Open Access is an initiative that aims to make scientific research freely available to all. To date our community has made over 100 million downloads. It’s based on principles of collaboration, unobstructed discovery, and, most importantly, scientific progression. As PhD students, we found it difficult to access the research we needed, so we decided to create a new Open Access publisher that levels the playing field for scientists across the world. How? By making research easy to access, and puts the academic needs of the researchers before the business interests of publishers.
We are a community of more than 103,000 authors and editors from 3,291 institutions spanning 160 countries, including Nobel Prize winners and some of the world’s most-cited researchers. Publishing on IntechOpen allows authors to earn citations and find new collaborators, meaning more people see your work not only from your own field of study, but from other related fields too.
The purpose of this chapter is to provide healthcare professionals, researchers and caregivers with insights on persistent somatic symptoms afflicting cancer survivors. These symptoms, including pain, fatigue, gastrointestinal distress, sexual dysfunction, respiratory issues, and cardiovascular, neurological and musculoskeletal complications often endure long after treatment completion, negatively impacting quality of life. Certain populations like childhood cancer survivors and those receiving intensive chemotherapy have higher somatic symptom burden. Possible mechanisms include accelerated aging, somatization tendencies, treatment side effects, mood disorders, and comorbidities. Assessing patient-reported outcomes and screening tools can facilitate early detection and management. Treatment strategies encompass pharmacological and nonpharmacological modalities targeting specific symptoms. Overall somatic symptom burden correlates with psychological distress and disability among survivors. Tailored, patient-centric rehabilitation programs over the cancer trajectory, from pretreatment through long-term survivorship, can mitigate symptoms. More research on persistent somatic complications is warranted to optimize evidence-based care for survivors’ multifaceted needs.
Department of Psychiatry, University of Missouri Kansas City School of Medicine, Kansas City, MO, USA
*Address all correspondence to: val.bellmanmd@gmail.com
1. Introduction
Imagine a cancer survivor, who, after undergoing rigorous treatments and conquering the disease, finds themself grappling with unexplained physical symptoms that persist long after their remission. Despite their triumph over cancer, they feel trapped in the shadows of persistent somatic symptoms, impacting their daily life. Unfortunately, this experience is not unique, as many cancer survivors face similar challenges even after their battle with the disease has ended. In this chapter, we delve into the often-overlooked aspect of persistent somatic symptoms in individuals who have emerged victorious against cancer. Survivors often face a range of physical, psychological, and emotional challenges that can persist long after treatment ends. These symptoms, which can manifest in various forms and intensities, significantly impact survivors’ daily functioning and overall quality of life.
By shedding light on this topic, we aim to provide healthcare professionals, researchers, and caregivers with valuable insights and evidence-based approaches to alleviate suffering and improve the lives of cancer survivors.
To ensure the depth and accuracy of our findings, we conducted a meticulous review of the existing literature on persistent somatic symptoms in cancer survivors. By examining a wide array of studies, we aim to present a comprehensive synthesis of current knowledge and identify gaps that warrant further investigation.
2. Prevalence and impact of persistent somatic symptoms in cancer survivors
Persistent somatic symptoms can substantially impact cancer survivors’ quality of life and well-being. These symptoms encompass physical and psychological issues like pain, fatigue, anxiety, depression, and sleep problems [1, 2, 3]. Long-term rare cancer survivors commonly report tiredness/lack of energy as the most prevalent and bothersome symptom [3]. Emotional distress symptoms like depression, anxiety, and somatization are common in childhood cancer survivors [4]. Notably, symptoms can persist long-term after treatment as late effects of cancer or therapy [5]. Comorbidities strongly predict early mortality in survivors [6]. Studies consistently link somatic symptom severity and frequency to fear of recurrence in childhood cancer survivors [7]. Symptom burden profoundly impacts health-related quality of life; survivors with high physical, somatic and psychological symptoms report remarkably poor physical and mental quality of life [8]. Somatic symptoms are associated with disability and increased healthcare use in cancer patients with pain/depression [9].
The prevalence and persistence of these symptoms can vary based on factors such as age, comorbidity, race, and cancer type. For instance, older breast cancer survivors commonly report symptoms such as cardiotoxic effects, peripheral neuropathy, cognitive problems, fatigue, anxiety, depression, and sleep disturbances [1]. Similarly, racial and ethnic disparities have been observed in the physical and mental health outcomes of cancer survivors, with Black, Hispanic, and Indigenous survivors experiencing poorer health outcomes [10]. Moreover, sexual orientation and racial/ethnic differences have been found to influence the physical and mental health outcomes of female and male cancer survivors [11]. For example, prostate cancer survivors with high symptom burden require more supportive information and tailored long-term survivorship care to address their needs effectively [12].
2.1 Factors contributing to higher risk of persistent somatic symptoms in certain survivor populations
Research suggests childhood cancer survivors may experience premature aging, potentially due to cancer therapy exposure leading to cellular senescence, reduced telomere length, epigenetic changes, somatic mutations, and mitochondrial DNA issues [13]. Biological pathways likely explain the occurrence of psychosomatic symptoms like pain, fatigue, and weakness in conditions such as somatization, depression, and chronic fatigue [14]. In cancer, somatization manifests as somatic symptoms including pain, fatigue, appetite changes, and low energy [15]. Minor bodily symptoms may be cognitively linked to fear of recurrence, influencing survivors’ well-being [16].
All survivors have poorer psychological health than cancer-free individuals, emphasizing the psychological impact of survivorship [17]. Childhood leukemia, Hodgkin’s disease, and lymphoma survivors who had intensive chemotherapy have an increased risk of depression and somatic distress [18]. Factors like female sex, low education, income, and unemployment are associated with increased physical distress in childhood cancer survivors [19]. Psychological distress persists in 20–40% of survivors, highlighting its enduring impact [20]. Long-term psychoactive drug use is associated with more somatic symptoms in psychiatric patients [21]. Worsening physical health, pain, and ending analgesics predict persistent distress in survivors [22]. Table 1 summarizes somatization aspects in survivors.
Factor
Description
Reference
High Prevalence
The manifestation of psychological distress through physical symptoms is a significant concern among 50% of cancer survivors.
3. Characteristics of persistent somatic symptoms in cancer survivors
Somatic symptoms are prevalent among cancer survivors. These symptoms include pain, fatigue, anxiety, depression, and somatic distress. Cunningham et al. highlighted that somatic symptoms, such as pain and fatigue, are common after childhood cancer and are associated with greater fear of cancer recurrence and poorer health-related quality of life [7]. Moreover, Heathcote et al. emphasized the prevalence and burden of somatic symptoms, particularly pain and fatigue, in adult survivors of childhood cancer [28]. Tuman et al. also found that breast cancer survivors with a tendency to make threatening interpretations experienced overall problematic somatic symptoms [29]. Furthermore, fear of cancer recurrence has been linked to somatic symptoms and perceived stress among cancer survivors [30].
3.1 Chronic pain in cancer survivors
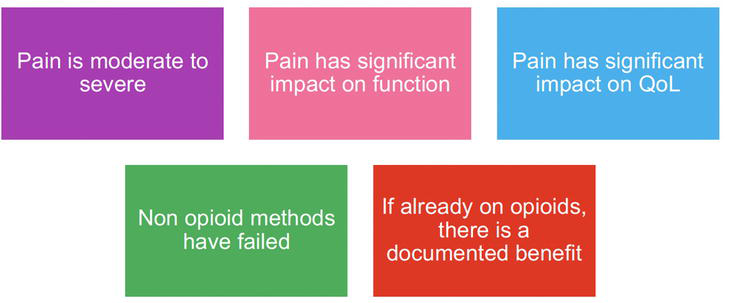
Chronic pain is a common issue among cancer survivors, significantly impacting their daily functioning [31]. Studies have shown that chronic pain is prevalent and disabling, affecting a substantial proportion of cancer survivors [32]. Pain is one of the most distressing symptoms experienced by cancer survivors, with a notable impact on their quality of life [33]. However, there is a lack of recognition among clinicians regarding the frequency of chronic pain in this population, which may lead to underestimation of its prevalence and severity [34, 35]. Therefore, tailored policies, guidelines, and comprehensive training for healthcare professionals in pain management are necessary to address the complexity of chronic pain in cancer survivors [36]. The management of pain in cancer survivors presents various challenges, including social and demographic inequalities in barriers to cancer pain management [37]. The use of opioids in cancer survivors with chronic pain raises concerns, and advanced therapeutic strategies may be necessary to ensure prolonged pain control [38]. Figure 1 summarizes the most common indications for opiates in this population.
Figure 1.
Indications for opioids in cancer survivors.
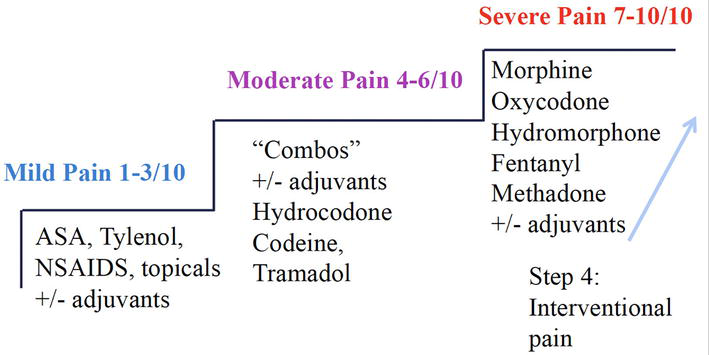
Additionally, cancer-specific psychosocial factors, such as pain catastrophizing and multisite pain, contribute to the pain experience in cancer survivors [39]. Healthcare professionals must manage the needs of cancer survivors in a manner that acknowledges the burden of pain in the context of other symptoms and morbidities experienced by long-term survivors [40]. Various interventions have been explored to address chronic pain in cancer survivors, including acupuncture, cognitive behavioral therapy, and breathing exercises, with some evidence of positive effects for pain relief [41, 42]. Moreover, the evaluation of medications and self-management techniques for controlling neuropathic symptoms in cancer survivors highlights the multifaceted approach required to address the complexities of pain management in this population [43]. Figure 2 summarizes pharmacological pain management in this population.
Figure 2.
World Health Organization (WHO) step ladder approach.
3.2 Chronic fatigue in cancer survivors
The prevalence of moderate to severe fatigue among cancer survivors has been reported to be as high as 66.1%, with a significant impact on their quality of life [44]. Studies have shown that fatigue is prevalent not only in breast cancer survivors but also in survivors of lung, colorectal, prostate, and other types of cancer [45]. Table 2 summarizes various instruments to screen or measure fatigue.
Screening Tool
Description
Brief Screening Tools
VAS 0–10 scales
Multi-symptom screening scales: ESAS, MSAS
Unidimensional Scales (physical impact of CRF)
Functional Assessment of Cancer Therapy Fatigue (FACT-F)
Diagnosis if six or more of the following symptoms are present daily or nearly daily during same 2 weeks in past month and at least one of symptoms is significant fatigue:
fatigue (diminished energy, increased need to rest disproportionate to
change in activity)
generalized weakness, limb heaviness
diminished concentration, attention
decreased motivation, interest in activities
insomnia, hypersomnia
non-restorative sleep
struggle to overcome inactivity
emotional reactivity to feeling fatigued (sadness, frustration, irritability)
difficulty with daily tasks because of fatigue
short-term memory problems
post-exertional malaise lasting several hours
Symptoms cause clinically significant distress or
impairment in social, occupational, or other important
areas of functioning
Evidence from history, physical examination, or
laboratory findings that symptoms are consequence of
cancer or cancer therapy
Symptoms not primarily consequence of comorbid
psychiatric disorders such as major depression,
somatization or somatoform disorder, or delirium
Table 2.
Screening for chronic fatigue syndrome.
ESAS: The Edmonton Symptom Assessment System.
VAS: Visual Analogue Scale.
MSAS: The Memorial Symptom Assessment Scale.
EORTC QLQ-C30: The EORTC Core Quality of Life questionnaire.
Furthermore, fatigue has been found to co-occur with other symptoms such as depression, insomnia, neuropathy, and pain, contributing to the overall burden experienced by cancer survivors [46]. It has also been noted that fatigue may persist for months after the completion of cancer treatment, affecting 30–60% of cancer survivors [47]. Table 3 summarizes possible underlying mechanisms behind chronic fatigue in cancer survivors.
Psychogenic
Organic disease
Mostly <6 months and fluctuates in severity
6 months
Related to various stressors
Obvious psychosocial sctressors are often absent
Sleeping disturbance with either insomnia or eary morning awakening
Varies. May be present but often related to the underlying illness
Worse in the morning, may be alleviated by activity
Less in the morning and worsened with activity
Multiple and nonspecific complaints along with a normal exam
Fewer and more specific symptoms. Exam may suggest potential underlying problem
Table 3.
Ethnology of cancer fatigue.
Furthermore, chronic fatigue has been found to be strongly associated with depression in cancer survivors, indicating a potential interplay between these two conditions [48]. While both fatigue and depression are prevalent among cancer survivors, it is essential to differentiate between these two conditions. Table 4 summarizes core findings and differences.
Chronic fatigue in cancer survivors
Depression in cancer survivors
Fatigue much more common than depression (60–90% vs. 20–25%)
Depression more likely in presence of
hopelessness, worthlessness, guilt
history or family history of depression
Depressive symptoms due to fatigue are often less severe and are attributed to consequences of fatigue by patients
Suicidal ideations, desire for death are not common in patients with fatigue
Table 4.
Fatigue and depression in cancer survivors.
The management of fatigue in cancer survivors is a complex challenge, as there is currently no somatic strategy specifically tailored to address this issue [49]. Furthermore, the experience of chronic fatigue post-treatment can have a profound impact on the family and social dynamics of cancer survivors [50]. Table 5 summarizes the main treatment strategies.
Interventions for Fatigue
Description
Depression treatment
Typical antidepressants
selective serotonin reuptake inhibitors (SSRIs) may be better tolerated than others
bupropion may be more activating (similar in structure to stimulants)
3.3 Impact of cognitive impairment on somatic symptoms in cancer survivors
Research has shown that long-term survivors are at risk for neurocognitive impairment due to multiple sources of risk [54]. The lack of information regarding cognitive impairment has been found to negatively impact the work and work capacity of cancer survivors [55]. Chemotherapy has been implicated in cognitive abnormalities in cancer survivors, including impairments of memory, attention, processing speed, and executive function [56]. Moreover, aging cancer survivors may report new-onset neurocognitive impairments, and there is a need to identify risk factors associated with such impairments [57]. Table 6 outlines assessment and diagnosis of cognitive impairment in cancer survivors.
History
Time course of cognitive decline (correlation with cancer, chemo, hospitalization)
Fluctuations/Sleep wake cycle
Assess for pain and discomfort
Cognitive, functional, behavioral history (current and baseline) with collateral from family and caregivers
h/o delirium or dementia, seizures, falls, h/o ICU stay
Medication list/ chemotherapy or other cancer therapies
ETOH, benzodiazepines
Vascular risk factors
Family history of neurodegenerative disorders
Examination
Mental Status Examination and cognitive/neuropsychological testing
Assessment of cognitive impairment in cancer survivors.
Cognitive rehabilitation has been proposed as a potential intervention, as concerns about impaired cognition are one of the most frequently reported post-treatment symptoms in cancer survivors [58]. Physical activity has been associated with better neurocognitive function in cancer survivors, suggesting a potential avenue for intervention [59]. The National Comprehensive Cancer Network recommends pharmacologic interventions as a last line of therapy:
Table 7 summarizes neuromodulation strategies utilized in cancer survivors.
Strategy
Description
Neurofeedback
Promising results in breast cancer patients.
Repetitive transcranial magnetic stimulation
Currently, no studies in cancer patients.
Transcranial Direct Current Stimulation
Non-invasive brain stimulation technology
Studied in patients with depression, pain syndromes, stroke, Alzheimer’s, and Parkinson’s disease in non-cancer settings with promising clinical evidence.
Table 7.
Neuromodulation strategies for cognitive difficulties in survivorship.
3.4 Impact of sleep disorders on somatic symptoms in survivors
Sleep disorders and somatic symptoms are prevalent among cancer survivors, impacting their quality of life and psychological well-being. Statistically, sleep medication use is prevalent among cancer survivors, with the prevalence of insomnia symptoms being nearly 40% in this population [60]. Research indicates that adult survivors of childhood cancer are more likely to experience fatigue, sleep disturbance, and daytime sleepiness [61]. For instance, a study by Schlarb et al. found that self-reported sleep quality, sleep onset latency, sleep disturbances, use of sleep medications, and daytime dysfunctioning were significant predictors of somatoform syndrome, while sleep efficiency and sleep duration indirectly influenced somatic complaints [62]. Insomnia severity is directly related to habitual somatic complaints and pain intensity [63]. Similarly, Sun et al. indicated that a high level of somatic symptoms exacerbates the adverse effects on sleep disturbance, emphasizing the bidirectional nature of the relationship [64]. Table 8 summarizes general principles and interventions in cancer patients and survivors with sleep problems.
Intervention
Characteristics
Nonpharmacological Interventions
Cognitive-behavioral therapy for insomnia (CBT-I) (+) strong evidence in cancer patients with therapeutic effects maintained long term.
Exercise Interventions: regular aerobic exercises, even of different durations and
weekly volumes, benefits patient sleep quality.
Pharmacological Interventions
The American Academy of Sleep Medicine does not recommend sleep medications for longer than 4 weeks.
The NCCN Survivorship Guidelines recommends assessment every 1 to 3 months to determine ongoing need for medications.
All medications have been shown to be more effective than placebo at improving short-term sleep outcomes in the general population.
The potential benefits of pharmacologic therapy on sleep quality and daytime function are balanced against the risk of side effects and dependence with long-term use.
Table 8.
Management of sleep difficulties in cancer survivors.
3.5 Sexual dysfunction in cancer survivors
Research shows sexual dysfunction is a prevalent issue among cancer survivors, especially childhood and young adult survivors. A review highlighted adolescent and young adult survivors experience substantial sexual dysfunction [65]. Another review identified the prevalence and risk factors for sexual dysfunction in childhood cancer survivors, emphasizing its link to quality of life and psychosocial outcomes [18]. Studies show childhood cancer survivors may experience sexual difficulties and delays in milestones due to the cancer’s impact on psychosexual development [66]. Sexual dysfunction is prevalent among female childhood cancer survivors, significantly impacting their psychosexual functioning [67]. There is an increased risk of sexual dysfunction in young adult survivors of childhood cancer, indicating a need for support in this population [68]. Another study emphasized the lack of information on sexual health for male childhood cancer survivors, showing further research and support is needed [69]. Standardized nursing care interventions reduced sexual dysfunction in cervical cancer survivors, underscoring potential benefits of targeted interventions [70]. These findings demonstrate sexual dysfunction is a common issue among survivors that interventions may help address. Table 9 summarizes NCCN guidelines regarding sexual dysfunction.
ASK
About sexual function at regular intervals
ASSESS
Using the Brief Sexual Symptom Checklist as a primary screening tool
REVIEW
Present and past sexual history and sexual concerns
DISCUSS
How cancer treatment has affected sexual functioning, intimacy, treatment-associated infertility and, if indicated, provide appropriate referrals
DIRECT
Patients to needed resources
Table 9.
Guidelines of sexual dysfunction.
3.6 Weight loss in cancer survivors
Weight loss and poor appetite are significant concerns among cancer patients and survivors. Another study highlighted that intermittent claudication and appetite loss are common among breast cancer survivors and are associated with cardiac dysfunction and mood disorders [71]. Similarly, it was found that self-reported distress among older cancer survivors was associated with weight change and poor appetite [72]. Additionally, identified appetite changes as one of the indicators of physical wellbeing in cancer survivors, emphasizing its impact on quality of life [73]. Table 10 summarizes the differences between starvation and cancer/post-treatment weight loss.
Starvation
Cancer/Post-Treatment Weight Loss
Loss of adipose tissue
Loss of fat and lean muscles
Hunger is present, significant
No hunger, no concerns about food
Decreased resting energy
Increased resting energy expenditure
No specific mediators or markers
Pro-inflammatory cytokines
Table 10.
Weight and appetite loss and cancer cachexia.
Furthermore, emphasized the consequences of weight loss for cancer survivors as a crucial issue in survivorship research, highlighting the need for interventions to address this concern [74]. Other authors also identified appetite loss as a part of a cluster of symptoms in breast cancer survivors, indicating its impact on their quality of life [75]. Research highlighted the importance of maintaining a healthy weight for cancer survivors, emphasizing the potential benefits for their overall well-being [76]. In addition, weight loss interventions have been studied in the context of cancer survivorship. Reported that behaviorally based weight loss interventions for breast cancer survivors resulted in significant weight losses, indicating the potential effectiveness of such interventions. Table 11 summarizes pharmacological and nonpharmacological management of cancer and post-treatment weight loss in cancer survivors.
Strategy
Description
Counseling
The nutritional counseling: liberalizing diet restrictions, encouraging patients to eat frequent small meals with preferably the bulk of calorie intake occurring in the morning.
Nonpharmacological Management
Ensuring sufficient energy and protein intake (nutritional support, consultation with a nutritionist)
Maintaining body weight, physical activity and muscle mass (exercise, PT)
Pharmacological Management
Appetite Stimulants
corticosteroids, cannabinoids, progesterone analogs, and serotonin modulators (olanzapine, mirtazapine).
Anabolic Agents
anabolic steroids
Growth hormone, ghrelin analogs
Cytokine and metabolic inhibitors
Eicosapentaenoic acid
Thalidomide
Table 11.
Weight and appetite loss management.
3.7 Gastrointestinal distress in cancer survivors
Nausea and vomiting are very common in cancer patients, including survivors. Research shows 70–80% of chemotherapy patients experience these symptoms [77], which continue into survivorship and hurt quality of life [78]. Over 60% of terminally ill patients have nausea and vomiting in their last 6 weeks [79]. Managing these symptoms is crucial for survivors’ wellbeing. Studies suggest high protein intake can lessen nausea and vomiting [80]. Acupressure has been explored to treat chemotherapy-induced nausea and vomiting [81]. Aromatherapy with ginger may alleviate nausea and vomiting after cervical cancer chemotherapy [82].
Constipation and diarrhea persist as major issues for survivors versus healthy controls [83]. More extreme gastrointestinal symptoms correlate with poorer physical and mental health [84]. Colorectal cancer survivors specifically reported high levels of constipation and diarrhea [85]. Physical activity improved diarrhea in prostate cancer survivors [86]. Exercise motivation plans and doctor recommendations together could raise exercise levels in breast and colorectal survivors, potentially improving constipation and diarrhea [87]. Beyond exercise, dietary changes and probiotics have been explored. One study promoted exercise and avoiding sedentary lifestyles for breast cancer survivors [88]. Probiotics during or after cancer treatment may alleviate certain gastrointestinal issues like diarrhea and abdominal pain [89].
3.8 Cardiovascular complications and symptoms in cancer survivors
Cardiovascular complications are a major concern for cancer survivors, as they continue facing increased risk of death from cardiovascular problems after remission or cure [90]. Understanding the mechanisms and diagnostic strategies with risk prediction is key to preventing cardiovascular issues in patients and survivors [91]. Additionally, acquiring modifiable cardiovascular risk factors, especially hypertension, heightens the risk of severe, life-threatening, and fatal cardiac events in survivors, regardless of cancer treatment risks [92]. Long-term cardiovascular effects of cancer treatments like radiotherapy and chemotherapy are well-documented in adult survivors [93]. Furthermore, survivors have high cardiovascular disease risk, with those at risk having significantly higher mortality than those without risk [94]. Preexisting cardiovascular risks and older age associate with heart failure and other cardiovascular diseases in survivors, particularly those who had anthracyclines [95]. Notably, people diagnosed with highly survivable cancers are more likely to die from cardiovascular disease than cancer recurrence, yet cardiovascular risks may be overlooked during survivorship care [96]. This is especially concerning as many breast cancer survivors are more likely to die from cardiovascular disease than breast cancer [97]. Moreover, compared to the general population, survivors have increased risk of cardiovascular events, and the odds of several cardiovascular risk factors are higher among middle-aged survivors [98]. It’s estimated cardiovascular disease is the number one comorbidity in survivors and causes many non-cancer deaths among them [99]. Therefore, continuous monitoring and aggressive management of modifiable cardiovascular risks could reduce the cardiovascular burden in cancer survivors.
3.9 Other somatic problems
3.9.1 Osteopenia and osteoporosis in cancer survivors
Osteopenia and osteoporosis are significant concerns for cancer survivors, particularly for breast and prostate cancer survivors. Table 12 summarizes various mechanisms of bone loss in cancer survivors.
Etiology of bone loss in cancer patients and survivors.
While osteoporosis or osteopenia may seem insignificant compared to other long-term side effects, these disorders can significantly restrict a survivor’s lifestyle [100]. Research has shown that younger breast cancer survivors, especially those aged ≤ 50 years, with estrogen receptor-positive tumors, and those treated with aromatase inhibitors alone or chemotherapy plus any hormone therapy, are at a higher risk for osteopenia and osteoporosis compared to cancer-free women [101]. Adult cancer survivors, including those with childhood leukemia, are also at risk, with approximately 50% of patients having osteopenia or osteoporosis [102]. Similarly, cancer survivors are at risk of developing osteoporosis and osteopenia due to cancer treatment [103]. These conditions often do not produce clinical symptoms until a fracture occurs—commonly seen in the wrist, hip, and spine from minimal trauma that would not typically break a healthy bone. Spinal compression fractures in particular may generate severe back pain, height loss, protruding abdomen, and reduced mobility. More general symptoms can include bone pain, joint aches, and difficulty with walking or daily tasks. Early detection and treatment can reduce fracture risk and related disability.
3.9.2 Respiratory problems in cancer survivors
It is evident that respiratory problems are a significant concern among cancer survivors. Research suggests that childhood cancer survivors had significant excesses in respiratory mortality, including pneumonia, fibrosis, pneumonitis, and other respiratory deaths, with standardized mortality ratios ranging from 7-fold to 17-fold higher than expected [104]. Similarly, highlighted that survivors of childhood and young adult cancer remain at a significantly increased risk of respiratory complications several decades after treatment, emphasizing the importance of clinical initiatives for prevention, early detection, and treatment [105]. Furthermore, reported that adverse health effects, including respiratory infections, were statistically significantly increased in breast cancer survivors, indicating the long-term impact of cancer and its treatment on respiratory health [106]. Additionally, compared the incidence of pulmonary outcomes among cancer survivors and found an increased risk of pulmonary complications, such as asthma, chronic cough, emphysema, lung fibrosis, and recurrent pneumonia, emphasizing the need for ongoing monitoring and management of respiratory health in this population [61].
4. Non-pharmacological approaches to alleviate persistent somatic symptoms
4.1 Physical therapy and rehabilitation
Physical therapy and rehabilitation play a vital role in the care and recovery of cancer survivors. Research has shown that cancer survivors are highly motivated to seek information about physical activity and dietary choices to enhance their response to treatment, expedite recovery, and improve their quality of life [107]. Cancer rehabilitation is a process that helps survivors achieve and maintain the highest possible physical, social, psychological, and vocational functioning within the limits created by cancer and its treatments [108]. In fact, a study evaluating survivors of the 10 most prevalent cancers found that 63% reported the need for at least one rehabilitation service, with physical therapy being the most frequently reported need [109]. Furthermore, investment in oncology physical therapy and the development of international standards of care can allow physical therapists to meet the rehabilitation needs of cancer survivors [110]. Rehabilitation intervention may be required at multiple time points along the cancer continuum, from prior to treatment to the early rehabilitation and long-term survivorship phases post-treatment [111]. Additionally, rehabilitation and exercise have been found to be effective for treating physical functional decline and addressing symptoms across multiple domains and at multiple points along the cancer disease continuum. Moreover, physical activity programs are recommended as part of cancer rehabilitation services [112]. However, there are challenges in implementing physical activity and rehabilitation guidelines in routine primary care cancer rehabilitation, and exploring professionals’ perceptions and preparedness to implement these guidelines is essential [113]. Rehabilitation is recommended to help cancer survivors regain functional independence and mitigate subsequent disability [114]. Home exercise programs have been found to be a useful adjunct to physical therapy programs for treating arm and shoulder morbidities in cancer survivors. The American College of Sports Medicine and the American Cancer Society have recommended physical activity as an intervention strategy to help cancer survivors manage symptoms, improve quality of life, and possibly even extend survival [115].
Furthermore, during re-entry after cancer treatment, clinicians can educate survivors on the benefits of healthy behaviors [116]. This period after the primary treatment for cancer ends requires support care for patients having physical, psychological, and social readjustments, making rehabilitation services crucial [117].
4.2 Psychological interventions for somatic symptoms in cancer survivors
Psychological interventions are crucial for addressing the somatic symptoms experienced by cancer survivors. Research shows that cognitive behavioral therapy and physical activity interventions effectively improve quality of life in survivors [118]. Cancer and its treatments can significantly influence psychological well-being and cause distress later in life [24]. Childhood cancer survivors have an increased risk of depression and somatic distress, exacerbated by intensive chemotherapy [18]. Psychological interventions like mindfulness and therapy reduce cancer-related fatigue [26]. Over 35% of survivors experience depressive symptoms during survivorship. Distress manifests as depression, anxiety, PTSD, worry, or anger [27]. Support interventions reduce distress in prostate cancer survivors [25]. Psychosocial interventions increasingly promote resilience and meaning to improve well-being [119, 120]. Disparities in rural survivors’ mental health indicate a need to increase their access to services [121]. In summary, a range of psychological interventions are vital to address survivors’ somatic symptoms and improve their overall quality of life.
4.3 Integrative therapies for somatic symptoms in cancer survivors
The use of complementary and alternative medicine (CAM) in cancer survivors is widespread and increasing [122]. Certain survivors, like childhood cancer survivors, have high psychological distress, cognitive dysfunction, and poor quality of life [18, 123]. CAM use is high among survivors, but reasons behind use and communication with doctors are not well understood [124]. Many survivors report somatic symptoms and stress. Elderly survivors may have more symptoms, distress, and unhealthy lifestyles [27]. However, lung cancer survivors reported fewer daily somatic symptoms than other survivors [125]. Use of complementary therapies has significantly increased, suggesting survivors are interested in supplementing treatment [126]. Most breast cancer survivors use CAM at some point [127]. Adult survivors of pediatric cancer had more affective, somatic and comorbid symptoms than sibling controls [128]. Even long-term survivors use healthcare differently than community controls [129]. Survivors with pain levels similar to people without cancer still engage more in CAM [130]. In summary, CAM use is increasing in survivors and tied to various symptoms, but reasons behind use and impact need further research.
Persistent somatic symptoms are highly prevalent in cancer survivors, negatively affecting quality of life across physical, psychological and social domains. Common symptoms include pain, fatigue, sexual dysfunction, cognitive changes, cardiovascular/gastrointestinal issues, respiratory problems, and musculoskeletal disorders. Risk factors like childhood cancer and intensive treatment can worsen burden. Proposed mechanisms involve accelerated aging, somatization, mood disorders, treatment side effects, and physical/psychosocial comorbidities.
Careful assessment of patient-reported outcomes is vital for early detection and management of somatic symptoms. Both drug and non-drug approaches help alleviate persistent symptoms. Evidence-based, patient-centered rehabilitation programs implemented early and continued long-term can significantly mitigate symptoms and improve functioning.
I would like to express my sincere gratitude to the faculty members at the Department of Psychiatry, University of Missouri-Kansas City School of Medicine for their guidance and support. Finally, the experiences and struggles of cancer survivors battling persistent somatic and psychological symptoms were the motivation behind this review. I hope my work can positively impact survivorship care and that emerging research continues to alleviate suffering among those courageously recovering from cancer.
1.Mandelblatt JS, Zhai W, Ahn J, et al. Symptom burden among older breast cancer survivors: The thinking and living with cancer (TLC) study. Cancer. 2019;126:1183-1192
2.Mao J, Armstrong K, Bowman M, Xie S, Kadakia R, Farrar J. Symptom burden among cancer survivors: Impact of age and comorbidity. The Journal of the American Board of Family Medicine. 2007;20(5):434-443. DOI: 10.3122/jabfm.2007.05.060225
3.Horick N, Muzikansky A, Gutierrez H, Boyd K, Finkelstein D. Physical symptoms in long-term survivors of rare cancer. Journal of Cancer Survivorship. 2018;12(6):835-842. DOI: 10.1007/s11764-018-0721-9
4.D’Agostino N, Edelstein K, Zhang N, Recklitis C, Brinkman T, Srivastava D, et al. Comorbid symptoms of emotional distress in adult survivors of childhood cancer. Cancer. 2016;122(20):3215-3224. DOI: 10.1002/cncr.30171
5.Zucca A, Boyes A, Linden W, Girgis A. All’s well that ends well? Quality of life and physical symptom clusters in long-term cancer survivors across cancer types. Journal of Pain and Symptom Management. 2012;43(4):720-731. DOI: 10.1016/j.jpainsymman.2011.04.023
6.Leach C, Weaver K, Aziz N, Alfano C, Bellizzi K, Kent E, et al. The complex health profile of long-term cancer survivors: Prevalence and predictors of comorbid conditions. Journal of Cancer Survivorship. 2014;9(2):239-251. DOI: 10.1007/s11764-014-0403-1
7.Cunningham S, Patton M, Schulte F, Richardson P, Heathcote L. Worry about somatic symptoms as a sign of cancer recurrence: Prevalence and associations with fear of recurrence and quality of life in survivors of childhood cancer. Psycho-Oncology. 2021;30(7):1077-1085. DOI: 10.1002/pon.5647
8.Shin H, Dudley W, Bhakta N, Horan M, Wang Z, Bartlett T, et al. Associations of symptom clusters and health outcomes in adult survivors of childhood cancer: A report from the st jude lifetime cohort study. Journal of Clinical Oncology. 2023;41(3):497-507. DOI: 10.1200/jco.22.00361
9.Kroenke K, Zhong X, Theobald D, Wu J, Tu W, Carpenter J. Somatic symptoms in patients with cancer experiencing pain or depression. Archives of Internal Medicine. 2010;170(18):1686-1694. DOI: 10.1001/archinternmed.2010.337
10.Karvonen K, Balay-Dustrude E, Do A, Bradford M, Phipps A, Rosenberg A. Race, ethnicity, and experienced racism are associated with adverse physical and mental health outcomes among cancer survivors. Cancer. 2023;129(19):3023-3033. DOI: 10.1002/cncr.34913
11.Boehmer U, Jesdale B, Streed C, Agénor M. Intersectionality and cancer survivorship: Sexual orientation and racial/ethnic differences in physical and mental health outcomes among female and male cancer survivors. Cancer. 2021;128(2):284-291. DOI: 10.1002/cncr.33915
12.Bernat J, Wittman D, Hawley S, Hamstra D, Helfand A, Haggstrom D, et al. Symptom burden and information needs in prostate cancer survivors: A case for tailored long-term survivorship care. British Journal of Urology. 2015;118(3):372-378. DOI: 10.1111/bju.13329
13.Ness K, Kirkland J, Gramatges M, Wang Z, Kundu M, McCastlain K, et al. Premature physiologic aging as a paradigm for understanding increased risk of adverse health across the lifespan of survivors of childhood cancer. Journal of Clinical Oncology. 2018;36(21):2206-2215. DOI: 10.1200/jco.2017.76.7467
14.Anderson G, Berk M, Maes M. Biological phenotypes underpin the physio-somatic symptoms of somatization, depression, and chronic fatigue syndrome. Acta Psychiatrica Scandinavica. 2013;129(2):83-97. DOI: 10.1111/acps.12182
15.Chaturvedi S, Maguire G, Somashekar B. Somatization in cancer. International Review of Psychiatry. 2006;18(1):49-54. DOI: 10.1080/09540260500466881
16.Barrineau M, Zarit S, King H, Costanzo E, Almeida D. Daily well-being of cancer survivors: The role of somatic amplification. Psycho-Oncology. 2014;23(9):1027-1033. DOI: 10.1002/pon.3509
17.Michel G, Harju E, Dehler S, Roser K. The long-term impact of cancer: Evaluating psychological distress in adolescent and young adult cancer survivors in Switzerland. Psycho-Oncology. 2019;28(3):577-585. DOI: 10.1002/pon.4981
18.Zebrack B, Zeltzer L, Whitton J, Mertens A, Odom L, Berkow R, et al. Psychological outcomes in long-term survivors of childhood leukemia, hodgkin’s disease, and non-hodgkin’s lymphoma: A report from the childhood cancer survivor study. Pediatrics. 2002;110(1):42-52. DOI: 10.1542/peds.110.1.42
19.Burghardt J, Klein E, Brähler E, Ernst M, Schneider A, Eckerle S, et al. Prevalence of mental distress among adult survivors of childhood cancer in Germany—Compared to the general population. Cancer Medicine. 2019;8(4):1865-1874. DOI: 10.1002/cam4.1936
20.Günther M, Schulze J, Jellestad L, Mehnert A, Känel R, Euler S. Mental disorders, length of hospitalization, and psychopharmacy–new approaches to identify barriers to psychological support for patients with cancer. Psycho-Oncology. 2021;30(10):1773-1781. DOI: 10.1002/pon.5743
21.Zheng W, Guo Z. A survey study on the status of somatic symptoms in young and middle-aged patients with mental illness during long-term hospitalization. Contrast Media & Molecular Imaging. 2022;2022:1-6. DOI: 10.1155/2022/1110941
22.Brinkman T, Zhu L, Zeltzer L, Recklitis C, Kimberg C, Zhang N, et al. Longitudinal patterns of psychological distress in adult survivors of childhood cancer. British Journal of Cancer. 2013;109(5):1373-1381. DOI: 10.1038/bjc.2013.428
23.Abdelhadi O, Pollock B, Joseph J, Keegan T. Psychological distress and associated additional medical expenditures in adolescent and young adult cancer survivors. Cancer. 2022;128(7):1523-1531. DOI: 10.1002/cncr.34064
24.Michel G, Rebholz C, Weid N, Bergstraesser E, Kuehni C. Psychological distress in adult survivors of childhood cancer: The swiss childhood cancer survivor study. Journal of Clinical Oncology. 2010;28(10):1740-1748. DOI: 10.1200/jco.2009.23.4534
25.Kamen C, Mustian K, Dozier A, Bowen D, Li Y. Disparities in psychological distress impacting lesbian, gay, bisexual and transgender cancer survivors. Psycho-Oncology. 2015;24(11):1384-1391. DOI: 10.1002/pon.3746
26.Hovaldt H, Suppli N, Olsen M, Steding-Jessen M, Hansen D, Møller H, et al. Who are the cancer survivors? A nationwide study in Denmark, 1943–2010. British Journal of Cancer. 2015;112(9):1549-1553. DOI: 10.1038/bjc.2015.68
27.Grov E, Fossa S, Dahl A. Is somatic comorbidity associated with more somatic symptoms, mental distress, or unhealthy lifestyle in elderly cancer survivors? Journal of Cancer Survivorship. 2009;3(2):109-116. DOI: 10.1007/s11764-009-0081-6
28.Heathcote L, Loecher N, Simon P, Spunt S, Jordan A, Tutelman P, et al. Symptom appraisal in uncertainty: A theory-driven thematic analysis with survivors of childhood cancer. Psychology and Health. 2020;36(10):1182-1199. DOI: 10.1080/08870446.2020.1836180
29.Tuman M, Roberts K, Corner G, Beard C, Fadalla C, Coats T, et al. Interpretation bias in breast cancer survivors experiencing fear of cancer recurrence. Frontiers in Psychology. 2021;12:682174. DOI: 10.3389/fpsyg.2021.682174
30.Hall D, Lennes I, Pirl W, Friedman E, Park E. Fear of recurrence or progression as a link between somatic symptoms and perceived stress among cancer survivors. Supportive Care in Cancer. 2016;25(5):1401-1407
31.Lowery A, Starr T, Dhingra L, Rogak L, Hamrick-Price J, Farberov M, et al. Frequency, characteristics, and correlates of pain in a pilot study of colorectal cancer survivors 1–10 years post-treatment. Pain Medicine. 2013;14(11):1673-1680. DOI: 10.1111/pme.12223
32.Yang M, Baser R, Li S, Hou Y, Chong K, Zhang Y, et al. Tibetan herbal pain-relieving plaster for chronic musculoskeletal pain among cancer survivors: Study protocol of a randomized, double-blind, placebo-controlled trial. Frontiers in Pharmacology. 2022;13:878371. DOI: 10.3389/fphar.2022.878371
33.Marshall V, Chavez M, Efre A, Lake P, Rigg K, Lubrano B, et al. Barriers to adequate pain control and opioid use among cancer survivors: Implications for nursing practice. Cancer Nursing. 2022;46(5):386-393. DOI: 10.1097/ncc.0000000000001126
34.Check D, Jones K, Fish L, Dinan M, Dunbar T, Farley S, et al. Clinician perspectives on managing chronic pain after curative-intent cancer treatment. Jco Oncology Practice. 2023;19(4):e484-e491. DOI: 10.1200/op.22.00410
35.O'Regan A, Fish L, Makarushka C, Somers T, Jones K, Merlin J, et al. Managing chronic pain in cancer survivorship: Communication challenges and opportunities as described by cancer survivors. The American Journal of Hospice & Palliative Care. 2022;41(1):78-86. DOI: 10.21203/rs.3.rs-2221806/v1
36.Sanford N, Sher D, Butler S, Xu X, Ahn C, Aizer A, et al. Prevalence of chronic pain among cancer survivors in the United States, 2010-2017. Cancer. 2019;125(23):4310-4318. DOI: 10.1002/cncr.32450
37.Stein K, Alcaraz K, Kamson C, Fallon E, Smith T. Sociodemographic inequalities in barriers to cancer pain management: A report from the american cancer society's study of cancer survivors-ii (scs-ii). Psycho-Oncology. 2016;25(10):1212-1221. DOI: 10.1002/pon.4218
38.Mercadante S, Grassi Y, Gebbia V. Cancer survivors: Long-term opioid therapy – The challenge. BMJ Supportive & Palliative Care. 2022;14(1):65-67. DOI: 10.1136/spcare-2022-003974
39.Jones K, Magee L, Fu M, Bernacki R, Bulls H, Merlin J, et al. The contribution of cancer-specific psychosocial factors to the pain experience in cancer survivors. Journal of Hospice and Palliative Nursing. 2023;25(5):E85-E93. DOI: 10.1097/njh.0000000000000965
40.Drury A, Payne S, Brady A. The cost of survival: An exploration of colorectal cancer survivors’ experiences of pain. Acta Oncologica. 2017;56(2):205-211. DOI: 10.1080/0284186x.2016.1266084
41.Mao J, Liou K, Baser R, Bao T, Panageas K, Romero S, et al. Effectiveness of electroacupuncture or auricular acupuncture vs usual care for chronic musculoskeletal pain among cancer survivors. JAMA Oncology. 2021;7(5):720. DOI: 10.1001/jamaoncol.2021.0310
42.Wang H, Liu X, Wang T, Tan J, Huang H. Breathing exercises for pain management in cancer survivors: A systematic review. Pain Management Nursing. 2022;24(3):299-310. DOI: 10.20944/preprints202203.0156.v1
43.Tofthagen C, González L, Visovsky C, Akers A. Self-management of oxaliplatin-related peripheral neuropathy in colorectal cancer survivors. Chemotherapy Research and Practice. 2013;2013:1-7. DOI: 10.1155/2013/547932
44.Kim S, Son B, Hwang S, Han W, Yang J, Lee S, et al. Fatigue and depression in disease-free breast cancer survivors: Prevalence, correlates, and association with quality of life. Journal of Pain and Symptom Management. 2008;35(6):644-655. DOI: 10.1016/j.jpainsymman.2007.08.012
45.Wang X, Zhao F, Fisch M, O’Mara A, Cella D, Mendoza T, et al. Prevalence and characteristics of moderate to severe fatigue: A multicenter study in cancer patients and survivors. Cancer. 2013;120(3):425-432. DOI: 10.1002/cncr.28434
46.Pachman D, Barton D, Swetz K, Loprinzi C. Troublesome symptoms in cancer survivors: Fatigue, insomnia, neuropathy, and pain. Journal of Clinical Oncology. 2012;30(30):3687-3696. DOI: 10.1200/jco.2012.41.7238
47.Yu C, Wang T, Chang C, Shen L, Shu W, Liu C, et al. Healthy life styles, sleep and fatigue in endometrial cancer survivors: A cross-sectional study. Journal of Clinical Nursing. 2020;29(7–8):1372-1380. DOI: 10.1111/jocn.15189
48.Daniëls L, Oerlemans S, Krol A, Creutzberg C, Poll-Franse L. Chronic fatigue in hodgkin lymphoma survivors and associations with anxiety, depression and comorbidity. British Journal of Cancer. 2014;110(4):868-874. DOI: 10.1038/bjc.2013.779
49.Gielissen M, Verhagen S, Witjes F, Bleijenberg G. Effects of cognitive behavior therapy in severely fatigued disease-free cancer patients compared with patients waiting for cognitive behavior therapy: A randomized controlled trial. Journal of Clinical Oncology. 2006;24(30):4882-4887. DOI: 10.1200/jco.2006.06.8270
50.Oktay J, Bellin M, Scarvalone S, Appling S, Helzlsouer K. Managing the impact of posttreatment fatigue on the family: Breast cancer survivors share their experiences. Families, Systems & Health. 2011;29(2):127-137. DOI: 10.1037/a0023947
51.Sprod L, Fernandez I, Janelsins M, Peppone L, Atkins J, Giguere J, et al. Effects of yoga on cancer-related fatigue and global side-effect burden in older cancer survivors. Journal of Geriatric Oncology. 2015;6(1):8-14. DOI: 10.1016/j.jgo.2014.09.184
52.Ikeuchi K, Ishiguro H, Nakamura Y, Izawa T, Kura N, Nin K. The relation between mindfulness and the fatigue of women with breast cancer: Path analysis. Biopsychosocial Medicine. 2020;14(1). DOI: 10.1186/s13030-020-0175-y. Available from: https://www.ncbi.nlm.nih.gov/pmc/articles/PMC7011601/
53.Peixoto T, Peixoto N, Santos C, Pinto C. Fatigue self-management strategies in cancer survivors: A systematic literature review. Revista De Enfermagem Referência. 2016;IV Série(10):113-124. DOI: 10.12707/riv16023
54.Prasad P, Hardy K, Zhang N, Edelstein K, Srivastava D, Zeltzer L, et al. Psychosocial and neurocognitive outcomes in adult survivors of adolescent and early young adult cancer: A report from the childhood cancer survivor study. Journal of Clinical Oncology. 2015;33(23):2545-2552. DOI: 10.1200/jco.2014.57.7528
55.Ah D, Storey S, Tallman E, Nielsen A, Johns S, Pressler S. Cancer, cognitive impairment, and work-related outcomes: An integrative review. Oncology Nursing Forum. 2016;43(5):602-616. DOI: 10.1188/16.onf.602-616
56.John T, Sender L, Bota D. Cognitive impairment in survivors of adolescent and early young adult onset non-cns cancers: Does chemotherapy play a role? Journal of Adolescent and Young Adult Oncology. 2016;5(3):226-231. DOI: 10.1089/jayao.2015.0025
57.Phillips N, Stratton K, Williams A, Ahles T, Ness K, Cohen H, et al. Late-onset cognitive impairment and modifiable risk factors in adult childhood cancer survivors. JAMA Network Open. 2023;6(5):e2316077. DOI: 10.1001/jamanetworkopen.2023.16077
58.Cherrier M, Anderson K, David D, Higano C, Gray H, Church A, et al. A randomized trial of cognitive rehabilitation in cancer survivors. Life Sciences. 2013;93(17):617-622. DOI: 10.1016/j.lfs.2013.08.011
59.Barlow-Krelina E, Chen Y, Yasui Y, Till C, Gibson T, Ness K, et al. Consistent physical activity and future neurocognitive problems in adult survivors of childhood cancers: A report from the childhood cancer survivor study. Journal of Clinical Oncology. 2020;38(18):2041-2052. DOI: 10.1200/jco.19.02677
60.Haque R, Hsu JW, Avila C, Olmstead R, Carroll JE, Irwin MR. Insomnia and susceptibility to depressive symptoms and fatigue in diverse breast cancer survivors. Journal of Women's Health (2002). 2021;30(11):1604-1615. DOI: 10.1089/jwh.2019.8135
61.Dietz AC, Chen Y, Yasui Y, et al. Risk and impact of pulmonary complications in survivors of childhood cancer: A report from the childhood cancer survivor study. Cancer. 2016;122(23):3687-3696. DOI: 10.1002/cncr.30200
62.Schlarb AA, Claßen M, Hellmann SM, Vögele C, Gulewitsch MD. Sleep and somatic complaints in university students. Journal of Pain Research. 2017;10:1189-1199. DOI: 10.2147/JPR.S125421
63.Wei Y, Blanken TF, Van Someren EJW. Insomnia really hurts: Effect of a bad night's sleep on pain increases with insomnia severity. Frontiers in Psychiatry. 2018;9:377. DOI: 10.3389/fpsyt.2018.00377
64.Sun Y, Wang L, Li C, Luo W. Sleep disturbance in Chinese college students with mental health problems: A moderated mediation model. International Journal of Environmental Research and Public Health. 2022;19(21):14570. DOI: 10.3390/ijerph192114570
65.Cherven B, Sampson A, Bober S, Bingen K, Frederick N, Freyer D, et al. Sexual health among adolescent and young adult cancer survivors: A scoping review from the children's oncology group adolescent and young adult oncology discipline committee. CA a Cancer Journal for Clinicians. 2020;71(3):250-263. DOI: 10.3322/caac.21655
66.Ford J, Kawashima T, Whitton J, Leisenring W, Laverdière C, Stovall M, et al. Psychosexual functioning among adult female survivors of childhood cancer: A report from the childhood cancer survivor study. Journal of Clinical Oncology. 2014;32(28):3126-3136. DOI: 10.1200/jco.2013.54.1086
67.Bjornard K, Howell C, Klosky J, Chemaitilly W, Srivastava D, Brinkman T, et al. Psychosexual functioning of female childhood cancer survivors: A report from the st. jude lifetime cohort study. Journal of Sexual Medicine. 2020;17(10):1981-1994. DOI: 10.1016/j.jsxm.2020.06.005
68.Hovén E, Fagerkvist K, Jahnukainen K, Ljungman L, Lähteenmäki P, Axelsson O, et al. Sexual dysfunction in young adult survivors of childhood cancer – A population-based study. European Journal of Cancer. 2021;154:147-156. DOI: 10.1016/j.ejca.2021.06.014
69.Ritenour C, Seidel K, Leisenring W, Mertens A, Wasilewski-Masker K, Shnorhavorian M, et al. Erectile dysfunction in male survivors of childhood cancer—A report from the childhood cancer survivor study. Journal of Sexual Medicine. 2016;13(6):945-954. DOI: 10.1016/j.jsxm.2016.03.367
70.El-Hosary E, Abd-Elsalam A. Effect of standard oncology nursing care intervention on reducing “sexual dysfunction” among cervical cancer survivors' women. Nursing & Primary Care. 2018;2(4):1-7. DOI: 10.33425/2639-9474.1072
71.Maass S, Boerman L, Brandenbarg D, Verhaak P, Maduro J, Bock G, et al. Symptoms in long-term breast cancer survivors: A cross-sectional study in primary care. The Breast. 2020;54:133-138. DOI: 10.1016/j.breast.2020.09.013
72.Schlairet M, Benton M. Quality of life and perceived educational needs among older cancer survivors. Journal of Cancer Education. 2011;27(1):21-26. DOI: 10.1007/s13187-011-0279-y
73.Sari N. Physical wellbeing in cervical and breast cancer survivors: A cross-sectional study in Surabaya, Indonesia. Indonesian Journal of Cancer. 2019;12(3):80. DOI: 10.33371/ijoc.v12i3.614
74.Jackson S, Williams K, Steptoe A, Wardle J. The impact of a cancer diagnosis on weight change: Findings from prospective, population-based cohorts in the UK and the US. BMC Cancer. 2014;14(1):926. DOI: 10.1186/1471-2407-14-926
75.Nho J, Kim S, Park M, Kweon S. Symptom clusters and quality of life in breast cancer survivors after cancer treatment in a tertiary hospital in Korea. European Journal of Cancer Care. 2018;27(6):e12919. DOI: 10.1111/ecc.12919
76.May C, Ho A, Yang Q, McCallum M, Iyengar N, Comander A, et al. Comparing outcomes of a digital commercial weight loss program in adult cancer survivors and matched controls with overweight or obesity: Retrospective analysis. Nutrients. 2021;13(9):2908. DOI: 10.3390/nu13092908
77.Naeim A, Dy S, Lorenz K, Sanati H, Walling A, Asch S. Evidence-based recommendations for cancer nausea and vomiting. Journal of Clinical Oncology. 2008;26(23):3903-3910. DOI: 10.1200/jco.2007.15.9533
78.Roiland R, Heidrich S. Symptom clusters and quality of life in older adult breast cancer survivors. Oncology Nursing Forum. 2011;38(6):672-680. DOI: 10.1188/11.onf.672-680
79.Wood G, Lynch B, Roenn J. Management of intractable nausea and vomiting in patients at the end of life. JAMA. 2007;298(10):1196. DOI: 10.1001/jama.298.10.1196
80.Puspita Z, Nissa C, Probosari E, Fitranti D. Consumption pattern score in cancer survivor with chemotherapy induced nausea and vomiting and non-cancer at shelter houses. Jurnal Gizi Indonesia (The Indonesian Journal of Nutrition). 2022;11(1):57-65. DOI: 10.14710/jgi.11.1.57-65
81.Taşpınar A, Şirin A. Effect of acupressure on chemotherapy-induced nausea and vomiting in gynecologic cancer patients in Turkey. European Journal of Oncology Nursing. 2010;14(1):49-54. DOI: 10.1016/j.ejon.2009.07.006
82.Sriningsih I, Elisa E, Lestari K. Aromatherapy ginger use in patients with nausea & vomiting on post cervical cancer chemotherapy. Jurnal Kesehatan Masyarakat. 2017;13(1):59-68. DOI: 10.15294/kemas.v13i1.5367
83.Thong M, Doege D, Weißer L, Jansen L, Bertram H, Eberle A, et al. Persisting deficits in health-related quality of life of colorectal cancer survivors 14–24 years post-diagnosis: A population-based study. Current Oncology. 2023;30(3):3373-3390. DOI: 10.3390/curroncol30030257
84.Deleemans J, Toivonen K, Reimer R, Carlson L. The chemo-gut study: A cross-sectional survey exploring physical, mental, and gastrointestinal health outcomes in cancer survivors. Global Advances in Health and Medicine. 2022;11. DOI: 10.1177/2164957x221145940. Available from: https://pubmed.ncbi.nlm.nih.gov/36583068/
85.Tang F, Wang J, Tang Z, Kang M, Deng Q, Yu J. Quality of life and its association with physical activity among different types of cancer survivors. PLoS One. 2016;11(11):e0164971. DOI: 10.1371/journal.pone.0164971
86.Zhuang J, Liu Y, Xu X, Cai Y, Liu M, Chen Z, et al. Association between physical activity and health-related quality of life: Time to deterioration model analysis in lung adenocarcinoma. Journal of Cancer Survivorship. 2022;17(6):1769-1779. DOI: 10.1007/s11764-022-01259-z
87.Park J, Lee J, Oh M, Park H, Chae J, Kim D, et al. The effect of oncologists' exercise recommendations on the level of exercise and quality of life in survivors of breast and colorectal cancer: A randomized controlled trial. Cancer. 2015;121(16):2740-2748. DOI: 10.1002/cncr.29400
88.Barchitta M, Maugeri A, Lio R, Quattrocchi A, Degrassi F, Catalano F, et al. The effects of diet and dietary interventions on the quality of life among breast cancer survivors: A cross-sectional analysis and a systematic review of experimental studies. Cancers. 2020;12(2):322. DOI: 10.3390/cancers12020322
89.Deleemans J, Gajtani Z, Baydoun M, Reimer R, Piedalue K, Carlson L. The use of prebiotic and probiotic interventions for treating gastrointestinal and psychosocial health symptoms in cancer patients and survivors: A systematic review. Integrative Cancer Therapies. 2021;20. DOI: 10.1177/15347354211061733. Available from: https://www.ncbi.nlm.nih.gov/pmc/articles/PMC8649088/
90.Mohammed T, Parekh T, Desai A. Cardiovascular risk management in cancer survivors: Are we doing it right? World Journal of Clinical Oncology. 2021;12(3):144-149. DOI: 10.5306/wjco.v12.i3.144
91.Kadowaki H, Akazawa H, Ishida J, Komuro I. Cancer therapeutics-related cardiac dysfunction — Insights from bench and bedside of onco-cardiology. Circulation Journal. 2020;84(9):1446-1453. DOI: 10.1253/circj.cj-20-0467
92.Armstrong G, Oeffinger K, Chen Y, Kawashima T, Yasui Y, Leisenring W, et al. Modifiable risk factors and major cardiac events among adult survivors of childhood cancer. Journal of Clinical Oncology. 2013;31(29):3673-3680. DOI: 10.1200/jco.2013.49.3205
93.Naaktgeboren W, Linschoten M, Graeff A, Rhenen A, Asselbergs F, Maas A, et al. Long-term cardiovascular health in adult cancer survivors. Maturitas. 2017;105:37-45. DOI: 10.1016/j.maturitas.2017.05.014
94.Lee S, Cartmell K. An association rule mining analysis of lifestyle behavioral risk factors in cancer survivors with high cardiovascular disease risk. Journal of Personalized Medicine. 2021;11(5):366. DOI: 10.3390/jpm11050366
95.Salz T, Zabor E, Brown P, Dalton S, Raghunathan N, Matasar M, et al. Preexisting cardiovascular risk and subsequent heart failure among non-hodgkin lymphoma survivors. Journal of Clinical Oncology. 2017;35(34):3837-3843. DOI: 10.1200/jco.2017.72.4211
96.Weaver K, Foraker R, Alfano C, Rowland J, Arora N, Bellizzi K, et al. Cardiovascular risk factors among long-term survivors of breast, prostate, colorectal, and gynecologic cancers: A gap in survivorship care? Journal of Cancer Survivorship. 2013;7(2):253-261. DOI: 10.1007/s11764-013-0267-9
97.Weaver K, Klepin H, Wells B, Dressler E, Winkfield K, Lamar Z, et al. Cardiovascular assessment tool for breast cancer survivors and oncology providers: Usability study. Jmir Cancer. 2021;7(1):e18396. DOI: 10.2196/18396
98.Loreti C, Castelli L, Coraci D, Fusco A, Giovannini S, Padua L. Polipharmacy and multimorbity in oncological patients: An open challenge. Current Oncology. 2021;28(1):273-274. DOI: 10.3390/curroncol28010030
99.Schoormans D, Vissers P, Herk-Sukel M, Denollet J, Pedersen S, Dalton S, et al. Incidence of cardiovascular disease up to 13 year after cancer diagnosis: A matched cohort study among 32,757 cancer survivors. Cancer Medicine. 2018;7(10):4952-4963. DOI: 10.1002/cam4.1754
100.Rodgers C, Monroe R. Osteopenia and osteoporosis in pediatric patients after stem cell transplant. Journal of Pediatric Oncology Nursing. 2007;24(4):184-189. DOI: 10.1177/1043454207303942
101.Ramin C, May B, Roden R, Orellana M, Hogan B, McCullough M, et al. Evaluation of osteopenia and osteoporosis in younger breast cancer survivors compared with cancer-free women: A prospective cohort study. Breast Cancer Research. 2018;20(1):134. DOI: 10.1186/s13058-018-1061-4
102.Choi Y, Park S, Cho W, Lee J, Hahn S, Jung M, et al. Factors related to decreased bone mineral density in childhood cancer survivors. Journal of Korean Medical Science. 2013;28(11):1632. DOI: 10.3346/jkms.2013.28.11.1632
103.Hershman D, Narayanan R. Prevention and management of osteoporosis in women with breast cancer and men with prostate cancer. Current Oncology Reports. 2004;6(4):277-284. DOI: 10.1007/s11912-004-0036-z
104.Fidler M, Reulen R, Bright C, Henson K, Kelly J, Jenney M, et al. Respiratory mortality of childhood, adolescent and young adult cancer survivors. Thorax. 2018;73(10):959-968. DOI: 10.1136/thoraxjnl-2017-210683
105.Smith G, Glaser A, Peckham D, Greenwood D, Feltbower R. Respiratory morbidity in young people surviving cancer: Population-based study of hospital admissions, treatment-related risk factors and subsequent mortality. International Journal of Cancer. 2019;145(1):20-28. DOI: 10.1002/ijc.32066
106.Heins M, Ligt K, Verloop J, Siesling S, Korevaar J, Berendsen A, et al. Adverse health effects after breast cancer up to 14 years after diagnosis. The Breast. 2022;61:22-28. DOI: 10.1016/j.breast.2021.12.001
107.Rock C, Doyle C, Demark-Wahnefried W, Meyerhardt J, Courneya K, Schwartz A, et al. Nutrition and physical activity guidelines for cancer survivors. CA a Cancer Journal for Clinicians. 2012;62(4):242-274. DOI: 10.3322/caac.21142
108.Stubblefield M. The underutilization of rehabilitation to treat physical impairments in breast cancer survivors. PM & R. 2017;9(9S2):S317-S323. DOI: 10.1016/j.pmrj.2017.05.010
109.Silver J, Baima J, Mayer R. Impairment-driven cancer rehabilitation: An essential component of quality care and survivorship. CA A Cancer Journal for Clinicians. 2013;63(5):295-317. DOI: 10.3322/caac.21186
110.Brennan L, Sheill G, O'Neill L, O'Connor L, Smyth E, Guinan E. Physical therapists in oncology settings: Experiences in delivering cancer rehabilitation services, barriers to care, and service development needs. Physical Therapy. 2022;102(3):pzab287. DOI: 10.1093/ptj/pzab287
111.Dunphy C, McNeely M. Growing the workforce in oncology physical therapy: From entry level to specialist care. Rehabilitation Oncology. 2022;40(1):5-6. DOI: 10.1097/01.reo.0000000000000277
112.Rossen S, Kayser L, Vibe-Petersen J, Christensen J, Ried-Larsen M. Cancer survivors’ receptiveness to digital technology–supported physical rehabilitation and the implications for design: Qualitative study. Journal of Medical Internet Research. 2020;22(8):e15335. DOI: 10.2196/15335
113.Neher M, Ludvigsson M, Enblom A. Preparedness to implement physical activity and rehabilitation guidelines in routine primary care cancer rehabilitation: Focus group interviews exploring rehabilitation professionals’ perceptions. Journal of Cancer Education. 2020;36(4):779-786. DOI: 10.1007/s13187-020-01704-6
114.Rafn B, Midtgaard J, Camp P, Campbell K. Shared concern with current breast cancer rehabilitation services: A focus group study of survivors’ and professionals’ experiences and preferences for rehabilitation care delivery. BMJ Open. 2020;10(7):e037280. DOI: 10.1136/bmjopen-2020-037280
115.Courneya K, Rogers L, Campbell K, Vallance J, Friedenreich C. Top 10 research questions related to physical activity and cancer survivorship. Research Quarterly for Exercise and Sport. 2015;86(2):107-116. DOI: 10.1080/02701367.2015.991265
116.Troeschel A, Leach C, Shuval K, Stein K, Patel A. Physical activity in cancer survivors during “re-entry” following cancer treatment. Preventing Chronic Disease. 2018;15:E65. DOI: 10.5888/pcd15.170277
117.Kang J, Park E, Lee J. Cancer survivorship in primary care. Korean Journal of Family Medicine. 2019;40(6):353-361. DOI: 10.4082/kjfm.19.0108
118.Weaver K, Forsythe L, Reeve B, Alfano C, Rodriguez J, Sabatino S, et al. Mental and physical health–related quality of life among U.S. cancer survivors: Population estimates from the 2010 national health interview survey. Cancer Epidemiology Biomarkers & Prevention. 2012;21(11):2108-2117. DOI: 10.1158/1055-9965.epi-12-0740
119.Holtmaat K, Spek N, Lissenberg-Witte B, Cuijpers P, Leeuw I. Positive mental health among cancer survivors: Overlap in psychological well-being, personal meaning, and posttraumatic growth. Supportive Care in Cancer. 2018;27(2):443-450. DOI: 10.1007/s00520-018-4325-8
120.Harms C, Cohen L, Pooley J, Chambers S, Galvão D, Newton R. Quality of life and psychological distress in cancer survivors: The role of psycho-social resources for resilience. Psycho-Oncology. 2018;28(2):271-277. DOI: 10.1002/pon.4934
121.Burris J, Andrykowski M. Disparities in mental health between rural and nonrural cancer survivors: A preliminary study. Psycho-Oncology. 2009;19(6):637-645. DOI: 10.1002/pon.1600
122.Adams M, Jewell A. The use of complementary and alternative medicine by cancer patients. International Seminars in Surgical Oncology. 2007;4(1):655-663. DOI: 10.1186/1477-7800-4-10
123.Zeltzer L, Recklitis C, Buchbinder D, Zebrack B, Casillas J, Tsao J, et al. Psychological status in childhood cancer survivors: A report from the childhood cancer survivor study. Journal of Clinical Oncology. 2009;27(14):2396-2404. DOI: 10.1200/jco.2008.21.1433
124.Mao J, Palmer C, Healy K, Desai K, Amsterdam J. Complementary and alternative medicine use among cancer survivors: A population-based study. Journal of Cancer Survivorship. 2010;5(1):8-17. DOI: 10.1007/s11764-010-0153-7
125.Aronson K, Wagstaff D, Farace E, Muscat J, Belani C, Almokadem S, et al. A week in the life of lung cancer survivors: Daily reports of stress, worry, mood, and symptoms. Journal of Health Psychology. 2016;21(10):2269-2282. DOI: 10.1177/1359105315574921
126.Husebø A, Husebø T. Quality of life and breast cancer: How can mind–body exercise therapies help? An overview study. Sports. 2017;5(4):79. DOI: 10.3390/sports5040079
127.Slocum-Gori S, Howard A, Balneaves L, Kazanjian A. Investigating the perceived feasibility of integrative medicine in a conventional oncology setting. Integrative Cancer Therapies. 2012;12(2):103-112. DOI: 10.1177/1534735412443851
128.Barone R, Gulisano M, Cannata E, Padalino S, Saia F, Maugeri N, et al. Self- and parent-reported psychological symptoms in young cancer survivors and control peers: Results from a clinical center. Journal of Clinical Medicine. 2020;9(11):3444. DOI: 10.3390/jcm9113444
129.Nord C, Mykletun A, Thorsen L, Bjøro T, Fosså S. Self-reported health and use of health care services in long-term cancer survivors. International Journal of Cancer. 2004;114(2):307-316. DOI: 10.1002/ijc.20713
130.Fouladbakhsh J, Stommel M. Comparative analysis of cam use in the U.S. cancer and noncancer populations. Journal of Complementary and Integrative Medicine. 2008;5(1):9-10. DOI: 10.2202/1553-3840.1140
Written By
Val Bellman
Submitted: 01 February 2024Reviewed: 02 February 2024Published: 02 April 2024