Open Access is an initiative that aims to make scientific research freely available to all. To date our community has made over 100 million downloads. It’s based on principles of collaboration, unobstructed discovery, and, most importantly, scientific progression. As PhD students, we found it difficult to access the research we needed, so we decided to create a new Open Access publisher that levels the playing field for scientists across the world. How? By making research easy to access, and puts the academic needs of the researchers before the business interests of publishers.
We are a community of more than 103,000 authors and editors from 3,291 institutions spanning 160 countries, including Nobel Prize winners and some of the world’s most-cited researchers. Publishing on IntechOpen allows authors to earn citations and find new collaborators, meaning more people see your work not only from your own field of study, but from other related fields too.
Platelet-rich plasma (PRP) is a biological product with regenerative capacity. It is used in different fields of medicine such as traumatology, dentistry and dermatology, among others. Classically, PRP has been obtained by centrifugation, which generates a plasma enriched in platelets and their components compared to basal levels. However, this process does not enrich all the biomolecules present outside the platelets. Recently, different collection systems have been developed based on different processes such as filtration, sedimentation, ultrasound, microfluidics or water absorption. These systems often provide a more efficient collection in terms of enrichment or speed of collection. Importantly, some of them also favor the enrichment of extraplatelet components. This is potentially an advantage over other systems, given that extraplatelet factors such as IGF-1 or HGF have been reported to play a key role in contributing to the regenerative capacity of PRP.
Advanced Biological Therapy Unit, Hospital Vithas Vitoria, Vitoria-Gasteiz, Spain
Maider Beitia
Advanced Biological Therapy Unit, Hospital Vithas Vitoria, Vitoria-Gasteiz, Spain
Diego Delgado
Advanced Biological Therapy Unit, Hospital Vithas Vitoria, Vitoria-Gasteiz, Spain
Pello Sánchez
Advanced Biological Therapy Unit, Hospital Vithas Vitoria, Vitoria-Gasteiz, Spain
Arthroscopic Surgery Unit, Hospital Vithas Vitoria, Vitoria-Gasteiz, Spain
Ane Miren Bilbao
Arthroscopic Surgery Unit, Hospital Vithas Vitoria, Vitoria-Gasteiz, Spain
Nicolas Fiz
Arthroscopic Surgery Unit, Hospital Vithas Vitoria, Vitoria-Gasteiz, Spain
Beatriz Aizpurua
Arthroscopic Surgery Unit, Hospital Vithas Vitoria, Vitoria-Gasteiz, Spain
Juan Azofra
Arthroscopic Surgery Unit, Hospital Vithas Vitoria, Vitoria-Gasteiz, Spain
Mikel Sánchez*
Advanced Biological Therapy Unit, Hospital Vithas Vitoria, Vitoria-Gasteiz, Spain
Arthroscopic Surgery Unit, Hospital Vithas Vitoria, Vitoria-Gasteiz, Spain
*Address all correspondence to: mikel.sanchez@ucatrauma.com
1. Introduction
In recent years, regenerative medicine has spread widely in both research and clinical use. One of the reasons is that both the goal and the treatments framed in this field can be cross-cutting and common to many medical specialties. This main objective is to restore and recover the function of damaged tissues by promoting cellular repair and regeneration processes [1]. Thus, therapies such as blood-derived or cell-based products have emerged to generate these biological processes through which different pathologies can be solved. While cell therapies are still in its infancy and have to overcome several challenges [2], blood derivatives such as platelet-rich plasma (PRP) have been applied for more than 15 years becoming a well-established treatment for certain conditions [3].
However, despite the progress made in the field of PRP, there are still many questions surrounding this treatment, which hinder the achievement of optimal clinical results. Factors that affect the efficacy of PRP can arise from different sources such as the patient, the pathology, the product applied or the application protocol [4]. Indeed, the medico-scientific community has already recognized the importance of collecting and analyzing data of this nature, and that conditions the clinical outcomes of PRP treatment [5].
Much of this data focuses on aspects related to the analysis of PRP composition, such as the presence of leukocytes or platelet concentration. In fact, the platelet has been the main element to which the efficacy of PRP is attributed so far. Because of this, the goal of many PRP systems is to achieve great platelet recovery in order to achieve a high platelet concentration [6, 7, 8]. Although this may be reasonable because of the importance of platelet content in tissue repair, high platelet concentrations do not guarantee optimal cell behavior [9]. Furthermore, it is necessary to emphasize that the effect of PRP does not depend only on platelets but also on other extraplatelet elements present in the plasma [10]. The synergistic action of all the components of PRP is one of the main factors responsible for the efficacy of this treatment [11]. However, increasing the levels of plasma molecules requires the development of techniques and systems that allow not only platelet but also molecular enrichment, which is not possible with conventional centrifugation.
Therefore, the intention of this chapter is to describe the main effector components of PRP, including and highlighting the extraplatelet components. In addition, a review of current systems for obtaining PRP is also made, focusing mainly on those that propose alternative methods to centrifugation and those that aim to obtain high levels of non-platelet molecules.
Platelet-rich plasma or PRP is a hemoderivative product classified as a biological therapy [12]. It is used in regenerative medicine due to its reparative capacity of injured tissues. Its restorative capacity lies in its enrichment in platelets and the biomolecules stored in them, such as growth factors or interleukins among others. Although this capacity has traditionally been thought to be driven by platelets and their factors, in recent years, it has been reported the essential role of the extraplatelet factors in these regenerative processes.
2.1 Platelets
Platelets are anucleate subcellular fragments derived from megakaryocytes. Megakaryocytes are large (30 μm diameter) polynucleated cells that are generated in the bone marrow and migrate to the endothelial barrier and pulmonary vasculature, where, through fragmentation, give rise to platelets [13]. These small discoid cell fragments called platelets are 2–5 μm in diameter and have a lifespan of 7–10 days [14]. They are found in the bloodstream and when blood vessels are disrupted by an injury, they adhere to the affected area by the binding of the von Willebrand factor (vWF) from the platelets to the exposed collagen of the affected vessel. In this manner, platelets aggregate with each other and plug the vessel injury, also being the first barrier of defense against external agents. Thus, platelets play an essential role in the generation of the blood clot in a wound. However, beyond that function, platelets are involved in the maintenance of hemostasis, immune system regulation and tissue repair. Notably, these functions are carried out by the molecular content of platelets.
2.2 Molecular content of the platelets
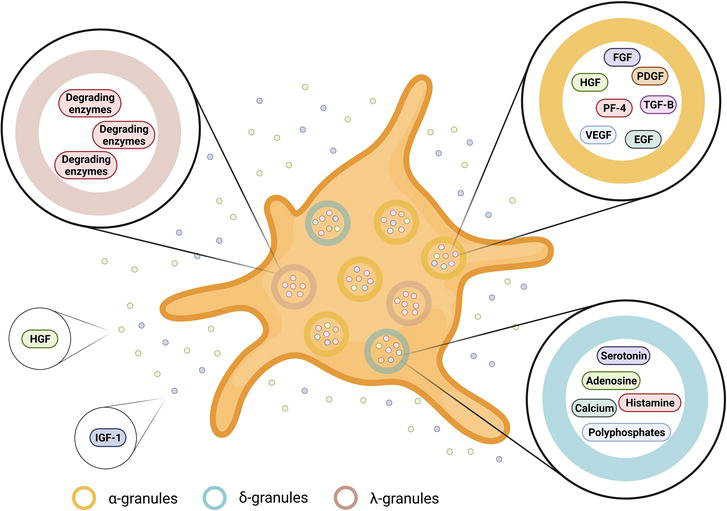
The molecular content of platelets is mainly stored in α-, δ- and λ-granules, although the most abundant are the former. The α-granules contain membrane-bound proteins (integrin and other receptors) as well as soluble bioactive proteins, such as growth factors and cytokines [15]. In turn, δ-granules, also called dense bodies, store proteins that trigger the clot formation, like bioactive amines such as serotonin and histamine, adenosine, polyphosphates and cations like calcium, among others [16]. Finally, λ-granules, also known as lysosomal type organelles, preserve the enzymes responsible for the degradation of proteins, lipids and carbohydrates to ensure the removal of affected tissue residues and infectious agents [17]. In addition, it is important to mention the presence of microvesicles, and exosomes in particular. These vesicles contain, on the one hand, the components synthesized by the megakaryocyte. Additionally, new molecular content is acquired from the medium and, in turn, released in a controlled manner as the platelet travels through the bloodstream [17, 18, 19, 20].
When platelets are activated, these granules are released into the extraplatelet medium, providing the medium with bioactive compounds. Among these, it is included the platelet-derived growth factor (PDGF) [21]. This factor has the capacity to stimulate the chemotaxis of immune system cells, stimulate the proliferation and differentiation of mesenchymal cells, osteoblasts and fibroblasts, among others, and regulate the secretion and synthesis of collagenases and collagen, respectively. Transforming growth factor-β (TGF-β) overall promotes the proliferation and differentiation of mesenchymal stem cells, fibroblasts and keratinocytes among others, and inhibits immune system cell proliferation, stimulates collagen production, inhibits metalloproteinase activity and promotes angiogenesis. However, its effects can vary on the basis of the interacting cells and molecules [21, 22, 23]. Vascular endothelial growth factor (VEGF) promotes angiogenesis and endothelial cell proliferation and migration [24, 25]. Epidermal growth factor (EGF) acts by stimulating the proliferation of keratinocytes, endothelial cells and fibroblasts [26]. Fibroblast growth factor (FGF) promotes the proliferation and migration of fibroblasts, as well as mesenchymal cells, chondrocytes and osteoblasts [27]. Platelet factor-4 (PF-4) acts by regulating the immune system, recruiting leukocytes to the injured area [28].
The bioactive molecular content of platelets is, thus, composed of a vast number of biomolecules that overall regulate coagulation and hemostasis, tissue repair and regeneration and inflammation among others (Figure 1).
Figure 1.
Schematic representation of the platelet content. α-granules (yellow) contain mainly growth factors (PDGF, TGF-β, VEGF, among others), while δ-granules (blue) contain ADP, ATP, Ca2+, neurotransmitters and hormones. Finally, λ-granules (purple) include degrading enzymes. In the extraplatelet medium other exclusive growth factors such as HGF or IGF-1 are present.
2.3 Extraplatelet biomolecules
Beyond the molecular content of the platelets, there are also extraplatelet growth factors and cytokines that exert essential functions in the restoration and reparation of the damaged tissues.
The hepatocyte growth factor (HGF) is present both inside and outside platelets. This factor takes an important part in the modulation of inflammatory processes. In a study by Zhang et al., they analyzed whether HGF had an anti-inflammatory function in tendons. To do this, they performed in vitro tests on tenocytes and in vivo tests on mouse’s Achilles tendon. In both cases, they added, in addition to PRP, recombinant HGF protein and measured cyclooxygenase-1 (COX-1) and 2 (COX-2) and interleukin 1 beta (IL-1β) in the in vitro model and prostaglandin E2 (PGE2) in the in vivo model. The conclusion was that the anti-inflammatory effect of PRP is largely mediated by HGF in a dose-dependent manner [29, 30]. In another study, they used an in vitro model of chondrocytes where they found that when PRP is activated, HGF, interleukin-4 (IL4) and tumor necrosis factor alpha (TNFα), among others, are concentrated. HGF and TNFα have been shown to inhibit the nuclear factor kappa (NF-κB) pathway, thus playing an important role in the anti-inflammatory function of PRP [31].
IGF-1, in turn, is a factor found exclusively outside platelets. In fact, according to some studies, it has been found that IGF-1 levels in both PRP and platelet-poor plasma (PPP) were similar, indicating that this factor is synthesized by other cell types. Concretely, IGF-1 is synthesized in the liver, smooth muscle, chondrocytes and placenta and it is transported throughout the plasma [32, 33, 34, 35]. Its main functions include its ability to promote the proliferation of different cell types. A study conducted in an in vitro model of skin fibroblasts concluded that the higher the concentration of the extraplatelet factor IGF-1, the higher the proliferation at 96 h. IGF-1 was the only growth factor analyzed that was statistically significant when it came to proliferation [10]. This proliferative capacity has been found in different cell types such as chondrocytes, tenocytes, neurons and retinal cells [36, 37, 38, 39].
In addition to proliferation, it has also been shown to play a role in the regulation of inflammation and specifically neuroinflammation, through the interaction with the growth hormone (GH) [40, 41, 42]. Moreover, IGF-1 secreted by chondrocytes has been shown to promote increased proteoglycan and collagen II synthesis and reduce matrix metalloproteinase-13 (MMP-13) synthesis [43]. As such, it helps to reduce the harmful effects of osteoarthritis. In addition, IGF-1 lowers the production of reactive oxygen species (ROS), producing an anti-apoptotic effect in a rat model [44]. All thisimplies that IGF-1 plays an important role in regenerative processes. In fact, in a study by Ortolani et al., PRP and a solution containing PDGF and IGF-1 were added to a rabbit animal model. In the study, they observed greater tissue regeneration when cultured with PDGF and IGF-1 than when cultured with PRP or the negative control (methyl cellulose gel) [45].
At present, there is a wide range of methods to obtain PRP that can be classified as standard and novel. In accordance with this, there are a plenty of commercially available kits to obtain these products, which differ from each other according to certain variables such as platelet, leukocyte and erythrocyte content. On the one hand, it is important to mention that although PRP may contain different concentrations of platelets, an increase in platelets is not directly related to better effectiveness. This could be explained by the possible antagonistic effect that an excess of certain growth factors may cause [46]. Different studies have shown that the optimal platelet concentration could be between 1.5 and 6 times compared to baseline levels in many treatments, with 1.5–3 being the most favorable concentration in most pathologies [9, 47, 48, 49, 50]. Regarding leukocytes, there is controversy as to whether their presence could have a beneficial or detrimental effect on the effectiveness of PRP. While some studies say that leukocytes may have an advantage in the antimicrobial response and, therefore, favor the release of more growth factors and proteinases [17, 51], others claim that leukocytes may increase the inflammatory response, as they induce the release of pro-inflammatory cytokines [52, 53, 54]. In addition, they may increase ROS levels by the action of the neutrophils and affect the wound-healing process [55]. Regarding the presence of erythrocytes, the vast majority of studies state that it can lead to hemolysis and erythrocytosis, generating products that promote inflammation, cellular stress and even cell death [50, 56]. Table 1 lists the systems described below and their properties.
Comparison of the different systems analyzed for the production of PRP for the concentration of platelet and plasma molecules. Different parameters such as type of PRP obtaining system, platelet enrichment fold, time of processing, modulation of extraplatelet factors and concentration of cytokines are evaluated.
3.1 Standard systems for PRP obtaining
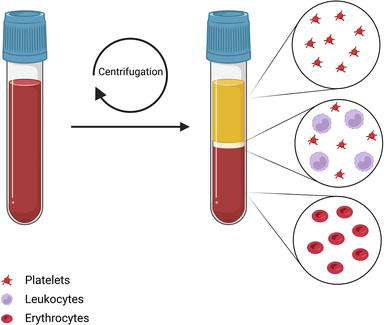
Most of the systems currently used commercially to obtain PRP are based on the centrifugation of blood and subsequent separation of the fractions obtained. The product varies depending on the speed and time parameters applied in the centrifugation, as well as the number of centrifugations carried out in the process (Figure 2). Furthermore, it is important to highlight the collection of the sample, since depending on the fraction or fractions collected, the composition of the PRP may vary. These collection steps have been modified to obtain different commercial PRP formulations. In fact, the final formulation may vary in its content in various aspects such as the number of platelets and the presence or absence of white and red blood cells [72, 73]. Furthermore, depending on the processing of the sample after centrifugation, it is possible to obtain, in addition to liquid formulations, gel formulations for wound application [74].
Figure 2.
Schematic representation of the centrifugation method to obtain the PRP. The blood collecting tube is centrifuged at a specific speed and time at certain cycles. After that, blood is fragmented into different layers. The lower one corresponds to the erythrocyte layer; the small white layer, or buffy coat, contains mostly erythrocytes and platelets; the upper layer corresponds to plasma and contains a gradient of platelets with higher concentration as it approaches the leukocyte layer.
Although centrifugation is the standard method for obtaining PRP, in recent years different methods have been investigated to obtain it more efficiently. These systems, in addition to minimizing user intervention, allow obtaining larger or smaller volumes of PRP depending on the desired application. The systems developed make use of filtration, sedimentation, ultrasound and even microfluidic systems for the separation and elimination of erythrocytes and leukocytes and platelet concentration.
3.2 Novel systems for PRP obtaining
3.2.1 Platelet-derived factor enrichment
Concerning to novel methods for the obtaining of PRP formulations, Jacofsky et al. developed a disposable system to achieve platelet enrichment by filtration. To do this, 60 mL of blood was drawn into a syringe. The contents of the syringe, after mixing them with an aqueous solution, were then passed through a blood filter where the platelets were trapped and all other blood components were removed. To recover the platelets, 7 mL aqueous solution was added, allowing their release and subsequent recovery. This PRP was compared to another one achieved by standard centrifugation where the same volume of PRP was obtained. Although the two products showed similar platelet levels, the collection time was significantly reduced in the new system, from 14 to 7 min [57].
Another system developed by Schmolz describes a PRP obtained by sedimentation and filtration. In short, they collected 8 mL of blood in a syringe with anticoagulant and a sedimentation accelerator. Thus, using a device developed by the group, after 1 h of incubation they achieve a separation of the different components of the blood, which allows the collection of the plasma fraction. This plasma was passed through a filter that traps platelets and removes all traces of the sedimentation accelerator by means of a washing buffer. They then added an aqueous solution to dissolve the platelets and collect the enriched fraction. Subsequent analyses were performed in comparison to baseline levels of unenriched plasma. The results of the study showed a significant increase in TGFβ and PDGF in the new product, compared to baseline levels [58].
In another system, PRP was obtained by ultrasound technology. They collected blood in a 10 mL syringe and applied ultrasounds using two piezoelectric ceramics to generate pressure nodes, causing the red blood cells to settle and, thus, fractionate the blood. In this manner, they obtained 4 mL PRP in 10 minutes. They compared this product with a PRP obtained using a commercial product that requires double centrifugation. Although the results showed a higher platelet fold increase in the new PRP than in the standard double centrifugation, the levels of the platelet growth factor PDGF were not increased [59].
Gifford et al. proposed a system for obtaining PRP by sedimentation and subsequent passage through a microfluidic device. A total of 250 mL of blood was drawn in a bag for blood collection and allowed to settle at a 10° inclination with the aid of two plates exerting pressure on the bag, so that the blood was segmented into fractions of erythrocytes, leukocytes and plasma. Sedimentation took 2.5 h, after which the plasma fraction was recovered. It was then passed through a microfluidic system where platelets were concentrated. As a comparison control, PRP obtained by a standard centrifugation system was used. Measurement of platelet counts revealed that, although both systems enriched the platelets, the standard PRP performed better. However, the new method had a lower percentage of platelets activated by the collection process than the centrifugation-based one [60].
An alternative method, also based on a microfluidic device, was developed by Laxmi et al. This polydimethylsiloxane (PDMS) device enables the Fåhraeus effect, which is based on the fact that when blood is applied at a certain flow rate in a small diameter channel, red blood cells are deformed causing them to move through the center of the channel [75]. Platelets, on the other hand, move through the periphery, where the plasma collection outlets of the channel are located. In this way, a plasma enriched in platelets, but devoid of red blood cells, is obtained. The results showed a platelet enrichment of 8.7% compared to baseline levels [61].
Dickson et al. proposed a microdevice that uses a filter to enrich platelets. To obtain PRP, they apply a constant blood flow through a device containing two filters. In the first one, the red blood cells are retained and only the plasma with platelets passes through to the second filter. In the second filter, only the plasma water passes through, but not the platelets, which are continuously transferred to a collector. The remaining plasma without platelets rejoins the whole blood to continue filtering continuously. It was found that by varying the size of the device and the flow rate applied, a high throughput could be achieved, obtaining up to 50 mL of plasma in as little as half an hour [62].
Something similar was proposed by Kim et al., using a device with two filters to first remove leukocytes and erythrocytes and then part of the plasma, concentrating the PRP. In this case, they used a lab-on-a-disc with a CD format device where they made use of tangential flow filtration. Using this system, a fold of four was obtained compared to baseline levels [63].
3.2.2 Platelet- and extraplatelet-derived factors and cytokine enrichment
To our knowledge, none of these systems have been commercialized and remain in the research phase. All of them focus solely on the enrichment of platelet components, but none take into account bioactive molecules outside platelets, such as IGF-1 and HGF. It is also important to note that pro- and anti-inflammatory cytokines are concentrated during the production of PRP. These play a key role in different biological processes, especially in the inflammatory response. However, there are commercially available novel devices that regulate the concentration of these cytokines in the final formulation.
On the one hand, Zimmer Biomed marketed a protein-based solution called nStride® where PRP enriched in anabolic growth factors and anti-inflammatory cytokines is obtained. To do this, PRP is generated by centrifugation and then passed through a polyacrylamide gel that absorbs part of the water. In addition to platelets, this system concentrates both red and white blood cells [64, 65].
The Orthokine® kit, on the other hand, obtains a serum with an increase in anti-inflammatory cytokines, such as IL-4, IL-10 and IL-1RA. To do this, they incubate a syringe of blood with CrSO4 spheres for 24 hours at 37°C. This causes the monocytes to become activated and the cytokines are released into the blood [76]. Then, by centrifugation, a plasma fraction enriched in anti-inflammatory cytokines is obtained. As a result, it is possible to enrich 140-fold IL-1RA, which, being an IL-1β antagonist, eliminates IL-1β as well [66].
Qrem® cytokine kit is an automatic device that requires no user intervention. It has two chambers, one for the separation of blood components and the other for the activation of both platelets and white blood cells, for the subsequent production of a serum enriched in growth factors and cytokines [67].
These commercial kits focus primarily on cytokine modulation. However, they do not focus on enriching extraplatelet factors. In fact, tissue repair is favored by the physiological balance of growth factors and cytokines, which contain anabolic and catabolic functions in supraphysiologic concentrations, directly into the site of injury optimizing the healing environment. Preserving a natural ratio of these biomolecules may allow the maintenance of the body’s homeostatic environment, which theoretically would provide an abundance of healing factors without disrupting in vivo cellular functions [55, 77, 78].
Concerning the above mention molecular balance, Celling Biosciences launched a device called ART PRP Plus® that is based on filtration. The device is filled with blood, centrifuged and the plasma obtained is passed through fibers with a pore size of 25 kDa several times to remove some of the water and keep all the molecules above this size. This results in PRP enriched not only in platelets but also in the growth factors VEGF, PDGF, TGFβ, alpha-2-macroglobulin (A2M), IL-1RA and fibrinogen. However, this system does not concentrate on the extraplatelet factor IGF-1, as it is smaller than the pore size of the fibers [34, 68].
Recently, new systems have been developed that focus on obtaining PRP by removing water to concentrate all components equally. For this purpose, three water removal systems have been used. The first common step in all three methods is to perform a centrifugation to obtain a PRP with blood-like levels of platelets. One system consists of evaporating the water from the plasma using a rotary evaporator, after applying a certain temperature and pressure. The second method uses centrifuge filtration units to remove some of the water content from the plasma. The last method is based on the use of acrylamide hydrogels to absorb approximately half of the plasma water. Although all three systems are able to enrich platelets and total plasma proteins in a similar way, they do not all succeed in concentrating growth factors equally. The evaporation method fails to concentrate HGF, while the other two systems do. Platelet activation is also higher in the evaporation system, which may be a drawback. In terms of the ability of the final PRP to promote the proliferation of dermal fibroblasts, the absorption system showed greater proliferative capacity, although in all three cases, it was better than that of a standard PRP [69, 70, 71].
Taking into account all these systems and the fact that the presence or absence and even the level of enrichment of different cellular components can affect the efficacy of the PRP product, the comparison between different products is difficult. This would explain the controversy in the literature on the properties of PRP. Because of this various classification systems have attempted to classify and code PRP products for consistency in both application and research.
Thus, Dohan Ehrenfest et al. proposed four categories of platelet concentrates depending on their leucocyte and fibrin content [79, 80]. Years later, Mishra et al. [81] and DeLong et al. [82] also gave importance to the activation of PRP in addition to the number of platelets. In the following classifications, there was also mentioned the presence of erythrocytes [83], the recovery efficiency or centrifugation and application methods addressed [84, 85], trying to classify as much as possible the different PRP products.
4.1 Universal classification system
After these classification systems, Kon et al. proposed a way of PRP coding by which all basic as well as clinical research groups, could make comparisons between results [86]. This system proposed the assignment of a six-digit code grouped in pairs to each PRP that indicates parameters of several variables with the aim of unifying the way PRP is classified for comparison. The code provides the number of basal and enriched platelets, the presence or absence of leukocytes and erythrocytes, and whether platelet activation has been carried out and, if so, which method has been used.
In addition, it is accompanied by informative tables that include data on the preparation and application of PRP, depending on whether the study is in vitro, in vivo or clinical. Finally, the nature of this system allows the code to evolve and expand to take into account future factors such as the extraplatelet molecules discussed in this chapter. Thus, this system extends and adapts the parameters for the Studies Evaluating Biologics in Orthopedics (MIBO) system to the PRP [87].
In conclusion, contrary to what has been considered in the past, platelet factors are not the only ones that play an important role in PRP but also extraplatelet factors are of importance, as demonstrated in multiple studies conducted in recent years. These molecules could enhance PRP effects such as cellular modulation, which would have an impact on its therapeutic potential. Thus, the development of novel systems that allow the enrichment of these factors is encouraged for their potential to improve the biological therapies.
1.Salgado AJ, Oliveira JM, Martins A, Teixeira FG, Silva NA, Neves NM, et al. Tissue engineering and regenerative medicine: Past, present, and future. International Review of Neurobiology. 2013;108:1-33. DOI: 10.1016/B978-0-12-410499-0.00001-0
2.Vizoso FJ, Costa LA, Eiro N. New era of mesenchymal stem cell-based medicine: Basis, challenges and prospects. Revista Clínica Española. 2023;223:619-628. DOI: 10.1016/j.rceng.2023.11.002
3.Cole BJ, Gilat R, DiFiori J, Rodeo SA, Bedi A. The 2020 NBA orthobiologics consensus statement. Orthopaedic Journal of Sports Medicine. 2021;9:23259671211002296. DOI: 10.1177/23259671211002296
4.Sánchez M, Jorquera C, de Dicastillo LL, Fiz N, Knörr J, Beitia M, et al. Real-world evidence to assess the effectiveness of platelet-rich plasma in the treatment of knee degenerative pathology: A prospective observational study. Therapeutic Advances in Musculoskeletal Disease. 2022;14:1759720X221100304. DOI: 10.1177/1759720X221100304
5.Hurley ET, Sherman SL, Stokes DJ, Rodeo SA, Shapiro SA, Mautner K, et al. Experts achieve consensus on a majority of statements regarding platelet-rich plasma treatments for treatment of musculoskeletal pathology. Arthroscopy: The Journal of Arthroscopic and Related Surgery: Official Publication of the Arthroscopy Association of North America and the International Arthroscopy Association. 2023:S0749-8063(23)00673-4;40:470-477.e1. DOI: 10.1016/j.arthro.2023.08.020
6.Muthu S, Krishnan A, Ramanathan KR. Standardization and validation of a conventional high yield platelet-rich plasma preparation protocol. Annals of Medicine and Surgery. 2022;82:104593. DOI: 10.1016/j.amsu.2022.104593
7.Perez AGM, Lana JFSD, Rodrigues AA, Luzo ACM, Belangero WD, Santana MHA. Relevant aspects of centrifugation step in the preparation of platelet-rich plasma. ISRN Hematology. 2014;2014:176060. DOI: 10.1155/2014/176060
8.Rossi R, Garg AK, Kurtzman GM. Novel protocols for the production of autologous blood concentrates with High platelet volume. Compendium of Continuing Education in Dentistry (Jamesburg, N.J.: 1995). 2022;43:140-145; quiz 146
9.Giusti I, D’Ascenzo S, Mancò A, Di Stefano G, Di Francesco M, Rughetti A, et al. Platelet concentration in platelet-rich plasma affects tenocyte behavior in vitro. BioMed Research International. 2014;2014:630870. DOI: 10.1155/2014/630870
10.Beitia M, Delgado D, Mercader J, Sánchez P, López de Dicastillo L, Sánchez M. Action of platelet-rich plasma on in vitro cellular bioactivity: More than platelets. International Journal of Molecular Sciences. 2023;24:5367. DOI: 10.3390/ijms24065367
11.van der Bijl I, Vlig M, Middelkoop E, de Korte D. Allogeneic platelet-rich plasma (PRP) is superior to platelets or plasma alone in stimulating fibroblast proliferation and migration, angiogenesis, and chemotaxis as relevant processes for wound healing. Transfusion (Paris). 2019;59:3492-3500. DOI: 10.1111/trf.15535
12.Alves R, Grimalt R. A review of platelet-rich plasma: History, biology, mechanism of action, and classification. Skin Appendage Disorders. 2018;4:18-24. DOI: 10.1159/000477353
13.Patel SR, Hartwig JH, Italiano JE. The biogenesis of platelets from megakaryocyte proplatelets. The Journal of Clinical Investigation. 2005;115:3348-3354. DOI: 10.1172/JCI26891
14.Josefsson EC, Vainchenker W, James C. Regulation of platelet production and life span: Role of Bcl-xL and potential implications for human platelet diseases. International Journal of Molecular Sciences. 2020;21:7591. DOI: 10.3390/ijms21207591
15.Blair P, Flaumenhaft R. Platelet α–granules: Basic biology and clinical correlates. Blood Reviews. 2009;23:177-189. DOI: 10.1016/j.blre.2009.04.001
16.Sharda A, Flaumenhaft R. The life cycle of platelet granules. F1000Research. 2018;7:236. DOI: 10.12688/f1000research.13283.1
17.Pavlovic V, Ciric M, Jovanovic V, Stojanovic P. Platelet rich plasma: A short overview of certain bioactive components. Open Medicine. 2016;11:242-247. DOI: 10.1515/med-2016-0048
18.Boilard E, Nigrovic PA. Platelets. In: Kelley and Firestein’s Textbook of Rheumatology. Amsterdam: Elsevier; 2017. pp. 264-273.e3. DOI: 10.1016/B978-0-323-31696-5.00016-4
19.Boswell SG, Cole BJ, Sundman EA, Karas V, Fortier LA. Platelet-rich plasma: A milieu of bioactive factors. Arthroscopy: The Journal of Arthroscopic and Related Surgery: Official Publication of the Arthroscopy Association of North America and the International Arthroscopy Association. 2012;28:429-439. DOI: 10.1016/j.arthro.2011.10.018
20.Maynard DM, Heijnen HFG, Horne MK, White JG, Gahl WA. Proteomic analysis of platelet alpha-granules using mass spectrometry. Journal of Thrombosis and Haemostasis. 2007;5:1945-1955. DOI: 10.1111/j.1538-7836.2007.02690.x
21.Qian Y, Han Q , Chen W, Song J, Zhao X, Ouyang Y, et al. Platelet-rich plasma derived growth factors contribute to stem cell differentiation in musculoskeletal regeneration. Frontiers in Chemistry. 2017;5:89. DOI: 10.3389/fchem.2017.00089
22.Yang EY, Moses HL. Transforming growth factor beta 1-induced changes in cell migration, proliferation, and angiogenesis in the chicken chorioallantoic membrane. The Journal of Cell Biology. 1990;111:731-741. DOI: 10.1083/jcb.111.2.731
23.Morikawa M, Derynck R, Miyazono K. TGF-β and the TGF-β family: Context-dependent roles in cell and tissue physiology. Cold Spring Harbor Perspectives in Biology. 2016;8:a021873. DOI: 10.1101/cshperspect.a021873
24.Ferrara N. Role of vascular endothelial growth factor in the regulation of angiogenesis. Kidney International. 1999;56:794-814. DOI: 10.1046/j.1523-1755.1999.00610.x
25.Ballmer-Hofer K. Vascular endothelial growth factor, from basic research to clinical applications. International Journal of Molecular Sciences. 2018;19:3750. DOI: 10.3390/ijms19123750
27.Farooq M, Khan AW, Kim MS, Choi S. The role of fibroblast growth factor (FGF) signaling in tissue repair and regeneration. Cells. 2021;10:3242. DOI: 10.3390/cells10113242
28.Field DJ, Aggrey-Amable AA, Blick SK, Ture SK, Johanson A, Cameron SJ, et al. Platelet factor 4 increases bone marrow B cell development and differentiation. Immunologic Research. 2017;65:1089-1094. DOI: 10.1007/s12026-017-8951-x
29.Zhang J, Middleton KK, Fu FH, Im H-J, Wang JH-C. HGF mediates the anti-inflammatory effects of PRP on injured tendons. PLoS ONE. 2013;8:e67303. DOI: 10.1371/journal.pone.0067303
30.Nakamura T. Structure and function of hepatocyte growth factor. Progress in Growth Factor Research. 1991;3:67-85. DOI: 10.1016/0955-2235(91)90014-U
31.Bendinelli P, Matteucci E, Dogliotti G, Corsi MM, Banfi G, Maroni P, et al. Molecular basis of anti-inflammatory action of platelet-rich plasma on human chondrocytes: Mechanisms of NF-κB inhibition via HGF. Journal of Cellular Physiology. 2010;225:757-766. DOI: 10.1002/jcp.22274
32.El-Sharkawy H, Kantarci A, Deady J, Hasturk H, Liu H, Alshahat M, et al. Platelet-rich plasma: Growth factors and pro- and anti-inflammatory properties. Journal of Periodontology. 2007;78:661-669. DOI: 10.1902/jop.2007.060302
33.Wen Y-H, Lin W-Y, Lin C-J, Sun Y-C, Chang P-Y, Wang H-Y, et al. Sustained or higher levels of growth factors in platelet-rich plasma during 7-day storage. Clinica Chimica Acta: International Journal of Clinical Chemistry. 2018;483:89-93. DOI: 10.1016/j.cca.2018.04.027
34.Laron Z. Insulin-like growth factor 1 (IGF-1): A growth hormone. Molecular Pathology. 2001;54:311-316
35.Nilsson A, Isgaard J, Lindahl A, Dahlström A, Skottner A, Isaksson OG. Regulation by growth hormone of number of chondrocytes containing IGF-I in rat growth plate. Science. 1986;233:571-574. DOI: 10.1126/science.3523759
36.de Figueiredo CS, Raony Í, Medina SV, de Mello SE, Dos Santos AA, Giestal-de-Araujo E. Insulin-like growth factor-1 stimulates retinal cell proliferation via activation of multiple signaling pathways. Current Research in Neurobiology. 2023;4:100068. DOI: 10.1016/j.crneur.2022.100068
37.Zhang B, Hu L, Zhang J, Wu H, Li W, Gou L, et al. Insulin growth factor-1 enhances proliferation and inhibits apoptosis of neural progenitor cells by phosphorylation of Akt/mTOR/p70S6K molecules and triggering intrinsic apoptosis signaling pathway. Cell and Tissue Banking. 2022;23:459-472. DOI: 10.1007/s10561-021-09956-2
38.Zhong J, Zhang J, Zhou Z, Pan D, Zhao D, Dong H, et al. Novel insights into the effect of deer IGF-1 on chondrocyte viability and IL-1β-induced inflammation response. Journal of Biochemical and Molecular Toxicology. 2023;37:e23227. DOI: 10.1002/jbt.23227
39.Disser NP, Sugg KB, Talarek JR, Sarver DC, Rourke BJ, Mendias CL. Insulin-like growth factor 1 signaling in tenocytes is required for adult tendon growth. FASEB Journal: Official Publication of the Federation of American Societies for Experimental Biology. 2019;33:12680-12695. DOI: 10.1096/fj.201901503R
40.Labandeira-Garcia JL, Costa-Besada MA, Labandeira CM, Villar-Cheda B, Rodríguez-Perez AI. Insulin-like growth factor-1 and neuroinflammation. Frontiers in Aging Neuroscience. 2017;9:365
41.Sukhanov S, Higashi Y, Shai S-Y, Vaughn C, Mohler J, Li Y, et al. IGF-1 reduces inflammatory responses, suppresses oxidative stress, and decreases atherosclerosis progression in ApoE-deficient mice. Arteriosclerosis, Thrombosis, and Vascular Biology. 2007;27:2684-2690. DOI: 10.1161/ATVBAHA.107.156257
42.Heemskerk VH, Daemen MA, Buurman WA. Insulin-like growth factor-1 (IGF-1) and growth hormone (GH) in immunity and inflammation. Cytokine & Growth Factor Reviews. 1999;10:5-14. DOI: 10.1016/s1359-6101(98)00022-7
43.Zhang M, Zhou Q , Liang Q-Q , Li C-G, Holz JD, Tang D, et al. IGF-1 regulation of type II collagen and MMP-13 expression in rat endplate chondrocytes via distinct signaling pathways. Osteoarthritis and Cartilage. 2009;17:100-106. DOI: 10.1016/j.joca.2008.05.007
44.Hossain MA, Adithan A, Alam MJ, Kopalli SR, Kim B, Kang C-W, et al. IGF-1 facilitates cartilage reconstruction by regulating PI3K/AKT, MAPK, and NF-kB signaling in rabbit osteoarthritis. Journal of Inflammation Research. 2021;14:3555-3568. DOI: 10.2147/JIR.S316756
45.Ortolani E, Guerriero M, Coli A, Giannuario AD, Minniti G, Polimeni A. Effect of PDGF, IGF-1 and PRP on the implant osseointegration. An histological and immunohistochemical study in rabbits. Annali di Stomatologia (Roma). 2014;5:66
46.Verma R, Kandwal A, Negi G, Chandra H. Factors affecting the quantity and quality of platelet-rich plasma and platelet-derived growth factor-BB: An observational study. Journal of Bio-X Research. 2021;4:67. DOI: 10.1097/JBR.0000000000000091
47.Sánchez M, Anitua E, Azofra J, Andía I, Padilla S, Mujika I. Comparison of surgically repaired Achilles tendon tears using platelet-rich fibrin matrices. The American Journal of Sports Medicine. 2007;35:245-251. DOI: 10.1177/0363546506294078
48.Torricelli P, Fini M, Filardo G, Tschon M, Pischedda M, Pacorini A, et al. Regenerative medicine for the treatment of musculoskeletal overuse injuries in competition horses. International Orthopaedics. 2011;35:1569-1576. DOI: 10.1007/s00264-011-1237-3
49.Hee HT, Majd ME, Holt RT, Myers L. Do autologous growth factors enhance transforaminal lumbar interbody fusion? European Spine Journal: Official Publication of the European Spine Society, the European Spinal Deformity Society, and the European Section of the Cervical Spine Research Society. 2003;12:400-407. DOI: 10.1007/s00586-003-0548-5
50.Everts PA, Malanga GA, Paul RV, Rothenberg JB, Stephens N, Mautner KR. Assessing clinical implications and perspectives of the pathophysiological effects of erythrocytes and plasma free hemoglobin in autologous biologics for use in musculoskeletal regenerative medicine therapies. A review. Regenerative Therapy. 2019;11:56-64. DOI: 10.1016/j.reth.2019.03.009
51.Zimmermann R, Jakubietz R, Jakubietz M, Strasser E, Schlegel A, Wiltfang J, et al. Different preparation methods to obtain platelet components as a source of growth factors for local application. Transfusion (Paris). 2001;41:1217-1224. DOI: 10.1046/j.1537-2995.2001.41101217.x
52.Wang S, Fan W, Jia J, Ma L, Yu J, Wang C. Is exclusion of leukocytes from platelet-rich plasma (PRP) a better choice for early intervertebral disc regeneration? Stem Cell Research & Therapy. 2018;9:199. DOI: 10.1186/s13287-018-0937-7
53.Xu Z, Yin W, Zhang Y, Qi X, Chen Y, Xie X, et al. Comparative evaluation of leukocyte- and platelet-rich plasma and pure platelet-rich plasma for cartilage regeneration. Scientific Reports. 2017;7:43301. DOI: 10.1038/srep43301
54.Liu T, Zhang L, Joo D, Sun S-C. NF-κB signaling in inflammation. Signal Transduction and Targeted Therapy. 2017;2:1-9. DOI: 10.1038/sigtrans.2017.23
55.Anitua E, Andia I, Ardanza B, Nurden P, Nurden A. Autologous platelets as a source of proteins for healing and tissue regeneration. Thrombosis and Haemostasis. 2004;91:4-15. DOI: 10.1160/TH03-07-0440
56.Braun HJ, Kim HJ, Chu CR, Dragoo JL. The effect of platelet-rich plasma formulations and blood products on human synoviocytes. The American Journal of Sports Medicine. 2014;42:1204-1210. DOI: 10.1177/0363546514525593
57.Jacofsky D, Scott M, Smith R, Jennings L, Sowemimo-Coker S, Long M, et al. Method to Prepare Platelet Rich Concentrate From Blood Without a Centrifuge. Vol. 30. Poster presented in the 51st Annual Meeting of the Orthopaedic Research Society. Feb 2005. pp. 20-35
58.Schmolz M, Stein GM, Hübner W-D. An innovative, centrifugation-free method to prepare human platelet mediator concentrates showing activities comparable to platelet-rich plasma. Wounds: A Compendium of Clinical Research and Practice. 2011;23:13
59.Wu Y, Kanna MS, Liu C, Zhou Y, Chan CK. Generation of autologous platelet-rich plasma by the ultrasonic standing waves. IEEE Transactions on Biomedical Engineering. 2016;63:1642-1652. DOI: 10.1109/TBME.2015.2449832
60.Gifford SC, Strachan BC, Xia H, Vörös E, Torabian K, Tomasino TA, et al. A portable system for processing donated whole blood into high quality components without centrifugation. PLoS ONE. 2018;13:e0190827. DOI: 10.1371/journal.pone.0190827
61.Laxmi V, Tripathi S, Joshi SS, Agrawal A. Separation and enrichment of platelets from whole blood using a PDMS-based passive microdevice. Industrial and Engineering Chemistry Research. 2020;59:4792-4801. DOI: 10.1021/acs.iecr.0c00502
62.Dickson MN, Amar L, Hill M, Schwartz J, Leonard EF. A scalable, micropore, platelet rich plasma separation device. Biomedical Microdevices. 2012;14:1095-1102. DOI: 10.1007/s10544-012-9675-2
63.Kim C-J, Ki DY, Park J, Sunkara V, Kim T-H, Min Y, et al. Fully automated platelet isolation on a centrifugal microfluidic device for molecular diagnostics. Lab on a Chip. 2020;20:949-957. DOI: 10.1039/C9LC01140D
64.Higgins JC, Woodell-May J, Hoeppner JC. Use of a Device for Obtaining Interleukin-1 Receptor Antagonist Rich Solutions. EP2567692A1; 2013
65.Muir SM, Reisbig N, Baria M, Kaeding C, Bertone AL. The concentration of plasma provides additional bioactive proteins in platelet and autologous protein solutions. The American Journal of Sports Medicine. 2019;47:1955-1963. DOI: 10.1177/0363546519849671
66.Meijer H, Reinecke J, Becker C, Tholen G, Wehling P. The production of anti-inflammatory cytokines in whole blood by physico-chemical induction. Inflammation Research: Official Journal of the European Histamine Research Society ... [et al.]. 2003;52:404-407. DOI: 10.1007/s00011-003-1197-1
67.Qrem Cytokine. 2023. Available from: https://qrem-regenerative.com/ [Accessed July 7, 2023]
68.Kyle MR, Coull T. Fluid Concentrator, Autologous Concentrated Body Fluids, and Uses Thereof. WO2009002849A2; 2008
69.Mercader Ruiz J, Beitia M, Delgado D, Sánchez P, Sánchez MB, Oraa J, et al. Method to obtain a plasma rich in platelet- and plasma-growth factors based on water evaporation. PLoS One. 21 Feb 2024;19(2):e0297001. DOI: 10.1371/journal.pone.0297001. PMID: 38381708; PMCID: PMC10880971
70.Mercader Ruiz J, Beitia M, Delgado D, Sánchez P, Guadilla J, Pérez de Arrilucea C, et al. Method based on ultrafiltration to obtain a plasma rich in platelet and plasma growth factors. Journal of Clinical Medicine. 2023;12:5941. DOI: 10.3390/jcm12185941
71.Mercader Ruiz J, Beitia M, Delgado D, Sánchez P, Arnaiz MJ, López de Dicastillo L, et al. New formulation of platelet-rich plasma enriched in platelet and extraplatelet biomolecules using hydrogels. International Journal of Molecular Sciences. 2023;24:13811. DOI: 10.3390/ijms241813811
72.Collins T, Alexander D, Barkatali B. Platelet-rich plasma: A narrative review. EFORT Open Reviews. 2021;6:225-235. DOI: 10.1302/2058-5241.6.200017
73.Magalon J, Brandin T, Francois P, Degioanni C, De Maria L, Grimaud F, et al. Technical and biological review of authorized medical devices for platelets-rich plasma preparation in the field of regenerative medicine. Platelets. 2021;32:200-208. DOI: 10.1080/09537104.2020.1832653
74.Gude W, Hagan D, Abood F, Clausen P. Aurix gel is an effective intervention for chronic diabetic foot ulcers: A pragmatic randomized controlled trial. Advances in Skin & Wound Care. 2019;32:416-426. DOI: 10.1097/01.ASW.0000577140.19174.9e
75.Fåhraeus R. The suspension stability of the blood. Physiological Reviews. 1929;9:241-274. DOI: 10.1152/physrev.1929.9.2.241
76.Schutte RJ, Parisi-Amon A, Reichert WM. Cytokine profiling using monocytes/macrophages cultured on common biomaterials with a range of surface chemistries. Journal of Biomedical Materials Research. Part A. 2009;88:128-139. DOI: 10.1002/jbm.a.31863
77.Creaney L, Hamilton B. Growth factor delivery methods in the management of sports injuries: The state of play. British Journal of Sports Medicine. 2008;42:314-320. DOI: 10.1136/bjsm.2007.040071
78.Mishra A, Woodall J, Vieira A. Treatment of tendon and muscle using platelet-rich plasma. Clinics in Sports Medicine. 2009;28:113-125. DOI: 10.1016/j.csm.2008.08.007
79.Dohan Ehrenfest DM, Rasmusson L, Albrektsson T. Classification of platelet concentrates: From pure platelet-rich plasma (P-PRP) to leucocyte- and platelet-rich fibrin (L-PRF). Trends in Biotechnology. 2009;27:158-167. DOI: 10.1016/j.tibtech.2008.11.009
80.Marín, Fermín T, Calcei JG, Della Vedova F, Martinez Cano JP, Arias Calderon C, Imam MA, et al. Review of Dohan Eherenfest et al. (2009) on “Classification of platelet concentrates: From pure platelet-rich plasma (P-PRP) to leucocyte- and platelet-rich fibrin (L-PRF)”. Journal of ISAKOS: Joint Disorders and Orthopaedic Sports Medicine. 2023;9:S2059-7754(23)00545-X. DOI: 10.1016/j.jisako.2023.07.010
81.Mishra A, Harmon K, Woodall J, Vieira A. Sports medicine applications of platelet rich plasma. Current Pharmaceutical Biotechnology. 2012;13:1185-1195. DOI: 10.2174/138920112800624283
82.DeLong JM, Russell RP, Mazzocca AD. Platelet-rich plasma: The PAW classification system. Arthroscopy: The Journal of Arthroscopic and Related Surgery. 2012;28:998-1009. DOI: 10.1016/j.arthro.2012.04.148
83.Mautner K, Malanga GA, Smith J, Shiple B, Ibrahim V, Sampson S, et al. A call for a standard classification system for future biologic research: The rationale for new PRP nomenclature. PM & R : The Journal of Injury, Function, and Rehabilitation. 2015;7:S53-S59. DOI: 10.1016/j.pmrj.2015.02.005
84.Magalon J, Chateau AL, Bertrand B, Louis ML, Silvestre A, Giraudo L, et al. DEPA classification: A proposal for standardising PRP use and a retrospective application of available devices. BMJ Open Sport & Exercise Medicine. 2016;2:e000060. DOI: 10.1136/bmjsem-2015-000060
85.Lana JFSD, Purita J, Paulus C, Huber SC, Rodrigues BL, Rodrigues AA, et al. Contributions for classification of platelet rich plasma—Proposal of a new classification: MARSPILL. Regenerative Medicine. 2017;12:565-574. DOI: 10.2217/rme-2017-0042
86.Kon E, Di Matteo B, Delgado D, Cole BJ, Dorotei A, Dragoo JL, et al. Platelet-rich plasma for the treatment of knee osteoarthritis: An expert opinion and proposal for a novel classification and coding system. Expert Opinion on Biological Therapy. 2020;20(12):1-14. DOI: 10.1080/14712598.2020.1798925
87.Murray IR, Geeslin AG, Goudie EB, Petrigliano FA, LaPrade RF. Minimum information for studies evaluating biologics in orthopaedics (MIBO): Platelet-rich plasma and mesenchymal stem cells. The Journal of Bone and Joint Surgery. American Volume. 2017;99:809-819. DOI: 10.2106/JBJS.16.00793
Written By
Jon Mercader Ruiz, Maider Beitia, Diego Delgado, Pello Sánchez, Ane Miren Bilbao, Nicolas Fiz, Beatriz Aizpurua, Juan Azofra and Mikel Sánchez
Submitted: 19 January 2024Reviewed: 31 January 2024Published: 28 March 2024