Open Access is an initiative that aims to make scientific research freely available to all. To date our community has made over 100 million downloads. It’s based on principles of collaboration, unobstructed discovery, and, most importantly, scientific progression. As PhD students, we found it difficult to access the research we needed, so we decided to create a new Open Access publisher that levels the playing field for scientists across the world. How? By making research easy to access, and puts the academic needs of the researchers before the business interests of publishers.
We are a community of more than 103,000 authors and editors from 3,291 institutions spanning 160 countries, including Nobel Prize winners and some of the world’s most-cited researchers. Publishing on IntechOpen allows authors to earn citations and find new collaborators, meaning more people see your work not only from your own field of study, but from other related fields too.
The history of physical activity and sport dates to ancient times, when it was not only a means of preparation for military readiness but also had religious and educational purposes. The relationship between physical activity and good health goes back centuries accepted, as formulated by Hippocrates 2500 years ago. In Greek antiquity, “gymnastike” highlighted physical beauty in harmony with the soul and spirit, perfecting simultaneously an individual’s personality and health. Lifelong exercise administered by gymnasts was applied to strengthen weak limbs, and contributed to the healing of patients when applied in the healthcare facilities of the time, as mentioned in “Asclepieia.” Nowadays, the idea that “exercise is medicine” has two components: (1) every patient’s treatment or rehabilitation plan should include physical activity and exercise training, but the prescription must be tailored to the patient’s specific needs and (2) doctors’ challenge lies in implementing this medical prescription for adapted physical activity (APA), which encourages patients to lead more active lives.
Laboratory of Adapted Physical Activity/Developmental and Physical Disabilities, National and Kapodistrian University of Athens, Greece
School of Physical Education and Sport Science, National and Kapodistrian University of Athens, Greece
Soteria Yiannaki*
School of Physical Education and Sport Science, National and Kapodistrian University of Athens, Greece
Faculty of History of Physical Education and Sport, National and Kapodistrian University of Athens, Greece
Dimitra Koutsouki
Laboratory of Adapted Physical Activity/Developmental and Physical Disabilities, National and Kapodistrian University of Athens, Greece
School of Physical Education and Sport Science, National and Kapodistrian University of Athens, Greece
*Address all correspondence to: kasonitou@phed.uoa.gr and sgiannaki@phed.uoa.gr
1. Introduction
According to Barbin [1], the term “adapted PA” (physical and sports activities) refers to any physical activity or sport that is modified and tailored to a person’s functional movement, restrictions, contraindications to certain exercises, and surroundings in order to provide a means of participation for those with a variety of disabilities or long-term medical conditions. Additionally, APA is frequently employed by medical practitioners as a rehabilitation strategy for social and educational engagement, reeducation, community reintegration, and the avoidance of secondary disorders [1].
Thornton et al. [2] have proposed that a cost-effective strategy for promoting physical activity (PA) would be to prescribe PA as part of primary healthcare. To guarantee appropriate PA prescription, individuals with disabilities must have their unique requirements, capacities, and indications considered when prescribing PA. Nonetheless, to guarantee appropriate PA prescription, the demands, capacities, and symptoms of everyone with a disability must be taken into account. Sedentary behavior among people with disabilities has been found to be influenced by both personal and environmental factors, such as pain, lack of energy, and self-consciousness about exercising in public. Personal factors include things such as pain, lack of exercise equipment, social exclusion, and inadequately trained and resourced health staff. For people of all ages, research clearly shows the advantages of maintaining an active lifestyle across a variety of physical and mental health concerns. The Department of Health and Human Services in the United States offers precise recommendations for physical exercise at various phases of life. Some recommendations and things to think about are included on this website [3] for persons who are pregnant, elderly, or have chronic health issues. Also, it is important to inform our doctor about the sort of activity we want to begin whether we are a new fitness enthusiast or have a particular medical issue. For a particular health issue, they might check the format to make sure it is safe (Figure 1).
Figure 1.
Impact of “sports on prescription” on the health and well-being of patients [4].
2. Exercise and ‘well-being’: from the past to the present
2.1 Exercise, health, and illness in antiquity
Movement constitutes the characteristic feature of life [5] and is considered an innate disposition of humans. Exercise consists of movements that, when applied, benefit both the body and the soul [5]. Games, physical activity, physical culture activities, and competitions found expression in the cultures of antiquity following the customs and culture they developed.
In those cultures, exercise was seen as essential for maintaining a healthy state and preventing diseases. Ancient Chinese culture placed importance on health and well-being through various practices. Practices such as qigong (breathing exercises) and yoga were used as forms of exercise to promote physical and mental health. In ancient India, while physical exercise was recognized and practiced, the focus was more on general physical activities rather than a structured exercise prescription for health purposes. In Greek antiquity, a strong emphasis was placed on physical fitness and exercise for maintaining a healthy body and mind [6].
In the ancient Greek world, the art of healing and preserving life was subject to the laws of the universe and protected by the Gods. Health, the daughter of the god Asclepius [7], is deified as people realized the importance of preserving and treating diseases, and Asclepieia existed scattered throughout the Hellenic territory. In classical antiquity, health was considered a harmonious state of body and soul. The central concept was the idea of balance and harmony of the individual, aiming for well-being, resulting in the development of a holistic approach to health and disease through exercise. Some representative beliefs of physicians and philosophers are cited below.
Hippocrates (460–377 BC) transformed hieratic or theocratic medicine into a rational discipline. In the works of the Hippocratic Corpus, it is argued that health depends on the balance between diet and exercise. Hippocratic physicians believed that physical well-being can only be achieved through appropriate education, with moderation adapted to the individual’s condition, age, and strength, which should avoid excess. They were opposed to both excessive athletic training and the avoidance of exercise, as well as to gluttony [8].
The fundamental layout of the Asclepieion in Kos indicates Hippocrates’ belief in a comprehensive healthcare model. In his school, scientific principles were combined with pharmaceutical treatment, dietary plans, and both physical and mental exercises, along with divine intervention. Additionally, at the Asclepieion of Kos, every patient received a comprehensive treatment regimen that incorporated physical activities, massages, and walks deemed essential for the restoration of health, the well-being of the soul, and inner peace [9].
Both physical and psychospiritual education became central interests, and Plato (427–347 BC), influenced by Socrates and Hippocrates, defined that proper education is divided into the education of the body and the education of the soul, the former being called gymnastics and the latter music. Consequently, the lessons corresponding to gymnastics and music were divided into physical perfection and mental well-being. Physical education was closely linked to psychospiritual education, so citizens should engage in physical exercise for life. According to Plato, good physical condition is shaped by gymnastics, the art that preserves health and physical disposition through proper diet and rules, and medicine, which operates therapeutically. The purpose of gymnastics is the improvement of bodies through physical care, as determined by the right reason. In his work “Timaeus,” he describes the result of the harmonious movement of body and soul: “From both these evils the one means of salvation is this—neither to exercise the soul without the body nor the body without the soul, so that they may be evenly matched and sound of health. Thus the student of mathematics, or of any other subject, who works very hard with his intellect must also provide his body with exercise by practicing gymnastics; while he who is diligent in molding his body must, in turn, provide his soul with motion by cultivating music and philosophy in general, if either is to deserve to be called truly both beautiful and virtuous: kalos kagathos” [10].
The attainment of eudaimonia was synonymous with balance, so health and illness, virtue and vice, were consequences of the symmetry or asymmetry of the soul to the body. Thus, the soul should not move without the body, nor the body without the soul, and both should be cared for to maintain balance and health. People should be educated in gymnastics from childhood and throughout their lives [11].
According to Aristotle (384–323 BC), “to act well and to live well” was the primary pursuit, meaning human happiness (eudaimonia). This happiness could be achieved through the harmony of the body. He considered gymnastics as the science of “moderation in pains” and thus distinguished athletic exertion from physical activity that contributed to the individual’s balance, provided it did not involve excessive or inappropriate exercises. Thus, the art of health was preserved [12].
Philological evidence from the Roman Imperial period indicates that intellectuals of that era redefined gymnastics in connection to medicine and the pursuit of well-being, aligning with the classic beliefs of Greek antiquity [13].
In the texts of Plutarch (46–120 AD), his belief in gymnastics is recorded, which, through appropriate exercises, ensures health and cultivates military readiness. The purpose of gymnastics was the well-being of the body, while medicine aimed at maintaining health. Exercises should not be exhaustive or specialized. The usefulness of gymnastics relates to the harmony and strength of the body, while when taken to excess or pursued for competitive goals, it becomes an obstacle to the spiritual development of young people [14].
The physician Galen (128–200 AD) defined that not every movement is exercise, only active movement, and set the criterion as the alteration of the normal rhythm of breathing. He urged those who exercised for health reasons not to overstrain themselves to avoid the psychosomatic dependence caused by athletes’ exercise. He recognized the connection between well-being and gymnastics and the preservation of health through gymnastics, as well as the therapeutic dimension of both medicine and gymnastics [15].
According to Philostratus (179–249 AD), gymnastics was created from the synthesis of the art of paidotribai and medicine but was more comprehensive than the former and a part of the latter. Suitable exercise could remove excess flesh and fat from the body, soften a hardened limb, or strengthen or warm the body. Gymnastics, along with appropriate diet and rubbing, could stop colds, excessive sweating, and wasting, which doctors treated with therapeutic measures [16].
Ancient Greek culture perceived health as a balanced state between exercise and diet. Hippocratic physicians promoted physical well-being through proper education and moderation in exercise, contrary to excess or avoidance. Plato and other philosophers considered gymnastics an integral part of education, promoting balance between body and soul. Similarly, well-being was regarded as a result of the harmony between body and spirit. With gymnastics being a “guardian” of health, exercise preserved and cultivated health while also preventing and treating illness.
2.2 From practice to theory and from theory to knowledge
The “gymnast” – the educated physical trainer – represented the evolution of the paidotribe (who dealt with gymnastics issues utilizing his experience and practical knowledge as a former athlete). Until the distinction of their competencies, there was a period when the two terms were used interchangeably.
Plato, in his work “Republic” refers to the paidotribe-gymnast Herodicus, who: “… was a paidotribe and became a valetudinarian, and blended gymnastics and medicine, for the torment first and chiefly of himself and then of many successors,” introducing therapeutic gymnastics. The knowledge of the paidotribe-gymnast is comparable to that of a physician, and one should equally take their comments seriously. Both are specialists for the body and can discern a patient. The two arts, gymnastics and medicine, thus the gymnasts and the physicians, can properly distinguish (possess the appropriate knowledge) the types of purification performed on living organisms. They also knew about diets and applied suitable nutrition. Therefore, we can understand that there was a period when the boundaries between the two were indistinct [17].
Over time, the gymnast acquired knowledge such as anatomy, physiology, pedagogy, the art of physiognomy (psychology), knew different exercises, and simultaneously the result of the exercises on the trainee; he can be characterized as a ‘pentathlete of knowledge’ [18]. At the peak of his scientific status, he could apply the appropriate exercises for training, rehabilitation, restoration, cultivation, and preservation of health.
2.3 The modern past: exercise is medicine
In the introduction of his paper, Berryman [19] highlights the pivotal significance of the texts of Hippocrates and Galen, referring to the stimulus that influenced the formation of the physical education movement in the nineteenth century. Specifically, he notes the context of the “six things nonnatural” (air, diet sleep and wake, exercise and rest, excretions and retentions, and passion of the mind). If the nonnaturals were observed and practiced in moderation, health would be the result.
Exercise was incorporated into the regimen, hygiene, and preventive medicine literature in the late nineteenth century and was primarily used for prophylaxis. It was recommended as a treatment for various ailments and was considered part of medicine. In New York, 1806, physician Shadrach Ricketson published “Means of Preserving Health and Preventing Diseases,” which discussed the negative effects of idleness and luxury on health and the importance of exercise.
In 1880, physicians took on leadership roles in physical education associations and published corresponding journals, oversaw gyms, gave lectures, and prescribed exercise. In 1900, the course of medicine began to change, emphasizing research, vaccines, and the scientific specialization of physicians. Later on, the Harvard Fatigue Laboratory (1930s–40s) conducted groundbreaking studies on exercise, laying the foundation for exercise science research in the 1960s.
Meanwhile, there was a shift in physical education from a focus on health and exercise led by physicians to a games and sports curriculum led by coaches. The new sports doctrine emphasized citizenship, teamwork, character, democratic living, and sportsmanship, but it was found that the health of millions of Americans had problems. It was reaffirmed that physical activity was a fundamental characteristic of health. In the 1970s, exercise entered people’s lives as a lifestyle, and in the following years, magazines and books were published connecting exercise with health. In 2007, the American Medical Association and American College of Sports Medicine inaugurated the Exercise is Medicine health initiative, making the culture of exercise and health in Greek antiquity come to life once more.
3. Medical usage of adapted physical activity (APA)
3.1 Exercise as medication for treating many chronic diseases
A five-year Swedish primary care study conducted by Joelsson and colleagues [20] investigates the effects of long-term prescription physical exercise on individuals who are physically inactive and have metabolic risk factors. The intervention involved prescriptions for tailored physical exercise together with follow-ups, which increased engagement and motivation. In fifteen basic healthcare clinics in Gothenburg, Sweden, individual interviews were subjected to a qualitative content analysis after a purposeful selection of interview participants. Ten patients responded to the intervention, whereas the remaining ten patients did not, for a total of twenty physically inactive individuals with one or more metabolic syndrome components. The patients’ mean age ranged from 25 to 73 years.
Three different impact groups were identified by the interviews. First, personal modifications led to a rise in physical activity. Second, maintaining and setting priorities for lifestyle modifications was made easier with the help of follow-up and support. Third, patients may be more motivated if they have control over their treatment and see results. Personalized physical exercise on prescription with frequent follow-ups can help to enhance and sustain motivation and physical activity levels.
In conclusion, physical activity levels were observed to rise with individually prescribed physical exercise for inactive adults with the metabolic syndrome. Patients exhibited more motivation when they created their own physical activity plans. Healthcare professionals’ support and follow-up made lifestyle changes priority, and experiences with positive health outcomes contributed to maintaining or increasing levels of physical activity.
Pedersen & Saltin [21] conducted a systematic review study that looked at the most recent evidence-based basis for prescribing exercise as medicine in the treatment of 26 different diseases: cancer; metabolic diseases (obesity, hyperlipidemia, metabolic syndrome, polycystic ovarian syndrome, type 2 diabetes, and type 1 diabetes); pulmonary diseases (chronic obstructive pulmonary disease, asthma, and cystic fibrosis); musculoskeletal disorders (osteoarthritis, osteoporosis, back pain, and rheumatoid arthritis); and psychological diseases (dementia, Parkinson’s disease, multiple sclerosis, dementia, polycystic ovarian syndrome, type 2 diabetes, type 1 diabetes, and cerebral apoplexy). Exercise therapy’s impact on the etiology and symptoms of disease is described, along with potential mechanisms of action. They have provided the reader with the finest advice for the type and amount of exercise that should be advised for each condition after analyzing the scientific literature.
According to the authors’ conclusion, it is customary in the medical field to recommend the evidence-based course of therapy that is most likely to be successful and have the fewest risks or adverse effects. According to the available data, exercise therapy may be more beneficial than medical treatment in some circumstances or may even enhance its effects in others. Now that so much knowledge has been gathered, it must be put into practice. It’s time for the health systems to put in place the necessary framework to guarantee that supervised exercise can be prescribed as medicine, even though there is still work to be done in defining the best kind and amount of exercise and investigating whether one-legged training, high-intensity interval training, or other more recent exercise modalities which will be appropriate for certain diagnoses.
Furthermore, it is critical that society encourages an active lifestyle. When you advise people to move, they do not. When the situation demands it, they shift. Accessibility is crucial to raising a population’s level of physical activity. Laws and political declarations on “health consequences” are necessary. Politicians should always consider concerns related to gender and ethnicity, but they should also take into account health-related issues, such as how design and infrastructure may affect how physically active a community is.
The goal of a cross-sectional study [22] conducted between February 2020 and July 2021 at the Nancy University Center of Sports Medicine and APA, France, was to determine the heart rate and level of exercise intensity in a sample of 71 patients with chronic illnesses who were not using beta-blockers from the departments of hematology, rheumatology, obesity, and other specialties who were taking part in a hospital-based adaptive physical activity program (APA). Physiotherapists and exercise specialists with academic degrees in adapted physical activity (APA) typically collaborate to offer APA in hospital settings. The APA program was customized for each patient, taking into account their expectations, psychological characteristics, physical fitness, and preferred forms of exercise.
A mean age of 42.6 and a mean BMI of 36.7 (±10.6) were found in the 52 female patients. About 57.3% of the patients had been referred because of obesity. There were 36 individuals with impaired exercise performance and 39 patients with normal exercise capacity. Prior to engaging in a supervised APA practice, the participants methodically completed a cardiopulmonary exercise test; heart rate (HR) was monitored during the first session via a telemetry wireless device. Drawing from the outcomes of the functional assessment of exercise performance examined two patient groups: (1) unrestricted exercise performance (maximal oxygen uptake exceeding 80% of the theoretical reference) and (2) restricted exercise performance (maximum oxygen uptake falling short of 80% of the theoretical value).
Patients in both groups had HRs that were higher than 70% of their true maximal HR during the most intense 15-minute APA session episode. Researchers found that people with a range of chronic illnesses had modest levels of APA exercise intensity. In terms of exercise intensity, they did not see any significant differences in the patients’ capacities—that is, between those with and without a maximum performance restriction. 69.2% of maximum capacity was the mean and median actual intensity level of exercise during hospital-based APA sessions among a sample of patients. The highest level of intensity (75.8% of maximum capacity) was only achieved during the most intense 15 minutes. The findings emphasize the need for a preventative functional evaluation of cardiopulmonary fitness in patients with fragile chronic conditions prior to prescribing any exercise, as intense activity is known to increase cardiovascular events.
However, it is critical to acknowledge the significance of exercise professionals in order to integrate them into the global healthcare strategy and secure their support. The findings consequently emphasize the critical role that medical practitioners play in both systematically assessing patients’ health state and encouraging frequent physical exercise in them. To facilitate a shift toward a less sedentary and more independent lifestyle, healthcare practitioners often prioritize patient-centered dialog, individualized physical activity recommendations accompanied by written prescriptions, and follow-up throughout patient treatment. The findings indicate that medical practitioners ought to carefully assess each patient’s condition of health, given the increased stress levels that accompany exercise. This will increase the efficacy of the WHO slogan for 2018–2030, “More active people for a healthier world.”
There are restrictions on this study. Firstly, any expansion of the results is impossible due to the sample size; a single medical center’s small sample of 75 APA practitioners participated in the study. Furthermore, a subgroup analysis of several chronic diseases was hampered by the high proportion of obese people. Consequently, HR has limits even if it is the most practical metric for assessing the intensity in an ecological setting. However, the HR curve is influenced by age, gender, and performance, among other factors.
This study investigated high levels of exercise intensity (>70% of HRpeak in exercise tests) in individuals with and without performance limitations who were suffering from various chronic conditions. The study’s primary strength is its novelty, as it allowed us to capture the real practice intensity throughout APA sessions using physiological data that were collected. In this study, individual capabilities and progressive exercise tests are included. In fact, VO2max is the gold standard for evaluating a patient’s functional abilities. Nonetheless, long-term research analyzing a broader sample would clarify these findings. The results show that safe exercise routines may be developed, and medical risk can be assessed by creating personalized exercise plans that are appropriate for the patient’s present health status [22].
4. Adaptive exercise prescription for special populations
4.1 People with brain impairment
An important loss or anomaly in the anatomy of the brain is called brain impairment (BI). Brain damage can result from a variety of medical diseases, such as stroke, traumatic brain injury, and cerebral palsy. Studies reveal that individuals with brain injury (BI) participate in much less physical activity compared to those without BI. The loss of muscular strength, flexibility, and cardiovascular fitness resulting from physical inactivity may worsen the secondary impairment. Furthermore, because BI patients tend to be highly sedentary, it has been proposed that they are more vulnerable to conditions including cancer, hypertension, myocardial infarction, chronic obstructive pulmonary disease, anxiety, and depression—all conditions associated with physical inactivity. Crucially, research indicates that increased physical activity can help people with BI improve a variety of indices, including as muscular strength, functional independence, and cardiorespiratory fitness [23]. Therefore, it is critical to plan and evaluate interventions that successfully promote physical activity participation in people with brain injuries.
A health professional with expertise in organized exercise prescription for people with disabilities, encouraging community involvement for people with disabilities, and utilizing evidence-based techniques for physical activity promotion is delivering the program. People go through Steps 1, 2, 3, and 4 in around ten in-person meetings spread out over a 12-week period. Each session lasts around 1 hour, and the intervals between sessions are customized based on the needs of the individual. As community access is arranged, skills are learned, habits are developed, and discussions on values, motivation, and physical activity involvement evolve; more sessions are often completed in the first 6 weeks [23].
Apart from the face-to-face sessions, Steps 2 and 3 also involve electronic notifications, emails, or reminder calls to reaffirm the session’s objectives and/or act as a catalyst for additional action (e.g., to talk about a participant’s first community exercise class or a prompt to contact a nearby sports club). How much use is made of these tactics will depend on the participant’s impairment profile (especially memory impairment), preferences, availability, and capacity for employing various communication strategies.
A community-based rehabilitation paradigm is used to provide the APAP. Services offered in a person’s home or community—that is, the actual surroundings they usually reside in or have easy access to—are referred to as community-based rehabilitation. To facilitate program replication and improvement for clinical practice, this document provides a thorough explanation of the program’s components together with a real case study example for researchers and practitioners to review. The purpose of presenting these elements is to help researchers and practitioners understand what information/knowledge and abilities are required in order to integrate the program into clinical practice [23].
This article outlines a community-based, specially designed program to encourage persons with BI to participate in physical exercise. It has been demonstrated that the program works well to encourage individuals with BI to undertake physical exercise. In contrast to previously assessed programs, the APAP stands out for its extensive pre-participation assessment that is mapped against the ICF domains to customize the program to everyone’s health, personal preferences, and environmental factors; it also uses a community-based rehabilitation model rather than providing care in a fixed facility and the application of specialized behavior modification techniques in addition to regimented exercise prescription and lifestyle physical activity engagement. Because customized community-based physical activity programs are associated with sustained physical activity participation, and they are inexpensive to administer, they are a good choice.
4.2 People with intellectual disabilities (ID)
Pre- and post-exercise intervention programs were evaluated by Asonitou and colleagues [24], who also looked at two other components of adult ID. The intervention and control groups differed from one another, and the two groups can become significantly different after the intervention program depending on two factors. The intervention group was expected to show improved anthropometry features and higher levels of physical fitness after a four-month training session.
The study comprised 38 adults with intellectual impairments who were split into two groups: the intervention group (n = 19) which underwent exercise training and the control group (n = 19) which did not get any exercise training. While the control group had no instruction and was just instructed to maintain their regular physical activity, the intervention group underwent an intense 16-week exercise program. Over the course of four consecutive months (16-week), the exercise intervention program was carried out twice a week. Every week, there were two 60-minute training sessions that included a range of motor tasks aimed at improving endurance, balance, coordination, speed, and muscular strength.
The testing was placed in the gym or courtyard of the daily care and training center, which met all facility requirements (health and sanitary standards, enough space, lighting, right flooring, enough equipment, accessories, and measuring tools). Although a few individuals required help to complete the tasks, none of the participants left the sessions early. The adapted physical education teachers led each training session, and the investigator supervised any interventions [24].
In order to encourage a more active and healthy way of life, the study demonstrated that adults with mild intellectual disabilities can benefit from a structural physical exercise program in terms of their physical fitness, particularly in terms of muscle strength and endurance, balance, flexibility, speed, and cardio-respiratory endurance as well as anthropometry characteristics such as weight, fat, and BMI.
This shows that persons with moderate ID can benefit from structured physical activity and a tailored training program as an effective intervention to increase their level of fitness. Therefore, more physical activity would enable people with ID to engage in community outdoor activities, foster integration with people without disabilities, and increase their physical fitness, so they can handle daily tasks more easily and lead healthier and more fulfilling lives.
4.3 Child obesity
The evidence-based intervention known as physical activity on prescription (PAP) has been found to have positive effects on adult physical activity levels in Swedish primary healthcare centers. It is crucial to address physical inactivity from an early age as it is a major contributing factor to childhood obesity, which is correlated with adult obesity. Bernhardsson and her colleagues [25] investigated the implementation of the PAP on obese children. This project’s main twofold goal was to assess (a) children’s, parents’, and healthcare professionals’ experiences with PAP and (b) the requirements, necessary conditions, factors, and viability of using PAP tailored to children with obesity in pediatric healthcare.
Swedish primary healthcare practitioners have identified two obstacles to adopting PAP for adults: a lack of organizational support and a lack of understanding about the intervention. Positive attitudes among coworkers and both local and central support networks are facilitators. It is important to include parents in any efforts to encourage physical activity as family support and parental role models are critical for children when adopting physical exercise [25].
Managers and medical staff from 26 pediatric clinics in Region Västra Götaland, Sweden, were invited to participate in an online survey during the study’s initial phase. A portion of this sample was used in a focus group investigation. PAP was customized to the target audience and circumstance based on the inferences made from these two pieces of data. In the second phase of the clinical research, 60 obese (ISO-BMI > 30) children between the ages of six and twelve, together with one of their parents or legal guardians, took part. The purpose of the study was to assess the personalized PAP intervention. The implementation process and clinical outcomes were assessed both before and after the intervention, as well as at the 8 and 12-month follow-ups. The four fundamental ideas of the Normalization Process Theory are implementation results; coherence, cognitive engagement, group work, and reflexive monitoring; as well as the suitability, practicality, and acceptability of the PAP intervention. Adherence, dosage, intervention fidelity, recruitment and retention rates, and other process outcomes are included. Clinical outcomes include BMI, metabolic risk factors, sleep, health-related quality of life, self-efficacy, and desire for physical activity in addition to patterns of physical activity. Finally, we will use semi-structured interviews to examine the viewpoints of kids and parents. The Normalization Process Theory served as the foundation for the investigations’ design and analysis [25].
Through this study, new information will be available on whether PAP is feasible for obese children as well as if and how evidence-based interventions may be implemented and modified for use with different populations and circumstances.
4.4 Breast cancer survivors (multidisciplinary approach)
The international literature emphasizes the importance of physical activity (PA) in the first steps after cancer surgery. The regular practice of physical exercise causes positive adaptations in several functional capacities, with positive consequences on patients’ quality of life. This study was designed to assess the impact of a post-operative training program on the functional abilities and quality of life of breast cancer (BC) survivors. The protocol was tailored to account for both cancer-related difficulties and the existence of comorbidities [26].
The collaboration of sport medicine doctors (who prescribe exercise and do risk assessment), kinesiologists (who train), and oncologists (who recommend patients) proved essential. A group of 35 post-surgery BC patients voluntarily chose to participate in either the Usual Care Group (UC Group) or an online Adapted PA (APA) program twice a week for 4 months. The results showed that the APA Group’s functional capacity rose by 13.1% (p = 0.000), while their perceived effort reduced by 19.7% (p = 0.020). Within the same cohort, there was a significant increase (p = 0.050) in the overall health as assessed by the EORTC-QLQ-C30 questionnaire. In the UC Group, no differences were discovered. Operation Phalco, which established a network of kinesiologists, sports medicine specialists, and oncologists, reaffirms the need to plan a post-operative course in which APA ought to be included in cancer patient care from the outset [26].
Based on the positive physiological and psychological outcomes that Schutz et al. have shown in BC survivors, the method could be able to overcome the PA barriers related to lack of individualization [27, 28]. To be more specific, the study’s results showed that the patient’s overall health status had improved because the patient felt less tired during the test and had a higher functional capacity as determined by the 6MWT, a test that assesses general health in BC patients. Skeletal muscular deconditioning is one among the main adverse consequences of BC [29].
Increased muscular strength may be a general predictor of functional lower limb strength and improved balance. The APA group demonstrated this by increasing the load lifted in the 1RM leg press and the number of repetitions completed during the 30” STS test [30, 31]. Otherwise, there were no appreciable changes in APA as indicated by the upper limb strength testing. This might occur because of the restricted overloads employed during the 4-month intervention (1–3 kg) and the fact that the exercise routine was delivered via video conference, which required the exercises to be safe. Furthermore, rather than focusing on increasing strength, “PHALCO” training was designed to restore the function of the operated limb. The findings showed that, even in a pandemic scenario, a multidisciplinary and integrated strategy including oncologists, sport doctors, and APA kinesiologists is safe and practicable during the post-operative BC period and can enhance the quality of life for these patients. Additionally, there were no unfavorable incidents or dropout rates during training sessions for the APA group.
“PHALCO” recommends varying degrees of exercise with specified FITT parameters based on the BC patient’s comorbidities and physical state. We might be able to specify even more precisely which exercise is best for each patient by using this framework as a basis for future therapeutical techniques depending on patient characteristics. Combined training appears to be the best APA strategy able to supplement the conventional therapy, as it has been demonstrated to improve QoL (quality of life), functional ability, muscular strength, and reduce the impression of tiredness. In conclusion, it needs to be incorporated into the BC patient’s rehabilitation process from the beginning [26].
4.5 Patients with type 2 diabetes
Globally, type 2 diabetes is a significant public health issue. Even though physical activity (PA) has been shown to have positive benefits on type 2 diabetic patients, a 2009 World Health Organization (WHO) study states that 27% of the disease is caused by physical inactivity [30, 31]. To assist reduce risk factors and avoid metabolic diseases, the French National Health Authority has promoted PA since 2011 by including it as a non-medicinal therapy and an essential component of the type 2 diabetes care route. As per the “Health System Modernization” regulation passed in France in 2016, General Practitioners (GPs) are authorized to recommend adapted physical activity (APA) to patients with long-term illness (LTD) as part of their treatment plan.
The ability to prescribe APA is also granted to paramedical health professionals, such as masseur-physiotherapists, occupational therapists, and psychomotor therapists, as well as health professionals who have completed an Adapted Physical Activity Teachers (APAT) program. In order to lessen the risk factors and functional restrictions associated with his chronic illness, the intervener’s job is to help the patient gradually transition to a regular, physically active lifestyle in a safe and customized way. Patient empowerment regarding PA practice is the aim.
The main healthcare providers that are most involved in the management of type 2 diabetes are general practitioners (GPs). For diabetic patients, physical activity (PA) seems to be an essential non-pharmacological treatment in addition to a well-balanced diet. Doctors highlight a few barriers to prescribing it, though. Evaluation of the procedures, obstacles, and elements supporting French Guiana general practitioners’ prescription of PA to patients with type 2 diabetes was the goal of the Dranebois et al.’s cross-sectional descriptive survey (2022).
Improving general practitioners’ training in the domain of prescribing physical exercise, developing therapeutic education—especially for paramedical staff—and fostering collaboration among various healthcare providers all seem to be crucial. A significant benefit in the treatment of type 2 diabetes would be the creation of sport-health organizations linking sports educators and caregiver’s aides. Health insurance may employ financial incentives to encourage physical activity, but in the spirit of health promotion, local governments should provide their citizens with the necessary infrastructures to maintain or improve their health through sports. This is a challenging goal to accomplish in an area where a significant infrastructure gap is caused by rapid population growth and unplanned city expansion. Conclusively, in order to effectively treat type 2 diabetes in French Guiana, it is imperative that general practitioners have better training in prescribing PA, that appropriate PA structures be developed, and that stakeholders in the sport-health system cooperate together [30, 31].
5. Effects of sports on prescription project on patient health and well-being
Programs that promote physical exercise have been shown to have positive benefits in preventing disease progression and primary prevention. A more integrated and multisectoral primary care healthcare delivery system is called for by the French national healthcare policy, “Ma Santé 2022,” with a larger emphasis on primary and secondary preventive programs including physical exercise and health education [32]. Since 2012, Sport Santé sur Ordonnance (SSSO), a physical activity program, has been supported by the city of Strasbourg through its Local Health Contracts (CLS), allowing local physicians to prescribe physical exercise to their patients. The three-year physical activity program, which includes individual monitoring (motivational counseling and physical activity assessments), regular sport sessions (adapted physical activity in groups), and sport sessions before to or following a clinical rehabilitation phase, is available to eligible patients without delay. Approximately 4000 people (mean age = 52 years old) were enrolled in these programs at this point [32].
This study was funded by EU through the JADECARE project and examined the functional status, well-being, and impact on healthcare service consumption of patients enrolled in the SSSO program between January 1, 2020, and December 31, 2021 (N = 864; 72% of female and 28% of male participants; 88% of patients have at least one chronic condition, and 28% have at least two). It was unknown how the use of health services may develop in the future. Information was gathered from the SSSO program participant database and cross-referenced with information from the public health insurer (CPAM du Bas Rhin). The patients’ functional condition was assessed at the beginning, middle, and end of the program. The utilization of healthcare services was compared between program participants’ health insurance data and matched non-participants’ data. There was matching in terms of diagnosis, age, gender, and location of residence.
Both the physical evaluation and the patient’s impression indicated a significant improvement in patients’ functional status, according to the research. The well-being score showed a notable improvement. Comparing SSSO service users to non-users, the study of health insurance data revealed some implications on healthcare expenditures, primarily in terms of the frequency of doctor visits and medication usage. It was not possible to demonstrate the benefits across the full intervention period, though, because health insurance data were only available for the first 2 years [32].
The current study suggests that empowering patients and those who are at risk to actively participate in their own health beyond what can be accomplished by medical therapies may benefit patients’ functional status and well-being as well as the state of the economy. Rather, it requires linking many databases to identify longitudinal patient data linked to concrete actions. The results’ significance may be limited as the current study used rather simplistic methods to match SSSO service users with non-users.
The goal of a related study was to prescribe adaptive physical exercise based on the expectations of patients visiting general practitioners in the Yvelines department in Northern France [33]. Adapted physical activity (APA) has been prescribed by general practitioners to individuals with long-term health issues in France since 2016. In nine doctor’s offices, 252 patients completed surveys. 95.2% of patients believe that prescribing APA is a good concept, 80.2% of patients were inspired to enroll in an APA program, and 67.4% of patients believed that prescribing APA would boost their motivation. The biggest barriers to engaging in physical activity were a lack of time (59.9%) and motivation (31.7%). Professional group meetings (64.7%) and follow-up visits with physicians (41.7%) were the main tactics that would help patients adhere to an APA program more successfully. About 53.2% of patients stated that using a connected device to monitor their exercise would be essential. In summary, the findings demonstrated a positive attitude among patients toward APA prescription, which is noteworthy for the promotion of PA in general care [33].
6. Μovements and alliances to promote physical activity as medicine
6.1 The “exercise is medicine®” Μovement
The “Exercise is Medicine® Health Care Providers’ Action Guide” includes easy and practical methods for incorporating physical activity into everyday practice. More than 40 of the most prevalent chronic health disorders may be prevented, treated, and managed for your patients by encouraging the appropriate “dosage” of physical exercise. The global health initiative “Exercise is Medicine” exists in 37 countries worldwide. This initiative aims to promote physical activity and exercise as a treatment for the prevention and treatment of diseases. The countries participating in the initiative are as follows: Argentina, Australia, Austria, Belgium, Brazil, Canada, Chile, China, Colombia, Cyprus, Denmark, Finland, France, Germany.
Hellas, India, Indonesia, Ireland, Israel, Italy, Japan, Latvia, Mexico, Netherlands, New Zealand, Norway, Peru, Philippines, Poland, Portugal, Russia, Singapore, South Africa, Spain, Sweden, Switzerland, and United Kingdom [34].
The prescription of physical exercise by doctors is a practice that has been implemented in various countries. The Central Health Council (KESY) of Greece has approved the workout recommendation, and it is currently being implemented. Training sessions on exercise prescription are offered by the National Center “Exercise is Medicine-Greece.” Additionally, some European nations, including France, as well as the United States, Canada, Sweden, England, and Scotland, have adopted the practice of prescribing exercise. The European Federation of Sports Medicine Associations (EFSMA) has provided information. The European Federation of Sports Medicine Associations (EFSMA) established exercise prescription for health to encourage physical activity as a way of illness prevention and treatment. These countries recognize the significant health benefits of physical activity and have integrated it into their healthcare systems.
For more than 20 years, physical exercise prescriptions have been part of healthcare for the first time in Sweden, for instance. Physical Activity on Prescription (PAP-S) is an approach that combines tailored counseling with diagnosis-specific physical activity guidelines. Physical activity can be prescribed by any qualified healthcare provider with the necessary experience. The Public Health Agency of Sweden coordinates an EU-funded project to support the implementation of this method in nine other European countries (Malta, Italy, Flemish, Portugal, Denmark, Germany, Catalonia-Spain, Lithuania, and Romania). For more detailed information, you may want to refer to the Europe Physical Activity Factsheet 2021.
The ultimate goals are to promote good health and avoid noncommunicable diseases by establishing country-based physical activity on prescription (PAP) programs in healthcare systems across various nations [35].
6.2 Exercise guidelines for health and home-based rehabilitation regarding physical activity
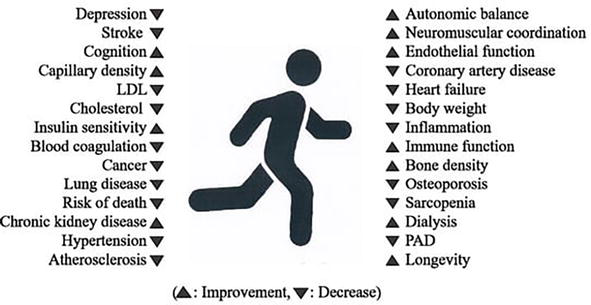
Despite being published for over 30 years, several prospective cohort studies on the benefits of regular physical activity have received little attention. However, Loellgen et al.’s research [36] has revealed evidence-based health advantages of exercise. Over a million subjects participate in activities for prevention, treatment, and rehabilitation. Sedentary lifestyle, including lack of exercise, excessive sitting and screen time, and smoking, is a major risk factor for numerous illnesses. After recovering from serious illnesses or being released from hospitals, people require rehabilitation as either inpatients at rehabilitation clinics or as outpatients in ambulant training groups or training facilities. Motivating patients to participate in an intense home-based rehabilitation program under the guidance of a certified training instructor is the main responsibility of a general practitioner. Rehabilitation and exercise training improves overall health, quality of life, physical performance, and longevity. Regular physical exercise is essential for both prevention and recovery. Physical exercise has a range of effects on numerous organs and their functioning. Figure 2 shows some of the good consequences of frequent physical activity.
Figure 2.
Some of the good consequences of frequent physical activity [36].
Long-term training typically leads to perceived improvements in activities in daily life (ADL) performance. Improved quality of life motivates patients to continue exercising on a regular basis.
The EFSMA prepared and distributed eighteen tables, which may be found at [37]. Training suggestions that are unique to everyone may be made using the sets of variables included in these tables. It is essential to create a formula that simplifies the many criteria and accounts for age, sickness risk, anthropometric data, and pre-participation test results. A fundamental stage in the intervention process to increase the desire for physical activity appears in Table 1 as a recommendation for exercise prescription for health (EPH).
The European sports physicians’ guidelines for children’s and adults’ physical activity.
Children
Engage in at least 60 minutes of moderate or strenuous physical exercise every day, including endurance, flexibility, balance, and muscular endurance training at least once.
Adults aged 18 to 65 years
Aim for 150 minutes of moderate-intensity aerobic activity each week, 75 minutes of vigorous-intensity activity, or a mix of both.
Adults aged 65 years and above
Aim for at least 150 minutes of moderate-intensity aerobic physical exercise each week, including at least 30 minutes on 5 days and 50 minutes on 3 days.
75 minutes a week of high-intensity aerobic exercise spread out throughout the week, or a similar mix of moderate-to-high-intensity exercise and moderate-to-intense strength training at least twice a week, along with muscular endurance, flexibility, and balance training.
Aerobic activity can be done at intervals of at least 10 minutes.
Elderly adults with poor mobility
Exercise to improve equilibrium avoiding falls for three or more days a week.
On at least 2 days each week, engage in muscle-strengthening exercises that target main muscle groups.
Remark: older persons should engage in as much physical exercise as their skills and conditions permit, even if they are unable to meet the recommended daily intake owing to health issues. Resistance exercise refers to physical activity when the patient works against resistance, such as weight.
Table 1.
The physical activity prescription for health (EPH).
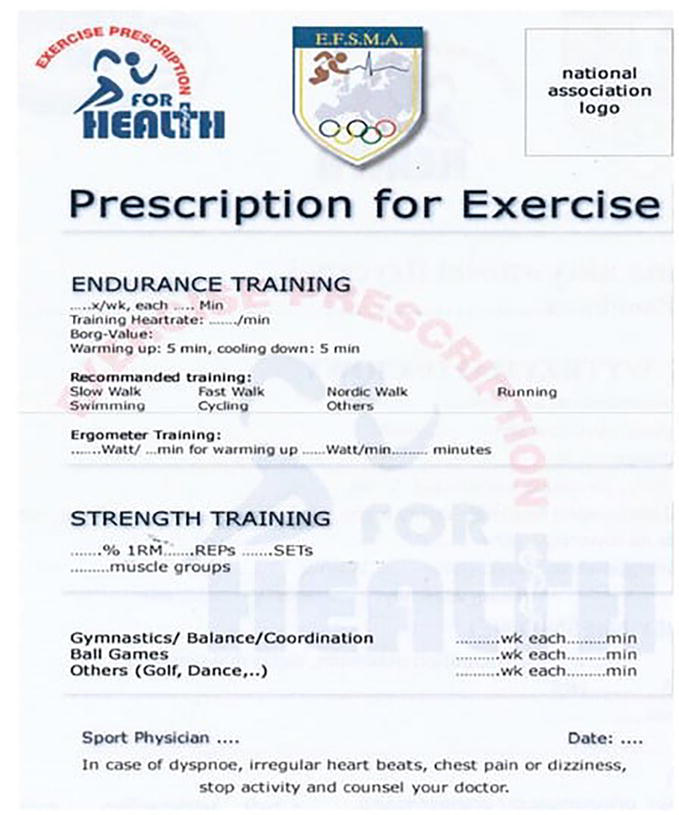
Exercise prescription for health (EPH) is a cost-effective method for motivating patients to engage in regular activity and stick to it for extended periods of time (Figure 3).
Figure 3.
The example of the recipe for the exercise prescription for health (see [36, 37]: www.efsma.eu).
6.3 The Hamburg declaration: an international alliance to promote physical activity
As a result of decreased PA, obesity is becoming a global epidemic. Children are impacted, as are all age groups. Insufficient PA leads to a great deal of issues for both people and society. Blood diseases, diabetes, heart disease, depression, and the uncontrollably rising demand on our health systems are all contributing factors, as are growing infrastructure costs and millions of dollars in lost productivity due to people’s inability to work. The solution is to encourage more individuals to move. This is the main objective of the “Global Alliance for the Promotion of Physical Activity,” which is backed by more than 139 organizations globally, including the IOC, and is spelled out in the Hamburg Declaration [38]. The main objective is to get individuals moving, regardless of their own baseline level, as a means of increasing physical activity and participation in sports. Achieving this goal will enhance people’s quality of life, save lives, save money, and promote world peace. These are the five key messages that the GA is promoting:
Promote physical activity as a kind of medicine. To spread the word that happiness, health, and well-being start at home, use role models and influencers in all facets of your life. PA is the most effective medication. Prevention is more effective than treatment.
Influencing those who make decisions. Develop tools and methods for GA members to persuade governments, corporations, and nongovernmental organizations to invest in PA to save lives, save money, and benefit society.
Adapting physical activity to individuals, communities, and environment. Individualized physical activity should take into account age, gender, socioeconomic status, cultural background, and climate conditions [39].
Make use of modern technology. Collaborate with major tech firms, pharmaceutical and healthcare organizations, and academic institutions to integrate wearable technology, cell phones, the Internet, and the metaverse into everyday life. To make it easy and fun for people to join PA, you can use gamification, incentives, and community growth.
A request for additional policy and program efficacy trials. Most knowledge on prevention comes from cohort studies. However, well-designed trials of physical exercise in communities and the healthcare system are urgently required, particularly for underserved minorities.
Licensed healthcare professionals in Swedish primary care, including physicians, physiotherapists, and nurses, can prescribe PA if they are trained in patient-centered counseling and the FaR method, as well as knowledge of the patient’s current state of health. Patients in primary care have higher levels of PA after 6 and 12 months of using the FaR technique in clinical settings. Fysisk aktivitet på recept (FaR), in English means ‘Physical activity on prescription’ (PAP-S) [40]. Implementation tools and delivery mechanisms must be easily accessible in order to reduce obstacles. Pedometer usage, the FaR method, and handbooks like FYSS are a few examples. The written prescription that results from the counseling is based on the FYSS guidebook [38].
Individual physical activity is preferred by many patients. It is said that walking is the most favored physical exercise. Pedometers are a frequent tool used by Swedish physiotherapists in response to the Swedish Council on Technology Assessment in Health Care (SBU) report to encourage greater levels of physical activity. The follow-up, which involves tracking improvement and even modifying the prescription, is crucial. It is feasible to close the gap between research and practice using a verified pedometer. The FaR system in Swedish used evidence-based strategies to promote physical activity and found that pedometer-based physical activity intervention programs had the biggest impact size [41].
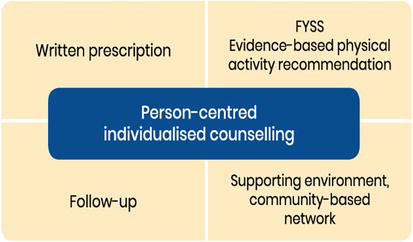
The way PAP-S’s five essential components interact is what makes it special. Individualized written prescriptions with follow-ups are produced by person-centered counseling that incorporates evidence-based, diagnosis-specific physical activity recommendations. Furthermore, healthcare providers work with local activity organizers to assist people improve and maintain their level of exercise [41, 42]. “An advantage of PAP-S in Sweden is that all licensed health professionals, with adequate expertise, can prescribe physical activity, not only doctors” (Physical Activity in the Prevention and Treatment of Disease, FYSS) (Figure 4).
Figure 4.
The PAP-S approach consists of five key components [40].
7. Authority and barriers in adaptive exercise prescription
7.1 Primary care doctors’
The “exercise pill” has never been more consistently recommended by scientific evidence and international standards for a wide range of chronic diseases, emphasizing the necessity of customizing the prescription to the patient’s circumstances (much as with pharmacological prescriptions). But does medicine actually recommend physical activity? Are medical professionals qualified to recommend exercise? Do fitness experts possess specialized knowledge about modifying exercise for those with long-term medical conditions? [43].
Based on current statistics, it appears that doctors still seldom prescribe structured, individual physical activity, and there is a significant cultural difference in the training that separates doctors from other healthcare providers [44]. Lack of a wide geographical network of facilities appropriate for the application of physical exercise programs as medical treatments for the primary chronic and noncommunicable illnesses makes a successful implementation even more difficult.
Based on these presumptions, the study by Battista et al. [43] examined the effects of a Massive Open Online Course (MOOC) on the functional assessment, recommendation, and usage of individually tailored physical exercise in medicine. This particular kind of instruction aims to close the gap between clinical settings and gyms by offering unique, cutting-edge, and engaging higher education tactics. “Exercise in Medicine: From Functional Evaluation to Adapted Exercise Training” is an MOOC that is made available to the public worldwide as an open-access educational resource by the Sports and Exercise Medicine Division of the Department of Medicine at the University of Padova (Italy).
Experts from across the world may share their thoughts and ideas through the e-learning platform Future Learn, which is facilitated by qualified educators. Additionally, this interactive MOOC can help worldwide projects focusing on exercise in medicine creating a network.
The ultimate goal of the MOOC is to teach participants how to include exercise as a medical treatment into healthcare systems and how to use functional evaluation for adapted exercise prescription. MOOC is a suitable educational method for physicians’ training. Worldwide, there is currently a deficiency in training about functional evaluation and prescription of exercises. The primary obstacle to prescribing and implementing exercise in everyday practice, according to several healthcare and fitness experts, is an ability gap that must be filled via training.
Given the excellent user satisfaction ratings that the MOOC has garnered, it appears that professionals with an interest in the subject matter find that the autonomous learner-centered training modalities and communication facilitate their ability to meet their requirements and accomplish the learning objectives [43].
To create a society that is healthier and more physically active in the future, healthcare and fitness experts, as well as the general public, need to start by sharing instructional materials and projects. For these strong reasons, policymakers and all major medical higher education institutions should have customized exercise prescription as a shared goal.
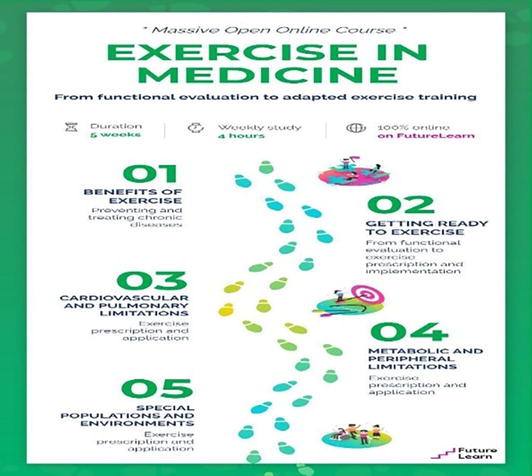
The authors suggested that fundamentals and advantages of a physically active and healthy lifestyle should be promoted among the public, and all health professionals should possess at least a basic understanding of how to prescribe and implement individualized exercise programs. In the constraints of their own surroundings, everyone will be able to contribute to the creation of a more active and hence healthier world in this way (Figure 5) [43].
Figure 5.
A diagram that summarizes the subjects covered in each course week. See the weekly summary of each week’s theme content may be viewed by clicking on [45].
Considerable new information was obtained from Tchirkov et al.’s meta-analytic study [46], which examined the challenges that doctors, and their patients continue to face, and which impede the usefulness and accessibility of adapted physical activity (APA). About 22 French medical theses between 2016 and 2020 were included in this meta-analysis. According to this study, General Practitioners (GPs) in France are now able to recommend APA to patients who have a long-term disease as a result of recent legislation aimed at modernizing the healthcare system (the 2016 French Healthcare Act and its Implementing Decree). The results showed that, during the time period under investigation, relatively few general practitioners prescribed APA in spite of the new laws. Insufficient time during consultations, inadequate training, uncertainty regarding patient referrals for APA, and skepticism toward APA practitioners seemed to be the primary barriers to APA prescription as a nonpharmacological treatment. The choice to prescribe APA appeared to be influenced by the GP’s lifestyle, the nature of the patient-physician connection, and the GP’s assessment of the patient’s attitude toward sports. Neither the scientific literature nor the most current regulations pertaining to the introduction of APA prescription in France have given much consideration to the perspective of general practitioners (physicians). The results of this meta-analysis indicate that further study and legislation are required, with a focus on taking into account the viewpoints of prescribing doctors and their interactions with patients.
The data in the single-case studies that were taken from the theses, which were frequently characterized by poor statistical significance and based on very small and unrepresentative samples, should be the first consideration when assessing the representativeness of the data in the present meta-analysis. Another theory is that the general practitioners who consented to take part in the research listed above were the ones who were most in favor of the APA’s prescription. Therefore, less weight was given to the opinions of general practitioners who disagreed with APA prescriptions. Between the interviewers, who were interns, and their interviewees, general practitioners who frequently oversaw interns, there was also a certain level of familiarity or respect [46].
The single-case studies that were taken from the theses, which were frequently characterized by poor statistical significance and based on very small and unrepresentative samples, were the first of the meta-analysis’ shortcomings. Additionally, there was a certain level of familiarity or deference between the interviewees (GPs who frequently oversaw interns) and the interviewers (interns). This meta-analysis was based on 22 internist medical theses that examined general practitioners’ opinions on APA. A lot of quantitative data revealed distinct patterns and provide a current summary of APA prescription practices in France.
Tchirkov et al.’s [47] literature review on the use of adapted physical exercise to treat chronic illness examined barriers to prescription. As physical exercise has been linked to so many health advantages, especially for chronic diseases, it is now recognized as a stand-alone therapy. Nonetheless, general practitioners continue to prescribe physical exercise infrequently and face many challenges. This study of the literature aims to pinpoint these challenges for doctors and patients with chronic illnesses, specifically in France. The literature evaluation was based on 44 relevant publications that were kept from peer-reviewed journals, medical theses, and public health reports that were published in either French or English between 2000 and 2020.
The biggest barriers for doctors to recommend adapted physical activity were time constraints during consultations, a lack of training, and ignorance of adapted physical activity or where to direct patients. Other barriers were the nature of the relationship between the physician and the patient or the personal habits and views of the doctors about physical exercise. Patients’ obstacles included not having enough time or desire, limited access to “sport for health” programs, and cultural distancing from physical activity. Noncompliance was found to be correlated with age, educational attainment, or socio-professional category.
The findings pointed to many directions for raising prescription rates and enhancing compliance with adapted physical activity. Enhancing medical education in this area, creating guidelines to make prescription processes easier, assessing patients’ physical and psychological states, and reducing socioeconomic disparities that affect people’s access to health services and physical exercise are a few examples. In order to mainstream health standards and accomplish public health goals, the main goal of “sport for health” programs is “to convert the person’s lifestyle into a physically active one” [48]. There are still numerous challenges in the way of efforts to enhance the health of individuals with chronic illnesses and encourage adaptive physical exercise. Neither patient expectations nor medical training nor practices have yet to firmly establish the recommendation for adapted physical activity.
The descriptive Survey of General Practitioners in Prescription Physical Activity: Case of Khouribga Province, Morocco, revealed similar results [49]. The study was conducted in 2021 between April and June to assess the general practitioners’ (GPs’) understanding of prescribing adapted physical activity (APA), as well as their viewpoints, experiences, feelings, and barriers to doing so (PA). According to the findings, 92% of general practitioners advised patients to get APAs. Just 6.41% of the physicians provided quantifiable goals to be met (the amount of time and frequency of physical exercise), and none of them said they provided a comprehensive program that specified the kind, level of intensity, frequency, and length of each session. Prescriptions from the APA were practically 100% oral.
The least common approach was the written prescription, while 30.58% of respondents gave a PA information leaflet. Both autonomy and quality of life are intended to be preserved by the planned APAs. The patients’ lack of enthusiasm, lack of time, and ignorance of the subject matter were the biggest obstacles to the prescription. Both the quantity and effectiveness of medical prescriptions for APA would surely be enhanced by better knowledge on APA prescription procedures and the frameworks that provide collaboration with sports medicine services and sports medicine educators [49].
7.2 Toolkit for fitness trainers and instructors
Important research [50] aimed to improve knowledge, skills, and self-efficacy among Adaptavie workers. After conducting focus groups and reviewing research, Adaptavie’s kinesiologists collaborated to develop an APA toolkit to meet this requirement. The APA toolkit demonstrated great usability and integrity, leading to increased knowledge and self-efficacy in the workplace. Kinesiologists reported that the toolkit improved knowledge, abilities, and confidence in accessing credible APA resources, leading to a substantial improvement in job self-efficacy after 1 year of use. Given that the toolkit’s prescriptions are supported by empirical data, kinesiologists who utilize it to prescribe APA may find that their clients with impairments benefit more from it. Personalized physical exercise programs have been linked to increased involvement, motivation, personal growth, and self-efficacy. The toolkit’s availability in both paper and electronic versions, as well as in French and English, should aid in its adoption and possible application in the field [50].
This study has limitations due to the limited sample size of kinesiologists from a single community group. Other health professionals that offer APA services include coaches, physical education experts, occupational therapists, and physiotherapists; these professionals were left out of this study. Furthermore, throughout the research period, there were personnel changes, and kinesiologists’ availability varied (e.g., through part-time work or a severe workload). As a result, there was variation among responders throughout the research.
Adaptavie highlighted the need for an evidence-based toolbox to promote knowledge and self-efficacy in delivering APA services for individuals with disabilities. The toolbox boosted self-efficacy in the workplace, and all participants found it useful. The future plan includes expanding the toolkit to additional community groups with comparable needs and incorporating it into the Quebec university curriculum for kinesiologists, where APA training is currently lacking [50].
The global project “exercise prescription for health and disease prevention” has its roots in antiquity, almost two millennia ago. Hippocrates of Greece was the first “recorded” physician to write an exercise prescription for a patient suffering from consumption, and Galen of Rome’s guidance on the use of exercise for patients in illness treatment remained influential until the sixteenth century. Exercise has historically been linked to diabetes, obesity, and inactivity as some medical practitioners have recommended it to reduce these health concerns. For both the body and the mind, “Exercise is Medicine” is among the most important healthcare concerns of the twenty-first century. Exercise is a modifiable lifestyle component as research has shown that it has a positive impact on holistic human performance across the lifetime. The lack of training appears to be the most significant barrier to the universality of PA prescription. Training organization and the development of particular tools for attending physicians appear to be interesting alternatives. The fourth most common cause of mortality worldwide is physical inactivity. Physical activity (PA) prescriptions by doctors are now outlined in legislation that emphasizes the primary role of family physicians. It is needed to be done more research on general practitioners’ (GPs’) needs regarding prescribing PA. It is proposed that enhancing individual motivation and ability in addition to using a systems approach (socio-ecological model) is necessary for the effective use of PA in healthcare [41].
Policymakers, healthcare leaders, and professional groups should all provide general support. Facilitating the process requires easily accessible implementation tools and delivery systems. Examples include evidence-based guidelines like FYSS and physical activity on prescription systems, as well as strategies like using pedometers. According to Hellenius and Sundberg [51], the FYSS book has been translated into English, Norwegian, and Vietnamese. Talks about translating it into other languages are still in progress. Swedish Professional Associations for Physical Activity actively seek international collaborators for future translations.
It has been proposed that a systems approach (socio-ecological model) and the development of personal motivation and competence are necessary for the successful use of physical activity counseling in healthcare [52]. To begin, legislators, healthcare leaders, and professional associations must all provide their support.
These actions boost motivation by raising awareness and validity.
References
1.Barbin J, Camy J, Communal DMF, Perrin C, Vergnault M. Référentiel d’activité et de compétences de l’enseignant en activité physique adaptée. 2015. Available from: http://pmbsoie.univlyon1.fr/doc_num.php?explnum_id=512
2.Thornton JS, Frémont P, Khan K, Poirier P, Fowles J, Wells GD, et al. Physical activity prescription: A critical opportunity to address a modifiable risk factor for the prevention and Management of Chronic Disease: A position statement by the Canadian academy of sport and exercise medicine. Clinical Journal of Sport Medicine. 2016;26(4):259-265. DOI: 10.1097/JSM.0000000000000363
3.Harvard-School of Public Health [Internet]. 2023. Available from: https://www.hsph.harvard.edu/nutritionsource/physical-activity-considerations-special-populations/
4.JADECARE insights in original Good Practice transfer: Effects of ‘Sports on Prescription’ on Patient Health and Wellbeing. 2023. Available from: https://www.jadecare.eu/jadecare-insights-in-original-good-practice-transfer-effects-of-sports-on-prescription-on-patient-health-and-wellbeing/
5.Plato, Theaetetus 153a-c
6.Tipton CM. Historical perspective: The antiquity of exercise, exercise physiology and the exercise prescription for health. World Review of Nutrition and Dietetics. 2008;98:198-245. DOI: 0.1159/000152989
9.Kleisiaris CF, Sfakianakis C, Papathanasiou IV. Health care practices in ancient Greece: The Hippocratic ideal. Journal of Medical Ethics and History of Medicine. 2014;7:6
13.Pavlogiannis O, Lomi C, Albanidis E, Konitsiotis S, Geroulanos S. Sport and medicine during Greek antiquity and roman imperial times. Journal of the Washington Academy of Sciences. 2007;93(1):59-75. Available from: http://www.jstor.org/stable/24536252
14.Plutarch, De liberis educanids 10.; Plutarch, De liberis educanids 9
15.Galen, De sanitate tuenda libri VI.85; Galen, Thrasybulus IX 820; Galen, Thrasybulus XXVIII 858; Galen, Thrasybulus IV 811-813; Galen, Thrasybulus XXXV 872-873
18.Yiannakis T. History of Physical Education (in Greek). Athens: Self-published; 1998. pp. 17-20
19.Berryman JW. Exercise is medicine: A historical perspective. Current Sports Medicine Reports. 2010;9(4):195-201. DOI: 10.1249/JSR.0b013e3181e7d86d
20.Joelsson Μ, Lundqvist S, Larsson MEH. Tailored physical activity on prescription with follow-ups improved motivation and physical activity levels. A qualitative study of a 5-year Swedish primary care intervention. Scandinavian Journal of Primary Health Care. 2020;38(4):399-410. DOI: 10.1080/02813432.2020.1842965
21.Pedersen BK, Saltin B. Exercise as medicine - evidence for prescribing exercise as therapy in 26 different chronic diseases. Scandinavian Journal of Medicine & Science in Sports. 2015;25(Suppl. 3):1-72. DOI: 10.1111/sms.12581
22.Allado E, Poussel M, Albuisson E, Paysant J, Temperelli M, Hily O, et al. Real intensity of physical activity capacity of patients with chronic disease: A cross-sectional study. Scientific Reports. 2022;12(1):12593. DOI: 10.1038/s41598-022-17047-9
23.Clanchy KM, Tweedy SM, Trost SG. The adapted physical activity program: A theory-driven, evidence-based physical activity intervention for people with brain impairment. Brain Impairment. 2019;20(1):81-95. DOI: 10.1017/BrImp.2018.16
24.Asonitou K, Mpampoulis T, Irakleous-Paleologou H, Koutsouki D. Effects of an adapted physical activity program on physical fitness of adults with intellectual disabilities. Advances in Physical Education. 2018;8:321-336. DOI: 10.4236/ape.2018.83028
25.Bernhardsson S, Boman C, Lundqvist S, et al. Implementation of physical activity on prescription for children with obesity in pediatric health care (IMPA): Protocol for a feasibility and evaluation study using quantitative and qualitative methods. Pilot and Feasibility Studies. 2022;8:117. DOI: 10.1186/s40814-022-01075-3
26.Murri A, Vitucci D, Tranchita E, Grazioli E, Gori S, Modena A, et al. “OPERATION PHALCO”—Adapted physical activity for breast cancer survivors: Is it time for a multidisciplinary approach? Cancers. 2023;15:34. DOI: 10.3390/cancers15010034
27.Schutz S, Aidar FJ. Different methods of physical training applied to women breast cancer survivors: A systematic review. Frontiers in Physiology. 2021;12:639406
28.Natalucci V, Villarini M, Emili R, Acito M, Vallorani L, Barbieri E, et al. Special attention to physical activity in breast cancer patients during the first wave of COVID-19 pandemic in Italy: The Diana web cohort. Journal of Personalized Medicine. 2021;11:381
29.Galiano-Castillo N, Arroyo- Morales M. The six-minute walk test as a measure of health in breast cancer patients. Journal of Aging and Physical Activity. 2016;24:508-515
30.Millor N, Lecumberri P. An evaluation of the 30-s chair stand test in older adults: Frailty detection based on kinematic parameters from a single inertial unit. Journal of Neuroengineering and Rehabilitation. 2013;10:86
31.Dranebois S, Lalanne-Mistrih ML, Nacher M, Thelusme L, Deungoue S, Demar M, et al. Prescription of physical activity by general practitioners in type 2 diabetes: Practice and barriers in French Guiana. Frontiers in Endocrinology. 2022;12:790326. DOI: 10.3389/fendo.2021.790326
32.Schuster C et al. Effects of a sports on prescription project on patient health and wellbeing. International Journal of Integrated Care. 2022;22(S3):249. DOI: doi.org/10.5334/ijic.ICIC22249
33.Kanso C, Blanchard J-C, Astruc A. P07-02 prescription of adapted physical activity: Expectations of patients consulting general practitioners in the department of Yvelines. European Journal of Public Health. 2022;32(Supplement_2):ckac095.102. DOI: 10.1093/eurpub/ckac095.102
34.Exercise is Medicine. Available from: https://www.exerciseismedicine.org/eim_map/
35.An effective model to increase physical activity. Available from: https://www.eupap.org/
36.Loellgen H, Zupet P, Bachl N, Debruyne A. Physical activity, exercise prescription for health and home-based rehabilitation. Sustainability. 2020;12(24):10230. DOI: 10.3390/su122410230
37.European Federation of Sports Medicine Associations. Available from: www.efsma.eu
38.Andersen P, Holmberg S, Årestedt K. et al. Factors associated with increased physical activity among patients prescribed physical activity in Swedish routine health care including an offer of counselor support: A 1-year follow-up. BMC Public Health. 2022;22:509. DOI: 10.1186/s12889-022-12940-4
39.Heath GW, Parra DC, Sarmiento OL, Andersen LB, Owen N, Goenka S, et al. Lancet physical activity series working group. Evidence-based intervention in physical activity: Lessons from around the world. Lancet. 2012;380(9838):272-281. DOI: 10.1016/S0140-6736(12)60816-2
40.20 years of Swedish experience with prescribed physical exercise. Available from: https://eurohealthnet-magazine.eu/physical-activity-on-prescription-exporting-20-years-of-swedish-experience/
41.Raustorp A, Sundberg CJ. The evolution of physical activity on prescription (FaR) in Sweden. Schweizerische Zeitschrift für Sportmedizin und Sporttraumatologie. 2014;62(2):23-25. DOI: 10.34045/ SSEM/2014/10
42.Lundqvist EB, Björk MP, Bernhardsson S. Physical activity on prescription in Swedish primary care: A survey on use, views, and implementation determinants amongst general practitioners. Scandinavian Journal of Primary Health Care. 2024;42(1):61-71. DOI: 10.1080/02813432.2023.2288126
43.Battista F, Sarri C, Foccardi G, Quinto G, Faggian S, Vecchiato M, et al. “Exercise in medicine: From functional evaluation to adapted exercise training”: A massive open online course to respond to the burning need for exercise prescription to combat chronic diseases. Deutsche Zeitschrift für Sportmedizin. 2023;74:193-196. DOI: 10.5960/dzsm.2023.574
44.Foccardi G, Hansen D, Quinto G, Favero C, Coninx K, Ruiz GR, et al. How do general practitioners assess physical activity and prescribe exercise in patients with different cardiovascular diseases? An Italian pilot study. European Journal of Preventive Cardiology. 2021;28:e20-e24. DOI: 10.1177/2047487320925221
45.The weekly summary of each week's theme content in each online course of MOOC. Available from: https://view.genial.ly/637f8df025d1600011c4c092
46.Tchirkov V et al. Methods and barriers to the prescription of physical activity to patients with chronic illness: The viewpoint of general practitioners. American Journal of Biomedical Science and Research. 2023;19(1):64-70. DOI: 10.34297/AJBSR.2023.19.002551
47.Tchirkov V, Didierjean R, Schuft L. Adapted physical activity to treat chronic disease: A literature review of obstacles to prescription and compliance. Trends in Medicine. 2021;21(3):1-5. DOI: 10.15761/TiM.1000274
48.Barth N, Perrin C, Camy J. Engaging in regular physical activity when you have type 2 diabetes: Between “disease trajectory” and “adapted physical activity (APA) career”. Loisir et Société/Society and Leisure. 2014;37:224-240
49.Imad FE. Survey of general practitioners in prescribing physical activity: Case of Khouribga Province. Journal of Medicine and Public Health. 2023;4(7):1087
50.de Serres-Lafontaine A, Périnet-Lacroix R, Batcho CS, Best KL. Co-creation and evaluation of an adapted physical activity toolkit: Guidelines to support practice among rehabilitation professionals in community organizations. Physical Activity and Health. 2023;7(1):166-177. DOI: 10.5334/paah.239
51.Hellénius ML, Sundberg CJ. Physical activity as medicine – Time to translate evidence into clinical practice (editorial). British Journal of Sports Medicine. 2011;45(3):158
52.Börjesson M, Sundberg CJ. FYSS (physical activity book for prevention and treatment): Behavioural change also for the physician? British Journal of Sports Medicine. 2013;47(15):937-938
Written By
Katerina Asonitou, Soteria Yiannaki and Dimitra Koutsouki
Submitted: 07 February 2024Reviewed: 07 February 2024Published: 21 March 2024