Open Access is an initiative that aims to make scientific research freely available to all. To date our community has made over 100 million downloads. It’s based on principles of collaboration, unobstructed discovery, and, most importantly, scientific progression. As PhD students, we found it difficult to access the research we needed, so we decided to create a new Open Access publisher that levels the playing field for scientists across the world. How? By making research easy to access, and puts the academic needs of the researchers before the business interests of publishers.
We are a community of more than 103,000 authors and editors from 3,291 institutions spanning 160 countries, including Nobel Prize winners and some of the world’s most-cited researchers. Publishing on IntechOpen allows authors to earn citations and find new collaborators, meaning more people see your work not only from your own field of study, but from other related fields too.
This chapter aims to provide guidelines on implementing treatment outcome measures (TOMs) in telemedicine. It outlines the definition and the ICF classification of TOMs and highlights the considerations for integrating TOMs in telemedicine. We identified the STEERING model, which guides toward the development of effective TM systems that have the potential to promote TOMs. Furthermore, the chapter provides a roadmap on how to administer TOMs in telemedicine, with an emphasis on facilitators and barriers to this process. Finally, the chapter provides a schematic representation of selected TM systems with and without hardware and highlights the implemented TOMs in the context of the STEERING model and the three-pronged approach.
Department of Physiotherapy, Faculty of Applied Medical Science, Al-Azhar University, Gaza, Palestine
Physiotherapy Program and Center for Healthy Ageing and Wellness, Faculty of Health Sciences (H-CARE), Faculty of Health Sciences, Universiti Kebangsaan Malaysia, Jalan Raja Muda Abdul Aziz, Kuala Lumpur, Malaysia
Arimi Fitri Mat Ludin
Biomedical Science Program and Center for Healthy Ageing and Wellness (H-CARE), Faculty of Health Sciences, Universiti Kebangsaan Malaysia, Jalan Raja Muda Abdul Aziz, Kuala Lumpur, Malaysia
*Address all correspondence to: dr.suad.physio@gmail.com
1. Introduction
Treatment outcomes are essential in monitoring patients’ progress, tracking success, and evaluating the cost-effectiveness of physical, occupational, and recreational therapy, nursing, speech and language pathology, and psychiatry [1, 2, 3, 4]. Additionally, treatment outcomes are meaningful for healthcare services and policymakers as they maximize their performance, payment potential, and reimbursement, leading to the enhancement of quality care. They also serve as a strategy for accountability [2]. Integrating TOMs into clinical settings has supported HCPs in clinical decision-making, enhanced their communication, and improved patient engagement; therefore, the adoption of TOMs has facilitated the administration of clinical trials and enhanced the evidence-based development [2, 5, 6]. The WHO has defined telemedicine (TM) as the delivery of healthcare services from remote locations by all HCPs and using Information and Communication Technology (ICT) to communicate valid data about diagnosis and evaluation, treatment and prevention, research, and education of diseases and injuries with the ultimate goal of enhancing the health of individuals and communities [7]. The TM system encompasses an interface between hardware, software and a communication channel to connect two distant locations to exchange data and enable tele-consultations [8]. Telerehabilitation (TR) is a crucial subdiscipline of TM and is just as significant as TM [9], and is ought to provide diagnosis, evaluation, monitoring, prevention, supervised interventions, education, and consultation through TR systems, which include software and hardware, through a communication channel with or without cloud [10, 11]. Thereby, the TM system will be used across this chapter to refer to both the TM and TR systems. Telemedicine, likewise, TR demonstrates a safe and convenient service delivery environment with the potential to enhance treatment outcomes, including function and QoL [10]. However, little is available about the implementation and evaluation of TOMs in TM [12], which highlights the necessity of identifying guidelines for integrating treatment outcomes in telemedicine.
2. What are the treatment outcome measures (TOMs)?
Treatment outcomes are defined as significant results following an intervention episode, which refers to aspects of measurement that healthcare professionals (HCPs) intend to enhance [5]. These measurements could relate to the patient, HCPs, process, or health care system, such as pain, function, and satisfaction. Likewise, outcome measures (OMs) are defined as procedures or tools for quantifying progress toward a particular objective [5], OMs can be published evaluations that create scores or measurement methodologies and can be replicated by HCPs [1, 5].
2.1 Reporting of TOMs
Patient-reported outcomes (PROs) are defined as any data obtained directly from the patient about the outcome of healthcare, without modifications or interpretations by HCPs [13]. Simply they reflect the patients’ voice about their experience with healthcare and their ability to engage in health behaviors and activities. Raw data from PROs may be subject to variable degrees of subjectivity and biases [13, 14]. This highlights the necessity to standardize such raw data through the implementation of Patient-reported Outcome Measures (PROM), which indicates the use of a structured, standardized tool to collect data directly from the patient about his health condition, behavior, and experience with healthcare. Using such structured, standardized tools yields quantitative data that enables comparisons, and minimizes bias [13, 15]. PROMs can be either self-reported or proxy-reported. Proxy, indicating a person responds about someone else, and proxy-reported outcome refer to the collection of data from someone else who takes care of or observes the patient, such as “observer-reported measures” [14] which collect data from parents or caregivers of young children or patients who are unable to answer questions, “clinician-reported measures” is another example of proxy-reported outcomes, which are essential in case there is a need to gather complementary data. However, sometimes, it lacks accuracy [13]. Lastly, the performance measure (PM) refers to the quantification of health care quality for a hospital, health plan, nursing home, clinician, etc. [13, 15]. Careful selection of PROMs, considering the concept model, validity, reliability, responsiveness, interpretability, feasibility, variable methods of administration, cultural and language adaptations, and electronic health records, helps employ them in performance measurement, particularly quality of care [13]. Although challenged, PROMs have been increasingly incorporated into various disciplines of clinical practice and research and have resulted in identifying care gaps and unmet needs, prioritizing patients’ requirements, and enhancing the quality of care [14, 16, 17].
2.2 Methods of administration of PROMs
PROMs vary in how they are administered in clinical practice; the source of data could be self-reported or proxy-reported [13, 14], and the method of administration may be paper and pencil or electronic using a computer or digital platforms such as app-based interface, web-based chatbot interface, and a speech-operated Alexa interface [13, 18]. They also vary in the mode of administration to be self-administered or interviewer-administered; the setting of administration either at home or in healthcare facilities; and finally, PROMs vary in their scoring system, which may administer raw data or probability data [13].
2.3 Barriers and facilitators of administering PROMs
In routine practice, the administration of PROMs has been challenged by factors related to the patients and caregivers, the healthcare system, and the HCPs [16, 19, 20]. Patients’ and caregivers’ related factors include the lack of time and understanding of the significance of PROMs, concerns about their privacy and relationship with HCPs, and difficulties using the assessment tools, either paper-based or electronic-based [16, 19]. The HCPs-related factors encompass lack of knowledge and experience in administering PROMs, lack of training opportunities, lack of time for the convenient administration of PROMs, interpretation, and integration of them into routine clinical practice, and difficulties in using the electronic-based PROMs [16, 19, 21]. System barriers include inadequate resources for implementing PROMs, lack of ICT infrastructure to administer electronic-based measures, difficulties in integrating PROs into routine clinical practice and workflow, inability to utilize PROMs data effectively, and low institutional support for implementing PROMs [16, 19, 20]. The contextual variations are crucial as well; most PROs have been developed and standardized for Western, well-resourced settings, which is unsuitable for other settings unless standardized [19].
Facilitators for administering PROMs are the identification of HCP roles, allocation of sufficient time and resources for implementing and interpreting them, enhancement of knowledge and skills related to the administration of PROMs, including training of professionals, awareness of patients and their caregivers, and consolidated evidence of PROMs role in saving time and enhancing quality care for policymakers. Additional facilitators would be integrating PROMs into clinical practice and flow through reliable procedures, and building up or making the ICT infrastructure available for HCPs [21].
2.4 Patient-centric care (PCC)
Patient-centered care is where HCPs partner with patients and their families to design and deliver individual healthcare by responding to their preferences, needs, and values. PCC has been associated with enhanced patient’ experience, positive TOMs, reduced cost of healthcare, and diminished length of hospital stay and rate of readmissions [22]. Patient-centric e-health identifies the patient’s focus, activity, and empowerment. However, evidence shows that the focus of e-health is the needs of healthcare providers and organizations, with consideration of patients’ acceptability factors [13]. The administration of PROMs in telemedicine has the potential to enhance patient centricity by enhancing access, engagement, ongoing tracking, and patient-HCP relationships [13, 18].
2.5 The ICF classification of function
The International Classification of Function (ICF) is a dictionary that sorts terms in logical and hierarchical order. It was identified by the World Health Organization (WHO) and underpins definitions, classifications, measurement, and policy of functions and disability of health conditions [23, 24]. The ICF identifies three levels of human performance: body, entire person, and whole person in a social setting. Thus, it integrates the medical and social domains and provides a comprehensive understanding of health [23]. The ICF has been utilized in defining research variables, locating literature in databases, describing patients’ health conditions in guidelines and formal documents, and assisting in developing and selecting the proper assessment tools (PROMs) for patients through the rehabilitation pathway [24]. For example, the ICF has been deployed in the development of TOMs for physiotherapy, occupational therapy, and speech pathology disciplines [25]; it has also been implemented to select the most appropriate items for the assessment of ankylosing spondylitis, which cover most of the ICF core set and best represent the patients’ health status [26]. The ICF has been implemented in clinical practice and research to categorize TOMs for body function and structure, activity, and participation [1, 2, 27]. Deploying the ICF has augmented neurorehabilitation strategies [28], simplified the common language of function and disability, encouraged innovative ways of measuring them [29], and provided more consistent results related to patients’ health recovery than conventional PROMs [30].
2.6 The ICF categories and core set
The ICF is a common framework to understand and describe function and disability [31]. The first prospect is body function and structure, denoted as “b” and “s”, respectively. It contains physiological and psychologic functions and anatomical characteristics. Activity denoted by “d” refers to a wide spectrum of purposeful planned actions performed by the individual within life situations, such as climbing stairs. Participation, also denoted by “d” is the activities that are crucial for economic and social life, such as holding a job. The environmental factors are the physical, social, and attitudinal factors individuals live and conduct their lives and are denoted by “e” [23, 31]. Personal factors are a particular background of an individual, such as gender, age, and education, but they are not yet coded within the ICF. The hierarchical classification of the ICF categories identifies four levels, represented by numerical codes, starting with the chapter number of one digit, followed by the second level, two digits, and then the third and fourth levels, each of one digit; the lower the level, the more incremental information. For example, b2 refers to sensory functions and pain (first level), b280 refers to the sensation of pain (second level), b2801 is the pain in the body part (third level), and b28013 is pain in the back (fourth level). The ICF categories are arranged in a stem-branch-leaf scheme, starting with the component letter with one, two, three, or four digits, corresponding to the code of the categories [24, 31]. The ICF qualifier is the state of the health level or the degree of severity of a problem of concern. It is coded as the first, second, third, or fourth number after the decimal point [24]. The ICF core set was developed based on a robust scientific methodology and provides a category list that is essential for specific medical conditions and contexts related to healthcare, which facilitates the creation of a patient’s functional profile in a variety of situations, including clinical practice [31].
2.7 How the ICF has been deployed for the mapping of PROMs?
Given that the ICF is the universal consolidated language of defining function and health, HCPs and researchers have been deploying the ICF to map PROMS qualitatively using the linkage rules, quantitatively using the Rasch model, and a combined quantitative and qualitative mapping to transfer information from electronic records. Qualitative mapping can also be utilized to compare the content of measuring instruments [32]. The PROMs have been coded using the ICF core set; for example, the EQ-5D-5L Dimension can be coded by identifying its main domains: mobility (d4), self-care (d5), usual activities unspecified: remunerative employment (d850), pain/discomfort (b152), anxiety/depression (b152) [30]. The ICF qualifiers for this instrument have been implemented before and after rehabilitation intervention on a 0–4 scale outlining the level of impairment, limitation, or restriction, stated as (4) complete; (3) severe; (2) moderate; (1) mild; and (0) no problem [30].
2.8 Administering TOMs in telemedicine
Administration of TOMs in telemedicine should consider factors related to changes in the context and environments of testing, changes in the method of data collection, and the lack of HCP supervision. We should also consider telemedicine’s objective to promote the health of individuals and communities.
2.9 Consider the psychometric properties
It is highly essential to deploy valid, reliable, and responsive TOMs, which contribute to the validity of results, the effectiveness of the intervention, and ultimately, the enhancement of the patients’ and community’s trust in healthcare service [33]. Validity refers to the extent to which an instrument measures what it is intended to measure [34], it entails the selection of an accurate, and appropriate assessment tool. For example, when treating a patient with diminished cardiovascular fitness, the six-minute walk test (6 MWT) is appropriate to assess aerobic capacity and endurance [35]. Criterion, concurrent, and predictive validity were also considered in clinical practice and research [1, 34]. Validity considers the population and the context of evaluation, suggesting that any changes in them would make changes in validity [1, 34]. For example, validity values of the six-MWD for geriatrics differ from those related to patients with stroke, COPD, or spinal cord injury (SCI), values of criterion and construct validity values also differ [35]. Reliability is the degree to which the TOM is free of random error, therefore, a test with high reliability produces consistent findings over several tries, and relative reliability identifies the inter-rater, intra-rater reliability, and internal consistency [1, 34]. Systematic errors can potentially influence reliable tests, leading to incorrect results. For example, errors due to fatigue, lack of attention, inaccuracy, or a lack of clear instructions and inaccurate interpretation [1, 34]. Responsiveness indicates response to change, which is the ability of the measure to identify change throughout the time of the construct to be examined [1, 33]. Thus, PROMs should be sensitive to detect changes induced by the healthcare intervention provided by TM. Limitations of responsiveness include the multi-trial scales, the PROMs that provide a categorical or limited number of response options, and PROMs with extended reporting periods are unlikely to detect responsiveness if they are implemented frequently over a short period [13].
2.10 The necessity for validation in the tele-contexts
Given that validity is defined concerning the context of measurement, including the study population and settings, it is crucial to consider the effects of utilizing different modes or procedures than the one used for validation of the PROMs [13]. In telemedicine, the application of TOMs raises many questions about the population, the PROMs, the technology, and the healthcare system [36]; besides, contextual factors, especially the site impact, the overall usage of the TM system [37]. The change in how data collection has been performed by the use of mHealh, web-based measures, sensors, cameras, movement trackers, or any combination of them, with possibility of miscalibration, misconduct, and potential measurement errors, including both random and systematic errors, draws questions about the PROMs applicability, validity, and reliability in remote settings and highlights the necessity for validation in tele-contexts [13, 18]. In total, the population, the measuring environment, the PROMs, and the context of evaluation along with the data collection methods should be re-evaluated in TM practice as they impose potential variations in validity and reliability values. On the contrary, electronic data collection facilitates the incorporation of data within health records, with increasing possibilities for integration in clinical practice workflow.
2.11 The complex barriers to administering PROMs in telemedicine
Barriers to integrating TOMs into telemedicine can be explained by considering the complex barriers of deploying both PROMs and TM systems in clinical practice. Barriers to deploying PROMs were attributed to personal, professional, as well as institutional factors, while the deployment of TM systems is challenged by the high cost of development, difficulties in implementing and utilizing high-tech solutions at personal and institutional levels, the low rates of technology acceptance, especially for the elderly, who claim that it is a disruption of their privacy and security, the low confidence in diagnostic accuracy despite of its adequacy, and the digital literacy, especially for elderly [8]. Specifically, barriers to implementing TOMs in telemedicine may include, but are not limited to, patient health literacy, HCPs’ resistance to deploying PROMs in practice, insufficient understanding of the optimal way to utilize TOMs results in clinical practice [36], issues related to platform design, inexperience with PROMs devices, computer literacy, and lack of IT infrastructure for data collection [18, 20]. In total, the Implementation of PROMs in telemedicine is challenged by patients, HCPs, and healthcare system-related factors, along with the difficulties in deploying the TM system. Therefore, it is recommended to provide adequate training to HCPs, with consideration of their contexts, and enhance awareness about TOMs for patients and administrative leaders [19]; additionally, it is recommended to consider PROMs impeded in telemedicine for patients with chronic disorders who require numerous consecutive visits, where PRO is essential for follow-up and monitoring. Any new patient admission requires the awareness and training of patients, HCPs, and administrative leaders [36].
2.12 Telemedicine and TOMs; the proposed approaches to simplify the complex equation
To simplify the concept of integrating TOMs in telemedicine, we worked in an organized manner to map the reported TOMs in the developed TM systems for noncommunicable diseases (NCDs) over the last 5 years. We identified keywords and synonyms, and developed search strings. We then searched on three databases: EBSCO, WOS, and PubMed. The resulting studies were screened through two stages: for the title and abstract, and then for the whole document. Accordingly, we randomly selected the mapped RCTs to represent the developed TM systems for the NCDs, including musculoskeletal [38], cancer [39, 40], metabolic disorders including DM [37, 41], cardiovascular disorders [42, 43], and chronic pulmonary diseases [44, 45]. Mapping of these RCTs has resulted in the identification of the STEERING model to develop TM systems for effectively enhancing TOMs and the identification of the three-pronged approach to integrate TOMs into TM systems.
2.13 The STEERING model: Develop effective TM systems to enhance TOMs
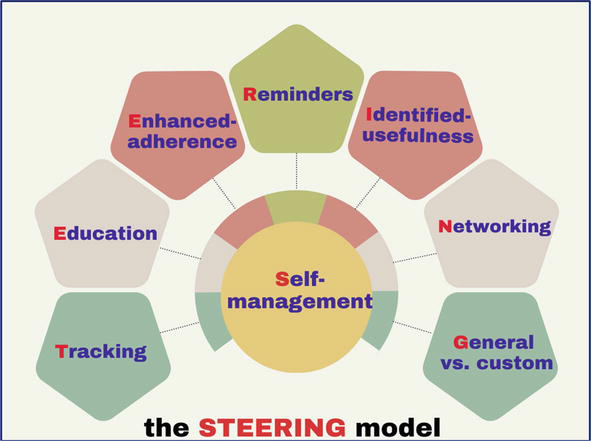
An effective TM system that contributes to the enhancement of the TOMs is based on eight pillars: self-management, tracking, education, enhanced adherence strategies, reminders, identified usefulness, networking, and generalized vs. individualized features, as shown in Figure 1.
Figure 1.
The STEERING model: development of an effective TM system that has the potential to enhance TOMs; self-management is the gear.
2.13.1 Self-management (SM)
Involves the transfer of knowledge and utilization of patients’ self-regulation skills to control their chronic disease, manipulate risk factors, and engage in healthy behaviors [46, 47]. SM skills encompass identifying goals, self-monitoring, reflective thinking, self-evaluation, decision-making, execution of certain behaviors, coping skills, and control of physical, emotional, and cognitive responses to changes in health conditions [46, 48]. Telemedicine has been successfully implemented to promote SM behaviors of chronic diseases and has contributed to the enhancement of TOMs [49, 50, 51]. The implemented SM programs were multicomponent, deployed mostly for adults, and occasionally for children and caregivers, either in clinical or home environments by multidisciplinary HCPs. Additionally, SM programs provide support for disease and symptoms management, drug management, psychosocial concerns, lifestyle modifications, communication, social support, and career planning [51].
2.13.2 Tracking
Refers to the information relating to itemized coding of procedures and costs associated with healthcare delivery, used as a means for tracking healthcare utilization, patterns of care, and treatment outcomes [52], it is an integral component of any TM system, that allows ongoing remote monitoring of changes in participant status of the body function and structure, activity, and participation through utilizing TOMs and other means [50, 53]. The literature highlighted the benefits of self-monitoring, implemented in TM, compared to traditional monitoring methods, and showed its contribution to enhancing SM and TOMs [54, 55, 56].
2.13.3 Education
Health education, in variable forms, is effective in enhancing knowledge and satisfaction and promoting readiness to engage in health behaviors [46, 57], and it has been implemented along with SM and contributed to enhancing its efficiency and effectiveness, along with improvements of TOMs [50, 57, 58, 59, 60]. such as fasting blood glucose, blood pressure, and QOL in chronic kidney disease [61], anxiety, weight loss, physical activity, and the post-enrolment rate at hospitals in chronic care [50].
2.13.4 Enhanced adherence
Adherence is the extent to which the users follow the program as intended [62]. Despite the effectiveness of TM in augmenting patients and healthcare systems in chronic disease management, there is a high rate of attrition and dropout among patients with health conditions [62, 63, 64]. Nonadherence has threatened treatment effectiveness, led to an increased number of hospitalizations, and is considered a significant concern in developing the TM system [62]. Engagement strategies to enhance adherence involve but are not limited to, portability [18], the development of customized features, push-up notifications, easy access, handling, and data sharing, along with adjustable speed [18, 62, 64]. Additionally, patient characteristics, and meeting their specific needs, along with appropriate recruitment channels pose the potential to enhance adherence; adherence and engagement scores can be computed and assist in more effective application [62, 64].
2.13.5 Reminders
Reminders, either automated or prompted by HCPs, are one of the mastery experience procedures of the mHealth apps [65], as they encourage adherence, commitment, and management of time constraints to the prescribed interventions targeting SM [62, 65, 66, 67], and enhances the participants’ self-efficacy levels by encouraging users to use the app, read self-care advice, or self-monitor symptoms [65]. Reminders can also be used to scale up the telemedicine interventions in cohort studies as a retention procedure [62].
2.13.6 Identified usefulness
This is one of the influential factors toward adherence to telemedicine. Typically, the belief factors, including perceived usefulness have been a part of the Technology Acceptance Model (TAM); a powerful tool implemented widely to measure the users’ acceptance of technology-based interventions such as telemedicine [68]. It is essential to discuss with patients and caregivers the actual benefits of the TM system and to avoid overstatement, as the expectation-confirmation theory states that the patients would confirm such usefulness while using the tool. Meeting users’ expectations through confirmation, has the potential to maximize their intention to use and enhance satisfaction, and therefore facilitate lifestyle improvements [69, 70].
2.13.7 Networking
Creating variable forms of networking, such as study communities [67], community clinical linkages [71], or peer-led SM programs [72] has enhanced users’ engagement, facilitated the transfer of knowledge and experience among patients, peers, researchers, and HCPs, augmented reminders about self-care tasks, served as a useful tool to update participants about the progress, empowered participants to overcome barriers and share their experience, facilitates problem-solving, daily management, and behavioral modifications, provided the social and emotional support, and enhanced suers’ linkages to clinical care, therefore, these benefits have the potential for motivation, self-efficacy, and SM and eventually improvement of TOMs and PM [67, 71, 72].
2.13.8 Generalized vs. customized features
The development of TM systems is initiated by targeting certain populations, identifying their needs, and developing general features to meet the population’s needs [10]. However, researchers recommend personalization of some features to enhance functionalities of the TM systems such as tailored education, symptoms management advice [66, 73], and the closed loop feedback system which allows HCPs to react in time with individualized adjustment to patient care [74]. The self-development of goals, reminders, and positive feedback upon achieving these goals have shown effectiveness in enhancing personal acceptance and commitment, facilitating personalized care, empowering behavioral changes, and eventually, improving the TOMs [75]. Moreover, personalized reminders, feedback, and stories have enhanced adherence, engagement, and SM [53, 62, 65].
Based on the mentioned methodology, we analyzed randomly several TM systems that were developed for variable NCDs, the mapped system, shown in Table 1. has been built upon the “STEERING” model. Self-management, tracking, and education have been reported in 9/9 of the mapped systems, networking and generalized vs. individualized features have been reported in 8/9 of the mapped systems, enhanced adherence and reminders have been reported in 7/9 of the charted systems, the identified usefulness has been charted only in one system; we assume that such low value is attributed to the usual practice of including awareness of the interventions in the education module. Almost seven out of nine interventions have positively enhanced the TOMs either in the body function and structure, participation, or in the environmental factors’ domain.
(−) 1ry OMs. (+) utilization & cost-efficient. - lead to less sedentary
√
√
√
√
—
—
√
√
Table 1.
The STEERING model for the development of an effective TM system to enhance the TOMs; (+) indicates improvement, (−) indicates no improvement.
2.14 TOMs in the scope of telemedicine and the ICF core set
TM refers to the utilization of ICT to provide healthcare services while the patient is physically presented in a different environment, this obliges the inclusion of new OMs related to the tele-contexts and constructs. On the other hand, the ICF classifies human function and health based on body function and structure, activity, participation, and with consideration of environmental factors. Utilizing the ICF framework in clinical practice and research has brought several advantages as described previously, which triggered our attempt to use the ICF classification to map the OMs, including both TOMs and PMs, across the developed TM systems. We hope that the results of this attempt will help researchers and HCPs plan, administer, and interpret the interventions including TOMs within the context of telemedicine.
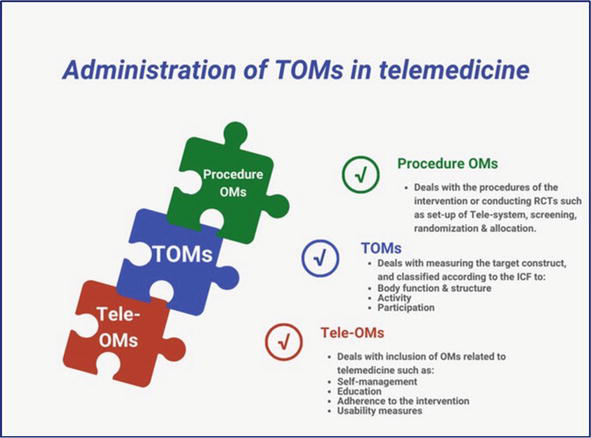
We employed the results of the search strategy described previously to analyze the randomly selected RCTs, accordingly, we identified the three-pronged approach to utilize the OMs across the developed TM systems as shown, in Figure 2. The first dimension is the procedure OMs, which refers to the pre-trial procedure that is implemented to initiate TM systems. The second is the TOMs, sorted based on the ICF’s body function and structure, activity, and participation, and refers to the change in the health status of the participants. The tele-OMs refer to the measurements of constructs related to the tele-contexts and are equivalent to the environmental factors of the ICF. It is worth noting that the three-pronged approach identified in Figure 2 and described in Table 2 is not synonymous with functional profile, nor is a mapping of the OMs using the ICF categories; such work requires more detailed description along with more collaboration of multidisciplinary teams, which is beyond the concept of this chapter. Rather, the three-pronged approach is an attempt to facilitate the administration of the OMs into telemedicine based on the ICF domains.
Figure 2.
Administration of OMs into telemedicine through the three-pronged approach: (1) Procedure OMs, (2) TOMs, and (3) tele-OMs.
DTSQs: The Diabetes Treatment Satisfaction Questionnaire status version
BP: blood pressure, SBP: systolic BP,
HP: hypertension, DBP: diastolic BP
MMAS-6: The 6-item Morisky Medication Adherence Scale
QLQ-C30 version 3: Core Quality of Life
EORTC: The European Organization for Research and Treatment of Cancer
PAID: problem areas in diabetes
GAS: goal attainment scaling
PEI: patient enablement instrument
MRC: medical research council
CAT: COPD assessment test
SDSCA: the summary of diabetes self-care activities measure
MSAS: Memorial Symptom Assessment Scale: global, psychological, and physical symptoms
EORTC QLQ-BR45: Updated Breast Cancer Module
MARS: Mobile App Rating Scale
SCNS-SF34: supportive Care Needs Survey Short-Form
STAI-R: State-Trait Anxiety Inventory-Revised
CASE-CANCER: Communication and Attitudinal Self-Efficacy Scale for cancer
WLQ: Work Limitations Questionnaire
PADS-revised: Physical Activity and Disability Survey–revised
CHD: Coronary Heart Disease
K-BILD: King’s Brief Interstitial Lung Disease health status questionnaire
PESaM: Patient Experiences and Satisfaction with Medication questionnaire
GRC: Global Rating of Change
DLCOc: Diffusing Capacity Of The Lungs For Carbon Monoxide
SGRQ: St. George’s Respiratory Questionnaire
BCKQ: Bristol COPD Knowledge Questionnaire
WC: Waist Circumference,
HC: Hip Circumference
PIH: Partners in Health
FACT-G: Functional Assessment of Cancer Therapy -General
Table 2.
Examples of administering TOMs in clinical research/RCTs.
2.14.1 Procedure OMs
Refers to the pre-trial procedures that are implemented by researchers and HCPs to initiate TM systems. This includes screening, randomization, allocation, and setting up the TM system for NCDs. For example, screening of patients with hypertension focused on baseline values of blood pressure > 140/90 mm Hg (b420), participants’ willingness to self-monitoring, and their access to the internet [42]. We tried to link these measures to their equivalent ICF categories; however, we could not locate an ICF equivalent to self-monitoring, instead, we located the closest category: self-care (d5), self-care unspecified (d599), or looking after one’s health (d570). The same issue applies to access to the internet within the e category; we located the closest category, products and technology for communication (e125), and products and technology, unspecified (e199).
2.14.2 Treatment OMs
Refers to the measurement of the intended change in the health status of participants. Regardless of the classification of these measures by the original work, here we classified the TOMs according to the ICF; therefore, TOMs will be grouped by body function and structure, activity, and participation. In the mentioned study of measuring OMs related to hypertension [42], body function expressed in systolic blood pressure (b420), weight equivalent to the body weight maintenance function (b530), physical activity could be equivalent to mobility unspecified (d499), or walking (d450), and moving (d469), healthy eating could be equivalent to eating (d550), salt and alcohol reduction could be equivalent to Products or substances for personal consumption (e110). The EuroQoL-5D-5L was coded previously to its main domains: mobility (d4), self-care (d5), and usual activities unspecified: remunerative employment (d850), pain/discomfort (b152), anxiety/depression (b152) [30].
2.14.3 Tele-OMs
Refers to the measures used to implement the telemedicine interventions through the tele-context, this dimension encompasses the environmental factors’ domain of the ICF as well as the performance measure of the healthcare service. This could include some instruments used to be implemented in routine clinical practice; however, administration of these instruments in tele-context requires revalidation and consideration of the new environment. For example, deploying self-management, self-monitoring, remote education, engagement, and adherence in tele-context would impose differences from the routine clinical practice. In the above-mentioned intervention, researchers implemented several instruments to measure patients’ interaction with the tele-context [42] such as engagement with the digital tool which is closely equivalent to products and technology, unspecified (e199), motivate healthy behaviors is closely equivalent to support and relationships, unspecified (e399), drug adherence is closely equivalent to products or substances for personal consumption (e110), cost of service is closely equivalent to health services, systems and policies (e580), and the patient enablement instrument focuses on participant’s ability to cope with life and illness, ability to keep health and help himself, and confident about health are equivalent to self-care unspecified (e599), along with understand illness which is equivalent to mental functions, unspecified (b199).
In concrete terms, the proposed approach to integrating OMs into telemedicine focuses on the deployment and distribution of these instruments over the pathway of conducting clinical interventions and research, starting from the preparatory phase until the final evaluation phase. Here we raise three major concerns: the first is that the distribution of the OMs is not always consistent with the ICF domain; for example, the EuroQoL-5D-5L was categorized under the ICF-participation domain while it constitutes body function, activity, and participation. The second concern is that we could not locate the exact ICF equivalent category for several measures, especially those related to tele-OMs, and we either identified an unspecified ICF category or kept that instrument without locating the equivalent category. This highlights the necessity for further work to identify concepts related to telemedicine in the ICF core set. Third, the procedure OMs, as described previously, has the potential to include measures from all ICF domains: body function, structure, activity, participation, and environmental factors. However, the personal factor is missing in the ICF despite its significance [76].
In conclusion, this chapter provides an overview of treatment outcomes, its measures, and reporting, focused on the value of integrating it into clinical practice and research, along with the barriers and facilitations of its implementation. The chapter also highlights the main issues of implementing TOMs in telemedicine, exemplified by the necessity of evaluating the TOMs in the tele-context for validity and reliability. We identified two measures to facilitate the administration of TOMs in telemedicine; the first is the STEERING model, which, we claim, would contribute to the development of an effective TM system that helps promote TOMs. The second is the three-pronged approach, which could facilitate the administration of TOMs through clinical intervention and research related to telemedicine.
This is groundwork that we hope to build upon in the future to provide more consolidated models and approaches that help HCPs and researchers implement TOMs in tele-contexts in clinical practice and research. Although we conducted a robust methodology in identifying the interventions eligible for analysis, we could only work with a small number of them to align the space of this chapter. We strongly recommend that future work include a large number of studies to further validate the STEERING model and the three-pronged approach. Finally, we highlighted the requirement to update the ICF core set to include telemedicine as an emerging discipline, however, few studies have been conducted on this aspect, and we urge researchers to focus on this area of research.
2.Hill K, Denisenko S, Miller K, Clements T, Batchelor F, Morgan P. Clinical Outcome Measurement in Adult Neurological Physiotherapy. 4th ed. Melbourne: Australian Physiotherapy Association, National Neurology Group; 2010. pp. 3-6
3.Liu Y, Avant KC, Aungsuroch Y, Zhang X-Y, Jiang P. Patient outcomes in the field of nursing: A concept analysis. International Journal of Nursing Sciences. 2014;1(1):69-74
4.Moyse K, Enderby P, Chadd K, Gadhok K, Bedwell M, Guest P. Outcome measurement in speech and language therapy: A digital journey. BMJ Health & Care Informatics. 2020;27(1):1-6
5.Kaplan SL. Outcome Measurement and Management: First Steps for the Practicing Clinician. USA: Philadelphia: F.A.Davis; 2007
6.Van Herck P, De Smedt D, Annemans L, Remmen R, Rosenthal MB, Sermeus W. Systematic review: Effects, design choices, and context of pay-for-performance in health care. BMC Health Services Research. 2010;10(1):1-13
7.World Health Organization. Telemedicine Opportunities and Developments in Member States. Geneva: WHO; 2010. ISBN 978 92 4 156414 4
8.Khemapech I, Sansrimahachai W, Toachoodee M. Telemedicine–meaning, challenges and opportunities. Siriraj Medical Journal. 2019;71(3):246-252
9.Brienza DM, McCue M. Introduction to Telerehabilitation. London: Springer London; 2012. pp. 1-11
10.Ghaben SJ, Mat Ludin AF, Mohamad Ali N, Beng Gan K, Singh DKA. A framework for design and usability testing of telerehabilitation system for adults with chronic diseases: A panoramic scoping review. Digital Health. 2023;9:20552076231191014
11.Shem K, Irgens I, Alexander M. Chapter 2 - getting started: Mechanisms of telerehabilitation. In: Alexander M, editor. Telerehabilitation. New Delhi: Elsevier; 2022. pp. 5-20
12.Yoshida Y, Patil SJ, Brownson RC, Boren SA, Kim M, Dobson R, et al. Using the RE-AIM framework to evaluate internal and external validity of mobile phone–based interventions in diabetes self-management education and support. Journal of the American Medical Informatics Association. 2020;27(6):946-956
13.Cella D, Hahn EA, Jensen SE, Butt Z, Nowinski CJ, Rothrock N, et al. Patient-reported outcomes in performance measurement. 2015
14.Huemer M, Bösch F. Measuring what matters: Why and how to include patient reported outcomes in clinical care and research on inborn errors of metabolism. Journal of Inherited Metabolic Disease. 2023;46(5):796-805
15.Van der Wees PJ, Nijhuis-Van Der Sanden MW, Ayanian JZ, Black N, Westert GP, Schneider EC. Integrating the use of patient-reported outcomes for both clinical practice and performance measurement: Views of experts from 3 countries. The Milbank Quarterly. 2014;92(4):754-775
16.Nguyen H, Butow P, Dhillon H, Sundaresan P. A review of the barriers to using patient-reported outcomes (PROs) and patient-reported outcome measures (PROMs) in routine cancer care. Journal of Medical Radiation Sciences. 2021;68(2):186-195
17.Sørensen NL, Hammeken LH, Thomsen JL, Ehlers LH. Implementing patient-reported outcomes in clinical decision-making within knee and hip osteoarthritis: An explorative review. BMC Musculoskeletal Disorders. 2019;20:1-8
18.Golden AH, Gabriel MH, Russo J, Price M, Ruhmel S, Nilsson A, et al. Let’s talk about it: An exploration of the comparative use of three different digital platforms to gather patient-reported outcome measures. Journal of Patient-Reported Outcomes. 2023;7(1):130
19.Barth CA, Donovan-Hall M, Blake C, Akhtar NJ, Al-Barawi S, Kazibwe H, et al. “Otherwise… he will be a beggar”: A focus group study to understand the perspectives of physiotherapists about measuring rehabilitation outcomes and impact in low-resource and conflict-affected settings. Disability and Rehabilitation. 2023;45:1-12
20.Spencer KL, Absolom KL, Allsop MJ, Relton SD, Pearce J, Liao K, et al. Fixing the leaky pipe: How to improve the uptake of patient-reported outcomes–based prognostic and predictive models in cancer clinical practice. JCO Clinical Cancer Informatics. 2023;7:e2300070
21.Nguyen H, Butow P, Dhillon H, Morris L, Brown A, West K, et al. Using patient-reported outcomes (PROs) and patient-reported outcome measures (PROMs) in routine head and neck cancer care: What do health professionals perceive as barriers and facilitators? Journal of Medical Imaging and Radiation Oncology. 2020;64(5):704-710
22.Santana M-J, Ahmed S, Lorenzetti D, Jolley RJ, Manalili K, Zelinsky S, et al. Measuring patient-centred system performance: A scoping review of patient-centred care quality indicators. BMJ Open. 2019;9(1):1-10
23.WHO. Towards a Common Language for Functioning, Disability and Health ICF. Geneva: WHO; 2002
24.Heerkens Y, Hendriks E, Oostendorp R. Assessment instruments and the ICF in rehabilitation and physiotherapy. Medical Rehabilitation. 2006;10:11-20
25.Perry A, Morris M, Unsworth C, Duckett S, Skeat J, Dodd K, et al. Therapy outcome measures for allied health practitioners in Australia: The AusTOMs. International Journal for Quality in Health Care. 2004;16(4):285-291
26.Kiltz U, Van Der Heijde D, Boonen A, Cieza A, Stucki G, Khan M, et al. Development of a health index in patients with ankylosing spondylitis (ASAS HI): Final result of a global initiative based on the ICF guided by ASAS. Annals of the Rheumatic Diseases. 2014. DOI: 10.1136/annrheumdis-2013-203967
27.Grover P, Holt D. Outcome Measurement in Rehabilitation. 2017.
28.Lexell J, Brogårdh C. The use of ICF in the neurorehabilitation process. NeuroRehabilitation. 2015;36(1):5-9
29.Madden RH, Bundy A. The ICF has made a difference to functioning and disability measurement and statistics. Disability and Rehabilitation. 2019;41(12):1450-1462
30.Calvo M, Subirats L, Ceccaroni L, Maroto JM, De Pablo C, Miralles F. Automatic assessment of socioeconomic impact on cardiac rehabilitation. International Journal of Environmental Research and Public Health. 2013;10(11):5266-5283
31.ICF Research Branch. ICF Core Sets in Clinical PRactice. ICF-Based Documentation Tool Göttingen. 2nd ed. Germany: Hogrefe; 2020. Available from: https://www.icf-core-sets.org/
32.Kelvin L. ICF-based classification and measurement of functioning. European Journal of Physical and Rehabilitation Medicine. 2008;44:315-328
33.Mokkink LB, Prinsen CA, Bouter LM, de Vet HC, Terwee CB. The consensus-based standards for the selection of health measurement instruments (COSMIN) and how to select an outcome measurement instrument. Brazilian Journal of Physical Therapy. 2016;20:105-113
34.Leslie G, Portney DG. Concepts of measurement validity. In: Pine J, editor. Foundations of Clinical Research: Applications to Evidence-Based Practice. 4th ed. Philadelphia, USA: F.A Davis; 2020. pp. 127-140
35.Physiopedia. Six Minute Walk Test / 6 Minute Walk Test. Available from: https://www.physio-pedia.com/Six_Minute_Walk_Test_/_6_Minute_Walk_Test
36.Schougaard LMV, Larsen LP, Jessen A, Sidenius P, Dorflinger L, de Thurah A, et al. AmbuFlex: Tele-patient-reported outcomes (telePRO) as the basis for follow-up in chronic and malignant diseases. Quality of Life Research. 2016;25:525-534
37.Agarwal P, Mukerji G, Desveaux L, Ivers NM, Bhattacharyya O, Hensel JM, et al. Mobile app for improved self-management of type 2 diabetes: Multicenter pragmatic randomized controlled trial. JMIR mHealth and uHealth. 2019;7(1):e10321
38.Plow M, Golding M. Using mHealth technology in a self-management intervention to promote physical activity among adults with chronic disabling conditions: Randomized controlled trial. JMIR mHealth and uHealth. 2017;5(12):e6394
39.Maguire R, McCann L, Kotronoulas G, Kearney N, Ream E, Armes J, et al. Real time remote symptom monitoring during chemotherapy for cancer: European multicentre randomised controlled trial (eSMART). BMJ. 2021;374(8301):1-14
40.Basch E, Schrag D, Henson S, Jansen J, Ginos B, Stover AM, et al. Effect of electronic symptom monitoring on patient-reported outcomes among patients with metastatic cancer: A randomized clinical trial. Journal of the American Medical Association. 2022;327(24):2413-2422
41.Yang Y, Lee EY, Kim H-S, Lee S-H, Yoon K-H, Cho J-H. Effect of a mobile phone–based glucose-monitoring and feedback system for type 2 diabetes management in multiple primary care clinic settings: Cluster randomized controlled trial. JMIR mHealth and uHealth. 2020;8(2):e16266
42.McManus RJ, Little P, Stuart B, Morton K, Raftery J, Kelly J, et al. Home and online management and evaluation of blood pressure (HOME BP) using a digital intervention in poorly controlled hypertension: Randomised controlled trial. BMJ. 2021;372(8276):1-13
43.Maddison R, Rawstorn JC, Stewart RA, Benatar J, Whittaker R, Rolleston A, et al. Effects and costs of real-time cardiac telerehabilitation: Randomised controlled non-inferiority trial. Heart. 2019;105(2):122-129
44.Stamenova V, Liang K, Yang R, Engel K, van Lieshout F, Lalingo E, et al. Technology-enabled self-management of chronic obstructive pulmonary disease with or without asynchronous remote monitoring: Randomized controlled trial. Journal of Medical Internet Research. 2020;22(7):e18598
45.Moor CC, Mostard RL, Grutters JC, Bresser P, Aerts JG, Chavannes NH, et al. Home monitoring in patients with idiopathic pulmonary fibrosis. A randomized controlled trial. American Journal of Respiratory and Critical Care Medicine. 2020;202(3):393-401
46.Ryan P, Sawin KJ. The individual and family self-management theory: Background and perspectives on context, process, and outcomes. Nursing Outlook. 2009;57(4):217-225 e6
47.Hessler DM, Fisher L, Bowyer V, Dickinson LM, Jortberg BT, Kwan B, et al. Self-management support for chronic disease in primary care: Frequency of patient self-management problems and patient reported priorities, and alignment with ultimate behavior goal selection. BMC Family Practice. 2019;20:1-10
48.Martz E. Promoting Self-Management of Chronic Health Conditions: Theories and Practice. New York, USA: Oxford University Press; 2017
49.Wang H, Ho AF, Wiener RC, Sambamoorthi U. The association of mobile health applications with self-management behaviors among adults with chronic conditions in the United States. International Journal of Environmental Research and Public Health. 2021;18(19):10351
50.Obro LF, Heiselberg K, Krogh PG, Handberg C, Ammentorp J, Pihl GT, et al. Combining mHealth and health-coaching for improving self-management in chronic care. A scoping review. Patient Education and Counseling. 2021;104(4):680-688
51.Allegrante JP, Wells MT, Peterson JC. Interventions to support behavioral self-management of chronic diseases. Annual Review of Public Health. 2019;40:127-146
52.Pubmed-Mesh. Administrative claims, healthcare. 2016. Available from: https://www.ncbi.nlm.nih.gov/mesh/2009747
53.Cho Y, Zhang H, Harris MR, Gong Y, Smith EL, Jiang Y. Acceptance and use of home-based electronic symptom self-reporting systems in patients with cancer: Systematic review. Journal of Medical Internet Research. 2021;23(3):e24638
54.Turner-McGrievy GM, Beets MW, Moore JB, Kaczynski AT, Barr-Anderson DJ, Tate DF. Comparison of traditional versus mobile app self-monitoring of physical activity and dietary intake among overweight adults participating in an mHealth weight loss program. Journal of the American Medical Informatics Association. 2013;20(3):513-518
55.Greenwood DA, Young HM, Quinn CC. Telehealth remote monitoring systematic review: Structured self-monitoring of blood glucose and impact on A1C. Journal of Diabetes Science and Technology. 2014;8(2):378-389
56.Ong T, Van Citters AD, Dowd C, Fullmer J, List R, Pai S-A, et al. Remote monitoring in telehealth care delivery across the US cystic fibrosis care network. Journal of Cystic Fibrosis. 2021;20:57-63
57.Bashi N, Fatehi F, Fallah M, Walters D, Karunanithi M. Self-management education through mHealth: Review of strategies and structures. JMIR mHealth and uHealth. 2018;6(10):e10771
58.Chatterjee S, Davies MJ, Heller S, Speight J, Snoek FJ, Khunti K. Diabetes structured self-management education programmes: A narrative review and current innovations. The Lancet Diabetes & Endocrinology. 2018;6(2):130-142
59.Howell D, Harth T, Brown J, Bennett C, Boyko S. Self-management education interventions for patients with cancer: A systematic review. Supportive Care in Cancer. 2017;25:1323-1355
60.Jang I. A systematic review on mobile health applications’ education program for patients taking oral anticoagulants. International Journal of Environmental Research and Public Health. 2021;18(17):8902
61.Sarker MHR, Moriyama M, Rashid HU, Rahman MM, Chisti MJ, Das SK, et al. Chronic kidney disease awareness campaign and mobile health education to improve knowledge, quality of life, and motivation for a healthy lifestyle among patients with chronic kidney disease in Bangladesh: Randomized controlled trial. Journal of Medical Internet Research. 2022;24(8):e37314
62.Jakob R, Harperink S, Rudolf AM, Fleisch E, Haug S, Mair JL, et al. Factors influencing adherence to mHealth apps for prevention or management of noncommunicable diseases: Systematic review. Journal of Medical Internet Research. 2022;24(5):e35371
63.Meyerowitz-Katz G, Ravi S, Arnolda L, Feng X, Maberly G, Astell-Burt T. Rates of attrition and dropout in app-based interventions for chronic disease: Systematic review and meta-analysis. Journal of Medical Internet Research. 2020;22(9):e20283
64.Winter N, Russell L, Ugalde A, White V, Livingston P. Engagement strategies to improve adherence and retention in web-based mindfulness programs: Systematic review. Journal of Medical Internet Research. 2022;24(1):e30026
65.Shi N, Wong AK, Wong FK, Sha L. Mobile health application-based interventions to improve self-management of chemotherapy-related symptoms among people with breast cancer who are undergoing chemotherapy: A systematic review. The Oncologist. 2023;28(4):e175-ee82
66.Mollard E, Michaud K. Self-management of rheumatoid arthritis: Mobile applications. Current Rheumatology Reports. 2021;23:1-8
67.Druce KL, Dixon WG, McBeth J. Maximizing engagement in mobile health studies: Lessons learned and future directions. Rheumatic Disease Clinics. 2019;45(2):159-172
68.Kim Y, Lee HS. Quality, perceived usefulness, user satisfaction, and intention to use: An empirical study of ubiquitous personal robot service. Asian Social Science. 2014;10(11):1
69.Leung L, Chen C. E-health/m-health adoption and lifestyle improvements: Exploring the roles of technology readiness, the expectation-confirmation model, and health-related information activities. Telecommunications Policy. 2019;43(6):563-575
70.Wang J, Cao Y. Factors affecting users’ continuance intention toward Mobile health: Integration of theory of consumption value and expectation confirmation. Open Access Library Journal. 2023;10(3):1-15
71.Steinman L, Heang H, van Pelt M, Ide N, Cui H, Rao M, et al. Facilitators and barriers to chronic disease self-management and mobile health interventions for people living with diabetes and hypertension in Cambodia: Qualitative study. JMIR mHealth and uHealth. 2020;8(4):e13536
72.Park PH, Wambui CK, Atieno S, Egger JR, Misoi L, Nyabundi JS, et al. Improving diabetes management and cardiovascular risk factors through peer-led self-management support groups in Western Kenya. Diabetes Care. 2015;38(8):e110-e1e1
73.Azizoddin D, Adam R, Kessler D, Enzinger A, editors. Leveraging mobile health technology and multidisciplinary methodology to optimize self-management education for advanced cancer pain: development of stamp. The 54th Hawaii International Conference on System Sciences. 2021. Kauai, Hawaii, USA. USA: University of Hawaiʻi at Mnoa Hamilton Library; 2021
74.Qudah B, Luetsch K. The influence of mobile health applications on patient-healthcare provider relationships: A systematic, narrative review. Patient Education and Counseling. 2019;102(6):1080-1089
75.Cooke M, Richards J, Tjondronegoro D, Raj Chakraborty P, Jauncey-Cooke J, Andresen E, et al. myPainPal: Co-creation of a mHealth app for the management of chronic pain in young people. Informatics for Health and Social Care. 2021;46(3):291-305
76.Karhula M, Saukkonen S, Xiong E, Kinnunen A, Heiskanen T, Anttila H. ICF personal factors strengthen commitment to person-centered rehabilitation–A scoping review. Frontiers in Rehabilitation Sciences. 2021;2:1-11
Written By
Suad J. Ghaben and Arimi Fitri Mat Ludin
Submitted: 12 February 2024Reviewed: 20 February 2024Published: 09 April 2024