
Abstract
Effective healthcare requires meaningful teamwork among individuals who have diverse knowledge, expertise, experiences, and perspectives. Members of multidisciplinary healthcare teams include many different healthcare professionals—including physicians, nurses, dentists, psychologists, nutritionists, physical therapists, social workers, technicians, researchers, staff, and administrators—as well as patients and their significant others. For multidisciplinary healthcare teams to work effectively and efficiently, it is important to understand teams, members of teams, team processes, relevant principles and practices of leadership and followership, and how to create and maintain high performing teams. This chapter describes each of these concepts; how to assess and develop team members; and how to integrate and apply three particular leadership/followership approaches to optimize or “AID” multidisciplinary healthcare teamwork: adaptive/allostatic, innovative, and distributed/shared/collective leadership and followership. In addition, this chapter discusses how to optimize cohesiveness, morale, performance, and communication of multidisciplinary healthcare teams in the ever-changing contexts in which they work.
Keywords
- leadership
- followership
- adaptive
- innovative
- distributed
- teams
- healthcare
1. Introduction
Modern healthcare is a team activity and multidisciplinary teamwork is essential in all healthcare contexts—including preventive medicine and activities to promote health and well-being; at the point of injury/accident and onset of illness; during medical transport; during visits and treatments in clinics, hospitals, and healthcare offices; in home care and hospice; while conducting healthcare research; during healthcare policy and strategic planning; and while administering and conducting healthcare procedures. The traditional, individualist, all-knowing physician working alone and making house calls is a paradigm of the past. Today, optimal healthcare requires input, performance, collaboration, and meaningful teamwork among individuals who have diverse knowledge, expertise, experiences, and perspectives, and who work in multiple settings, both in-person and virtually.
Multidisciplinary teams work across disciplines, generations, professions, and groups to determine how best to provide “STEEP”—safe, timely, effective, efficient, equitable, and patient-centered—care [1]. For multidisciplinary healthcare teams to operate effectively and efficiently, it is important to understand and apply relevant principles and practices of leadership and followership to create and maintain high performing teams.
This chapter first identifies four categories of the many types of multidisciplinary healthcare team members. Next, we discuss what constitutes a team, the two distinctive categories or roles of team members (i.e., as leaders and followers), and team processes. Then, we address how to assess and develop leaders and followers. With this information as a foundation, we describe three leadership and followership approaches that we believe are best suited to “AID” multidisciplinary teams in healthcare settings: adaptive/allostatic; innovative; and distributed/shared/collective. Finally, we present ways to optimize team morale, cohesiveness, performance, including seven strategies for high performing teams and effective communication principles and tips for team members.
1.1 Current members of multidisciplinary healthcare teams
Members of multidisciplinary healthcare teams all contribute to healthcare and well-being. These team members can be categorized into four groups:
healthcare professionals and practitioners who deal directly with patients and healthcare activities, including: physicians and nurses with a wide variety of specialties, dentists, psychologists, nutritionists, physical therapists, occupational therapists, social workers, medical equipment and laboratory technicians, case managers, counselors, spiritual advisers, and others
healthcare researchers and staff who investigate and identify healthcare best practices and who perform essential operational functions, including: scientists, administrators, fund raisers, operation supervisors, strategic planners, budget and financial analysts, physical plant maintenance workers, purchasing agents, insurance reimbursement staff, policy makers, and others
patients and their significant others who are now considered to be members of the healthcare team because it is their care and involvement that is central to mission and because they have ready access to healthcare information via the Internet
technology and artificial intelligence (AI) might also be considered as an additional group within multidisciplinary healthcare teams because of contributions to the other three groups’ activities.
These groups differ with regard to backgrounds, experiences, education, roles and responsibilities; yet all contribute to and are essential to the well-being of patients and healthcare successes and failures. The challenges for multidisciplinary healthcare teams are: (1) how to work together effectively and efficiently to obtain desired outcomes for patients; (2) to maintain and enhance the well-being of the healthcare team members; and (3) to support the mission and vision of the institutions and systems in which they work. There are opportunities for each individual to contribute meaningfully, to experience pride and joy from their contributions, and to receive support and share comradery with colleagues and the healthcare team of which they are members. For multidisciplinary teams to succeed, it is important to understand teams and team processes; the types, roles, and responsibilities of leaders and followers on teams; leadership and followership approaches best suited to multidisciplinary teams in healthcare settings; and how to maximize team performance and well-being. With such a diverse group, it also is critical to know how to optimize communication, cohesiveness, morale, individual and team performance.
1.2 What is a team?
Teams consist of “two or more individuals brought together by an organization or shared mission who are working or interacting on important common goals and are assigned different roles and responsibilities while embedded in an organizational system with linkages to the broader system” ([1], p. 128). More simply, teams are two or more individuals with different roles and responsibilities working together to achieve common goals. Effective teams are: cohesive, have high morale, communicate to achieve mutual understanding, and perform well. Effective teams also reduce errors, improve outcomes, increase job satisfaction, reduce burnout, and use resources effectively [2, 3].
1.3 Members of a team: types and their activities
Teams consist of individuals who are leaders and individuals who are followers (or team members). Leadership and followership refer to activities performed by leaders and followers.
1.3.1 Leaders and leadership relevant to teams
Day [4] defined “leader” as referring to human capital and intrapersonal knowledge, skills, abilities, attitudes, and motivations, whereas “leadership” involves social capital, interpersonal relationships, and organization culture. Of the many definitions offered for each of these words, perhaps the most common single word that describes leaders and leadership is the word “influence” [5, 6, 7, 8]. With this emphasis in mind, it is important to recognize that leaders are aspirational and inspirational individuals who influence other individuals, groups, organizations, and systems. Leadership involves the activity of influencing individuals and groups by enhancing behaviors (actions), cognitions (perceptions, thoughts, and beliefs), and motivations (why we act and think as we do) to achieve goals that benefit the individuals and groups [5, 6, 7, 8].
Many leader types have been defined, described, and championed as the “best” way to lead. But, in fact, various leader types can be effective depending on the individual leader, team of followers, situation, and context [9, 10]. A partial list of leader types and approaches (in alphabetical order) include: adaptive, affiliative, allostatic, authentic, authoritative, autocratic, change, charismatic, coercive, collective, courageous, cross-cultural, culturally-competent, democratic, distributed, facilitative, heart-centered, innovative, inspirational, laissez-faire, participative, principle-centered, resonant, servant, shared, situational, strategic, thought, transactional, transformational, virtuous, and visionary [7, 10, 11, 12, 13, 14, 15, 16, 17, 18, 19, 20, 21, 22, 23, 24, 25, 26, 27, 28, 29, 30, 31, 32, 33].
Each of these leader types and approaches has value and may be well-suited for particular individuals, teams, and situations. However, even a relatively brief description of each of these types of leaders and leadership would require many pages and we believe that is unnecessary to address all of these types and approaches in this chapter about healthcare teams. Instead, we submit that there are three types and approaches that are particularly appropriate and relevant for multidisciplinary teams in healthcare settings:
Adaptive/allostatic
Innovative
Distributed/shared/collective
These three types and approaches “AID” multidisciplinary team success in healthcare settings and are discussed in detail below.
1.3.2 Followers (team members) and followership relevant to teams
In the past, the term follower often has been used to describe individuals who are passive, dependent, or submissive. But this is not how followers are considered today. It is certainly true that leaders usually have more power and authority than do followers. But the importance of leaders is often overestimated, while the importance of followers is often underestimated. Followership refers to the activities of individuals who are not in designated leadership roles.
Followers or “team members” are members of a team who contribute (or not), align (or not) with the leader, and adapt (or not) to the situations and contexts in which they work. Follower types have received much less attention than have leader types. Robert Kelley, Barbara Kellerman, and Ira Chaleff each have written about and described various types of followers. Kelley [34, 35] proposed five follower types classified on two dimensions: dependent-independent thought and passive-active involvement:
Passive followers do not think for themselves and act passively
Conformist followers do not think critically, depend on others, and act in accordance with others
Alienated followers can think for themselves but act passively
Effective followers are independent thinkers and actively contribute
Pragmatic survivors adapt to the situation
Kellerman [36] distinguished among five follower types along the dimension of low to high engagement:
An Isolate is a person who is either physically of psychological assigned to the group, but is not engaged
A Bystander appears to be physically present and engaged, but does not contribute
A Participant is probably the most common type of follower and is engaged and contributes to the team’s activities
An Activist is engaged and also initiates conversations, offers ideas and perspectives, and suggests alternative approaches for the team to achieve its goals
A Diehard is a do or die extremist; it’s their way or no way at all
Chaleff [37, 38] focused on whether followers have the courage to either support or to oppose the leader and identified seven ways followers can either be courageous or not:
Assuming responsibility for self, team, and organization
Serving the leader
Challenging others about what is ethically and morally right
Participating in transformation if change is needed
Taking moral action if they decide to oppose the leader
Speaking to the hierarchy about the organization
Convincing leaders to listen to followers in support of courageous followership
Barry and Grunberg [39] built upon all three of these models of follower types by: using a dimension of engagement based on Kellerman and similar to Kelley’s activity dimension; adding an orthogonal dimension ranging from aligned or not aligned with the leader and/or team; and indicating that followers may or may not have the courage (per Chaleff) to align or not align with the leader. According to this integrated model of follower types (see Figure 1):
An Isolate is neither aligned or not aligned with the leader and/or team
A Bystander may appear to be aligned with the leader and/or team, but their lack of engagement leaves them essentially neutral with regard to alignment
A Participant can either align with the leader and/or team or cannot align, possibly depending on and in accordance with the alignment of the other followers
An Activist can align with the leader and/or team and contribute in ways to support the leader and/or team or cannot align and contribute in ways that oppose the leader and/or team
A Diehard is the most extreme type of follower and either aligns 100% with the leader and/or team or opposes the leader and/or team 100%
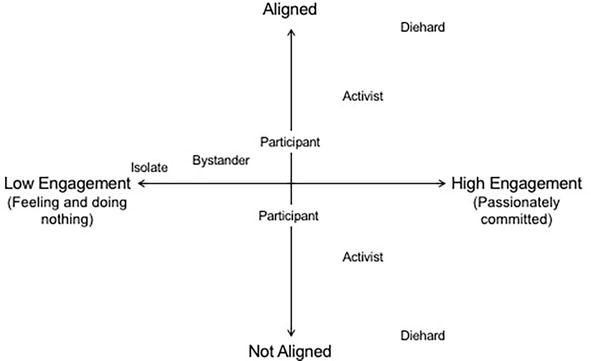
Figure 1.
Follower styles along the axes of engagement and alignment.
In Figure 1, notice that the position of the five types is not linear on the alignment dimension, but exponential as once followers start engaging, there is more evidence of alignment or no alignment with the leader and/or team.
It also is noteworthy that follower type, with regard to engagement and alignment, might vary (or adapt) depending on situations and context where context includes urgency of mission/goal, time, resources, leader and leadership types and approaches, and relationships among team members. It is also important to note that being “not aligned” is sometimes the best approach. For example, if the leader is taking the group in an inappropriate direction, then followers should have the courage to not align. Or, if the demands required to align with the leader are unreasonable or impossible, then the followers should have the courage to not align.
Each of these follower types has value and may be well-suited for particular individuals, teams, and situations. However, as indicated above regarding leader types, we submit that the three types of leader/leadership that we advocate as particularly appropriate and relevant for multidisciplinary teams in healthcare settings, also should be applied to followers/followership on multidisciplinary teams in healthcare settings:
Adaptive/allostatic
Innovative
Distributed/shared/collective
These three types of leadership/followership that AID team success are discussed in more detail below.
1.4 Team processes
Leaders and followers can interact effectively in different ways. According to Richard Hackman [40], the roles and responsibilities of leaders and team members (i.e., followers) can vary, but that it is important for all members to understand their roles and responsibilities and the team process that is operating (see Figure 2). Specifically, in:
Leader-led teams, the leader sets the overall direction, designs the team and organizational context, monitors and manages the work of the team, while team members perform the team tasks
Self-managing teams, the leader sets the overall direction and designs the team and organizational context, while the team members monitor, manage, and perform the work
Self-designing teams, the leader sets the overall direction, while the team members design the team and organizational context, monitor, manage, and perform the work
Self-governing teams, team members set the overall direction, design the team and organizational context, monitor and manage the work, and perform the tasks
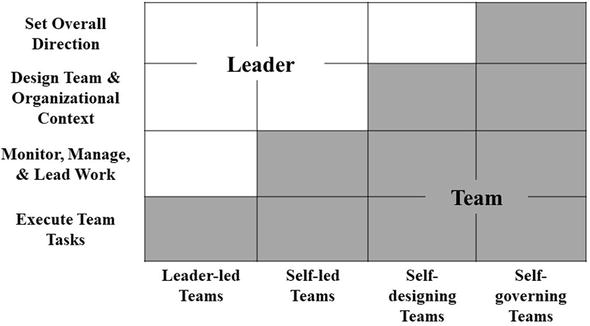
Figure 2.
Team processes based on Hackman [
As mentioned above, it is important to think about leadership and followership as activities and not as static positions [41, 42]. Based on this principle, anyone can lead and anyone can follow, from any position, anytime, anywhere. One person may lead the group in particular situations or through specific tasks while other team members follow; and other team members (who are usually followers) may either lead when they have knowledge, skills, or perspectives to share that will optimize team performance and goal attainment. To lead, you must take ownership of what you are doing and engage others to get them engaged to achieve mission and common goals.
1.5 Team processes in healthcare settings
The particular team process best suited to multidisciplinary teams in healthcare settings depends on several factors, including: knowledge, experience, skills of the team members (including leader and followers); the healthcare setting and conditions; resources available; time and urgency of decision-making and actions; potential outcomes and consequences of actions. For example, the best team process in a busy Emergency Room with an unstable patient, where decisions and actions must be made quickly differs from the best team process in a discussion of a complex, multifaceted medical case for which the patient is stable. The best team process in a field setting (e.g., at the site of a traffic accident, military conflict under fire, or humanitarian relief effort to a natural disaster) differs from the best team process during a strategic planning session among hospital financial analysts and administrators discussing what healthcare specialties or services to add or to cut and what real estate to purchase. The best team process for laboratory bench scientists studying biopsychosocial mechanisms underlying a particular disease differs from the best team process for researchers and staff conducting community outreach and gathering survey data. The best team process used by a team of experienced members who have worked together successfully for years differs from a team led by an experienced individual and staffed by novice followers. It is important for all members of a team to understand their roles and responsibilities, team process options, and which team process is being applied and why in order to optimize buy-in and meaningful participation from all members and to minimize interpersonal conflict that often results from misunderstandings or poor communication. It also is important for teams to regularly reevaluate the team process that is in effect to determine if the process should be changed as the team members and situation change.
2. How to assess and develop leaders and followers (including oneself and others): the leader-follower framework (LF2)
Regardless of individual leader and follower types as well as the team process best suited to each multidisciplinary team and each healthcare setting, it is essential to be able to assess and develop ourselves and other team members as leaders and as followers as well as assess and develop as a team. One conceptual framework for assessment and development is the Leader-Follower Framework (LF2) [5, 6] that was developed through a comprehensive review of the relevant, extant, scholarly, and historical literatures and the leader development approaches used by the U.S. Army, Navy, Air Force, Coast Guard, and Public Health Service. The LF2 includes four “C” elements—Character, Competence, Context, Communication—that are applied and interact across four psychosocial levels—Personal, Interpersonal, Team, and Organizational. We believe the LF2 provides a valuable way to assess and develop all members of teams. Each element of the LF2 is briefly explained below.
Character (Who we are) includes physical and psychological aspects of each individual. Character includes physical demographics and appearance, personality, attitudes, beliefs, and values. To know and understand our own Character requires internal self-awareness. To know and understand how others perceive and react to us requires external self-awareness. Effective leaders and followers work to develop Character in positive ways, adapting to situations, changing to meet new situations optimally, and adjusting to team processes and to other team members to optimize team morale, cohesiveness, and performance.
Competence (What we know and do) refers to the knowledge and skills relevant to perform a particular role (e.g., health care professionals, practitioners, scientists, administrators, support staff, patients, significant others). Competence also includes the broader knowledge and skills that transcend those particular roles (e.g., critical thinking, decision-making, problem solving, motivating others, conflict resolution, emotional intelligence). Effective leaders and followers work to develop Competence in themselves and others to optimize team morale, cohesiveness, and performance.
Context (When and Where we act) includes physical states outside of us (e.g., day/night; hot/cold; urban/rural), physical states within us (e.g., full/poorly nourished; rested/tired; healthy/unhealthy), our psychological condition (e.g., calm, anxious, depressed), social group and team (e.g., number of people, relationships among the individuals), and cultural (e.g., lived experiences, cultural norms, values, belief systems) environments. Context also includes effects of stress (physical and psychological) that can alter well-being, individual and team interactions, and performance. Demands and consequences of healthcare activities and outcomes are often extremely stressful and must be addressed and mitigated to avoid deleterious effects on individuals and teams, including burnout and medical errors.
Communication (How we exchange information) includes both sending and receiving information, verbally and nonverbally. Verbal communication can be transmitted in writing or orally. Nonverbal communication includes body language, spatial distance, facial expressions, and paralanguage (e.g., volume, tone, phrasing, speed). Verbal and nonverbal communication must be clear, respectful, and consistent to optimize team performance. Sending and receiving communication skills are relevant to communicate critical information and to achieve mutual understanding. Clear, understandable, and accurate information is of the utmost importance among all members of multidisciplinary teams in healthcare settings. Communication is so important to team success that Principles and Elements of Communication are presented in more detail later in this chapter.
Personal refers to each individual. Interpersonal refers to dyadic relationships and interactions among any two people, including leader with follower, team member with another team member. Team refers to all of the members (leader and followers) of the group of people who are mutually committed to common goals. Organizational refers to large groups, institutions, and systems.
3. Leadership and followership approaches for multidisciplinary teams in healthcare settings
As discussed above, there are many different types and approaches relevant to leadership and followership. The best approach depends on the individual people involved as well as the situation and resources available. However, we believe that there are three approaches that are especially relevant to multidisciplinary teams to optimize performance, mission accomplishment, and well-being of team members. We offer the acronym “AID” to help remember that the application and integration of these three approaches—adaptive/allostatic, innovative, distributed/shared/collective—will help multidisciplinary teams succeed in healthcare settings. Each of these three approaches is described below.
3.1 Adaptive/allostatic leadership and followership
Heifetz et al. [16] described “adaptive” leaders as those who use their skills and insights to respond and adapt to challenging situations; manage themselves depending on environmental demands; and help team members tolerate and respond to challenging conditions. Adaptive leaders respond effectively to variable, uncertain, complex, and ambiguous (VUCA) environments. As such, this approach is well-suited to the challenges, demands, and opportunities of healthcare situations and settings to perform effectively and to avoid burnout.
Yarnell and Grunberg [23] built upon Heifetz and colleagues’ notion by advocating for “allostatic” leaders and leadership—adaptation that includes learning, changing, and strengthening following each experience. These ideas can, and should, be considered within followers and followership as well. The process of allostasis refers to adaptive processes that involve “achieving stability through change” [43]. This type of adaptation is in response to a given situation or challenge and often results in a post-challenge strengthening. Allostatic individuals, therefore, adapt to, learn from, and change in response to experiences and challenges in ways that improve their abilities to respond effectively to future challenges and to minimize negative responses and burnout. Using a physiological analogy, increases in heart rate and blood pressure to physical or psychological stressor are adaptive and return to baseline values post-stress. In contrast, immunological responses to infections are allostatic as they adapt to the infections and are changed and strengthened post-infection to be prepared to better respond to future, similar infections. Similarly, adaptive individuals respond to challenge, whereas allostatic individuals adapt and change in response to a challenge. Both adaptive and allostatic approaches are valuable for all members of multidisciplinary teams in healthcare settings where adapting to challenge is necessary. Additionally, the strengthening post-challenge is valuable to maintain physical and psychological well-being to be well-prepared for subsequent situations and challenges.
3.2 Innovative Leadership and followership
Innovative leadership and followership emphasize acceptance of (or “structured”) change within oneself; the team members; and the skills, knowledge, and tools relevant to each situation. Innovative leadership and followership seek to maximize engagement, cohesiveness, and performance of the team. Innovative individuals constantly develop and grow by learning new, relevant approaches and unlearning old, outdated approaches. This approach also requires understanding, inspiring, and engaging followers/followership to change appropriately in order to achieve team successes, cohesiveness, and morale. Innovative leadership and followership are especially relevant to healthcare settings today because of the rapid and profound changes in knowledge and best practices, as well as current advances in technology and Artificial Intelligence relevant to healthcare issues. In fact, Metcalf et al. [44] recently addressed these issues in
Strategic activities—inspiring team members and setting organization vision and culture
Tactical activities—influencing team members’ actions and organization systems and processes
Holistic activities—aligning team members with their organization
Self-awareness—consisting of internal self-awareness (i.e., awareness of our values, personality, style, strengths, biases, and so on) and external self-awareness (how others perceive our values, personality, style, strengths, biases, etc.)
In addition, it is relevant to consider and develop the seven elements central to the Innovative Leadership Framework. These elements are categorized either with regard to Individual Development (for oneself and others) or Organizational Development:
Elements of Individual Development
Leader type refers to core predispositions, traits, and attitudes
Developmental perspective is how to make sense of experiences
Mindset includes beliefs, attitudes, and assumptions that guide thoughts and actions
Resilience is the ability to adapt to change
Skills and behaviors are specific abilities and actions
Elements of Organizational Development
Organizational context and situational analysis involve understanding interactions with teams and organizations
Lead followers and organization to optimize wellness and performance of team members
3.3 Distributed/shared/collective leadership and followership
In addition to applying leadership and followership approaches to multidisciplinary health settings that emphasize Adapting and Innovating, it also is essential for the members of healthcare teams to understand and embrace approaches that allow and encourage those team members (i.e., designated leaders and followers) who have the most relevant knowledge, skills, perspectives to perform leadership activities. There are three related, but distinct, approaches to achieve this type of team activity: distributed, shared, and collective leadership and followership. Each of these approaches is of value to teams in healthcare settings. Which of these related approaches is optimal, depends on the members of the team, situation, and the context.
3.3.1 Distributed Leadership and followership
Distributed leadership and followership focus on distributing the leadership and followership roles, tasks, and decision-making authority across various individuals or teams within an organization depending on the situation and context. This approach often involves different units or departments within an organization, where leadership responsibilities are divided based upon knowledge, skills, and specializations enabling a flexible, adaptive structure. Distributed leadership and followership emphasize interactions among units and team members [24, 25, 26].
3.3.2 Shared leadership and followership
Shared leadership and followership emphasize the active participation and collaboration among all members of the team who, as a whole, collectively influence and guide the group’s decisions and activities. The key to shared leadership and followership is the influence of the group versus the influence of one or a few members of the group. This approach usually occurs within a specific small team, where team members collaborate and share leadership and followership responsibilities based on their differences in expertise. Shared leadership and followership involve all team members contributing to the team’s performance in service of mission and goals where every team member assumes responsibility for their contributions to the team and mission [27, 28, 29, 30].
3.3.3 Collective leadership and followership
Collective leadership and followership emphasize collaboration and equal participation among all members, regardless of each individual’s roles or positions. The focus is on leveraging diverse perspectives and fostering a sense of shared ownership. This approach is more holistic and encompasses the entire organization or community—everyone is encouraged to contribute their own unique insights, perspectives, knowledge, and skills to achieve the common goal. This approach maximizes inclusive and democratic decision-making process [30, 31, 32, 33]. Collective leadership and followership emphasize consensus building and, where necessary, conflict resolution regarding team-relevant decisions requiring mutual trust, effective communication, and shared learning among team members as roles and responsibilities shift [45]. Collective leadership and followership emphasize transformation, participation, collaboration, and commitment [46].
4. How to optimize team morale, cohesiveness, performance
Understanding leaders/leadership, followers/followership, team process options, and leadership and followership approaches will help to optimize multidisciplinary team cohesiveness, morale, and performance in healthcare settings. It is important to be aware of and to apply strategies that are central to high performing teams. In addition, it is useful to be aware of characteristics of effective versus dysfunctional teams.
4.1 Seven strategies for high performing teams
There are seven strategies to optimize performance of teams.
4.1.1 Vision
Creating a clear vision, sense of purpose, and goal(s) for the team is extremely important and is built on communication. Without a clear vision or sense of purpose, teams will struggle to know what to do, to feel valued, and to want to complete the work [47]. When everyone knows the end state, the team members can work collaboratively towards the goal and hold each other accountable. This communication allows leadership to let everyone know where the team is heading, but they do not need to provide every detail about how the team will get there. Interestingly, the best way to lead a team is when the leader specifies the ends (i.e., goals) but does not tell the team members exactly how to achieve the goal (i.e., the means) [40]. This strategy enables team members to offer their own ideas, approaches, and skills to achieve the team goal, allowing each team member to maximize contributions and feel valued and part of the team. In many cases, leaders assume that they need to specify both the ends and the means, yet this approach often leads to wasted human resources because it does not allow or encourage team members to offer their own ideas or maximally contribute their knowledge and skills to the work. When neither the ends or the means are specified, the result is likely anarchy—team members do not know the goal they are working towards and they do they know how to work towards that unknown goal. When ends are not specified, but the means are specified, team members have no idea what they are working towards, but they are being micromanaged and told exactly what to do, which may lead to apathy and burn out.
4.1.2 Clarity around roles
All team members need to have clarity around roles. They need to understand their own roles and responsibilities as well as the roles and responsibilities of the other team members. Without this information, individuals may unknowingly complete the same tasks, which could lead to conflict, misunderstandings, and wasted time and resources. When roles are known to all members of the team, they are able to complete their parts and also step in to help others when needed. It also allows for teams to work collectively towards the common goal and can improve decision making, action plans, and commitment to the team [47, 48, 49].
4.1.3 Respect
Teams that have mutual respect and appreciate all team members—leaders and followers—are highly effectively. Each member of the team recognizes that each individual has valuable skills and experiences to bring to the team. This perspective allows all team members to value each other and to feel valued as members of the team [47].
4.1.4 Flexibility
Flexibility is essential from all team members to allow them to adapt to on-going changes within the team and the context in which they work. In many cases, healthcare teams work in physically and emotionally challenging environments that may constantly change [50] and team members need to be aware of the context and how it is relevant to team performance [47, 48].
4.1.5 Safety
It is also important to create a psychologically safe environment for all members of a team to allow for transfer of ideas, conflict management, and movement between leader and follower roles [47, 51, 52]. Every team member should be able to speak up and to contribute to the team, including input that criticizes some aspect of the current team or identifies an emerging problem. In a psychologically safe space, all team members can offer ways to improve the team’s functioning, even if that means speaking up against the direction set by the leader or by other team members. For teams to operate with psychological safety, it is particularly important for members to [53]:
Demonstrate engagement (e.g., being present and focusing on the conversation)
Show understanding (e.g., summarize input from others and indicate understanding)
Be inclusive in interpersonal settings (e.g., express gratitude for input from others)
Be inclusive in decision making (e.g., solicit input from others)
Show confidence and conviction without appearing to be inflexible (e.g., manage effectively)
4.1.6 Manage conflict
It is important for individuals to effectively manage conflict that occurs on the team and to be aware how each team members perceives conflict. Many people have a negative perception of conflict, whereas others perceive conflict as opportunities to understand others’ viewpoints. How individuals deal with team conflict can impact team effectiveness. Adam Grant [54] distinguishes between relationship conflict and task conflict. Relationship conflict refers to personal, emotional clashes that include friction and animosity, and task conflict refers to clashes about ideas and opinions. In his research Grant found that poor performing teams focus more on relationship conflicts. High performing teams minimize relationship conflict and, instead, focus on task conflict to emphasize finding the best path forward rather than personal feelings.
4.1.7 Celebrate achievement
Individual and team achievements should be clearly valued and celebrated. When team members feel valued and respected, they will want to perform to the best of their ability to support the team. Feeling valued can build trust and cohesion and a supportive environment where teams can more effectively adapt when challenges arise.
5. Communication principles and elements to optimize team performance
As discussed above, Communication is the “how” of leadership and followership. Effective communication is critical for multidisciplinary teams in healthcare settings because whether communication is clear and understood or unclear and misunderstood can be the difference between sound healthcare versus medical errors, well-being versus injury/illness, life versus death. Effective communication also is central to establishing and building high performing teams. Therefore, we address principles and elements of communication in more detail here. The principles listed below are based on the extant psychology literature regarding persuasive communication. The elements listed below are how to best structure communication.
5.1 Principles to optimize effective communication among team members
Authenticity is best conveyed when you have high self-awareness of your values, attitudes, beliefs, biases, and genuinely express your views, interest in others, commitment to your role and responsibilities, and awareness of how you are perceived by othersClarity refers to whether information is understandable to the receiver of communicationsCognitive heuristics and biases refer to ways of perceiving and thinking that affect whether we believe, understand, remember particular information, and make decisionsConsistency of verbal and non-verbal communication is important to strengthen and reinforce a given communicationPerceived credibility refers to the credentials, expertise, or standing of an individual relevant to information conveyed and influences the impact of the communicationPerceived self-interest refers to whether the communicator has a real or perceived vested interest or personal interest in the information conveyed which can undermine or weaken their credibilityPoint/counterpoint refers to presentation of alternatives with support and opposition to the alternatives that are presentedPrimacy refers to the fact that people tend to focus on and remember information that they first receive and first impressionsRecency refers to the fact that people also focus on and remember the most recent information they receive, including “take-home” messagesRepetition refers to the fact that people focus on, believe, and remember information that is repeated“Sleeper” effect refers to the phenomenon that people tend to forget the source of information while remembering content or emotion associated with a communication. Therefore, the power of information has the greatest long-lasting effect
5.2 Elements of communication relevant to effective communication
Be present because effective communication requires senders and receivers to convey that they are genuinely interested in othersBody language , including hand gestures, touching, distance, can affirm or detract from effective communication and should be consistent with content and intentFacial expressions can be as or even more powerful and informative than words, so they must be consistent with words and communication intentHumor can be a powerful part of communication, but senders must be sensitive to receivers’ reactions, especially when conveying serious information common in healthcare settingsPhrasing of oral words within communications affects understanding (e.g., grouping subjects, predicates, asides, series, and other elements of sentences)Pitch and intonation in oral communications convey emotion and should be consistent with content and intentRhythm in speech conveys emotion, can come across as more relaxed versus more serious and, therefore, should be adjusted depending on content and intent of communicationSilence is important at appropriate points in communication for information to be processed, exchanged, and understoodTempo is the speed of delivery and depends on individual differences, culture, age, and state of arousal, and should be adjusted to maximize understandingTone of voice conveys emotions and should be consistent with content and intent of communicationsVerbal tics refer to the unintentional sounds or words that add “noise” to communications and should be avoided. They include: um, ah, you know, sort of, kind of, I mean, rightVocabulary, phrases, jargon, grammar, syntax includes words and phrases that accurately represent the information intended to be conveyed and should be understandable to receivers of communicationsVolume is how loud or soft the sender communicates verbal information and must consider setting, ambient sound, receivers hearing, and intent of communication
6. Summary and conclusions
Effective multidisciplinary teamwork in healthcare settings is essential to maximize team success and well-being. Members of multidisciplinary healthcare teams include: healthcare professionals and practitioners, healthcare researchers and staff, patients and their significant others; technology and Artificial Intelligence. To create and maintain effective multidisciplinary teams in healthcare settings, it is important to understand: types and activities of team members (including leaders and followers); team processes; how to assess and develop team members. It also is important to understand leadership and followership approaches, especially three approaches that can “AID” multidisciplinary healthcare teams: adaptive/allostatic; innovative; distributed/shared/collective. In addition, to optimize team cohesiveness, morale, and performance, it is important to practice high-performing team strategies and to communicate effectively.
Acknowledgments
References
- 1.
Higginson J, Hofler L, Hammoud MM. Principles of teamwork and team science. In: Skochelak SE, Hammoud MM, Lomis KD, Borkan JM, Gonzalo JD, Lawson LE, Starr SR, editors. Health Systems Science. Philadelphia, PA: Elsevier; 2021. pp. 127-138 - 2.
Rosen MA et al. Teamwork in healthcare: Key discoveries enabling safer, high-quality care. American Psychologist. 2018; 73 (4):433 - 3.
Bisbey TM et al. Teams of psychologists helping teams: The evolution of the science of team training. American Psychologist. 2019; 74 (3):278 - 4.
Day DV. Leadership development: A review in context. The Leadership Quarterly. 2001; 11 (4):581-613 - 5.
Barry ES, Grunberg NE. A conceptual framework to guide leader and follower education, development, and assessment. Journal of Leadership, Accountability, and Ethics. 2020; 17 (1):127-134 - 6.
Callahan CW, Grunberg NE. Military medical leadership. In: O’Connor FG, Schoomaker EB, Smith DC, editors. Fundamentals of Military Medicine. San Antonio, TX: Borden Institute; 2019. pp. 51-66 - 7.
Northouse PG. Leadership: Theory and Practice. 8th ed. Los Angeles, CA: Sage Publications; 2018 - 8.
Yukl G. Leadership in Organizations. Upper Saddle River, NJ: Pearson Education; 1981 - 9.
Day DV, The nature of leadership development. In: Day DV, Antonakis J, editors. The Nature of Leadership. Thousand Oaks, CA: Sage Publications; 2012 - 10.
Goethals G, Sorenson G, Burns J. Encyclopedia of Leadership. Thousand Oaks, CA: Sage Publications; 2004 - 11.
Bean-Mellinger B. Six Leadership Styles. 2017. Available from: http://smallbusiness.chron.com/six-leadership-styles-54300.html - 12.
Blanken R. 8 Common Leadership Styles. 2017. Available from: https://www.asaecenter.org/resources/articles/an_magazine/2013/january/8-common-leadership-styles - 13.
Boyatzis R, McKee A. Resonant Leadership: Renewing Yourself and Connecting with Others Through Mindfulness, Hope, and Compassion. Boston, MA: Harvard Business School Press; 2005 - 14.
Covey SR. Principle-Centred Leadership. New York, NY: Simon and Schuster; 1991 - 15.
Day DV, Antonakis J, The Nature of Leadership. In: Day DV, Antonakis J, editors. Thousand Oaks. CA Sage: Publications; 2012 - 16.
Heifetz RA, Linsky M, Grashow A. The Practice of Adaptive Leadership: Tools and Tactics for Changing Your Organization and the World. Cambridge, MA: Harvard Business Press; 2009 - 17.
Johnson, R. 5 Different Types of Leadership Styles. 2017. Available from: http://smallbusiness.chron.com/5-different-types-leadership-styles-17584.html - 18.
Kilburg RR. Virtuous Leaders: Strategy, Character, and Influence in the 21st Century. Washington, DC: American Psychological Association; 2012 - 19.
Lewin K, Lippit R, White RK. Patterns of aggressive behavior in experimentally created social climates. Journal of Social Psychology. 1939; 10 :271-301 - 20.
Raza, A. 12 Different Types of Leadership Styles. 2017. Available from: http://wisetoast.com/12-different-types-of-leadership-styles/ - 21.
Thornton PB. 2013. Four Types of Leaders: All Leaders Want to Change the Status Quo, but they Use Different Means. Available from: https://trainingmag.com/four-types-leaders - 22.
Crowe RP et al. Defining components of team leadership and membership in prehospital emergency medical services. Prehospital Emergency Care. 2017; 21 (5):645-651 - 23.
Yarnell A, Grunberg NE. Developing “allostatic leaders”: A psychobiosocial perspective. In: Clark M, Gruber C, editors. Leader Development Deconstructed. Cham, Switzerland: Springer International Publishing; 2017. pp. 23-50 - 24.
Whitby GB. Distributive leadership as an emerging concept. Australian Centre for Educational Leadership. 2006; 22 (2):08 - 25.
Woods PA et al. Variabilities and dualities in distributed leadership: Findings from a systematic literature review. Educational Management Administration & Leadership. 2004; 32 (4):439-457 - 26.
Beirne M. The reforming appeal of distributed leadership. British Journal of Healthcare Management. 2017; 23 (6):262-270 - 27.
Zhu J et al. Shared leadership: A state-of-the-art review and future research agenda. Journal of Organizational Behavior. 2018; 39 (7):834-852 - 28.
Carson JB, Tesluk PE, Marrone JA. Shared leadership in teams: An investigation of antecedent conditions and performance. Academy of Management Journal. 2007; 50 (5):1217-1234 - 29.
Janssens S et al. Shared leadership in healthcare action teams: A systematic review. Journal of Patient Safety. 2021; 17 (8):e1441-e1451 - 30.
Yammarino FJ et al. Collectivistic leadership approaches: Putting the “we” in leadership science and practice. Industrial and Organizational Psychology. 2012; 5 (4):382-402 - 31.
Contractor NS et al. The topology of collective leadership. The Leadership Quarterly. 2012; 23 (6):994-1011 - 32.
Friedrich TL, Griffith JA, Mumford MD. Collective leadership behaviors: Evaluating the leader, team network, and problem situation characteristics that influence their use. The Leadership Quarterly. 2016; 27 (2):312-333 - 33.
Mumford MD et al. Collective leadership: Thinking about issues vis-à-vis others. Industrial and Organizational Psychology. 2012; 5 (4):408-411 - 34.
Kelley RE. Rethinking followership. In: Riggio RE, Chaleff I, Lipman-Blumen J, editors. The Art of Followership: How Great Followers Create Great Leaders and Organizations. San Francisco, CA: Jossey-Bass; 2008. pp. 5-16 - 35.
Kelley RE. In praise of followers. Harvard Business Review. 1988; 66 :142-148 - 36.
Kellerman B. Followership: How Followers Are Creating Change and Changing Leaders. Boston, MA: Harvard Business School Press Boston; 2008 - 37.
Chaleff I. The Courageous Follower: Standing uSp to & for Our Leaders. Berrett-Koehler Publishers; 2009 - 38.
Chaleff I. The Courageous Follower. San Francisco, CA: Berrett-Koehler Publishers; 1995 - 39.
Barry ES, Grunberg NE. Healthcare teams. In: Quinn JF, White BA, editors. Cultivating Leadership in Medicine. Dubuque, IA: Kendall Hunt Publishing Company; 2019. pp. 117-130 - 40.
Hackman JR. Leading Teams: Setting the Stage for Great Performances. Boston, MA: Harvard Business School Publishing Corporation; 2002 - 41.
Green C, McBride JF. Teaching Leadership: Case-in Point, Case Studies and Coaching. Wichita, KS: KLC Press; 2015 - 42.
O’Malley E, McBride JF. When Everyone Leads the Toughest Challenges Get Seen and Solved. Portland, OR: Bard Press; 2023 - 43.
Sterling P, Eyer J. Allostasis: A new paradigm to explain arousal pathology. In: Fisher S, Reason JT, editors. Handbook of Life Stress, Cognition, and Health. Chicester, NY: Wiley; 1988 - 44.
Metcalf M et al. Leadership and Followership in the Age of AI: A Guide to Creating Your Future as Leader, Follower, and AI Ally. Phronesis Publishing; 2023 - 45.
Shonk K. What Is Collective Leadership. Daily Blog: Program of Negotiation Harvard Law School; 2023 - 46.
Collar M. 2013. Available from: https://www.shrm.org/hr-today/news/hr-news/pages/spring-2013-collective-leadership.aspx - 47.
Barry ES et al. Leadership and followership in military interprofessional healthcare teams. Military Medicine. 2021; 186 (S3):7-15 - 48.
Varpio L et al. Interprofessional healthcare teams in the military: A scoping literature review. Military Medicine. 2018; 183 (11/12):e448-e454 - 49.
Bell ST et al. Team composition and the ABCs of teamwork. American Psychologist. 2018; 73 (4):349 - 50.
Ervin JN et al. Teamwork in the intensive care unit. American Psychologist. 2018; 73 (4):468 - 51.
Edmondson AC et al. Understanding psychological safety in health care and education organizations: A comparative perspective. Research in Human Development. 2016; 13 (1):65-83 - 52.
O’Donovan R, McAuliffe E. Exploring psychological safety in healthcare teams to inform the development of interventions: Combining observational, survey and interview data. BMC Health Services Research. 2020; 20 (1):1-16 - 53.
Edmondson AC. The Fearless Organization: Creating Psychological Safety in the Workplace for Learning, Innovation, and Growth. Hoboken, NJ: John Wiley & Sons; 2018 - 54.
Grant A. Think Again: The Power of Knowing What You Don’t Know. New York, NY: Penguin; 2021