Open Access is an initiative that aims to make scientific research freely available to all. To date our community has made over 100 million downloads. It’s based on principles of collaboration, unobstructed discovery, and, most importantly, scientific progression. As PhD students, we found it difficult to access the research we needed, so we decided to create a new Open Access publisher that levels the playing field for scientists across the world. How? By making research easy to access, and puts the academic needs of the researchers before the business interests of publishers.
We are a community of more than 103,000 authors and editors from 3,291 institutions spanning 160 countries, including Nobel Prize winners and some of the world’s most-cited researchers. Publishing on IntechOpen allows authors to earn citations and find new collaborators, meaning more people see your work not only from your own field of study, but from other related fields too.
A pressure ulcer, from its inception, represents a multifaceted challenge, encompassing health, social, and financial dimensions, thereby deteriorating the patient’s overall quality of life. The mitigation of pressure ulcers commences with a methodical evaluation of the dermal condition of individuals deemed at considerable risk. This proactive approach includes vigilant skin care, the utilization of appropriately designed support surfaces, and the regular repositioning of affected patients. This investigation’s main aim is to assess the proficiency of healthcare personnel in pressure ulcer prevention and treatment within the inpatient context. This empirical study featured the participation of 115 healthcare practitioners employed at Nova Gorica General Hospital. The research instrument employed in this inquiry was an adapted questionnaire derived from the work of Pieper Zulkowski, which incorporated 83 items encompassing preventive strategies, wound characteristics, and wound stage categorization. The amassed data were subjected to statistical analysis using IBM SPSS version 29. The internal consistency reliability, as measured by Cronbach’s alpha, for the comprehensive questionnaire was proven at 0.913. However, it is unmistakably evident that a pressing need for continuous and systematic educational interventions concerning pressure ulcer management remains essential and indispensable for healthcare professionals.
Vipava Unit at Faculty of Health Sciences, University of Primorska, Vipava, Slovenia
Rosanda Drufovka
Nova Gorica General Hospital, Šempeter pri Gorici, Slovenia
*Address all correspondence to: melita.persolja@fvz.upr.si
1. Introduction
Pressure ulcer is a localized injury of the skin or underlying tissue, most commonly occurring over bony prominences, caused by pressure or a combination of pressure and shear forces [1]. From the moment a pressure ulcer develops, it becomes a health, social, and financial problem that diminishes the patient’s quality of life. The development of pressure ulcers is influenced by the interaction of numerous risk factors [2]. External factors for the formation of pressure ulcers include unrelieved pressure, shear force, friction, and repeated pressure [3]. Internal factors contributing to pressure ulcer development include malnutrition, immobility, impaired sensation of pressure or pain, urinary and fecal incontinence, consciousness disorders, increased body weight, age, chronic diseases, elevated body temperature, and certain medications [4]. Sites, where pressure ulcers commonly develop, include the hips, sacrum, elbows, ankles, heels, occiput, shoulders, scapulae, fingers, knees, and ears [1]. Pressure ulcers that occur in atypical locations, such as behind the ears, the nose and nostrils, cheeks, forehead, penis, urethral meatus, and lower lip, raise particular concern [5]. The most vulnerable patients for pressure ulcer development are those with limited ability to change positions, spending a significant amount of time in bed or in a chair [6], such as critically ill and injured patients in the intensive care unit, patients with spinal cord injuries, overweight patients, undernourished patients, and patients in the operating room [7].
Preventing pressure ulcers involves skin assessment, nutritional status evaluation, regular repositioning, and the use of preventive cushions. Skin is protected from excretions and excessive moisture, and lotions and skincare creams are used. During pressure ulcer prevention, it is crucial not to massage the skin or rub it in at risk-prone areas [3]. Daily skin inspections are conducted and findings are documented. Care is taken to prevent skin damage from medical devices and equipment such as nasogastric tubes, urinary catheters, oxygen catheters, etc.
The development of a pressure ulcer is a progressive process. If preventive measures to reduce contributing factors are not taken in the presence of a pressure ulcer, it can progress to a more severe stage [8]. Regular assessment of the risk of pressure ulcer development should be carried out as frequently as the patient’s condition requires. The Waterlow assessment scale is most commonly used for assessing the risk of pressure ulcer development. Other scales, such as Norton’s, Braden’s, and others, are also known [9]. Before classifying a pressure ulcer, it is essential to assess the patient and the type of wound. Confirming the presence of pressure and/or shear force as causative factors is crucial in diagnosing pressure ulcers. The nursing staff must have adequate anatomical knowledge to correctly assess the stage of a pressure ulcer as treatment and preventive measures depend on this [10].
Despite efforts, pressure ulcers remain one of the most significant challenges in healthcare. The occurrence of pressure ulcers (the prevalence rate of pressure ulcers in Europe is ranging from 4.6% to 27.2%) represents a deviation that requires serious attention to determine the causes, timing, and key contributing factors to reduce the incidence [11, 12]. A fundamental aspect of providing quality healthcare to prevent pressure ulcer development is the planning and execution of high-quality healthcare. In Slovenia, we follow and adhere to international guidelines for pressure ulcer prevention, harmonized by the European Pressure Ulcer Advisory Panel (EPUAP) and the National Pressure Ulcer Advisory Panel (NPUAP). Healthcare personnel receive basic theoretical knowledge on pressure ulcer prevention during formal education. The continuity of professional education and training must be ensured as it elevates knowledge levels and improves the quality of care [13]. Healthcare staff must possess the necessary skills for accurate wound assessment. To ensure high-quality and effective healthcare for patients with pressure ulcers, continuous education, the study of new guidelines, and collaboration with other healthcare professionals are essential [14] as basic theoretical knowledge on pressure ulcer prevention during formal education alone is insufficient for high-quality patient care [15]. Assessing the knowledge of healthcare staff allows for identifying training needs, priorities, and supports the development of new strategies to enhance the quality of prevention and care for pressure ulcers [16].
This research’s purpose was to examine and present the competence of healthcare professionals in pressure ulcer prevention and care for hospitalized patients. The research aims were to determine the extent to which hospital healthcare employees are knowledgeable about the development, classification, other characteristics of pressure ulcers, their knowledge of preventive measures, tools, prevention, and modern pressure ulcer care.
Based on the research aims, the following research questions were formulated:
What is the proportion of healthcare personnel who have the requisite qualifications to competently manage pressure ulcers in the context of hospitalized patients?
To what degree do the attributes of the respondents correlate with their competency levels?
To what extent do healthcare personnel comprehend the attributes of pressure ulcers?
To what degree are healthcare employees acquainted with pressure ulcer prevention measures?
To what extent are healthcare employees well-versed in the diverse materials and tools for pressure ulcer prevention and care?
To what extent are healthcare employees familiar with current approaches to pressure ulcer care?
Data for the research were obtained using the original PZ-PUKT questionnaire by authors Pieper and Zulkowski [17]. The authors provided us with the questionnaire via email. The research instrument was translated from English to Slovene, and for the purpose of verifying comprehensibility, it was distributed among 20 nurses. The results of the pilot study were considered in preparing the final version of the questionnaire, which consists of 83 questions, with 72 of them assessing the knowledge about pressure ulcers.
The research instrument is divided into two parts. The first part comprises demographic data, including gender, age, education, years of experience, specialized knowledge, and education. The second part consists of three sets of questions related to pressure ulcers: the stages and characteristics of pressure ulcer development (21 questions), wound care (20 questions), and pressure ulcer prevention (31 questions). Respondents had three options for each statement: “True,” “False,” and “I do not know.” Completing the questionnaire required 20 to 30 minutes.
We calculated the internal reliability of the questionnaire (Cronbach’s alpha coefficient), which was found to be 0.913 (n = 72). Piper and Zulkowski [17] reported a preliminary internal reliability of the original questionnaire as 0.800 (n = 72).
The research was conducted from January 2023 to February 2023, on selected departments at the General Hospital Dr. Franca Derganca in Nova Gorica, where healthcare personnel regularly meet patients with pressure ulcers. At the beginning of the research, there were 393 healthcare employees in the hospital, distributed across various departments: internal medicine department 36, orthopedics 10, gynecology 9, rehabilitation and youth disability department 34, surgery 18, intensive care unit for internal medicine, and surgical specialties 36 employees.
The research sample included 120 randomly selected healthcare employees from these departments who received a paper questionnaire during the research period. Of the 120 distributed questionnaires, 115 (95.8%) were returned properly filled out, and 5 were incomplete and had to be discarded.
Most respondents were female (n = 94), while there were 21 males. Nearly half (47.8%) of the respondents had a high school education, while 43.6% had higher professional, college, or university education. A total of 6.1% of respondents held a master’s degree in nursing, and 2.6% had vocational education. The average age of the respondents was 39.28 years (min. 21, max. 63, Sd = 10.9). Slightly over half of the respondents had 15 or more years of experience in healthcare.
The majority (93.0%, n = 107) of the respondents did not have specialized knowledge in wound care. A vast majority, 98.3% (n = 113), also did not possess a license for wound care. One-third of the respondents had never attended any wound care education, and more than a third of them had received education more than 4 years ago. Only 14.4% (n = 16) of the respondents had attended wound care education within the past year or less (Table 1).
Time
Value
N
%
Never
34
30.6
Over 4 years ago
38
34.2
2–3 years ago
15
13.5
More than one, but less than 2 years ago
8
7.2
Within the past year or less
16
14.4
Table 1.
Time of attendance at wound care education (n = 111).
Legend: n = number, % = percent.
We see also that slightly less than one-third (n = 30) of the respondents have been reading literature on wound care in the past year, while 13.5% (n = 15) have never read anything on this topic. Internet literature on pressure ulcers had been read by 33.3% (n = 37) of the respondents within the past year.
We obtained permission to conduct the research from the hospital director, the nursing service, and the commission for medical ethics of the hospital under investigation. The healthcare employees voluntarily participated in the research. They were informed about the research’s purpose and the possibility to decline participation and were ensured about confidentiality and the protection of personal data. The paper questionnaire was enclosed in an envelope, which the participants filled out and sealed. The research was conducted following the Code of Ethics in Healthcare and Nursing in Slovenia (Official Gazette of the Republic of Slovenia, Principle VII, [18]).
The questionnaire responses were entered into an electronic database. Microsoft Excel 2019 was used for presenting the results in tables. Statistical analysis and data processing were performed using IBM SPSS 29.0.
In the analysis, responses were scored as either 0 (incorrect answer or “I do not know”) or 1 (correct answer). At the end, the sum of points from the entire questionnaire was categorized into five levels: below 59% correct answers as low (insufficient) competence, 60–69% as moderate (acceptable) competence, 70–79% as good competence, 80–89% as particularly good competence, and 90% or more as excellent competence.
Characteristics were presented with frequency (n) and percentages (%), maximum (max), minimum (min), mean (M), and standard deviation (Sd). The normality of variable distributions was assessed using Skewness and Kurtosis tests. The association between variables was examined through linear correlation analysis, and the strength of the relationship was expressed using the Pearson coefficient. Associations, following the guidelines from Field (2009), were described with values: 0.00—no association; 0.01–0.19—negligible association; 0.20–0.39—low/weak association; 0.40–0.69—moderate/moderate association; 0.70–0.89—high/strong association; 0.90–0.99—very high/very strong association; 1.00—perfect (functional) association. An analysis of variance (ANOVA) and t-test for independent samples were also conducted to examine the significance of the results. The significance level was considered 0.05.
Respondents scored a minimum of 16 and a maximum of 72 points on the test, which means that the percentage of correct answers ranged from a minimum of 22% to a maximum of 100%. On average, the respondents scored 45.14 out of 72 (62.6 9%, SD = 9.26). We assessed the knowledge of the respondents on a five-point scale, where a minimum of 60% correct answers (43/72) was needed to pass the test. The average result of the entire group of respondents can be classified as “acceptable.”
We found that about 40% of the respondents were unsuccessful (Table 2). Nine respondents (7.8%) proved very good or excellent knowledge, while 59 (51.3%) showed acceptable and good knowledge. The skewness coefficient (0.134) and kurtosis (0.447) show a normal distribution of the results.
Score
Value
n
%
Insufficient (0–59%)
47
40.9
Acceptable (60–69%)
31
27.0
Good (70–79%)
28
24.3
Very good (80–89%)
3
2.6
Excellent (90% or more)
6
5.2
Table 2.
Results of respondents’ points on the test.
Legend: n = number, % = percent.
7.2 Accuracy of responses based on respondent characteristics
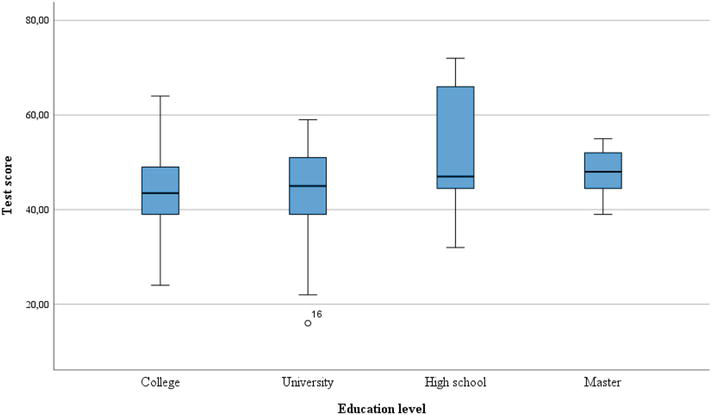
The average number of correct answers increases with age and experience. However, the differences based on both parameters are too small to be statistically significant. We found that the differences in the average number of correct answers are statistically significant based on the level of education. The lowest average score is associated with university education, while the highest is associated with higher professional education (Table 3 and Figure 1).
Sample
Test score
Attribute
n
%
M
F
p
Age, years
20–30
27
24.3
43.96
1.17
0.323
31–40
33
29.7
43.60
41–50
31
27.9
47.51
More than 50
20
18.0
45.71
Years of work
< 1
5
4.3
43.0
1179
0.324
1–5
27
23.5
43.26
5–10
17
14.8
42.76
10–15
12
10.4
44.25
15–20
18
15.7
45.94
20 and more
36
31.3
47.86
Education
College
59
50.4
44.03
University
34
29.6
43.55
3.75
0.013
High school
16
13.9
51.81
Master
7
6.1
47.86
Table 3.
Test score related to demographic attributes (n = 115).
Legend: n = number, % = percent, F = ANOVA value, p = statistical significance.
Figure 1.
Test result related to education level (n = 115).
The differences in test scores between the genders are not significant (t (113) = −0.883; p = 0.379), with men averaging 43.52 (Sd = 8.35) points and women averaging 45.5 (Sd = 9.46) points.
We also investigated the relationship between the number of correct answers and various methods of knowledge acquisition (Table 4). The analysis showed a weak but statistically significant correlation between a successful test outcome and various learning methods such as reading professional literature, searching for content online, and education in wound care. However, we did not find significant correlations with obtaining a license and specialized knowledge in the field.
Education methods
Test score
r
p
Reading nursing care literature
0.298
0.01
Searching internet
0.268
0.004
Education workshops and seminars
0.265
0.004
License
−0.125
0.182
Specialized knowledge
−0.011
0.909
Table 4.
Correlation between education methods and test score (n = 115).
The majority of respondents correctly knew that scars resulting from pressure ulcers are more likely to develop new ulcers than undamaged skin. They also understood that pressure ulcers of stage 3 may appear shallow if they are on the ear, ankle, or heel. Over half of the respondents were aware that moist necrosis is yellow or creamy devitalized tissue on the wound bed and that stage 1 pressure ulcers are characterized by intact skin with unbleachable redness over a bony prominence. A high proportion of respondents correctly noted that pressure ulcers can develop around the ears in individuals using oxygen. Additionally, most respondents knew that if a wound had necrotic tissue with visible or palpable bone, it would be classified as a stage 4 ulcer. The appearance of a blister on the heel was recognized as a cause for concern, and the majority knew that stage 3 pressure ulcers might appear shallow when found on the ear, ankle, or heel. Most respondents were also aware that deep tissue injury can progress to another stage of ulcer.
However, there were gaps in knowledge regarding the stages of pressure ulcer formation. Only one-third believed that an unstageable pressure ulcer, after necrotic tissue removal, should be classified as a stage 2 pressure ulcer. A similar percentage correctly answered that when the wound bed is entirely covered with moist necrosis, the stage cannot be determined. More than half did not know that skin tears are classified as stage 2 pressure ulcers, nor did they realize that stage 3 pressure ulcers involve damage to the epidermis and/or dermis (Table 3). Most respondents were unaware that unbleachable redness occurring anywhere on the body is not a stage 1 pressure ulcer, and the majority did not know that, when a heel wound heals, a dry, adherent scab should not be removed. Most also incorrectly answered that a pressure ulcer on a mucous membrane due to medical equipment is a stage 3 ulcer. Furthermore, most respondents did not know that stage 4 pressure ulcers do not always involve tissue breakdown beneath the skin (Table 5).
Statement
Answer n (%)
Do not know
Wrong
Correct
Wet necrosis is devitalized tissue, yellow or creamy in color, on the wound bed. (P)
7 (6.1)
32 (27.8)
76 (66.1)
A stage 3 pressure ulcer is an injury to the skin that involves the epidermis and/or dermis. (N)
12 (10.4)
58 (50.4)
45 (39.1)
A scab is a healthy tissue. (N)
11 (9.6)
39 (33.6)
65 (56.6)
A pressure ulcer of an undetermined stage, once necrotic tissue is removed, is classified as a stage 2 pressure ulcer. (N)
43 (37.4)
44 (37.4)
45 (37.4)
Healing in chronic wounds is often slowed in the proliferative phase of healing. (N)
23 (23,0)
70 (60.9)
22 (19.1)
To heal a heel wound, a dry, adherent crust should be removed. (N)
12 (10.4)
38 (33.0)
65 (56.5)
In large and deep pressure ulcers, the number of dressings used should be counted and documented so that all dressings are removed during the next change. (P)
10 (8.7)
18 (15.7)
87 (75.7)
A stage 1 pressure ulcer is intact skin with non-blanchable redness over a bony prominence. (P)
11 (9.6)
26 (22.6)
78 (67.8)
When the wound bed is entirely covered with wet necrosis, the ulcer’s stage cannot be determined. (P)
30 (26.1)
57 (49.6)
28 (24.3)
A dressing should keep the wound bed moist and the surrounding area dry. (P)
15 (13.0)
9 (7.8)
91 (79.1)
Hydrocolloid and film dressings should be removed quickly to reduce pain. (N)
11 (9.6)
13 (11.3)
91 (56.5)
Skin tears are classified as stage 2 pressure ulcers. (N)
35 (30.6)
26 (22.6)
54 (47.0)
Stage 3 pressure ulcers may appear shallow when located on the ear, ankle, or heel. (P)
16 (13.9)
13 (11.3)
86 (74.8)
Hydrocolloid dressings should be used on infected stage 2 pressure ulcers. (N)
37 (32.2)
34 (29.6)
44 (38.3)
Pressure ulcers should not be cleaned with drinking water. (N)
11 (9.6)
51 (44.3)
53 (46.1)
Alginates can be used for stage 3 and 4 pressure ulcers with moderate exudate. (P)
28 (24.3)
7 (6.1)
80 (69.6)
Film dressings absorb a significant amount of exudate. (N)
14 (12.2)
36 (31.3)
65 (56.5)
Skin protection cream should be applied around the wound to protect the surrounding tissue from moisture. (P)
10 (8.7)
14 (31.3)
91 (56.5)
Non-blanchable redness anywhere on the body is a stage 1 pressure ulcer. (N)
9 (7.80)
66 (57.4)
40 (34.8)
A stage 2 pressure ulcer is a complete loss of skin thickness. (N)
27 (23.5)
33 (28.7)
55 (47.8)
A stage 2 pressure ulcer can have wet necrosis at the base. (N)
22 (19.1)
58 (50.4)
35 (30.40)
If necrotic tissue is present on the wound, and bone is visible or directly palpable, we classify the ulcer as stage 4. (P)
11 (9.6)
6 (5.2)
98 (85.2)
A pressure ulcer of an undetermined stage, once necrotic tissue is removed, is classified as a stage 2 pressure ulcer. (N)
43 (37.4)
28 (24.3)
44 (28.3)
Blanching refers to the whiteness that occurs when pressure is applied to a reddened area. (P)
26 (22.6)
16 (13.9)
73 (63.5)
A blister on the heel is not a cause for concern. (N)
5 (4.3)
18 (15.7)
92 (80.0)
Early changes related to pressure ulcer development are often overlooked in individuals with dark skin. (P)
33 (28.7)
12 (10.4)
70 (60.9)
In a stage 3 pressure ulcer, bones, tendons, or muscles may be exposed. (N)
13 (11.3)
50 (43.5)
52 (45.2)
The difference between moisture-related skin damage and pressure ulcers can be challenging. (P)
31 (27.0)
17 (14.8)
67 (58.3)
To heal a heel wound, dry, adherent crust should be removed. (N)
20 (17.4)
51 (44.3)
44 (38.3)
A pressure ulcer on mucous membranes due to medical equipment use is stage 3. (N)
46 (40.0)
30 (26.1)
39 (33.9)
Pressure ulcers can develop around the ears in individuals using a nasal cannula for oxygen. (P)
1 (0.9)
11 (9.6)
103 (89.6)
A stage 1 pressure ulcer is intact skin with non-blanchable redness over a bony prominence. (N)
11 (9.6)
26 (22.6)
78 (67.8)
When the wound bed is entirely covered with wet necrosis, its stage cannot be determined. (P)
30 (26.1)
57 (49.6)
28 (24.3)
Stage 3 pressure ulcers may appear shallow when located on the ear, ankle, or heel. (P)
16 (13.9)
13 (11.3)
86 (74.8)
Pressure ulcers should not be cleaned with drinking water. (N)
11 (9.6)
51 (44.3)
53 (46.1)
Alginates can be used for stage 3 and 4 pressure ulcers with moderate exudate. (P)
28 (24.3)
7 (6.1)
80 (69.6)
Deep tissue injury will not progress to another stage of pressure ulcer. (P)
18 (15.7)
17 (14.8)
80 (69.6)
Stage 4 pressure ulcers always lead to tissue breakdown beneath the skin. (N)
13 (11.1)
73 (67.8)
24 (20.9)
Table 5.
Knowledge of pressure ulcers characteristics (n = 115).
Legend: n = number, % = percent, P = positive, the statement is correct, N = negative, the statement is wrong.
7.4 Knowledge of pressure ulcer prevention measures
Table 6 presents responses to the research question regarding knowledge of preventive measures for pressure ulcer prevention.
Statement
Answer n (%)
Do not know
Wrong
Correct
Sitting for individuals at risk of pressure ulcers should be brief and on an appropriate chair/wheelchair with a pressure redistribution cushion. (P)
0 (0.0)
9 (7.8)
106 (92.2)
Individuals with pressure ulcers at high risk should be turned on an individualized schedule regardless of their mobility level unless contraindicated. (P)
4 (3.5)
6 (5.2)
105 (93.3)
New pressure ulcers can be expected sooner on the site of a scar resulting from a pressure ulcer than on undamaged skin. (P)
10 (8.7)
9 (7.8)
96 (83.5)
Dragging a patient across a bed increases friction. (P)
0 (0.0)
14 (12.4)
101 (87.7)
Elevated body temperature is a risk factor for pressure ulcers. (P)
4 (3.5)
21 (18.3)
90 (78.3)
Diabetes mellitus does not increase a person’s risk of pressure ulcers. (N)
3 (2.6)
20 (17.4)
92 (80.0)
Individuals with pressure ulcers and incontinence should use high-absorbency incontinence products. (P)
8 (7.0)
9 (5.2)
101 (87.8)
Anti-decubitus cushions regulate tissue load and skin microclimate. (P)
2 (1.7)
6 (5.2)
107 (93.0)
Individuals at high risk of pressure ulcers should typically supplement their regular diet with nutritional supplements. (P)
16 (13.9)
12 (10.4)
87 (75.7)
When the heel is elevated, the leg’s weight should be evenly distributed longitudinally to prevent pressure ulcer formation. (P)
10 (8.7)
10 (8.7)
95 (82.6)
Ring-shaped cushions help prevent pressure ulcers. (N)
11 (9.6)
85 (73.9)
19 (16.5)
New pressure ulcers can be expected sooner on the site of a scar resulting from a pressure ulcer than on undamaged skin. (P)
10 (8.7)
7 (6.1)
98 (85.2)
A nutritional assessment should be performed in individuals at risk of pressure ulcers. (P)
11 (9.6)
10 (8.7)
94 (81.7)
Critically ill patients may require slow, gradual turning due to hemodynamic instability. (P)
17 (14.8)
15 (13.0)
83 (72.2)
In immobile patients whose feet do not reach the floor, a footstool should not be used. (N)
32 (27.8)
15 (13.0)
68 (59.1)
Massaging bony prominences is essential for quality skin care. (N)
12 (10.4)
52 (45.2)
51 (44.3)
Improper positioning in a wheelchair can be a cause of pressure ulcers. (P)
4 (3.5)
7 (6.1)
104 (90.4)
In individuals with incontinence, the skin should be cleaned after elimination and at routine intervals. (P)
3 (2.6)
3 (2.6)
109 (94.8)
Patients with spinal cord injuries need knowledge about pressure ulcer prevention and self-care. (P)
3 (2.6)
2 (1.7)
110 (95.7)
A pressure ulcer on the mucous membrane resulting from medical equipment use is of stage 3. (N)
46 (40.0)
30 (26.1)
39 (33.9)
Immobile individuals who can be taught should shift their weight while sitting in a chair every 30 minutes. (P)
11 (9.6)
79 (68.7)
25 (21.7)
The selection of an anti-decubitus cushion considers the risk level for pressure ulcer development in a specific person. (N)
5 (4.3)
92 (80.0)
18 (15.7)
A patient using an anti-decubitus cushion is not at risk for shear force injuries. (N)
3 (2.6)
18 (15.7)
94 (81.7)
Patients with spinal cord injuries do not need an assessment of their sitting ability. (N)
15 (13.0)
19 (16.5)
81 (70.4)
To prevent pressure ulcers, the bed’s headrest should be elevated at an angle greater than 45 degrees. (N)
16 (13.9)
17 (14.8)
82 (71.3)
The urinary catheter tube should be placed under the leg. (N)
9 (7.8)
14 (12.2)
92 (80.0)
Properly sized equipment can help prevent pressure ulcers in bariatric patients. (P)
37 (32.2)
3 (2.6)
75 (65.2)
Nurses should avoid turning the patient onto a reddened area. (P)
6 (5.2)
19 (16.5)
90 (78.3)
A person with a spinal cord injury has a lifelong responsibility for pressure ulcer care. (P)
6 (5.2)
7 (6.1)
102 (88.7)
Table 6.
Knowledge of pressure ulcer prevention measures (n = 115).
Legend: n = number, % = percent, P = positive, the statement is correct, N = negative, the statement is wrong.
Most respondents knew that patients with spinal cord injuries need knowledge about pressure ulcer prevention and self-care. They were also aware that individuals with incontinence should clean their skin after each elimination and at routine intervals. Respondents also knew that alternating pressure mattresses regulate both tissue pressure and skin microclimate. Most correct answers were obtained for statements such as the need to use high-absorbency incontinence products for individuals with pressure ulcers and incontinence, the likelihood of new ulcers at the scar site, and the increased risk of pressure ulcers in individuals with diabetes.
The response to the statement that ring cushions help prevent pressure ulcers surprised us. Most respondents incorrectly answered this, and just over half of the respondents provided a wrong answer to the statement that massaging bony prominences is necessary for quality skin care. Similarly, more than half of the respondents gave an incorrect answer to the statement that individuals with limited mobility who are capable should be instructed to shift their weight while sitting every 30 minutes (Table 6).
7.5 Knowledge of materials/equipment for care and prevention of pressure ulcers
The vast majority of respondents correctly answered that a nurse must ensure the proper operation of specialized beds and document this. Most also gave the correct response that pain-relieving agents help manage acute pain in pressure ulcers. Respondents were aware that patients using alternating pressure mattresses are less exposed to the risk of shear forces and that the head of the bed should not be elevated more than 30 degrees in pressure ulcer prevention. They also knew that overweight patients require appropriately sized equipment that can help prevent pressure ulcers (Table 7).
Statement
Answer n (%)
Do not know
Wrong
Correct
Foam dressings can increase pain in the wound. (N)
17 (14.80)
18 (17.40)
80 (67.80)
Hydrogel dressings should not be used on pressure ulcers with granulation tissue. (N)
28 (24.3)
30 (26.1)
57 (49.6)
Individuals with pressure ulcers and incontinence should use high-absorbency incontinence products. (P)
8 (7.0)
6 (5.2)
101 (87.8)
An anti-decubitus cushion regulates tissue load and skin microclimate. (P)
2 (1.7)
6 (5.2)
107 (93.0)
Ring-shaped cushions help prevent pressure ulcers. (N)
11(9.6)
85 (73.9)
19 (16.5)
The nurse’s responsibility is to ensure that the specialized bed functions correctly and record its usage. (P)
10 (8.7)
7 (6.1)
98 (85.2)
Critically ill patients may require slow, gradual turning as they are hemodynamically unstable. (P)
17 (14.8)
15 (13.0)
83 (72.2)
In immobile patients whose feet do not reach the floor, a footstool should not be used. (N)
32 (27.8)
15 (13.0)
68 (59.1)
Local opioids can help manage acute pain in pressure ulcers. (P)
18 (15.7)
30 (26.1)
67 (58.3)
Biofilm on a wound is associated with reduced wound exudate. (N)
35 (30.4)
28 (33.0)
42 (36.5)
Massaging bony prominences is essential for quality skin care. (N)
12 (10.4)
52 (45.2)
51 (44.3)
In individuals with incontinence, the skin should be cleaned after elimination and at routine intervals. (P)
3 (2.6)
3 (2.3)
109 (94.8)
Immobile individuals who can be taught should shift their weight while sitting in a chair every 30 minutes. (P)
11 (9.6)
79 (68.7)
25 (21.7)
The selection of an anti-decubitus cushion considers the risk level for pressure ulcer development in a specific person. (N)
5 (4.3)
92 (80.0)
18 (15.7)
A patient using an anti-decubitus cushion is not at risk for shear force injuries. (N)
3 (2.6)
18 (15.7)
94 (81.7)
To prevent pressure ulcers, the bed’s headrest must be elevated at an angle greater than 45 degrees. (N)
16 (13.9)
17 (14.8)
82 (71.3)
The urinary catheter tube should be positioned under the leg. (N)
9 (7.8)
14 (12.2)
92 (80.0)
Properly sized equipment can help prevent pressure ulcers in bariatric patients. (P)
37 (32.2)
3 (2.6)
75 (65.2)
Nurses should avoid turning the patient onto a reddened area. (P)
6 (5.2)
19 (16.5)
90 (78.2)
A person with a spinal cord injury has a lifelong risk of pressure ulcers. (P)
6 (5.2)
7 (6.1)
102 (88.7)
Table 7.
Knowledge of materials/equipment for care and prevention of pressure ulcers (n = 115).
Legend: n = number, % = percent, P = positive, the statement is correct, N = negative, the statement is wrong.
The majority of incorrect answers were provided in response to the statement that the level of risk for pressure ulcer development in a specific individual should be considered when using an alternating pressure mattress. Additionally, one-third of the respondents did not know that foam dressings do not increase pain at the wound site. Nearly the same percentage of respondents did not realize that a footrest should not be used for immobile patients whose feet do not reach the ground.
7.6 Knowledge of modern approaches in pressure ulcer care
The majority of respondents are aware that pressure ulcers are not sterile wounds. They also know that dressings should keep the wound bed moist while keeping the surrounding area dry. They understand that it is necessary to assess the pain intensity in individuals with pressure ulcers and that a nutritional assessment is needed for such patients. Respondents are also aware that hydrocolloid and film dressings should not be removed quickly, and they know that the goal of palliative care is not wound healing.
However, more than half of the respondents incorrectly believe that wound healing often slows down in the proliferative phase of chronic wounds. They are also unaware that hydrogel dressings can be used for pressure ulcers with granulation tissue, that biofilm on a wound is not associated with reduced wound exudate, and that pressure ulcers can be cleansed with drinking water (Table 8).
Statement
Answer n (%)
Do not know
Wrong
Correct
Alkaline soaps are used for wound cleaning. (P)
28 (24.30)
34 (6.10)
53 (46.10)
Hydrogel dressings should not be used on pressure ulcers with granulation tissue. (N)
28 (26.1)
30 (26.1)
57 (49.6)
Pain intensity should be assessed in individuals with pressure ulcers. (P)
7 (6.1)
10 (8.7)
98 (85.2)
Sterile dressings can be used to protect the skin. (N)
6 (5.2)
47 (40.9)
62 (53.9)
A nutritional assessment should be performed in individuals at risk of pressure ulcers. (P)
11 (9.6)
10 (8.7)
94 (81.7)
Biofilms can develop on any type of wound. (P)
28 (24.3)
28 (24.3)
59 (51.3)
Critically ill patients may require slow, gradual turning due to hemodynamic instability. (P)
17 (14.8)
15 (13.0)
83 (72.2)
Local opioids can help manage acute pain in pressure ulcers. (P)
18 (15.7)
30 (26.1)
67 (58.3)
Biofilm on a wound is associated with reduced wound exudate. (N)
35 (30.4)
28 (33.0)
42 (36.5)
Healing in chronic wounds is often slowed in the proliferative phase of healing. (N)
23 (20.0)
70 (60.9)
22 (19.1)
To heal a heel wound, a dry, adherent crust should be removed. (N)
12 (10.4)
38 (33.0)
65 (56.5)
In large and deep pressure ulcers, the number of dressings used should be counted and documented so that all dressings are removed during the next change. (P)
10 (8.7)
18 (15.7)
87 (75.7)
Dressings should keep the wound bed moist and the surrounding area dry. (P)
15 (13.0)
9 (7.8)
91 (79.1)
Hydrocolloid and film dressings should be removed quickly to reduce pain. (N)
6 (5.2)
19 (16.5)
90 (78.3)
Hydrocolloid dressings should be used on infected stage 2 pressure ulcers. (N)
37 (32.2)
34 (29.6)
44 (38.3)
Pressure ulcers should not be cleaned with drinking water. (N)
11 (9.6)
51 (44.3)
53 (46.1)
Alginates can be used for stage 3 and 4 pressure ulcers with moderate exudate. (P)
28 (24.3)
7 (6.1)
80 (69.9)
Table 8.
Knowledge of modern approaches in pressure ulcer care (n = 115).
Legend: n = number, % = percent, P = positive, the statement is correct, N = negative, the statement is wrong.
In this research, we assessed the knowledge of healthcare professionals in hospital nursing through a questionnaire. Overall, the knowledge of the participants regarding the prevention and care of pressure ulcers in hospitalized patients is considered acceptable.
We found that over half of the respondents scored above 60% of correct answers, thus successfully passing the test. Similar results have been reported in other studies employing the same questionnaire. For instance, in the study conducted by Foolbrook et al. [14], a total of 65% correct answers were achieved, while Miller et al. [19] reported a score of 72%. Researchers believe that this percentage represents satisfactory knowledge, considering the comprehensive nature of the questionnaire used.
In our study, we identified a correlation between the length of work experience and the knowledge of healthcare professionals. In contrast, a study conducted in Ireland by Eskes et al. [20] argues that long-term experience alone is not a guarantee of knowledge; rather, it requires support from healthcare policymakers, educational organizations, and employees themselves through knowledge exchange in clinical settings. Like our study, Barakat-Johnson et al. [21], Tirgari et al. [22], and Li et al. [23] suggest that respondents with several years of experience own more knowledge. Furthermore, Parisod et al. [24] report that respondents with extensive work experience not only showed better knowledge but also displayed a more positive attitude toward pressure ulcer prevention and self-evaluation, which can be used to identify individuals in the work environment who require additional training. On the opposite, Miller et al. [19] found that younger nurses with less work experience had more knowledge about wound stages.
In our research, we also saw a correlation between the level of education and the knowledge of the respondents regarding pressure ulcers. Similar conclusions have been drawn by Ebi et al. [25] and De Mayer et al. [26], who linked the level of education with knowledge about pressure ulcers. Ilesanmi et al. [27] in their study in Nigeria and Nuru et al. [28] in Ethiopia found that the knowledge of healthcare staff with higher education, additional training, and more years of work experience is better. Similarly, Fulbrook et al. [14] and Al-Shidi [29] observed that more experienced and highly educated nurses had more knowledge about pressure ulcers than others. But here we find an important finding—the lowest score on the test was from university-educated nurses. It could be the consequence of the educational system as in Slovenia we do not have a university level study for nursing, so the nurses are forced to study other sciences such as economics, management, or others. McCluskey and McCarthy [30] emphasize the importance of informal knowledge sources, which include experiential learning and intuition in pressure ulcer care. Fulbrook et al. [14] found that over half of the respondents had sought education and information about pressure ulcers online. Sengul and Karadag [31] also noted a higher level of knowledge among nurses in Turkey who regularly read literature on pressure ulcer prevention. Similar findings were reported by Gonzaga de Faria et al. [32] and Ferreira et al. [33]. They not only observed the use of informal knowledge sources but also identified a lack of protocol or guideline utilization in the clinical setting. They found that while theoretical knowledge was satisfactory, staff often struggled to apply it in practice.
The data obtained in our research indicates that most respondents lack specialized knowledge in pressure ulcer care. We found that nearly one-third of the respondents had never attended any seminars, and an equal proportion had not read any literature on pressure ulcers in the past year. While Sever and Bregar [34] noted that nursing students are already aware of the need for specialization due to new technologies, new knowledge, an increasing number of patients with chronic illnesses, longer life expectancies, a burdened healthcare system, and growing healthcare service demands, the survey results are somewhat surprising. Continuous knowledge enhancement and the development of evidence-based healthcare are essential for maintaining the quality and advancing the nursing profession. This responsibility applies to every healthcare professional [35, 36].
Based on the findings, we can conclude that healthcare professionals are well-versed in stages 1 and 2 of pressure ulcers but less so in stages 3 and 4. The issue may stem from the confusion between pressure ulcer stages and the assessment of a patient’s risk for developing pressure ulcers, which are not equivalent. Also, Gul et al. [37], similar to Cox and Roche [38], discovered a knowledge deficit among nurses, particularly concerning wound classification. Fulbrook et al. [14] similarly found that among Australian nurses, their weakest area of knowledge was in wound descriptions. Ferreira et al. [33] identified knowledge deficiencies in various aspects of wound care, such as the accurate classification of pressure ulcers by stages, unfamiliarity with clinical guidelines and protocols in specific clinical settings, and improper choice of dressings, among other issues. We can infer that healthcare personnel partly use wound classification in their work and attempt to assess the stage of wounds, but struggle with recognizing stages 3 and 4 of pressure ulcers.
With the third research question, we assessed knowledge about pressure ulcer prevention. We were surprised to find that over half of the respondents incorrectly believed that ring-shaped cushions help prevent pressure ulcers and that massaging bony prominences is necessary for quality skin care. In Australia, Fulbrook et al. [14] also obtained a high percentage of incorrect answers related to the use of doughnut-shaped cushions. Lawrence et al. [39] were also surprised by the responses related to prevention. Incorrect answers from respondents were associated with doughnut-shaped cushions, heel protectors, massaging exposed areas, and the timeframe within which erythema is still reversible. Saleh et al. [40] and Gedamu et al. [41] reported unsatisfactory knowledge of pressure ulcer prevention and treatment. Beeckman et al. [42] reported that 70% of nurses mentioned regular skin observation as a common practice in the presence of erythema in patients at high risk of pressure ulcers. Respondents had a good understanding of when to perform anogenital care, which incontinence products to use, the appropriate intervals for repositioning patients, and similar aspects. We presume that in our research, healthcare professionals may not have been informed about the latest guidelines and recommendations.
The analysis of the fifth research question focused on the use of a modern approach in pressure ulcer care. A significant proportion of our respondents correctly answered that dressings should keep the wound bed moist and the peri-wound area dry, that assessing pain intensity is necessary, and that a nutritional assessment of the patient should be conducted. However, most respondents did not know that wound healing does not slow down in the proliferative phase of healing, that biofilm on a wound is not associated with reduced wound exudate, and that pressure ulcers can be cleaned with drinking water. Sharp et al. [43] found that nursing staff were knowledgeable about and used modern dressings for the care of stage 2 and 3 ulcers such as hydrocolloids, foams, and alginates. They also observed that outdated methods, such as iodine preparations, saline solutions, hydrogen peroxide, gauze, and others, were still in use. Gillespie et al. [44] aimed to investigate the practice of nurses in wound care in an Australian hospital. In their survey, 75.6% of respondents reported that the appearance of the wound was the most crucial factor in choosing a suitable dressing. Almost half of the respondents did not consider national standards for chronic wound care in their work. Therefore, the authors concluded that although hospital nurses were well-versed in wound healing processes, they did not use recommended clinical guidelines for wound care in their practice.
The research had some limitations. Some respondents wrote down primary education in the questionnaire, which was either an intentional or unintentional error. These questionnaires had to be excluded from the study before the analysis. The sample size was small, so the results cannot be generalized. The questionnaire, in our opinion and according to the respondents, was somewhat lengthy, and the concentration of respondents waned during completion. The questions were not logically sequenced, and they were intermingled, which could have contributed to the study’s suboptimal results. It appears that the questionnaire might have been too demanding, and it should be revised and adapted to our specific context in the future. Further, research is called for, potentially involving a modified questionnaire, to ease meaningful comparisons with the questionnaire authors’ results.
The results indicate that participants had varying levels of knowledge about pressure ulcers, their prevention, and care. While many participants proved good knowledge in some areas, there were gaps in their understanding in other areas. The findings highlight areas, where there is room for improvement in educating healthcare professionals or individuals about pressure ulcers and their management. These insights can be used to design more targeted training programs or materials. It is necessary to implement a comprehensive approach to elevate the knowledge, attitudes, and practices of healthcare staff with the goal of enhancing the quality of patient care. Emphasizing the importance of continuous knowledge and practice enhancement for nurses is imperative.
References
1.Haesler E, editor. Prevention and Treatment of Pressure Ulcers: Quick Reference Guide. Perth, Australia: National Pressure Ulcer Advisory Panel, European Pressure Ulcer Advisory Panel and Pan Pacific Pressure Injury Alliance; 2014
2.Alderden J, Rondinelli J, Pepper G, Cummins M, Whitney J. Risk factors for pressure injuries among critical care patients: A systematic review. International Journal of Nursing Studies. 2017;71:97-114. DOI: 10.1016/j.ijnurstu.2017.03.012
3.Moore ZE, Cowman S. Repositioning for treating pressure ulcers. Cochrane Database of Systematic Reviews. 2015;1:1. DOI: 10.1002/14651858.CD006898
4.Boyko TV, Longaker MT, Yang GP. Review of the current management of pressure ulcers. Advances in Wound Care. 2018;7(2):57-67. DOI: 10.1089/wound.2016.0697
5.Perko D. Razjede zaradi pritiska. In: Perko VD, Borovničar A, editors. Kazalniki kakovosti v zdravstvu, Letno poročilo za leto 2019. Ljubljana: Nacionalni inštitut za javno zdravje, Ministrstvo za zdravje Republike Slovenije; 2019. pp. 20-21. Available from: https://www.gov.si/assets/ministrstva/MZ/DOKUMENTI/staro/1-PODROCJA-ZDRAVJE/1-Kakovost-varnost-in-dostopnost-zdravstvenega-varstva/1-Kakovost-zdravstvenega-varstva/Kazalniki-kakovosti-v-zdravstvu-2019.pdf
6.Yavuz A, Çakmak M. Razjeda/poškodba zaradi pritiska. In: Hudin VD, editor. Sodobna oskrba kroničnih ran. Ljubljana: Srednja zdravstvena šola; 2020. pp. 45-63. Available from: http://szslj.splet.arnes.si/files/delightful-downloads/2020/11/SODOBNA-OSKRBA-KRONI%C4%8CNIH-RAN-PRIRO%C4%8CNIK.pdf [Accessed: December 09, 2022]
7.Tomc D. Razjeda zaradi pritiska – preventiva in oskrba. In: Straus VKK, editor. Usmerjeni v stroko zdravstvene nege in oskrbe – usmerjeni v potrebe bolnikov: zbornik predavanj z recenzijo, Zreče 29.-30. marec 2019. Ljubljana: Zbornica zdravstvene in babiške nege Slovenije – Zveza strokovnih društev medicinskih sester, babic in zdravstvenih tehnikov Slovenije, Strokovna sekcija medicinskih sester in zdravstvenih tehnikov v socialnih zavodih; 2019. pp. 11-24
8.Fatur M. Preprečevanje razjede zaradi pritiska pri osebah s paraplegijo (diplomska naloga). Ljubljana: Univerza v Ljubljani; 2020
9.Šáteková L, Žiaková K, Zeleníková R. Predictive validity of the Braden scale, Norton scale and Waterlow scale in Slovak Republic. Central Europenal Jurnal Nursing and Midwifery. 2015;6(3):283-290. DOI: 10.1111/ijn.12499
10.Edsberg LE, Black JM, Goldberg M, McNichol L, Moore L, Sieggreen M. Revised national pressure ulcer advisory panel pressure injury staging system: Revised pressure injury staging system. Journal of Wound, Ostomy, and Continence Nursing. 2016;43(6):585
11.Simonič S. Majhni koraki-veliki prihranki: vloga medicinske sestreza preventivo razjede zaradi pritiskana oddelku intenzivne terapije. In: Doberšek VD, Kočevar R, Perko AN, Peternelj K, editors. Anesteziologija, intenzivna terapija, transfuziologija: skupaj za pacienta: zbornik predavanj z recenzijo, Rogaška Slatina, 1.in 2. april.2016. Ljubljana: Zbornica zdravstvene in babiške Slovenije - Zveza strokovnih društev medicinskih sester, babic in zdravstvenih tehnikov Slovenije, Sekcija medicinskih sester in zdravstvenih tehnikov v anesteziologiji, intenzivni terapiji in transfuziologiji; 2016. pp. 35-39
12.Moore ZE, Patton D. Risk assessment tools for the prevention of pressure ulcers. The Cochrane Database of Systematic Reviews. 2019;1(1):CD006471. DOI: 10.1002/14651858.CD006471.pub4
13.Gaballah S, El-Deen DS. Pressure injury care program effects on nurses’ performance and patients’ pressure injury wound healing outcomes. American Journal of Nursing Research. 2021;9(3):76-84. DOI: 10.12691/ajnr-9-3-2
14.Fulbrook P, Lawrence P, Miles S. Australian nurses' knowledge of pressure injury prevention and management: A cross-sectional survey. Journal of Wound, Ostomy, and Continence Nursing. 2019;46(2):106-112. DOI: 10.1097/WON.0000000000000508
15.Soban LM, Kim L, Yuan AH, Miltner RS. Organisational strategies to implement hospital pressure ulcer prevention programmes: Findings from a national survey. Journal of Nursing Management. 2017;25(6):457-467. DOI: 10.1111/jonm.12416
16.Fernandes C, Lima A, Santos M. Pressure injury prevention: Attitudes and knowledge of nursing students. Journal of Nursing & Healthcare. 2021;11(3):e2111320924. Available from: https://periodicos.ufpel.edu.br/ojs2/index.php/enfermagem/article/view/20924
17.Pieper B, Zulkowski K. The Pieper-Zulkowski pressure ulcer knowledge test. Advances in Skin & Wound Care. 2014;27(9):413-420. DOI: 10.1097/01.ASW.0000453210.21330.00
18.Official Gazette of the Republic of Slovenia. Uradni list RS. št.71/2014 (29.3.2014). 2014. Available from: https://www.uradni-list.si/glasilo-uradni-list-rs/vsebina/2014-01-2937/kodeks-etike-v-zdravstveni-negi-in-oskrbi-slovenije
19.Miller DM, Neelon L, Kish-Smith K, Whitney L, Burant CJ. Pressure injury knowledge in critical care nurses. Journal of Wound Ostomy & Continence Nursing. 2017;44(5):455-457. DOI: 10.1097/WON.0000000000000350
20.Eskes AM, Maaskant JM, Holloway S, van Dijk N, Alves P, Legemate DA, et al. Competencies of specialised wound care nurses: A European Delphi study. International Wound Journal. 2014;11(6):665-674. DOI: 10.1111/iwj.12027
21.Barakat-Johnson M, Barnett C, Wand T, White K. Knowledge and attitudes of nurses toward pressure injury prevention. Journal of Wound, Ostomy and Continence Nursing. 2018;45(3):233-237. DOI: 10.1097/WON.0000000000000430
22.Tirgari B, Mirshekari L, Forouzi MA. Pressure injury prevention: Knowledge and attitudes of Iranian intensive care nurses. Advances in Skin & Wound Care. 2018;31(4):1-8. DOI: 10.1097/01.ASW.0000530848.50085.ef
23.Li Z, Zhou X, Cao J, Li Z, Wan X, Li J, et al. Nurses’ knowledge and attitudes regarding major immobility complications among bedridden patients: A prospective multicentre study. Journal of Clinical Nursing. 2018;27(9-10):1969-1980. DOI: 10.1111/jocn.14339
24.Parisod H, Holopainen A, Koivunen M, Puukka P, Haavisto E. Factors determining nurses’ knowledge of evidence-based pressure ulcer prevention practices in Finland: A correlational cross-sectional study. Scandinavian Journal of Caring Sciences. 2022;36(1):150-161. DOI: 10.1111/scs.12972
25.Ebi WE, Hirko GF, in Mijena, D. A. Nurses’ knowledge to pressure ulcer prevention in public hospitals in Wollega: A cross-sectional study design. BMC Nursing. 2019;18(1):1-12. DOI: 10.1186/s12912-019-0346-y
26.De Meyer D, Verhaeghe S, Van Hecke A, Beeckman D. Knowledge of nurses and nursing assistants about pressure ulcer prevention: A survey in 16 Belgian hospitals using the PUKAT 2.0 tool. Journal of Tissue Viability. 2019;28(2):59-69. DOI: 10.1016/j.jtv.2019.03.002
27.Ilesanmi RE, Ofi BA, Adejumo PO. Nurses' knowledge of pressure ulcer prevention in Ogun state, Nigeria: Results of a pilot survey . Ostomy/Wound Management. 2012;58(2):24-32
28.Nuru N, Zewdu F, Amsalu S, in Mehretie, Y. Knowledge and practice of nurses towards prevention of pressure ulcer and associated factors in Gondar University Hospital, Northwest Ethiopia. BMC Nursing. 2015;14(1):1-8. DOI: 10.1186/s12912-015-0076-8
29.Al Shidi AS. Pressure ulcer management in Oman: Nurses’ knowledge and views [doctoral thesis]. Glasgow: University of Glasgow; 2016. Available from: https://theses.gla.ac.uk/7635/
30.Mccluskey P, Mccarthy G. Nurses'knowledge and competence in wound management. Wounds UK. 2012;8(2):37-47
31.Sengul T, Karadag A. Determination of nurses' level of knowledge on the prevention of pressure ulcers: The case of Turkey. Journal of Tissue Viability. 2020;29(4):337-341. DOI: 10.1016/j.jtv.2020.06.005
32.De Faria G, Begido G, Prado TN. Knowledge and practice of nurses on the care of wounds. Journal of Nursing UFPE/Revista de Enfermagem UFPE. 2016;10(12):4532-4538. DOI: 10.5205/reuol.9978-88449-6-ED1012201614
33.Ferreira AM, Rigotti MA, da Silva Barcelos L, Simão CMF, Ferreira DN, Gonçalves RQ. Knowledge and practice of nurses about care for patients with wounds. Revista de Pesquisa Cuidado é Fundamental Online. 2014;6(3):1178-1190. DOI: 10.9789/2175-5361.2014v6n3p1178
34.Sever M, Bregar B. Specializacije v zdravstveni negi: pogled študentov. Obzornik zdravstvene nege. 2015;49(1). DOI: 10.14528/snr.2015.49.1.49
35.Kadivec S, Skela Savič B, Kramar Z, Zavrl Džananović D, Bregar B. Strategija razvoja zdravstvene nege in oskrbe v sistemu zdravstvenega varstva v republiki Sloveniji za obdobje od 2011 do 2020: povzetek. Slovenian Nursing Review. 2013;47(1):97-112
36.Kramar Z. Kakovost in varnost v zdravstvu: priročnik. Ljubljana: Zbornica zdravstvene in babiške nege Slovenije - Zveza strokovnih društev medicinskih sester, babic in zdravstvenih tehnikov Slovenije. 2022. Available from: https://www.zbornica-zveza.si/wp-content/uploads/2022/03/Kakovost-in-varnost-v-zdravstvu_prirocnik.pdf [Accessed: February 04, 2023]
37.Gul A, Andsoy II, Ozkaya B, Zeydan A. A descriptive, cross-sectional survey of Turkish nurses’ knowledge of pressure ulcer risk, prevention, and staging. Ostomy/Wound Management. 2017;63(6):40-46
38.Cox J, Edsberg LE, Koloms K, VanGilder CA. Pressure injuries in critical care patients in US hospitals: Results of the international pressure ulcer prevalence survey. Journal of Wound, Ostomy, and Continence Nursing: Official Publication of The Wound, Ostomy and Continence Nurses Society. 2022;49(1):21-28
39.Lawrence P, Fulbrook P, in Miles, S. A survey of Australian nurses' knowledge of pressure injury/pressure ulcer management. Journal of Wound, Ostomy and Continence Nursing. 2015;42(5):450-460. DOI: 10.1097/WON.0000000000000141
40.Saleh MYN, Papanikolaou P, Nassar OS, Shahin A, Anthony D. Nurses' knowledge and practice of pressure ulcer prevention and treatment: An observational study. Journal of Tissue Viability. 2019;28(4):210-217. DOI: 10.1016/j.jtv.2019.10.005
41.Gedamu H, Abate T, Ayalew E, Tegenaw A, Birhanu M, in Tafere, Y. Level of nurses’ knowledge on pressure ulcer prevention: A systematic review and meta-analysis study in Ethiopia. Heliyon. 2021;7(7):e07648. DOI: 10.1016/j.heliyon.2021.e07648
42.Manderlier B, Van Damme N, Verhaeghe S, Van Hecke A, Everink I, Halfens R, et al. Modifiable patient-related factors associated with pressure ulcers on the sacrum and heels: Secondary data analyses. Journal of Advanced Nursing. 2019;75(11):2773-2785. DOI: 10.1111/jan.14149
43.Sharp C, Burr G, Broadbent M, Cummins M, Casey H, Merriman A. Pressure ulcer prevention and care: A survey of current practice. Journal of Quality in Clinical Practice. 2000;20(4):150-157. DOI: 10.1046/j.1440-1762.2000.00384.x
44.Gillespie BM, Chaboyer W, Allen P, Morely N, Nieuwenhoven P. Wound care practices: A survey of acute care nurses. Journal of Clinical Nursing. 2014;23(17-18):2618-2627. DOI: 10.1111/jocn.12479
Written By
Melita Peršolja and Rosanda Drufovka
Submitted: 30 October 2023Reviewed: 08 November 2023Published: 14 February 2024