Open Access is an initiative that aims to make scientific research freely available to all. To date our community has made over 100 million downloads. It’s based on principles of collaboration, unobstructed discovery, and, most importantly, scientific progression. As PhD students, we found it difficult to access the research we needed, so we decided to create a new Open Access publisher that levels the playing field for scientists across the world. How? By making research easy to access, and puts the academic needs of the researchers before the business interests of publishers.
We are a community of more than 103,000 authors and editors from 3,291 institutions spanning 160 countries, including Nobel Prize winners and some of the world’s most-cited researchers. Publishing on IntechOpen allows authors to earn citations and find new collaborators, meaning more people see your work not only from your own field of study, but from other related fields too.
The Local Health Unit, called ASL Roma 3, is focused on the best organizational and technological solutions that allow citizens, especially those with greater fragility and disabilities, to benefit from assistance at home. To facilitate both the collaboration between operators and citizens and the provision of telemedicine, ASL Roma 3 recently introduced Participative Art as an innovative model to empower citizens and strengthen the use of telemedicine services, modernizing its approach. Here, we describe how participative art facilitates the new model of relation between Institutions and empowered citizens, called City Competent. IPACS, Institutional & Public Coaching Services supported ASL Roma 3 with coaching and participative art to achieve change in homecare culture and positive relationships between institutional operators and citizens. As a result of upskilling in communication, negotiation, and decision making, the diffusion of telemedicine services increases, strengthening home care and remote collaboration between professionals facilitated by the City Competent Model.
CEO of IPACS, Institutional & Public Coaching Services, Italy
Daniela Sgroi
Health Director Local Health Authority Roma 3, Roma, Italy
Tiziana Chiriaco
Telemedicine and Unitary Coordination of Single Access Points Unit Manager, Local Health Authority Roma 3, Roma, Italy
Marina Cerbo
Head of Scientific Committee of IPACS, Institutional and Public Coaching Services, Italy
Francesca Milito
General Manager Local Health Authority Roma 3, Roma, Italy
*Address all correspondence to: francescacioffi2@gmail.com
1. Introduction
The NRRP [1] Mission 6 - Health - aims to strengthen and reorient the National Health Service (NHS) to improve its effectiveness in responding to people’s care needs, also considering critical issues emerged during the pandemic emergency, and is divided into two components:
Component 1: Proximity networks, intermediate structures, and telemedicine for territorial assistance.
Component 2: Innovation, research, and digitalization of the National Health Service.
Component 1 aims to strengthen the services provided in the area thanks to the improvement of territorial structures and facilities (such as Community Houses and Community Hospitals), the reinforcement of home care, the development of telemedicine, and more effective integration of all social and health services.
Telemedicine, or the provision of remote health services, represents a pillar for the innovation of health services, as it facilitates collaboration between professionals and citizens; in this view, strengthening of telemedicine services has become one of the “enabling” interventions within the NRRP to bolster digital public services and modernize the National Health Service.
The European Commission has attributed particular importance to the topic of telemedicine for over a decade.
With the European Communication “Telemedicine for the benefit of patients, health systems and society,” of November 4, 2008, a series of actions were identified that involve all levels of government, in the both community and individual Member States, to encourage greater integration of telemedicine services into clinical practice, removing the main barriers that hinder their full and effective application.
For a systematic use of telemedicine within the National Health Service and to implement European Communication, the Technical Table on telemedicine was established at the Superior Council of Health, which has drawn up specific national guidelines for:
place the priority areas of application of telemedicine.
analyze models, processes, and methods of integrating telemedicine services into clinical practice.
define common taxonomies and classifications.
define the aspects concerning the legislative and regulatory profiles and the economic sustainability of telemedicine services and performances.
Being the world-leading continent toward a truly democratic future engaged with Care at Home, the European Union faces a series of needs. In line with the 2030 Agenda—which has also been reaffirmed by Next-Generation EU—the care at home needs to be accompanied by the digital transition, which may be viewed as providing important operational support to both professionals and citizens. It is a bottom-up approach where individuals can be educated and motivated to intelligently collaborate with public sector institutions and the various levels of government. Educating and motivating such intelligent bottom-up collaboration is exactly the prerogative of the City Competent persons who result from the Competence Economy Project (www.competenceconomy.it).
In 2018, IPACS (www.ipacs.it) intercepted, with a regional survey of 30 Italian Local Health Authorities (LHA), two essential needs not satisfied in the political-institutional field: (1) developing the ability to interact and forming an alliance between the institutions and the citizens; and (2) developing attitude to work with an interdisciplinary approach, as informal leaders in action, to manage complex contexts and adapt the organization to rapid changes.
In June 2019, in an institutional event, with the patronage of the Ministry of Health and the Ministry of Cultural Heritage, IPACS validated and launched the use of Participatory Art, as a learning strategy, to accelerate the process to work with interdisciplinary perspective in action, as well as to develop policies, such as bringing telemedicine to citizens” [2, 3, 4, 5].
Competence Economy think tank (www.competenceconomy.it) introduces the new organizational and learning model that connects territorial operation centers (COT) with the hospital operation center (COO), empowering the main skill called “emotional intelligence,” essential to achieve social objectives (such as those of NRRP) and inclusiveness in a short period of time, and measuring the related impact on social economy.
During 2022 and 2023, ASL Roma 3 has carried out several activities of training for representatives of all the operational units and clinical services for the use of the digital and telemedicine systems, besides the definition of institutional procedures for telemedicine.
Moreover, in ASL Roma 3, there is an institutional office that deals with the coordination of telemedicine services with monthly meetings to manage process and applicative problems and for proposals regarding service improvement. A service center for support and resolution of IT problems is also set up.
To support the access to tele visits by patients, doctors and nurses involved in tele visit activities provide guidance and indicate to patients/caregivers how to access the system and the European Social Fund (ESF). The information is also accessible on the company website and posted in the clinics to increase citizens’ access to the ESF.
Currently, the present and future challenges for national and local institutions are to achieve the best use of the NRRP resources to strengthen telemedicine services, encourage the digitalization and reorganization of the management processes, and renovating the mode of interaction between LHA and patients, reducing distances, and increasing their digital and self-care skills.
The methodology implemented in ASL Roma 3 is based on the intention of intercepting citizens eligible to become City Competent leaders who help communities and institutions to give practical solutions and implement plan of action to address unmet social needs, specifically concerning the implementation of Care at Home and Telemedicine.
The expected impact of potential City Competent leaders will be: (1) developing the ability to interact and create alliances between institutions and the communities to reduce access inequalities to telemedicine; (2) developing an “informal leadership,” among citizens and institutions to manage complex contexts of remembrance and adapt to rapid changes of Care at Home. We are in the trend called “empowerment of the citizen” and in the OECD guideline “lifelong adult learning.” After step 1, where the potential City Competent are selected from the whole population, citizens are placed in a learning and evolution art and coaching pathway (step 2), together with the managers of public administration, to achieve the common system objective. The aim is to build communities by activating at least n.10 additional citizens for each City Competent empowered (in a ratio of 1:10). Step n.3 is aimed at certifying City Competent, putting them in a reputational list, and involving them in further system objectives useful to communities and institutions.
Adhering to the City Competent Model, citizens are allowed to access the following four benefits:
Citizens are certified as “City Competent” able to implement telemedicine, and are listed on a specific reputation ranking list.
Citizens will be part of a community recognized nationally and internationally as facilitators of “Social, Economic and Healthcare Innovations.”
Citizens will be strengthened in the meta-skills identified as strategic for their community and territory. The results will be measured with an assessment pre and post the IPACS’ integrated pathway. Results are measured as well in terms of progress in system objective plans (e.g., number of activities put in place).
The participatory Art method will ensure intergenerational and interdisciplinary exchange of experiences, practical knowledge, achievements, resources, values, mindset, and perspective.
The level of skills acquired influences people’s well-being and opens opportunities that would otherwise be precluded; on the other side, lifelong learning is useful for building and participating in contemporary society. In a society where a low level of trust in politics and democratic institutions is replaced by an innovative approach with Participative Art, which deconstructs people’s beliefs and builds a bridge between institutions and citizens, among citizens of a community, to reach specific common objectives, working, and co-creating together. We would like to emphasize that our innovative methodology starts with an analysis of the social and cultural issues, opportunities, and social needs, upon which we will build a survey to list activities and behaviors to be implemented through the empowerment of meta-skills. The IPACS’ vision, mission, and scientific results are pointed out in Table 1 and Appendix B.
IPACS is a Social Enterprise Ltd who aims to empower citizens, including managers of the Public Administration in soft skills useful for developing policies, through a skills-based economy model, which connects the system objective with the soft skills functional to it. Its mission is to perform social research, starting from the concreteness of the experience of “Competence Economy” (www.competenceconomy.it), to measure results of empowerment on individuals and target communities, after providing a learning experiential pathway, integrated with coaching and participatory art, lasting about 6 months (research protocol). Participatory art helps citizens to find common goals and benefits, to develop critical and creative thinking; coaching supports citizens to develop creative solutions to system constraints.
3. The context in which the city competent model is applied
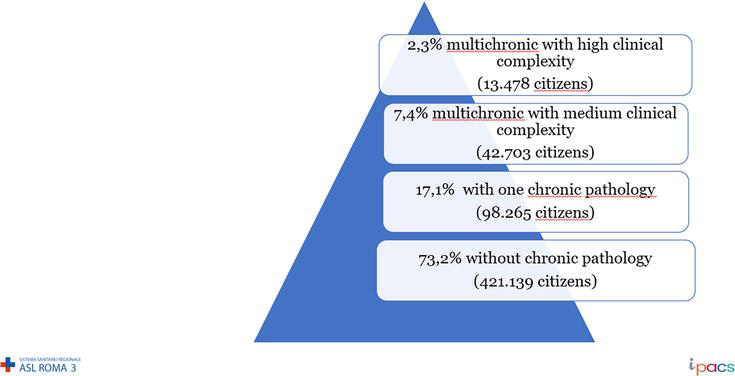
The resident population in the territory of the Local Health Institution ASL Roma 3 is equal to 575,585 people, of which 9.8% are affected by two or more pathologies. These patients, mostly elderly, require multi-professional and multidisciplinary assistance to prevent further complications, guaranteeing, where possible, permanence in the socio-family environment, with a respectful approach that protects the dignity of life of the person and the family.
Inspired by the principles of equality and fairness, the ASL Roma 3 has for years been engaged in researching the best organizational solutions that allow citizens, especially those with greater fragility and disabilities, to benefit from assistance at home.
Telemedicine, or the provision of remote health services, represents a pillar for this organizational innovation of health services, as it facilitates collaboration between professionals and their relationship with citizens, and the strengthening of telemedicine services has become one of the “enabling” interventions within the NRRP to strengthen digital public services and modernize the National Health Service.
Currently, the present and future challenges for our institution are to achieve the best use of the NRRP resources to strengthen Telemedicine services, and encourage the digitalization and reorganization of the management processes and a new mode of interaction between ASL and patients, reducing distances, and increasing their digital and self-care skills.
The ASL Roma 3 has a territorial area of 517 square km, which corresponds to the Municipalities of Rome and the territory of the Municipality of Fiumicino.
It has a catchment area of 604,787 inhabitants divided into four districts, coinciding with the mentioned municipalities.
Of the 604,787 [6] residents in the Asl’s territory, 52.39% are female and 47.61% are masculine. The demographic structure is characterized by a significant share of the elderly population (22.6% of those over 65) but with a value that does not differ from the regional average (equal to 22.8%).
The analysis of the demographic structure of the population highlights a certain lack of homogeneity in the company territory. In fact, urban areas are characterized by an older population, in particular Municipality XII, in which the fraction of people over 65 is equal to 25.7%, and of these, over half are over 75 years old.
In contrast, the coastal areas are characterized by a younger population, in particular, the Municipality of Fiumicino, in which the fraction of people over 65 is equal to 17.9%.
The ASL old age index is equal to 164.9, lower than the regional average [7], but with significant differences between the different districts, in fact in Municipality XII, the old age index is equal to 212.9, while in the Municipality of Fiumicino is 118.7.
The dependency ratio also shows how the aging population “weights” on active population, once again remaining higher in the two Roman districts (average regional 55.5 [7]).
The resident foreign population stands on average at 11.3% compared to a regional average of 10.8%, with a greater presence of immigrants regularly registered in Municipality XI.
The trend in mortality of residents in the Company, in the last decade, shows a trend decreasing, with a standardized rate of 817.1 per 100,000 in 2019, in line with the average regional.
Cardiovascular diseases, in line with the regional average, represent the leading cause of death in both women and men, followed by malignant tumors (with a slightly higher percentage than the regional figure) and respiratory diseases. Also, for other causes of death, we observe an overlap with regional data.
The analysis conducted by the Department of Epidemiology of the Lazio Regional Health Service – ASL Rome 1 (DEP Lazio) in 2021 [7] on the estimate of the healthcare needs of the ASL population highlights that 9.8% suffer from at least two chronic pathologies (2.3% of cases are characterized from high complexity), takes polypharmacological therapy, and presents, in 17.6% of cases, a socio-economic vulnerability.
The epidemiological, social, and demographic context described above, as well as the economic impact of multichronicity in the Health Service, have led the ASL to adopt an approach to chronic and multi-chronic population centered on the Case Management and Transitional Care model through the definition of personalized care paths aimed at avoiding fragmentation of care and ensuring, as far as possible, that the patient remains at its own home. This approach is consistent with the interventions envisaged by Component 1 of Mission 6, “Networks of proximity, structures, and telemedicine for local healthcare” of the NRRP [1], and materializes in a series of actions, some already carried out and others in the implementation phase inspired by the following principles:
Equity and universality: guaranteeing healthcare services to all citizens without distinction of individual, social, and income conditions.
Centrality of the person: pursuing “global” care of the person, and in particular of the person with fragility and chronicity, activating the appropriate health and social-health interventions according to the paradigm of proximity, accessibility to care, and integration between services hospital and local, with the contribution of telemedicine services.
Participation: promote the participation of citizens, associations, and the community.
Initiative healthcare: prevention and improvement of chronic disease management in every stage, from primary prevention to early diagnosis, to clinical and healthcare management, to the prevention of complications, through proactive follow-up also supported by telemonitoring and teleassistance tools, for the global management of multimorbidity.
4. Sustainability and innovative management of human resources through the creation of mixed groups composed of local health authority employees and competent citizens
The Ministerial Decree of May 23rd, 2022, n. 77 “Regulation containing the definition of models and standards for the development of territorial assistance in the National Health Service,” published in the Official Gazette no. 144 of June 22nd, 2022, identifies the qualitative, structural, technological, and quantitative standards of the structures dedicated to territorial assistance and the prevention system in the health, environmental, and climate fields. The new approach involves the use of population stratification systems and the definition of functions of the professional figures already operating within the Health Institution within the new territorial services, as summarized in Table 2.
Interdisciplinary team
Main contact for
General Practitioner, Community Doctor, Service doctor
Main contact for clinical pathway, for territory planning, and Community House activities
Nurse
Main contact for global needs analysis
Specialized doctor
Main contact for diagnostic and therapeutic complexity
Pharmacist
Main contact for pharmacological therapeutic program
Psychologist
Main contact for the assessment of psychological needs
Social worker
Main contact for the assessment of social needs
Table 2.
Main contact for the new territorial services.
Working on digital skills and the well-being of your employees becomes more fundamental than ever. Digital transformation paths represent a real opportunity to put this new concept of human resources at the center of the reorganization of service strategies.
In this context, health institutions are called upon to promote a real corporate culture oriented toward change. It is necessary to encourage a transformation of leadership roles and styles, as well as identify the skills and professional figures necessary for the management of innovation. The final goal is to become a digital organization founded on a new managerial culture, on the valorization of people’s talent and on cutting-edge digital skills. With the spread of new technologies, the complexity of the term digital competence grows today. It not only refers to a set of technological skills that go beyond the simple use of the computer but also requires flexibility and speed of learning.
A survey—carried out by Piessepi and Nomisma with the support of Gidp [8] on human resources managers belonging to a panel of leading Italian companies, which evaluated events in the last 24 months, in relation to the organization, initiatives in favor of organizational well-being and for the enhancement of digital skills—has documented that almost half of the companies involved declare having carried out technical training activities in the last 24 months, 42% have carried out soft skills training activities, and 23% have undertaken individual coaching courses that support people in their growth phase.
In fact, in addition to hard skills (such as technical-professional skills such as qualifications, experiences, and certificates), for the new health services being activated, it is necessary to evaluate additional transversal skills and aptitudes such as:
Internal transversal skills: These are the skills through which one perceives and interacts with oneself.
External transversal skills: these are the skills through which one perceives and interacts with others.
Even in the healthcare sector, it is important to introduce, in addition to the evaluation of skills in the clinical and healthcare fields, methods of evaluating soft skill indicators (behavioral attitudes) for the following additional areas:
Adaptability
Cultural contribution
Interpersonal skills
Leadership
Growth potential
Time and priority management
Analytical skills
Problem solving
Team working
Multitasking
Passion and enthusiasm
These skills, translated as transversal skills, represent the personal qualities, or rather, attitudinal characteristics, of a candidate: character traits, personal attributes, communication skills, and a whole series of signals that could facilitate success at work.
In the context of the reorganization of territorial and hospital services in light of Ministerial Decree 77 and in the realization of the objectives of the NRRP, it is therefore crucial to increase the aforementioned skills in all professionals and identify the specific skills to guide the choice of personnel who will be dedicated to the new services, and at the same time activate new staff search methods to evaluate all the aforementioned types of skills.
4.1 Sustainability
To guarantee the sustainability of the services being activated with the NRRP, beyond the time horizon of the plan, it is important to define the framework of activities and functions of the new services in order to evaluate a company standard, in addition to the personnel standards defined by the Ministerial Decree 77/2022, to identify the professionalism to be dedicated to the Territorial Operations Centers (COT), Community Nurses, Single Access Point (PUA), Community Houses (CDC), and Telemedicine Service Centre.
For example, to define an activity benchmark for the Operations Centers, it would be appropriate to evaluate the number of activations of home, rehabilitation, and residential programs and the number of services provided in the national and regional information flows.
Furthermore, for an evaluation of the population that may need telemedicine assistance for chronic patients and home services, the stratification of the same by risk profiles, through predictive algorithms, allows to differentiate the intervention strategies for the population and for taking charge of patients based on the level of risk, health needs, and consumption of resources.
In our region, it is possible to use the stratification of the population resident in the territory carried out by the SSR Department of Epidemiology (DEP). In the territory of ASL Roma 3, we have the following population stratification summarized in Figure 1.
Figure 1.
ASL Rome 3 population stratification.
Finally, the use of digital applications in the context of the activities of management of care and assistance paths allows the evaluation of workloads, duration of activities and search for benchmarks for a series of innovative performances both in favor of patients and for the cooperation with other professionals, provided in the COT, CDC, and Telemedicine Services. In this regard, the development process of the services requires the acquisition of new professional figures and the continuous integrated training of those present through a process of continuous monitoring of the required skills and abilities.
The necessary professionals will have to carry out global responsibility tasks that will accompany the patient-user in the system and will have to govern the system itself in such a way as to limit the use of acute hospital facilities to a minimum, constantly accompanying the patient, thanks to digital tools and of telemedicine, in its healthcare needs. See the summary in Table 3.
Community Houses
Physical and easily identifiable place to which citizens can access for health, social and healthcare needs. In the Community House all professionals work in an integrated and multidisciplinary manner for the planning and provision of health and social integration interventions.
7–11 Nurses 1 Social Assistants 5–8 Administrative—Social Operation support
Community Nurses
Reference professional figure who ensures nursing care at different levels of complexity in collaboration with all the professionals present in the community
1 community nurse every 3000 inhabitants
1 UCA pract. and nurse) x 100.000 inhab
Continuity of Care Unit
District mobile team for the management and support of taking charge of individuals, or communities, who find themselves in particularly complex clinical-care conditions and which involve a proven operational difficulty
1 nurses coordinator, 3–5 nurses 1–2 Operation support
Territorial Operation Center
Organizational model, which carries out a function of coordination of taking care of the person and connection between services and professionals involved in the different care settings: territorial, health and socio-health, hospital activities, and dialogs with the emergency-urgency network.
7–11 Nurses 1 Social Assistant, 5–8 Operation support
Table 3.
Standard resources and services locations in ministerial decree n.77/2022.
Appendix A summarizes the innovative human resources management introduced by Ministerial Decree 77/2022 (DM77).
In order to put in place and combine the needs for information, training in the field of digital services, telemedicine, and new healthcare models of social and health integration during 2023, the ASL Roma 3 and IPACS (Institutional and Public Coaching Services) have launched the City Competent Model on Telemedicine topics, with the aim of making citizens and operators of the ASL Roma 3 literate about the new healthcare in the area, and about the digital tools available.
Making the citizens of ASL Roma 3 literate means making sure that they understand how it works and how to access the new health care in the area, how assistance works after hospitalization at home, what are the digital tools that bring citizens closer to ASL professionals, such as they are digital self-care tools.
Literalizing the internal and external operators of ASL Roma 3 means ensuring that they understand how services are integrated into the new treatment path for fragile patients, how healthcare interventions for citizens can be improved from self-care to home assistance, how to guide citizens to access health services, such as coordinating nurses on local services.
5. Role and impact of participatory art in the competent citizen model
An interdisciplinary team of economists, artists, pedagogists, coaches, and psychologists has launched since 2021 under the coordination of Prof. Francesca Cioffi (www.competenceconomy.it), the Manifest of Competence Economy to study how emotional intelligence may enhance the ability of individuals to improve change and flexibility to accept an innovation such as telemedicine. The central idea is that enhancing emotional intelligence could empower transformative participatory citizenship. Moreover, publications [9] show that higher emotional intelligence enhances happiness and flourishing, compensates for the negative effect of perceived inequality, and creates an indirect effect on happiness and flourishing by nurturing sustainable and innovative consumption such as telemedicine’s services. Taking all these results together, the team envisages a possible future in which City Competent people can help nurture a more technological society where individuals become the main characters of their own future. In this chapter, we want to point out that telemedicine implementation is facilitated with the participative art methodology. The project will allow the testing of this last hypothesis, allowing the design of coaching and participative art activities that consider the main findings of the research to focus on elements that can enhance individuals’ emotional intelligence.
Competence Economy and City Competent Model (Empowerment Platform and Participative Art content) are covered by copyright.
Table 4 points out milestones of the City Competent Model.
Milestone
Description
Date
Measure the relationship between empowered professionals and activated citizens in a specific territory and in response to the achievement of a specific system objective, such as bringing telemedicine to citizens
The research by IPACS in 2019 and 2020 on a total of 112 Public Managers (n.41 in 2019 and n.71 in 2020) showed that 112 enhanced professionals activated around 1000 citizens. The 112 professionals were strengthened in their core skills (goal orientation, networking, and teamwork communication), reaching the achievement of 80% of the action plan. The selected and achieved system objectives have shown that the empowerment of professionals determines the ability of patients and citizens to take action (i.e., adhere to HCV drug therapy and return to follow-up).
2019 2020
Relationship between empowered professionals and activated citizens confirmed
IPACS research in 2021 on a total of about 142 empowered professionals on five soft skills (the four core plus the emotional intelligence soft skill) confirmed the relationship between one empowered professional and ten activated citizens, which is maintained at a ratio of 1:10.
2021
Strengthening the set of five soft skills (goal orientation, networking, teamwork, communication, emotional intelligence) allows the achievement of the action plan
The IPACS research in 2022 on a total of 48 professionals who worked—from an interdisciplinary perspective—with 40 citizens in the same interinstitutional meetings demonstrated that the achievement of the action plan is 100% against the strengthening of the set of five soft skills (goal orientation, networking, teamwork communication, emotional intelligence).
2022
Accelerate the implementation of strategic system objectives
The City Competent Model is aimed at creating institutional interdisciplinary roundtables composed of Citizens and Public Managers to facilitate the learning and accelerate the implementation of strategic system objectives.
6. Description of results achieved in Italy in telemedicine, since 2012
The first national guidelines on Telemedicine were approved by the General Assembly of the Superior Council of Health on July 10th, 2012. On February 20, 2014, in order to guarantee the “coordinated, harmonious and coherent development of telemedicine within the National Health Service,” the Agreement was signed between the Government, the Regions, and the autonomous Provinces of Trento and Bolzano on the document “Telemedicine – National guidelines.”
The Agreement represents a particularly relevant result considering the need to rethink the organizational and structural model of our country’s National Health Service, with respect to the fact that the diffusion of telemedicine services across the territory can constitute an important enabling factor.
The implementation of the national guidelines on Telemedicine was assessed during LEA obligations up to 2017 to verify their adoption. Since 2018, all regions have implemented the guidelines themselves with their own resolutions.
In 2019, as part of the work of the NSIS control room, the Ministry approved the establishment of a working group on telemedicine, which includes representatives of the regions Lombardia, Veneto, Emilia Romagna, Piemonte and Tuscana, as well as the National Center for Telemedicine and New Assistance Technologies of the National Institute of Health (ISS), which has created a national mapping of regional experiences and produced uniform indications across the entire national territory for the provision of remote services.
Following the State-Regions Agreement of February 20, 2014, and the Reports of the ISS COVID-19 n. 12/2020 “Interim indications for telemedicine healthcare services during the COVID-19 health emergency” of April 13, 2020 and n.60/2020 “Interim indications for telemedicine healthcare services in pediatrics during and beyond the COVID-19 pandemic” of October 10, 2020, in the meeting of the NSIS control room on July 28, 2020, the Ministry of Health and the Regions and Autonomous Provinces of Trento and Bolzano shared the need to provide uniform indications across the entire national territory for the provision of remote services, with particular attention to specialist activities, extending medical and healthcare practice beyond the physical spaces in which it usually takes place according to traditional procedures, also in relation to the initiatives launched by some regions during the Covid emergency period.
The working group on telemedicine, also integrated by experts and representatives of the national federations of health professions (FNOMCeO and FNOPI), has therefore prepared the document:
“National indications for the provision of telemedicine services,” which was approved by the NSIS control room in the session of October 28th, 2020, and was adopted with the Agreement in the State-Regions Conference of December 17th 2020 (Repertoire of documents no. 215/CSR). This document intends to provide the indications to be adopted at a national level for the provision of some telemedicine services such as tele visits, medical teleconsultation, medical-health teleconsultation, teleassistance by health professionals, telereporting, so that the possibility of using telemedicine services (e.g., tele visits for check-ups) represents a concrete element of organizational innovation in the care process.
“Indications for the provision of telerehabilitation benefits and services by healthcare professions,” which was approved by the Control Room in the session of 9 April last and was adopted with Agreement in the State-Regions Conference on November 18, 2021 (Repertory of Acts no. 231/CSR).
This document intends to provide uniform indications for the entire Italian healthcare system regarding telerehabilitation services by healthcare professionals, as well as the services that can derive from the combination of the services with each other and with other healthcare services. Just like rehabilitation, telerehabilitation also finds application in all age groups, from developmental age to the elderly, in various areas including cognitive motor, neuropsychological, occupational, communication, swallowing, behavior, cardiological, and telerehabilitation pulmonary. In consideration of their specificity, the specific aspects of the fields of cardiac and pulmonary telerehabilitation are not covered; subsequent national indication documents will be dedicated to them.
The first National Consensus Document on telemedicine for cardiovascular diseases was published: indications for telerehabilitation and telemonitoring. The document aims to define the medical indications for performing telecardiology services: the appropriate telemedicine activities are indicated for chronic patients with heart failure, arrhythmias, atrial fibrillation, chronic ischemic heart disease, adults with congenital heart diseases, and for the prevention of pathologies cardiovascular.
For this purpose, three types of services were examined: telereporting, telemonitoring, and telerehabilitation.
As part of the NRRP’s Health mission, Home as a place of care and telemedicine, the Ministry of Health has also planned the creation of a single telemedicine system, integrated with national digital health systems.
It was initiated by the notice published by Agenas as the implementing institution for the design, implementation, and management of the enabling services of the National Telemedicine Platform, as decided by the Interministerial Committee for the digital transition on December 15, 2021. The objective is to bridge the gap between territorial disparities and offer greater integration between regional health services and national platforms, through innovative solutions. The development of telemedicine is among the interventions that have made the home the first place of care. The National Telemedicine Platform is understood as the set of different services (tele visit, teleconsultation, telemonitoring, and teleassistance) which, by cooperating and interoperating in synergy, create the final services for patients and operators, guaranteeing the monitoring of the processes at the different levels of government involved.
The Organizational Guidelines containing the digital model for the implementation of Home Care (Milestone EU M6C1–4) contain the fundamental components of the telemedicine services home organizational model, with the following principal lines:
The home care service, which guarantees continuity of assistance in the modalities indicated by national and regional legislation.
The planning of home access, developed over the entire second week as provided for by the legislation, considering the clinical-care complexity of the patients.
The home care service integrated with remote telemedicine services.
It aims to contribute to the achievement of the following system objectives:
Increase the number of patients cared for at home, allowing the threshold value of 10% of patients aged over 65 to be reached.
Guarantee the entire population the same level of care and quality of care provided, improving organizational efficiency even in geographically disadvantaged contexts.
Provide the patient with assistance that includes responses to clinical-care needs and psychological needs to reduce the negative impact of the patient’s illness experience.
Reduce access to the emergency room, hospitalization, and exposure to related risks, as well as the use of institutionalization.
Allow a protected discharge from hospitalization facilities by ensuring home care continuity of assistance and equally effective treatments.
Reduce day hospital visits by developing alternative responses at home.
7. Description of impact of the city competent model on telemedicine in ASL Roma 3
The 9.8% of resident population in the territory of the Local Health Institution ASL Roma 3 is affected by two or more pathologies. These patients, mostly elderly, require multi-professional and multidisciplinary assistance to prevent further complications, guaranteeing, where possible, permanence in the socio-family environment, with a respectful approach that protects the dignity of life of the person and the family.
Inspired by the principles of equality and fairness, the ASL Roma 3 has for years been engaged in researching the best organizational solutions that allow citizens, especially those with greater fragility and disabilities, to benefit from assistance at home.
In ASL Roma 3, are active multiple telemedicine services such as teleconsultation, tele visit, telemonitoring, and home teleassistance, which were also launched through projects prior to the pandemic period and which have allowed our Institution to use the skills already acquired in strengthening home care of patients and remote collaboration between professionals.
Specifically, for the management of patients in emergency procedures, a teleconsultation service has been active since 2020 between the doctors of the Emergency Department of the Giovan Battista Grassi Hospital and the specialists of the reference Hubs hospital for the emergency networks, infectious diseases, stroke, trauma, which are at least 20 km away. Since the start of the service, approximately 2000 teleconsultations have been carried out, which confirms the importance of telemedicine as a collaboration tool between professionals involved in emergency patient care despite the territorial distance between the structures.
In line with the national and regional indications on tele visit, an institutional procedure has been adopted in our ASL, with the aim of promoting the uniform application of the rules and regulations of the legal system for the execution of tele visits for patients belonging to outpatient specialist care settings, protected discharge, local and home services, mental health outpatient services, and consultancy, and therefore to promote the improvement of the quality of the Service Healthcare.
In the outpatient setting, 12 tele visit ambulatories have been activated since 2020, at both hospital and local levels, including, since July 2020, over 5500 follow-up tele visits for follow-up and for the renewal of treatment plans for cardiological, endocrinological, and pneumological devices and drugs. Specifically for the renewal of treatment plans, the company-wide service has been active since November 2020 at the Acilia Polyclinic, and the company website “Therapeutical plans - ASL Roma 3” provides details to facilitate access by citizens to this service and to the Electronic Health Record.
Furthermore, for over 10 years, the Cardiology Unit of the P.O. G.B. Grassi Hospital has an active telemonitoring and teleassistance service dedicated to patients with cardiac devices (pacemakers, defibrillators, and loop recorders, with approximately 1450 telemonitoring), while at the Nephrology Unit, a teleassistance service has been active for about 3 years for 30 patients undergoing dialysis treatment at your domicile.
Finally, since March 2020, a teleassistance nursing service has been activated for more than 48.000 COVID-19 patients, under home management and for patients with chronic pathologies or in fragile conditions during the regional “Heat Waves” prevention campaign, in collaboration with the District Coordination and the general practitioners and pediatricians. In total, 80 users including doctors and nurses have been enabled for the system, with an institutional procedure. If, during teleassistance, the need for a re-evaluation for a chronic pathology or renewal of a cardiological, endocrinological, or pneumological therapeutic plan emerges, the nurses will contact the doctors of the company’s territorial tele visit service.
During 2022 and 2023, this service was extended to patients at greater risk of side effects from heat according to the relevant prevention regional plan. During 2023, 6553 patients resident or domiciled in ASL Roma 3 were followed via teleassistance, as follows:
Health District X Municipality: 2127 assisted.
Health District XI Municipality: 1861 assisted.
XII Municipality Health District: 1801 assisted.
Municipality of Fiumicino Health District: 764 patients.
Furthermore, in the 2020–2021 emergency period, the Mental Health Department of our Institution has remotely followed 4272 patients (2032 aged 0–17 years and 2240 > 18 years) for a total of 11,651 services, including consultations, clinical evaluations, visits medical, interviews, psychotherapy, as well as liaison activities with the bodies involved in the individual case.
8. Results of city competent model achieved in ASL Roma 3 on telemedicine driving objectives
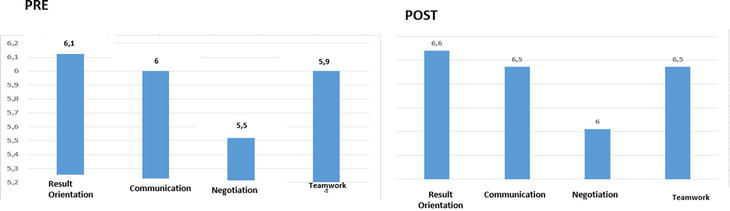
Based on the result analysis of the incoming and outcoming skill assessment test, summarized in Figure 2, we empowered the behaviors of 24 potential Competent Citizens and Local Health Authority Operators aimed at overcoming internal obstacles, in the medium term, through the result and process indicators, summarized in Table 5 for Municipalities X, XI, XII, and Fiumicino.
Figure 2.
Analysis of the assessment test in and out skills linked to the guiding objective.
Making the citizen of ASL Roma 3 literate means making sure that they understand how it works and how to access the new healthcare in the area, how assistance works after hospitalization at home, what are the digital tools that bring citizens closer to ASL professionals, what are the digital self-care tools
Indicators
1. Dedicated time-territory/area.
2. Number of virtuous behaviors performed (grounded in everyday life) in the role of City Competent (e.g. suspension of judgment regarding the ideas and opinions of others, introspection, giving feedback, asking open questions, understanding one’s own and others’ emotions and own and others’ needs, activate trust, mediate needs, mediate communications, expose oneself personally without fear of being judged, and feeling vulnerable)
3. Number of citizens and ASL operators contacted
4. Evaluation of the doctor/specialist-patient interaction
5. Comparative assessment of the needs of the front office operator (non-empathic communication) and analysis of URP complaints
6. Exam booking report analysis
7. Number of common spaces managed with volunteers, GPs, PUA operators, district
8. Number of integrated and uniformly implemented forms
9. Reduction of complaints for failure to integrate services
Literacy of the internal and external operators of ASL Roma 3 means ensuring that they understand how the services are integrated into the new treatment path for fragile patients, how the healthcare intervention for citizens can be improved from self-care to home assistance, how to guide citizens to access health services, how citizens can be improved from self-care to home assistance, how to coordinate operators in local services.
Table 5.
Impact of the City competent process on behavior, indicators, and activities in the medium term in ASL Rome 3.
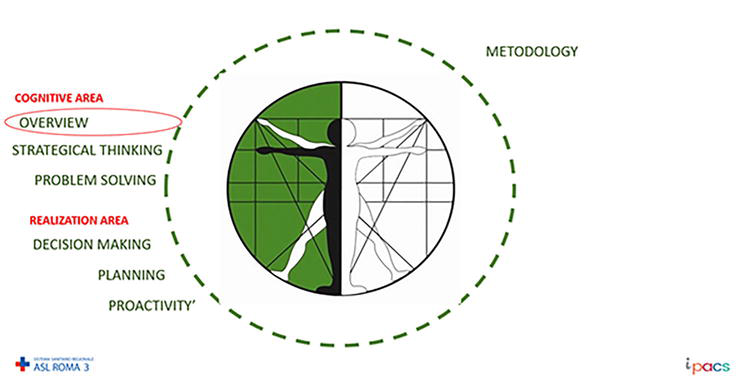
Participatory Art, with the tool of dialog and feedback, used in the co-design of two landing pages, moved the team from an approach centered on themselves, on their own vision of reality, to a vision integrated with the perspectives of others. The development of an overall vision was preparatory for the interdisciplinary team to define a working methodology and activity planning, training both the cognitive area (strategic thinking) and the implementation area (planning). The summary is shown in Figure 3.
Figure 3.
Summary of the main critical issues overcome with the tool of participatory art.
Participatory Art has trained dialog and comparison between City Competent and Institutional managers, which has facilitated City Competent to think in an analytical, strategic way and to benefit from the areas of implementation, improving planning, and decision making.
To achieve the objective of implementing telemedicine services in existing care pathways is necessaire a literacy project for operators and citizens regarding the new digital and organizational tools of the NRRP, including telemedicine. It is also helpful to start a certification process for representatives of some patient associations, operating in the territory of our ASL, as competent citizens to support the realization of the socio-health objectives of the NRRP.
Participative art accelerates the community’s empowerment in emotional intelligence soft skills, specifically concerning dialog and empathic communication.
Expanding on the issues addressed by the Competence Economy Model, digital transformation and telemedicine impose the need for new digital skills required. In turn, updating skills redesigns contents and teaching targets, including adult people needing permanent training. Work changes influence training dynamics: Lifelong learning processes become an enduring need for people in all sectors and roles. Today’s skills will not match tomorrow’s telemedicine’s services, as newly acquired skills could quickly become obsolete [10]. It has been estimated that 85% of the jobs that today’s citizens will have in 2030 have not yet been invented, and 90% will require digital skills. However, according to Digital Europe (2020), 44% of EU citizens still lack basic digital skills. In a ranking provided by DESI (Digital Economy and Society Index), Italy ranked 25th among the EU-28 in 2017, well below the European average: only 44% have “basic or above” digital skills (vs. the EU-28 average of 56%). Currently, 52% of the European workforce needs retraining due to changes in the labor market—it drops to 32% if we shorten the horizon to 2025 (Digital Europe, 2020). If we look at Italy, the numbers are further burdensome: We have 13 million adults with an eighth-grade level of education, and the estimate for those in need of retraining in the 25–64 range is up to 59%. These numbers justify the need to find new patterns of lifelong learning process, enabling fruitful overlapping between schools, universities, and workplaces to identify and satisfy the stakeholders’ needs (e.g., employer/unemployed).
Moreover, the need for hard skills must be accompanied by the development and strengthening of soft skills, such as adaptability/learnability, cognitive flexibility, and emotional intelligence. This last one is considered the attribute that is perhaps the most influential to enable all the other soft skills (such as teamwork, communication, result orientation, and managing conflicts), which are considered more and more essential for success on the one hand and also for retraining on the other. These are the skills that are hardest to understand and systematize and the skills that give—and will continue to provide—humans an edge over robots [11]. According to Deloitte (2019), two-thirds of jobs created between now and 2030 will strongly rely on soft skills. Unfortunately, we already face significant shortages, which are forecasted to worsen.
These inequalities in skills will result in inequality in access and use of resources, exacerbating the already high disparities within and between countries that have been growing again in the last few years. Participative art is aimed at changing culture through disseminating value as dialog to overcome social inequalities [12]. As emphasized by the ILO in its updated version of the “Declaration on Social Justice for a Fair Globalization” [13], labor is not a commodity, and poverty anywhere constitutes a danger to prosperity everywhere. The persistence and growth of inequalities affect social cohesion [14], calling for strengthening social justice (it can be understood as Rawlsian primary goods or as Capabilities and Functioning by Sen and Nussbaum), which should not be underestimated. Even if the concept of justice—understood in the sense of what is considered right—is a concept that varies and evolves over time according to historical, institutional, and social conditions, societies’ ambition toward instances of justice is always at work.
The access to digital medicine ensures health and health to social-economic systems, as it ensures harmony between the expectations of citizens and what is practiced is essential for stable and resilient societies. Here comes into play the role of Institutions that are called to adopt participatory patterns in promoting the capacities and skills to be productively effective in implementing telemedicine and common well-being [13]. This is of primary importance and true everywhere, even more in Europe.
The City Competent Model should be escalated to a higher part of the population to measure the impact among citizens empowered communities in realizing telemedicine system objectives.
Appendix A. Ministerial Decree n.77/2022 – multi-professional management summary
New professions. New skills translate into new digital professions, all capable of managing the complexity of new technologies. From the Data Scientist to the IoT Software Engineer, it is necessary to identify suitable figures and integrate them with those already present in the company. Furthermore, with Ministerial Decree 77/2022, transitional care management services are activated, which involve the use of multi-professional and multidisciplinary resources, with a global vision of the clinical-care pathways available and a great capacity for communication and team working relationships.
Job market. Thanks to the Legislative Decree n. 80/20211 (converted with law no. 113 of 6 August 2021), it is possible to recruit staff specifically intended to carry out the projects of the administrations for which they have direct ownership of implementation. To speed up the procedures for the recruitment of fixed-term staff for the implementation of the NRRP, it is possible for the administrations involved to stipulate fixed-term employment contracts and collaboration contracts for a total period exceeding 36 months but not exceeding the duration of implementation of the relevant projects (not exceeding 31 December 2026). Failure to achieve the intermediate and final goals and objectives envisaged by the project constitutes just cause for the administration to withdraw from the contract pursuant to art. 2119 of the civil code. Furthermore, the administrations can carry out competitive procedures relating to the recruitment of staff with fixed-term employment contracts for the implementation of NNRP projects using digital methods. To this end, the Department of Public Function has created a unique platform for recruitment in Central administrations and strategic personnel planning, with fast, transparent, and rigorous selection paths to select the technical and managerial profiles necessary for the implementation of the NRRP. The portal aims to improve the quality of public administration recruitment through an innovative digital system that simplifies and speeds up the matching of supply and demand for public jobs. To support strategic staff planning, the definition of development plans, and the identification of any training gaps, the platform will be integrated with information regarding the skills and abilities of existing staff, with the aim of valorizing the data collected through artificial intelligence and business intelligence systems. At the base, a defined set of “skills descriptors” (including soft ones, i.e., behavioral ones) to be used to compose the different professional profiles and to be used as a reference parameter for hiring policies to improve consistency between skills possessed and career paths and to design training courses starting from the actual detection of skills gaps.
To encourage the selection and rapid hiring of specialist profiles, it will also be possible to activate selection paths other than the competition, for example, through agreements with universities, higher education centers, and professional associations. The staff thus selected will be on a fixed-term contract, and the experience and skills gained may be valorized for the purposes of hiring in relation to the achievement of objectives linked to the individual projects, following a specific selection procedure.
Social Recruiting. Social Recruiting is an increasingly frequent method adopted by professionals to find work and by companies to hire new collaborators. Furthermore, through a targeted strategy on the part of organizations, it is not only possible to recruit the best candidates, but also to retain their employees.
Employer Branding. To make quality hires, the company must also be able to be chosen. For this reason, an employer branding strategy is increasingly necessary, i.e., a promotion process aimed at standing out from other organizations and attracting qualified personnel. In the context of healthcare companies, it could therefore be useful to define a social strategy aimed at finding new talent, sharing job offers, and consolidating a set of processes to promote a company as an ideal employer for a specific target that the company intends to attract, hire, and retain. In this way, it is possible to be a “great place to work,” that is, to have the image of a collaborative, stimulating work environment where it is possible to achieve company objectives thanks to a common vision – an environment from which employees can therefore benefit. Collaborators and management. This results in quality hires, loyal employees, and an increase in productivity due to the satisfaction of both management and candidates.
Evaluation of soft skills and aptitudes. The evaluation of soft skills can often make a difference and be decisive in choosing the best candidate and successfully completing the entire recruitment process. It is well known that 89% of hires are wrong due to the candidate’s lack of personality or motivation, often due to the lack of in-depth analysis of soft skills2.
Analysis of soft skills
Hard skills (such as technical and professional skills such as computer skills, university diplomas, certificates, references, and experiences) represent a good starting point in the initial phase of a recruitment process, but they are not enough: intuition, empathy, ambition, emotional intelligence, tenacity to achieve professional objectives, a strong ability to organize work, exemplary behavior in a working environment, the aptitude for team collaboration, for example, represent crucial transversal skills for starting a successful professional career, in all professional environments, even the most technical.
It is not easy to quantify and identify soft skills: it can be very complicated, for example, to identify them in a group interview because they do not always emerge from aptitude or personality tests. The quality of the questions, during a structured selection process, therefore, becomes fundamental: they must be targeted and effective to achieve the final objective. The moment of the interview is therefore central, with questions aimed at evaluating the response methods that reflect the candidates’ orientations in specific aptitudes.
During the interview, there are some precautions to keep in mind so as not to choose the wrong candidate and to avoid not achieving the desired result. Below is an example of red flags to pay attention to when trying to evaluate a candidate’s soft skills.
When candidates give canned answers. Sometimes candidates, when faced with generic and usual questions such as “Describe your role within the team,” provide standard and predefined answers. It becomes important, therefore, to add to the questions, scenarios, and hypothetical situations that take the candidate by surprise, “forcing” him to make instant reflections.
When the candidate is inconsistent. To research and satisfy a specific soft skill you do not need to focus on just one path. Comparing, for example, candidates’ answers during the interview with their emails or their performance in a certain task is a good way to evaluate the consistency of the candidate’s skills.
The candidate does not provide specific examples. A good resource must be able to relate his or her soft skills to real-life experiences. A candidate who never provides specific examples related to his life experiences is probably a resource not to focus on.
The candidate does not have a cultural fit. The best candidate is the one who has a background and mentality that fits perfectly with the culture, vision, and company logic. In this direction, the image communicated by the company through a perfect Employer Branding strategy becomes fundamental.
There are also selection process support systems that allow you to set up personalized evaluation forms for the role you are looking for, the assignment of tags, and video interviews.
Setting up the selection process with a structured analysis (also with the support of specialized companies) of hard and soft skills not only allows you to identify the correct figures for specific roles but also reduces time and the risk of staff impatience.
Employee well-being. A first step could be to introduce corporate welfare through non-monetary benefits, which have the aim of improving the well-being and quality of life of human resources and their families. Since they are not monetary compensation, the goods and services do not burden the employer’s finances and, at the same time, favor the improvement of the productivity of collaborators and employees.
Benefits of Age Management. Another factor, important for promoting the inclusion of human resources, concerns initiatives aimed at encouraging dialog and cooperation between generations, often very different in terms of skills and working approaches. Compared to recent decades, the percentage of senior workers has increased, and conversely, the number of junior figures has decreased. Age Management initiatives are therefore becoming increasingly indispensable.
Smart Working. Smart Working refers to a flexible organizational model that links digital elements to those of personal well-being. However, doing Smart Working does not simply mean “working from home.” In fact, we are talking about a real managerial philosophy, capable of bringing benefits in terms of productivity and cost reductions. Before the health emergency, only a few large companies had reaped the benefits of Smart Working. Today, however, things have changed, and other companies understand the importance of this new agile working model. Even in the healthcare sector, the areas of analysis, planning, reporting, and telemedicine activities can encourage the articulation of work even remotely, in order to promote integration between work, personal, and family activities.
Development of digital skills. Another key element of the PNRR in the field of work is the development of digital skills by Italian citizens, necessary to fully seize the opportunities offered by technological innovation, support the green and digital transition, and enhance economic growth. According to the results of the DESI Index today in Italy, only 42% of people aged between 16 and 74 have at least basic digital skills (compared to 58% in the EU), far from the 70% threshold, which the European Commission has set out to achieve by 2025. The support measures envisaged by the plan are:
Recognition of tax credits to companies that invest in training activities for digitalization and the development of related skills.
Development of a managerial retraining model (for digital), focused on SMEs with ad hoc training programs, involving the involvement of trade associations and the use of dissemination models focused on digital platforms.
Ad hoc training programs during layoff periods, incentivized through the (temporary) cut in the tax wedge for both the company and the worker, with a view to digital upskilling.
Establishment of the Digital Civil Service, a specific area of implementation of the universal civil service to enhance the role of young people as “digital facilitators” with the task of helping approximately one million users acquire basic digital skills.
Strengthening professional education, in particular Higher Technical Institutes and STEM disciplines. Greater investments planned for Higher Technical Education and infrastructural interventions, such as the preparation of learning environments connected and enriched by digital tools.
Continuous training. Most of the initiatives envisaged by the Plan are linked to active labor policies and only have a limited impact on those who are already working. However, the challenges linked to the continuous updating of skills, and the development of digital knowledge, involve the entire workforce, and corporate training takes on an increasingly strategic role for the competitiveness of companies. The doubt is that it remains limiting to talk about training almost exclusively in relation to worker mobility, relocation, and finding your first job.
In an increasingly fluid labor market like the one expected soon, the real objective will be to guarantee continuous training (lifelong learning) to all workers, and on this, the actions envisaged in the PNRR do not appear to be effective.
It is important, however, during the implementation of the interventions envisaged by the NRRP, to guarantee adequate training of staff in the use of digital systems and in the new ways of working and relating required, for example, in the management of transitional care paths or telemedicine services.
The mapping of internal skills (also within the scope of the six soft skills mentioned previously), the benchmarking with internal and external resources, and the identification of gaps, are certainly key points from which to start for the construction of more effective training paths, for activate strategic planning of new resources to be included and for the more fluid management of careers and promotions. However, to follow up on a significant change of this magnitude, administrations and staff will need coaching paths, change management programs, and specific training plans, in addition to the use of online courses and the communities of practices currently envisaged by the Plan.
In the healthcare sector, it would be appropriate to integrate the training courses already in place with the digital skills development actions and the internship in the operational realities that will be foreseen as early as 2024, such as COT, CdC, and IFEC. These integrated paths will allow entry into the world of work of personnel already oriented in the operational paths created for the implementation of the NRRP interventions. The training path should create a process of osmosis between skills also favored by the support of the technological component.
The importance of an immediate definition of integrated training paths for the creation of new professional figures (e.g., transitional care experts) in some cases, and in other cases retrained ones, becomes a critical factor in the success/failure of structural and system that are being undertaken with the NRRP. The change in roles and technological innovation would also become an element of help in this phase of structural shortage of professional figures, as well as helping to trigger useful motivational processes in professionals.
“Urgent measures to strengthen the administrative capacity of public administrations functional to the implementation of the National Recovery and Resilience Plan (PNRR) and for the efficiency of justice.”
1.NRRP Missions and Component. Update nov 2022. Available from: www.governo.it
2.Cioffi et al. How does Emotional Intelligence act on Institutional Policies? A New Set of Behaviors to Facilitate Implementation of the Recovery and Resilience Plan (RRP) in local Health Units in Italy. 2023. Available from: https://hpr.termedia.pl/How-does-emotional-intelligence-act-on-institutional-policies-A-new-set-of-behaviors,166564,0,2.html
3.Cioffi et al. A scientific and integrated coaching training pathway to accelerate HCV eradication and use of telemedicine for Covid 19 patients in 5 local health units in Italy. Special Report- Interdisciplinary Journal of Virtual Learning in Medical Sciences. 2022;13(2):137-140. DOI: 10.30476/IJVLM2022.95094.1150
4.Cioffi et al. Tools for Developing and Measuring Skills for Clinical Innovation: The Case of Telemedicine and the Case of the Eradication of the HCV viru2021_13_FRANCOANGELI_Mecosan_118_2021.indd 133 09/07/21. 2021
5.Cioffi et al. Testing of an inter-disciplinary model to develop institutions and policy based on the value of skills. 2019. DOI: 10.23753/htafocus2019.03.014
6.ISTAT. Available from: https://www.istat.it/it/dati-analisi-e-prodotti/open-data [Accessed: December 31, 2023]
7.Available from: https://www.opensalutelazio.it/salute/ [Accessed: December 10, 2023]
8.Workshop 2022 October 24. Available from: https://www.nomisma.it/press-area/competenze-benessere-organizzativo-piessepi-gidp/
9.Cornelissen G, Pandelaere M, Warlop L, Dewitte S. Positive cueing: Promoting sustainable consumer behavior by cueing common environmental behaviors as environmental. International Journal of Research in Marketing. 2008;25(1):46-55
10.World Employment Social Outlook 2019- International Labour Organization. Available from: https://www.ilo.org
11.Kim S. Working with robot: Human resource development considerations in human-robot interaction. 2022;21. DOI: 10.1177/15344843211068810
12.Ritratti. Seven Women tell their stories. May 25062019. ISBN 9788897708292ù
13.The ILO and the future of work. The politics of global labour policy 2022
14.OECD labour force statistics 2024. Updated Jan 2024. Available from: https://www.oecd.org
Written By
Francesca Cioffi, Daniela Sgroi, Tiziana Chiriaco, Marina Cerbo and Francesca Milito
Submitted: 22 January 2024Reviewed: 29 January 2024Published: 09 April 2024