
Abstract
Donor-derived cell-free DNA (Dd-cfDNA) is a novel biomarker with many diagnostic applications in various areas of medicine and particularly transplantation. This biomarker is derived from donor cells that have undergone apoptosis or cell death and thus reflects possible graft damage. Regarding the field of liver transplantation, dd-cfDNA can contribute to the diagnosis of complications that include signs of rejection or other types of possible graft injury. Measurements of dd-cfDNA also depend on the graft’s size and origin; therefore, these data should be considered for the estimation and explanation of dd-cfDNA values. Despite the utility of this novel diagnostic technique, it comes with some limitations and application exclusions, such as cases where there is a blood relation between the donor and recipient. Combination of dd-cfDNA evaluation with the assessment of other currently used biomarkers, such as liver enzymes, or other novel biomarkers can result to high diagnostic value.
Keywords
- liver transplantation
- non-invasive
- biomarkers
- dd-cfDNA
- evaluation of liver graft
1. Introduction
Liver transplantation (LT) is the only treatment option for end-stage liver failure and the best option for some specific cases of liver cancer. In 1963, Starzl et al. performed the first liver transplantation [1]. It took over a decade for LT to overcome the challenges associated with the immune response, with a noteworthy breakthrough being the application of cyclosporine, yielding positive long-term outcomes for patients [2]. Despite a steady increase in the number of LT operations with nowadays more than 35,000 liver transplants being performed globally, long-term survival beyond the first year after LT has not significantly improved in the past decades due to many factors, including the long-term effects of immunosuppression and graft dysfunction [3].
A significant obstacle to LT long-term graft and patient’s survival is the lack of a reliable and non-invasive biomarker that monitors graft function and detects graft injury early. Reliable, non-invasive detection of possible damage of liver graft constitutes a prominent area of research in transplantation, with various biomarkers and biomarker panels already being researched about their specificity and sensitivity.
In this chapter, we aimed to describe the possible role of donor-derived cell-free DNA (dd-cfDNA) in the evaluation of liver graft and monitoring of liver transplant recipients.
2. Liver histology
Liver is a parenchymal organ, covered by a peritoneal lining consisting of a single-layer mesothelium disposed on a thin layer of sub-mesothelial connective tissue [4]. Regarding the morphology of the liver, this is based on morpho-functional units called hepatic lobules [5]. Each hepatic lobule appears as an area of polygonal shape, made up of laminae of epithelial cells, the hepatocytes. In the spaces between the hepatocytes, there is a dense vascular network consisting of capillaries called hepatic sinusoids. In the center of the lobule, there is a central (centrilobular) vein, while in the periphery, there are terminal branches of the portal vein and of the hepatic artery, which in combination of branches of bile ducts, they form the portal or porto-biliary spaces. Apart from this morphology model, there are some other ones proposed like the portal lobule and hepatic acinus [6]. Concerning the cell types that consist liver histology, those apart from hepatocytes include endothelial cells, hepatic stellate cells, Kupffer cells, lymphocytes, and cholangiocytes, which consist the intrahepatic bile ducts [7, 8, 9, 10].
3. Pathophysiology of LT-related pathologies
There are many pathologies related to liver transplantation that may result in dysfunction or even non-function of the graft. These pathologies include subclinical graft injury, chronic or acute rejection, infections, and cancer. For the accurate, non-invasive diagnosis of those pathologies, a background knowledge of their pathophysiology is needed.
The most common pathology that occurs in LT and the base of other LT-related pathologies as well is the graft injury. Graft injury can be caused by ischemia-reperfusion process, with the anoxia occurring in liver tissue resulting in the generation of reactive oxygen species and initiation of a cellular cascade leading to inflammation and cell death. Apart from cell cascade and oxygen free radicals, T cells and Kupffer cells have found to be in the center of liver graft injury resulting in the observed in surveillance liver graft biopsies (svLBxs) neutrophil inflammation [11, 12, 13].
Rejection is also considered a form of graft injury with liver dysfunction being observed as well. There are two major types of rejection classified based on the time of occurrence: acute and chronic. Moreover, rejection types can be classified based on the pathophysiology mechanism on T-cell (TCR) and antibody-mediated (AMR). TCR usually occurs early, and the diagnosis is based on biopsy findings including dense portal-based mixed inflammatory cell infiltrate with the evidence of damage to biliary epithelium, portal and hepatic vein endothelium, and hepatocytes [14]. During liver inflammation, the expression of MHC class I is increased in all cell types, instead of being limited to Kupffer cells like in the normal liver, and MHC class II expression is stimulated in endothelium, biliary epithelium, and hepatocytes. Activated donor-derived dendritic cells arriving in the lymph node act as a potent immunological stimulus for recipient-derived naive CD4+ T cells. CD8+ and CD4+ T cells are participating in rejection pathophysiology by differentiating into different T-cell subtypes, primarily polarized toward the Th1 response with the secretion of many cytokines. AMR can happen early and later on, with the most severe form being the hyperacute rejection that occurs in ABO-incompatible grafts [15]. In AMR, donor-specific antibodies (DSA) play a pivotal role. They can be preformed or de novo produced by the interaction of B cells with alloantigens [16].
LT recipients are also prone to different infections due to their immunosuppressive treatment scheme. Viral infections of the liver graft like cytomegalovirus (CMV), EBV, and HCV can result in various pathophysiological alterations and dysfunction. CMV infection has a high prevalence in the general population and can be serious in recipients who were seronegative prior to liver transplantation. The pathophysiology of liver damage in CMV infections is based both on the direct effect of the virus in mesenchymal and endothelial cells and to the modulation of the immune system that may result to acute early allograft rejection or late allograft dysfunction [17]. HCV infection can be acute or chronic and, apart from immediate immune alterations, can result in liver fibrosis [18, 19].
Cancer is a very serious, rare complication of chronic immunosuppression. Apart from the rare occurrence of cancer as a result of immunosuppression, LT recipients operated for hepatocellular carcinoma (HCC) based on Milan criteria show a risk of recurrence in 8–20% of the cases [20, 21]. HCC is a highly heterogeneous cancer, both at the molecular and histological level. There is a strong correlation between HCC with fibrosis, molecular mechanisms related to comprise telomere maintenance, Wnt/β-catenin signaling and cell cycle regulation, TERT promoter alterations, and CTNNB1 and TP53 mutations [22].
4. Current methods of liver graft evaluation
In today’s clinical practice, the established everyday clinical practice for graft evaluation includes the serum measurement of alanine aminotransferase (ALT) and aspartate aminotransferase (AST), along with the performance of surveillance liver graft biopsy (svLBxs). Each of those methods of evaluation is not optimal and opposes certain limitations. Particularly, for the liver function enzymes evaluation, main limitations include their lack of liver specificity, the reflection of damage of specific cell types (hepatocytes or cholangiocytes), and their long half-lives [23, 24]. Regarding svLBxs, despite its specificity in detecting and diagnosing different graft injuries and pathologies, when considering the complexity and large size of the liver, its sensitivity is far from 100%, which often leads to inaccurate diagnosis. Moreover, it remains an invasive procedure with certain risks for the patient and a high cost, all of the above leading to this not being an evidence-based applied procedure to most of the liver transplantation centers [25].
5. Recent breakthroughs in non-invasive liver graft evaluation
In recent years, precision medicine research is focused on unraveling the molecular pathways associated with specific liver graft pathologies [26]. A primary objective of this field of research is the investigation of the potential role of liver-specific biomarkers in the non-invasive accurate diagnosis. For a biomarker to be considered suitable for everyday clinical practice application, it has to fulfill certain qualifications. These include the non-invasive detection, the specificity about liver graft and sensitivity about different pathologies. Shorter half-life time and cost effectiveness are also desirable characteristics of a possible biomarker [27, 28]. There has already been found a correlation between graft dysfunction, pathologies, and different types of biomarkers including nucleic and protein ones, metabolites, and the recently discovered extracellular vesicles [29, 30, 31]. Among protein biomarkers are those involved in immune responses, like in complement system activation (C3a, C5a, and sC5b-9), C-reactive Protein, cytokines, MHC class I polypeptides, and different types of CD blood cells, enzymes such as ATP citrate lyase, apolipoprotein A1, and butyrylcholinesterase, structural proteins such as fibrinogen alpha chain, and signaling proteins such as VEGF [32, 33, 34, 35, 36].The majority of the research although so far is focused on nucleic biomarkers which include different types of miRNAs, mRNAs, long non-coding RNAs(lncRNAs), DNAs, and dd-cfDNA [37, 38, 39, 40, 41, 42].
6. Role of dd-cfDNA
dd-cfDNA has emerged as a non-invasive, precise biomarker for monitoring liver transplant recipients by many researchers. Over the past few years, the utilization of dd-cfDNA has witnessed a notable increase, with potential applications including the early detection of cancer and graft dysfunction in various types of transplantation [43]. Dd-cfDNA was first used by Sigdel et al. as a rapid non-invasive assay for the detection of renal transplant injury [44]. Originating from apoptotic cells within the graft, dd-cfDNA exhibits remarkable specificity, with a limitation in sensitivity. Dd-cfDNA has applications in every type of solid organ transplantation, a characteristic that justifies the extensive research existing about this emerging biomarker [45].
7. Methods of evaluation of dd-cfDNA
Dd-cfDNA is measured most usually in serum or in plasma and sometimes in urine, especially when it comes to kidney transplantation monitoring [46]. Its assessment includes an evaluation of its quantity, but also an investigation of some quality characteristics, such as the size of the fragments and methylation patterns [47]. Particularly, for its detection in serum, various types of polymerase chain reaction (PCR) are available, and alternatively, an approach used for female recipients with male donors is the amplification of Y-chromosome specific genes [48]. Distinguishing the donor-derived cfDNA from the recipient-derived type is a process including the following steps. Firstly, SNP (single-nucleotide polymorphism) selection is conducted, followed by the targeted amplification and sequencing of the cfDNA samples [49]. The next step is the statistical determination of the recipient’s heterozygous cutoff, on whose basis dd-cfDNA is estimated. Additionally, the value of the technique is increased by sample quality control and analytical validation [50]. Dd-cfDNA is a biomarker with a short half-life (<1.5 h), a characteristic adding accuracy in its clinical value [51]. Evaluation techniques of dd-cfDNA can be found in Figure 1.
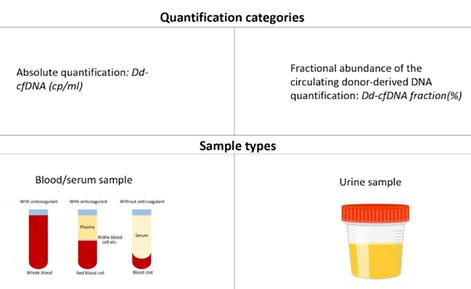
Figure 1.
Dd-cfDNA evaluation methods.
8. Applications of dd-cfDNA evaluation in liver transplantation
Dd-cfDNA has many applications in the diagnosis of LT complications and in the monitoring of LT recipients. Those include early detection of pathological lesions, diagnosis of infections related to transplantation, monitoring of the patients, and cancer recurrence in cases of LT performed as treatment for hepatocellular cancer. Figure 2 includes a scheme about applications of dd-cfDNA in LT.
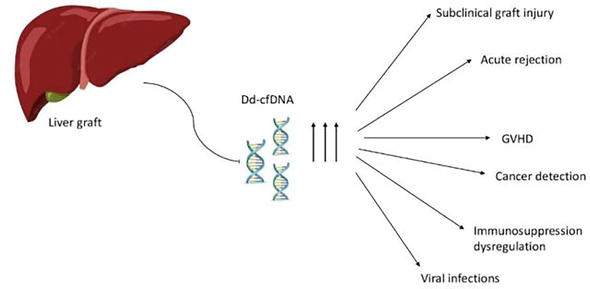
Figure 2.
Applications of dd-cfDNA in liver transplantation.
8.1 Dd-cfDNA and subclinical graft injury evaluation
Subclinical graft injury refers to notable histological inflammation, while liver enzyme levels remain relatively normal, particularly under 2× ULN [52]. Using svLBxs, it has been observed that over 25% of liver transplant recipients with regular liver enzymes show graft injuries indicative of T-cell-mediated rejection (TCMR) [53, 54]. While svLBxs are very specific when it comes to detecting subclinical T-cell-mediated rejection (SubTCMR), their invasive nature and potential risks limit their frequent application in clinical settings. Dd-cfDNA emerges as a promising noninvasive marker for early identification of sub-TCMR. Several studies highlight a relationship between increased dd-cfDNA levels and sub-TCMR. For instance, there has been mentioned notably elevated fractional dd-cfDNA in patients exhibiting sub-TCMR, with a sensitivity and specificity of this method being 73 and 52%. Despite the differences in fractional dd-cfDNA levels, there were no significant differences in absolute dd-cfDNA levels between those with or without graft damage [50]. Furthermore, during the investigation of personalized immunosuppressive treatment schemes, elevated graft cell-free DNA (GcfDNA) has been identified in cases of subclinical graft damage due to inadequate tacrolimus levels and connections between dd-cfDNA levels, tacrolimus concentrations, and the frequency of graft injuries have been also found, resulting in an optimal level of tacrolimus at around 6.8 μg/L [54, 55]. Moreover, increased GcfDNA percentage (graft cfDNA/total cfDNA) has been correlated with graft injury, reaching levels even above 50% after ischemia-reperfusion [54]. Lastly, short dd-cfDNA fractions specifically were also linked to graft impairments, indicating that small/large fragments ratio lower than 0.6 is correlated with stability of the graft function. [47].
8.2 Dd-cfDNA and diagnosis of rejection
In cases of rejection, and particularly acute rejection, the use of dd-cfDNA proved to be more sensitive and diagnostically valuable than liver function tests (LFTs), enabling an earlier and more accurate detection. Many studies have indicated that LT recipients experiencing acute rejection exhibit higher serum levels of dd-cfDNA compared to those without rejection, with the median dd-cfDNA percentage being three-fold higher comparing to before rejection diagnosis levels [50, 56, 57, 58, 59]. The sensitivity and specificity of dd-cfDNA-based acute rejection diagnosis differentiated, ranging between 72 and 100% and 53–91% based on different cutoff levels. Additionally, it has been highlighted that dd-cfDNA serves not just as a non-invasive diagnostic tool for acute rejection but also allows for earlier detection than biopsies and conventional LFTs, detecting possible graft damage 1–2 days earlier than conventional methods [54]. A strategy to pinpoint the source of dd-cfDNA and diagnose complications in the recipient involves analyzing the fractions ratio, particularly patients undergoing acute rejection tend to have an elevated ratio of short fragments compared to individuals with healthy grafts [43].
8.3 Dd-cfDNA in graft versus host disease diagnosis
Graft versus host disease (GVHD) is a rare but life-threatening complication related to transplantation of mostly bone marrow and in rare cases solid organs [60]. It is recognized to have an asymptomatic phase, allowing for early identification and intervention by adjusting immunosuppressive drug levels [61]. Traditional methods for early GVHD detection, which rely on molecular techniques targeting macro chimerism, have been neither cost-effective nor feasible for routine clinical use [62]. Dd-cfDNA has been the center of a newly introduced, innovative diagnostic approach for GVHD detection. This method identifies GVHD based on criteria like increased serum dd-cfDNA levels, elevated proportions of donor-origin T and B cells, and the presence of donor-derived genomic-DNA (dd-gDNA) in skin samples. Such findings suggest the presence of multisystemic GVHD and potential concurrent infections. These strategies could serve as non-invasive tools for immune surveillance, facilitating quicker GVHD identification and thus resulting in an earlier treatment [48].
8.4 Dd-cfDNA in liver graft viral infections diagnosis
Transplant patients are following a medication scheme of continuous immunosuppression making them particularly susceptible to various opportunistic infections, including EBV and CMV. This susceptibility highlights the importance of having a non-invasive marker to assess potential viral infections in LT patients. There has been found that individuals with EBV or CMV exhibited notably elevated percentages and median quantities of dd-cfDNA, with CMV patients showing even higher levels than those with EBV (0.866 vs. 0.764 dd-cfDNA (cp/mL)) [63]. Furthermore, LT patients are prone to HCV infection. HCV-positive patients displayed a somewhat elevated and more variable GcfDNA proportion compared to those in stable health [54, 62].
8.5 Dd-cfDNA and early detection of cancer recurrence
It is known that liver transplantation is an evidence-based worldwide accepted treatment option for patients with liver tumors [64]. Usually, LT is performed in patients with hepatocellular cancer (HCC) according to Milan criteria, but in recent years, it has been applied in a series of patients with cholangiocarcinoma as well [65, 66, 67]. LT recipients require immunosuppression treatment in order to avoid rejection-related complications; thus, they are susceptible to cancer recurrence, with tumor recurrence rate after LT is estimated to be 8–20% [20, 21]. The gold standard of screening tests in these patients include imaging methods, tissue biopsies, and serum alpha-fetoprotein (AFP) follow-up [68]. Although those tests show great sensitivity and specificity in cancer detection, they result in radiation intake and many complications related to invasive biopsy procedure. Cell-free DNA (CfDNA), also referred to as liquid biopsy, appears to be an emerging biomarker of early, non-invasive diagnosis of cancer recurrence in LT recipients. Diagnostic approach of cancer is based on qualitative, with methylation profiles and different gene mutations being the main focus, and quantitative assessment, [69, 70]. CfDNA and other nucleic acid biomarkers diagnostic accuracy in HCC detection has been a field of research in the part, with promising results [70, 71, 72, 73, 74, 75]. Apart from the diagnosis of cancer, those biomarkers have been used for the evaluation of biological activity and metastatic profile of the tumor [73]. When it comes to LT recipients, cfDNA-based diagnosis of cancer recurrence follows the same principles, with practically the tumor-related cfDNA being actually graft derived dd-cfDNA [64, 76, 77, 78]. Particularly, positive preoperative cfDNA is related to tumor characteristics such as larger size, multiple lesions, microvascular invasion, and advanced stages. Additionally, cfDNA is also a predictive factor for disease free and overall survival, with positive preoperative cfDNA status being correlated with shorter overall (mean 22.5 vs. 40.0 months) and disease-free survival (mean 16.6 vs. 35.3) [78].
8.6 Monitoring of immunosuppressant LT recipients
The value of evaluating dd-cfDNA clinically stems from its non-invasive nature and swift assessment. These attributes advocate for the inclusion of dd-cfDNA in routine monitoring for all LT recipients. Specifically, there has already been mentioned previously the significance of correlating dd-cfDNA concentrations with tacrolimus levels [79, 80].Moreover, dd-cfDNA has been used for the personalization of dosage and monitoring of patients receiving tocilizumab and belatacept in kidney transplant recipients, with possible application to liver transplant recipients as well. [81, 82]. The success of tocilizumab treatment is evaluated with the decrease of levels of dd-cfDNA (%), with a decrease of 47% being reported after 12 months of treatment [81]. Although there are no specific official guidelines about the testing times for dd-cfDNA evaluation, days 7 and 14 after transplantation, followed by monthly testing over 6 months and every 3-month time points have been suggested [80].
9. Limitations of cfDNA application in everyday clinical practice
Even though dd-cfDNA can potentially be the gold standard in LT recipients monitoring, its application does not come without certain limitations. Firstly, due to factors like immunosuppression or underlying medical conditions, LT recipients may experience conditions such as leukopenia, leukocytosis, and inflammatory diseases, which could impact the accurate measurement of fractional dd-cfDNA. Additionally, as previously mentioned, while dd-cfDNA serves as a potential marker for various LT complications linked to graft damage, resulting in lack of specificity [83]. Moreover, there are specific scenarios in LT where dd-cfDNA might not serve as a viable biomarker, such as cases involving identical twin donors or donors and recipients from closely related families. Additionally, the use of dd-cfDNA for diagnosis becomes challenging in scenarios like dual organ transplants from a single donor or multiple organ transplants from diverse donors [84]. Lastly, dd-cfDNA is influenced by parameters like the size of the graft and its origin [55]. Higher peaks of dd-cfDNA in cases of deceased donor LT are most likely explained by higher levels of ischemia–reperfusion injury, but also by the fact that elevations in dd-cfDNA are more dramatic in larger grafts from deceased donors than from partial grafts in living donors [62, 85].
10. Conclusion
Although major progress has been made in the recent years when it comes to biomarkers research and particularly dd-cfDNA use in non-invasive monitoring of LT recipients, certain areas remain unexplored. The predominant focus of research lies on the use of dd-cfDNA for post-transplantation diagnosis. With the increase of the usage of machine perfusion, even in liver transplantation, dd-cfDNA could possibly serve as an useful biomarker for early pre-transplantation evaluation of the quality of the graft [86].
Another obstacle when it comes to clinical application of dd-cfDNA is the difficulty, expense, and time-intensive nature of its evaluation technique. Newly developed assays based on spectrophotometry, electrophoresis, or quantitative PCR (qPCR), next-generation sequencing, BEAMing (beads, emulsion, amplification, and magnetics), or droplet digital PCR (ddPCR), could possibly be applied in the dd-cfDNA assessment process and lead to faster accurate results [87, 88].
Lastly, the role of Artificial Intelligence (AI) in transplantation research is fundamental. AI has the potential to contribute significantly to the development of new applications of dd-cfDNA, with the formations of algorithms for graft evaluation based on dd-cfDNA values and with the detection of new genes and methylation patterns for the precise diagnosis of graft pathologies.
Conflict of interest
The authors declare no conflict of interest.
References
- 1.
Starlz TE, Marchioro TL, Vonkaulla KN, Hermann G, Brittain RS, Wadell WR. Homotransplantation of the liver in humans. Surgery, Gynecology & Obstetrics. 1963; 117 :659-676 - 2.
Calne RY, Rolles K, White DJ, et al. Cyclosporin a initially as the only immunosuppressant in 34 recipients of cadaveric organs: 32 kidneys, 2 pancreases, and 2 livers. Lancet. 1979; 2 (8151):1033-1036. DOI: 10.1016/s0140-6736(79)92440-1 - 3.
International report on organ donation and Available at: https://www.transplant-observatory.org/wp-content/uploads/2022/12/2021-data-global-report-1.pdf [Accessed: 26 January 2024] - 4.
Carotti S, Morini S, Carpino G, Gaudio E. Liver histology. In: Radu-Ionita F, Pyrsopoulos N, Jinga M, Tintoiu I, Sun Z, Bontas E, editors. Liver Diseases. Cham: Springer; 2020. DOI: 10.1007/978-3-030-24432-3_2 - 5.
Francis K. The anatomy and physiology of the liver. Philosophical Transactions of the Royal Society. 1833; 123 :123711-123770. DOI: 10.1098/rstl.1833.0031 - 6.
Mall FP. A study of the structural unit of the liver. American Journal of Anatomy. 1906; 5 :227-308 - 7.
Poisson J et al. Liver sinusoidal endothelial cells: Physiology and role in liver diseases. Journal of Hepatology. 2017; 66 (1):212-227. DOI: 10.1016/j.jhep.2016.07.009 - 8.
Dixon LJ, Barnes M, Tang H, Pritchard MT, Nagy LE. Kupffer cells in the liver. Comprehensive Physiology. 2013; 3 (2):785-797. DOI: 10.1002/cphy.c120026 - 9.
Peng H, Wisse E, Tian Z. Liver natural killer cells: Subsets and roles in liver immunity. Cellular & Molecular Immunology. 2016; 13 :328-336. DOI: 10.1038/cmi.2015.96 - 10.
Alvaro D, Mancino MG, Glaser S, et al. Proliferating cholangiocytes: A neuroendocrine compartment in the diseased liver. Gastroenterology. 2007; 132 (1):415-431. DOI: 10.1053/j.gastro.2006.07.023 - 11.
Kupiec-Weglinski JW, Busuttil RW. Ischemia and reperfusion injury in liver transplantation. Transplantation Proceedings. 2005; 37 (4):1653-1656. DOI: 10.1016/j.transproceed.2005.03.134 - 12.
Kageyama S, Kadono K, Hirao H, et al. Ischemia-reperfusion injury in allogeneic liver transplantation: A role of CD4 T cells in early allograft injury. Transplantation. 2021; 105 (9):1989-1997. DOI: 10.1097/TP.0000000000003488 - 13.
Abu-Amara M, Yang SY, Tapuria N, Fuller B, Davidson B, Seifalian A. Liver ischemia/reperfusion injury: Processes in inflammatory networks--a review. Liver Transplantation. 2010; 16 (9):1016-1032. DOI: 10.1002/lt.22117 - 14.
Shetty S, Adams DH, Hubscher SG. Post-transplant liver biopsy and the immune response: Lessons for the clinician. Expert Review of Clinical Immunology. 2012; 8 (7):645-661. DOI: 10.1586/eci.12.65 - 15.
Heidt S, Hester J, Shankar S, Friend PJ, Wood KJ. B cell repopulation after alemtuzumab induction-transient increase in transitional B cells and long-term dominance of naïve B cells. American Journal of Transplantation. 2012; 12 (7):1784-1792. DOI: 10.1111/j.1600-6143.2012.04012.x - 16.
O'Leary JG, Kaneku H, Demetris AJ, et al. Antibody-mediated rejection as a contributor to previously unexplained early liver allograft loss. Liver Transplantation. 2014; 20 (2):218-227. DOI: 10.1002/lt.23788 - 17.
Onpoaree N, Sanpavat A, Sintusek P. Cytomegalovirus infection in liver-transplanted children. World Journal of Hepatology. 2022; 14 (2):338-353. DOI: 10.4254/wjh.v14.i2.338 - 18.
Berumen J, Baglieri J, Kisseleva T, Mekeel K. Liver fibrosis: Pathophysiology and clinical implications. WIREs Mechanisms of Disease. 2021; 13 :e1499. DOI: 10.1002/wsbm.1499 - 19.
Irshad M, Gupta P, Irshad K. Immunopathogenesis of liver injury during hepatitis C virus infection. Viral Immunology. 2019; 32 (3):112-120. DOI: 10.1089/vim.2018.0124 - 20.
Sapisochin G, Goldaracena N, Laurence JM, et al. The extended Toronto criteria for liver transplantation in patients with hepatocellular carcinoma: A prospective validation study. Hepatology. 2016; 64 (6):2077-2088. DOI: 10.1002/hep.28643 - 21.
Silva MF, Sherman M. Criteria for liver transplantation for HCC: What should the limits be? Journal of Hepatology. 2011; 55 (5):1137-1147. DOI: 10.1016/j.jhep.2011.05.012 - 22.
Calderaro J et al. Molecular and histological correlations in liver cancer. Journal of Hepatology. 2019; 71 (3):616-630. DOI: 10.1016/j.jhep.2019.06.001 - 23.
Pratt DS, Kaplan MM. Evaluation of abnormal liver-enzyme results in asymptomatic patients. The New England Journal of Medicine. 2000; 342 (17):1266-1271. DOI: 10.1056/NEJM200004273421707 - 24.
Center SA. Interpretation of liver enzymes. Veterinary Clinics of North America: Small Animal Practice. 2007b; 37 (2):297-333. DOI: 10.1016/j.cvsm.2006.11.009 - 25.
Rocque B, Zaldana A, Weaver C, et al. Clinical value of surveillance biopsies in Pediatric liver transplantation. Liver Transplantation. 2022; 28 (5):843-854. DOI: 10.1002/lt.26399 - 26.
Gracia-Sancho J, Casillas-Ramírez A, Peralta C. Molecular pathways in protecting the liver from ischaemia/reperfusion injury: A 2015 update. Clinical Science (London, England). 2015; 129 (4):345-362. DOI: 10.1042/CS20150223 - 27.
de Miranda FS, Barauna VG, dos Santos L, Costa G, Vassallo PF, Campos LCG. Properties and application of cell-free DNA as a clinical biomarker. International Journal of Molecular Sciences. 2021; 22 (17):9110. DOI: 10.3390/ijms22179110 - 28.
Aronson JK, Ferner RE. Biomarkers—A general review. Current Protocols in Pharmacology. 2017; 76 (1):9.23.1-9.23.17. DOI: 10.1002/cpph.19 - 29.
Lin Z, Li H, He C, et al. Metabolomic biomarkers for the diagnosis and post-transplant outcomes of AFP negative hepatocellular carcinoma. Front. Oncologia. 2023; 13 :1072775. Published 2023 Feb 9. DOI: 10.3389/fonc.2023.1072775 - 30.
Zhu H, Wang M, Xiong X, et al. Plasma metabolomic profiling reveals factors associated with dose-adjusted trough concentration of tacrolimus in liver transplant recipients. Frontiers in Pharmacology. 2022; 13 :1045843. Published 2022 Oct 31. DOI: 10.3389/fphar.2022.1045843 - 31.
De Stefano N, Calleri A, Faini AC, et al. Extracellular vesicles in liver transplantation: Current evidence and future challenges. International Journal of Molecular Sciences. 2023; 24 (17):13547. Published 2023 August 31. DOI: 10.3390/ijms241713547 - 32.
Budkowska M, Ostrycharz E, Serwin NM, et al. Biomarkers of the complement system activation (C3a, C5a, sC5b-9) in serum of patients before and after liver transplantation. Biomedicine. 2023; 11 (7):2070. Published 2023 July 23. DOI: 10.3390/biomedicines11072070 - 33.
Yu J, Shi X, Ma J, et al. C-reactive protein is an independent predictor of 30-day bacterial infection post-liver transplantation. Biomolecules. 2021; 11 (8):1195. Published 2021 Aug 12. DOI: 10.3390/biom11081195 - 34.
Boix F, Legaz I, Minhas A, et al. Identification of peripheral CD154+ T cells and HLA-DRB1 as biomarkers of acute cellular rejection in adult liver transplant recipients. Clinical and Experimental Immunology. 2021; 203 (2):315-328. DOI: 10.1111/cei.13533 - 35.
Decker SO, Krüger A, Wilk H, et al. Concurrent change in serum cholinesterase activity and Midregional-Proadrennomedullin level could predict patient outcome following liver transplantation. Biomolecules. 2022; 12 (7):989. Published 2022 Jul 15. DOI: 10.3390/biom12070989 - 36.
Wang W, Wang B, Liu C, et al. Serum proteomic predicts effectiveness and reveals potential biomarkers for complications in liver transplant patients. Aging (Albany NY). 2020; 12 (12):12119-12141. DOI: 10.18632/aging.103381 - 37.
Morsiani C, Collura S, Sevini F, et al. Circulating miR-122-5p, miR-92a-3p, and miR-18a-5p as potential biomarkers in human liver transplantation follow-up. International Journal of Molecular Sciences. 2023; 24 (4):3457. Published 2023 Feb 9. DOI: 10.3390/ijms24043457 - 38.
Keshavarz Z, Zareei N, Afshari A, Karimi MH, Yaghobi R, Malekhosseini SA. TLR2 and TLR4 mRNA expression levels in liver transplant patients with acute rejection. Immunobiology. 2021; 226 (4):152107. DOI: 10.1016/j.imbio.2021.152107 - 39.
McClure T, Goh SK, Cox D, Muralidharan V, Dobrovic A, Testro AG. Donor-specific cell-free DNA as a biomarker in liver transplantation: A review. World Journal of Transplantation. 2020; 10 (11):307-319. DOI: 10.5500/wjt.v10.i11.307 - 40.
Huang A, Guo DZ, Zhang X, et al. Serial circulating tumor DNA profiling predicts tumor recurrence after liver transplantation for liver cancer. Hepatology International. Published online November; 2023; 18 :254-264. DOI: 10.1007/s12072-023-10594-x - 41.
Wehrle CJ, Raj R, Aykun N, et al. Liquid biopsy by ctDNA in liver transplantation for colorectal cancer liver metastasis. Journal of Gastrointestinal Surgery. 2023; 27 (7):1498-1509. DOI: 10.1007/s11605-023-05723-8 - 42.
Avramidou E, Vasileiadou S, Antoniadis N, Katsanos G, Kofinas A, Karakasi K-E, et al. Liver transplantation and dd-cfDNA: A small solution for a big problem. Liver. 2023; 3 (1):76-81. DOI: 10.3390/livers3010007 - 43.
Fernández-Galán E, Badenas C, Fondevila C, Jiménez W, Navasa M, Puig-Butillé JA, et al. Monitoring of donor-derived cell-free DNA by short tandem repeats: Concentration of Total cell-free DNA and fragment size for acute rejection risk assessment in liver transplantation. Liver Transplantation. 2022; 28 (2):257-268. DOI: 10.1002/lt.26272 - 44.
Sigdel TK, Vitalone MJ, Tran TQ , et al. A rapid noninvasive assay for the detection of renal transplant injury. Transplantation. 2013; 96 (1):97-101. DOI: 10.1097/TP.0b013e318295ee5a - 45.
Grskovic M, Hiller DJ, Eubank LA, et al. Validation of a clinical-grade assay to measure donor-derived cell-free DNA in solid organ transplant recipients. The Journal of Molecular Diagnostics. 2016; 18 (6):890-902. DOI: 10.1016/j.jmoldx.2016.07.003 - 46.
Kueng N, Arcioni S, Sandberg F, et al. Comparison of methods for donor-derived cell-free DNA quantification in plasma and urine from solid organ transplant recipients. Frontiers in Genetics. 2023; 14 :1089830. Published 2023 Jan 27. DOI: 10.3389/fgene.2023.1089830 - 47.
Ng HI et al. Analysis of fragment size distribution of cell-free DNA: A potential non-invasive marker to monitor graft damage in living-related liver transplantation for inborn errors of metabolism. Molecular Genetics and Metabolism. 2019; 127 (1):45-50. DOI: 10.1016/j.ymgme.2019.03.004 - 48.
Lewis D et al. High levels of donor-derived cell-free DNA in a case of graft-versus-host-disease following liver transplantation. American Journal of Transplantation. 2022b; 22 (3):973-976. DOI: 10.1111/ajt.16894 - 49.
Altuğ Y, Liang N, Ram R, et al. Analytical validation of a single-nucleotide polymorphism-based donor-derived cell-free DNA assay for detecting rejection in kidney transplant patients. Transplantation. 2019; 103 (12):2657-2665. DOI: 10.1097/TP.0000000000002665 - 50.
Baumann AK, Beck J, Kirchner T, Hartleben B, Schütz E, Oellerich M, et al. Elevated fractional donor-derived cell-free DNA during subclinical graft injury after liver transplantation. Liver Transplantation. 2022; 28 (12):1911-1919. DOI: 10.1002/lt.26479 - 51.
Lehmann-Werman R, Magenheim J, Moss J, et al. Monitoring liver damage using hepatocyte-specific methylation markers in cell-free circulating DNA. JCI. Insight. 2018; 3 (12):e120687. Published 2018 Jun 21. DOI: 10.1172/jci.insight.120687 - 52.
Londoño M-C et al. Molecular profiling of subclinical inflammatory lesions in long-term surviving adult liver transplant recipients. Journal of Hepatology. 2018; 69 (3):626-634. DOI: 10.1016/j.jhep.2018.04.012 - 53.
Saunders EA et al. Outcome and safety of a surveillance biopsy guided personalized immunosuppression program after liver transplantation. American Journal of Transplantation. 2022; 22 (2):519-531. DOI: 10.1111/ajt.16817 - 54.
Schütz E et al. Graft-derived cell-free DNA, a noninvasive early rejection and graft damage marker in liver transplantation: A prospective, observational, Multicenter cohort study. PLoS Medicine. 2017; 14 (4):e1002286. DOI: 10.1371/journal.pmed.1002286 - 55.
Oellerich M, Schütz E, Kanzow P, Schmitz J, Beck J, Kollmar O, et al. Use of graft-derived cell-free DNA as an organ integrity biomarker to Reexamine effective tacrolimus trough concentrations after liver transplantation. Therapeutic Drug Monitoring. 2014; 36 (2):136-140. DOI: 10.1097/FTD.0000000000000044 - 56.
Höfer A, Jonigk D, Hartleben B, et al. Non-invasive screening for subclinical liver graft injury in adults via donor-specific anti-HLA antibodies. Scientific Reports. 2020; 10 :14242. DOI: 10.1038/s41598-020-70938-7 - 57.
Kanamori H, Yamada Y, Ito Y, et al. Noninvasive graft monitoring using donor-derived cell-free DNA in Japanese liver transplantation. Hepatology Research. 2024; 54 (3):300-314. DOI: 10.1111/hepr.13978 - 58.
Taylor AL, Gibbs P, Sudhindran S, Key T, Goodman RS, Morgan CH, et al. Monitoring systemic donor lymphocyte macrochimerism to aid the diagnosis of graftversus-host disease after liver transplantation. Transplantation. 2004; 77 (3):441-445. DOI: 10.1097/01.TP.0000103721.29729.FE - 59.
Cox DRA, McClure T, Zhang F, et al. Graft-derived cell-free DNA quantification following liver transplantation using tissue-specific DNA methylation and donor-specific genotyping techniques: An orthogonal comparison study. Epigenomes. 2023; 7 (2):11. Published 2023 Jun 9. DOI: 10.3390/epigenomes7020011 - 60.
Hülsdünker J, Zeiser R. Insights into the pathogenesis of gvhd: What mice can teach us about man. Tissue Antigens. 2014; 85 (1):2-9. DOI: 10.1111/tan.12497 - 61.
Taylor AL, Gibbs P, Bradley JA. Acute graft versus host disease following liver transplantation: The enemy within. American Journal of Transplantation. 2004; 4 (4):466-474. DOI: 10.1111/j.1600-6143.2004.00406.x - 62.
Oellerich M, Walson PD, Beck J, Schmitz J, Kollmar O, Schütz E. Graft-derived cell-free DNA as a marker of transplant graft injury. Therapeutic Drug Monitoring. 2016; 38 (Suppl. 1):S75-S79. DOI: 10.1097/FTD.0000000000000239 - 63.
Zhao D, Zhou T, Luo Y, et al. Preliminary clinical experience applying donor-derived cell-free DNA to discern rejection in pediatric liver transplant recipients. Scientific Reports. 2021; 11 :1138. DOI: 10.1038/s41598-020-80845-6 - 64.
Abdelrahim M, Esmail A, Abudayyeh A, et al. Transplant oncology: An emerging discipline of cancer treatment. Cancers (Basel). 2023; 15 (22):5337. Published 2023 Nov 9. DOI: 10.3390/cancers15225337 - 65.
Xu X, Lu D, Ling Q , et al. Liver transplantation for hepatocellular carcinoma beyond the Milan criteria. Gut. 2016; 65 (6):1035-1041. DOI: 10.1136/gutjnl-2014-308513 - 66.
Mazzaferro V, Regalia E, Doci R, et al. Liver transplantation for the treatment of small hepatocellular carcinomas in patients with cirrhosis. The New England Journal of Medicine. 1996; 334 (11):693-699. DOI: 10.1056/NEJM199603143341104 - 67.
Eletta OA, Panayotova GG, Lunsford KE. Liver transplant for intrahepatic Cholangiocarcinoma. The Surgical Clinics of North America. 2024; 104 (1):215-225. DOI: 10.1016/j.suc.2023.07.006 - 68.
Filgueira NA. Hepatocellular carcinoma recurrence after liver transplantation: Risk factors, screening and clinical presentation. World Journal of Hepatology. 2019; 11 (3):261-272. DOI: 10.4254/wjh.v11.i3.261 - 69.
Luo B, Ma F, Liu H, et al. Cell-free DNA methylation markers for differential diagnosis of hepatocellular carcinoma. BMC Medicine. 2022; 20 (1):8. Published 2022 Jan 14. DOI: 10.1186/s12916-021-02201-3 - 70.
Zhang X, Wang Z, Tang W, et al. Ultrasensitive and affordable assay for early detection of primary liver cancer using plasma cell-free DNA fragmentomics. Hepatology. 2022; 76 (2):317-329. DOI: 10.1002/hep.32308 - 71.
Ng CKY, Di Costanzo GG, Terracciano LM, Piscuoglio S. Circulating cell-free DNA in hepatocellular carcinoma: Current insights and outlook. Frontiers in Medicine (Lausanne). 2018; 5 :78. Published 2018 Mar 26. DOI: 10.3389/fmed.2018.00078 - 72.
Lu CY, Chen SY, Peng HL, Kan PY, Chang WC, Yen CJ. Cell-free methylation markers with diagnostic and prognostic potential in hepatocellular carcinoma. Oncotarget. 2017; 8 (4):6406-6418. DOI: 10.18632/oncotarget.14115 - 73.
Zhou C, Weng J, Liu S, et al. Whole-exome sequencing reveals the metastatic potential of hepatocellular carcinoma from the perspective of tumor and circulating tumor DNA. Hepatology International. 2023; 17 (6):1461-1476. DOI: 10.1007/s12072-023-10540-x - 74.
Bae M, Kim G, Lee TR, et al. Integrative modeling of tumor genomes and epigenomes for enhanced cancer diagnosis by cell-free DNA. Nature Communications. 2023, 2017. Published 2023 Apr 10; 14 (1). Article number: 2017 (2023). DOI: 10.1038/s41467-023-37768-3 - 75.
Zhu GQ , Liu WR, Tang Z, et al. Serial circulating tumor DNA to predict early recurrence in patients with hepatocellular carcinoma: A prospective study. Molecular Oncology. 2022; 16 (2):549-561. DOI: 10.1002/1878-0261.13105 - 76.
Manzi J, Hoff CO, Ferreira R, et al. Cell-free DNA as a surveillance tool for hepatocellular carcinoma patients after liver transplant. Cancers (Basel). 2023; 15 (12):3165. Published 2023 Jun 13. DOI: 10.3390/cancers15123165 - 77.
Reddy T, Esmail A, Chang JC, Ghobrial RM, Abdelrahim M. Utility of cell-free DNA detection in transplant oncology. Cancers (Basel). 2022; 14 (3):743. DOI: 10.3390/cancers14030743 - 78.
Wang J, Huang A, Wang YP, et al. Circulating tumor DNA correlates with microvascular invasion and predicts tumor recurrence of hepatocellular carcinoma. Annals of Translational Medicine. 2020; 8 (5):237. DOI: 10.21037/atm.2019.12.154 - 79.
Oellerich M, Shipkova M, Asendorf T, et al. Absolute quantification of donor-derived cell-free DNA as a marker of rejection and graft injury in kidney transplantation: Results from a prospective observational study. American Journal of Transplantation. 2019; 19 (11):3087-3099. DOI: 10.1111/ajt.15416 - 80.
Oellerich M, Budde K, Osmanodja B, et al. Donor-derived cell-free DNA for personalized immunosuppression in renal transplantation. Therapeutic Drug Monitoring. 2023; 45 (1):20-25. DOI: 10.1097/FTD.0000000000001023 - 81.
Boonpheng B, De Castro ICC, Ng YH, et al. Tocilizumab for treatment of chronic active antibody-mediated rejection in kidney transplant recipients. Clinical Transplantation. 2023; 37 (5):e14936. DOI: 10.1111/ctr.14936 - 82.
Osmanodja B et al. Donor-derived cell-free DNA for kidney allograft surveillance after conversion to belatacept: Prospective pilot study. Journal of Clinical Medicine. 2023; 12 (6):2437. DOI: 10.3390/jcm12062437 - 83.
Kanzow P, Kollmar O, Schütz E, Oellerich M, Schmitz J, Beck J, et al. Graft-derived cell-free DNA as an early organ integrity biomarker after transplantation of a marginal HELLP syndrome donor liver. Transplantation. 2014; 98 (5):e43-e45. DOI: 10.1097/TP.0000000000000303 - 84.
Oellerich M et al. Donor-derived cell-free DNA as a diagnostic tool in transplantation. Frontiers in Genetics. 2022; 13 :1031894. DOI: 10.3389/fgene.2022.1031894 - 85.
Ng H-I, Sun L-Y, Zhu Z-J. Detecting graft-derived cell-free DNA through amplification refractory mutation system polymerase chain reaction in living-donor liver transplantation: Report of 2 cases. Transplantation Proceedings. 2019; 51 (3):820-822. DOI: 10.1016/j.transproceed.2018.11.011 - 86.
Da Silva S, Richard X, Weber A, Dutkowski P, Clavien P-A. Machine perfusion in liver transplantation. Hepatology. 2022; 76 (5):1531-1549. DOI: 10.1002/hep.32546 - 87.
Mojtabanezhad Shariatpanahi A, Rokni P, Shahabi E, et al. Simple and cost-effective laboratory methods to evaluate and validate cell-free DNA isolation. BMC Research Notes. 2018; 11 :757. DOI: 10.1186/s13104-018-3866-8 - 88.
Mauger F et al. Comprehensive evaluation of methods to isolate, quantify, and characterize circulating cell-free DNA from small volumes of plasma. Analytical and Bioanalytical Chemistry. 2015; 407 (22):6873-6878. DOI: 10.1007/s00216-015-8846-4