Open Access is an initiative that aims to make scientific research freely available to all. To date our community has made over 100 million downloads. It’s based on principles of collaboration, unobstructed discovery, and, most importantly, scientific progression. As PhD students, we found it difficult to access the research we needed, so we decided to create a new Open Access publisher that levels the playing field for scientists across the world. How? By making research easy to access, and puts the academic needs of the researchers before the business interests of publishers.
We are a community of more than 103,000 authors and editors from 3,291 institutions spanning 160 countries, including Nobel Prize winners and some of the world’s most-cited researchers. Publishing on IntechOpen allows authors to earn citations and find new collaborators, meaning more people see your work not only from your own field of study, but from other related fields too.
Regenerative medicine has gained prominence in recent decades and originated from the growing need for medical intervention in degenerative diseases associated with age. This need is believed to be enhanced also by the increase in the average life expectancy of pets, aliased with the growing social integration of pets into human lives, and the development of specialized veterinary medical care. Platelet-rich products, such as platelet-rich fibrin (PRF), have received attention in clinical veterinary settings. PRF therapy has been proposed for the treatment of skin wounds of various etiologies. Traumatic skin wounds are a frequent occurrence in veterinary practice, constituting an opportunity for PRF therapy application, as an adjunct to medical and surgical treatments. The PRF biomaterial is a hemoderivative obtained after single whole-blood centrifugation. In the process, platelets and leukocytes are activated, resulting in a fibrin clot rich in growth factors and cytokines. Considering the young age of PRF regenerative therapy, it is imperative to promote well-characterized PRF biomaterials using standardized preparation methods in both clinical and research scenarios. This step is critical to promote the comparison and allow a critical analysis of platelet-based therapies, allowing its development and rational clinical use.
Center for Animal and Veterinary Science (CECAV), AL4AnimaLS, Department of Veterinary Sciences, School of Veterinary Sciences, University of Trás-os-Montes and Alto Douro (UTAD), Vila Real, Portugal
VetLamaçães, Veterinary Clinic, Braga, Portugal
CIVG, Vasco da Gama Research Center/EUVG – Vasco da Gama University School, Coimbra, Portugal
Pedro P. Carvalho
Vetherapy – Research and Development in Biotechnology, Coimbra, Portugal
Maria dos Anjos Pires
Center for Animal and Veterinary Science (CECAV), AL4AnimaLS, Department of Veterinary Sciences, School of Veterinary Sciences, University of Trás-os-Montes and Alto Douro (UTAD), Vila Real, Portugal
*Address all correspondence to: carlasoares.medvet@gmail.com
1. Introduction
1.1 Contextualization
The veterinary regenerative medicine is an emerging field and has gained prominence in recent decades. Regenerative medicine for veterinary patients will follow a translational model, encouraged by the investment and biotechnological advances achieved in humans [1, 2].
Regenerative medicine originated from the growing need for medical intervention in degenerative diseases associated with age, such as osteoarthritis. It is believed to be enhanced also by pets’ life expectancy increase, aliased with the growing social integration of pets into human families, and the development of specialized veterinary medical care [1, 3].
Regenerative medicine is a clinical area whose main objective is to promote the regeneration of damaged tissues, restoring the human/animal healthy state or improving the condition and well-being, with the application of the individual’s biological products [4, 5, 6].
Therapy with platelet-derived products (PDPs) and with adult stem cells derived from tissues such as fat or bone marrow is increasingly being used as valid and effective therapeutic options, often in combination with pharmacological therapies [1, 7].
PDPs are hemoderivatives, being obtained from whole blood separation, attained from simple blood harvesting. They have been explored mainly as autologous or allogeneic sources of growth factors, cytokines, and structural proteins, with immunological, healing, and regenerative potential for both tissue engineering approaches and regenerative therapies [1]. PDPs, also frequently addressed as platelet-based therapies, have been used primarily in the treatment of traumatic injury or degenerative processes, with the main objective of promoting the restoration of tissue homeostasis (assessed later, Section 6). This is based on inflammation triggering, involving biochemical and metabolic phenomena, and proliferation and differentiation of several cell populations, with strong emphasis on angiogenesis [6].
1.2 Summary of the most important PDPs: platelet-rich plasma (PRP) and PRF (platelet-rich fibrin)
The various PDPs used in human and veterinary medicine can be broadly classified into platelet-poor and platelet-rich products, distinguished mainly by the presence of platelets. Depending on the platelet and fibrin content, blood-derived biomaterials include platelet concentrate (recognized as PC, but sometimes referred to as platelet-rich plasma, PRP), platelet-poor plasma (also nominated as PPP), and platelet-rich fibrin (PRF), among others [1, 8]. Nowadays, the leukocyte quantification in the formulation is also considered as inherent to the categorization of the related PDP [9]. This feature is explained by the prominence of several cytokines associated with immunological features in the local of their action, when the formulation is applied in situ, which happens in clinical applications [10, 11].
The term PRP was first used in the 1970s by human hematologists. It refers to plasma with a platelet count higher than that of peripheral blood and was initially used to treat patients with thrombocytopenia. Ten years later, PRP was first used in maxillofacial surgery as platelet-rich fibrin (PRF). Furthermore, these blood-derived products have been used in various surgical areas, including cardiology, pediatric surgery, gynecology, urology, plastic surgery, and ophthalmology [6, 12].
PRP is produced by centrifugation of anticoagulated blood, which means, whole blood with anticoagulant solution. This process separates the blood fractions based on the density of its components. Typically, the formulation of PRP involves two sequential centrifugations. The first centrifugation separates erythrocytes from the plasma, and the second one concentrates the platelets and the leukocytes [1]. In addition, single centrifugation protocols are described [13]. Furthermore, PPP is a plasmatic solution containing low to vestigial platelets and other blood element concentration, rich in fibrinogen. PPP is obtained from the centrifugation of anticoagulated blood, as a subproduct of PRP manufacture [1, 14]. The presence of angiogenic factors and biomolecules in PPP has been associated with bone repair in human and canine studies.
On the other hand, the hemoderivative PRF has been relevant in recent years. Also entitled as leukocyte-PRF (L-PRF), it was developed by Choukroun, in France, in oral and maxillofacial surgical areas, to improve bone healing in implant dentistry [15]. The PRF is produced by a single centrifugation of whole blood deprived anticoagulant, which allows the natural formation of a clot, with simultaneous platelet activation [9, 16]. PRF is a reliable PDP, mentioned as second-generation platelet concentrate, and its production is the only one that is consistently described among all hemoderivatives [17]. The manufacturing procedure for PRF production is minimalistic, safe, easy, and cost-effective and does not require advanced manufacturing skills, once that its preparation has low variables, being a highly reproducible methodology [1].
2. Inclusion of platelet-derived products (PDPs) in veterinary regenerative dermatology: a brief introduction
In the last decade, there has been a significant clinical and biotechnological investment in platelet-rich products [1, 18, 19, 20]. Both autologous PRP and PRF therapy is advocated in human dermatology, in different etiology wound treatment and, allogenic platelet therapy has also been proposed [21, 22, 23, 24]. Regarding veterinary medicine, PRF and even PRP therapy has been advocated for wound regeneration, using autologous, allogenic, and xenogenic administration [3, 25, 26, 27, 28].
PDPs, due to their characteristic of being ‘ready to use’ in clinical facilities, have become increasingly embraced by clinicians. Platelets are well-known for their role in hemostasis and thrombogenesis, as well as their crucial contribution to the initiation and development of the healing process. This complex process begins with the event of inflammation, stimulating the recruitment of leukocytes and progenitor cells, as well as the stimulation of angiogenesis. Products rich in platelets are eminently suitable for wound healing [1, 29, 30].
2.1 Traumatic skin wounds in dogs and cats: an occasional problem or a frequent complaint?
Bite wounds in companion animals are understudied compared to the incidence of bite wounds in humans. Isolated reports estimate that 10–15% of veterinary trauma cases in pets are bite wounds [31].
Traumatic skin lesions are a frequent occurrence in pets’ veterinary practice and can have various causes. In dogs and cats, many of these lesions become colonized by bacteria either during the initial trauma or during the healing process.
The skin is the body’s largest organ, and it is composed of various cell populations, including epithelial, mesenchymal, and cells with immunological functions such as resident Langerhans and dendritic cells, T lymphocytes, macrophages, and mast cells, and also stem cells [32]. Physical assault to the skin leads to loss of integrity and invasion by saprophytes and pathogens/microorganisms into sterile compartments within the organism; as a consequence, the infected tissue becomes necrotized, increasing the inflammatory response. Severe tissue trauma, with or without infection, can trigger a systemic inflammatory response syndrome (SIRS), which potentiates inflammation, with multiple exponential cascades of cytokines, coagulation, and fibrinolytics. In severe cases, the infection can lead to sepsis [33].
Normal and intact skin is intended to control the surface microbial populations and to prevent the underlying tissue from being colonized and invaded by potential pathogens. The presence and proliferation of bacteria in wounds has been identified as a major cause of overdue healing and infection in both acute and chronic wounds [34].
In 2018, a study was conducted on bacterial contamination in 45 skin wounds (36 dogs and 9 cats). The study found that Staphylococcus spp. was the most frequently isolated agent from contaminated wounds. The study also revealed that the most common cause of skin injury was animal bites (26.67%), followed by the dehiscence of surgical wounds (22.22%). Injuries of unknown origin accounted for 11.11% [35].
In a different study involving 79 dogs and 8 cats, the most common agents were from the genera Staphylococcus spp. and Pseudomonas spp. It is important to note that this is a subjective evaluation, and further research is needed to confirm these findings [36]. In this study, only gentamicin and amikacin demonstrated resistance rates below 50.0%. Infections can delay wound healing, increasing the animal and owner’s stress and costs of treatment, requiring the use of antibiotics. In recurrent situations, antibiotics are often applied empirically, which can contribute to the emergence of antimicrobial resistance [26, 36]. Nevertheless, studies have found a high incidence of resistant bacterial strains in open wounds when compared, highlighting the need for alternatives to antibiotics [37].
In veterinary medicine, the contaminated wound healing occurs through secondary intention, or per secundam, where the wound repairs itself without surgical intervention or suturing. In this case, the clinician’s role is to provide medical support, including systemic administration of antimicrobials if necessary. Moreover, the wound healing is achieved after granulation tissue formation, followed by contraction and epithelialization of the lesion [38, 39].
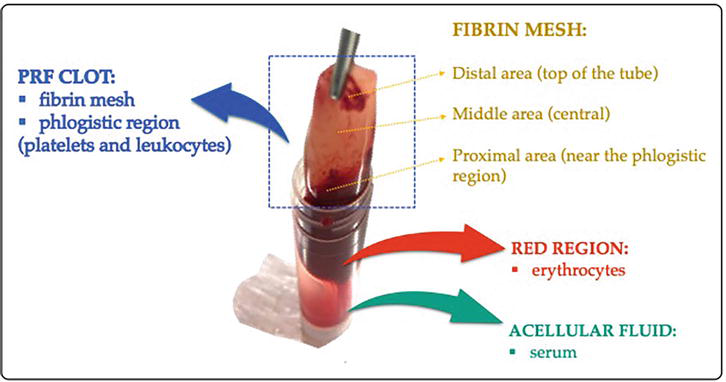
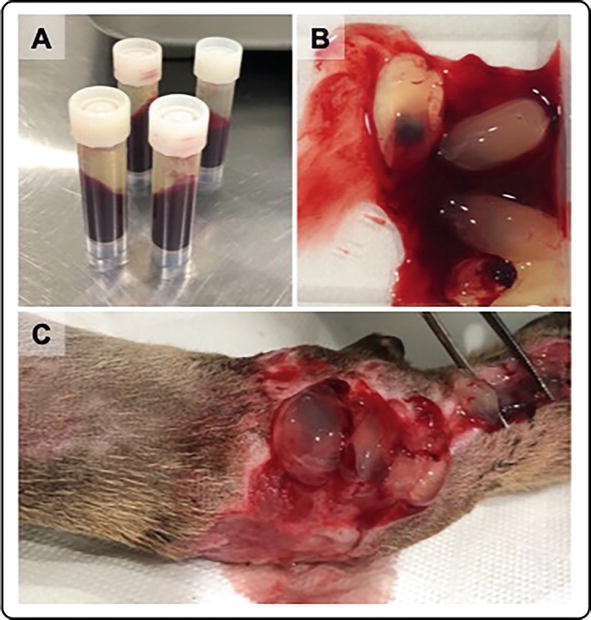
The veterinary clinical use of PRF is gaining attention. The PRF clots are prepared during a single whole blood centrifugation process, without biochemical blood handling, where platelets are activated by the endogenous coagulation cascade, through the action of autologous thrombin [40, 41]. Fibrinogen polymerizes into fibrin, resulting in a clot formation that is composed of three distinct zones (Figure 1): (1) the red zone at the bottom of the tube, which comprises erythrocytes; (2) a flexible fibrin matrix, which retains in its mesh platelets and leukocytes, corresponding to the volume of blood collected, located immediately above the interface with the red zone (also designated the phlogistic region); and (3) the acellular zone, corresponding to serum [1, 42]. Furthermore, the structure of the fibrin matrix can also be divided into three distinct zones based on histological and ultrastructural analysis: the proximal zone (immediately after the phlogistic region), the intermediate zone (middle region of the white fibrin matrix), and the distal zone (located in the upper part of the tube) [3, 41]. This is mainly due to its composition that PRF is described as a biodegradable material, which acts as a reservoir of growth factors and cytokines, fundamental to regeneration, also behaving as a biological scaffold for regenerative and tissue engineering strategies [43].
Figure 1.
After centrifugation of whole blood without anticoagulants, a platelet-rich fibrin (PRF) is obtained.
The platelet concentration within the PRFs is generally not stated in the scientific works, contrary to that stated for platelet-rich formulations, settled as having higher levels of platelets when compared with baseline whole blood [44].
This happens because it is technically difficult to calculate with precision the platelet within a solid material (the clot). Historically, Marx has defined PRP formulations should contain 1,000,000 platelets/mL in a 5 mL volume of plasma, due to the scientific evidence of bone and soft tissue healing enhancement [45]. PRF contains platelets which are concentrated in a specific region of the clot, as explained in the previous section. Especially because the single spin allows the recovery of all platelets within the fibrin clot that is formed during the process, with no loss of any plasmatic fraction as may occur in PRP produced using the double centrifugation method, it is assumed that all the platelets from the blood sample are concentrated and used in the clot. The protocol established by our group uses 5 mL of whole blood to produce one PRF clot, without the use of anticoagulant solutions. Thus, dilution does not occur. Considering that domestic dogs and cats have a median of 350 × 103 platelets/mL in baseline whole blood, a PRF clot produced from 5 mL whole blood contains 1.75 × 109 platelets/mL, overcoming platelet-rich formulation such as PRP [3].
Overall, in PRP methodology, the fraction is rich in platelets, with vestigial or low leukocytes according to the protocol, involving more manipulation and the addition of an anticoagulant solution. In the PRF method, the formulation is platelet and leukocyte concentrated with these elements being condensed in a natural fibrin matrix, also involving less manipulation and less platelet loss.
3.2 Structural and biochemical characteristics of PRF biomaterial
The regenerative properties of PRFs are due to the presence of growth factors that are released from the clot after its formation. This occurs actively and progressively over time as the PRF degrades and incorporates itself into the lesion [3, 25, 41, 46].
In tissue regeneration, cytokines, along with growth factors, play a crucial role due to their regulatory effects on inflammatory and their ability to promote cell differentiation, proliferation, and regeneration. Recent scientific research indicates that leukocytes play a pivotal function, actively participating in wound healing by providing local immune protection (e.g., macrophages, whose main function is phagocytosis) and growth factor production in a manner analogous to thrombocytes and platelets [47].
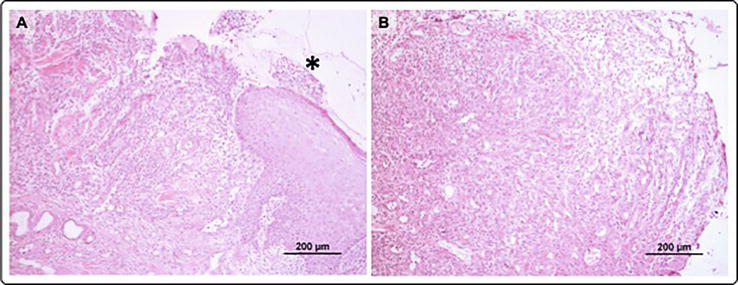
Our research group conducted an in vitro study which confirmed that canine and feline PRFs, obtained using a standardized protocol, released PDGF-BB, TGF-β1, and VEGF-A by day 10. In addition, both PRFs initially release IL-8, a prominent driver of neutrophil recruitment and degranulation [3, 48]. The use of platelet-rich fibrin (PRF) on wounds results in the promotion of significant granulation tissue production, even in cases of extensive tissue loss, and induces normal epithelialization [26, 49, 50]. Macroscopically, the granulation tissue (Figure 2) is characterized by an intense red color and is friable to touch as a consequence of the content of numerous microvessels (formed by neovascularization), which are essential for the oxygenation of the area after a period of hypoxia in which anabolic and catabolic events occurred [25].
Figure 2.
Histological images of a wound after two autologous PRFs treatments in a dog with a road traffic accident wound. (A) The margin of the lesion is visible with epidermis and granulation tissue, without any bacterial contamination. Fibrin and a small amount of necrosis are observed on the surface (*). (B) Another area of the previous lesion, with granulation tissue under the surface fibrin matrix. Inflammatory cells in necrosis can be observed, but there is no bacterial contamination (H&E).
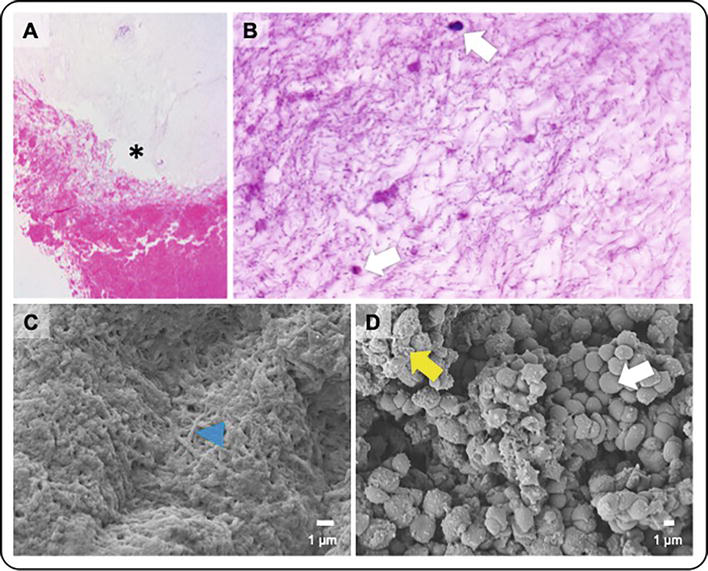
PRFs of human, equine, canine (Figure 3), and feline origin (Figure 4) share a similar structure [51, 52, 53]. In PRFs, the high density of platelets and leukocytes is in the proximal region of the clot, immediately above the typical red fraction (which is discarded). This region is estimated to contain around 97% of the platelets and at least 50% of the leukocytes of the clot, as compared to circulating whole blood. This is particularly true in the case of human PRFs [54]. Platelets are positioned in an organized pattern, with their presence decreasing along the axis of the PRF toward its most distal end. The fibrin mesh also exhibits a distinct organization along the PRF axis, with a reticular and dense pattern in the proximal area and an elongated arrangement in the distal area [3, 55].
Figure 3.
Canine-origin PRF: This is a histological image of the intermediate region of the clot. The red fraction is observed, along with the central zone where leukocytes and platelets are concentrated and the initial part of the fibrin matrix (*). The image was taken using a 10x objective and stained with H&E. (B) The proximal region of the fibrin matrix is located immediately after the anterior or phlogistic region. This region contains small cellular elements such as platelets and rare leukocytes (white arrow). The background has a fibrillar appearance, which is due to fibrin (blue arrowhead) (100x objective, H&E). (C, D) the ultra-dimensional structure of the PRF is composed of fibrin fibrils (blue arrowhead) that retain leukocytes, erythrocytes, and platelets (scanning electron microscopy).
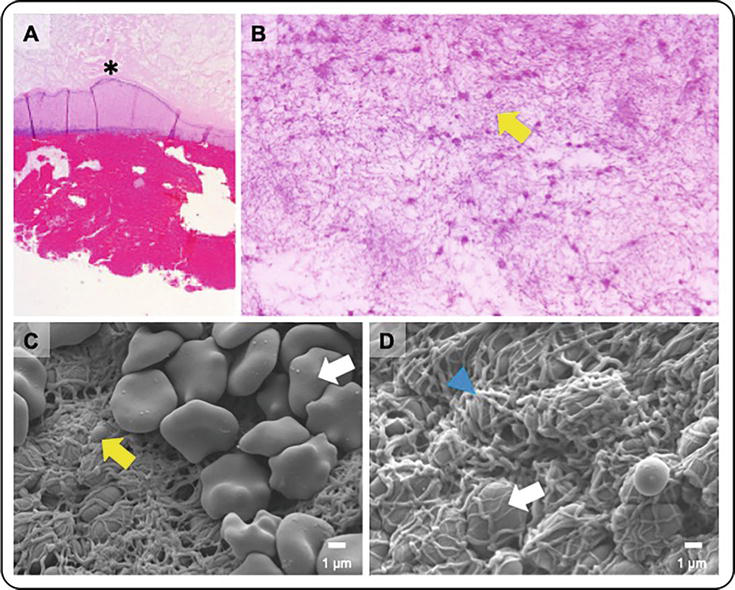
Figure 4.
Feline-origin PRF: The intermediate region of the clot is shown, highlighting the red fraction, the central zone of concentration of platelets and leukocytes, and the beginning of the fibrin clot (*) (10x, H&E). (B) The fibrin matrix is located immediately after the anterior region (proximal fibrin zone). It contains cellular elements such as platelets and occasional leukocytes, arranged under a background with a reticular appearance, which corresponds to fibrin fibrils (blue arrowhead) (100x, H&E). (C, D) scanning electron microscopy shows fibrin fibrils (blue arrowhead), leukocytes, and platelets.
4. Standardized PRF therapy in veterinary wound regeneration
Within the first hour after the preparation of the PRF clot, cytokines and growth factors such as PDGF-BB, VEGF-V, TGF-β1, and IL-8 are released by platelets and leukocytes retained in the PRF matrix. To maximize the collection of platelets and leukocytes present in the phlogistic region of the fibrin clot, it is essential to cut the PRF at the level of the red fraction [3]. The region rich in cellular elements that produce cytokines and growth factors must be placed in direct contact with the lesion, or in the deeper areas of the wound (when the injury has significant tissue loss). PRFs will be applied immediately after their polymerization, or in the first hours after their preparation, so that growth factors and cytokines are released directly at the site of the lesion, with direct application in situ, in a technique similar to that performed in epidermal grafts, in which the PRF is the material to be implanted.
When applied directly to the damaged skin tissue, PRF acts as a bioactive dressing and is therefore a methodology to be considered in companion animals, aiming the regeneration of skin injuries such as lacerations, ulcers, fistulas, burns, and abscesses being chronic or critical injuries [3, 26]. In addition, skin trauma that involves deep structures or infected soft tissues is also suitable for PRF therapy.
The group has optimized the technique for the preparation of canine and feline PRFs in order to obtain a standardized protocol for both species, using reduced volumes of peripheral blood (Figure 5) [26].
Figure 5.
Preparation and application of PRFs. (A) Appearance of the tubes immediately after centrifuging the blood. (B) White component of the blood clot, which constitutes the PRF, ready to be applied. (C) PRFs applied to the wound bed.
Feline PRFs are typically slightly smaller than those of dogs and have a shiny appearance [3]. The risk of accidental contamination during preparation should be minimal because only one centrifugation is required to obtain PRFs, in a sterile, closed tube and the red fraction removing with sterility. Therefore, it can be easily carried out in surgical environment [3].
After the initial phase, PRF treatments are typically administered two times within the first week, being prolonged until the second week in more extended wounds, followed by single weekly treatments from the second/third week onward.
Skin wounds should ideally be mechanically debrided on the day of presentation to remove any necrotic tissue, if present. All skin lesions should be irrigated with sterile 0.9% saline or ringer and dried immediately prior to the grafting of the new PRF treatments to remove any inflammatory exudate or debris.
PRF treatment consisted of the application of freshly prepared PRFs to the recipient site. At the end of the PRF application, a closed dressing is applied using sterile petroleum jelly or paraffin-embedded gauzes, to maintain the clot at the recipient wound site. The number of PRFs applied to the recipient site depended on the size of the individual wound. The average PRF application was one PRF per 2.5 cm2 of the wound surface. Contact between the platelet and leukocyte rich area of the clot and the lesion’s bed is essential to guarantee the grafting of the biomaterial. PRF clots are naturally gelatinous and tend to slide over the wound, which facilitates the healing process. It is important to apply and immobilize the PRFs conveniently in the wound bed, as explained previously.
The treatment is finalized only when significant wound contraction is observed, preceded by the formation of granulation with exophytic characteristics (noticeable proliferation of granulation tissue that extends beyond the wound boundaries), with the formation of epithelial tissue being observed. Continuity of the dressing procedure is carried out only by applying a dressing with fatty material and compresses, until the wound has completely healed [56, 57].
Wounds treated using PRF biomaterials do not receive topical antiseptics, antibiotics, or topical drugs to promote wound healing during the treatment. PRF therapy has been claimed to have effective topical antimicrobial activity, and this has been confirmed by our group (under submission) [58, 59, 60]. The absence of wound infection during PRF therapy may reveal an important intrinsic antimicrobial property of the clots, especially considering that no local antiseptic or antibiotic was used during the treatments of the wounds addressed in the research of our group.
The search for biodegradable and biological solutions to reduce the ecological footprint must also consider healthcare for human and veterinary patients, following the One Health approach. To develop a method that is easy to perform in a clinical-veterinary environment, we obtain PRFs using polypropylene tubes. This plastic is recommended for medical use due to its shock-resistant, durable, economical, recyclable, thermo-resistant, and sterilizable properties, making it ideal for our purposes [3, 61]. Thus, PRF therapy is defined as an ecologically sustainable technique. It can be used on infected and contaminated wounds without the need for topical antiseptics or antimicrobials. This helps to reduce waste accumulation in the environment. The polypropylene tubes used in the therapy can be reused if they are properly sanitized and sterilized [26]. Alternatively, glass tubes may be used, respecting the same dimensions to provide the adequate concentration of platelets and leukocytes.
Larger wounds require a higher number of PRFs. The number of clinic visits for wound treatment and bandage change is reduced using PRF therapy when compared to the bandage changes/wound treatment necessary on conventional medical wound bandaging/treatments, that are required for 2–3 days until wound closure is achieved [39]. This represents less visits to the clinic, less wound manipulation, and indirect decrease in the associated cost (such as travel and hospital waste generated). Dogs and cats treated with PRF therapy in our clinical trials tolerated the repeated wound manipulation of PRF grafting and subsequent dressings extremely well without the use of topical anesthesia. In fact, the analgesic effect associated with PRF therapy has been confirmed by recent reports [26, 62, 63].
In addition, the PRF therapy technique can be highlighted as an environmentally sustainable technique as the polypropylene tubes used to produce the standardized PRFs could be reused, thereby reducing waste and supporting ecological practices in clinical research.
5. PRF as a natural homeostasis-mimetic patch for regenerative dermatology
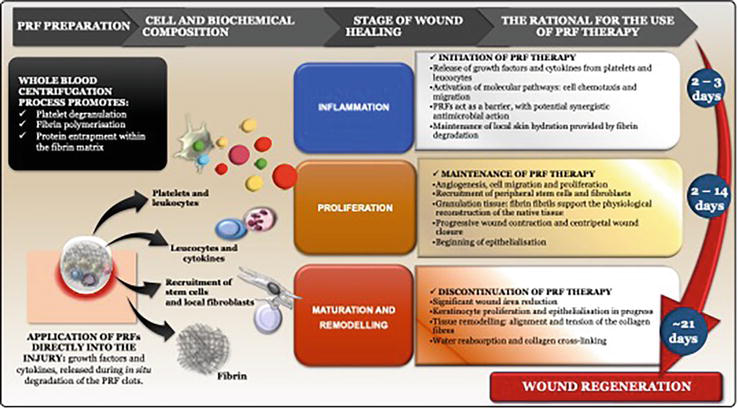
Clinical performance of PRFs can be compared to natural and physiological in situ thrombus formation, which occurs whenever there is tissue damage (see Figure 6) [55]. Effectively, PRF acts as a biological filling material accompanied by the release, by the platelets and leukocytes concentrated in it, of bioactive structural proteins, in quantities greater than physiological ones, which promote angiogenesis and remodeling of the surrounding tissue [3].
Figure 6.
Characterization of the physiological events that occur during tissue regeneration using PRF therapy, describing the physiological events that occur during the clinical application of PRF biomaterials.
Tissue regeneration can be characterized by four phases. When tissue damage occurs, such as a skin wound, two phases begin almost simultaneously: hemostasis and inflammation, which lasts for 1–3 days [64]. During these stages, platelets migrate to the site of injury where they become activated, a process known as platelet degranulation, in which chemotactic proteins are released and a clot forms. Other factors, such as the presence of bacteria or necrotic tissue, can promote degranulation [65]. This leads to the build-up of the fibrin matrix, which is essential for tissue healing as it acts as a scaffold for cells that arrive at the site by chemotaxis, such as immune cells, fibrocytes, keratinocytes, and even stem cells [40, 66, 67].
The inflammatory phase occurs simultaneously, and neutrophils are the initial leukocytes to be recruited to the site. Following the involvement of neutrophils, macrophages migrate to the site and undergo polarization, a process that alters their phenotype [68, 69].
Subsequently, these cells differentiate into M1 or M2 macrophage populations. The former exhibit pro-inflammatory action upon exposure to endotoxins such as lipopolysaccharides (LPS) or interferon gamma (IFN-gamma), inducing a humoral immune response and expressing tumor necrosis factor-alpha (TNF-alpha) and cytokines IL-1, IL-6, IL-12, and IL-23 (36, 52). M2 macrophages display anti-inflammatory properties, with a goal of controlling and resolving inflammation, with a high expression of IL-10 and low expression of IL-12, subdivided into M2a, M2b, M2c, and M2d. M2a polarization is stimulated by IL-4, IL-13, and infections associated with helminth parasites or fungi and is associated with the humoral Th2 response. M2b macrophages are activated by toll-Like receptors (TLR) and their binding proteins or by IL-1, which subsequently moderates the immune response. M2c polarization is stimulated by IL-10 and TGF-beta (peptide secreted by PRF), contributing to tissue remodeling and extracellular matrix synthesis, while M2d macrophages are stimulated by IL-6 and adenosine [70, 71].
Inflammation is a response to tissue damage, such as wounds, and triggers a series of events, beginning with hemostasis. The loss of cellular integrity activates immunological factors, including Danger/Damage Associated Molecular Patterns (DAMPs). DAMPs trigger stress signals in the body, leading to innate immune responses. These responses begin with the chemotaxis of neutrophils and other leukocytes to respond to and resolve the injury. The inflammatory response aims to eliminate the antigen that caused it and restore tissue homeostasis, minimizing damage. Platelet-rich formulations are utilized in regenerative medicine to enhance the regeneration of damaged tissues. They contain proteins from intraplatelet granules, such as platelet-derived growth factor (PDGF), transforming growth factor 1 beta (TGF-1 beta), and epidermal growth factor (EGF). These proteins trigger paracrine interactions and signaling pathways at the site of injury [72].
The proliferation phase of cell growth commences 2–3 days after the trauma. This is marked by the formation of granulation tissue, which is composed of fibroblasts and angioblasts. Additionally, there is a decrease in the population of inflammatory cells at the site [64]. Granulation tissue forms as a result of the migration of various cell types, stimulated by the release of PDGF and TGF-1 beta from the inflammatory cells and platelets previously present in the area. Fibroblasts, cells responsible for matrix synthesis, myofibroblasts, responsible for contraction of the lesion throughout the regenerative process, and endothelial cells, which induce the process of neoangiogenesis, are stimulated by the peptides VEGF and FGF (fibroblast growth factor) and form granulation tissue [64, 73]. The process of re-epithelialization occurs later and is characterized by the migration and proliferation of keratinocytes from the periphery of the lesion toward the centre of the wound. At the same time, granulation tissue develops to fill and approximate the edges of the defect [31].
The final stage is remodeling, which can take longer, starting around 3 weeks after the initial damage and lasting for more than a year [64]. During this stage, all previously initiated processes are halted, and many previously active cells undergo apoptosis. The stage is hallmarked by intense deposition of extracellular matrix composed of fibronectin, glycosaminoglycans, proteoglycans, and hyaluronic acid, with type III collagen being the most predominant and gradually replaced by type I collagen [73].
In vitro studies have predominantly been conducted in humans [54, 67] and horses [74] to evaluate the release kinetics of various proteins and growth factors contained in PRF. These studies have shown an active pattern up to 20 days after the production of this biomaterial. Recent in vitro studies in canine and feline species have also demonstrated a progressive release of these compounds over time, up to a maximum of 10 days [3]. However, in a real biological context, PRFs applied directly to the lesion are degraded on site within 3–5 days and are rarely macroscopically visible between dressing changes.
Autologous hemoderivatives are frequently used in both human and veterinary regenerative interventions, addressing biosafety requirements. This method helps to prevent the recipient from being at the risk of secondary infection. It is a widely documented approach [75, 76].
Nonetheless, considering that the use of allogenic blood products is currently widespread and properly regulated (e.g., blood transfusions are essentially allogeneic), the same principle can be extended to the use of PRFs in skin regenerative interventions. No adverse side effects of allogenic (in canine species) or even xenogenic use of PRFs were found in several studies, including the ones performed by our group [26, 75]. Allogenic PRF therapy was assessed within canine species, and in the xenogenic approach, canine-origin PRFs were applied compromised in cats (Figure 7) [26].
Figure 7.
This study documents the phases of healing evolution in different lesions treated with PRF therapy using various approaches. (A) Laceration in a cat that received xenogenic PRFs from a donor dog; evidence of exophytic granulation tissue after treatments with PRFs, displaying an intense red color. (B) PRFs incorporated into the wound, in a dog referred for autologous PRF therapy, after three treatments with PRFs. (C) The presence of exophytic granulation tissue with the formation of epithelium and contraction of the lesion, dog treated with an autologous approach, after four treatments.
Cats produce reduced volumes of blood, limiting autologous production of PRF, which is in itself contraindicated in the presence of concomitant hematological, immunological, and/or metabolic disorders [77, 78]. Xenogenic use should be seen as one of the advantages conferred on PRF therapy as an innovative regenerative interventionist methodology. When considering this methodology, it is important to strictly comply with requirements aimed at ensuring the biosafety of the recipient. This includes screening for infectious diseases and considering the principles and guidelines applied to veterinary blood transfusions, as well as the geographic prevalence of blood-transmitted diseases. It is also important to consider emerging pathologies that are intrinsically associated with current climate changes [1, 79, 80].
To date, blood typing for PDPs which are intended to be applied topically (for example, treatment of skin wounds) is considered unnecessary to date, considering the few clinical studies that exist to date [1, 22, 26, 27, 28, 81, 82].
PRF therapy for wound management has been described as an ecological technique, as it avoids the use of topical antiseptics. This is directly associated with antimicrobial, anti-inflammatory, and analgesic properties attributed to the PRF biomaterial, both in in vitro and in vivo studies [26, 59, 60, 83]. Our research indicates that the direct application of PRFs to the wound bed reduces the requirement for additional antimicrobial or chemical agents and may even obviate the need for some soft tissue surgery (Table 1) [26].
Domain
Advantages
Disadvantages
Technique
Easy to prepare:
Reduced peripheral blood volume
Equipment accessible in the clinic (centrifuge)
Economical technique, without the use of other reagents
Fast and easily reproducible technique (low operator dependence)
Used autologously in most cases Allogenic and xenogenic uses are equally possible
Consider a single centrifuge for processing PRFs The aseptic technique must be used systematically throughout the preparation process
Characteristics of the biomaterial
Biological, biocompatible, and biomimetic of physiological tissue regeneration
Moldable/easily adaptable to the defect
Fibrin polymerization may not occur after 60 minutes after centrifugation (rare; e.g., hematological, hepatic pathology, etc.)
Clinical use
Allows temporal release of growth factors and cytokines directly at the site
Possible actions:
Antibiotic/antiseptic
Anti-inflammatory/analgesic
The interval between dressings using the PRFs biomaterial is longer (in the initial phase of treatment) compared to conventional dressings
PRF therapy does not apply to extensive skin lesions (on the surface)
Biological risks
The risk of contamination during processing is low
If allogenic and xenogenic: screened donors are mandatory:
Consider the possibility of a subclinical period of infectious disease
Consider the geographic area and associated blood-borne diseases
Use indoor living donors, with no travel history
Environmental Issues
Biological and biodegradable
Ecologically sustainable technique:
Avoid the use of topical antiseptics and antimicrobials, contributing to reducing the accumulation of hospital waste
Polypropylene tubes are reusable (after decontamination and sterilization, it is possible by autoclaving)
Table 1.
Summary of the advantages and disadvantages of PRF therapy in skin wounds.
The interval between dressings using the PRF biomaterial is lengthier than in other wound medical treatments, even in the initial phase of treatment, in which large (or deep) wounds appear quite exudative, contaminated, or even infected [39, 75]. Our experience with PRF therapy in wound treatment indicates advantages over other methodologies such as bandages with chemical hydrogels, healing ointments, or commercial wound materials. This results in the need for fewer dressings and less systemic antibiotic therapy for majority of cases [26].
The benefits of PRF therapy outweigh the drawbacks, which are primarily viewed as risks and critical points. The primary limitation of this therapy is linked to extensive defects or lesions. Considering our protocol for collecting five milliliters of blood to produce a platelet-rich fibrin clot sufficient to cover an average of 2.0–2.5 cm2 of the lesion area, it is evident that extensive lesions would require a large volume of blood to be collected for exclusive PRF treatment [3, 26, 55].
On the other hand, non-autologous PRF therapy, which involves allogenic and xenogenic application, requires the screening of donor animals, detailing the screening of blood-borne agents, in the same way as those carried out in the context of transfusion medicine. In these circumstances, the biosafety criteria involved in obtaining blood products for veterinary clinical applications must be followed, always considering the potential risk of transmission of infectious agents in periods of subclinical disease, which is generally not identified by the clinician [1, 79].
7. Anticipating the future of PRF therapy in veterinary regenerative dermatology
Recently and in a similar way, human medicine has also used PRFs for the treatment of complicated wounds, such as those recurrent in diabetic patients, burns, and varicose venous ulcers [49, 84, 85]. PRF therapy has been used for corneal lesions, such as ulcers, in humans with an autologous approach [3, 86, 87].
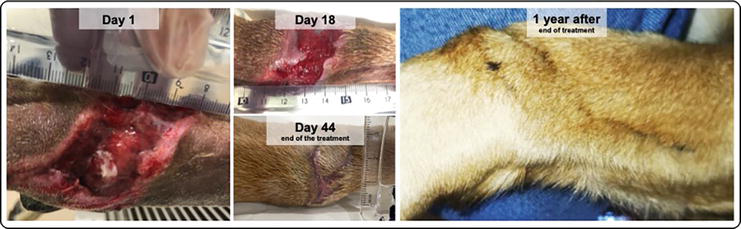
As researchers and clinicians, we recommend PRF therapy as an adjunct to medical and surgical treatments, especially for skin defects or wounds that require second healing soft tissue closure, requiring induction of granulation tissue (Figure 8).
Figure 8.
Scarring evolution documented during autologous PRF therapy, in a female canine, 1 year and 8 months old. Wound resulting from being run over, right anterior limb. On day 1, the lesion appears, before starting regenerative therapy. Until the 18th, three treatments with PRFs were carried out, from which date PRF therapy was suspended, as it was no longer considered necessary. Complete closure was reached on the 44th day. The owner provided a photograph of the region, 1 year after the end of the PRF treatments.
Autologous methodology should be considered limited in small-sized dogs and in cats, especially in the treatment of wounds, where several PRF clots are required, at different timepoints. Moreover, autologous PRFS combined with precision medicine strategies may be suitable to achieve. We have described an innovative surgical approach for the correction of recurrent oronasal fistula in a senior cat in 2018, in which the application of autologous PRF was combined with bone marrow aspirate, leading to the formation of a matrix rich in cells and molecules with regenerative action [25]. In this case, PRF was used as a strategy associated with tissue engineering. A polycaprolactone implant, obtained by 3D printing, was completely adapted to the animal’s defect in a precision regenerative medicine approach. In autologous PRF therapy, it is important to assess (a) the extension and depth of the injury; (b) estimate how many treatments may be required (two or certainly more?); (c) the collaboration of the patient regarding the blood the blood collections; (d) the absence of hematological abnormalities or the administration of pharmaceutical drugs that may result in impaired platelet or leucocyte concentrations.
When not all the requirements of the autologous method are met, allogenic (from other canine donor) or xenogenic PRFs (from canine origin for feline patients) are advocated for wound therapy in patients for whom autologous methodology is not suitable due to co-morbidities or other reasons that prevent blood collection, such as low body weight or non-cooperation for venous collection [26].
The clinical application of PRFs in wounds leads to the rapid formation and proliferation of granulation tissue, which is characterized by intense red color and exuberant vascularization, with a peripheral-to-the-center healing pattern being observed in all wounds. This is particularly important in lesions with extensive tissue deficit. We also observed a significant contraction of the treated traumatic injuries, especially in larger wounds, with subsequent re-epithelialization and crust formation. All treatments carried out by us resulted in minimal esthetic scarring [75].
8. The boundaries of platelet therapy: mandatory use of standardized treatment protocols
In clinical practice, studies focusing standardized and optimized protocols for platelet-rich hemoderivatives arrived only after its clinical use. In veterinary medicine, some PDPs are administered based solely on the patient’s platelet composition and clinical response, which can be a limiting factor [1]. Furthermore, the clinical application of platelet-based formulations is associated with uncertainties due to the lack of a standard protocols, doses, or therapeutic procedures for various lesions and species in which they have been used. For instance, degenerative joint disease is one of the conditions for which the clinical use of PDPs has been extensively documented in both human and animal patients, even prior to the biochemical characterization of the PDPs used [1, 5, 82]. This provides evidence for the growing need to fully and clearly characterize the products used in regenerative strategies. This is essential for the advancement of the field at a clinical level [88]. In addition to these critical points of standardization, these works also question other subjects such as the composition of the PDPs. It is not always described, and the methodology and diversity of clinical studies that use PDPs are obtained through non-standardized protocols. Often, they do not follow similar therapeutic regimens nor they apply similar number of applications and concentration administered, and therefore, they are comparable to each other [89, 90, 91]. This diversity is evident in the studies conducted on both human and animal patients.
As occurring in PRP, different protocols to prepare the PRF are reported in human patients. In fact, one of the most boundaries is the lack of critical evaluation of the different studies by comparative meta-analysis [21]. There are still few reports of PRF therapy in veterinary area compared with human field, and it is important that newcomer researchers apply standardized protocols, in order to allow the comparison between studies, avoiding the heterogenicity of results such as those observed in the report of PRP clinical documentation in the literature. This has been the main propose of our research group, where the same PRF protocol is applied in all clinical cases, after its optimization and biochemical characterization. To increase objectivity, several studies are using nomenclature for the PDPs that is not universally recognized [92].
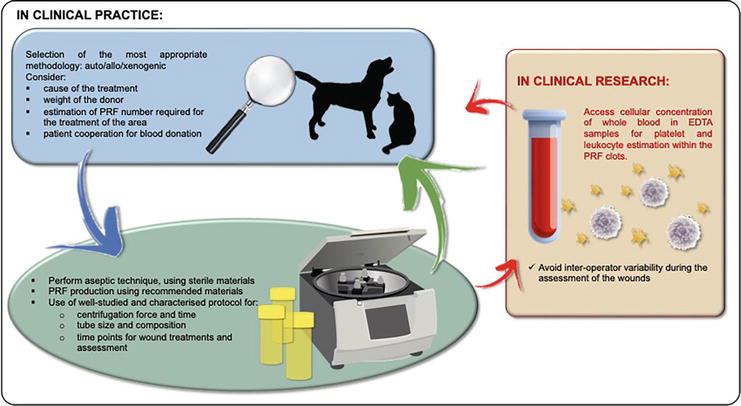
It is imperative to promote well-characterized veterinary PDPs such as PRF, using standardizing methods, in both clinical and research scenarios (Figure 9). Also, comparative research based on consistent and well-defined criteria, using representative numbers of participants and with long-term follow-up periods, should be carried out to better understand the benefits of this biomaterial [1, 8].
Figure 9.
Suggested criteria to consider when implementing PRF therapy, both in clinical practice and research.
The rise of several human-sourced PDPs such as PRP and PRF, and even other derived formulations, has promoted misperception and debate among the scientific community once that different formulations were indistinctly cited in the literature. In 2009, the working group of Dohan Eherenfest suggested four categories of platelet concentrates (P-PRP, L-PRP, P-PRF, and L-PRF), as an attempt to use categorized and standardized PDPs. Furthermore, this claim promoted scientific research to understand and explain the intrinsic biochemical proprieties of PDPs, assuming the demanding need to validate their use, in clinical settings [93]. In 2012, the group of DeLong presented their classification PAW system, based on the report of three constituents in PRP preparation: number of platelets, platelet activation method, and the presence or absence of white blood cells [94]. Until the present, there are no consensual documents in veterinary setting proposing key parameters for the preparation of characterized PDPs, and the only scientific document addressing this issue was published in 2021, by Soares et al. [1].
In summary (Table 2), the use of key parameters to prepare and document well-characterized PDPs is strongly demanded, to avoid dubious and incomparable scientific data related to platelet therapy.
(A1) Size and weight of the centrifuge required for the method (A2) Duration of the procedure (from blood harvest to surgical application) (A3) Budget (initial cost of equipment and repeated costs for reagents and kits) (A4) Technicity of the kit (including required manipulations) and complexity of the procedure
B: Platelets and leukocytes
(B1) Final volume of platelet gel material (relative to initial blood harvest) (B2) Platelet recovery efficiency (B3) Leucocyte recovery efficiency (B4) Preservation of the platelets and leucocytes
C: Fibrin matrix
(C1) Fibrinogen concentration and fibrin density (C2) Fibrin polymerization typology
PAW system: classification of platelet-rich plasma formulations, human area
P: PLT concentration
Subdivision in four groups, according to PLT concentration present: (P1) Above baseline values (P2) Between baseline and 750,000 platelets/μL (P3) Between 750,000 and 1,250,000 platelets/μL (P4) Superior to 1,250,000 platelets/μL
A: Activation system
Exogenous activator used/ or not used
W: WBC existence
Subdivision in two groups, according to WBC concentration present:
Above baseline
Below baseline
Sectioning according to neutrophil concentration: (α) Above baseline (β) Below baseline
PRF is an environmentally sustainable biomaterial as it is biodegradable and obtained through blood centrifugation promoting platelets and leucocytes concentration in a specific region of the matrix. This forms a natural and biocompatible matrix containing higher than physiological concentrations of cells (platelets and leukocytes) with regenerative activity, mimicking the natural healing process. Studies evaluating the kinetics of the cytokines and growth factors released by the PRF biomaterial have proven that this occurs actively and progressively over time. Autologous, allogenic, and xenogenic PRF therapy can be considered as an effective therapeutic strategy in the veterinary clinic. It constitutes an alternative biological regenerative treatment, suitable for wound regeneration in veterinary practice, accelerating wound healing by second intention mechanism.
The PRF enhances the mechanism of local tissue regeneration through the sustained release of molecules that signal the systems involved in the skin healing cascade. However, further clinical studies are required for complete validation, particularly for the xenogenic methodology. In this sense, chronic or critical injuries that are inaccessible or unresponsive to surgical reconstruction, even if infected or contaminated, such as burns, abscesses, and/or skin trauma involving deep structures, are appropriate candidates for PRF therapy, considering that, in these cases of wound regeneration by second intention, it is the appropriate therapeutic decision.
This present work was supported by the Ph.D. grant SFRH/BD/118871/2016 and by the project UIDB/00772/2020 (Doi:10.54499/UIDB/00772/2020) funded by the Portuguese Foundation for Science and Technology (FCT).
Conflict of interest
Pedro P. Carvalho is the C.E.O. of the biotechnology company, Vetherapy, which commercializes veterinary regenerative therapies.
The authors declare that there are no other conflicts of interest.
Notes/thanks/other declarations
The authors thank the Laboratory of Histology and Anatomic Pathology and the Centre for Veterinary and Animal Research (CECAV), both at the University of Trás-os-Montes E Alto Douro.
Appendices and nomenclature
DAMPs
damage associated molecular patterns
EGF
epidermal growth factor
FGF
fibroblast growth factor
g
g-force or gravitational force equivalent
H&E
hematoxylin and eosin stain
IFN-gamma
interferon gamma
IL
interleukin
LPS
lipopolysaccharides
PC
platelet concentrate
PDGF-BB
platelet-derived growth factor, subunit BB
PLT
platelet
PPP
platelet-poor plasma
PRF
platelet-rich fibrin
PRP
platelet-rich plasma
PDP
platelet-derived products
Rpm
rotations per minute
SIRS
inflammatory response syndrome
TNF-alpha
tumor necrosis factor alpha
TNR
toll-like receptors (TLR)
TGF-β1
transforming growth factor beta 1
VEGF-A
vascular endothelial growth factor A
μL
microliter
WBC
white blood cells, or leukocytes
References
1.Soares CS, Babo PS, Reis RL, Carvalho PP, Gomes ME. Platelet-derived products in veterinary medicine: A new trend or an effective therapy? Trends in Biotechnology. 2021;39:225-243. DOI: 10.1016/j.tibtech.2020.07.011
2.Webb TL, Spaas JH, Guest DJ. Editorial: One health and veterinary regenerative medicine: Translational applications. Frontiers in Veterinary Science. 2022;9:9-11. DOI: 10.3389/fvets.2022.959564
3.Soares CS, Babo PS, Faria S, Pires MA, Carvalho PP. Standardized platelet-rich fibrin (PRF) from canine and feline origin: An analysis on its secretome pattern and architectural structure. Cytokine. 2021;148:155695. DOI: 10.1016/j.cyto.2021.155695
4.Barrett JG. A set of grand challenges for veterinary regenerative medicine. Frontiers in Veterinary Science. 2016;3:1-4. DOI: 10.3389/fvets.2016.00020
5.Canapp SO, Canapp DA, Ibrahim V, Carr BJ, Cox C, Barrett JG. The use of adipose-derived progenitor cells and platelet-rich plasma combination for the treatment of supraspinatus tendinopathy in 55 dogs: A retrospective study. Frontiers in Veterinary Science. 2016;3:61. DOI: 10.3389/fvets.2016.00061
6.Andia I, Rubio-Azpeitia E, Martin JI, Abate M. Current concepts and translational uses of platelet rich plasma biotechnology. In: Biotechnology. London, UK: InTechOpen; 2015. p. 13. DOI: 10.5772/59954
7.Bogers SH. Cell-based therapies for joint disease in veterinary medicine: What we have learned and what we need to know. Frontiers in Veterinary Science. 2018;5. DOI: 10.3389/fvets.2018.00070
8.Ehrenfest DMD, Sammartino G, Shibli JA, Wang H, Zou D, Bernard J. Guidelines for the publication of articles related to platelet concentrates (platelet-rich plasma - PRP, or platelet-rich fibrin - PRF): The international classification of the POSEIDO. POSEIDO Journal. 2013;1:17-27
9.Dohan Ehrenfest DM, Rasmusson L, Albrektsson T. Classification of platelet concentrates: From pure platelet-rich plasma (P-PRP) to leucocyte- and platelet-rich fibrin (L-PRF). Trends in Biotechnology. 2009;27:158-167. DOI: 10.1016/j.tibtech.2008.11.009
10.Bielecki T, Ehrenfest DMD, Everts PA, Wiczkowski A. The role of leukocytes from L-PRP/L-PRF in wound healing and immune defense: New perspectives. Current Pharmaceutical Biotechnology. 2012;13:1153-1162. DOI: 10.2174/138920112800624373
11.Lana JF, Huber SC, Purita J, Tambeli CH, Santos GS, Paulus C, et al. Leukocyte-rich PRP versus leukocyte-poor PRP - The role of monocyte/macrophage function in the healing cascade. Journal of Clinical Orthopaedics and Trauma. 2019;10:S7-S12. DOI: 10.1016/j.jcot.2019.05.008
12.Mościcka P, Przylipiak A. History of autologous platelet-rich plasma: A short review. Journal of Cosmetic Dermatology. 2021;20:2712-2714. DOI: 10.1111/jocd.14326
13.Anitua E, Sánchez M, Orive G. The importance of understanding what is platelet-rich growth factor (PRGF) and what is not. Journal of Shoulder and Elbow Surgery. 2011;20:23-24. DOI: 10.1016/j.jse.2010.07.005
14.Martínez CE, Smith PC, Palma Alvarado VA. The influence of platelet-derived products on angiogenesis and tissue repair: A concise update. Frontiers in Physiology. 2015;6:290. DOI: 10.3389/fphys.2015.00290
15.Naik B, Karunakar P, Jayadev M, Marshal VR. Role of platelet rich fibrin in wound healing: A critical review. Journal of Conservative Dentistry. 2013;16:284. DOI: 10.4103/0972-0707.114344
16.Choukroun J, Adda F, Schoeffler C, Vervelle A. Une opportunité en paro-implantologie: Le PRF. Implantodontie. 2001;42:55-62
17.Dohan DM, Choukroun J, Diss A, Dohan SL, Dohan AJJ, Mouhyi J, et al. Platelet-rich fibrin (PRF): A second-generation platelet concentrate. Part I: Technological concepts and evolution. Oral Surgery, Oral Medicine, Oral Pathology, Oral Radiology, and Endodontology. 2006;101:e37-44. DOI: 10.1016/j.tripleo.2005.07.008
18.Farghali HA, AbdElKader NA, AbuBakr HO, Ramadan ES, Khattab MS, Salem NY, et al. Corneal ulcer in dogs and cats: Novel clinical application of regenerative therapy using subconjunctival injection of autologous platelet-rich plasma. Frontiers in Veterinary Science. 2021;8:1-17. DOI: 10.3389/fvets.2021.641265
19.Perego R, Spada E, Moneta E, Baggiani L, Proverbio D. Use of autologous leucocyte- and platelet-rich plasma (L-PRP) in the treatment of aural hematoma in dogs. Veterinary Sciences. 2021;8:172. DOI: 10.3390/vetsci8090172
20.Carr BJ, Canapp SO. Regenerative medicine for soft tissue injury and osteoarthritis. Today’s Vet Paractice. 2016;53:53-60
21.de Carvalho CKL, Fernandes BL, de Souza MA. Autologous matrix of platelet-rich fibrin in wound care settings: A systematic review of randomized clinical trials. Journal of Functional Biomaterials. 2020;11:31. DOI: 10.3390/jfb11020031
22.Jo CH, Shin JS, Lee SY, Shin S. Allogeneic platelet-rich plasma for rotator cuff repair. Acta Ortopedica Brasileira. 2017;25:38-43. DOI: 10.1590/1413-785220172501163417
23.Greppi N, Mazzucco L, Galetti G, Bona F, Petrillo E, Smacchia C, et al. Treatment of recalcitrant ulcers with allogeneic platelet gel from pooled platelets in aged hypomobile patients. Biologicals. 2011;39:73-80. DOI: 10.1016/j.biologicals.2011.01.002
24.Zhang Z-Y, Huang A-W, Fan JJ, Wei K, Jin D, Chen B, et al. The potential use of allogeneic platelet-rich plasma for large bone defect treatment: Immunogenicity and defect healing efficacy. Cell Transplantation. 2013;22:175-187. DOI: 10.3727/096368912X653183
25.Soares CS, Barros LC, Saraiva V, Gomez-Florit M, Babo PS, Dias IR, et al. Bioengineered surgical repair of a chronic oronasal fistula in a cat using autologous platelet-rich fibrin and bone marrow with a tailored 3D printed implant. Journal of Feline Medicine and Surgery. 2018;20:835-843. DOI: 10.1177/1098612X18789549
26.Soares CS, Dias IR, Pires MA, Carvalho PP. Canine-origin platelet-rich fibrin as an effective biomaterial for wound healing in domestic cats: A preliminary study. Veterinary Sciences. 2021;8:213. DOI: 10.3390/vetsci8100213
27.Chung T, Baek D, Kim N, Park J, Park C. Topical allogeneic platelet-rich plasma treatment for a massive cutaneous lesion induced by disseminated intravascular coagulation in a toy breed dog. Irish Veterinary Journal. 2015;68:4. DOI: 10.1186/s13620-015-0032-7
28.Kim SE, Lee M-K, Seo K. Clinical application of serum eye drops for herpetic keratitis in cats: A pilot. International Journal of Applied Research in Veterinary Medicine. 2018;16:221-225
29.Ghoshal K, Bhattacharyya M. Overview of platelet physiology: Its hemostatic and nonhemostatic role in disease pathogenesis. Scientific World Journal. 2014;2014:1-16. DOI: 10.1155/2014/781857
30.Ratajczak J, Vangansewinkel T, Gervois P, Merckx G, Hilkens P, Quirynen M, et al. Angiogenic properties of ‘leukocyte- and platelet-rich fibrin’. Scientific Reports. 2018;8:1-10. DOI: 10.1038/s41598-018-32936-8
31.Englar RE. Common Clinical Presentations in Dogs and Cats. Wiley; 2019. DOI: 10.1002/9781119414612
32.Souci L, Denesvre C. 3D skin models in domestic animals. Veterinary Research. 2021;52:21. DOI: 10.1186/s13567-020-00888-5
33.Holt DE, Griffin G. Bite wounds in dogs and cats. The Veterinary Clinics of North America. Small Animal Practice. 2000;30:669-679. DOI: 10.1016/S0195-5616(00)50045-X
34.Bowler PG, Duerden BI, Armstrong DG. Wound microbiology and associated approaches to wound management. Clinical Microbiology Reviews. 2001;14:244-269. DOI: 10.1128/CMR.14.2.244-269.2001
35.Kožár M, Hamilton H, Koščová J. Types of wounds and the prevalence of bacterial contamination of wounds in the clinical practice of small animals. Folia Veterinaria. 2018;62:39-47. DOI: 10.2478/fv-2018-0036
36.Ishii JB, Freitas JC, Arias MVB. Resistência de bactérias isoladas de cães e gatos no Hospital Veterinário da Universidade Estadual de Londrina (2008-2009). Pesquisa Veterinaria Brasileira. 2011;31:533-537. DOI: 10.1590/S0100-736X2011000600013
37.Nolff MC, Reese S, Fehr M, Dening R, Meyer-Lindenberg A. Assessment of wound bio-burden and prevalence of multi-drug resistant bacteria during open wound management. The Journal of Small Animal Practice. 2016;57:255-259. DOI: 10.1111/jsap.12476
38.Bosco J. Principles of wound Care & Bandaging Techniques. Today’s Veterinary Practice. 2012;2:61-67. DOI: 10.7748/ns.3.38.52.s69
39.Tobias K. Basic wound care. NAVC Clinician's Brief. 2012:74-78
40.Gupta V, Bains VK, Singh GP, Mathur A, Bains R. Regenerative potential of platelet rich fibrin in dentistry: Literature review. Asian Journal of Oral Health & Allied Sciences. 2011;1:23
41.Castilho MS, Rahal SC, das Dias Neto RN, Pereira AC, de Francia CCDA, dos Mesquita LR, et al. Preparation and characterization of leukocyte- and platelet-rich fibrin membrane derived from cats’ blood. Microscopy Research and Technique. 2021:jemt.23737. DOI: 10.1002/jemt.23737
42.Dohan DM, Choukroun J, Diss A, Dohan SL, Dohan AJJ, Mouhyi J, et al. Platelet-rich fibrin (PRF): A second-generation platelet concentrate. Part III: Leucocyte activation: A new feature for platelet concentrates? Oral Surgery, Oral Medicine, Oral Pathology, Oral Radiology, and Endodontology. 2006;101:e51-e55. DOI: 10.1016/j.tripleo.2005.07.010
43.Kobayashi E, Flückiger L, Fujioka-Kobayashi M, Sawada K, Sculean A, Schaller B, et al. Comparative release of growth factors from PRP, PRF, and advanced-PRF. Clinical Oral Investigations. 2016;20:2353-2360. DOI: 10.1007/s00784-016-1719-1
44.Fitzpatrick J, Bulsara MK, McCrory PR, Richardson MD, Zheng MH. Analysis of platelet-rich plasma extraction: Variations in platelet and blood components between 4 common commercial kits. Orthopaedic Journal of Sports Medicine. 2017;5:1-8. DOI: 10.1177/2325967116675272
45.Marx RE. Platelet-rich plasma (PRP): What is PRP and what is not PRP? Implant Dentistry. 2001;10:225-228. DOI: 10.1097/00008505-200110000-00002
46.Kornsuthisopon C, Pirarat N, Osathanon T, Kalpravidh C. Autologous platelet-rich fibrin stimulates canine periodontal regeneration. Scientific Reports. 2020;10:1850. DOI: 10.1038/s41598-020-58732-x
47.Jansen EE, Braun A, Jansen P, Hartmann M. Platelet-therapeutics to improve tissue regeneration and wound healing—Physiological background and methods of preparation. Biomedicine. 2021;9:869. DOI: 10.3390/biomedicines9080869
48.Nasirzade J, Kargarpour Z, Hasannia S, Strauss FJ, Gruber R. Platelet-rich fibrin elicits an anti-inflammatory response in macrophages in vitro. Journal of Periodontology. 2020;91:244-252. DOI: 10.1002/JPER.19-0216
49.Somani A, Rai R. Comparison of efficacy of autologous platelet-rich fibrin versus saline dressing in chronic venous leg ulcers: A randomised controlled trial. Journal of Cutaneous and Aesthetic Surgery. 2017;10:8-12. DOI: 10.4103/JCAS.JCAS_137_16
50.Miron RJ, Fujioka-Kobayashi M, Bishara M, Zhang Y, Hernandez M, Choukroun J. Platelet-rich fibrin and soft tissue wound healing: A systematic review. Tissue Engineering. Part B, Reviews. 2017;23:83-99. DOI: 10.1089/ten.teb.2016.0233
51.Jiménez-Aristazábal RF, Carmona JU, Prades M. Changes on the structural architecture and growth factor release, and degradation in equine platelet-rich fibrin clots cultured over time. Journal of Equine Veterinary Science. 2019;82:102789. DOI: 10.1016/j.jevs.2019.102789
52.Dohan Ehrenfest DM, Bielecki T, Jimbo R, Barbé G, Del Corso M, Inchingolo F, et al. Do the fibrin architecture and leukocyte content influence the growth factor release of platelet concentrates? An evidence-based answer comparing a pure platelet-rich plasma (P-PRP) gel and a leukocyte- and platelet-rich fibrin (L-PRF). Current Pharmaceutical Biotechnology. 2012;13:1145-1152. DOI: 10.2174/138920112800624382
53.Pavlovic V, Ciric M, Jovanovic V, Trandafilovic M, Stojanovic P. Platelet-rich fibrin: Basics of biological actions and protocol modifications. Open Medicine. 2021;16:446-454. DOI: 10.1515/med-2021-0259
54.Dohan Ehrenfest DM, Del Corso M, Diss A, Mouhyi J, Charrier J-B. Three-dimensional architecture and cell composition of a Choukroun’s platelet-rich fibrin clot and membrane. Journal of Periodontology. 2010;81:546-555. DOI: 10.1902/jop.2009.090531
55.Soares C, Dias I, Pires MA, Carvalho P. Autologous platelet-rich fibrin (PRF) in canine regenerative wound therapy: A natural haemostasis mimetic. Journal of Comparative Pathology. 2022;191:60. ISSN 0021-9975. DOI: 10.1016/j.jcpa.2021.11.138. Available from: https://www.sciencedirect.com/science/article/pii/S002199752100284X
56.Zinder R, Cooley R, Vlad LG, Molnar JA. Vitamin A and wound healing. Nutrition in Clinical Practice. 2019;34:839-849. DOI: 10.1002/ncp.10420
57.Lin P-H, Sermersheim M, Li H, Lee P, Steinberg S, Ma J. Zinc in wound healing modulation. Nutrients. 2017;10:16. DOI: 10.3390/nu10010016
58.Burnouf T, Chou M-L, Wu Y-W, Su C-Y, Lee L-W. Antimicrobial activity of platelet (PLT)-poor plasma, PLT-rich plasma, PLT gel, and solvent/detergent-treated PLT lysate biomaterials against wound bacteria. Transfusion. 2013;53:138-146. DOI: 10.1111/j.1537-2995.2012.03668.x
59.Feng M, Wang Y, Zhang P, Zhao Q , Yu S, Shen K, et al. Antibacterial effects of platelet-rich fibrin produced by horizontal centrifugation. International Journal of Oral Science. 2020;12:1-8. DOI: 10.1038/s41368-020-00099-w
60.Shariati A, Moradabadi A, Azimi T, Ghaznavi-Rad E. Wound healing properties and antimicrobial activity of platelet-derived biomaterials. Scientific Reports. 2020;10:1-9. DOI: 10.1038/s41598-020-57559-w
61.Maddah HA. Polypropylene as a promising plastic: A review. American Journal of Polymer Science. 2016;6:1-11. DOI: 10.5923/j.ajps.20160601.01
62.Albilia J, Herrera-Vizcaíno C, Weisleder H, Choukroun J, Ghanaati S. Liquid platelet-rich fibrin injections as a treatment adjunct for painful temporomandibular joints: Preliminary results. Cranio. 2020;38:292-304. DOI: 10.1080/08869634.2018.1516183
63.Al-Hamed FS, Tawfik MA-M, Abdelfadil E. Clinical effects of platelet-rich fibrin (PRF) following surgical extraction of lower third molar. Saudi Journal of Dental Research. 2017;8:19-25. DOI: 10.1016/j.sjdr.2016.05.002
64.Park J, Hwang S, Yoon I-S. Advanced growth factor delivery systems in wound management and skin regeneration. Molecules. 2017;22:1259. DOI: 10.3390/molecules22081259
65.Nurden AT. Platelets, inflammation and tissue regeneration. Thrombosis and Haemostasis. 2011;105:13-33. DOI: 10.1160/THS10-11-0720
66.Crisci A, Manfredi S, Crisci M. The L-PRF membrane (fibrin rich in platelets and leukocytes) and its derivatives useful as a source of stem cells in wound surgery. Journal of Stem Cell Reports. 2019;1:1-11
67.Ghanaati S, Booms P, Orlowska A, Kubesch A, Lorenz J, Rutkowski J, et al. Advanced platelet-rich fibrin: A new concept for cell-based tissue engineering by means of inflammatory cells. The Journal of Oral Implantology. 2014;40:679-689. DOI: 10.1563/aaid-joi-D-14-00138
68.Mariani E, Roffi A, Cattini L, Pulsatelli L, Assirelli E, Krishnakumar GS, et al. Release kinetic of pro- and anti-inflammatory biomolecules from platelet-rich plasma and functional study on osteoarthritis synovial fibroblasts. Cytotherapy. 2020;22:344-353. DOI: 10.1016/j.jcyt.2020.02.006
69.Ellis S, Lin EJ, Tartar D. Immunology of wound healing. Current Dermatology Reports. 2018;7:350-358. DOI: 10.1007/s13671-018-0234-9
70.Lee KY. M1 and M2 polarization of macrophages: A mini-review. Medical Biological Science and Engineering. 2019;2:1-5. DOI: 10.30579/mbse.2019.2.1.1
71.Orekhov AN, Orekhova VA, Nikiforov NG, Myasoedova VA, Grechko AV, Romanenko EB, et al. Monocyte differentiation and macrophage polarization. Vessel Plus. 2019;3:10. DOI: 10.20517/2574-1209.2019.04
72.McGrath MH. Peptide growth factors and wound healing. Clinics in Plastic Surgery. 1990;17:421-432
73.Tottoli EM, Dorati R, Genta I, Chiesa E, Pisani S, Conti B. Skin wound healing process and new emerging technologies for skin wound care and regeneration. Pharmaceutics. 2020;12:735. DOI: 10.3390/pharmaceutics12080735
74.Jiménez-Aristizabal RF, López C, Álvarez ME, Giraldo C, Prades M, Carmona JU. Long-term cytokine and growth factor release from equine platelet-rich fibrin clots obtained with two different centrifugation protocols. Cytokine. 2017;97:149-155. DOI: 10.1016/j.cyto.2017.06.011
75.Soares CS, Barros LC, Dias IR, Pires MA, Carvalho PP. Clinical insights of platelet-rich fibrin (PRF) as an active biomaterial for wound regeneration. In: 17th Montenegro International Veterinary Congress Santa Maria da Feira, Portugal. 2021
76.Soares CS, Barros LC, Dias IR, Pires MA, Carvalho PP. Platelet-rich fibrin in regenerative wound therapy: Preliminary outcomes in canine patients. In: South. Eur. Vet. Conf., Barcelona, Spain. 2020
77.Gemignani F, Perazzi A, Iacopetti I. Use of canine sourced platelet-rich plasma in a feline contaminated cutaneous wound. The Canadian Veterinary Journal. 2017;58:141-144
78.Karina Gomes Barros A, Bruno Nascimento B, Inara Guastini D, Eliane Szücs Dos S, Cecília Braga L, Gisele Alborghetti N, et al. Effects of heterologous platelet-rich plasma gel on standardized dermal wound healing in rabbits. Acta Cirúrgica Brasileira. 2015;30:209-215. DOI: 10.1590/S0102-865020150030000008
79.Wardrop KJ, Birkenheuer A, Blais MC, Callan MB, Kohn B, Lappin MR, et al. Update on canine and feline blood donor screening for blood-borne pathogens. Journal of Veterinary Internal Medicine. 2016;30:15-35. DOI: 10.1111/jvim.13823
80.Gibson G. Transfusion medicine. In: King L, Boag A, editors. BSAVA Man. Canine Feline Emerg. Crit. Care. 2nd ed. Quedgeley, Gloucs United Kingdom: British Small Animal Veterinary Association; 2007. pp. 215-227
81.Hamed MA, Abouelnasr KS, El-Adl M, Abo Elfadl EA, Farag A, Lashen S. Effectiveness of allogeneic platelet-rich fibrin on second-intention wound healing of experimental skin defect in distal limb in donkeys (Equus asinus). Journal of Equine Veterinary Science. 2019;73:131-138. DOI: 10.1016/j.jevs.2018.12.014
82.Catarino J, Carvalho P, Santos S, Martins Â, Requicha J. Treatment of canine osteoarthritis with allogeneic platelet-rich plasma: Review of five cases. Open Veterinary Journal. 2020;10:226-231. DOI: 10.4314/ovj.v10i2.12
83.Ozgul O, Senses F, Er N, Tekin U, Tuz HH, Alkan A, et al. Efficacy of platelet rich fibrin in the reduction of the pain and swelling after impacted third molar surgery: Randomized multicenter split-mouth clinical trial. Head & Face Medicine. 2015;11:37. DOI: 10.1186/s13005-015-0094-5
84.Ozer K, Colak O. Leucocyte- and platelet-rich fibrin as a rescue therapy for small-to-medium-sized complex wounds of the lower extremities. Burn Trauma. 2019;7:11. DOI: 10.1186/s41038-019-0149-0
85.Pinto NR, Ubilla M, Zamora Y, Del Rio V, Dohan Ehrenfest DM, Quirynen M. Leucocyte- and platelet-rich fibrin (L-PRF) as a regenerative medicine strategy for the treatment of refractory leg ulcers: A prospective cohort study. Platelets. 2018;29:468-475. DOI: 10.1080/09537104.2017.1327654
86.Arnalich F, Rodriguez AE, Luque-Rio A, Alio JL. Solid platelet rich plasma in corneal surgery. Ophthalmology and Therapy. 2016;5:31-45. DOI: 10.1007/s40123-016-0051-9
87.Alio JL, Rodriguez AE, WróbelDudzińska D. Eye platelet-rich plasma in the treatment of ocular surface disorders. Current Opinion in Ophthalmology. 2015;26:325-332. DOI: 10.1097/ICU.0000000000000169
88.Mariani E, Pulsatelli L. Platelet concentrates in musculoskeletal medicine. International Journal of Molecular Sciences. 2020;21:1328. DOI: 10.3390/ijms21041328
89.Anitua E, Alkhraisat MH, Orive G. Perspectives and challenges in regenerative medicine using plasma rich in growth factors. Journal of Controlled Release. 2012;157:29-38. DOI: 10.1016/j.jconrel.2011.07.004
90.McNamee MJ, Coveney CM, Faulkner A, Gabe J. Ethics, evidence based sports medicine, and the use of platelet rich plasma in the English premier league. Health Care Analysis. 2018;26:344-361. DOI: 10.1007/s10728-017-0345-7
91.Dohan Ehrenfest DM, Bielecki T, Mishra A, Borzini P, Inchingolo F, Sammartino G, et al. In search of a consensus terminology in the field of platelet concentrates for surgical use: Platelet-rich plasma (PRP), platelet-rich fibrin (PRF), fibrin gel polymerization and leukocytes. Current Pharmaceutical Biotechnology. 2012;13:1131-1137. DOI: 10.2174/138920112800624328
92.Mautner K, Malanga GA, Smith J, Shiple B, Ibrahim V, Sampson S, et al. A call for a standard classification system for future biologic research: The rationale for new PRP nomenclature. Journal of Physical Medicine and Rehabilitation. 2015;7:S53-S59. DOI: 10.1016/j.pmrj.2015.02.005
93.Marín, Fermín T, Calcei JG, Della Vedova F, Martinez Cano JP, Arias Calderon C, Imam MA, et al. Classification of platelet concentrates: From pure platelet-rich plasma (P-PRP) to leucocyte- and platelet-rich fibrin (L-PRF). Journal of ISAKOS. 2023;S2059-7754(23)00545-X. DOI: 10.1016/j.jisako.2023.07.010
94.Delong JM, Russell RP, Mazzocca AD. Platelet-rich plasma: The PAW classification system. Arthroscopy: The Journal of Arthroscopic & Related Surgery. 2012;28:998-1009. DOI: 10.1016/j.arthro.2012.04.148
Written By
Carla S. Soares, Pedro P. Carvalho and Maria dos Anjos Pires
Submitted: 27 January 2024Reviewed: 01 February 2024Published: 26 April 2024