
ICIs in patients with chemotherapy-refractory mCRC.
Abstract
Metastatic colorectal cancer is a major health problem, accounting for 8.1% of US cancer cases. Although 5-FU-oxaliplatin-irinotecan-based chemotherapy combination regimens and targeted therapies have increased 5-year survival rates to around 13%. The still low rate of this rate increases the demand for new treatment options. Advances in the discovery of tumor biology have made it possible to better define the subtypes and resistance mechanisms of metastatic colorectal cancer. In this regard, personalized treatment strategies are becoming increasingly important in the treatment of advanced stages of metastatic colorectal cancer. New therapeutic options, immune checkpoint inhibitors, monoclonal antibodies against various targets, and multitargeted tyrosine kinase inhibitors are available in the treatment of later lines of metastatic colorectal cancer. The treatment strategy is based on patients’ performance status, residual toxicity, and especially molecular profile.
Keywords
- treatment
- metastatic colorectal cancer
- beyond progression
- immunotherapy
- rechallenge
- monoclonal antibody
1. Introduction
Metastatic colorectal cancer (mCRC) is the third most common cause of newly diagnosed cancer and the second most common cause of cancer-related death in both sexes [1]. Approximately, 8.1% of newly diagnosed cancer cases in the United States are colorectal cancers. At the time of diagnosis, approximately, 21% of patients are diagnosed in the metastatic stage. As systemic treatment options, 5 fluorouracil (5-FU)-based chemotherapy combination regimens with monoclonal antibodies, multitargeted kinase inhibitors alone, and immunotherapy agents are important treatment arguments. With these treatment options, 5-year survival rates in patients with metastatic colorectal cancer have improved significantly, reaching approximately 13% [2]. In addition, according to the surveillance epidemiology and end results (SEER) medicare database analysis for mCRC, the increase in treatment lines correlates with an increase in overall survival times (Figure 1) [3]. In other words, in unresectable mCRC patients who exhausted the first two lines of treatment options, overall survival (OS) durations of 23–24 months are known to increase with the drugs used after beyond progression, with a significant additional contribution to overall OS durations. In addition, after the first two treatment lines, approximately, 63.3% of patients at baseline can reach to the third-line setting [4]. Designing the treatment regimen for patients who have progressed to the third-line setting should be acknowledged as the “art of science.” Because the probability rate of clinical benefit with treatment in this patient group is approximately 35.2% [4]. In these patients, comorbidity and performance status, tumor burden, residual toxicity, and most importantly, the current molecular profile of the disease (biomarker analysis) should be considered at beyond progression. Moreover, an investigation into the genomic landscape of this ailment has allowed to therapeutic expansion, encompassing targeted therapies and immunotherapy. Given these considerations, treatment options can be divided into two groups: biomarker-driven therapy or non-biomarker-driven treatment pathways. In this section, treatment standards and especially current approaches will be mentioned, especially in terms of the standard treatment approach, which is limited especially after beyond progression, and an evaluation was made in terms of the current developments in terms of precision medicine.
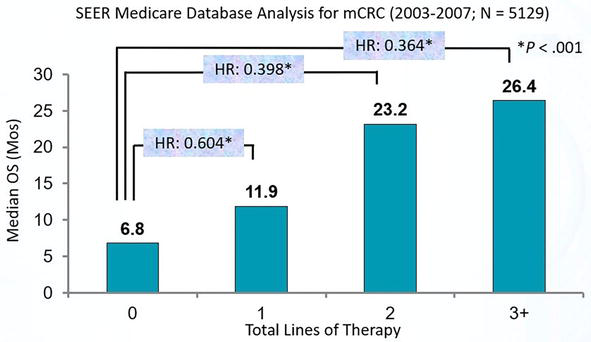
Figure 1.
Overall survival correlated with increased treatment lines.
Advertisement
2. Biomarker—driven treatment options
2.1 dMMR/MSI-H status
Mismatch repair deficient/high microsatellite instability (dMMR/MSI-H) status is recognized as a tumor-agnostic biomarker, demonstrating potential benefits from immunotherapy when identified across all solid cancers. In clinical studies, its prevalence has been reported to be approximately 4–5% in patients with metastatic colorectal cancer [5]. Deficiency in the protein products of the MSH2, PMS-2, MLH1, and MSH6 genes results in an inability to efficiently detect mismatched and unpaired bases, leading to the expression of abnormal proteins that can be recognized by the immune system as neoantigens. It is a poor prognostic marker before the era of immunotherapy and has been particularly associated with resistance to conventional 5-FU-based chemotherapy combinations. These patients may have both sporadic and familial dMMR. In patients with sporadic dMMR, tumor location is more likely to be a proximal colon, high grade, mucinous pathology, diploid, and closely associated with BRaf proto-oncogene (BRAF) V600E mutations. Approximately, one in four patients with dMMR present with familial Lynch syndrome. Sporadic dMMR tumors differ from familial dMMR-Lynch syndrome in terms of female gender, smoking, and younger age at diagnosis. Although individuals with Lynch syndrome typically receive a diagnosis at an age below 45, it is essential to consider the possibility of concurrent or subsequent extra-colonic tumors.
Patients with deficient mismatch repair (dMMR) status are eligible for immunotherapy in any line of therapy. In cases where these patients undergo chemotherapy in the initial two lines and experience disease progression, the subsequent line of therapy is appropriate for immunotherapy treatment. Checkpoint inhibitor treatment options encompass nivolumab ± ipilimumab, pembrolizumab, or dostarlimab-gxly (Table 1).
| Study | Phase | Agent | Line | Outcome |
|---|---|---|---|---|
| Keynote-164 | Phase 2 | Pembrolizumab | ≥ 2 prior lines | ORR: 33% PFS: 2.3 mo OS: 31.4 mo |
| Pembrolizumab | ≥ 1 prior lines | ORR: 33% PFS: 4.1 mo OS: NR | ||
| Checkmate-142 | Phase 2 | Nivolumab | ≥ 2 prior lines | ORR: 35.8% 1-year PFS: 50.4% 1-year OS: 73.4% |
| Nivolumab+Ipilimumab | ≥ 2 prior lines | ORR:65% (CR:13%) PFS: NR OS: NR | ||
| Garnet* | Phase 1 | Dostarlimab | ≥ 2 prior lines | ORR: 43.5% PFS: 8.4 mo OS: NR |
Table 1.
32.1% of study population was mCRC.
The KEYNOTE 164 study conducted a thorough investigation into the efficacy of pembrolizumab among patients diagnosed with mCRC characterized by MSH or dMMR. This patient cohort had undergone at least one series of standard therapy. KEYNOTE-164, a phase 2 study, enrolled a total of 124 participants. Cohort A was stratified based on patients who had undergone one or more sequential treatments, while cohort B was categorized into patients who had received two or more sequential treatments. The objective response rate was 33% (95% CI, 21–46%) for both cohort A and cohort B, and the median duration of response was not reached in either cohort. The median progression-free survival (PFS) was 2.3 months (95% CI, 2.1–8.1) for cohort A and 4.1 months (95% CI, 2.1–18.9) for cohort B. Median overall survival was 31.4 months (95% CI, 21.4 months to not reached) for cohort A and not reached (95% CI, 19.2 months to not reached) for cohort B. The rates of Grade 3–4 side effects were similar in the two groups [6]. The responses obtained with the use of pembrolizumab in MSI-H/dMMR CRC proved that the use of pembrolizumab is appropriate in patients with MSI-H/dMMR CRC, regardless of mutation status and the number of prior lines of therapy. It showed us that we should consider the option of immunotherapy in patients with MSI-H/dMMR CRC who have not received immunotherapy before.
The efficacy of nivolumab was investigated in the CheckMate-142 studies. A phase 2 cohort first published in 2017 investigated the efficacy of nivolumab in patients with dMMR mCRC who had received at least one prior series of standard therapy. Nivolumab was administered IV at a dose of 3 mg/kg every 2 weeks. While complete response could not be achieved, partial response was achieved in 23 patients and stable disease in 28 patients. The objective response rate (ORR) for these patients was 31.1% (95% CI, 20.8–42.9), and 69% of patients achieved disease control for at least 3 months. 1-year PFS was 50% and OS was 73%. ORR was 28.6% in 21 patients with programmed death-ligand 1 (PDL-1) ≥1%, and ORR was 27.7% in 47 patients with PDL-1 < 1%. Grade 3–4 adverse events were observed in 20% patients [7]. These results in patients with dMMR mCRC showed that nivolumab alone had a positive effect on treatment response independent of tumor PD-L1 expression level.
Another cohort within CheckMate-142 investigated the efficacy of nivolumab plus ipilimumab in patients with dMMR mCRC who had received at least one prior series of therapy. In the study of 119 patients, 76% had received two or more series of standard therapy. Patients received nivolumab (3 mg/kg) plus ipilimumab (1 mg/kg) at 3-week intervals (four doses) followed by nivolumab (3 mg/kg) at 2-week intervals. ORR increased from 55% at 13.4 months to 65% at 50.9 months, and disease control rate was 81%. Complete response (CR) rate increased from 3% at 13.4 months to 13% at 50.9 months. Partial response (PR) was observed in 52% of patients, stable disease (SD) in 21%, and progressive disease (PD) in 12%. Adverse events occurred in 32% of patients, and 13% had to discontinue treatment due to adverse events [8]. These results demonstrated the long-term benefit of the combination of nivolumab and ipilimumab in treatment-refractory MSI-H/dMMR mCRC patients.
Dostarlimab is a humanized anti-PD-1 monoclonal antibody that acts by binding to the PD-1 receptor [9]. The efficacy of dostarlimab was first demonstrated in MSI-H metastatic or recurrent endometrial cancer [10]. Next, the efficacy of the GARNET study in the F cohort of non-endometrial solid tumors previously treated with dMMR was demonstrated. Of the 106 patients in this cohort, 69 were diagnosed with CRC. Patients received 500 mg dostarlimab Q3W for four cycles followed by 1000 mg Q6W until progression. The ORR in patients with mCRC was 36.2% (CI 25.0–48.7%) [11]. Based on the outcomes derived from this cohort, dostarlimab has emerged as a viable treatment option for patients with dMMR mCRC who have undergone previous therapeutic options.
Currently, with the dMMR test serving as the primary reflex test, immune checkpoint inhibitor options are employed as the initial treatment for patients in this group. In instances where patients experience progression following IO, they are transitioned to other therapeutic options rather than immunotherapy options.
2.2 Anti-HER-2 treatments
HER-2 (human epidermal growth factor receptor 2) is a transmembrane protein and a member of the human epidermal growth factor receptor family. It acquires oncogenic characteristics through amplification or overexpression, potentially leading to the development of various cancers. One of these cancers is colorectal cancer [12]. It is detected in approximately 2–6% of colorectal cancers [13]. Currently, for patients with chemorefractory HER2-positive and RAS wild-type mCRC, there is evidence supporting the utilization of a dual anti-HER2 regimen. Tucatinib plus trastuzumab regimen has received initial FDA approval for this specific clinical scenario [14]. Furthermore, a combined PFS of 6.2 months indicates that HER2-targeted treatment regimens are linked with a significant enhancement in survival outcomes within this population (Table 2) [15].
| Study | Phase | Agent | Line | Outcome |
|---|---|---|---|---|
| MyPathway | Phase 2 | Trastuzumab+Pertuzumab | ≥ 2 prior lines | ORR: 38% PFS: 4.6 mo OS: 10.3 mo |
| HERACLES-A | Phase 2 | Trastuzumab+Lapatinib | ≥ 2 prior lines | ORR: 30% PFS: 5.3 mo OS: 11.5 mo |
| DESTINY-CRC01 | Phase 2 | Trastuzumab deruxtecan | ≥ 2 prior lines | ORR: 45.3% PFS: 6.3 mo OS: 15.5 mo |
| MOUNTAINEER | Phase 2 | Trastuzumab+Tucatinib | ≥ 2 prior lines | ORR: 52.2% PFS: 8.1 mo OS: 18.7 mo |
Table 2.
Anti-HER-2 treatment trials in patients with chemotherapy-refractory mCRC.
2.2.1 Trastuzumab and pertuzumab
The MyPathway, TAPUR, and TRIUMPH studies have investigated the effectiveness of the combination of trastuzumab and pertuzumab in patients with HER-2 positive mCRC who have undergone multiple lines of treatment. The MyPathway study is a multicenter, open-label, phase 2a, multiple-basket trial. A total of 57 patients were enrolled in the study, with one patient showing a complete response and 17 patients demonstrating partial responses. The ORR was determined to be 32% [95% CI 20–45]. The estimated median PFS was 2.9 months [95% CI 1.4–5.3], and the estimated median OS was 11.5 months [95% CI 7.7 – not estimable (NE)]. Additionally, four patients exhibited a response lasting longer than 12 months [13]. The TAPUR study was a phase 2 basket trial. A total of 28 patients with HER-2 amplification were enrolled in the study. In the ERBB2 amplification cohort, durable clinical benefit (DCB) and ORR were observed in 54 and 25% of patients, respectively. The median PFS and median OS (95% confidence interval) were 17.2 weeks [95% CI 11.1–27.4] and 60.0 weeks [95% CI 32.1 to 102.3], respectively [16]. The TRIUMPH study showed that these patients who had received multiple lines of treatment, the ORR was found to be 35%, and the median PFS was 4 months [17]. The most important observed side effects in these studies include anemia, lymphopenia, and left ventricular dysfunction.
2.2.2 Trastuzumab ve tucatinib
Tucatinib is an orally administered antitumoral agent that exerts its effects by reversibly inhibiting the HER-2 tyrosine kinase inhibition [18]. The MOUNTAINEER study was a global, phase 2 trial that included 117 patients with chemotherapy-resistant, HER2-positive, RAS wild-type, unresectable, or metastatic colorectal cancer. Tucatinib (300 mg orally twice daily) plus intravenous trastuzumab (initial loading dose of 8 mg/kg, followed by 6 mg/kg every 21 days) was administered. Patients were divided into three cohorts. In cohorts A and B, covering 84 patients, the combination of Tucatinib and trastuzumab was given, while in cohort C, tucatinib monotherapy was provided. In cohorts A and B, the overall response rate (ORR) was 38.1% [95% CI 27.7–49.3], with complete response in three patients and partial response in 29 patients. The median duration of response (DOR) was 12.4 months [95% CI 8.5–20.5]. Median progression-free survival (PFS) was 8.2 months [95% CI 4.2–10.3], and median overall survival (OS) was 24.1 months [95% CI 20.3–36.7]. Comparable positive outcomes were not achieved in cohort C [19]. The achievement of a median survival of 2 years in this metastatic patient group resistant to combination therapy can be considered promising for the future.
2.2.3 Trastuzumab deruxtecan (T-DXd)
Trastuzumab deruxtecan, an antibody-drug conjugate (ADC), is formed through the covalent binding of the humanized anti-HER2 IgG1 monoclonal antibody (mAb) and the topoisomerase 1 inhibitor deruxtecan [20]. The efficacy of Trastuzumab deruxtecan in patients with mCRC has been demonstrated through a phase 2 study, DESTINY-CRC01. The study included patients with HER2-positive mCRC who had received at least two prior lines of treatment. The patients were divided into two groups: Group A consisted of 53 patients with HER2-positive, immunohistochemistry (IHC) 3+ or IHC 2+/
2.2.4 Trastuzumab ve lapatinib
Lapatinib, epidermal growth factor receptor (HER1/EGFR/ERBB1) and HER2/ERBB2 inhibition, is a dual-acting oral antitumoral agent [22]. HERACLES, a multicenter, open-label, and phase 2 trial, was conducted to assess the effectiveness of the combination of trastuzumab and lapatinib in patients with mCRC who are KRAS wild-type and HER2 positive. Patients received IV trastuzumab at a loading dose of 4 mg/kg, followed by maintenance doses of 2 mg/kg weekly, along with oral lapatinib at a dose of 1000 mg daily. Out of the 27 patients included in the study, eight achieved an objective response [%30, 95% CI 14–50]; one patient achieved CR [%4, 95% CI 3–11], and seven patients achieved PR [%26, 95% CI 9–43]. SD was observed in 12 patients [%44, 95% CI GA 25–63]. No serious drug-related side effects were detected. The study concluded that the combination of trastuzumab and lapatinib demonstrated antitumoral efficacy in HER2-positive mCRC patients resistant to treatment [23].
2.3 KRAS G12C inhibitors
The KRASG12C mutation is identified in 2–4% of mCRC. The presence of the KRASG12C mutation is associated with a poor response to chemotherapy and an unfavorable prognosis. Selective KRASG12C inhibitors, such as sotorasib and adagrasib, have demonstrated indications of antitumor activity in mCRC. Adagrasib and sotorasib are agents developed against the KRAS G12C mutation. They function by irreversibly binding to the cysteine protein of KRAS G12C, thereby blocking KRAS signaling. This interruption halts cell growth and induces apoptosis [24]. Initially investigated for the treatment of non-small cell lung cancer, the use of these agents has later come to the forefront in the treatment of mCRC patients.
These studies showed that adagrasib and sotorasib, both as monotherapy and in combination, had a positive effect on survival in patients with mCRC with KRAS 12C mutation. Although monotherapies appeared safer in terms of side effect profile, they had a more modest effect in terms of efficacy. In combination with panitumumab and cetuximab, the effects on survival appear to be more significant. In this respect, the guidelines primarily recommend combination therapies.
2.4 Anti-NTRK fusion-positive targets
RK fusions are infrequent but can be targeted mutations found across various cancer types. NTRK gene fusion is less common in CRC compared to other mutations (0.2–1%) [29]. Genetic profiling of 2519 colonic and rectal tumors revealed an approximate prevalence of 0.7% for NTRK-positive CRC [30]. Additionally, NTRK-positive CRC tumors demonstrated very high tumor mutation burden (median 53 mut/MB), microsatellite instability-high (MSI-H, 76%), and an enrichment of concurrent POLE and POLD1 mutations. This information can be valuable in directing molecularly driven treatment strategies, including targeted therapy and immunotherapy, for NTRK-positive CRC patients. Screening for NTRK fusions is recommended for patients with dMMR/MSI-H or high tumor mutational burden (TMB) CRC [30].
Larotrectinib and entrectinib are pan-tropomyosin receptor kinase (TRK) inhibitors that target TRKA, TRKB, and TRKC. These TRKs are encoded by the NTRK genes. The intracellular activation of these kinases normally regulates cell growth and differentiation. However, fusion proteins resulting from DNA damage in NTRK genes lead to uncontrolled cell growth. Larotrectinib and entrectinib inhibit these TRKs, preventing uncontrolled cell growth and differentiation. Importantly, they exhibit these effects in a tumor-agnostic manner, demonstrating efficacy across various types of cancer [31]. Indeed, due to their tumor-agnostic efficacy in targeting NTRK gene fusions, both larotrectinib and entrectinib, have received approval from regulatory bodies, such as the FDA (Food and Drug Administration) and EMA (European Medicines Agency). This approval allows the use of these drugs across various cancer types where NTRK gene fusions are present [32]. In a pooled analysis encompassing 55 patients under investigation for the efficacy of larotrectinib, it was observed that four patients exhibited colorectal cancer. The overall response rate, as determined by independent assessment, was 75% (95% CI, 61–85). At the end of the first year, responses were sustained in 71% of cases, and 55% of patients remained free of progression. Larotrectinib was administered orally at a dosage of 100 mg twice daily, and it was well-tolerated in 93% of patients. Third or fourth-degree AEs occurred in 5% of the patient population [33]. While larotrectinib and entrectinib have gained approval for tumor-agnostic use in solid tumors with NTRK fusion, it is crucial to note that the studies conducted, thus far have included a limited number of patients with mCRC. Consequently, there is a substantial disparity in treatment responses, with larotrectinib showing a 75% response rate compared to entrectinib’s 25%. Given this divergence, it is imperative to conduct studies with larger patient cohorts to better demonstrate the efficacy of these agents in metastatic colorectal cancer. This will contribute to a more comprehensive understanding of their safety and effectiveness in the context of mCRC.
2.5 RET inhibitors
RET (Rearranged during Transfection) is a proto-oncogene that codes for a transmembrane receptor possessing a tyrosine kinase domain. Various alterations, such as mutations or rearrangements, lead to the activation of the kinase function of the receptor [34, 35].
In colorectal cancer, gene rearrangements have been reported in less than 1% of cases. Among these cases, common gene fusions identified in primary CRC tumors include ALK, ROS1, RET, NTRK3, BRAF, and RSPO1. These gene fusions represent a novel paradigm of oncogenic addiction in CRC [36]. Notably, tumors harboring RET fusions are characterized by their location in the right colon, older age at diagnosis, wild-type RAS and BRAF, and predominantly microsatellite instability-high (MSI-H), possibly defining a distinct subtype of colorectal cancer [37]. From a therapeutic perspective, given the highly positive results reported in phase II and III clinical trials for thyroid and lung cancers, there is an expectation that other types of tumors with positive RET status could benefit from anti-RET drugs. However, due to the rarity of such cases, conducting specific clinical trials for each disease is not feasible. Consequently, data regarding the antitumor activity of these drugs are often derived from early trials, emphasizing the need for further research and exploration in a broader range of cancer types with positive RET status. Selpercatinib is a receptor tyrosine kinase (RET) inhibitor. It is approved for use as a tumor agnostic in patients with RET fusion [38]. However, studies showing efficacy in mCRC are limited. Only 10 of the patients included in the phase 1–2 basket study LIBRETTO-001 were diagnosed with CRC. These patients had received at least two series of treatments. The ORR in the CRC group was 20% [95% CI, 2.5–55.6]. No complete response was detected in patients with CRC. The median duration of response for the colon cancer subgroup was 9.4 months [95% CI, 5.6–13.3]. Selpercatinib was used orally at a dose of 160 mg twice daily without interruption in phase 2 of the study [39]. While the use of selpercatinib in solid tumors is approved as tumor-agnostic, the LIBRETTO-001 study revealed that CR could not be achieved in patients with mCRC, and only 20% of patients showed a partial response. This underscores the necessity for studies with larger patient populations, specifically including those with mCRC, to better demonstrate efficacy. Further research in this context is crucial for a comprehensive understanding of the drug’s effectiveness in treating metastatic colorectal cancer.
2.6 Anti-EGFR inhibitors rechallenge or reintroduction
Monoclonal antibodies that target the epidermal growth factor receptor (EGFR), such as cetuximab or panitumumab, represent foundational elements in the therapeutic approach to advanced-stage CRC [40]. As CRC progresses to the second, third, or fourth line of treatment, the overall prognosis for patients tends to worsen, and the available treatment options become more constrained. Additionally, a growing proportion of mCRC patients become ineligible for further cytotoxic chemotherapy, either due to a decline in performance status, severe adverse effects from prior chemotherapy, or personal choices made by the patients. Consequently, depending on the response to initial cytotoxic and anti-EGFR-based therapy, the rechallenge or reintroduction to anti-EGFR treatment emerges as a promising approach in later lines of treatment [41]. The CRICKET study, a prospective single-arm trial designed as a proof of concept, aimed to evaluate the efficacy of rechallenging with cetuximab plus irinotecan as a third-line treatment for patients with RAS and BRAF wild-type mCRC. The study demonstrated that anti-EGFR re-exposure exhibited clinical activity in mCRC cases that had developed acquired resistance to anti-EGFR treatment [42]. Additionally, a single-arm phase II CAVE trial (cetuximab rechallenge plus avelumab) enrolled 77 mCRC patients, concluding that cetuximab plus avelumab are effective treatment strategies with manageable toxicity profiles [43]. Conversely, the prospective CHRONOS trial has recently shown that liquid biopsy-driven rechallenge strategies can be considered feasible, offering potential improvements in clinical management [44]. Another study from a pooled analysis of the TRIBE and TRIBE2 studies investigated the efficacy of third and later-line treatments in subgroups of the study. This study included 1187 mCRC patients. After second progression, 53% of patients were able to receive treatment. In the subgroup analysis of patients with wild-type KRAS, NRAS, and BRAF, the administration of cetuximab or panitumumab as a third-line treatment resulted in a prolonged progression-free survival (PFS) compared to alternative treatments (6.4 vs. 3.9 months, p = 0.02). This finding suggests a potential benefit of using cetuximab or panitumumab in this specific patient subgroup [45]. Upon analysis of data from the CHRONOS, CRICKET, and TRIBE trials, it was observed that patients had undergone chemotherapy ± bevacizumab for a minimum of 4 months or longer in either the second series or in the previous series. This extended exposure to chemotherapy and bevacizumab may contribute to a reduction in the tumor population, potentially diminishing the presence of anti-EGFR resistance, thereby enhancing the efficacy of rechallenge with cetuximab or panitumumab in this patient group. Notably, the CHRONOS study demonstrated that the clearance of the RAS mutant allele, as determined by liquid biopsy, was similarly achieved within a 4-month as well [44]. Hence, it is noteworthy that within this patient population, a disease control rate of 63% was achieved, and there was evidence of prolongation in PFS [42, 44, 45]. Despite promising efficacy observed in prospective studies, there is a need for phase 3 trials conducted on a larger population to further validate these findings. Large-scale and well-designed phase 3 studies will provide more robust evidence regarding the effectiveness and safety of the rechallenge strategies in the treatment of metastatic colorectal cancer.
2.7 BRAF/MEK inhibitors
BRAF V600E mutation is observed in about 5–10% in patients with metastatic colorectal cancer, and this rate was found to be 9% in a meta-analysis of 6391 patients [46]. The efficacy of agents, such as encorafenib and vemurafenib, which are utilized in the treatment of other cancers, has been investigated in the management of metastatic colorectal cancer.
2.7.1 Vemurafenib
Vemurafenib is a competitive kinase inhibitor that acts against V600E mutated BRAF [47]. Its efficacy in the treatment of mCRC was demonstrated in the SWOG S1406 study, a randomized, phase 2 trial. The study included 106 patients with mCRC who had received at least 1 prior series of treatment. Patients were divided into two groups: irinotecan and cetuximab with or without vemurafenib (960 mg PO twice daily). Median PFS was 4.2 and 2.0 months in the vemurafenib and control arms, respectively. PFS was significantly longer in the vemurafenib arm [95% CI, 0.32–0.76, P = 0.001]. OS was not significantly different between the two arms [(HR, 0.77, 95% CI), 0.50–1.18, P = 0.23]. Response rate and disease control rate were 17% and 65% in the vemurafenib arm compared to 4% and 21% in the control arm [48]. The response rate and PFS duration demonstrated that the combination of vemurafenib with irinotecan and cetuximab is an option for patients with BRAF V600E mutant mCRC who have received multiple lines of therapy.
2.7.2 Encorafenib and cetuximab or panitumumab and/or binimetinib
Encorafenib is a small molecule BRAF inhibitor that targets enzymes in the MAPK signaling pathway [49]. Binimetinib is a potent and selective inhibitor of MEK (Mitogen-Activated Protein Kinase Kinase), and it is administered orally. MEK is a central kinase in the MAPK (Mitogen-Activated Protein Kinase) pathway, which plays a crucial role in promoting tumor growth [50]. The efficacy of the combination of encorafenib and cetuximab or panitumumumab in patients with mCRC was demonstrated in a phase 3 open-label study involving 665 patients. The study included patients with BRAF V600E mutated metastatic colorectal cancer whose disease progressed after one or two standard regimens. Patients were divided into three groups such as encorafenib, binimetinib, and cetuximab (triple therapy group), encorafenib and cetuximab (dual therapy group), and cetuximab and irinotecan or cetuximab and FOLFIRI (folinic acid, fluorouracil and irinotecan) (control group) in a 1:1:1 ratio. The median overall survival was 9.0 months in the triple therapy group and 5.4 months in the control group [HR 0.52; 95%CI, 0.39 to 0.70; P < 0.001]. The response rate was 26% [95% CI, 18–35] in the triple therapy group and 2% [95% CI, 0–7, P < 0.001] in the control group. The median overall survival in the dual treatment group was 8.4 months [HR vs. control, 0.60; 95% CI, 0.45 to 0.79; P < 0.001]. The response rate in the dual treatment group was 22% [95% CI, 14–33]. Grade 3 or higher adverse events occurred in 58% of patients in the triple treatment group, 50% in the dual treatment group, and 61% in the control group [51]. Adverse events were seen in more than 50%, but less frequently than in the standard arm. The combination of encorafenib and cetuximab, in particular the combination of encorafenib, cetuximab, and binimetinib, resulted in significantly longer overall survival and a higher response rate compared to standard therapy in previously treated patients with BRAF V600E mutation. This strengthens clinicians’ hand for the future as an important weapon in mCRC patients with BRAF V600E mutation.
2.8 Tumor mutation burden or POLE mutations
Tumor mutational burden (TMB) quantifies the cumulative somatic coding mutations within a specific coding region of the tumor genome and is assessable through Next-generation sequencing (NGS) techniques. Extensive research has identified TMB as a potential biomarker indicative of immunotherapy response. Pembrolizumab has received FDA approval for patients with unresectable or metastatic solid tumors exhibiting high TMB (TMB-H), defined as 10 or more mutations/megabase by an FDA-approved test, who have progressed post-prior treatment with no satisfactory alternative options. The approval stems from the phase 2 study, KEYNOTE-158, involving patients with advanced solid tumors. In this study, those with TMB-H tumors treated with pembrolizumab demonstrated an ORR of 29%, contrasting with 6% in non-TMB-H tumors. A report from the phase II TAPUR basket study, focusing on 27 patients with TMB-H advanced CRC treated with pembrolizumab, noted one partial response and seven cases with stable disease for at least 16 weeks, resulting in a disease control rate of 28% and an ORR of 4%. Another TAPUR study abstract, covering 12 patients with TMB-H advanced CRC treated with nivolumab plus ipilimumab, concluded that this combination therapy lacks sufficient clinical activity in microsatellite stable, TMB-H CRC [52, 53, 54]. Although TMB-H demonstrated therapeutic significance in the KEYNOTE 158 study, some studies also showed that a TMB-H cutoff value of ≥10 for patients with MSS CRC was not associated with clinically meaningful response to immunotherapy.
Patients with colorectal cancer harboring POLE mutations exhibit distinctive clinical characteristics, including a younger age at diagnosis, a higher proportion of males compared to females, diagnosis at earlier stages, and a noteworthy increase in tumor mutation burden [55]. Furthermore, in the GARNET trial, a limited number of patients with POLE mutations were observed, with the majority of these cases being gastrointestinal cancers. Notably, dostarlimab treatment demonstrated a promising response in this specific population. Patients with microsatellite stable CRC carrying POLE or POLD-1 mutations may exhibit an increased likelihood of benefiting from immunotherapy.
Advertisement
3. Non-targeted therapies
3.1 Chemotherapy rechallenge or reintroduction
Chemotherapy rechallange therapy can be defined as the readministration of a treatment that was previously used but discontinued due to reasons such as toxicity, patient choice, and especially disease progression, after receiving at least one different treatment regimen. Reintroduction is defined as using the same treatment regimen again after discontinuation of treatment without previous disease progression. It is frequently preferred by clinicians, especially in patients receiving multiple serial treatments and in cases where accessible treatment options are reduced. Its efficacy in mCRC has been discussed for a long time. Many studies with positive results have been published [42, 56, 57]. Careful selection of patients, especially when choosing the rechallenge approach in the third step, should take into account their disease burden and residual toxicity. There are many studies showing clinical benefit in appropriate patients [58]. There are also small group studies showing increased efficacy of chemotherapy rechallenge after regorafenib [59]. Briefly, rechallange strategy may be an important treatment option in patients eligible for standard chemotherapy when treatment options are limited, taking into account performance status, previous treatment response, and especially residual toxicities.
3.2 Regorafenib
Regorafenib (BAY 73–4506) is an orally available small-molecule multikinase inhibitor. It inhibits angiogenic kinases (VEGFR1–2-3, platelet-derived growth factor receptor α (PDGFRα) and fibroblast growth factor receptor 1 (FGFR-1)) and mutant oncogenic kinases KIT, RET, and BRAF. It shows antitumoral effect through these mechanisms [60]. The effect of regorafenib on mCRC was first demonstrated in the CORRECT study, an international, multicenter, phase 3 trial. Patients with mCRC who had progression during or within 3 months of the last standard treatment were randomized. A total of 74% of patients received 3 or more serial treatments. Median overall survival was 6.4 months (IQR 3.6–11.8) in the regorafenib group and 5.0 months (IQR 2.8–10.4) in the placebo group. The HR for overall survival was 0.77 [95% CI 0.64–0.94; p = 0.0052]. Median PFS was 1.9 months in the regorafenib group (IQR 1.6–3.9) and 1.7 months in the placebo group (1.4–1.9). The HR for PFS was 0.49 [95% CI 0–42–0-58; p < 0.0001] for regorafenib vs. placebo [61]. After regorafenib entered daily routine use, studies showing real-life data were conducted. In one of the most important of these studies, the CONCUR study, the real-life data and side effect profile of regorafenib in the Asian population were presented in more details. In this study, median overall survival was 8.8 months [95% CI 7.3–9.8] in the regorafenib group and 6.3 months [95% CI 4.8–7.6] in the placebo group. Overall survival was significantly better with regorafenib than with placebo (HR 0.55, [95% CI 0.40–0-77p = 0–00016]). The most common side effects were hand-foot skin reaction (73%), hyperbilirubinemia (36%), alanine aminotransferase concentration and aspartate aminotransferase concentration increased (24%), and hypertension (23%) as well [62].
3.2.1 Trifluridin ve tipirasil hidroklorürden (TAS-102)
Trifluridine (FTD) and tipiracil hydrochloride (TPI), also known as TAS-102, is an oral antimetabolic agent. FTD is a thymidine-based nucleoside analog, which is incorporated into DNA in the form of triphosphate, causing single-strand and double-strand breaks. TPI is a potent thymidine phosphorylase inhibitor. It prevents the rapid degradation of FTD, and thus ensures a sustained high concentration of FTD after oral administration [63]. In 2015, the RECOURSE study, the results of which were published in 2015, demonstrated its efficacy in mCRC. The RECOURSE study, a randomized phase 3 trial, included 800 patients with mCRC who had received at least two series of standard chemotherapy and had progressed in the last 3 months. The FTD/TPI arm was compared with the placebo arm. Median OS was 7.1 months [95% CI, 6.5–7.8] in the FTD/TPI arm and 5.3 months [95% CI, 4.6–6.0] in the placebo arm. The HR for mortality for FTD/TPI compared with placebo was 0.68 [95% CI, 0.58–0.81; P < 0.001]. Median PFS was 2.0 months [95% CI, 1.9–2.1] in the FTD/TPI arm and 1.7 months [95% CI, 1.7–1.8] in the placebo arm. The HR for progression (FTD/TPI vs. placebo) was 0.48 [95% CI, 0.41–0.57; P < 0.001]. A total of 38% patients had neutropenia, 21% had leukopenia, and 4% had febrile neutropenia [64]. After the RECOURSE study, the results of the C-TASK FORCE study, a phase 1–2 study, were published in 2017. This study compared the use of FTD/TPI alone versus in combination with bevacizumab. After a median follow-up of 10 months, the median PFS was 2.6 months for trifluridine-tipiracil alone and 4.6 months in combination with bevacizumab [HR, 0.45; 95% CI, 0.29–0.72; P = .0015]. These results showed that the use of FTD/TPI with bevacizumab was more effective than its use alone [65]. SUNLİGHT trial, phase 3, international, prospective, randomized, active-controlled, and trial involving patients with refractory metastatic colorectal cancer showed that treatment with FTD–TPI plus bevacizumab resulted in significantly longer overall survival and progression-free survival and better disease control than treatment with FTD–TPI alone. Although a minority of patients did not receive the trial treatment as third-line therapy, this trial was predominantly a third-line trial (>90% of patients had received two previous lines of therapy). The duration of overall survival in the FTD–TPI group was consistent with previous observations, a finding that suggests the benefits observed with FTD–TPI plus bevacizumab will be applicable to all suitable patients with refractory disease [66]. In conclusion, FTD/TPI, both alone and in combination with bevacizumab, improves OS and PFS in patients with mCRC who have received multiple series of treatment. Since combined use with bevacizumab is more effective than monotherapy, combined use may be preferred.
3.2.2 Fruquintinib (HMPL-013)
Fruquintinib (HMPL-013) is a novel oral small molecule that selectively inhibits vascular endothelial growth factor receptors 1, 2, and 3 and has potent inhibitory effects on multiple human tumor xenografts [67]. Its efficacy in patients with mCRC who had received at least 2 prior lines of therapy was examined in the FRESCO study, a phase 3 trial. Median overall survival was significantly prolonged with fruquintinib compared with placebo (9.3 months [95% CI, 8.2–10.5] vs. 6.6 months [95% CI, 5.9–8.1]); the hazard ratio (HR) for mortality was 0.65 (95% CI, 0.51–0.83; P < .001). Median progression-free survival was also significantly increased with fruquintinib (3.7 months [95% CI, 3.7–4.6] vs. 1.8 months [95% CI, 1.8–1.8]); HR for progression or mortality was 0.26 (95% CI, 0.21 to 0.34; P < .001) [68]. The FRESCO-2 study was then conducted, again comparing the fruquintinib arm with the placebo arm. Patients with mCRC included in the study had previously received a median of four lines (IQR 3–6) of systemic therapy and 502 of 691 patients (73%) received more than three lines. Median overall survival was 7.4 months (95% CI 6.7–8.2) in the fruquintinib group vs. 4.8 months in the placebo group ([95% CI 4.0–5.8], HR 0.66, [95% CI 0.55–0.80; p < 0.0001)], PFS was 3.7 months in the fruquintinib arm and 1.8 months in the placebo arm (HR 0.32; [95% CI: 0.27–0.39]; p < 0.001). Side effects seen in the fruquintinib arms in the FRESCO and FRESCO two studies were similar. Grade 3 and above toxicity was seen in more than 60% in both studies. Arterial hypertension was the most common, while hand-foot skin reaction, asthenia, and proteinuria may be observed [69]. Fruquintinib was approved for use in previously treated mCRC by the United States Food and Drug Administration (FDA) in November 2023. Fruquintinib dose is 5 mg orally once daily, for the first 21 days of each 28-day cycle until disease progression or unacceptable toxicity. Despite the elevated occurrence of Grade 3 and above toxicity, signifying the need for caution regarding potential side effects during fruquintinib use, it has emerged as a significant therapeutic option for patients who have undergone multiple sequential treatments.
Advertisement
4. Brief recommendations from guidelines
4.1 ESMO recommendations
The European Society for Medical Oncology (ESMO) metastatic colorectal cancer guideline was last updated in October 2022. In mCRC patients, the approach recommendations in the first, second, and third treatment steps were clearly separated. Since the previous sections mentioned the recommendations for first- and second-line treatments, here, we will only talk about the recommended treatment approaches in the third line and beyond. If progression did not develop during first-line indication therapy, it was suggested that the same treatment could be given as reintroduction after the second series. Single-agent anti-EGFR (panitumumab or cetuximab) was recommended if RAS/BRAF wild patients were not previously treated with anti-EGFR. In RAS/BRAF wild irinotecan-refractory patients, the combination of irinotecan plus cetuximab was recommended more strongly than single-agent cetuximab. The use of another anti-EGFR was not recommended in patients who had previously progressed under anti-EGFR. Dual HER2 blockade was recommended in RAS/BRAF wild-HER2 positive patients. Based on the HERACLES study, the combination of trastuzumab and lapatinib was among the recommendations. The combination of encorafenib and cetuximab was recommended as the best option in series three in patients with previously treated BRAF V600E-mutated mCRC. In all patients, regardless of RAS/BRAF status, the oral agents reegorafenib or trifluridineetipiracil (TAS-102), which have previously shown superiority over BSC, were recommended. It is noteworthy that immunotherapy options (pembrolizumab, nivolumab, ipilimumab, and nivolumab) were recommended in the first- and second-line setting rather than third-line setting [70].
4.2 NCCN recommendations
First, NCCN divided patients into two groups: pMMR/MSS and dMMR/MSI-H. In the dMMR/MSI-H patient group, checkpoint inhibitor immunotherapy (pembrolizumab, nivolumab, nivolumab plus ipilimumab, or dostarlimab-gxly) was recommended as the first line of treatment. In patients who progressed under immunotherapy, systemic therapies were recommended in the next-line treatments. Cetuximab or panitumumab ±irinotecan treatment was recommended in the third step in patients with KRAS/NRAS/BRAF wild type located only in the left arm who had not received anti-EGFR therapy before. Cetuximab or panitumumab ±irinotecan treatment in the third line was suggested to be used in patients who received irinotecan-based treatment in the first series plus oxaliplatin-based treatment + anti-EGFR in the second series. However, emphasizing the number of patients and patient distribution of the studies on rechallenge, rechallenge was not recommended for treatment regimens under which progression had previously occurred. However, it was suggested that treatments that were discontinued due to conditions, such as adjuvant therapy, cumulative toxicity, treatment break, and patient preference, could be reintroduced in advanced steps. In the pMMR/MSS patient group, fruquintinib, regorafenib, trifluridine + tipiracil ± bevacizumab (primarily in combination with bevacizumab) treatments were recommended regardless of any mutation status in patients who received standard treatment in previous series [71].
4.3 ASCO recommendations
The ASCO guideline was last updated in October 2022. For this, the most recent treatments such as fruquintinib, sotorasib, and adagrasib were not included. Pembrolizumab treatment was recommended in MSH patients. Standard chemotherapy and anti-VEGFs were recommended in RAS mutant patients.
Standard chemotherapy and anti-EGFR antibodies were recommended in RAS/BRAF wild patients with left colon localization. Encorafenib plus cetuximab was recommended in BRAF V600E mutant patients with progression who had received at least one prior series of treatment [72].
Advertisement
5. Summary
Discoveries in tumor biology and advances in molecular diagnostic methods help to determine the most appropriate approach to treatment by analyzing the genetic structure of tumors of patients with mCRC in detail. This increases the importance of personalized treatment strategies in the treatment of advanced stages of mCRC. The dMMR/MSI-H status of the tumor, HER2 amplification or overexpression, KRAS 12C mutation, NTRK mutation, RET mutation, BRAF/MET status, TMB or POLE mutation status are prominent in evaluating treatment options.
Pembrolizumab, dostalizumab, nivolumab, and nivolumab plus ipilimumab treatments may be preferred in patients with dMMR/MSI-H if immunotherapy option was not used in previous lines. In particular, nivolumab plus ipilimumab treatment is ahead of the other treatments with an ORR of 65%, but dostalimab also draws attention with an ORR of 43.5%.
Trastuzumab and pertuzumab, trastuzumab and tucatinib, trastuzumab deruxtecan (T-DXd), trastuzumab and lapatinib may be preferred in patients with HER2 amplification or overexpression. Among these treatment options, trastuzumab+tucatinib treatment seems to be more prominent than other treatment options with higher ORR, PFS, and OS values.
Although adagrasib and sotorasib monotherapies have shown their efficacy in patients with KRAS 12C mutation, better survival results have been obtained in combination with anti-EGFR. Therefore, the preference for combined use in KRAS 12C mutant patients will be a more accurate approach than monotherapies.
Larotrectinib and entrectinib in solid tumors with NTRK fusion, and selpercatinib in patients with RET fusion have been approved for tumor-agnostic use, but the number of patients with mCRC in these studies is quite small. and it seems clear that new studies are needed to support the data. Encorafenib and cetuximab or panitumumab and/or binimetinib have demonstrated safety in terms of efficacy and side effect profile in patients with BRAF V600E mutated mCRC.
Regorafenib, trifluridine and tipiracil hydrochloride (TAS-102), fruquintinib have been replaced by regorafenib, Trifluridine and tipiracil hydrochloride (TAS-102) in patients who are not suitable for targeted therapies or who do not respond to these therapies. While regorafenib and fruquintinib are used as monotherapy, TAS-102 can be used as monotherapy or in combination with bevacizumab. Bevacizumab combination gives better results compared to monotherapy.
In cases where accessible treatment options are reduced, the use of conventional chemotherapies as rechallenge or reintroduction is frequently preferred by clinicians. They can also be used in patients who cannot be controlled with targetable agents. In addition, conventional chemotherapies are indispensable for many clinicians when financial toxicities are considered.
Despite all these developments, treatment responses and survival rates show that new developments are still needed in this field.
References
- 1.
Siegel RL, Giaquinto AN, Jemal A. Cancer statistics, 2024. CA: a Cancer Journal for Clinicians. 2024; 74 (1):12-49 - 2.
Society TAC. Survival rates for colorectal cancer. In: Cancer Facts & Figures 2024. American Cancer Society; 2024. Available from: https://www.cancer.org/cancer/types/colon-rectal-cancer/detection-diagnosis-staging/survival-rates.html - 3.
Nader Hanna CW, Zheng Z, Onukwugha E, Seal BS, Mullins CD. Survival benefit associated with the number of chemotherapy/biologic treatment lines in 5,129 metastatic colon cancer patients. Journal of Clinical Oncology. 2014; 32 :559. DOI: 10.1200/jco.2014.32.3_suppl.559 - 4.
Tampellini M, Di Maio M, Baratelli C, Anania L, Brizzi MP, Sonetto C, et al. Treatment of patients with metastatic colorectal cancer in a real-world scenario: Probability of receiving second and further lines of therapy and description of clinical benefit. Clinical Colorectal Cancer. 2017; 16 (4):372-376 - 5.
Buchler T. Microsatellite instability and metastatic colorectal cancer - a clinical perspective. Frontiers in Oncology. 2022; 12 :888181 - 6.
Le DT, Kim TW, Van Cutsem E, Geva R, Jäger D, Hara H, et al. Phase II open-label study of pembrolizumab in treatment-refractory, microsatellite instability-high/mismatch repair-deficient metastatic colorectal cancer: KEYNOTE-164. Journal of Clinical Oncology. 2020; 38 (1):11-19 - 7.
Overman MJ, McDermott R, Leach JL, Lonardi S, Lenz HJ, Morse MA, et al. Nivolumab in patients with metastatic DNA mismatch repair-deficient or microsatellite instability-high colorectal cancer (CheckMate 142): An open-label, multicentre, phase 2 study. The Lancet Oncology. 2017; 18 (9):1182-1191 - 8.
André T, Lonardi S, Wong KYM, Lenz HJ, Gelsomino F, Aglietta M, et al. Nivolumab plus low-dose ipilimumab in previously treated patients with microsatellite instability-high/mismatch repair-deficient metastatic colorectal cancer: 4-year follow-up from CheckMate 142. Annals of Oncology. 2022; 33 (10):1052-1060 - 9.
Markham A. Dostarlimab: First approval. Drugs. 2021; 81 (10):1213-1219 - 10.
Oaknin A, Pothuri B, Gilbert L, Sabatier R, Brown J, Ghamande S, et al. Safety, Efficacy, and Biomarker Analyses of Dostarlimab in Patients with Endometrial Cancer: Interim Results of the Phase I GARNET Study. Clinical Cancer Research. 14 Nov 2023; 29 (22):4564-4574. DOI: 10.1158/1078-0432.CCR-22-3915. PMID: 37363992; PMCID: PMC10643997 - 11.
André T, Berton D, Curigliano G, Sabatier R, Tinker AV, Oaknin A, et al. Antitumor activity and safety of dostarlimab monotherapy in patients with mismatch repair deficient solid tumors: A nonrandomized controlled trial. JAMA Network Open. 2023; 6 (11):e2341165 - 12.
Ross JS, Fakih M, Ali SM, Elvin JA, Schrock AB, Suh J, et al. Targeting HER2 in colorectal cancer: The landscape of amplification and short variant mutations in ERBB2 and ERBB3. Cancer. 2018; 124 (7):1358-1373 - 13.
Meric-Bernstam F, Hurwitz H, Raghav KPS, McWilliams RR, Fakih M, Vander Walde A, et al. Pertuzumab plus trastuzumab for HER2-amplified metastatic colorectal cancer (MyPathway): An updated report from a multicentre, open-label, phase 2a, multiple basket study. The Lancet Oncology. 2019; 20 (4):518-530 - 14.
Zheng-Lin B, Bekaii-Saab TS. Treatment options for HER2-expressing colorectal cancer: Updates and recent approvals. Therapeutic Advances in Medical Oncology. 2024; 16 :17588359231225037 - 15.
Chitkara A, Bakhtiar M, Sahin IH, Hsu D, Zhang J, Anamika F, et al. A meta-analysis to assess the efficacy of HER2-targeted treatment regimens in HER2-positive metastatic colorectal cancer (mCRC). Current Oncology. 2023; 30 (9):8266-8277 - 16.
Gupta R, Meric-Bernstam F, Rothe M, Garrett-Mayer E, Mangat PK, D'Andre S, et al. Pertuzumab plus Trastuzumab in patients with colorectal cancer with ERBB2 amplification or ERBB2/3 mutations: Results from the TAPUR study. JCO Precision Oncology. 2022; 6 :e2200306 - 17.
Yoshikawa A, Nakamura Y. Treatment strategies for HER2-positive metastatic colorectal cancer. Gan to Kagaku Ryoho. 2023; 50 (7):763-767 - 18.
Kulukian A, Lee P, Taylor J, Rosler R, de Vries P, Watson D, et al. Preclinical activity of HER2-selective tyrosine kinase inhibitor tucatinib as a single agent or in combination with trastuzumab or docetaxel in solid tumor models. Molecular Cancer Therapeutics. 2020; 19 (4):976-987 - 19.
Strickler JH, Cercek A, Siena S, André T, Ng K, Van Cutsem E, et al. Tucatinib plus trastuzumab for chemotherapy-refractory, HER2-positive, RAS wild-type unresectable or metastatic colorectal cancer (MOUNTAINEER): A multicentre, open-label, phase 2 study. The Lancet Oncology. 2023; 24 (5):496-508 - 20.
Iwata TN, Ishii C, Ishida S, Ogitani Y, Wada T, Agatsuma T. A HER2-targeting antibody-drug conjugate, trastuzumab deruxtecan (DS-8201a), enhances antitumor immunity in a mouse model. Molecular Cancer Therapeutics. 2018; 17 (7):1494-1503 - 21.
Yoshino T, Di Bartolomeo M, Raghav K, Masuishi T, Loupakis F, Kawakami H, et al. Final results of DESTINY-CRC01 investigating trastuzumab deruxtecan in patients with HER2-expressing metastatic colorectal cancer. Nature Communications. 2023; 14 (1):3332 - 22.
Nelson MH, Dolder CR. Lapatinib: A novel dual tyrosine kinase inhibitor with activity in solid tumors. The Annals of Pharmacotherapy. 2006; 40 (2):261-269 - 23.
Sartore-Bianchi A, Trusolino L, Martino C, Bencardino K, Lonardi S, Bergamo F, et al. Dual-targeted therapy with trastuzumab and lapatinib in treatment-refractory, KRAS codon 12/13 wild-type, HER2-positive metastatic colorectal cancer (HERACLES): A proof-of-concept, multicentre, open-label, phase 2 trial. The Lancet Oncology. 2016; 17 (6):738-746 - 24.
Awad MM, Liu S, Rybkin II, Arbour KC, Dilly J, Zhu VW, et al. Acquired resistance to KRAS(G12C) inhibition in cancer. The New England Journal of Medicine. 2021; 384 (25):2382-2393 - 25.
Fakih MG, Kopetz S, Kuboki Y, Kim TW, Munster PN, Krauss JC, et al. Sotorasib for previously treated colorectal cancers with KRAS(G12C) mutation (CodeBreaK100): A prespecified analysis of a single-arm, phase 2 trial. The Lancet Oncology. 2022; 23 (1):115-124 - 26.
Fakih MG, Salvatore L, Esaki T, Modest DP, Lopez-Bravo DP, Taieb J, et al. Sotorasib plus panitumumab in refractory colorectal cancer with mutated KRAS G12C. The New England Journal of Medicine. 2023; 389 (23):2125-2139 - 27.
Bekaii-Saab TS, Yaeger R, Spira AI, Pelster MS, Sabari JK, Hafez N, et al. Adagrasib in advanced solid tumors harboring a KRAS(G12C) mutation. Journal of Clinical Oncology. 2023; 41 (25):4097-4106 - 28.
Yaeger R, Weiss J, Pelster MS, Spira AI, Barve M, Ou SI, et al. Adagrasib with or without cetuximab in colorectal cancer with mutated KRAS G12C. The New England Journal of Medicine. 2023; 388 (1):44-54 - 29.
Gatalica Z, Xiu J, Swensen J, Vranic S. Molecular characterization of cancers with NTRK gene fusions. Modern Pathology. 2019; 32 (1):147-153 - 30.
Wang H, Li ZW, Ou Q , Wu X, Nagasaka M, Shao Y, et al. NTRK fusion positive colorectal cancer is a unique subset of CRC with high TMB and microsatellite instability. Cancer Medicine. 2022; 11 (13):2541-2549 - 31.
Dunn DB. Larotrectinib and entrectinib: TRK inhibitors for the treatment of pediatric and adult patients with NTRK gene fusion. Journal of the Advanced Practitioner in Oncology. 2020; 11 (4):418-423 - 32.
Carlson JJ, Italiano A, Brose MS, Federman N, Lassen U, Kummar S, et al. Comparative effectiveness of larotrectinib and entrectinib for TRK fusion cancer. The American Journal of Managed Care. 2022; 28 (2 Suppl):S26-s32 - 33.
Drilon A, Laetsch TW, Kummar S, DuBois SG, Lassen UN, Demetri GD, et al. Efficacy of larotrectinib in TRK fusion-positive cancers in adults and children. The New England Journal of Medicine. 2018; 378 (8):731-739 - 34.
Santos C, Sanz-Pamplona R, Salazar R. RET-fusions: a novel paradigm in colorectal cancer. Annals of Oncology. 2018; 29 (6):1340-1343 - 35.
Jhiang SM. The RET proto-oncogene in human cancers. Oncogene. 2000; 19 (49):5590-5597 - 36.
Le Rolle AF, Klempner SJ, Garrett CR, Seery T, Sanford EM, Balasubramanian S, et al. Identification and characterization of RET fusions in advanced colorectal cancer. Oncotarget. 2015; 6 (30):28929-28937 - 37.
Pietrantonio F, Di Nicolantonio F, Schrock AB, Lee J, Tejpar S, Sartore-Bianchi A, et al. ALK, ROS1, and NTRK Rearrangements in Metastatic Colorectal Cancer. Journal of the National Cancer Institute. 1 Dec 2017; 109 (12). DOI: 10.1093/jnci/djx089. PMID: 29370427 - 38.
Duke ES, Bradford D, Marcovitz M, Amatya AK, Mishra-Kalyani PS, Nguyen E, et al. FDA approval summary: Selpercatinib for the treatment of advanced RET fusion-positive solid tumors. Clinical Cancer Research. 2023; 29 (18):3573-3578 - 39.
Subbiah V, Wolf J, Konda B, Kang H, Spira A, Weiss J, et al. Tumour-agnostic efficacy and safety of selpercatinib in patients with RET fusion-positive solid tumours other than lung or thyroid tumours (LIBRETTO-001): A phase 1/2, open-label, basket trial. The Lancet Oncology. 2022; 23 (10):1261-1273 - 40.
Sidaway P. From AACR 2022. Nature Reviews. Clinical Oncology. 2022; 19 (6):359 - 41.
Schulz MS, Wolf S, Struck V, Thomas N, Husman G, Zeuzem S, et al. Anti-EGFR reintroduction and rechallenge in metastatic colorectal cancer (mCRC): A real-world analysis. Cancers (Basel). 2022; 14 (7):1641 - 42.
Cremolini C, Rossini D, Dell'Aquila E, Lonardi S, Conca E, Del Re M, et al. Rechallenge for patients with RAS and BRAF wild-type metastatic colorectal cancer with acquired resistance to first-line cetuximab and irinotecan: A phase 2 single-arm clinical trial. JAMA Oncology. 2019; 5 (3):343-350 - 43.
Martinelli E, Martini G, Famiglietti V, Troiani T, Napolitano S, Pietrantonio F, et al. Cetuximab rechallenge plus avelumab in pretreated patients with RAS wild-type metastatic colorectal cancer: The phase 2 single-arm clinical CAVE trial. JAMA Oncology. 2021; 7 (10):1529-1535 - 44.
Sartore-Bianchi A, Pietrantonio F, Lonardi S, Mussolin B, Rua F, Crisafulli G, et al. Circulating tumor DNA to guide rechallenge with panitumumab in metastatic colorectal cancer: The phase 2 CHRONOS trial. Nature Medicine. 2022; 28 (8):1612-1618 - 45.
Rossini D, Germani MM, Lonardi S, Pietrantonio F, Dell'Aquila E, Borelli B, et al. Treatments after second progression in metastatic colorectal cancer: A pooled analysis of the TRIBE and TRIBE2 studies. European Journal of Cancer. 2022; 170 :64-72 - 46.
Cohen R, Liu H, Fiskum J, Adams R, Chibaudel B, Maughan TS, et al. BRAF V600E mutation in first-line metastatic colorectal cancer: An analysis of individual patient data from the ARCAD database. Journal of the National Cancer Institute. 2021; 113 (10):1386-1395 - 47.
Kim G, McKee AE, Ning YM, Hazarika M, Theoret M, Johnson JR, et al. FDA approval summary: Vemurafenib for treatment of unresectable or metastatic melanoma with the BRAFV600E mutation. Clinical Cancer Research. 2014; 20 (19):4994-5000 - 48.
Kopetz S, Guthrie KA, Morris VK, Lenz HJ, Magliocco AM, Maru D, et al. Randomized trial of irinotecan and cetuximab with or without vemurafenib in BRAF-mutant metastatic colorectal cancer (SWOG S1406). Journal of Clinical Oncology. 2021; 39 (4):285-294 - 49.
Koelblinger P, Thuerigen O, Dummer R. Development of encorafenib for BRAF-mutated advanced melanoma. Current Opinion in Oncology. 2018; 30 (2):125-133 - 50.
Wu PK, Park JI. MEK1/2 inhibitors: Molecular activity and resistance mechanisms. Seminars in Oncology. 2015; 42 (6):849-862 - 51.
Kopetz S, Grothey A, Yaeger R, Van Cutsem E, Desai J, Yoshino T, et al. Encorafenib, binimetinib, and cetuximab in BRAF V600E-mutated colorectal cancer. The New England Journal of Medicine. 2019; 381 (17):1632-1643 - 52.
Fancello L, Gandini S, Pelicci PG, Mazzarella L. Tumor mutational burden quantification from targeted gene panels: Major advancements and challenges. Journal for Immunotherapy of Cancer. 2019; 7 (1):183 - 53.
Marabelle A, Fakih M, Lopez J, Shah M, Shapira-Frommer R, Nakagawa K, et al. Association of tumour mutational burden with outcomes in patients with advanced solid tumours treated with pembrolizumab: Prospective biomarker analysis of the multicohort, open-label, phase 2 KEYNOTE-158 study. The Lancet Oncology. 2020; 21 (10):1353-1365 - 54.
Meiri E, Garrett-Mayer E, Halabi S, Mangat P, Shrestha S, Ahn E, et al. Pembrolizumab (P) in patients (pts) with colorectal cancer (CRC) with high tumor mutational burden (HTMB): Results from the targeted agent and profiling utilization registry (TAPUR) study. Journal of Clinical Oncology. 2020; 38 :133 - 55.
Hu H, Cai W, Wu D, Hu W, Dong Wang L, Mao J, et al. Ultra-mutated colorectal cancer patients with POLE driver mutations exhibit distinct clinical patterns. Cancer Medicine. 2021; 10 (1):135-142 - 56.
Costa T, Nuñez J, Felismino T, Boente L, Mello C. REOX: Evaluation of the efficacy of retreatment with an oxaliplatin-containing regimen in metastatic colorectal cancer: A retrospective single-center study. Clinical Colorectal Cancer. 2017; 16 (4):316-323 - 57.
Liu X, George GC, Tsimberidou AM, Naing A, Wheler JJ, Kopetz S, et al. Retreatment with anti-EGFR based therapies in metastatic colorectal cancer: Impact of intervening time interval and prior anti-EGFR response. BMC Cancer. 2015; 15 :713 - 58.
Köstek O, Hacıoğlu MB, Sakin A, Demir T, Sarı M, Ozkul O, et al. Regorafenib or rechallenge chemotherapy: Which is more effective in the third-line treatment of metastatic colorectal cancer? Cancer Chemotherapy and Pharmacology. 2019; 83 (1):115-122 - 59.
Bertocchi P, Aroldi F, Prochilo T, Meriggi F, Beretta GD, Zaniboni A. Chemotherapy rechallenge after regorafenib treatment in metastatic colorectal cancer: Still hope after the last hope? Journal of Chemotherapy. 2017; 29 (2):102-105 - 60.
Wilhelm SM, Dumas J, Adnane L, Lynch M, Carter CA, Schütz G, et al. Regorafenib (BAY 73-4506): A new oral multikinase inhibitor of angiogenic, stromal and oncogenic receptor tyrosine kinases with potent preclinical antitumor activity. International Journal of Cancer. 2011; 129 (1):245-255 - 61.
Grothey A, Van Cutsem E, Sobrero A, Siena S, Falcone A, Ychou M, et al. Regorafenib monotherapy for previously treated metastatic colorectal cancer (CORRECT): An international, multicentre, randomised, placebo-controlled, phase 3 trial. Lancet. 2013; 381 (9863):303-312 - 62.
Li J, Qin S, Xu R, Yau TC, Ma B, Pan H, et al. Regorafenib plus best supportive care versus placebo plus best supportive care in Asian patients with previously treated metastatic colorectal cancer (CONCUR): A randomised, double-blind, placebo-controlled, phase 3 trial. The Lancet Oncology. 2015; 16 (6):619-629 - 63.
Bendell JC, Rosen LS, Mayer RJ, Goldman JW, Infante JR, Benedetti F, et al. Phase 1 study of oral TAS-102 in patients with refractory metastatic colorectal cancer. Cancer Chemotherapy and Pharmacology. 2015; 76 (5):925-932 - 64.
Mayer RJ, Van Cutsem E, Falcone A, Yoshino T, Garcia-Carbonero R, Mizunuma N, et al. Randomized trial of TAS-102 for refractory metastatic colorectal cancer. The New England Journal of Medicine. 2015; 372 (20):1909-1919 - 65.
Kuboki Y, Nishina T, Shinozaki E, Yamazaki K, Shitara K, Okamoto W, et al. TAS-102 plus bevacizumab for patients with metastatic colorectal cancer refractory to standard therapies (C-TASK FORCE): An investigator-initiated, open-label, single-arm, multicentre, phase 1/2 study. The Lancet Oncology. 2017; 18 (9):1172-1181 - 66.
Prager GW, Taieb J, Fakih M, Ciardiello F, Van Cutsem E, Elez E, et al. Trifluridine-tipiracil and bevacizumab in refractory metastatic colorectal cancer. The New England Journal of Medicine. 2023; 388 (18):1657-1667 - 67.
Cao J, Zhang J, Peng W, Chen Z, Fan S, Su W, et al. A phase I study of safety and pharmacokinetics of fruquintinib, a novel selective inhibitor of vascular endothelial growth factor receptor-1, -2, and -3 tyrosine kinases in Chinese patients with advanced solid tumors. Cancer Chemotherapy and Pharmacology. 2016; 78 (2):259-269 - 68.
Li J, Qin S, Xu RH, Shen L, Xu J, Bai Y, et al. Effect of fruquintinib vs placebo on overall survival in patients with previously treated metastatic colorectal cancer: The FRESCO randomized clinical trial. Journal of the American Medical Association. 2018; 319 (24):2486-2496 - 69.
Dasari A, Lonardi S, Garcia-Carbonero R, Elez E, Yoshino T, Sobrero A, et al. Fruquintinib versus placebo in patients with refractory metastatic colorectal cancer (FRESCO-2): An international, multicentre, randomised, double-blind, phase 3 study. Lancet. 2023; 402 (10395):41-53 - 70.
Cervantes A, Adam R, Roselló S, Arnold D, Normanno N, Taïeb J, et al. Metastatic colorectal cancer: ESMO clinical practice guideline for diagnosis, treatment and follow-up. Annals of Oncology. 2023; 34 (1):10-32 - 71.
NCCN. NCCN Clinical Practice Guidelines in Oncology-Colon Cancer Version 4.2023. NCCN; 2023. Available from: http://www.nccn.org/ - 72.
Morris VK, Kennedy EB, Baxter NN, Benson AB 3rd, Cercek A, Cho M, et al. Treatment of metastatic colorectal cancer: ASCO guideline. Journal of Clinical Oncology. 2023; 41 (3):678-700