
Abstract
Perioperative preparation for emergency patients is paramount, as it entails a comprehensive approach to ensure the safety, well-being, and successful outcomes of individuals facing urgent surgical interventions. In the preoperative phase, rapid but essential steps are taken, such as assessing the patient’s medical history, conducting diagnostic tests, and stabilising their condition to minimise risks during surgery. So in this chapter, we will discuss the importance of formation of the multidisciplinary team, efficiency improvements, identifying the need for emergency department (ED) to operating room (OR) Handoff Standardisation, and integration of ED nurses into the OR. It begins by establishing the criteria for identifying patients needing urgent surgery, encompassing traumatic injuries and acute medical conditions. It extensively covers the interdisciplinary collaboration required among ED staff, OR teams, anaesthesiologists, surgeons, and nurses. The scope includes patient assessment and stabilisation procedures conducted in the ED, focusing on diagnostics, interventions, and life-saving measures. Furthermore, the chapter delves into handoff protocols and communication strategies, highlighting their crucial role in ensuring safe and efficient patient transfers. It addresses resource allocation, emphasising the optimisation of operating rooms, equipment, and personnel. The chapter also acknowledges the importance of patient and family engagement, stressing clear communication, informed consent, and emotional support.
Keywords
- perioperative preparation
- emergency patients
- emergency room
- operating room
- emergency department
1. Introduction
1.1 Perioperative care
Perioperative care, as defined in the discussion, is a comprehensive system of medical strategies to ensure patient well-being throughout the surgical journey [1]. It comprises three essential phases: preoperative, intraoperative, and postoperative care. In the preoperative phase, healthcare professionals meticulously prepare patients for surgery through assessments such as blood tests, scans, and psychological counselling, ensuring they are physically and mentally ready for the procedure. During the volatile intraoperative phase, nurses and anaesthesiologists monitor vital signs, maintain a sterile environment, and prioritise safety in the operating room. Postoperative care focuses on patient recovery, including pain management, wound care, and monitoring progress in the Post Anaesthesia Care Unit (PACU) [2]. Comprehensive perioperative care is vital as it not only enhances the patient experience by alleviating stress but also contributes to better health outcomes, enabling patients to return to normal life faster and reducing healthcare costs per capita. Integrating digital health solutions, such as the Buddy Care Platform, further streamlines and enhances perioperative care by facilitating remote monitoring, patient engagement, and data collection, ultimately making healthcare more accessible and patient-centred [2]. Essentially, perioperative care encompasses a holistic approach to surgical patients’ well-being, from preparation to recovery, focusing on safety, comfort, and efficient healthcare delivery.
1.2 Importance of perioperative preparation for emergency patients
Perioperative preparation for emergency patients is paramount, as it entails a comprehensive approach to ensure the safety, well-being, and successful outcomes of individuals facing urgent surgical interventions. In these critical moments, when time is of the essence, the significance of perioperative care pathways becomes evident. These preoperative, intraoperative, and postoperative phases offer a structured framework for healthcare professionals to navigate the complexities of emergency surgeries. In the preoperative phase, rapid but essential steps are taken, such as assessing the patient’s medical history, conducting diagnostic tests, and stabilising their condition to minimise risks during surgery. The surgical team takes centre stage in the intraoperative stage, meticulously monitoring vital signs, maintaining sterile conditions, and responding swiftly to unforeseen challenges that may arise, especially in emergencies involving life-threatening conditions such as trauma or ruptured organs. While shorter in emergency cases, postoperative care is equally critical, involving continuous monitoring, pain management, and vigilance against complications, ensuring a smooth recovery process.
Beyond the immediate medical aspects, perioperative care pathways also prioritise the patient experience, recognising emergency situations’ emotional and psychological tolls. Compassionate and comprehensive care reduces patient anxiety and enhances their satisfaction with the healthcare system. Moreover, efficient perioperative care pathways contribute to cost-effectiveness by optimising resource allocation, minimising hospital stays, and preventing complications. With the rising demand for surgical interventions, particularly in emergencies, these pathways help healthcare systems meet the challenges of an evolving healthcare landscape. Central to perioperative care is collaboration among healthcare professionals, including surgeons, anaesthesiologists, nurses, and specialists, fostering an interdisciplinary approach that enhances patient safety and care quality. In essence, perioperative preparation for emergency patients is a holistic endeavour, ensuring that individuals receive the best possible care during critical junctures in their healthcare journey, where timely, effective, and compassionate care can make all the difference in their outcomes and overall well-being (Figure 1).
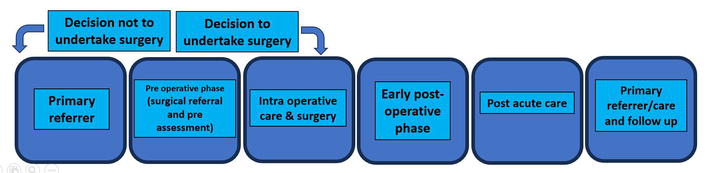
Figure 1.
Perioperative care journey. Source [
1.3 Overview of the transition from the emergency department (ED) to the operating room (OR)
According to Atzema and Maclagan [3], the transition from the emergency department (ED) to the operating room (OR) involves a standardised handoff process that was developed by a multidisciplinary team to improve patient care and efficiency. This process was motivated by the success of similar handoff processes in other departments, such as from the OR to PICU and NICU to the OR. Here is an overview of the transition from the ED to the OR:
1.3.1 Formation of the multidisciplinary team
The journey to standardise the transition from the emergency department (ED) to the operating room (OR) began with the formation of a multidisciplinary team. An adverse event did not prompt this initiative but rather the success of standardising handoff processes in other hospital departments [3]. The team comprised frontline staff from various departments, including Respiratory Therapy, ICU Nursing, OR Nursing, Anaesthesiology, and Paediatric Intensivists. The motivation behind this collaboration was to establish a more structured and intentional transition of care for patients moving from the ED to the OR.
The team did not anticipate the level of efficiency the new handoff process would bring. Anaesthesiology teams could transport patients to the Paediatric Intensive Care Unit (PICU) significantly faster than before. This initiative also encouraged staff to ask more pertinent questions during handoffs and created an environment where parents could observe the process without hesitation. These initial successes fuelled the team’s determination to continue improving the handoff process. Also, it is crucial to include the emergency drugs in “Critical Medication Bag” including basic ACLS medicines for all critical patient transports for the management of any emergency scenarios.
1.3.2 Efficiency improvements
One of the remarkable outcomes of the new handoff process was the substantial improvement in efficiency. For example, the Anaesthesiology teams saw a 25% reduction in the time it took to transfer patients to the PICU. Similarly, in the Neonatal Intensive Care Unit (NICU), report times decreased from an average of 16 minutes to just 6 minutes, even when including the transfer of the baby from the cart to the bed [3]. These improvements directly resulted from enhanced communication and a more streamlined handoff process that became integral to daily healthcare routines.
The success of this transition process was built on the idea that when all stakeholders in patient care are involved in the process improvement efforts, the results can be exceptional. The team’s collaboration involved six different departments and seven distinct roles, emphasising the importance of each component in delivering efficient and safe patient care. As the handoff process continued to evolve and improve, ongoing engagement with staff from the Emergency Department, OR, and Anaesthesiology was crucial to maintaining these positive outcomes. The experience revealed that the best solutions often emerge when those directly involved in patient care come together, making the standardisation of the ED-to-OR handoff a prime example of healthcare improvement [4].
1.3.3 Identifying the need for ED to OR handoff standardisation
While standardisation of handoff processes existed in various healthcare settings, the transition of patients from the emergency department (ED) to the operating room (OR) had yet to be thoroughly addressed [4]. This was a critical gap in patient care, especially for Class A surgeries that required swift and efficient transfers. The relationship between the ED and the OR was often strained due to the urgency of these cases, which further underscored the need for a standardised process.
1.3.4 Identifying key roles
While developing the standardised handoff, the team recognised that the ED nurse often possessed the most comprehensive information about the patient, including vital situational awareness. This information was highly relevant to Anaesthesiology and OR Nursing, as it impacted their ability to provide timely and appropriate care to the patient [4]. Realising that the ED nurse played a pivotal role in the handoff process was a crucial insight that guided the subsequent improvements.
1.3.5 Integration of ED nurses into the OR
The team decided that the ED nurse and the Surgical Resident would accompany the patient directly to the assigned OR room to facilitate a seamless handoff process, especially in emergencies. This proactive approach ensured the ED nurse could provide essential information and context during the handoff. It was a practical solution that eliminated ambiguity about whether ED nurses were welcome in the OR, a concern that had previously hindered efficient handoffs. Additionally, the minimal requirement for the ED nurse to don a surgical mask and hat streamlined the transition further.
1.3.6 Importance of full attention during handoff
Recognising the importance of focused attention during the handoff, the team scripted specific steps to ensure effective communication. The Surgical Resident would announce critical patient details and procedures upon entering the OR room. Anaesthesiology would call for a moment of quiet, and the ED nurse would deliver a report tailored to the severity of the patient’s condition. This scripting provided clarity and emphasised the need for everyone involved to actively engage and concentrate on the handoff.
1.3.7 Continued collaboration
The success of the transition from the ED to the OR was a testament to the power of collaboration among various departments and roles within the hospital. This complex process involved six departments and seven distinct roles, all essential to its improvement. These groups’ ongoing collaboration and engagement were crucial for the continued success and sustainability of the standardised handoff process [4]. The experience underscored the principle that those closest to work often have the best insights into solving the associated problems, making this process a shining example of healthcare improvement through teamwork and communication.
1.4 Purpose and scope of the chapter
The chapter on “Perioperative Preparation of Emergency Patients from ED to OR” serves a critical purpose by exploring the intricacies of transitioning emergency patients from the ED to the OR. Its primary objective is to enhance the clinical understanding of healthcare professionals, equipping them with the knowledge and skills necessary to navigate the unique challenges presented by critically ill patients requiring surgical intervention following emergencies. This chapter prioritises patient safety and resource efficiency, emphasising the importance of standardised protocols for information exchange, equipment readiness, and interdisciplinary collaboration. It begins by establishing the criteria for identifying patients needing urgent surgery, encompassing traumatic injuries and acute medical conditions. It extensively covers the interdisciplinary collaboration required among ED staff, OR teams, anaesthesiologists, surgeons, and nurses. The scope includes patient assessment and stabilisation procedures conducted in the ED, focusing on diagnostics, interventions, and life-saving measures.
Furthermore, the chapter delves into handoff protocols and communication strategies, highlighting their crucial role in ensuring safe and efficient patient transfers. It addresses resource allocation, emphasising the optimisation of operating rooms, equipment, and personnel. The chapter also acknowledges the importance of patient and family engagement, stressing clear communication, informed consent, and emotional support.
2. The role of the emergency department in patient evaluation and stabilisation
2.1 Initial assessment and triage in the ED
Initial assessment and triage in the ED are a critical process that is pivotal in providing timely and appropriate care to patients, especially in paediatric cases. The Paediatric Assessment Triangle (PAT) is a valuable tool for rapidly and systematically evaluating a child’s condition upon arrival at the ED [5]. The first step in triage involves a quick assessment of appearance, breathing, and circulation (ABC) using PAT. This initial visual and auditory assessment helps categorise the patient’s illness as stable or unstable. Unstable conditions are further classified into life-threatening and non-life threatening. Patients in the former category, such as those with cardiac arrest, cardio-respiratory failure, decompensated shock, deep coma, or severe stridor, require immediate resuscitation (Figure 2).
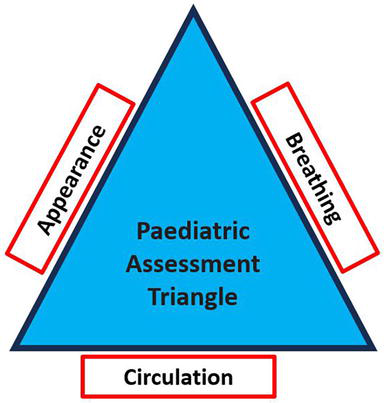
Figure 2.
Paediatric assessment triangle (PAT) (source: [
Once a child is on the path to stabilisation, the primary assessment (ABCDE approach) is conducted. This involves a detailed examination of the airway (A), breathing (B), circulation (C), neurologic abnormalities (D), and a head-to-toe examination (Exposure). This thorough assessment, completed within 1–3 minutes, helps determine the patient’s physiological abnormalities and assigns them to one of five levels of acuity: Resuscitation, Emergent care, Urgent care, Less urgent, or Non-urgent care [5].
The goals of the triage system in the ED are to ensure that the right patient receives the right care from the right provider at the right time to achieve the right outcome. This involves rapidly identifying patients with life-threatening illnesses, initiating appropriate first-aid measures, and continuously monitoring paediatric patients who can deteriorate rapidly. The general PAT assessment is crucial in identifying patients requiring immediate life-saving interventions. Appearance, work of breathing, and circulation are assessed to determine the child’s condition. Abnormal findings in any of these categories may indicate a need for urgent attention.
2.2 Diagnostic procedures in the ED
Advancements in medical technology over the last 25 years have revolutionised emergency medicine, particularly in diagnostic procedures. EDs faced limitations in obtaining diagnostic information in the past, relying mainly on basic lab tests and plain radiographs [6]. However, the landscape has shifted dramatically with the advent of cutting-edge diagnostic tools and improved accessibility to these tests. Today, the emergency department serves as a hub for diagnostic testing, where physicians can efficiently coordinate a patient’s care, and most test results are available within a few hours. This rapid turnaround time is critical in initiating prompt and definitive care, significantly impacting patient outcomes. Advanced diagnostic imaging modalities such as ultrasounds, CT scans, and even MRI studies can be obtained swiftly, allowing for timely diagnoses of conditions such as intracranial haemorrhage, pulmonary embolism, aortic aneurysm, and more [7].
Nevertheless, the ease of obtaining these diagnostic studies comes at a cost. The American College of Radiology reports that diagnostic imaging is the fastest growing medical expenditure in the United States, with an annual growth rate of 9%, triple that of general medical expenditures [6]. Over the past decade, the number of MRI and CT scans performed in EDs quadrupled, and ultrasounds more than doubled. Despite these technological advances, it is crucial to emphasise that diagnostic testing should differ from the importance of a thorough history and physical examination (H&PE) [8]. Before ordering any diagnostic test, clinicians should consider several key questions. They should contemplate how the test results will guide their actions, whether the test will help confirm or exclude a diagnosis, and how the results will impact their overall diagnostic strategy, management plan, or final decision regarding patient disposition. These questions are valuable guides when deciding whether to order a diagnostic test, whether a simple blood test or a costly imaging study.
It is important to note that diagnostic tests should primarily aim to rule in or rule out specific conditions based on the patient’s presenting symptoms and the differential diagnosis generated from their H&PE [7]. However, tests are often ordered for various reasons, including clinical suspicion, established practices, perceived standard of care, requests from consultants or primary care physicians, patient requests, and risk management considerations. Sometimes, diagnostic workups may be influenced by pattern recognition and anecdotal experience, highlighting the blend of art and science in medicine. Consultant physicians can also influence the choice of diagnostic tests [6]. For instance, when a patient presents with abdominal pain, a consultant may request specific tests. However, normal test results should not sway the clinician’s clinical suspicion, and it is an opportunity to educate colleagues about the utility of certain tests in specific contexts.
Statistical considerations play a crucial role in understanding diagnostic testing. Sensitivity and specificity are fundamental concepts. Sensitivity refers to the likelihood of a test being positive in the presence of a disease. At the same time, specificity pertains to the likelihood of a negative test without disease. Tests with high sensitivity are effective at ruling out disease, whereas those with high specificity are good at ruling it in. Positive and negative predictive values (PPV and NPV) consider the prevalence of disease in the population and influence the reliability of a test result [7]. Communication with patients about the rationale behind test orders is essential to manage expectations.
The concept of pretest and post-test probability is also valuable in evaluating the significance of diagnostic test results. It involves considering the patient’s risk factors, clinical presentation, and test outcomes. While evidence-based guidelines exist for many conditions, medicine encompasses science and art, and there may be times when a particular test is not indicated. Bedside ultrasound by emergency physicians has become increasingly prevalent in recent years [6]. This technology allows for rapid assessments and has been shown to improve patient outcomes and the efficiency of care in the ED. It aids in making decisions regarding speciality consultations, operative management, and patient dispositions, often reducing the time needed for these critical determinations.
2.3 Communication between ED and OR teams
Effective communication between the ED and OR teams is paramount in ensuring patient safety and seamless care transitions, particularly in high-stress situations where quick decisions and rapid responses are essential. The significance of communication in healthcare settings, including the ED, has been underscored by various studies, acknowledging that patient safety incidents often occur due to communication breakdowns. A study published in The Journal of Emergency Medicine highlighted the critical role of communication in the ED and its implications for patient care excellence [9]. The authors found that poor ED communication contributed significantly to unfortunate patient outcomes. One prominent issue was inadequate and ineffective staff communication, a challenge exacerbated within the demanding environment of the ED. Problems with the transfer of medical information and orders, especially during shift handoffs, were identified as communication-based factors impacting patient safety. Instances where changes in vital signs were not promptly communicated to attending physicians led to patient safety incidents. Delays in treatment due to communication failures were documented, illustrating the dire consequences of inadequate communication within the ED [9].
Medication management issues, such as incorrect doses, medication errors, delays, and miscalculations, were also attributed to communication problems within the ED. Compliance with patient safety protocols, such as infection control, proper clerical and laboratory processes, and complete discharge instructions, was emphasised as areas where communication lapses could compromise patient safety [10]. Strategies for improving ED outcomes have been proposed to address these communication challenges. One key issue is ambient noise within the ED, which can hinder effective communication. Solutions include noise monitoring, equipment alarm adjustments, and using single-person rooms to reduce noise levels. Communication schemes, such as urgency-based plans and limited overhead paging, have effectively enhanced communication efficiency [10]. Recognising that different healthcare roles require tailored communication approaches and acknowledging the varying communication needs of physicians, nurses, and staff can improve information transfer.
Attention to team dynamics is also crucial. Provider organisations with strong teamwork and communication principles deliver higher-quality care while reducing costs. The Joint Commission has identified communication failures as a common cause of sentinel events. Therefore, promoting teamwork and effective communication within the ED is essential [10]. Implementing daily interdisciplinary huddles, establishing communication channels for departmental information sharing, and encouraging feedback from frontline staff can enhance communication and foster a culture of continuous improvement.
3. Preoperative assessment and planning
3.1 Transfer of care from ED to surgical team
A patient transitioning from the Emergency Department to the surgical team marks the crucial starting point of preoperative assessment and planning. This transition is the foundation for ensuring the patient’s safety and well-being throughout the surgical process. It involves establishing a solid partnership between the anaesthesiologist and the patient. This partnership is built upon mutual understanding, which involves outlining the anaesthesia technique and recognising any associated risks. Simultaneously, it aims to offer premedication drugs and carry out necessary interventions before surgery [11]. A key aspect of risk assessment involves tailored investigations and referrals from other medical specialities. Effective preoperative assessment helps prevent last-minute delays or postponements of surgery, ensuring a smoother and more efficient process.
3.2 Comprehensive patient evaluation
A thorough preoperative evaluation is the cornerstone of optimal surgical preparation. It encompasses a detailed patient history, comprehensive physical examination, and essential laboratory investigations. The history-taking process delves into past adverse reactions to anaesthesia, difficulties with intravenous access, airway management complications, extended recovery times, postoperative nausea and vomiting, and delirium experiences. It also considers specific details, such as whether the patient is scheduled for elective or emergency surgery, if they have cardiac issues undergoing non-cardiac procedures, or if they are taking anticoagulants, among other factors [12]. Assessing functional status through comprehensive measures is crucial for geriatric patients to identify those at risk and anticipate potential complications. This comprehensive evaluation includes recording all medications, doses, and a detailed history of over-the-counter and herbal drugs, illicit substance use, addiction history, malignant hyperthermia susceptibility, and other adverse reactions [11]. Anthropometric measurements and hemodynamic parameters should also be documented. The examination must carefully inspect the airway and spine and systematically review various organ systems, ensuring a holistic understanding of the patient’s health.
3.3 Identifying comorbidities and special considerations
The healthcare landscape has evolved over the years, resulting in many surgical candidates with advanced age and multiple comorbidities, often on multiple medications. This shift has necessitated adaptations in perioperative patient care. Identifying comorbidities and addressing special considerations are critical steps in preoperative planning. Risk assessment tools, such as the American Society of Anaesthesiologists physical status (ASA PS) grading, aid in shaping the anaesthesia plan. However, while valuable, these tools may only encompass some preoperative physiological and functional aspects, the type of surgery, and postoperative care [13]. To enhance comorbidity assessment, age-adjusted scores, such as the National Surgical Quality Improvement Programme (NSQIP) model, the Charlson comorbidity index (CCI), or the revised cardiac risk index (RCRI), are recommended, particularly for cardiac perioperative risk stratification. Functional status, often measured in metabolic equivalents (METS), quantifies an individual’s exercise capacity and ability to withstand surgical stress. Cardiopulmonary exercise testing (CPET) provides a more in-depth assessment but requires specialised facilities and trained personnel [12]. Surgical risk varies based on the type of procedure, with minor surgeries presenting lower cardiovascular risk and major surgeries, such as peripheral vascular or transplant surgeries, associated with higher-risk percentages.
3.4 Informed consent and shared decision-making
Preoperative assessment tools must align with patient sensitivities in an era of heightened patient awareness, knowledge, and safety expectations. Informed consent and shared decision-making have taken on greater significance. Patients should be informed about the planned surgery, potential risks, and alternative options. Engaging patients in these discussions empowers them to actively participate in their care journey [12]. Additionally, when evaluating patients for surgery, special attention should be given to identifying risk factors related to obstructive sleep apnoea (OSA). Although polysomnography is the gold standard for diagnosing OSA, its routine use as a screening tool is impractical [11]. Various questionnaires, such as the STOP-Bang questionnaire, can aid in identifying patients at risk for OSA. These assessments help tailor perioperative care plans to mitigate OSA-related complications. Preoperative investigations should be guided by protocols, such as those outlined by the Indian Society of Anaesthesiologists, taking into account the patient’s circumstances and validity periods of previous tests [14].
3.5 Preoperative optimisation/prehabilitation
Preparing patients for surgery involves assessing risks and optimising their physical condition. Preoperative optimisation minimises perioperative complications, such as bronchospasm, aspiration, pulmonary infections, wound infections, and myocardial events [11]. Optimisation strategies may include lifestyle modifications such as smoking and alcohol cessation, adjustments to antihypertensive and antidiabetic treatments, incentive spirometry to improve lung function, management of anaemia, and enhancement of exercise tolerance [12]. Prehabilitation, a related concept, focuses on improving physical functionality through exercises tailored to specific surgical procedures. While direct evidence of its impact on postoperative pain and functionality remains under investigation, prehabilitation has shown promise in reducing rehabilitation unit admissions. Emotional and psychological support through preoperative counselling also helps alleviate patient anxiety and fear, enhancing their overall surgical experience [15].
3.6 Decision to defer surgery
Finally, the decision to defer surgery is a patient-specific assessment that considers factors such as medication use, the severity of comorbidities, surgical risk, and hypertension control. Different types of surgeries have varying thresholds for postponement. Urgency, institutional practices, monitoring capabilities, and clinician and patient preferences all influence this decision. High-risk procedures, especially those impacting airway or cardiopulmonary function, may necessitate a lower threshold for surgery delay, particularly for patients with uncontrolled obstructive sleep apnoea (OSA) [11, 16]. Preoperative evaluation clinics play a vital role in making these determinations, along with the availability of sleep testing when needed.
References
- 1.
Karioja P. What is Perioperative Care? [Online]. 2021. Available from: https://www.buddyhealthcare.com/en/blog/what-is-perioperative-care ;www.buddyhealthcare.com - 2.
CPOC. What is Perioperative Care? Centre for Perioperative Care [Online]. 2023. Available from: https://cpoc.org.uk/about-cpoc/what-perioperative-care ;cpoc.org.uk - 3.
Atzema CL, Maclagan LC. The transition of care between emergency department and primary care: A scoping study. Academic Emergency Medicine. 2017; 24 (2):201-215. DOI: 10.1111/acem.13125 - 4.
Medcom. Standardizing Emergency Department to Operating Room handoff for Class A surgery - The Loop [Online] The Loop. 2015. Available from: https://medcom.uiowa.edu/theloop/quest-newsletter/standardizing-emergency-department-to-operating-room-handoff-for-class-a-surgery - 5.
Jayashree M, Singhi SC. Initial assessment and triage in ER. The Indian Journal of Pediatrics. 2011; 78 (9):1100-1108. DOI: 10.1007/s12098-011-0411-3 - 6.
SAEM. Diagnostic Testing in the Emergency Department Default [Online]. 2022. Available from: https://www.saem.org/about-saem/academies-interest-groups-affiliates2/cdem/for-students/online-education/m3-curriculum/group-diagnostic-testing/diagnostic-testing-in-the-emergency-department - 7.
Kayathri P. What Are the Diagnostic Tests Done in an Emergency Setup? [Online]. 2023. Available from: https://www.icliniq.com/articles/first-aid-and-emergencies/diagnostic-tests-during-emergency ;www.icliniq.com [Accessed: September 4, 2023] - 8.
Shallik N, Zaghw A, Dogan Z, Rahman W. The use of virtual endoscopy for diagnosis of traumatic supra-glottic airway stenosis. JCAO. 2017; 2 (103):2 - 9.
Healthline. Improving Communication in the Emergency Room Default [online]. 2021. Available from: https://www.healthstream.com/resource/blog/improving-communication-in-the-emergency-room - 10.
O’Daniel M, Rosenstein AH. Professional Communication and Team Collaboration NCBI [Online]. 2018. Available from: https://www.ncbi.nlm.nih.gov/books/NBK2637/ - 11.
Jindal P, Patil V, Pradhan R, Mahajan HC, Rani A, Pabba UG. Update on preoperative evaluation and optimisation. Indian Journal of Anaesthesia [online]. 2023; 67 (1):39-47. DOI: 10.4103/ija.ija_1041_22 - 12.
Teach Me Surgery. The Pre-Operative Assessment - TeachMeSurgery [online]. TeachMeSurgery. 2018. Available from: https://teachmesurgery.com/perioperative/preoperative/assessment/ - 13.
Shallik N, Karmakar A. Is it time for high flow nasal oxygen to be included in the difficult airway algorithm? British Journal of Anaesthesia. 2018; 121 (2):511-512 - 14.
Shallik N. Anesthetic Management for Drug Induced Sleep Endoscopy. Middle East Journal of Anaesthesiology. 2015; 23 (2):131-135 - 15.
Dardeer A, Shallik N. Perioperative anaphylaxis: A new visit to an old topic. Trends in Anaesthesia and Critical Care. 2019; 26 (27):1e10 - 16.
Dardeer A, Alhammad MF, Shallik NA. Anesthesia management in OSA patient. In: Delakorda M, de Vries N. (eds) The Role of Epiglottis in Obstructive Sleep Apnea. Cham: Springer; 2023. DOI: 10.1007/978-3-031-34992-8_26