the therapeutic needs identified in the literature, and ascertaining the tangible and intangible qualities of homes (Table 10).
Activity: Visit, record and analyse the physical attributes of the provider’s homes. Generated: Four general principles were identified.
Reflection As the physical settings were fully recorded, the qualities of the spaces could be analysed for such intangible qualities as location, orientation, lighting and noise. However, the occupants were not interviewed. Personal items used by the occupant were only considered if indicating adequate storage or adequate space for typical furniture layouts and the like. The four general principles were based on the identified design elements or environmental attributes, which can influence the level of sensory overload and/or social participation. Limitations of accommodation included size and layouts, access and external areas in relation to climate, as well as quality of building services.
It was evident from the accommodation audit that the potential of services (lighting, air temperature, air quality) and technologies for improving quality of life for people with ICF needed to be updated considering currently available technology. The sector was contacted to ascertain if they considered there was a need to adopt alternative housing designs to improve the residents’ wellbeing (Table 11).
Activity: A telephone and email survey of local providers. Generated: Little useable information was available.
Reflection There was lack of clarity in 2015 regarding the need for change across the sector; although it was noted that accommodation was not being tailored to particular people with special needs. Principles of Universal Design are integrated; yet distinctions between people with cognitive and physical disabilities were not made. Some organisations have their own guidelines for general adaptable designs; and although not available, the National Disability Insurance Agency was thought to be developing their own guidelines at the time.
Table 11.
Needs analysis.
The lack of clarity across the sector means that the likely adoption of this research by the sector needs monitoring. That will increase the likelihood of uptake and environmental improvements. To encourage adoption, a comprehensive tool to assist designers and providers was proposed (Table 12). The researchers’ aim was to develop a tool to assist designers and providers to generate supportive environments for those with ICF.
Activity: Generation of a tool based on what is known to date. Generated: A Matrix consisting of: Indicators of a Supportive Environment axis and Design Directives axis.
Reflection Lesson learned: Home (building and interior) and setting (garden) have the potential to impact on an occupant with reduced cognitive functioning by: 1. providing a setting, which affords certain ways of perceiving, using and experiencing it. 2. the qualities of the physical setting can induce a sense of coherence. 3. a sense-of-wellbeing can be fostered. The intersection of a person’s CI with indicators for supportive environments is proposed as a point to start to improve residential environments.
The resultant Matrix was a forerunner to resident interviews to enable an in-depth understanding of the PER relationship, as well as informing the refinement of the Matrix. Research was proposed to understand the relationship between a particular condition and the physical environment and to build on what was already known about such relationships (Table 13). A list of considerations to increase the environmental affordance toward a supportive environment for those with ICF unfolded.
Activity: Interview three residents who live in accommodation that was previously audited. Generated: A set of considerations to inform the development of a design tool for designers and providers.
Reflection Some understandings were challenged or extended by interviews. Observations and telling of first-hand experiences were critical to understanding the opportunities and limitations of current homes and future strategies.
Table 13.
Interviews with residents who have schizophrenia.
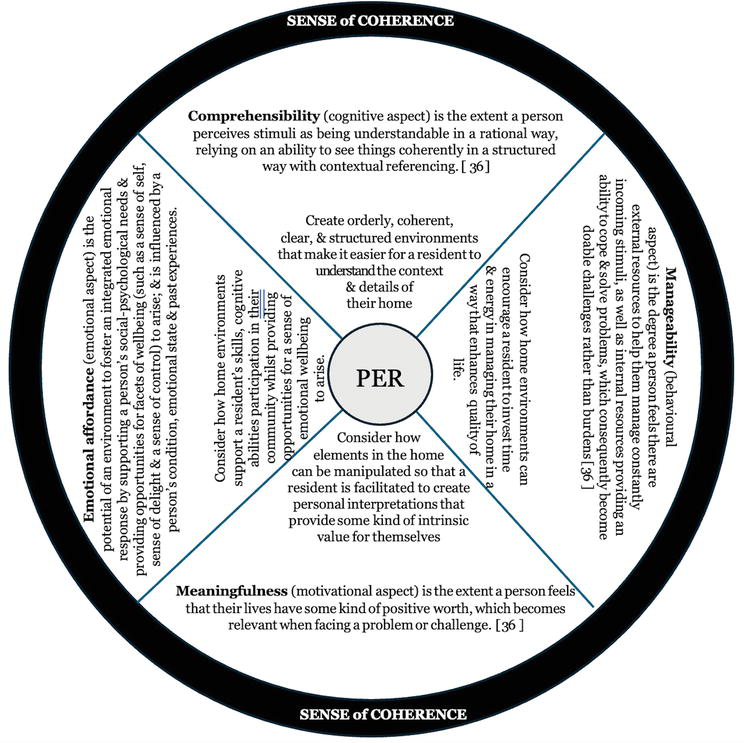
Our initial understandings developed by listening to the first-hand experiences of people with schizophrenia. Further research showed that the intangible qualities of design and their impact on a person with ICF can be examined by assessing if a person with ICF is better able to cope with activities of daily living when they are able to comprehend, manage and find meaningfulness in their home. Collectively these three aspects of support are referred to as enabling a sense of coherence [36, 37]. Our research and reflections identified an additional aspect of the PER, the emotional aspect. This relates to a person feeling that their abilities are accepted, they are supported to participate in their community and can get involved. We refer to this as emotional affordance: a concept that complements the work of others [20, 25]. Collectively these four aspects of support in this chapter are referred to as enabling a sense of coherence (SoC). Although the person-environment relationship is complex as discussed previously, in our work were able to relate the four aspects of SoC to some foregrounded designing qualities as shown in Figure 2.
Figure 2.
Aspects of SoC related to PER.
It became clear that SoC needed to be integrated into the tools being developed. This led to a more refined Matrix (Table 14).
Activity: Refine the Matrix based on what is known to date including principles of Salutogenic Design [36] Generated: A tool providing a practical way of enhancing the design of a physical home environment to help reduce negative impacts and increase supportive qualities.
Reflection The homes of the interviewees achieved differing degrees of SoC. They catered for daily requirements, interaction/ socialisation, non-sedentary activities within common forms of accommodation and were comprehensible. The overall SoC should include what is emotionally afforded through the PER. This adds another dimension to developing a design model. This dimension aligns with the previously generated Facets of Wellbeing. Overall the development of a new multidimensional tool to embrace the complex and competing demands of provider, designer, and resident is required while not sacrificing the non-functional for the functional.
To further refine the proposed strategy (and resultant tools) that was emerging, further research was required across various aspects including more interviews and observations that involved people with schizophrenia. In particular, areas requiring additional study included links between meaningfulness and environmental contexts; fine-grain understanding and links between specific environmental elements and the four dimensions of SoC. The theoretical basis reflecting these developments was also integrated. These realisations brought the project to a point where clear principles needed to be communicated to enable design practitioners to embrace the findings to inform their approach to designing accommodation for people with schizophrenia.
3.2.2 Refinement of outcomes
There were three cycles of research in the Outcomes and Refinement Phase. All related to creating an easily accessible way for designers, architects and service and accommodation providers to understand the impact of the home environment on their clients with ICF. Initially, we produced a generic Framework through which to tackle the design of accommodation for those with ICF. The generic Framework evolved to explicitly address the requirements of accommodation for people with schizophrenia. Schizophrenia was addressed rather than another condition of ICF for the following reasons. Our literature review indicated an initial depth of knowledge that we could build on. The provider of services and accommodation who initially approached us, advised that a large percentage of the clients presenting to them were people with schizophrenia and we had been able to interview some of them. In addition, we were able to procure further interviews with people with schizophrenia through another service provider.
Having contextualised the parameters that influence design practice such as the user (resident) and the condition (such as schizophrenia), we aimed to reflect upon the development of the Framework and test its application. The final DEKS Practice Document [38], which includes the Framework, contextualises the users’ condition (schizophrenia). The Practice Document enables a reader to move from understanding the reasons why a person with ICF may respond to the environment in particular ways to examine the design aspects to be considered to positively influence the wellbeing of a person with ICF. Details of the Framework are described in detail below.
The Framework suggests incorporating specific design features in an environment so that the wellbeing of a person with schizophrenia can be impacted positively (and avoid negative impacts). This section summarises critical aspects of the Framework, describes two applications which continued our action research approach and analyses the educative value of the process as well as the challenges in applying the Framework in practice.
4.1 The framework
The overall intent of the Framework is to enable a practitioner to appreciate the reason why a person with ICF may respond to the environment in particular ways and to examine design aspects that impact on SoC to positively influence wellbeing. The Framework itself consists of 3 parts: Guiding Parameters, Design Considerations and Potential Overall Impact on Wellbeing. The Guiding Parameters include two sets of principles. The first principle provides explicit descriptions of symptoms of a specific condition that may influence how a person responds to the environment. The second principle identifies in sweeping terms what is needed to create a positive supportive physical environment. One that creates a sense of coherence and thus can be responsive to the needs of a resident. The second part of the Framework essentially provides the designing cues. The Design Considerations establish how each of the four aspects of SoC can be met to help a person better cope with everyday living. The Design Considerations include general design instructions and detailed design strategies to explain the environmental requirements necessary to facilitate an integrated approach to accommodation design. The final part of the Framework describes the potential overall impact on wellbeing resulting from addressing the Design Considerations. Table 15 summarises the generic Framework.
Guiding parameters
Design considerations
Potential overall impact on well-being
ICF Principles
Designing Principles
Design Intentions
Design Provisions
A designer is required to understand: ICF may include ‘an ongoing impairment in comprehension, reason, adaptive functioning, judgement, learning or memory’ [39]. The symptoms a person may exhibit when they have a particular condition of ICF.
Establish how the four SoC dimensions (cognitive, behavioural, motivational and emotional affordance) can be fostered in the home for a person’s particular condition.
Provide instructions for a designer to enable them to address each dimension of SoC for the target group.
Establish a series of design strategies that contribute to fulfilling the Design Intentions
Establish expected beneficial experiences for the home occupant.
Table 15.
The generic framework.
The generic Framework was populated to address the needs of people with schizophrenia. This resulted in a total of 12 general Design Intentions and 25 detailed Design Provisions. Table 16 shows the first part of the Framework relating to providing the cognitive aspect of support to contribute to a SoC.
Designing Principles
Design Intentions
Design Provisions
Potential overall impact on wellbeing
COMPREHENSION Create orderly, coherent, clear, and structured environments that make it easier for a resident to understand the context and details of their home.
A. Create an uncomplicated comprehensible home environment for activities of daily living; B. Reduce likelihood of negative perceptions of ordinary spaces or amplifications of perceptions of non-existing dangers.
Simple (uncomplicated) orderly design solutions;
Home layout that provides intuitive way-finding based on recognisable spatial clues and focal points;
Clear sight lines and straightforward entry points;
*Increase a resident’s ability to function and perform activities of daily living; *Reduce anxiety levels; *Assist replenishment of cognitive energy; *Reduce depression; *Reduce feelings of helplessness; *Reduce mental load on functioning;
Table 16.
Part of framework related to supporting comprehension for people with schizophrenia.
4.2 Applying the framework
We utilised the Framework on two test projects. The first project was a virtual redesign of a home occupied by a person with schizophrenia and the second was to review design development drawings for a new home where one of the occupants has schizophrenia.
4.2.1 Virtual redesign with resident feedback
One of the volunteers, who had participated in the interviews as we were refining the Framework (Section 3.2.2), agreed that we could redesign his home using it. He was prepared to comment on the result. This person had lived in his accommodation for 25 years and was an avid collector of books, records and CDs. Three designer-researchers independently set about redesigning the existing 62 square metres two-bedroom home for him, within practical limits, using all 25 of the Design Provisions incorporated in the Framework. The three designer-researchers came together to assess their design proposals and, after reviewing and discussing the proposals, agreed on a final design that best met the Design Intentions and Design Provisions. A document was prepared to record the designer-researcher’s commentary on how each of the Design Provisions had been met in the final design. It is acknowledged that some of the Design Provisions could not be fully achieved due to the inherent nature of the building; the home is within a complex of home units, so orientation of windows is predetermined. However, most of the Design Provisions could be met.
The final design was digitised into a three-minute video that enabled a viewer to move virtually through the home [40]. Figure 3 shows a view of the living space. The indicative sketch of the original space is on the left, while a screen save from the video is on the right.
Figure 3.
Abstracted existing living space (left); screen save of living space from the video (right).
The occupant viewed the video with the three designer-researchers. His comments are discussed below. The occupant said he liked the proposal saying:
I love it. I mean it’s really clever use of space… There are some aspects of it that are really good.
However, he had some general reservations saying:
A person with schizophrenia might find it a little bit too organised… A lot of people I hang around with are generally disorganised in how they live… have stuff everywhere.
Another reservation related to how light the space looked. Although he seemed to appreciate the additional light he said:
the space, the light… it’s a lot lighter… I’d feel kind of exposed or vulnerable in such a light, bright environment. I’d have to get used to it. I might have chosen, with the colour of the storage, something slightly darker. Even the dining room table…because I’m so used to this place… A dark environment for me makes me kind of feel more cosy… I would not kind of feel as exposed or vulnerable as in such a light, bright environment.
It is not uncommon for people to express trepidation to a change in a familiar setting and imagining their possessions set in unfamiliar surroundings. Foremost in a person’s mind are associations with memories of the current or previous home [41] and the emotional relationship they have with the familiar environment they call home [14].
The comment relating to a darker environment feeling more cosy may be about nostalgia or could be about hiding/not wanting to be seen/being suspicious of the outside world/feeling secluded when feeling unwell. In our interviews with numerous people with schizophrenia, a number talked about choosing to live in darker environments and keeping curtains and blinds drawn during the day.
Therefore, in order to enable the resident to control their environment during the day as their emotions and requirements shifted, strategies needed to be integrated. In the redesign, curtains or blinds were provided on all glazing. Also, dimmer switches were proposed on living area lights. However, on reflection, a darker finish on the storage units may have made for a more mellow environment. The Designing Principles of coherence and manageability are both at play here.
In talking about storage units, that are integral to the Designing Principles of comprehension, manageability and meaningfulness for this person with his collections of books, compact discs and records, he said:
I would use it, but I do not know if somebody else would…I’m not talking about everyone with a mental illness, I’m talking about people I know… And how they kind of, they have storage but they do not use it… So it depends how organised their thinking is – or obsessive – and how they do things when they are actually using what they have got in their flat… Not just using the storage but using what they have collected.
In our conversations with people with schizophrenia, appropriate storage was raised as a means of decreasing anxiety and agitation. One person talked about the calming effect of being able to put away kitchen condiments in a shallow cupboard that enabled her to see the contents at a glance. Another person in rental accommodation with no doors on her wardrobe talked about how upsetting this was whilst a third person, who liked to paint had to go to great lengths to arrange his home so that he could store his paintings.
Another of the reservations expressed related to the notion of ‘discriminatory practices’ where society projects onto a person with schizophrenia certain expectations. In addition, the resident has an embodied construct about their place in society (and what built forms are appropriate for a person complying with that construct). The ‘habitus’ is reflected in the transcript below; that is, they are not worthy of living in a carefully designed home. This relates to one of the Designing Principles identified in our Framework, emotional affordance. The occupant said:
I’d have a bit of trouble living in this space that was a little bit - too designed… so I’m kind of living in this space but I’m feeling I’d be living beyond my means in a sense… and also I’d be a bit worried about spoiling it.
In conclusion, in talking about the appropriateness of the redesign for others with schizophrenia, the interviewee said:
I can see they would like the design… how useful it would be to them I do not know – they would be impressed as a place they’d like to live – but whether they would actually use it the way it’s designed – maybe – maybe not… the problem with schizophrenia is that some of the negative symptoms are that kind of lack of living skills - lack of motivation – general apathy and things like that… So people like that cannot really get it together to do something in their own space…. Their minds are elsewhere.
Statements such as these complement others made in our earlier user interviews. They challenge designers to reconceptualise what is required and how to resolve the issues. Spaces and furniture may have to be rethought and move beyond the taken-for-granted resolutions to address the issues at hand that surround, for example, storage. The intangible needs as well as the pragmatic requirements need to be integrated purposefully.
4.2.2 Review design development drawings
A local designer, with a large client base, was working with a client where one senior member of the family had schizophrenia (referred to as H in this chapter). The designer agreed to apply the Framework to his design and have it evaluated by the researchers. To this end the designer and his team were briefed on the Practice Document and were given the document to study. During the briefing, the researchers used a number of the designer’s previous projects to demonstrate how the Framework could have been incorporated. The designer prepared a preliminary design of a 2-storey house based on his client’s brief and on his understanding of the Framework.
Two designer-researchers independently evaluated that preliminary design in relation to the brief, the family needs, the needs of the family member having schizophrenia and the four Designing Principles of comprehension, manageability, meaningfulness and emotional affordance. They both identified similar inadequacies but came up with different design suggestions to better address the Designing Principles. Major limitations revolved around confusing circulation spaces and contorted access to H’s room, poor sight lines to major spaces and lack of daylight in critical circulation areas. These design limitations could impact on H’s wellbeing by decreasing her ability to function, increase agitation and anxiety, disturb circadian rhythms, create high demand on cognitive energy and suppress her identity.
The researchers advised the designer of the limitations identified. The designer recognised that the design had some limitations and agreed to try to integrate some of the points raised by the researchers. However, from the point of view of a wholehearted commitment to working toward achieving the Design Provisions in the Framework, Bourdieu’s concept habitus may be implicated. The designer’s ‘sense of the game’ or unspoken rules may be overriding the opportunity to delve into the issues from different perspectives. The pragmatics of a speedy and cost effective design was the designer’s mode of practice. With the agreement of the designer, the researchers attempted to meet independently with the client to better understand the needs of H. This did not eventuate so this review project was terminated.
Questions regarding some common myths about designing for people with ICF were raised. These myths include that:
designing for people with ICF is essentially about universal design and functionality,
architecture is of minor value to improving a residents’ quality of life and wellbeing,
ICF is irrelevant if a ‘humanistic’ approach to design is adopted (i.e. generic ‘good design’ will always encompass attributes to cater for the needs of people with ICF).
Further reflection on our work with the designer highlighted another consideration when using the Framework to evaluate a design. As the evaluation is confined to addressing the 12 Design Intentions which are all connected with creating a sense of coherence, no other aspects of ‘good design’ are addressed. The assumption is that the 12 Design Intentions will be used to enhance a ‘good design’.2 If a design does not have the qualities of ‘good design’ (and it is recognised that this is a contestable space) will the application of our Framework still be able to create a sense of coherence for the occupant of the home? By raising this question we are also implying that good design is a deep understanding known and practiced by all of those associated with the design disciplines, including architecture. Through enculturation and experience accepted ways of practicing and who belongs due to their social capital – and in this case architectural cultural capital—determine or map ‘the field’. Therefore, assessing good design when creating environments for positive support and wellbeing raises further issues for discussion.
As stated throughout this chapter, the Framework is a tool to assist designers and providers to create informed accommodation designs to support those with schizophrenia. The underlying principles acknowledge (in keeping with salutogenic design) [37] that having a sense of coherence enables a person to adapt to a situation and lead a desirable lifestyle for themself. The environment potentially reflects who the resident is in the eyes of others as well as to the individual themselves. It supports the functional requirements and has the potential to also do so for the emotional requirements.
As people do live somewhere, ignoring the physical environment assumes that its role is minimal or insignificant. However, it is well documented that an environment can facilitate functional needs, influence the atmosphere, construct a person’s identity, influence judgements made about the resident and add to or reduce the level of stigmatisation. Everyday examples indicate how environmental qualities can influence actions and behaviours; lighting levels, glare levels, temperatures, noise levels, or boundary design can add to insecurities, agitation, anxiety, and the like.
When designing we have proposed that designers and providers need to commence by understanding any conditions that a person from the target-resident group are likely to have, and how it will influence their experience of their day-to-day life at home. And how in turn the environment may play a role, impacting on their quality of life. In summary: Schizophrenia is a condition that some people acquire/have. When designing for such people it is important to consider not only the functional aspects of home, but also how they experience their world emotionally, socially and culturally as well through the PER.
Designers need to be reflective practitioners [43]. Firstly, by being aware that if the person is defined only in terms of their condition, then the functional aspects will dominate the thinking and the outcomes. Also, by being aware that cultural hegemonies infiltrate what people generally believe, everyday myths can be assessed; for example, the proposition that a person with schizophrenia is typically dangerous or violent. Such assumptions influence how the person is integrated into the community, neighbourhood, street, or housing complex—and environmental design is an important component of these situations.
Secondly, as a designer (or provider), it is imperative that they become aware of the assumptions of what the accommodation should be like and what the target-resident will be like. The design process allows the designer to offer innovation through exploration. The innovation will be influenced by the limits of possibilities we set, without reflecting upon where the boundary-construct has come from. In this case, how the collective body of professionals and society conceptualise people with schizophrenia, generates the tacit beliefs that underpin the accommodation typology and its resolution.
With the increasing numbers of people with ICF in our societies across the world it seems timely to look at design and how we assist marginalised groups through our practices. We seek to invite designers and providers to reconsider their practices. At the core of this is the person environment relationship; particularly where the person is part of an interdependent relationship as one defines and influences the other; or in the extreme case where the relationship is no longer noticed. This is where ones habitus may reside [7]. The environment is not just objectified or a removed entity, rather it can be much more integral to a person’s being and lifestyle.
Therefore, by designers joining this multidisciplinary ‘field’, maybe more existing players will develop a greater awareness of the relationship between home and the wellbeing of people with ICF. Perhaps preconceptions of the sort of homes that people with schizophrenia (or other conditions relating to impeded cognitive functioning) deserve can be reconsidered.
Will the Framework be useful? We envisage that this tool will continually evolve. Firstly, as medical knowledge concerning ICF evolves, so will the knowledge of the condition and the impacts identified. Secondly, as building and digital technologies change, likewise opportunities for sensitive designs will evolve. And thirdly, sociological theories and new understandings of practice may also inform and challenge concepts such as disabilities and mental health. Consequently, the taken-for-granted beliefs and practices may be thrown into relief. Importantly, we established that design-based interventions, for people with cognitive impairment, in domestic situations are low risk and potentially high benefit. The Framework, therefore, has the potential to remain relevant to designers and providers. This comment supports our premise that design considerations can only ever be part of a comprehensive package of support for people with schizophrenia.
We envisage that the process embedded in the Practice Document, including the Framework, will be tested further through its application to constructed projects (houses, units). Testing is complex due to the length of time and cost of construction, the multitude of procurement variables involved and the mix of experiential qualitative aspects with functional and measurable attributes therein. Through assessing the experiences of people living in those homes, the Framework can potentially become more sensitive to the target-resident requirements. Both their daily experiences and the resultant impacts need to be ascertained rather than focusing purely on the pragmatic and functional dimensions. Once again, gauging shifts in peoples’ experiences of place and their wellbeing suggest the benefits in marrying disciplines. With all players on the field, opportunities for new understandings at the disciplinary boundaries arise.
We acknowledge the assistance of two service providers, Rise and Neami National, including their role in enabling us to contact interviewees who have schizophrenia. We also acknowledge Gaia Sebastiani for her informed input into several of the projects.
References
1.Swartz D. Culture and Power: The Sociology of Pierre Bourdieu. Chicago: University of Chicago Press; 1997
2.Owen C, Lorrimar-Shanks J. Framing the field: The award for sustainable architecture. Art. 2015;4(2):34-48. DOI: 10.3390/arts4020034
3.Bourdieu P, Wacquant L. An Invitation to Reflexive Sociology. London: University of Chicago Press; 1992
4.Miller D, Branson J. Pierre Bourdieu: Culture and Praxis. In: Austin-Broos D, editor. Creating Culture: Profiles in the Study of Culture. Sydney, NSW: Allen and Unwin; 1987. pp. 210-225
5.Minami H, Tanaka K. Social and environmental psychology: Transaction between physical space and group-dynamic processes. Environment and Behavior. 1995;27(1):43-55
6.Potter FM. Constructing Trust in Acute Inpatient Mental Healthcare Facilities: The Role of Physical, Social and Symbolic Environments of Care in Supporting Therapeutic Safety [Thesis]. Sydney: UTS; 2017
7.Smith D. Architectural Experience: A Composition of Viewpoints [Thesis]. Brisbane: Queensland University of Technology; 2000
8.Malone P. Bourdieu in London. The Journal of Architecture. 2020;25(6):679-696. DOI: 10.1080/13602365.2020.1800792
9.Matthewson G, Stead N, Burns K. Women and leadership in the Australian architecture profession: Prelude to a research project. In: Seizing the Initiative: Australian Women Leaders in Politics, Workplaces and Communities. Melbourne: eScholarship Research Centre, The University of Melbourne; 2012. p. 10
10.Australian Bureau of Statistics. Housing Circumstances of People Using Mental Health Services and Prescription Medications [Internet]. Canberra: ABS; 2011 . Available from: https://www.abs.gov.au/statistics/health/mental-health/housing-circumstances-people-using-mental-health-services-and-prescription-medications/latest-release [Accessed: February 1, 2024].
11.Tehve K, Furgiuele A. Taste and the modern interior, a seminar. In: Proceed-ings of Interior Design Educators Council; 24–27 March 2010. Atlanta, GA: IDEC; 2010. p. 584
12.Pallasmaa J. The Eyes of the Skin: Architecture and the Senses. New York: John Wiley; 2005
13.Ioannidou E. Home no. 7 (a sample of). Interiors. 2021;11(1):1-16. DOI: 10.1080/20419112.2020.1836804
14.Gibson J. The Ecological Approach to Visual Perception. Boston, MA: Houghton Mifflin; 1979
15.Gifford R. Environmental Psychology: Principles and Practice. Colville, WA: Optimal Books; 2002
16.Bechtel R, Churchman A, editors. Handbook of Environmental Psychology. New York: Wiley; 2002
17.Karol E, Smith D. Impact of design on emotional, psychological, or social well-being for people with cognitive impairment. Health Environments Research & Design Journal. 2019;12(3):220-232
18.Chrysikou E. Why we need new architectural and design paradigms to meet the needs of vulnerable people. Palgrave Communications. 2018;4(1):6. DOI: 10.1057/s41599-018-0171-z
19.Erwine B. Creating Sensory Spaces: The Architecture of the Invisible. New York, NY: Routledge; 2017
20.Golembiewski J. The designed environment and how it affects the brain. Health Environments Research & Design Journal. 2016;9(2):161-171. DOI: 10.1177/1937586715609562
21.Rivlin L, Moore J. Home-making: Supports and barriers to the process of home. Journal of Social Distress and the Homeless. 2001;10(4):323-336
22.Diener E, Chan M. Happy people live longer: Subjective well-being contributes to health and longevity. Applied Psychology Health Well-Being. 2011;3(1):1-43
23.Lyons G. Quality of life for persons with intellectual disabilities: A review of the literature. In: Kober R, editor. Enhancing the Quality of Life of People with Intellectual Disabilities: From Theory to Practice. Dordrecht: Springer; 2011. pp. 73-126
24.Saruwono M. Shouting in silence: Expression of self in private homes. Procedia. Social and Behavioral Sciences. 2012;42:34-41
25.Lockard E. Human Migration to Space: Alternative Technological Approaches for Long-Term Adaptation to Extraterrestrial Environments. New York: Springer eBooks; 2014. p. 2014
26.Hudson K. Salutogenesis: The origin of health. Nursing Management. 2013;44(11):12-30. DOI: 10.1097/01.NUMA.0000436369.45139.81
27.Breakwell G, Hammond S, Fife-Schaw C, Smith J. Research Methods in Psychology. 3rd ed. London: Sage Publications; 2006. p. 311
28.McTaggart R. Is validity really an issue for participatory action research. Studies in Cultures, Organizations & Societies. 2005;4(2):10245286
29.Hart E, Bond M. Action Research for Health and Social Care: A Guide to Practice. Buckingham: Open University Press; 1995. ISBN 0 335 19262 9
30.Karol E, Smith D. Using creative practice to re-conceptualize provision of services in intractable situations. The International Journal of Design in Society. 2015;8(3/4):15-25. DOI: 10.18848/2325-1328/CGP/v08i3-4/38567
31.Smith D, Karol E. Improving chances? A design strategy to improve health and wellbeing for marginalised people. Australasian Medical Journal. 2017;10(6):478-488. DOI: 10.21767/AMJ.2017.2993
32.Karol E, Smith D. Impact of design on emotional, psychological, or social well-being for people with cognitive impairment. HERD: Health Environments Research & Design Journal. 2018;12(3):220-232. Advanced online publication. DOI: 10.1177/1937586718813194
33.Smith D, Karol E. Beyond the Tangible [Internet]. 2017. Available from: https://beyondtangible.wixsite.com/beyondtangibledesign [Accessed: January 30, 2024]
34.Karol E, Smith D. Expanding design approaches to create supportive home environments for people with impeded cognitive functioning. Design for Health. 2020;4(1):43-62. DOI: 10.1080/24735132.2020.1732730
35.Smith D, Karol E. An accommodation design matrix to assist the provision of supportive accommodation for people with altered cognitive functioning. Design for Health. 2019;3(2):261-282. DOI: 10.1080/24735132.2019.1641398
36.Riopel L. What does it mean to have a sense of coherence? (+ Scale) [Internet]. 2020. Available from: https://positivepsychology.com/sense-of-coherence-scale/ [Accessed: February 21, 2024]
37.Dilani A. Psychosocially supportive design: A salutogenic approach to the design of the physical environment. Design and Health Scientific Review. 2008;1(2):47-55
38.Karol E, Smith D. Beyond the Tangible-DEKS Practice Document [Internet]. 2017. Available from: https://beyondtangible.wixsite.com/beyondtangibledesign [Accessed: January 30, 2024]
39.NSW Law Reform Commission. People with Cognitive and Mental Health Impairments in the Criminal Justice System – Diversion. Sydney, Australia: NSW Law Reform Commission. Report No. 135 June 2012. 2012. Available from: https://lawreform. nsw.gov.au/documents/Publications/Reports/Report-135.pdf [Accessed: February 21, 2024]
40.Smith D, Karol E. Beyond the Tangible-Testing the Framework: Virtual redesign [Internet]. 2024. Available from: https://beyondtangible.wixsite.com/beyondtangibledesign. [Accessed: January 30, 2024]
41.Rybczynski W. Home: Á Short History of an Idea. New York: Penguin Books; 1987
42.Vitruvius M. The 10 Books of Architecture. New York: Dover Publications; 1960
43.Schon D. The Reflective Practitioner: How Professionals Think in Action. New York: Basic Books; 1983
Notes
Throughout the chapter various terms and acronyms are used to describe these people’s condition. They include cognitive impairment (CI), impeded cognitive functioning (ICF), impaired cognitive functioning and impaired cognitive abilities. The reason is that over the past couple of decades terminology describing conditions (or the collection of people experiencing the condition) has evolved. As this chapter captures a series of projects that occurred over time, the terms of the day are used here as well as in the reporting of the published outcomes.
In the only treatise on architecture to survive from antiquity, De Architectura, the Roman architect and engineer, Vitruvius, defined three characteristics of good design. They are:Durability–It should stand up robustly and remain in good conditionUtility–It should be useful and function well for the people using itBeauty–It should delight people and raise their spirits [42].
Written By
Dianne Smith and Elizabeth Karol
Submitted: 21 February 2024Reviewed: 23 February 2024Published: 25 March 2024