
Abstract
Over the past decades, the incidence rate of inflammatory bowel disease (IBD) has significantly risen all over the world. Most of the patients with IBD suffer from severe symptoms and complications. Being an autoimmune disease, recent research indicates that certain factors, such as environmental changes, disturbances in intestinal microbiota, abnormal immune responses, and genetic susceptibility, play a role in the pathogenesis of IBD. Nevertheless, the precise cause of IBD remains ambiguous. Therefore, there is no known cure for IBD. Moreover, traditional medications have troublesome side effects. For these reasons, some phytochemicals with more tolerance and less adverse effects capture the interest of medical scientists. Flavonoid, a natural anti-inflammatory compound, has recently been validated for its efficacy in IBD treatment. Among the extensive flavonoid family, comprising over 5000 members, quercetin has emerged as a promising drug candidate for treating IBD, supported by substantial preclinical evidence. Currently, quercetin participates in regulating IBD through several pathways, such as antioxidant properties, improvement of the intestinal barrier, modulation of the microbiota, immune response, and regulation of the enteroendocrine system in the gut. In brief, quercetin, a natural compound with anti-inflammatory activity, demonstrates a huge potential as a candidate drug for IBD treatment.
Keywords
- flavonoid
- quercetin
- phytochemical
- therapy
- inflammatory bowel disease
1. Introduction
Inflammatory bowel disease (IBD) encompasses Crohn’s disease (CD), ulcerative colitis (UC), as well as IBD unclassified (IBDU). IBD is a set of chronic or recurrent inflammatory conditions, mainly affecting the small and large intestine [1]. The most observed symptoms of IBD are abdominal pain, unexplained fever, fatigue, diarrhea, and loss of appetite, as well as weight loss [2]. UC manifests as persistent inflammation predominantly in the colon, whereas CD exhibits localized inflammation across the entire gastrointestinal tract. Furthermore, inflammation in UC is restricted to one layer, namely the colonic mucosa. Contrastingly, CD can affect two or multiple layers of the intestinal wall [3]. Presently, the global prevalence of IBD is on the rise. Projections suggest that the population afflicted with IBD in the Western world could surpass 10 million by 2030 [4]. In addition, the prevalence of IBD in Asia has significantly increased, leading to substantial economic burdens on individuals and societies [5]. To date, studies have shown that its pathogenesis is associated with environmental factors, immunity, microbiota, and genetics. However, the etiology of IBD is still a mystery [6]. Therefore, IBD is not possible to cure. At present, IBD treatment involves drug therapy and surgery. The medications have troublesome side effects with long-term use. In contrast, surgery does not cure CD, and the benefits are usually temporary [7].
Quercetin is a member of the flavonoid family, widely distributed in plants. Quercetin (≥99.5%) has been granted Generally Recognized As Safe (GRAS) status by the U.S. Food and Drug Administration (FDA) and is permitted for incorporation into established food additives in Japan and Korea. For the past few years, the medicinal significance of quercetin has increasingly garnered attention. Like other flavonoids, quercetin possesses antioxidant, anti-tumor, anti-diabetic, anti-hypertensive, and anti-depressant properties [8, 9]. Recent studies suggest that several pathways of quercetin participate in the regulation of IBD, comprising antioxidant properties, maintenance of the intestinal barrier, modulation of the microbiota, immune response, and regulation of the enteroendocrine system in the gut [10, 11]. However, these research findings are predominantly based on preclinical evidence. Therefore, the specific mechanisms need further investigation in the human body. In conclusion, the chapter is mainly aimed to illuminate the therapeutic potential of quercetin in IBD treatment.
2. The pathogenesis of IBD
Recent research suggests that the pathogenesis of IBD, as illustrated in Figure 1, is mainly associated with four factors, namely environmental factors, gut microbiota, and genetic susceptibility, as well as excess immunity [6]. Regarding environmental influences, it has been reported that a diet abundant in fruits and vegetables has a positive correlation with a reduced morbidity of Crohn’s disease [12]. Conversely, the consumption of fast food high in sugar and fat may trigger the initiation of IBD [13]. Additionally, factors such as smoking, medication, oxidative stress, and psychological stress may impact the development of IBD [14, 15, 16].
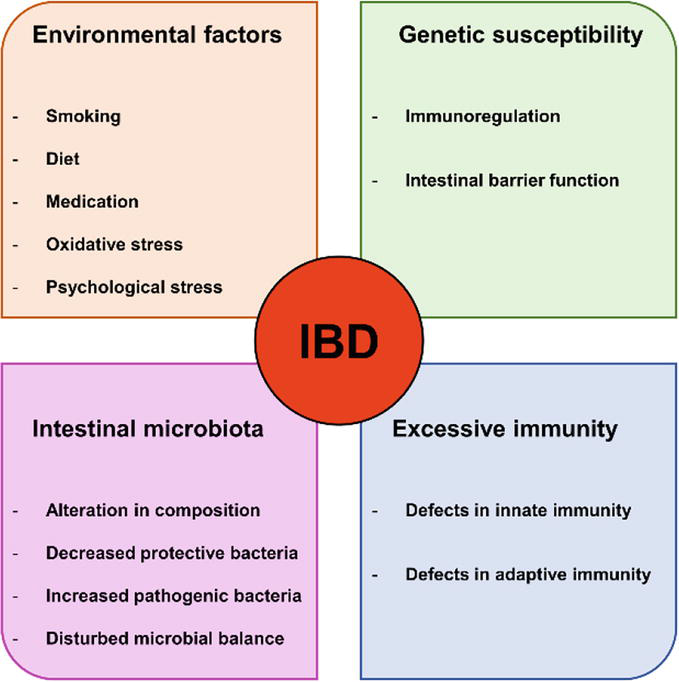
Figure 1.
Possible factors leading to IBD development.
Furthermore, several studies have demonstrated significant distinctions in the gut microbiota between individuals with IBD and healthy counterparts. The microbiota in IBD patients exhibits altered composition, reduced levels of protective bacteria, and increased presence of pathogenic bacteria, as well as disrupted microbial balance. These observed changes may play a role in the progression of IBD [17, 18, 19].
The intestinal immune system consists of both innate and adaptive immunity. Among them, innate immunity encompasses the protective barrier function of the intestinal mucosa, antibacterial proteins, gastric acid, and immune cells, as well as innate cytokines and molecules. In contrast, adaptive immunity (T and B cells) is pathogen-specific and is typically activated when the response of the innate immune system to a pathogen is ineffective [20]. Regulating the immune response to the intestinal microbiota is crucial for maintaining a delicate equilibrium between defensive inflammation and immune tolerance. Any disturbance to this equilibrium can lead to abnormal immunity, ultimately initiating the development of IBD [21].
Genetic susceptibility has also occurred in individuals with IBD [22]. Immune regulation and epithelial barrier function are crucial steps for keeping intestinal stability, as revealed by the investigation of genes and genetic loci associated with IBD. An impairment of the epithelial barrier can enable the invasion of microbes, subsequently recognized by the innate immune system. This recognition triggers various responses, including tolerogenic, inflammatory, and restorative responses. These responses are partly mediated by the secretion of extracellular mediators, attracting T or B cells [23]. Nonetheless, the exact pathogenesis of IBD is still uncertain so far [6].
3. Current diagnosis and treatment of IBD
3.1 Diagnosis procedure
Consistent or recrudescent bloody diarrhea, accompanied by abdominal pain and frequent defecation should raise suspicion of IBD, particularly in the case of young patients. To confirm a diagnosis of IBD, an array of tests and procedures is imperative for patients.
Laboratory tests of blood and stool typically serve as the initial diagnostic step. Biomarkers, comprising proteins identified in blood and stool, are integral components of these tests and play a crucial role in inflammation detection. Monitoring specific biomarker levels over time is valuable in optimizing therapeutic interventions and ensuring effective control of inflammation. C-reactive protein (CRP) and erythrocyte sedimentation rate (ESR) are blood biomarkers utilized to discern the presence of inflammation in the body. Concurrently, calprotectin and lactoferrin, both proteins found in stool, serve as fecal biomarkers indicative of gastrointestinal inflammation [24]. Moreover, the assessment of fecal calprotectin and lactoferrin proves valuable in monitoring the activity of IBD and predicting the probability of an impending clinical relapse [25].
To further validate an IBD diagnosis, the operation of endoscopy is necessary, which can facilitate the visual examination of the presence and localization of inflammation, as well as the assessment of its severity, and collect tissue samples via biopsies. Moreover, endoscopic procedures can monitor the therapeutic efficacy. Endoscopies used in IBD diagnosis encompass colonoscopy, upper GI endoscopy, sigmoidoscopy, pouchoscopy, and video capsule endoscopy [24].
Conventional endoscopy faces limitations in accessing approximately two-thirds of the small intestine except for capsule endoscopy. Based on it, various radiologic examinations and diagnostic imaging modalities are employed to assess these segments of the intestines, as well as to appraise the integrity of the bowel wall and adjacent areas external to the bowel. These imaging procedures encompass X-rays, barium contrast studies, computed tomography scanning (CT scan), and magnetic resonance imaging (MRI) [24].
3.2 Treatment
IBD is hardly possibly cured because its etiology remains elusive. Therefore, the main objective of treating IBD is to decrease inflammation level and alleviate the signs and symptoms experienced by patients. In best cases, this may lead not only to relieve symptoms but also to reduce risks of complications (tissue fibrosis, stenosis, fistulas, and colon cancer). Typically, the treatment of IBD includes both medication and surgical interventions.
IBD drug therapy primarily encompasses anti-inflammatory drugs, immune system suppressors, biologics, antibiotics, and other medications, as well as nutritional support. Anti-inflammatory drugs often constitute the initial approach in the treatment of IBD, particularly for cases characterized by mild to moderate severity. This category encompasses aminosalicylates (mesalamine, balsalazide, olsalazine) and corticosteroids. Immune system suppressors involve mercaptopurine, methotrexate, azathioprine, and some oral “small molecules” (tofacitinib, upadacitinib, and ozanimod). These drugs can inhibit the immune response, which discharges inflammation-inducing chemicals into the human body. Once released, these chemicals can cause the impairment of the digestive tract. Biologics are an emerging category of therapy, which are targeted at neutralizing proteins causing inflammation in the body. The current products on the market include infliximab, adalimumab, golimumab, certolizumab, vedolizumab, and ustekinumab, as well as risankizumab. Antibiotics may be utilized in conjunction with other medications when infection is a concern in cases of perianal Crohn’s disease. Beyond inflammation control, certain medications, such as anti-diarrheal medications and pain relievers, may alleviate the signs and symptoms of IBD. Additionally, under conditions of compromised nutrient absorption or severe weight loss, vitamins and nutritional supplements are indispensable.
Surgery is the last option when all conservative treatments cannot ameliorate the signs and symptoms of IBD, which involve changes in diet and lifestyle and drug therapy as well as alternative medicine. Notwithstanding, the side effects of surgery bring great inconvenience and burden to patients with UC. Moreover, surgery does not cure CD, and the benefits are usually temporary [7].
4. The association between the intake of dietary quercetin and IBD
As of now, there is no direct evidence supporting the mitigation of IBD through dietary quercetin consumption. However, flavonoid intake plays a positive role in alleviating IBD [26, 27]. Because quercetin belongs to the flavonoid family, the intake of dietary quercetin has been indirectly associated with the amelioration of IBD. Currently, several studies have focused on the impacts of flavonoid consumption on healthy individuals and IBD patients. For instance, Bai et al. reported that the mean total flavonoid intake by U.S. adults was 344.83 ± 9.13 mg/day [28]. Kölbel et al. investigated the correlation between the consumption of dietary flavonoids and the overall severity of IBD. They found that in the average Western diet, the total daily intake of flavonoids typically falls within the range of 200–1000 mg/day, but it decreases to 144 mg/day in individuals with IBD. In addition, a low dietary flavonoid intake has a positive correlation with severe IBD [27]. Furthermore, a randomized trial demonstrated that adhering to the Mediterranean diet, abundant in flavonoids, enhanced clinical scores and reduced inflammatory markers among children and adolescents with mild to moderate active IBD were observed [26].
5. Mechanisms of quercetin regulating IBD
Galsanov et al. reported the potential of quercitrin (a glycoside form of quercetin) as an agent to ameliorate intestinal inflammation in 1976 [29]. Following this discovery, other flavonoids have gradually been recognized for their anti-inflammatory properties in IBD. Notably, quercetin stands out as the first identified flavonoid capable of mitigating intestinal inflammation. Currently, several pathways of quercetin regulating IBD have been identified. As depicted in Figure 2, these include antioxidant activity, preservation of the epithelial barrier, the regulation of microbiota, and immune system in the gut, as well as the modulation of the enteroendocrine system (Figure 2).
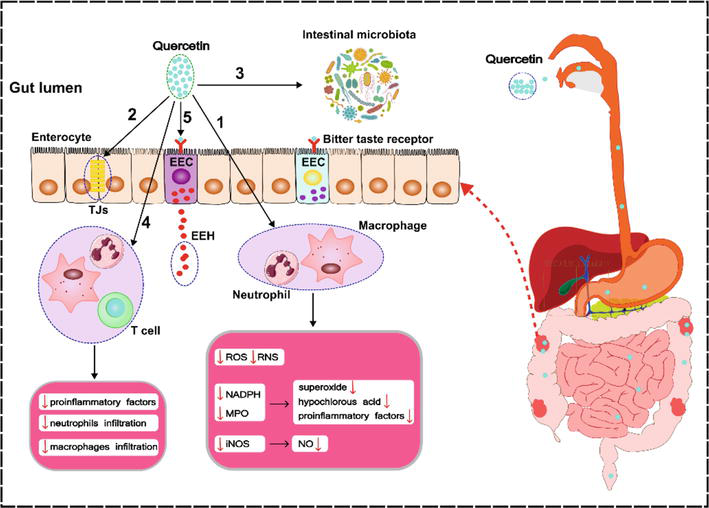
Figure 2.
Mechanisms of quercetin regulating IBD: (1) Antioxidant activity. (2) Preservation of the impaired epithelial barrier. (3) Shaping the intestinal microbiota. (4) Immunomodulatory function. (5) Modulation of the enteroendocrine system (RNS-reactive nitrogen species, ROS-reactive oxygen species, MPO-myeloperoxidase, NADPH-nicotinamide adenine dinucleotide phosphate, NO-nitric oxide, iNOS-inducible nitric oxide synthase, Tjs-tight junctions, EEH-enteroendocrine hormones, EEC-enteroendocrine cell).
5.1 Antioxidant property
Oxidative stress is recognized as a factor that exacerbate symptoms of IBD, such as diarrhea and abdominal pain. In addition, it contributes to the development of IBD [30]. In this process, reactive nitrogen species (RNS) and reactive oxygen species (ROS) have emerged as crucial contributors to the pathogenesis of IBD [31]. Recent research has revealed high levels of RNS and ROS in the inflamed intestine [32]. In IBD patients, excessive mononuclear cells and neutrophils aggregate in the inflamed intestinal tissue followed by increased myeloperoxidase (MPO) level and activated nicotinamide adenine dinucleotide phosphate (NADPH) oxidase system, resulting in the overproduction of superoxide and hypochlorous acid, which have direct cytotoxicity to the affected tissue [33]. Additionally, this pathway also generates a considerable number of pro-inflammatory factors [34]. Nonetheless, quercetin can significantly decrease MPO levels and inhibit ROS overproduction in colitis models, thereby blocking the following tissue damage [30, 35]. In normal physiological circumstances, a small amount of nitric oxide (NO) provides protection against inflammatory injury. On the contrary, in the inflammatory state, the overexpression of inducible nitric oxide synthase (iNOS) results in excessive NO production, causing an overproduction of peroxynitrites and followed by intestinal destruction under the action of superoxide anions [36]. Recent studies have shown that quercetin can curb the expression of iNOS, leading to a noticeable decrease in NO production [37, 38]. Therefore, quercetin can decrease the NO-induced enterotoxicity.
5.2 Preserving epithelial barrier
The epithelial barrier in the gut is an essential interface, dividing the external environment and the host tissue and playing a vital role in maintaining intestinal homeostasis [39]. While the loss of the epithelial barrier is a common event in the development of IBD, preserving the integrity of the intestinal epithelial barrier is a critical step in preventing the progression of IBD [40]. Studies have shown that quercetin may have a beneficial effect on the epithelial barrier [41]. For instance, Riemschneider et al. established murine colitis models induced by dextran sulfate sodium (DSS) and found that oral administration of quercetin restored the loss of epithelial integrity by the induction of tight junction proteins [42].
5.3 Shaping microbiota
The dysbiosis of gut microbiota is a vital participant in the development of IBD, characterized by diminished biodiversity, reduced stability, and an elevated presence of
5.4 Immunomodulatory function
IBD is closely associated with the aberrant response of the intestinal immune system, which contains the innate immune system comprising dendritic cells, macrophages, and neutrophils, as well as the adaptive immune system including T lymphocytes and B lymphocytes. Quercetin is able to diminish the infiltration of macrophages, neutrophils, and Th17 cells, concurrently promoting an increase in Treg cell proportions [42]. In the lipopolysaccharide (LPS)-stimulated macrophages, quercetin was found to inhibit the mRNA expression of key proinflammatory cytokines, namely tumor necrosis factor-alpha (TNF-α), interleukin-1 beta (IL-1β), and interleukin-6 (IL-6), primarily by interfering with the mitogen-activated protein kinase (MAPK) and nuclear factor-κB (NF-κB) pathways [46]. Lin et al. further elucidated the anti-inflammatory properties of quercetin, revealing its ability to suppress the production of IL-17, TNF-α, and IL-6 (proinflammatory cytokines) while simultaneously boosting the release of IL-10 (anti-inflammatory cytokine) in colon tissues [45]. Specifically, quercetin suppresses TNF-α and IL-6 production by modulating the miR-369-3p/C/EBP-β axis in dendritic cells, thereby showing its anti-inflammatory properties [47]. This consistent effect is also observed in intestinal epithelial cells, wherein the restraint on C/EBP-β signaling by quercetin explains its protective activity against IL-6 production induced by the heat shock response in the intestinal mucosa [48].
5.5 The modulation of the enteroendocrine system
Currently, there is a lack of evidence supporting the enteroendocrine regulation of quercetin in IBD. However, flavonoids have potential protective effects against IBD through the enteroendocrine pathway [11]. Accordingly, we conclude that quercetin may also protect against IBD via enteroendocrine regulation.
The mechanisms of flavonoids regulating the enteroendocrine system are as follows: flavonoids can stimulate the secretion of cholecystokinin (CCK), ghrelin, glucagon-like peptide (GLP-1), and glucagon-like peptide (GLP-2) [49, 50, 51, 52]. GLP-1/2; exhibit considerable potential in treating IBD due to their ability to promote the restoration of the impaired epithelial barrier; regulate T lymphocyte differentiation and function; and modulate innate immune cells, such as macrophages and dendritic cells [53, 54, 55, 56]. Ghrelin has also been shown to mitigate intestinal inflammation in colitis mice [57]. In addition, CCK has demonstrated anti-inflammatory effects [58]. For these reasons, it can be inferred that flavonoids exhibit therapeutic effects on IBD through the enteroendocrine approach.
6. Clinical application of quercetin in IBD
Bioavailability is defined as “the speed and degree to which the active component of a drug is absorbed and become accessible at the site of action”, which are crucial factors affecting the efficacy of bioactive compounds in organisms. Similar to other flavonoids, quercetin demonstrates low bioavailability, thereby contributing to reduced efficacy in vivo [59]. Accordingly, the clinical application of quercetin in IBD is unsatisfactory. It has been reported that the bioavailability can be affected by several factors, including glycosylation, molecular weight, and metabolic conversion, as well as interaction with colonic microbiota [60]. Instability, poor absorption and solubility, rapid metabolism, and systemic elimination may result from the above confounding factors, which cause low bioavailability of quercetin and other flavonoids. Consequently, their delivery efficiency and therapeutic efficacy in vivo are significantly decreased.
To enhance the in vivo bioavailability of quercetin, researchers have directed their attention toward optimizing various metabolic processes associated with bioavailability, such as augmenting intestinal absorption [61], improving metabolic stability [62], and modifying the site of absorption [63], among others. In recent years, nano-delivery systems have been utilized for quercetin to accomplish the above objective [64, 65]. For instance, Wang et al. formulated novel quercetin-loaded nanoparticles (NPs) using sodium alginate and N-succinyl chitosan. Their findings indicate that these NPs show enhanced therapeutic efficacy in alleviating DSS-induced colitis in mice, compared with free quercetin [66]. In addition, Jing et al. developed a colon-targeted quercetin delivery system, of which the pectin/Ca2+ microspheres were prepared and then crosslinked with oligochitosan. The therapeutic outcomes observed in vivo study indicated that these quercetin microspheres could alleviate symptoms of colitis and preserve both the colon length and the intestinal barrier integrity [67].
7. Conclusions
Quercetin is a common flavonol belonging to the flavonoid family. The current preclinical studies show that quercetin has the potential to protect against IBD. The underlying mechanisms include antioxidant activity, improving the intestinal epithelial barrier, modulating the intestinal microbiota, immunomodulatory function, and regulating the enteroendocrine system. Unfortunately, the clinical application of quercetin in IBD is unsatisfactory due to its low bioavailability. In the future, the design of novel material will contribute to improving the bioavailability of quercetin, thereby promoting its therapeutical effect on IBD.
Author contributions
Mingrui Li drafted, edited and visualized this chapter. Yun Gao supervised and revised the chapter.
References
- 1.
Nakase H, Uchino M, Shinzaki S, Matsuura M, Matsuoka K, Kobayashi T, et al. Evidence-based clinical practice guidelines for inflammatory bowel disease 2020. Journal of Gastroenterology. 2021; 56 (6):489-526 - 2.
Hendrickson BA, Gokhale R, Cho JH. Clinical aspects and pathophysiology of inflammatory bowel disease. Clinical Microbiology Reviews. 2002; 15 (1):79-94 - 3.
Bouma G, Strober W. The immunological and genetic basis of inflammatory bowel disease. Nature Reviews. Immunology. 2003; 3 (7):521-533 - 4.
Kaplan GG, Windsor JW. The four epidemiological stages in the global evolution of inflammatory bowel disease. Nature Reviews. Gastroenterology & Hepatology. 2021; 18 (1):56-66 - 5.
Banerjee R, Pal P, Mak JWY, Ng SC. Challenges in the diagnosis and management of inflammatory bowel disease in resource-limited settings in Asia. The Lancet Gastroenterology & Hepatology. 2020; 5 (12):1076-1088 - 6.
Guan Q. A comprehensive review and update on the pathogenesis of inflammatory bowel disease. Journal of Immunology Research. 2019; 2019 :7247238 - 7.
(IBD) Ibd: Mayo Clinic 2022. Available online: https://wwwmayoclinicorg/diseases-conditions/inflammatory-bowel-disease/diagnosis-treatment/drc-20353320 [Accessed: December 1, 2023] - 8.
Dodda D, Chhajed R, Mishra J. Protective effect of quercetin against acetic acid induced inflammatory bowel disease (IBD) like symptoms in rats: Possible morphological and biochemical alterations. Pharmacological Reports. 2014; 66 (1):169-173 - 9.
Dodda D, Chhajed R, Mishra J, Padhy M. Targeting oxidative stress attenuates trinitrobenzene sulphonic acid induced inflammatory bowel disease like symptoms in rats: Role of quercetin. Indian Journal Of Pharmacology. 2014; 46 (3):286-291 - 10.
Hu S, Zhao M, Li W, Wei P, Liu Q , Chen S, et al. Preclinical evidence for quercetin against inflammatory bowel disease: A meta-analysis and systematic review. Inflammopharmacology. 2022; 30 (6):2035-2050 - 11.
Li M, Weigmann B. A novel pathway of flavonoids protecting against inflammatory bowel disease: Modulating enteroendocrine system. Metabolites. 2022; 12 (1):31-48 - 12.
Dolan KT, Chang EB. Diet, gut microbes, and the pathogenesis of inflammatory bowel diseases. Molecular Nutrition & Food Research. 2017; 61 (1):10-29 - 13.
Hibi T, Ogata H. Novel pathophysiological concepts of inflammatory bowel disease. Journal of Gastroenterology. 2006; 41 (1):10-16 - 14.
Ardizzone S, Bianchi Porro G. Biologic therapy for inflammatory bowel disease. Drugs. 2005; 65 (16):2253-2286 - 15.
Ho SM, Lewis JD, Mayer EA, Plevy SE, Chuang E, Rappaport SM, et al. Challenges in IBD research: Environmental triggers. Inflammatory Bowel Diseases. 2019; 25 (Suppl. 2):S13-S23 - 16.
Lakatos PL. Environmental factors affecting inflammatory bowel disease: Have we made progress? Digestive Diseases. 2009; 27 (3):215-225 - 17.
Glassner KL, Abraham BP, Quigley EMM. The microbiome and inflammatory bowel disease. The Journal of Allergy and Clinical Immunology. 2020; 145 (1):16-27 - 18.
Nishida A, Inoue R, Inatomi O, Bamba S, Naito Y, Andoh A. Gut microbiota in the pathogenesis of inflammatory bowel disease. Clinical Journal of Gastroenterology. 2018; 11 (1):1-10 - 19.
Richard ML, Sokol H. The gut mycobiota: Insights into analysis, environmental interactions and role in gastrointestinal diseases. Nature Reviews. Gastroenterology & Hepatology. 2019; 16 (6):331-345 - 20.
Ince MN, Elliott DE. Immunologic and molecular mechanisms in inflammatory bowel disease. The Surgical Clinics of North America. 2007; 87 (3):681-696 - 21.
Abraham C, Cho JH. Inflammatory bowel disease. The New England Journal of Medicine. 2009; 361 (21):2066-2078 - 22.
Annese V. Genetics and epigenetics of IBD. Pharmacological Research. 2020; 159 :104892 - 23.
Khor B, Gardet A, Xavier RJ. Genetics and pathogenesis of inflammatory bowel disease. Nature. 2011; 474 (7351):307-317 - 24.
Crohn’s & Colitis Foundation. Available online: https://wwwcrohnscolitisfoundationorg/what-is-ibd/diagnosing-ibd [Accessed: December 15, 2023] - 25.
Grifka J, Schiegl Geb Gotz J, Fenk-Mayer A, Benditz A. Injection treatment for cervical and lumbar syndromes: Special infiltration techniques. Orthopadie (Heidelb). 2023; 46 (1):195-208 - 26.
El Amrousy D, Elashry H, Salamah A, Maher S, Abd-Elsalam SM, Hasan S. Adherence to the Mediterranean diet improved clinical scores and inflammatory markers in children with active inflammatory bowel disease: A randomized trial. Journal of Inflammation Research. 2022; 15 :2075-2086 - 27.
Kölbel B, Hamacher S, Hellmich M, Kruis W. Low dietary flavonoid consumption is associated to severe inflammatory bowel disease. Gastro Hep Advances. 2024; 3 (1):31-37 - 28.
Bai W, Wang C, Ren C. Intakes of total and individual flavonoids by US adults. International Journal of Food Sciences and Nutrition. 2014; 65 (1):9-20 - 29.
Galsanov Sh B, Tourova AD, Klimenko ED. Effect of quercitrin on structural changes in the large and small intestines in experimental enterocolitis. Biulleten’ Eksperimental’noĭ Biologii i Meditsiny. 1976; 81 (5):623-625 - 30.
Dong Y, Hou Q , Lei J, Wolf PG, Ayansola H, Zhang B. Quercetin alleviates intestinal oxidative damage induced by H(2)O(2) via modulation of GSH: In vitro screening and In vivo evaluation in a colitis model of mice. ACS Omega. 2020; 5 (14):8334-8346 - 31.
Rezaie A, Parker RD, Abdollahi M. Oxidative stress and pathogenesis of inflammatory bowel disease: An epiphenomenon or the cause? Digestive Diseases and Sciences. 2007; 52 (9):2015-2021 - 32.
Piechota-Polanczyk A, Fichna J. Review article: The role of oxidative stress in pathogenesis and treatment of inflammatory bowel diseases. Naunyn-Schmiedeberg’s Archives of Pharmacology. 2014; 387 (7):605-620 - 33.
Alzoghaibi MA. Concepts of oxidative stress and antioxidant defense in Crohn’s disease. World Journal of Gastroenterology. 2013; 19 (39):6540-6547 - 34.
Pavlick KP, Laroux FS, Fuseler J, Wolf RE, Gray L, Hoffman J, et al. Role of reactive metabolites of oxygen and nitrogen in inflammatory bowel disease. Free Radical Biology & Medicine. 2002; 33 (3):311-322 - 35.
Hong Z, Piao M. Effect of quercetin monoglycosides on oxidative stress and gut microbiota diversity in mice with dextran sodium Sulphate-induced colitis. BioMed Research International. 2018; 2018 :8343052 - 36.
Veljaca M, Lesch CA, Pllana R, Sanchez B, Chan K, Guglietta A. BPC-15 reduces trinitrobenzene sulfonic acid-induced colonic damage in rats. The Journal of Pharmacology and Experimental Therapeutics. 1995; 272 (1):417-422 - 37.
Khater SI, Lotfy MM, Alandiyjany MN, Alqahtani LS, Zaglool AW, Althobaiti F, et al. Therapeutic potential of quercetin loaded nanoparticles: novel insights in alleviating colitis in an experimental DSS induced colitis model. Biomedicine. 2022; 10 (7):1654-1677 - 38.
Romero M, Vera B, Galisteo M, Toral M, Galvez J, Perez-Vizcaino F, et al. Protective vascular effects of quercitrin in acute TNBS-colitis in rats: The role of nitric oxide. Food & Function. 2017; 8 (8):2702-2711 - 39.
Turner JR. Intestinal mucosal barrier function in health and disease. Nature Reviews. Immunology. 2009; 9 (11):799-809 - 40.
Sommer K, Wiendl M, Muller TM, Heidbreder K, Voskens C, Neurath MF, et al. Intestinal mucosal wound healing and barrier integrity in IBD-crosstalk and trafficking of cellular players. Frontiers in Medicine (Lausanne). 2021; 8 :643973 - 41.
Suzuki T, Hara H. Role of flavonoids in intestinal tight junction regulation. The Journal of Nutritional Biochemistry. 2011; 22 (5):401-408 - 42.
Riemschneider S, Hoffmann M, Slanina U, Weber K, Hauschildt S, Lehmann J. Indol-3-carbinol and quercetin ameliorate chronic DSS-induced colitis in C57BL/6 mice by AhR-mediated anti-inflammatory mechanisms. International Journal of Environmental Research and Public Health. 2021; 18 (5):2262-2278 - 43.
Nishino K, Nishida A, Inoue R, Kawada Y, Ohno M, Sakai S, et al. Analysis of endoscopic brush samples identified mucosa-associated dysbiosis in inflammatory bowel disease. Journal of Gastroenterology. 2018; 53 (1):95-106 - 44.
Sultan S, El-Mowafy M, Elgaml A, Ahmed TAE, Hassan H, Mottawea W. Metabolic influences of gut microbiota dysbiosis on inflammatory bowel disease. Frontiers in Physiology. 2021; 12 :715506 - 45.
Lin R, Piao M, Song Y. Dietary quercetin increases colonic microbial diversity and attenuates colitis severity in Citrobacter rodentium-infected mice. Frontiers in Microbiology. 2019; 10 :1092 - 46.
Cho SY, Park SJ, Kwon MJ, Jeong TS, Bok SH, Choi WY, et al. Quercetin suppresses proinflammatory cytokines production through MAP kinases andNF-kappaB pathway in lipopolysaccharide-stimulated macrophage. Molecular and Cellular Biochemistry. 2003; 243 (1-2):153-160 - 47.
Galleggiante V, De Santis S, Liso M, Verna G, Sommella E, Mastronardi M, et al. Quercetin-induced miR-369-3p suppresses chronic inflammatory response targeting C/EBP-beta. Molecular Nutrition & Food Research. 2019; 63 (19):e1801390 - 48.
Hungness ES, Robb BW, Luo GJ, Pritts TA, Hershko DD, Hasselgren PO. Proteasome inhibitors activate the transcription factors C/EBP-beta and delta in human intestinal epithelial cells. Biochemical and Biophysical Research Communications. 2002; 290 (1):469-474 - 49.
Al Shukor N, Ravallec R, Van Camp J, Raes K, Smagghe G. Flavonoids stimulate cholecystokinin peptide secretion from the enteroendocrine STC-1 cells. Fitoterapia. 2016; 113 :128-131 - 50.
Gonzalez-Abuin N, Martinez-Micaelo N, Margalef M, Blay M, Arola-Arnal A, Muguerza B, et al. A grape seed extract increases active glucagon-like peptide-1 levels after an oral glucose load in rats. Food & Function. 2014; 5 (9):2357-2364 - 51.
Grau-Bove C, Gonzalez-Quilen C, Terra X, Blay MT, Beltran-Debon R, Jorba-Martin R, et al. Effects of flavanols on enteroendocrine secretion. Biomolecules. 2020; 10 (6):844-856 - 52.
Kato M, Tani T, Terahara N, Tsuda T. The anthocyanin Delphinidin 3-Rutinoside stimulates glucagon-like Peptide-1 secretion in murine GLUTag cell line via the Ca2+/calmodulin-dependent kinase II pathway. PLoS One. 2015; 10 (5):e0126157 - 53.
Anbazhagan AN, Thaqi M, Priyamvada S, Jayawardena D, Kumar A, Gujral T, et al. GLP-1 nanomedicine alleviates gut inflammation. Nanomedicine. 2017; 13 (2):659-665 - 54.
Bang-Berthelsen CH, Holm TL, Pyke C, Simonsen L, Sokilde R, Pociot F, et al. GLP-1 induces barrier protective expression in Brunner’s glands and regulates colonic inflammation. Inflammatory Bowel Diseases. 2016; 22 (9):2078-2097 - 55.
Buchman AL, Katz S, Fang JC, Bernstein CN, Abou-Assi SG, Teduglutide Study G. Teduglutide, a novel mucosally active analog of glucagon-like peptide-2 (GLP-2) for the treatment of moderate to severe Crohn’s disease. Inflammatory Bowel Diseases. 2010; 16 (6):962-973 - 56.
Qi KK, Lv JJ, Wu J, Xu ZW. Therapeutic effects of different doses of polyethylene glycosylated porcine glucagon-like peptide-2 on ulcerative colitis in male rats. BMC Gastroenterology. 2017; 17 (1):34 - 57.
Gonzalez-Rey E, Chorny A, Delgado M. Therapeutic action of ghrelin in a mouse model of colitis. Gastroenterology. 2006; 130 (6):1707-1720 - 58.
Saia RS, Ribeiro AB, Giusti H. Cholecystokinin modulates the mucosal inflammatory response and prevents the lipopolysaccharide-induced intestinal epithelial barrier dysfunction. Shock. 2020; 53 (2):242-251 - 59.
Enayat S, Seyma Ceyhan M, Taskoparan B, Stefek M, Banerjee S. CHNQ , a novel 2-Chloro-1,4-naphthoquinone derivative of quercetin, induces oxidative stress and autophagy both in vitro and in vivo. Archives of Biochemistry and Biophysics. 2016; 596 :84-98 - 60.
Thilakarathna SH, Rupasinghe HP. Flavonoid bioavailability and attempts for bioavailability enhancement. Nutrients. 2013; 5 (9):3367-3387 - 61.
Shen Q , Li X, Li W, Zhao X. Enhanced intestinal absorption of daidzein by borneol/menthol eutectic mixture and microemulsion. AAPS PharmSciTech. 2011; 12 (4):1044-1049 - 62.
Walle T. Methylation of dietary flavones greatly improves their hepatic metabolic stability and intestinal absorption. Molecular Pharmaceutics. 2007; 4 (6):826-832 - 63.
Nielsen IL, Chee WS, Poulsen L, Offord-Cavin E, Rasmussen SE, Frederiksen H, et al. Bioavailability is improved by enzymatic modification of the citrus flavonoid hesperidin in humans: A randomized, double-blind, crossover trial. The Journal of Nutrition. 2006; 136 (2):404-408 - 64.
Blanco E, Shen H, Ferrari M. Principles of nanoparticle design for overcoming biological barriers to drug delivery. Nature Biotechnology. 2015; 33 (9):941-951 - 65.
Kou L, Bhutia YD, Yao Q , He Z, Sun J, Ganapathy V. Transporter-guided delivery of nanoparticles to improve drug permeation across cellular barriers and drug exposure to selective cell types. Frontiers in Pharmacology. 2018; 9 :27 - 66.
Wang L, Fu R, Meng Y, Liang J, Xue W, Hu H, et al. pH sensitive quercetin nanoparticles ameliorate DSS-induced colitis in mice by colon-specific delivery. Molecular Nutrition & Food Research. 2023; 11 (7):e2300051 - 67.
Jing S, Chen H, Liu E, Zhang M, Zeng F, Shen H, et al. Oral pectin/oligochitosan microspheres for colon-specific controlled release of quercetin to treat inflammatory bowel disease. Carbohydrate Polymers. 2023; 316 :121025