Open Access is an initiative that aims to make scientific research freely available to all. To date our community has made over 100 million downloads. It’s based on principles of collaboration, unobstructed discovery, and, most importantly, scientific progression. As PhD students, we found it difficult to access the research we needed, so we decided to create a new Open Access publisher that levels the playing field for scientists across the world. How? By making research easy to access, and puts the academic needs of the researchers before the business interests of publishers.
We are a community of more than 103,000 authors and editors from 3,291 institutions spanning 160 countries, including Nobel Prize winners and some of the world’s most-cited researchers. Publishing on IntechOpen allows authors to earn citations and find new collaborators, meaning more people see your work not only from your own field of study, but from other related fields too.
Adult tapeworms, known as cestodes, reside in the small intestine where they feed off the host’s food. They are attached to the intestinal wall by a structure called the scolex, which is connected to a chain of segments known as proglottids that make up the strobila. Each proglottid contains both male and female reproductive systems and are categorized as immature, mature, or gravid based on their stage of development. Gravid proglottids are found at the end of the strobila and contain a fully developed uterus filled with eggs, which is often used for identification purposes. The eggs and the scolex can also be used to identify the specific species of the tapeworm. Cestodes have complex life cycles that involve intermediate and definitive hosts. In some cases, humans can be the definitive hosts with adult worms living in the intestine (Diphyllobothrium latum, Taenia saginata, Hymenolepis diminuta, and Dipylidium caninum), while in other cases humans can serve as both the definitive and intermediate hosts (T. solium and H. nana). Tapeworms have been documented as far back as 1500 BC and are among the oldest known human parasites. The prevalence of human intestinal tapeworms is not well understood, but it is estimated that millions of people are infected with various species of tapeworms. While the presence of adult tapeworms in the intestine is not typically life threatening, infection with larval tapeworms can be serious and potentially fatal.
*Address all correspondence to: samedeeq@yahoo.com
1. Introduction
Tapeworms are flatworms that live in the intestinal tracts of their hosts. Beyond depriving their hosts of certain micronutrients, like vitamins, adult tapeworms do little harm to their hosts. The size of adult tapeworms ranges from 0.04 inches to 50 feet long, and they are visible to the unaided eye. Cestodiasis is the name for a tapeworm infection. Tapeworms are flatworms that live in the digestive tracts of their hosts. They are classified into two orders: Pseudophyllidea and Cyclophyllidea. The heads (scolex), neck, and proglottids (strobila) are the three components that make up an adult worm. Succkers or grooves, depending on the order, can be found on the scolex, the organ that attaches to the intestinal mucosa. New proglottids form in the growth region of the neck. The proglottids are divided into three segments: premature, adult, and gravid, with the gravid segment containing eggs in the uterus. Tapeworms possess both male and female reproductive systems in every segment, making them hermaphrodites. They lack bodily cavities or alimentary canals, through which nutrients are absorbed by their outer layer. The two orders of tapeworms, Cyclophyllidea and Pseudophyllidea, differ in terms of their eggs. Cyclophyllidea eggs contain hexacanth embryos equipped with hooklets, while Pseudophyllidea eggs have operculums (Table 1) [1].
Characteristic
Diphyllobothrium latum
Taenia saginata
Taenia saginata asiatica
Taenia solium
Hymenolepis nana
Hymenolepis diminuta
Dipylidium caninum
Common intermediate hosts
Fish and copepods
Cattle
Pig
Pig
1: different arthropods (fleas, beetles); or none
2: Different arthropods (beetles, fleas)
1: different arthropods (fleas, dog, lice)
Source of infection
consuming plerocercoid (sparganum) from fish that has been infected
Consumption of beef contaminated with cysticercus
consumption of infected tissue, mainly liver with cysticercus
Cysticercus consumption in contaminated pork
Consumption of an egg directly or consuming a cysticercoid within an infected arthropod; autoinfection is also a possibility.
Consumption of cysticercoid in an infected arthropod
Consumption of cysticercoid within fleas, lice
The prepatent phase
3 to 5 weeks
10 to 12 weeks
10 to 12 weeks
5 to 12 weeks
2 to 3 weeks
About 3 weeks
3 to 4 weeks
The average life span
A maximum of 25 years
A maximum of 25 years
A maximum of 25 years
A maximum of 25 years
Due to autoinfection, possibly for a number of years
Usually less than a year
Usually less than a year
Size
4 to 10 meters
4 to 12 meters
4 to 8 meters
1.5–8 meters
2.5 to 4 cm
20 to 60 cm
10 to 70 cm
Scolex
With two shallow grooves (bothria) and a spatulate, 3 × 1 mm shape, it lacks rostellum and hooklets.
Four suckers, quadrate, 1–2 mm in diameter, without rostellum or hooklets
Four suckers, quadrate, 1–2 mm in diameter, without rostellum or hooklets
Four suckers, rostellum, hooklets, and a quadrate with a diameter of 1 mm.
Has four suckers, rostellum, and hooklets; knoblike but rarely seen
Has four suckers; rostellum but no hooklets; knoblike but rarely found
0.2–0.5 mm in diameter, with four suckers and a conical, retractile rostellum equipped with four to seven rows of tiny hooklets.
D. latum is a member of the group of tapeworms known as pseudophyllideans. One distinguishing feature of this group is the presence of two bothria, or sucking organs, on the scolex [1]. This is in contrast to the Taenia tapeworms, which have a scolex with four suckers. The common name for D. latum is fish tapeworm or broad tapeworm (Table 1) [2].
2.1 Distribution
This disease is prevalent worldwide.
2.2 Predilection site
In the human small intestine, the ileum is where the adult worm is normally found.
2.3 Morphology
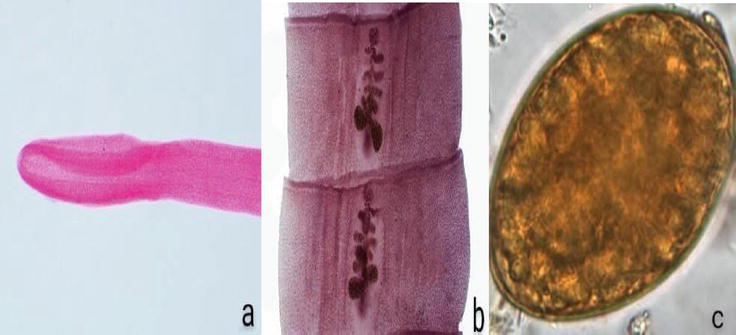
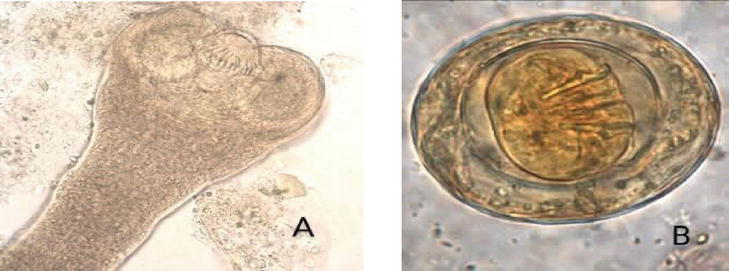
Adults can reach a length of 10 m or more and have up to 3000 proglottids inside of them [3]. This is the biggest tapeworm that lives in the human small intestine. The spoon-shaped, elongated scolex of D. latum measures approximately 2–3 mm in length and 1 mm in width. It features two long sucking grooves (Figure 1a), one on the ventral surface (bothria) and the other on the dorsal surface. The neck lacks segmentation and is thin. Strobila is made up of approximately 3000–4000 proglottids [3]. The width of a plottid is greater than its length (Figure 1b). Midventrally, the genital pores open. The egg has a thick, light brown shell and is roughly ovoid, measuring 65 by 45 μm (Figure 1c). At one end, it has an operculum. It grows fully in freshwater and is excreted in feces [5]. Humans are not infected by the egg [2].
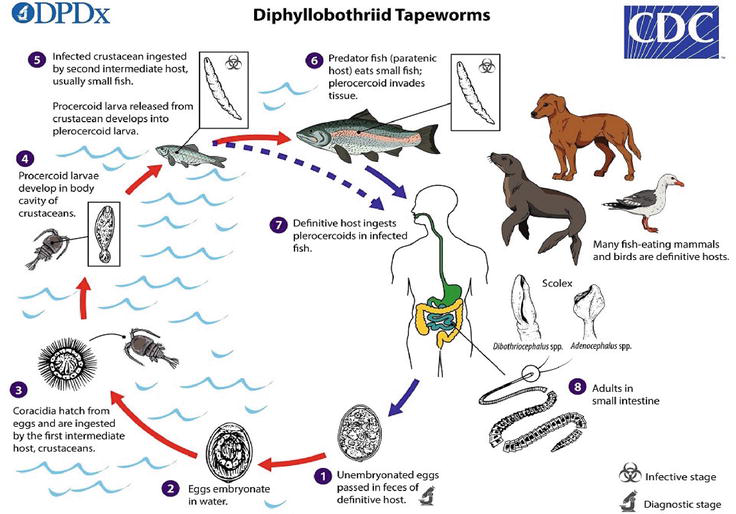
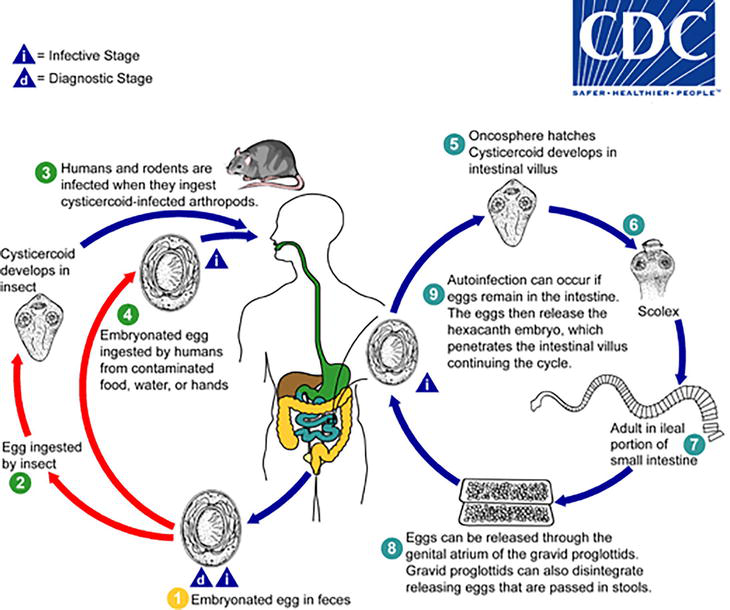
(1) Infected humans excrete feces that contain immature eggs. Secondly, eggs develop in water. (3) Crustaceans consume the coracidia after they hatch from their eggs. (4) The body cavity of crustaceans is where procercoid larvae develop. (5) Procercoid larvae become plerocercoid larvae after being eaten by small freshwater fish that have come into contact with the contaminated crustaceans. (6) Small infected fish are eaten by predator fish. (7) Humans become infected when they consume raw or undercooked fish that is contaminated with pleurocercoid larvae. In the small intestine, adults develop. (9) Immature eggs released by proglottids are excreted in the feces. In the body cavity of crustaceans, procercoid larvae develop. (5) When an intermediate host, such as fish, reptiles, or amphibians, consumes infected crustaceans, the procercoid larvae transform into plerocercoid larvae. (6) Predators, including dogs and cats, consume the infected second intermediate host. (7) The small intestines of dogs and cats are where plerocercoid larvae mature into adults. Of procercoid larvae in crustaceans or plerocercoid larvae in second intermediate hosts, or the application of raw poultices made of second intermediate hosts containing plerocercoid larvae for medicinal purposes on open wounds, lesions, or the eyes, can result in infection in humans (Figure 2) [4].
Figure 2.
Life cycle of Diphyllobothrium latum [4].
2.5 Pathogenesis and clinical symptoms
In the human gut, the second intermediate host—amphibians, reptiles, and fish—releases the sparganum, or plerocercoid larvae. Infected water can also infect humans if they consume cyclops that contain procercoid larvae. The larvae of procercoid will mature into plerocercoid larvae, which will migrate to other organs and subcutaneous tissue after penetrating the intestinal wall. Early migration phases do not cause any symptoms. As it reaches its destination, it starts to spread and inflame the tissues around it, causing pain. No encyst occurs in the larvae. The organs or tissues that are affected by sparganosis determine its clinical features, which can include subcutaneous nodules, periorbital edema, seizures, parasthesias, and hemiparesis in the central nervous system [6]. While Intestinal obstruction is a possible presentation in some patients, infections can also be asymptomatic [2]. The typical symptoms include anemia, weakness, diarrhea, nausea, and abdominal pain [7, 8]. The worms reside in the ileum, which is also the site of vitamin B12 absorption. It can cause anemia by competing with the host for vitamin B12 [3].
2.6 Diagnosis
2.6.1 Microscopical examination
Typically, the diagnosis is made after the proglottids, or characteristic eggs, have been recovered and identified [3]. The operculum should be visible after closely examining the eggs. Tapping on the wet preparation’s coverslip can cause it to pop open if it is difficult to see. To make the operculum easier to see, the light should be turned down a little. Proglottids are frequently passed in chains that range in length from a few inches to several feet. Furthermore, the uterine structure is visible in the center of the gravid proglotids, which are significantly wider than long (rosette).
There is no risk of cysticercosis from handling the specimens, but all fecal specimens should be handled carefully as they may contain other organisms that could be infectious.
2.7 Treatment
Oral praziquantel (5–10 mg/kg in one dose) [10]. Anemia caused by a vitamin B12 deficiency should be treated with parenteral vitamin B12 [3].
Beef tapeworm (Taenia saginata) and pork tapeworm (Taenia solium) are common intestinal parasites [1].
3.1 Distribution
Worldwide distribution is observed for Taenia saginata and Taenia solium [11].
3.2 Predilection site
Both Taenia saginata and Taenia solium adult worms reside in the human small intestine.
3.3 Morphology
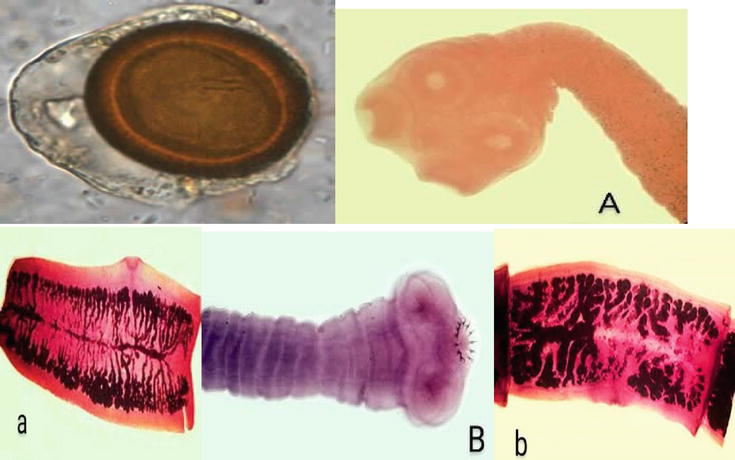
The adult Taenia saginata is segmented and flattened dorsoventrally, with a length of 5–10 m. With four suckers for attachment, T. saginata’s scolex has a diameter of approximately 1–2 mm. There are no hooklets or rostellum on the scolex (Figure 3A). The shape of the neck is long and narrow. There are 1000–2000 proglottids in each strobila. They have the characteristics of a hermaphrodite. The lateral branches of each gravid segment range from 15 to 30, and each gravid segment is roughly 20 mm in length and 5 mm in width (Figure 3a). The segments of gravid material separate and exit separately through the anus of the host. It is possible to see the gravid segment moving actively. Both T. solium and T. saginata have identical eggs. They have a diameter of 31–43 μm, are brown, and are spherical. As shown in Figure 3, the shell has striating radially. Six hooklets are present in the embryo (oncosphere). The larva of Taenia saginata is called Cysticercus bovis. The stage at which humans are infected is the larva. It is a single perforated scolex (bladder worm) inside a milky-white, ovoid, fluid-filled, opalescent vesicle that measures approximately 5 by 10 mm in diameter. Infected cattle’s muscles contain cysticerci. In the contaminated beef (measly beef), they are obscenely visible as white dots. At 2–3 meters in length, the mature T. solium is segmented and flattened dorsoventrally. T. solium has four suckers on its scolex, which has a diameter of approximately 1 mm. A rostellum and hooklets are present on the scolex (Figure 3B). It has a short neck. Less than 1000 proglottids make up the strobila. Each gravid segment has seven to thirteen lateral uterine branches, and they are roughly 12 mm long and 6 mm broad (Figure 3b). They possess hermaphrodite properties. Through the host’s anus, the gravid segments are released in chains. The human-infecting form of T. solium is known as Cysticercus cellulosae, which is also its larval form. Both in humans and in pigs, it can develop in different organs. It resembles Cysticercus bovis in morphology. The adult scolex of Taenia solium and the invaginated scolex of Cysticercus cellulosae share a similar morphology [1].
Figure 3.
Taenia sp. egg. (A) Scolex of T. saginata. Note the four large suckers and lack of rostellum and rostellar hooks. (a) Mature proglottid of T. saginata. (B) Scolex of T. solium. Note the four large suckers and rostellum containing two rows of hooks. (b) Mature proglottid of T. solium [12].
3.4 Life cycle
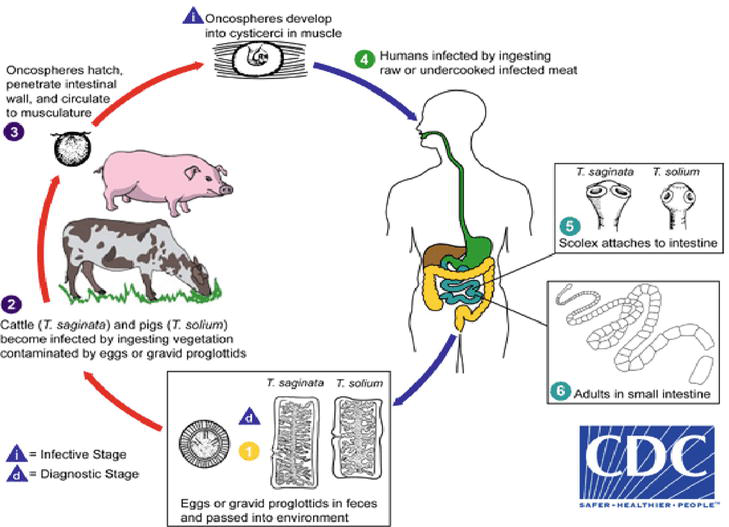
The life cycle is depicted in Figure 4 (1). Infected humans excrete eggs or gravid proglottids. (2) Ingestion of vegetation contaminated with eggs or gravid proglottids causes infection in cattle (Teania saginata) and pigs (Taenia solium). (3) After emerging from the eggs, oncospheres pass through the intestinal wall and travel to the muscles, where they mature into cystcerci. (4) Humans become infected by consuming raw or undercooked infected meat containing larvae. The larvae. (5) In the human small intestine, the larvae mature into adult tapeworms. (6) The tapeworm’s head, or scolex, adheres to the small intestine mucosa [1, 13].
Figure 4.
Life cycle of Taenia saginata and T. solium [12].
3.5 Pathogenesis and clinical symptoms
T. saginata and T. solium cause intestinal taeniasis. Symptomatic infection leads to nausea, diarrhea, indigestion, weight loss, and vague abdominal pain. The larval stages of T. solium (cysticercus cellulosae) cause cysticercosis [11, 14]. Humans become infected after consuming T. solium eggs in contaminated food or water. It can affect any organ or tissue, but the brain, eyes, and subcutaneous tissues are the most commonly affected. Except in the eye and brain ventricles, the cysticercus is encased in a fibrous capsule. The cellular response induced by degenerating larvae involves neutrophils, eosinophils, lymphocytes, and plasma cells. Calcification results from the subsequent fibrosis and larval death. The affected site influences the clinical signs. Acute myositis is the symptom of muscular cysticercosis; subcutaneous nodules are usually asymptomatic. The most prevalent and dangerous type, known as neurocysticercosis (brain cysticercosis), results in adult-onset epilepsy [15]. Another common condition is headaches. Vision loss or blurriness are common symptoms of ocular cysticercosis [16].
3.6 Diagnosis
Specimen: blood, muscle tissue, CSF, and feces.
Macroscopic examination: Specimen examined for segments or proglottids. Dark yellow feces contrast sharply with the whitish segment. Identification of distinct eggs, gravid proglottids, or scolex (Taenia soluim has a row of hooks, whereas Taenia saginata does not) in feces. Acid-fast staining can be used to diagnose the species because the eggs of T. soluim and T. saginata are similar. While T. saginata eggs are acid-fast, T. soluim eggs are not [13, 14].
Antigen detection: Employed for screening intestinal taeniasis. Polyclonal antisera is used in ELISA to capture antigens.
Serodiagnosis: Anti-cysticercus antibodies in serum or CSF are found via serological tests. ELISA and immunoelectrotransfer blot were employed [14].
Histopathological diagnosis: NCC is diagnosed by demonstrating cysticerci in brain biopsy tissue. Skeletal cysticercosis is diagnosed by histological examination of biopsy [13].
Imaging: X-rays and CT scans are used to detect dead, calcified, and multiple cysts in different body regions. MRI shows mural nodules as pathognomonic for NCC [13, 14, 15].
Other tests: Elevated CSF protein levels and lymphocytosis are commonly observed in neurocysticercosis. Glucose levels may be low. Eosinophils in CSF are common but nonspecific [17].
3.7 Treatment
Praziquantel (5–10 mg/kg orally, given as a single dose) is the recommended treatment for intestinal taeniasis. An alternative would be to take 2 g of niclosamide orally in one dose [16]. When cysts are accessible, excision is the most effective treatment for cysticercosis. For cerebral cysticercosis, two possible treatments are albendazole (15 mg/kg daily, up to 800 mg/day for 8 days) and praziquantel (50 mg/kg in three divided doses daily for 15 days). To lessen inflammatory responses brought on by dead cysticerci, corticosteroids may be given in combination with albendazole or praziquantel. It is necessary to administer antiepileptic medications. Hydrocephalus requires surgical intervention [18].
3.8 Prevention and control
Ensuring that beef and pork are cooked thoroughly.
Maintaining proper sanitation practices.
Practicing good personal hygiene.
Avoiding eating raw veggies cultivated in contaminated soil to stop cysticercosis from developing.
Treat individuals with Taeniasis solium, as they are at risk of developing cysticercosis through self-infection.
4. Taenia saginata asiatica (Asian Taenia or Taenia asiatica)
There is a close relationship between Taenia saginata asiatica and T. saginata. Though it is smaller in size, its morphology is similar to that of T. saginata. Its intermediate host is the pig, and its cysticerci are mostly found in the pig’s liver. Treatment, diagnosis, and clinical characteristics are comparable to T. saginata.
4.1 Distribution
Taenia saginata asiatica is found mainly in Asia. Originally identified as Taiwan Taenia sp., this cestode was initially found in Taiwanese aboriginal people [19].
4.2 Predilection site
The human intestine and the liver of pigs and wild boars are the sites of T. asiatica infection.
4.3 Morphology
Similar to other species of taenia, the eggs of T. asiatica measure 30–35 micrometers in diameter and have radial striations (Figure 3). The oncosphere inside the eggs has six refractile hooks. The scolex of T. asiatica has rudimentary hooklets arranged in a wart-like formation. The proglottids of T. asiatica resemble those of T. saginata and have more than 12 primary uterine branches (Figure 3A) [12]. T. asiatica larvae develop in the liver of pigs, cattle, and goats, not in their muscles like T. saginata or T. solium. The mature worm in T. asiatica still has an armed protoscolex, but the hooklets are absent; unlike T. saginata, the adult T. asiatica worm is smaller, measuring 4 to 8 m long and having 300 to 1000 proglottids. Furthermore, the cysticerci of T. asiatica are significantly smaller, with dimensions of approximately 0.5 to 1.7 mm by 0.5 to 2.0 mm, compared to T. saginata or T. solium. mm by 0.5 to 2.0 mm, compared to T. saginata or T. solium [2].
4.4 Life cycle
Although T. asiatica cysticerci are smaller and form in the liver of pigs, cattle, and goats rather than the muscles of cattle like T. saginata or T. solium, their life cycle is similar to that of T. saginata (Figure 4) [12].
4.5 Pathogenesis and clinical symptoms
Generally, taeniasis brought on by T. solium or T. saginata is characterized by mild, nonspecific symptoms [20]. Many individuals with taeniasis asiatica also do not experience symptoms and only become aware of the infection when they pass proglottids in their feces. Even though there are no symptoms, patients infected with the tapeworm can experience emotional distress for a prolonged period while expelling the proglottids. When taeniasis asiatica is symptomatic, it exhibits similar mild and nonspecific signs. Some of the main clinical symptoms include the shedding of proglottids in the stools, abdominal pain, nausea, diarrhea, constipation, dizziness, increased appetite, headache, and itching around the anus [2].
4.6 Diagnosis
The diagnosis of T. asiatica and T. saginata is challenging due to their similar morphologies [17]. Previously, diagnosing human intestinal taeniasis relied on finding bile-stained eggs and gravid proglottids in the feces. However, recent studies suggest that microscopic examination alone is not reliable for distinguishing T. saginata from T. asiatica due to their similarities [16]. This raises the possibility that the true prevalence of T. asiatica may be underestimated. To address this, newer and more reliable detection methods, such as serological and molecular techniques, have been developed.
4.7 Treatment
Praziquantel or niclosamide are recommended for treating taeniasis. The adult worm is eliminated using the same treatment strategy that is employed for T. solium and T. saginata. Generally, therapy is highly effective. Retreatment is required if proglottids reappear in the stool or emerge from the anus [16].
4.8 Control and prevention
Ensure thorough cooking of pig liver.
Practice proper sanitation.
Maintain good personal hygiene.
Treat individuals with T. asiatica to prevent self-infection and the development of cysticercosis
H. Nana has been referred to as the dwarf tapeworm. The life cycle does not require an intermediate host.
5.1 Distribution
Its distribution is worldwide. Infection is most prevalent in children.
5.2 Predilection site
Adult worms live in the ileum of humans.
5.3 Morphology
Morphologically, Hymenolepis nana is the smallest cestode that can infect humans. The adult worm is less than 1 mm thick and ranges in length from 5 to 45 mm. It has a retractile rostellum with a single row of hooklets and a scolex with four suckers (Figure 5A). With a narrow neck, the worm has a strobila made up of at least 200 proglottids, which are wider than they are long. The uterus has three round testes. Gravid segments disintegrate to release eggs into the intestine. The eggs are roughly spherical or ovoid, approximately 30–40 μm in size. They have an inner embryophore that encloses the hexacanth oncosphere and a thin outer membrane (Figure 5B). Between the two membranes, there are 4–8 thread-like polar filaments that arise from two knobs on the embryophore. Eggs are immediately infectious when passed in feces [20].
Figure 5.
(A) Scolex of H. nana. H. nana Egg in an unstained formalin ethyl acetate (FEA) wet mount is shown in (B) Four of the oncosphere hooks can be seen clearly in this image [21].
5.4 Life cycle
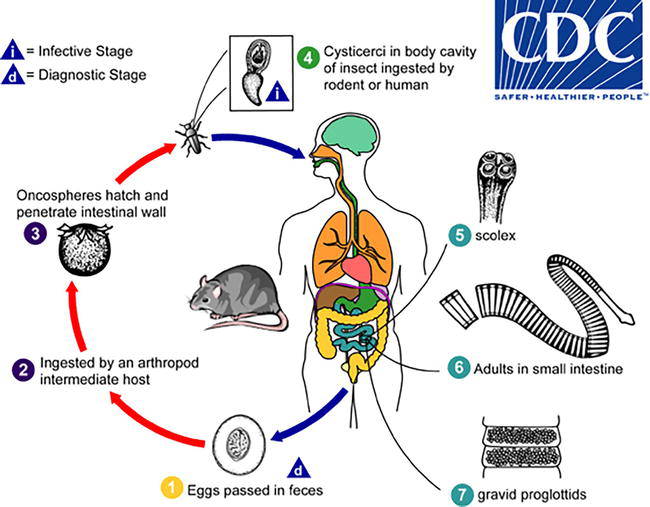
(1) Infected humans pass out embryonic eggs in their feces. (2) Insects (flea, beetle) ingest the eggs and develop into cysticercoid larvae. (3) When humans or rodents consume arthropods contaminated with cysticercoid mites, they become infected. (4) Consuming embryonated eggs from contaminated food, water, or hands can also expose humans to infection. (5) In the intestinal villus, the egg hatches and releases an oncosphere that matures into a cysticercoid. (6–7) The larva develops into an adult worm after emerging from the villus in the small intestine lumen. The adult worm’s scolex is attached to the small intestine’s ileal region. (8) The gravid proglottids release the eggs, which are then excreted in feces (Figure 6) [21].
Figure 6.
Life cycle of Hymenolepis nana [21].
5.5 Pathogenesis and clinical symptoms
In humans, adult H. nana worms mainly reside in the upper section of the ileum. A H. nana infection may be asymptomatic, even if there is a high number of worms present [22]. Symptoms that can occur include headache, Anal pruritus, dizziness, loss of appetite, abdominal pain, diarrhea, and possible irritability, particularly when there are 1000 to 2000 worms [22, 23]. Some patients may experience mild eosinophilia (5% or more). Young children with severe infections may have loose stools or diarrhea with mucus. The most common symptom reported is persistent, widespread abdominal pain [24]. Heavy infections in humans can be caused by internal autoinfection, where the eggs hatch in the intestine and complete the normal life cycle to become adult worms. This feature of the life cycle can lead to complications in individuals with weakened immune systems [25].
5.6 Diagnosis
Adult worms or proglottids are seldom observed in stool samples.
Microscopic examination: the presence of characteristic eggs with a thin shell, a six-hooked oncosphere, and polar filaments confirms the infection
Egg morphology is best observed in fresh specimens or those preserved in formalin-based fixatives.
It is important to note that works against the intestinal villi’s cysticercoids as well as the adult worms. The eggs are infectious, so caution should be exercised when handling unpreserved stools.
5.7 Treatment
The preferred treatment is praziquantel (25 mg/kg in a single dose). It acts both against the adult worms and the cysticercoids in the intestinal villi. Nitazoxanide is an alternative drug [23].
5.8 Prevention and control
Maintain good personal hygiene.
Ensure proper sanitation practices.
Steer clear of consuming food and water that may be contaminated by fleas or beetles.
H. diminuta is rarely found in humans, despite being frequently found in rats and mice.
6.1 Distributions
H. diminuta has a worldwide distribution.
6.2 Morphology
In terms of morphology, H. diminuta differs from H. nana in that the scolex of H. diminuta lacks hooks on the rostellum. It is common to find multiple worms, each shorter in length than a single worm. While some adult worms (measuring 20 to 60 cm long) may occasionally be passed in the stool, eggs are usually obtained and identified. These eggs resemble those of H. nana, but they are larger and measure between 60 and 79 μm. They contain a six-hooked oncosphere and a clear area without polar filaments, unlike H. nana, which has polar filaments that arise from polar thickenings. This area in H. diminuta contains a gelatinous matrix (see Figure 7) [21, 26].
Figure 7.
Egg of H. diminuta in a wet mount stained with iodine. Four of the hooks are visible at this level of focus [21].
6.3 Life cycle
The eggs of Hymenolepis diminuta, a parasite found in rodents and humans, are passed out through feces. (1). These mature eggs are consumed by intermediate hosts like arthropods. (2). once ingested, oncospheres are released from the eggs and penetrate the host’s intestinal wall (3). Then they develop into cysticercoid larvae. Tribolium species commonly serve as intermediate hosts for H. diminuta. Mammals become infected with H. diminuta by ingesting an intermediate host carrying the cysticercoid larvae (4). Humans can accidentally contract the infection by ingesting insects present in precooked cereals, other food items, or directly from the environment (especially children exploring orally). After ingestion, the arthropod tissue is digested, releasing the cysticercoid larvae in the stomach and small intestine. Shortly after being released, the larvae evaginate their scoleces. (5). Using the scolex’s four suckers, the parasite attaches to the small intestine wall. Within 20 days, the parasites mature and can grow up to an average length of 30 cm. (6). Gravid proglottids in the small intestine release eggs (7), which are expelled into the environment through the mammalian host’s feces (Figure 8) [21].
Figure 8.
Life cycle of Hymenolepis diminuta [21].
6.4 Pathogenisis and clinical symptoms
Most tapeworm infections in humans are typically well-tolerated, often without any noticeable symptoms. While the majority of infections have been observed in children under the age of 3, cases of infected adults have also been documented. In some instances, symptoms such as diarrhea, loss of appetite, nausea, headaches, and dizziness have been reported, primarily in children with severe infection [2].
6.5 Diagnosis
Although human infection is uncommon, it can be diagnosed by recovering and identifying the distinctive eggs, which have a thin shell, a six-hooked oncosphere, and no polar filaments.
As part of proficiency testing programs, laboratories may occasionally receive these eggs for identification, and it is crucial to distinguish them from H. nana eggs.
Unlike H. nana eggs, the eggs of H. diminuta are not contagious between individuals.
6.6 Treatment
Praziquantel is recommended as a single dose of 5 to 10 mg/kg of body weight [27].
6.7 Prevention and control
To prevent the infection, it is advised to avoid accidentally ingesting intermediate arthropod hosts. Implementing rat control programs may also reduce the risk of human exposure.
This common double-pore tapeworm of dogs and cats may cause human infection, mainly in children.
7.1 Distribution
Dipylidium caninum is distributed globally.
7.2 Predilection site
The adult tapeworm resides in the small intestine of the host.
7.3 Morphology
The adult intestinal worm measures approximately 10–70 cm in length. Its scolex features four prominent suckers and a retractable rostellum with up to seven rows of spines (Figure 9B). It consists of 60–175 proglottids that resemble melon seeds. Each mature proglottid has two genital pores, one on each side. Gravid proglottids, which contain egg packets enclosed in capsules, are released through the host’s anus individually or in clusters (Figure 9B) [2, 21, 28, 29].
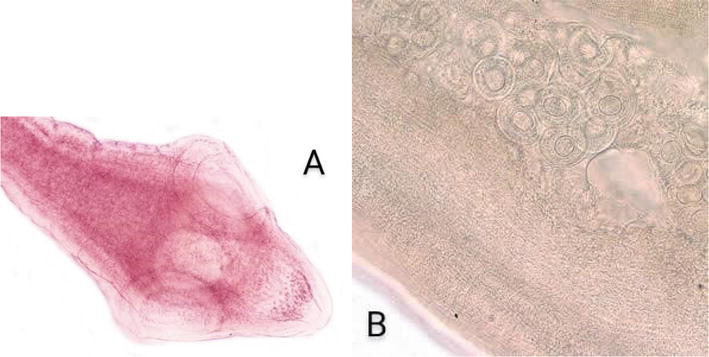
Figure 9.
(A) D. caninum scolex. (B) D. Caninum proglottid partially cleared with lactophenol, showing eggs and egg packets [28].
7.4 Life cycle
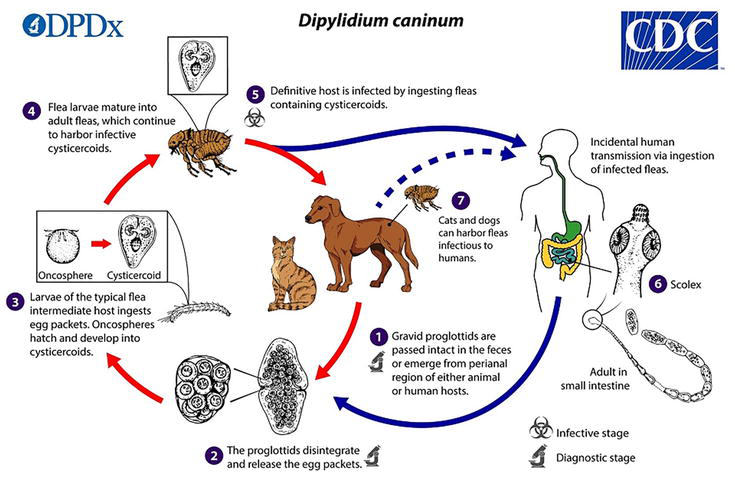
(1–2) Eggs or proglottids from dogs and cats are consumed by larvae of dog fleas (Ctenocephalides canis) and cat fleas (C. felis). (3) Oncospheres hatch and enter the intestinal wall, developing into cysticercoids in the body cavity of the flea larvae. (4) Adult fleas carry the infectious cysticercoids. (5–7) Definitive hosts, including humans, become infected by ingesting fleas that contain cysticercoids. (8) The adult worm develops with its scolex attached to the small intestine (Figure 10) [28].
Figure 10.
The life cycle of Dipylidium caninum [28].
7.5 Pathogenesis and clinical symptoms
It is possible for gravid proglottids to actively migrate out of the anus. Human infections are usually asymptomatic. Some patients may experience abdominal pain, diarrhea, or anal pruritus.
7.6 Diagnosis
The diagnosis is often made using highly distinctive egg packets.
The shape of the proglottids (rice grains when dry, cucumber seeds when fresh) and the presence of recoverable egg packets from a ruptured proglottid are used to identify them.
7.7 Treatment
The drug of choice is praziquantel (5–10 mg/kg orally in a single-dose therapy).
7.8 Prevention and control
Regular deworming of infected dogs and cats
Prevention of flea infestation to avoid reinfection of the animals
Treating affected cases.
References
1.Mahmud R, Lim YAL, Amir A. Medical Parasitology. Gewerbestrasse, Switzerland: Springer International Publishing; 2017. DOI: 10.1007/978-3-319-68795-7
2.Garcia LS. Diagnostic medical parasitology. Santa Monica, California: ASM Press eBooks; 2016. DOI: 10.1128/9781555819002
3.Scholz T, Garcia HH, Kuchta R, Wicht B. Update on the human broad tapeworm (genus diphyllobothrium), including clinical relevance. Clinical Microbiology Reviews. 2009;22(1):146-160. Table of Contents
4.CDC - Dpdx - Diphyllobothriasis. 2019. Centers for Disease Control and Prevention. Available from: www.cdc.gov/dpdx/diphyllobothriasis/index.html
5.Kuchta R, Radačovská A, Bazsalovicsová E, Viozzi G, Semenas L, Arbetman M, et al. Host switching of zoonotic broad fish tapeworm (Dibothriocephalus latus) to salmonids, patagonia. Emerging Infectious Diseases. 2019;25(11):2156-2158
6.Choi HJ, Lee J, Yang HJ. Four human cases of Diphyllobothrium latum infection. The Korean Journal of Parasitology. 2012;50(2):143-146
7.Tsuboi M, Hayakawa K, Yamasaki H, Katanami Y, Yamamoto K, Kutsuna S, et al. Clinical characteristics and epidemiology of intestinal tapeworm infections over the last decade in Tokyo, Japan: A retrospective review. PLoS Neglected Tropical Diseases. 2018;12(2):e0006297
9.Waeschenbach A, Brabec J, Scholz T, Littlewood DTJ, Kuchta R. The catholic taste of broad tapeworms - multiple routes to human infection. International Journal for Parasitology. 2017;47(13):831-843
10.Lloyd AE, Honey BL, John BM, Condren M. Treatment options and considerations for intestinal helminthic infections. The Journal of Pharmacy Technology. 2014;30(4):130-139
11.Dermauw V, Dorny P, Braae UC, Devleesschauwer B, Robertson LJ, Saratsis A, et al. Epidemiology of Taenia saginata taeniosis/cysticercosis: A systematic review of the distribution in southern and eastern Africa. Parasites & Vectors. 2018;11(1):578
12.CDC - Dpdx – Taeniasis. Available from: www.cdc.gov/dpdx/taeniasis/index.html [Accessed: March 2, 2024]
13.Garcia HH, O'Neal SE, Noh J, Handali S. Cysticercosis working Group in Peru. Laboratory diagnosis of Neurocysticercosis (Taenia solium). Journal of Clinical Microbiology. 2018;56(9):e00424-e00418
14.Silva CV, Costa-Cruz JM. A glance at Taenia saginata infection, diagnosis, vaccine, biological control and treatment. Infectious Disorders Drug Targets. 2010;10(5):313-321
15.Reddy DS, Volkmer R. Neurocysticercosis as an infectious acquired epilepsy worldwide. Seizure. 2017;52:176-181
16.Okello AL, Thomas LF. Human taeniasis: Current insights into prevention and management strategies in endemic countries. Risk Management and Healthcare Policy. 2017;10:107-116
17.Yamasaki H, Allan JC, Sato MO, Nakao M, Sako Y, Nakaya K, et al. DNA differential diagnosis of Taeniasis and cysticercosis by multiplex PCR. Journal of Clinical Microbiology. 2004;42:548-553. DOI: 10.1128/JCM.42.2.548-553.2004
18.Webb CM, White AC. Update on the diagnosis and Management of Neurocysticercosis. Current Infectious Disease Reports. 2016;18(12):44
19.Ooi HK, Ho CM, Chung WC. Historical overview of Taenia asiatica in Taiwan. The Korean Journal of Parasitology. 2013;51:31-36. DOI: 10.3347/kjp.2013.51.1.31
20.King CH, Mandell GL, Bennet JE, Dolin R. Mandel, Douglas and Bennett’s Principles and Practice of Infectious Disease. 7th ed. Philadelphia: Churchill Livingstone Elsevier; 2010. Cestodes (tapeworms)
21.CDC - Dpdx - Hymenolepiasis. Centers for Disease Control and Prevention. 2017. Available from: www.cdc.gov/dpdx/hymenolepiasis/index.html
22.Cabada MM, Morales ML, Lopez M, Reynolds ST, Vilchez EC, Lescano AG, et al. Hymenolepis nana impact among children in the highlands of Cusco, Peru: An emerging neglected parasite infection. The American Journal of Tropical Medicine and Hygiene. 2016;95(5):1031-1036. DOI: 10.4269/ajtmh.16-0237
24.Muehlenbachs A, Bhat Nagar J, Agudelo CA, Hidron A, Eberhard ML, Mathison BA, et al. Malignant transformation of Hymenolepis nana in a human host. The New England Journal of Medicine. 2015;373(19):1845-1852. DOI: 10.1056/NE-JMc1600490
25.Thompson RC. Neglected zoonotic helminths: Hymenolepis nana, Echinococcus canadensis and Ancylostoma ceylanicum. Clinical Microbiology and Infection. 2015;21(5):426-432. DOI: 10.1016/j.cmi.2015.01.004
26.Rozario T, Newmark PA. A confocal microscopy-based atlas of tissue architecture in the tapeworm Hymenolepis diminuta. Experimental Parasitology. 2015;158:31-41. DOI: 10.1016/j.exppara.2015.05.015
27.Woolsey ID, Fredensborg BL, Jensen PM, Kapel CMO, Meyling NV. An insect–tapeworm model as a proxy for anthelminthic effects in the mammalian host. Parasitology Research. 2015;114:2777-2780. DOI: 10.1007/s00436-015-4477-0
28.CDC - Dpdx - Dipylidium Caninum. Centers for Disease Control and Prevention. 2019. Available from: www.cdc.gov/dpdx/dipylidium/index.html#tabs-1-2
29.Benitez-Bolivar P, Rondón S, Ortiz MI, Díaz-Díaz J, León C, Riveros J, et al. Morphological and molecular characterization of the parasite Dipylidium caninum infecting an infant in Colombia: A case report. Parasites & Vectors. 2022;15(1):463. DOI: 10.1186/s13071-022-05573-4
Written By
Samatar Abshir Mahamed
Submitted: 27 January 2024Reviewed: 29 January 2024Published: 10 April 2024