
Abstract
Cancer is a major health issue that significantly contributes to mortality worldwide. In 2023, an estimated 1,958,310 new cancer cases were projected in the United States. Individuals with cancer may suffer from physical impairments, fatigue, psychological and social issues that reduce their quality of life. Cancer treatments (post-operation, chemotherapy, or radiotherapy) can cause several side effects. Exercises or physical activity are safe and offer a positive impact before, during, and after cancer treatment, encompassing aerobic, resistance, balance, flexibility exercises and others. Exercises improve quality of life, muscle power, and cardiovascular fitness, while also preventing other diseases and reducing the risk of cancer recurrence and death. The aim of this chapter is to clarify exercises’ role in cancer patients. The choice of exercises depends on the diagnosis and patient tolerance, considering contraindications. Physical activity programs should be informed by guidelines, and individualized in intensity, duration, type, and frequency to achieve maximum positive impact.
Keywords
- oncology
- cancer survivors
- exercises
- physical activity
- cancer related symptoms
1. Introduction
Cancer is a major health issue that significantly contributes to mortality worldwide. In 2023, an estimated 1,958,310 new cancer cases and 609,820 cancer deaths were projected in the United States, with over 15.5 million cancer survivors [1]. Cancer survivors may experience long-term health issues that result from the disease, its treatment, and related comorbid conditions. The risk of cancer increases with age. The majority of cancer patients are known to be elderly [2].
Cancer patients require abundant care, especially during the treatment period. Cancer can impact physical, psychological, social, and economic health, leading to dysfunction for many years following treatments, difficulty returning to work, or independent living, and poor quality of life. For example, common side effects of chemotherapy include but are not limited to, neuropathy, fatigue, nausea, bone marrow suppression, and immune system suppression [3]. Radiotherapy side effects may include tightness of skin, loss of range of motion, loss of bone density, secondary pain, fatigue, and whole-body symptoms similar to the effects of chemotherapy [4]. Additionally, possible side effects of surgery may include pain, scar tissue, swelling, and a reduction in mobility and strength in the affected limb [5]. Cancer-related fatigue is one of the most frequent complaints among individuals who have undergone various cancer treatments. It can also be accompanied by feelings of anxiety, depression, and negativity, or it may increase the mortality rate [6].
There is sufficient evidence to indicate that specific exercise guidelines for cancer patients improve quality of life, physical fitness, and independence in daily activities. In addition, it helps prevent cancer recurrence [7]. Exercise can play an important role in the management of cancer-related fatigue, reduction of pain, improving bone density, improving and maintaining flexibility of tissues, as well as stimulating the bone marrow immune response. The Physical Activity Guidelines recommend 150 minutes of moderate-intensity aerobic exercises spread over 3–5 days. Additionally, twice-weekly resistance training is recommended, ideally engaging major muscle groups [8]. Another useful exercise is yoga; it helps with flexibility and breathing. The choice of exercise should be determined by the patient’s specific condition. A patient’s response to a specific physical activity may vary due to comorbidities, age-related demographic characteristics, mobility limitations, or therapeutic side effects [9].
Certain exercises should be avoided or adjusted, especially in cases of bone metastases, bone cancer or lung cancer, as the treatment may cause the bones to be more brittle and weaker. Some patients need to avoid resistance and high-impact exercises, which may increase the risk of injury. Conditions such as anemia, characterized by a low red blood cell count, are often a result of treatment and should be considered before initiating a physical activity program [6].
Overall, exercises show clinical effects that can improve cancer-related health outcomes such as fatigue, lymphedema, urinary incontinence, muscle weakness, osteoporosis, and cancer-related obesity. This chapter introduces common cancer-related dysfunctions and outlines the importance of exercises based on evidence among cancer patients.
2. Cancer-related fatigue
The most common issue among cancer patients is fatigue, tiredness, and exhaustion [10]. It is described as a distressing and persistent symptom related to both cancer and its treatments. Cancer-related fatigue (CRF) differs from normal fatigue; it is prolonged, more generalized, not relieved by rest or sleep, and leads to a loss of desire for activities [11]. Most studies reporting cancer prevalence rates found that 65% of individuals complained of fatigue, with figures rising to 80–90% during chemotherapy or radiotherapy [12]. In addition to hormonal therapy, fatigue can result from targeted therapy, immune therapy and surgery. The extent of fatigue from surgery depends on the type of operation, but most people tend to improve with time. Fatigued patients take 2–3 months to return to normal, but for some, it may take longer [11]. Cancer-related fatigue affects many aspects of a patient’s life—physically (performance and activities of daily living), psychologically (mood, self-confidence), and socially (social activities, relationships)—and causes impairment in overall quality of life [12].
Assessment of the CRF should be comprehensive. Self-reporting is an efficient and highly recommended method for measuring CRF. Recent studies suggest that the most effective screening tool is a numerical rating scale (10-point rating scale). Patients are asked to score their fatigue level, with 0 indicating no fatigue and 10 indicating the worst possible fatigue [13]. Moreover, contributing factors such as comorbidities, mental and medical status, and other factors like anemia, infection, and conditions such as thyroid, renal, or cardiopulmonary diseases need to be assessed with specific attention as these factors significantly contribute to CRF [11].
Prolonged inactivity can lead to a reduction in musculoskeletal mass and power, psychological well-being, cardiovascular fitness, and activities of daily living [11]. Exercises can be beneficial at different stages of CRF, with no specific form of exercise found to be more beneficial than others. Exercises have not only been found effective in reducing CRF but also in improving cardiovascular fitness, psychological well-being, and quality of life. According to the current exercise guidelines, individuals should engage in 150 minutes per week of aerobic exercises, 2 days per week of resistance training, and flexibility exercises on days when no aerobic or resistance exercise is performed [11].
Resistance exercises not only reduce cancer-related fatigue, but also increase muscle strength, engage large muscle groups, lower blood lipids, optimize immune activity and promote an anti-inflammatory state [11, 14]. Randomized control trials (RCTs) have indicated that both resistance training and endurance exercises are safe and recommended whether performed at high-intensity or low-to-moderate intensity (with 12-week exercising program, twice per week). The exercises targeted large muscle groups with the aim of maximizing improvements in cardiorespiratory fitness; the relative improvements in peakVO2 (15–20%) for high-intensity and low-to-moderate, across different types of cancer diseases [14]. Therefore, combining resistance exercise with aerobic training improves physical functions and reduces chemotherapy related symptoms, including fatigue [15]. In a meta-analysis involving 3254 participants diagnosed with varying cancer types and stages during or after treatment, it was observed that combining resistance exercise with aerobic training at moderate to high intensity for a 6-month follow-up resulted in significantly less decline in cardiorespiratory fitness (ES, 0.14), improved physical functioning (ES, 0.68), reduced nausea and vomiting (ES, 1.00), decreased pain (ES, 0.60), and better outcomes for muscle strength (ES, 0.45) and physical fatigue(ES, 0.51). Additionally, low intensity exercises implemented as a home program prove to be beneficial for women who may be unable or unwilling to adhere to a higher-intensity program [16]. Aerobic training alone has been suggested as a treatment for CRF. As demonstrated in another systematic review comprising 40 trials, aerobic training exercises such as running, swimming, and walking, conducted over a 12-week follow-up, were found to significantly decrease fatigue in cancer survivors (the effect size in EORTC QLQ-C30 fatigue scale was −22.45 and in Liner analog self-assessment scale was −19.00). This positive effect was observed even when the exercise interventions were reported as either moderate to vigorous or low to moderate intensity [17].
For fatigued patients, brisk walking, stationary cycling, or treadmill exercises, along with other exercises, is recommended for at least 30–60 minutes per week. Patients can start their exercise routine with a low intensity, such as 5 minutes per week, and gradually increase up to 30 minutes over the course of a week or month [18]. Walking at a moderate intensity (50–70% of maximum heart rate) during chemotherapy and radiation therapy for breast cancer, starting from 10 to 45 minutes daily, for 4–6 days per week over 6 months, has been shown to reduce CRF and improve quality of life in non-cachectic patients [19].
Yoga exercise is another important intervention for preventing fatigue. A study conducted with breast cancer women shows that yoga, especially with deep breathing exercises, offers symptomatic relief for depression, sleep disorders, and results in a substantial reduction in fatigue. It can include different positions, such as the “Dead Men’s Position” (“Shavasana”) or “The Lying Butterfly” (“Supta Baddha Konasana”). Each of these positions was practiced for up to 7–10 minutes for an eight-week program [18]. Yoga is considered a low-intensity mind-body exercise (BMT). A systematic review and meta-analysis were conducted to evaluate the effects of yoga, Tai chi, and Qigong in alleviating the adverse effects of chemotherapy (breast, lung, and colorectal cancer). Quality of life, fatigue, and the six-minute walk test (6 MWT) were screened. The study found a significant reduction in fatigue among colorectal cancer patients undergoing chemotherapy after MBT interventions. The mean difference was observed in Fatigue: −1.35, 6MWT: −36.05, Quality of life: 3.88 [20]. Long duration of practicing yoga is more beneficial than short term intervention. A meta-analysis evaluated the effect of yoga on cancer-related fatigue in 2183 patients with breast cancer. It was concluded that supervised yoga classes had a significant effect on CRF (SMD = −0.31, 95% CI(−0.52, −0.10)); the eight-week program demonstrated a large effect compared to the six-week program, which had a moderately beneficial effect for 60–90 minutes in each session [21].
Exercises are recommended as a potential treatment for CRF and are supported by strong evidence (Figure 1). The patient should be encouraged to initiate physical activity, and the therapist should tailor the intensity and duration of the intervention based on the patient’s abilities, as outlined in the program’s benefits. However, future research is required to fully understand the factors and practical obstacles that hinder cancer patients from engaging in physical activity both before and after their treatment. Additionally, there is need to develop appropriate guidelines or protocols for CRF. Further studies are needed to assess the effectiveness of yoga exercises in other type of cancer treatments.
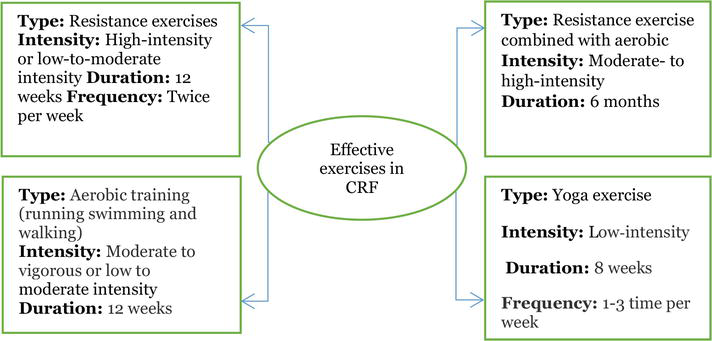
Figure 1.
Exercise recommendation for CRF.
3. Lymphedema
Lymphedema, a localized form of tissue swelling, is the accumulation of excessive amounts of interstitial fluid in the tissues, resulting in chronic swelling and other associated symptoms in one or more regions of the body [22]. Lymphedema develops in approximately 20–25% of women after axillary lymph node dissection and about 5% after sentinel lymph node biopsy [23].
Lymphedema can occur during or after many months or years after radiotherapy or immediately following lymph node dissection, significantly impacting people’s lives physically, functionally, psychologically, and economically. Patients may report physical effects of the treatment, including swelling, discomfort, and heaviness. Breast cancer-related lymphedema can increase the risk of cellulitis and cause skin and tissue changes, further affecting musculoskeletal issues. For example, trauma to the long thoracic nerve during axillary dissection and lymph node removal can lead to shoulder weakness, resulting in scapular instability due to serratus anterior weakness, frozen shoulder, decreased grip strength, and postural malalignment. The patient may experience changes in daily tasks, such as household chores, self-care tasks, leisure activities, and sleep/rest patterns. This, in turn, can then impact activity, participation, and the overall quality of life [24]. Moreover, it can lead to psychological issues, including changes to sexual drive, body image, energy levels, anxiety, depression, and fear. Breast cancer-related lymphedema may further exacerbate these concerns [25].
The evaluation and examination of lymphatic function starts with patient history, noting any history of trauma, surgery, radiation, chemotherapy, as well as details about the duration, onset, and period of chemotherapy. Furthermore, an examination of skin integrity, a pitting test, circumferential tape measure readings, and bioimpedance spectroscopy (BIS) are conducted [26].
There is currently no cure for lymphedema, and the primary objective of treatment is to restore the lymphedema to the latency stage as much as possible. The gold-standard treatment for lymphedema is the complex decongestive therapy (CDT) protocol, which includes manual lymphatic drainage (MLD), compression therapy, exercises, and skin care. In comprehensive management and rehabilitation, the effectiveness and limitations should be determined by the therapist. The complex decongestive therapy is divided into two stages: the first stage focuses on intensive treatment for reduction, while the second stage is dedicated to long-term management for maintenance. The first stage at the beginning includes a manual lymphatic drainage—a light repetitive stroking massage movement designed to stimulate the lymph nodes and improve their activity. Compression therapy varies depending on the stage of treatment. In the initial stage, low-stretching bandages are used, offering low resting pressure and high working pressure throughout the day. As patients transition from the initial stage to the maintenance stage, compression garments are used during the daytime, providing high resting pressure and low working pressure [27, 28].
Various forms of exercise seem to be safe interventions for treating lymphedema and offer benefits such as improved quality of life, strength, BMI, and decreased pain [29]. The standard guidelines recommend avoiding weight lifting using affected limbs to prevent exacerbations of lymphedema. However, in a controlled trial assessing the effectiveness of weight lifting among 141 breast-cancer survivors with stable arm lymphedema, it was concluded that weight lifting did not significantly alter the severity of lymphedema associated with breast cancer, as measured by displaced water volume (an absolute rise of ≥5 percentage points in the limb volume difference). Additionally, weight lifting resulted in a decreased incidence of exacerbations of lymphedema, reduced symptoms, and increased strength. The exercises consisted of high-frequency dynamic and moderate training, which included a cardiovascular warm-up, abdominal and back exercises, and weight lifting exercises. The upper-body exercises included seated rows, chest press, lateral or front raises, bicep curls, and triceps pushdowns. Additionally, the lower-body exercises included leg press, back extension, leg extension, and leg curl (for a 90-minute session, twice weekly for a year) [30].
The compression bandage must be worn during exercises to avoid lymphatic backflow. This is because the muscle contractions enhance the movement of lymph within lymph vessels, resulting in reduced volume and an increased strength pattern [31]. For example, a study examined the impact of low-intensity strengthening exercises, either associated with or without Complex Physical Therapy (CPT). The exercises, involving the use of a TheraBand, stick, and a little ball, were performed for 10–15 repetitions on 2–3 sets, twice a week over 8 weeks. The study concluded that exercises, whether associated with CPT or not, can be implemented safely and result in similar increases in range of movement and muscle strength without the risk of increasing upper limb volume with edema. Whereas, the mean difference of limb volume reduction after exercising with CPT: 119 mm compared to without CPT: 297 mm [32]. In a single randomized controlled crossover trial, it was found that gynecological cancer-related lower limb lymphedema was significantly reduced after high-load active exercise with compression therapy (AECT) compared to low-load AECT (The mean change (95%CI) of Lower-limb volume; 31.7–93.3 and 19.5–80.6, respectively). The study used the Strength Ergo™240 bicycle ergometer, with durations ranging from 15 to 60 minutes [33]. Another systematic review and meta-analysis evaluated the effects of aerobic, resistance, and mixed exercise on cancer-related lymphedema, specifically determining the need for wearing compression during exercise over a period ranging from 8 weeks to more than 12 weeks. The study observed immediate significant reductions in limb swelling after exercises. However, long-term effect was not found to be significant. The standardized mean differences (SMD) from all analyses were ranging between −0.2 and 0.1 [34].
In addition, stretching and flexibility exercises are strongly recommended to alleviate hypomobility in soft tissues and joints [31]. In addition to deep breathing exercises (abdominal diaphragmatic), they assist in the movement of lymphatic fluid during deep inspiration, maximum expiration, and abdominal contraction [31]. Other interventions to reduce lymphedema are yoga exercises, which have shown positive results in treating breast cancer survivors. In a span of 8–12 weeks, yoga interventions were found to reduce tissue induration in the affected upper arm compared to usual care [35, 36].
Resistance exercises combined with aerobics or yoga with or without CPT may be beneficial and safe to reduce lymphedema (Figure 2), but most studies have found that exercises decreased the incidence of exacerbations. Overall, there is insufficient scientific evidence to strongly support this point.
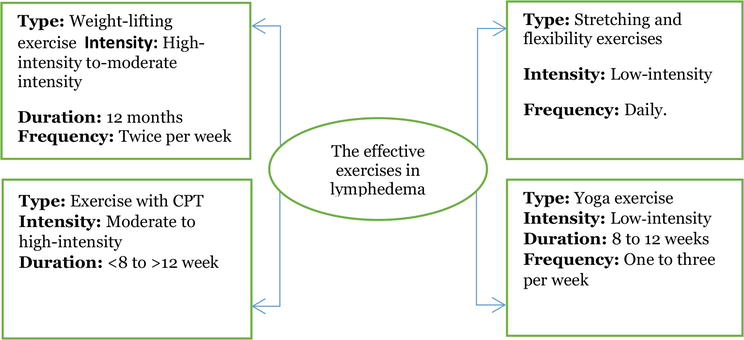
Figure 2.
Exercise recommendation for lymphedema.
4. Chemotherapy-induced peripheral neuropathy (CIPN)
Approximately 68% of cancer patients experience chemotherapy-induced peripheral neuropathy within the first month of receiving chemotherapy [37]. It is a syndrome characterized by highly distressing symptoms of varying degrees of severity that significantly impact daily functioning [3]. Its presentation varies depending on the type of affected nerve fibers [37]. If sensory nerves are affected, symptoms may include numbness, tingling, stinging, pain, weakness, or burning. Conversely, damage to the motor nerves can cause muscle spasms and muscle wasting, a loss of muscle dexterity and diminished strength. Additionally, damage in the autonomic system may affect and cause autonomic symptoms related to orthostatic hypotension [38].
There are six specific chemotherapy drugs that are more likely to cause peripheral neuropathy, such as platinum-based drugs, taxanes, vinca alkaloids, bortezomib, epothilones, proteasome inhibitors, and immunomodulatory drugs. The mechanisms of these therapeutic drugs are diverse and include both DNA and microtubular targets to arrest cell division and induce cell death. The pathophysiological processes are multifactorial, including oxidative stress, apoptotic mechanisms, altered calcium homeostasis, axon degeneration and membrane remodeling, immune processes and neuro-inflammation [37].
The diagnosis of CIPN should include patient history, current treatments, social history, physical examination, lab tests, electrodiagnostic studies, and nerve biopsy if needed [38].
Exercise may treat or prevent CIPN, as suggested by the RCT study involving 355 patients who received chemotherapy. The study evaluated a standardized, individualized, home-based progressive walking and resistance exercise program compared to those without a standard care control group. Their results stated that exercises can reduce CIPN symptoms of hot or coldness in hands or feet, numbness, and tingling by nearly 0.5 units on the 0–10 scales compared to the participants in the control group. Moreover, the exercise program included low to moderate-intensity home-based walking (60–85% of heart rate reserve) and low to moderately intense resistance exercise (squat, side bend, leg extension, leg curl, chest press, row, calf raise, overhead press, biceps curl, triceps extension) along with four optional band exercises (front raise, lateral raise, internal rotation, external rotation). Participants performed these exercises daily for a 6-week period, with a maximum of 4 sets of 15 repetitions [39]. Furthermore, CIPN symptoms may be better managed effectively in individuals who are younger, fitter, and leaner by utilizing high-intensity aerobic activity (180 minutes per week, 3 times per week) instead of low-intensity exercise (90 minutes per week). This was demonstrated during treatment in 301 women with breast cancer in an RCT [40].
Overall, several clinical trials and studies have demonstrated the potential advantages of various types of exercise and intensities for cancer patients receiving chemotherapy or following chemotherapy who have been diagnosed with CIPN (mixed cancer types and stages and CIPN severity). Balance, walking, resistance, and aerobic exercises, or combined exercises (Figure 3), provided not only benefits in patients with CIPN but also improved quality of life, Barthel index, the 6-minute walk test (6MWT), balance, and muscle strength [15, 41, 42, 43, 44].
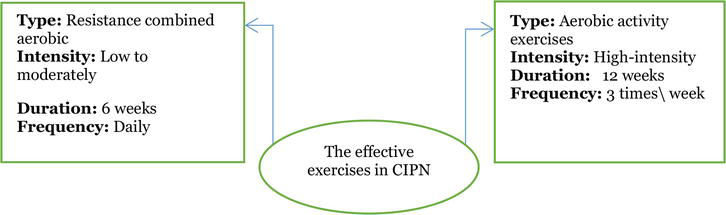
Figure 3.
Exercise recommendation for CIPN.
5. Urinary incontinence
Urinary incontinence (UI) is an involuntary loss of urine or the inability to control urination. The subtype of UI includes urge urinary incontinence, characterized by involuntary leakage immediately preceded by urgency. It occurs when the bladder contracts abnormally during filling, creating a progressively stronger and undeniable sensation of the need to urinate. Urinary incontinence can be associated with an overactive bladder; individuals may be “at least slightly bothered by frequent urination” and/or experience “leakage related to feeling of urgency”. Stress incontinence is involuntary leakage related to physical activity, coughing, or sneezing. It happens due to increased intra-abdominal pressure and when the urethral sphincter is unable to maintain a pressure higher than that exerted on the bladder. Mixed urinary incontinence is characterized by the presence of both stress and urge incontinence [45, 46].
Approximately 34% of women treated for the three main types of gynecologic cancers—cervical, endometrial, and ovarian—complained of urinary incontinence [47]. Additionally, it may occur after prostatectomy or radiation therapy [48], or following surgical treatment of rectal cancer [49]. Furthermore, 38% of cervical cancer survivors report chronic pelvic pain, chronic enteritis, proctitis, cystitis, and tenesmus-associated urinary or fecal urgency as common radiation-related adhesions [50]. The genital system can be impacted during cancer intervention, leading to dyspareunia secondary to menopause, decreased vaginal lubrication from radiation, and vaginal stricture or fibrosis resulting from radiation. Approximately 34–58% of women experience UI, a higher prevalence compared to men [50]. On the other hand, UI is a common problem in patients with early-stage breast cancer receiving neoadjuvant therapy. Approximately 79.8% of women experienced UI before the initiation of systemic therapy in the year following primary treatment, with symptoms related to chemotherapy. Endocrine therapy and adjuvant chemotherapy can exacerbate bladder control problems, hot flashes, and vaginal issues, particularly in older women, and these challenges are sometimes difficult to resolve [51]. There are other factors associated with UI and their impact on quality of life aside from cancer treatment, such as age, menopausal status, body mass index (BMI), race or ethnicity, history of smoking, and parity (0, 1, 2, or ≥ 3 births) [52].
The examination for UI includes manual evaluation or electrical devices to assess muscle power, contraction, endurance, and dermatome. The treatment program is determined according to the level of weakness.
The pelvic floor rehabilitation program improves pelvic floor dysfunction and quality of life in gynecological cancer patients. The contractions effectively inhibit detrusor muscle hypertrophy, increasing mechanical pressure on urethra and preventing urinary incontinence. An excellent example of strengthening exercises is Kegel exercises. Studies have demonstrated that the exercises could help prevent cystocele, rectocele, and urinary stress incontinence. However, about 30% of women could not contract the pelvic floor muscles correctly [53]. A Study involving 90 urogynecology women aimed to assess the effects of home-based Kegel exercises in women with stress and mixed urinary incontinence. The study revealed statistically significant improvements in outcomes, including the Incontinence Impact Questionnaire (IIQ-7), Urogenital Distress Inventory (UDI-6), and the Patient Global Impression of Improvement (PGI-I) questions (The mean changes in SUI: 24, 29, 26 and SUI: 9, 11, 14, respectively), after 8 weeks of exercising. The Kegel exercises for stress UI and mixed UI consisted of 10 sets of contractions and 10 repetitions daily for at least 8 weeks [54]. The short duration of exercise, specifically a four-week pelvic floor rehabilitation program (PFRP), involved only one session per day. This program included a second set of 20 to 30 seconds of fast pelvic floor contractions in addition to the first set of longer contractions. The results showed improvements in pelvic floor strength and sexual function (mean difference (MD) =14.22,
Pelvic floor muscle training could include coordination training, strength training, abdominal and trunk stabilization, or relaxation training, with or without the use of biofeedback, as recommended. The use of biofeedback increases men’s ability to isolate the pelvic floor muscle and differentiate between muscle contraction and relaxation. Studies have indicated that incorporating biofeedback with PFMT during the preoperative and early postoperative period helps expedite the recovery of continence in both the short and long term. These exercises consist of repeated, high-intensity muscle contractions [58]. Research is needed to determine the most effective treatment, as there is no established exercise protocol for urinary incontinence in cancer patients. The duration, intensity, and frequency varied, but they contributed to improving the UI. Most studies assessed the effectiveness of PFMT without specifying the type of exercises performed. Overall PFMT is recommended for cancer patients (Figure 4).
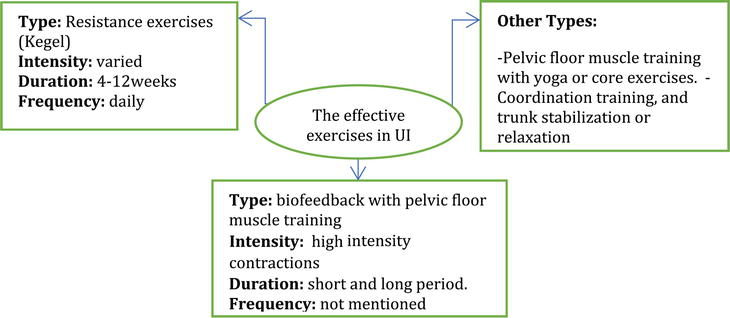
Figure 4.
Exercise recommendation for UI.
6. Osteoporosis
Osteoporosis is essentially the loss of bone mass in the trabecular region, leading to diminished density and an increased risk of fractures. It increases the risk of mortality and affects quality of life. All cancers can have significant negative effects on the skeleton through various mechanisms, either directly impacted by cancer cells or due to cancer treatments, including chemotherapy, corticosteroids, aromatase inhibitors, hormonal therapy such as tamoxifen for women with breast cancer, and androgen deprivation therapy for patients with prostate cancer [59]. Additionally, these effects are observed in gastric cancer patients who underwent gastrectomy [60] and gynecological cancer [61]. Besides, older patients or postmenopausal women are at a greater risk of bone loss and fractures compared to premenopausal women. Metastatic bone involvement is one of the complications of solid tumors and can affect the spine, pelvis, skull, ribs, proximal humerus, and femur [60].
Fractures caused by osteoporosis are termed fragility fractures. Common sites include the wrist and hip, often resulting from falls impacting either on an outstretched hand or directly onto the hip. However, the most common fracture occurs in the vertebral region. This fracture typically develops silently, accompanied by changes in posture, poor mechanics, repeated bending, and end-range forces. Exercises can contribute to improving bone remodeling, matrix mineralization, and bone marrow health. However, health professionals should carefully assess the risk of bone fragility and metastatic cancer, apply safe principles for alignment, and individualize the exercise program to prevent complications [60, 61]. Contraindications should also be taken into account.
Exercises are safe for cancer patients with osteoporosis and show effectiveness in maintaining or improving bone health during or after cancer treatment. Additionally, they help prevent comorbidities related to cancer such as obesity, cardiovascular disease, and type 2 diabetes [62]. This was supported by a 26-week study on female cancer survivors involving combined aerobic and resistance training, which reported significant improvements in bone mass density (BMD) at the spine (2.5%), hip (1.5%), and whole body (2.0%) as investigated using dual-energy X-ray absorptiometry (DXA). The exercises were performed 3 days per week, with sessions consisting of 20 minutes of cardiorespiratory training, 25 minutes of circuit-style resistance training, and 15 minutes of abdominal exercises and stretching [61]. Strengthening and weight training exercises, when combined with medication such as risedronate, calcium, and vitamin D, have been found to have effects and may prevent the loss of BMD at the femoral neck (SMD = +0.29%), total hip (SMD = +0.34%), spine (SMD = +0.23%), total radius (SMD = +0.30%) in postmenopausal women [63]. On the other hand, aerobic weight-loaded exercise did not show significant changes in serum osteocalcin, serum NTX, or lean muscle mass among women within 2 years of menopause who had completed adjuvant chemotherapy and adjuvant endocrine therapy. The participants engaged in a 6–24-week supervised walking exercise plus weight loading (1–4 times per week, with progressively increased weight). At the end of the study, it was suggested that a weight-loaded aerobic exercise intervention has the potential to maintain bone mass in women at risk for bone loss [64].
Only 41.9% of men with prostate cancer undergoing androgen deprivation therapy engage in the recommended amount of exercise, indicating a higher level of inactivity [65]. The most crucial aspect is to develop a habit for exercising. Patients may be advised to start with brief workouts (15 minutes per day, several times per week) before establishing a routine [66]. Nine RCTs provided a combination of aerobic, resistance, and impact-loading exercise or an hour-long football training lasting for 6 weeks to 12 months, with varied intensity and frequency (2–5 days per week). Participants could safely engage in exercise programs to preserve bone health and successfully exercise as a crucial part of their lifestyle. The findings demonstrate that exercises are relatively feasible and safe, and such exercises have the potential to reduce the risk of accidental falls, fractures, and associated morbidity and mortality rates. Moreover, this review shows a higher adherence rate from 43% to 96.3% and the retention rate from 71.9–100% in experimental exercise programs [67].
All types of exercise contribute to improving bone density and reducing risk of falls, injuries, with a significant impact on health-related quality of life. Regular exercise not only reduces mortality but should also be adopted as a long-term lifestyle habit (Figure 5).
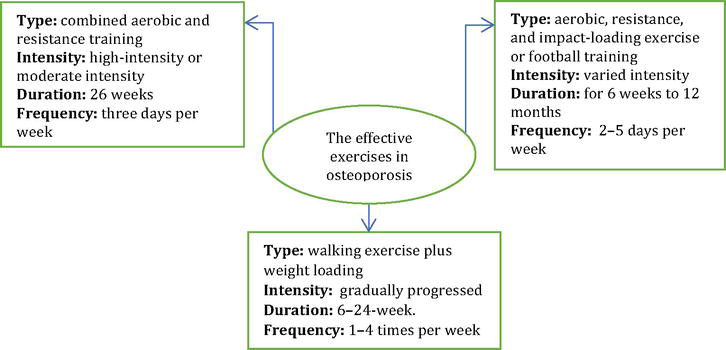
Figure 5.
Exercise recommendation for osteoporosis.
7. Obesity-related cancer
Many cancer patients experience weight gain after diagnosis, which is more common in those undergoing chemotherapy. Some patients also complain of loss of muscle mass and concomitant gain of adipose tissue, a condition referred to as cachexia [68]. Obesity increases the risk of cancer, with more than 40,000 cancer diagnoses each year attributed to obesity [69]. It is also linked to poorer cancer outcomes in breast, prostate, and colorectal cancers. More than two-thirds of survivors of breast, prostate, gynecologic, pancreatic, colorectal, ovarian cancer, and hematologic malignancies are overweight or obese [70]. Obesity in cancer survivors is a risk factor for developing comorbidities, such as heart disease, cerebrovascular disease, and diabetes [71]. Overweight is categorized as a BMI greater than or equal to 25, and obesity is categorized as a BMI greater than 30 [68].
The American Society of Clinical Oncology (ASCO) is committed to reducing the impact of obesity on cancer survivors and encourages participation in weight loss programs after the completion of adjuvant chemotherapy and radiotherapy [68]. A reduction in obesity through physical activity can improve insulin sensitivity, decrease circulating glucose and insulin levels, improve immune surveillance and recirculation of immunoglobulin, neutrophils, cytotoxic T cells, and immature B cells, and improve blood lipids and metabolic health [72]. Research has shown that weight loss strategies combining nutrition, physical activity, and psychological support can enhance the quality of life and lower the BMI of individuals who have survived breast cancer [73, 74]. For example, a study involving 351 survivors of breast cancer with overweight or obesity for a 52-week treatment program concluded that both increased physical activity and calorie restriction may lead to more significant weight loss (mean change: −6.68 kg) compared to caloric restriction (mean change: −5.39 kg) or increased physical activity (mean change: −0.06 kg) alone [74].
Generally, physical exercise is associated with weight reduction, a lower BMI, a lower percentage of body fat, and an increase in the quality of life. It is recommended either alone or in combination with other interventions. Future studies, including other types of cancer, are needed (Figure 6).
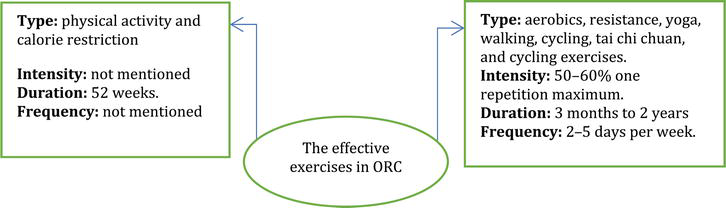
Figure 6.
Exercise recommendation for obesity related cancer.
8. Conclusions
Cancer patients suffer from multiple symptoms during treatments or as side effects after treatment. Physical activity helps improve quality of life, reduce mortality, and prevent the recurrence of cancer. There are no specific types or frequency that should be followed; the exercise program built up depends on the patient’s tolerance and other factors. In this chapter the evidence showed different effectiveness of exercises as follows:
The current exercise guidelines indicate that cancer patients should engage in 150 minutes of moderate-intensity resistance, aerobic, and flexibility exercises.
All studies demonstrate a significant effect of exercises of all types on improving fatigue, cardiovascular fitness, and other aspects related to quality of life. A longer duration of intervention is better than a short period.
Exercises are safe for lymphedema patients and help prevent exacerbations, but weight lifting or combined aerobics showed immediate effects after exercises in reducing swelling. However, there was no significant alteration in the severity of lymphedema whether associated with CPT or not. Only one study related to gynecological cancer-related lower limb lymphedema shows the opposite.
Balance, walking, resistance, and aerobic exercise or combined exercises are recommended for patients with CIPN.
The pelvic floor rehabilitation program, especially Kegel exercises, is important for cancer patients with urinary incontinence or sexual dysfunction of both genders. Using biofeedback with pelvic floor muscle training is effective as a short- or long-term intervention.
Aerobic and resistance training are safe for cancer patients with osteoporosis and help prevent the loss of BMD in postmenopausal women or prostate cancer patients with ADT.
Exercises alone or in combination with other interventions are recommended, but studies have shown a limited impact on body composition and BMI.
Acknowledgments
I would like to express my deepest gratitude to the head of holistic care in Sultan Qaboos comprehensive cancer care and research center for moral support and inspiration.
References
- 1.
Siegel RL, Miller KD, Wagle NS, Jemal A. Cancer statistics, 2023. CA: A Cancer Journal for Clinicians. 2023; 73 (1):17-48. DOI: 10.3322/caac.21763 - 2.
Miller KD, Siegel RL, Lin CC, Mariotto AB, Kramer JL, Rowland JH, et al. Cancer treatment and survivorship statistics, 2016. CA: A Cancer Journal for Clinicians. 2016; 66 (4):271-289. DOI: 10.3322/caac.21349. Epub 2016 Jun 2 - 3.
Brzeziński K. Chemotherapy-induced polyneuropathy. Part I. Pathophysiology. Contemporary Oncology (Pozn). 2012; 16 (1):72-78. DOI: 10.5114/wo.2012.27341. Epub 2012 Feb 29 - 4.
Chaput G, Regnier L. Radiotherapy: Clinical pearls for primary care. Canadian Family Physician. 2021; 67 (10):753-757. DOI: 10.46747/cfp.6710753 - 5.
Lovelace DL, McDaniel LR, Golden D. Long-term effects of breast Cancer surgery, treatment, and survivor care. Journal of Midwifery & Women's Health. 2019; 64 (6):713-724. DOI: 10.1111/jmwh.13012. Epub 2019 Jul 19 - 6.
Campbell KL, Winters-Stone KM, et al. Exercise guidelines for Cancer survivors: Consensus statement from international multidisciplinary roundtable. Medicine and Science in Sports and Exercise. 2019; 51 (11):2375-2390. DOI: 10.1249/MSS.0000000000002116 - 7.
COSA Exercise and Cancer Group Executive Committee. Clinical oncology Society of Australia position statement on exercise in cancer care. The Medical Journal of Australia. 2019; 210 (1):54-54.e1. DOI: 10.5694/mja2.12039. Epub 2018 Dec 7 - 8.
Schmitz KH, Campbell AM, et al. Exercise is medicine in oncology: Engaging clinicians to help patients move through cancer. CA: A Cancer Journal for Clinicians. 2019; 69 (6):468-484. DOI: 10.3322/caac.21579. Epub 2019 Oct 16 - 9.
Parker NH, Arlinghaus KR, Johnston CA. Integrating physical activity into clinical Cancer care. American Journal of Lifestyle Medicine. 2018; 12 :220-223. DOI: 10.1177/1559827618759478 - 10.
Mock V, Atkinson A, Barsevick A, Cella D, Cimprich B, Cleeland C, et al. National Comprehensive Cancer Network. NCCN practice guidelines for Cancer-related fatigue. Oncology (Williston Park). 2000; 14 (11A):151-161 - 11.
Fabi A, Bhargava R, Fatigoni S, Guglielmo M, Horneber M, Roila F, et al. Electronic address: clinicalguidelines@esmo.org . Cancer-related fatigue: ESMO clinical practice guidelines for diagnosis and treatment. Annals of Oncology. 2020;31 (6):713-723. DOI: 10.1016/j.annonc.2020.02.016. Epub 2020 Mar 12 - 12.
Bower JE, Ganz PA, Desmond KA, Bernaards C, Rowland JH, Meyerowitz BE, et al. Fatigue in long-term breast carcinoma survivors: A longitudinal investigation. Cancer. 2006; 106 (4):751-758. DOI: 10.1002/cncr.21671 - 13.
Fisher MI, Davies C, Lacy H, Doherty D. Oncology section EDGE task force on Cancer: Measures of Cancer-related fatigue—A systematic review. Rehabilitation Oncology. 2018; 36 (2):93-105. DOI: 10.1097/01.REO.0000000000000124 - 14.
Kampshoff CS, Chinapaw MJ, Brug J, Twisk JW, Schep G, Nijziel MR, et al. Randomized controlled trial of the effects of high intensity and low-to-moderate intensity exercise on physical fitness and fatigue in cancer survivors: Results of the resistance and endurance exercise after ChemoTherapy (REACT) study. BMC Medicine. 2015; 13 :275. DOI: 10.1186/s12916-015-0513-2 - 15.
Courneya KS, Segal RJ, et al. Effects of aerobic and resistance exercise in breast cancer patients receiving adjuvant chemotherapy: A multicenter randomized controlled trial. Journal of Clinical Oncology. 2007; 25 (28):4396-4404. DOI: 10.1200/JCO.2006.08.2024. Epub 2007 Sep 4 - 16.
van Waart H, Stuiver MM, et al. Effect of low-intensity physical activity and moderate- to high-intensity physical exercise during adjuvant chemotherapy on physical fitness, fatigue, and chemotherapy completion rates: Results of the PACES randomized clinical trial. Journal of Clinical Oncology. 2015; 33 (17):1918-1927. DOI: 10.1200/JCO.2014.59.1081. Epub 2015 Apr 27 - 17.
Mishra SI, Scherer RW, Geigle PM, Berlanstein DR, Topaloglu O, Gotay CC, et al. Exercise interventions on health-related quality of life for cancer survivors. Cochrane Database of Systematic Reviews. 2012; 2012 (8):CD007566. DOI: 10.1002/14651858.CD007566.pub2 - 18.
Eidenberger M. Physiotherapeutic management in breast cancer patients. In: Breast Cancer Updates. IntechOpen; 3 May 2023. Crossref. DOI: 10.5772/intechopen.108946 - 19.
Mock V, Pickett M, Ropka ME, Muscari Lin E, Stewart KJ, Rhodes VA, et al. Fatigue and quality of life outcomes of exercise during cancer treatment. Cancer Practice. 2001; 9 (3):119-127. DOI: 10.1046/j.1523-5394.2001.009003119.x - 20.
Bailey LE, Morris MA. Mind-body therapies adjuvant to chemotherapy improve quality of life and fatigue in top cancers: A systematic review and meta-analysis. Complementary Therapies in Clinical Practice. 2023; 54 :101811. DOI: 10.1016/j.ctcp.2023.101811. Epub ahead of print - 21.
Dong B, Xie C, Jing X, Lin L, Tian L. Yoga has a solid effect on cancer-related fatigue in patients with breast cancer: A meta-analysis. Breast Cancer Research and Treatment. 2019; 177 (1):5-16. DOI: 10.1007/s10549-019-05278-w. Epub 2019 May 24 - 22.
Casley-Smith JR, Gaffney RM. Excess plasma proteins as a cause of chronic inflammation and lymphodema: Quantitative electron microscopy. The Journal of Pathology. 1981; 133 (3):243-272. DOI: 10.1002/path.1711330307 - 23.
Greene AK, Goss JA. Diagnosis and staging of lymphedema. Seminars in Plastic Surgery. 2018; 32 (1):12-16. DOI: 10.1055/s-0038-1635117. Epub 2018 Apr 9 - 24.
Ververs JM, Roumen RM, Vingerhoets AJ, et al. Risk, severity and predictors of physical and psychological morbidity after axillary lymph node dissection for breast cancer. European Journal of Cancer. 2001; 37 (8):991-999 - 25.
Shih YC, Xu Y, Cormier JN, Giordano S, Ridner SH, Buchholz TA, et al. Incidence, treatment costs, and complications of lymphedema after breast cancer Among women of working age: A 2-year follow-up study. Journal of Clinical Oncology. 2009; 27 (12):2007-2014. DOI: 10.1200/JCO.2008.18.3517. Epub 2009 Mar 16 - 26.
Shahpar H et al. Risk factors of lymph Edema in breast Cancer patients. International Journal of Breast Cancer. 2013; 2013 (Article ID 641818):7. DOI: 10.1155/2013/641818 - 27.
Huang TW, Tseng SH, et al. Effects of manual lymphatic drainage on breast cancer-related lymphedema: A systematic review and meta-analysis of randomized controlled trials. World Journal of Surgical Oncology. 2013; 11 :15. DOI: 10.1186/1477-7819-11-15 - 28.
Tzani I, Tsichlaki M, Zerva E, Papathanasiou G, Dimakakos E. Physiotherapeutic rehabilitation of lymphedema: State-of-the-art. Lymphology. 2018; 51 (1):1-12 - 29.
Panchik D, Masco S, Zinnikas P, Hillriegel B, Lauder T, Suttmann E, et al. Effect of exercise on breast Cancer-related lymphedema: What the lymphatic surgeon needs to know. Journal of Reconstructive Microsurgery. 2019; 35 (1):37-45. DOI: 10.1055/s-0038-1660832. Epub 2018 Jun 23 - 30.
Baumann FT, Reike A, Reimer V, Schumann M, Hallek M, Taaffe DR, et al. Effects of physical exercise on breast cancer-related secondary lymphedema: A systematic review. Breast Cancer Research and Treatment. 2018; 170 (1):1-13. DOI: 10.1007/s10549-018-4725-y. Epub 2018 Feb 22 - 31.
Kisner C, Colby L, Borstad J. Therapeutic Exercise: Foundations and Techniques, 7e. McGraw Hill; 2018. Available from: https://fadavispt.mhmedical.com/content.aspx?bookid=2262§ionid=175446320 - 32.
Luz RPC, Simao Haddad CA, Rizzi SKLA, Elias S, Nazario ACP, Facina G. Complex therapy physical alone or associated with strengthening exercises in patients with lymphedema after breast Cancer treatment: A controlled clinical trial. Asian Pacific Journal of Cancer Prevention. 2018; 19 (5):1405-1410. DOI: 10.22034/APJCP.2018.19.5.1405 - 33.
Fukushima T, Tsuji T, Sano Y, Miyata C, Kamisako M, Hohri H, et al. Immediate effects of active exercise with compression therapy on lower-limb lymphedema. Supportive Care in Cancer. 2017; 25 (8):2603-2610. DOI: 10.1007/s00520-017-3671-2. Epub 2017 Apr 6 - 34.
Singh B, Disipio T, Peake J, Hayes SC. Systematic review and Meta-analysis of the effects of exercise for those with Cancer-related lymphedema. Archives of Physical Medicine and Rehabilitation. 2016; 97 (2):302-315.e13. DOI: 10.1016/j.apmr.2015.09.012. Epub 2015 Oct 9 - 35.
Saraswathi V, Latha S, Niraimathi K, Vidhubala E. Managing lymphedema, increasing range of motion, and quality of life through yoga therapy among breast Cancer survivors: A systematic review. International Journal of Yoga. 2021; 14 (1):3-17. DOI: 10.4103/ijoy.IJOY_73_19. Epub 2021 Feb 5 - 36.
Loudon A, Barnett T, Piller N, Immink MA, Williams AD. Yoga management of breast cancer-related lymphoedema: A randomised controlled pilot-trial. BMC Complementary and Alternative Medicine. 2014; 14 :214. DOI: 10.1186/1472-6882-14-214 - 37.
Starobova H, Vetter I. Pathophysiology of chemotherapy-induced peripheral neuropathy. Frontiers in Molecular Neuroscience. 2017; 10 :174. DOI: 10.3389/fnmol.2017.00174 - 38.
Kraychete DC, Sakata RK. Painful peripheral neuropathies. Revista Brasileira de Anestesiologia. 2011; 61 (5):641-658, 351-360. English, Portuguese, Spanish. DOI: 10.1016/S0034-7094(11)70075-7 - 39.
Kleckner IR, Kamen C, Gewandter JS, Mohile NA, Heckler CE, Culakova E, et al. Effects of exercise during chemotherapy on chemotherapy-induced peripheral neuropathy: A multicenter, randomized controlled trial. Supportive Care in Cancer. 2018; 26 (4):1019-1028. DOI: 10.1007/s00520-017-4013-0. Epub 2017 Dec 14 - 40.
Courneya KS, McKenzie DC, Mackey JR, Gelmon K, Friedenreich CM, Yasui Y, et al. Subgroup effects in a randomised trial of different types and doses of exercise during breast cancer chemotherapy. British Journal of Cancer. 2014; 111 (9):1718-1725. DOI: 10.1038/bjc.2014.466. Epub 2014 Aug 21 - 41.
Zhang S. Chemotherapy-induced peripheral neuropathy and rehabilitation: A review. Seminars in Oncology. 2021; 48 (3):193-207. DOI: 10.1053/j.seminoncol.2021.09.004. Epub 2021 Sep 22 - 42.
Guo S, Han W, Wang P, Wang X, Fang X. Effects of exercise on chemotherapy-induced peripheral neuropathy in cancer patients: A systematic review and meta-analysis. Journal of Cancer Survivorship. 2023; 17 (2):318-331. DOI: 10.1007/s11764-022-01182-3. Epub 2022 Feb 11 - 43.
Kanzawa-Lee GA, Larson JL, Resnicow K, Smith EML. Exercise effects on chemotherapy-induced peripheral neuropathy: A comprehensive integrative review. Cancer Nursing. 2020; 43 (3):E172-E185. DOI: 10.1097/NCC.0000000000000801 - 44.
Diotti D, Puce L, Mori L, Trompetto C, Saretti E, Contenti C, et al. The role of physical activity against chemotherapy-induced peripheral neuropathy: A narrative review. Exploration of Neuroprotective Therapy. 2022; 2 :87-99 - 45.
Chung CP, Behrendt C, Wong L, Flores S, Mortimer JE. Serial assessment of urinary incontinence in breast Cancer survivors undergoing (neo)adjuvant therapy. Journal of the National Comprehensive Cancer Network. 2020; 18 (6):712-716. DOI: 10.6004/jnccn.2020.7535 - 46.
Ghaderi F, Oskouei AE. Physiotherapy for women with stress urinary incontinence: A review article. Journal of Physical Therapy Science. 2014; 26 (9):1493-1499. DOI: 10.1589/jpts.26.1493. Epub 2014 Sep 17 - 47.
Skjeldestad FE, Hagen B. Long-term consequences of gynecological cancer treatment on urinary incontinence: A population-based cross-sectional study. Acta Obstetricia et Gynecologica Scandinavica. 2008; 87 (4):469-475. DOI: 10.1080/00016340801948326 - 48.
Yang EJ, Lim JY, Rah UW, Kim YB. Effect of a pelvic floor muscle training program on gynecologic cancer survivors with pelvic floor dysfunction: A randomized controlled trial. Gynecologic Oncology. 2012; 125 (3):705-711. DOI: 10.1016/j.ygyno.2012.03.045. Epub 2012 Apr 1 - 49.
Wallner C, Lange MM, Bonsing BA, Maas CP, Wallace CN, Dabhoiwala NF, et al. Cooperative clinical investigators of the Dutch Total Mesorectal excision trial. Causes of fecal and urinary incontinence after total mesorectal excision for rectal cancer based on cadaveric surgery: A study from the cooperative clinical investigators of the Dutch total mesorectal excision trial. Journal of Clinical Oncology. 2008; 26 (27):4466-4472. DOI: 10.1200/JCO.2008.17.3062 - 50.
Glare PA, Davies PS, Finlay E, Gulati A, Lemanne D, Moryl N, et al. Pain in cancer survivors. Journal of Clinical Oncology. 2014; 32 (16):1739-1747. DOI: 10.1200/JCO.2013.52.4629. Epub 2014 May 5 - 51.
Ganz PA, Petersen L, Bower JE, Crespi CM. Impact of adjuvant endocrine therapy on quality of life and symptoms: Observational data over 12 months from the mind-body study. Journal of Clinical Oncology. 2016; 34 (8):816-824. DOI: 10.1200/JCO.2015.64.3866. Epub 2016 Jan 19 - 52.
Wojcik M, Jarzabek-Bielecka G, Merks P, Plagens-Rotman K, Pisarska-Krawczyk M, Kedzia W, et al. The role of visceral therapy, Kegel’s muscle, core stability and diet in pelvic support disorders and urinary incontinence – Including sexological aspects and the role of physiotherapy and osteopathy. Ginekologia Polska. 2022; 93 (12):1018-1027. DOI: 10.5603/GP.a2022.0136 - 53.
Huang YC, Chang KV. Kegel Exercises. In: StatPearls. Treasure Island (FL): StatPearls Publishing; 2023 - 54.
Cavkaytar S, Kokanali MK, Topcu HO, Aksakal OS, Doğanay M. Effect of home-based Kegel exercises on quality of life in women with stress and mixed urinary incontinence. Journal of Obstetrics and Gynaecology. 2015; 35 (4):407-410. DOI: 10.3109/01443615.2014.960831. Epub 2014 Sep 29 - 55.
Rutledge TL, Rogers R, Lee SJ, Muller CY. A pilot randomized control trial to evaluate pelvic floor muscle training for urinary incontinence among gynecologic cancer survivors. Gynecologic Oncology. 2014; 132 (1):154-158. DOI: 10.1016/j.ygyno.2013.10.024. Epub 2013 Oct 29 - 56.
Brennen R, Lin KY, Denehy L, Frawley HC. The effect of pelvic floor muscle interventions on pelvic floor dysfunction after Gynecological Cancer treatment: A systematic review. Physical Therapy. 2020; 100 (8):1357-1371. DOI: 10.1093/ptj/pzaa081 - 57.
Xin L, Li M, Pan M. The therapeutic effect of pelvic floor muscle training on stress urinary incontinence following prostatectomy: A systematic review and meta-analysis. Translational Andrology and Urology. 2023; 12 (7):1155-1166. DOI: 10.21037/tau-23-337. Epub 2023 Jul 24 - 58.
Huri M, Akel BS, Sahin S. Rehabilitation of patients with prostate cancer [Internet]. In: Prostate Cancer - Leading-edge Diagnostic Procedures and Treatments. InTech; 2016. doi: 10.5772/63989 - 59.
Drake MT. Osteoporosis and cancer. Current Osteoporosis Reports. 2013; 11 (3):163-170. DOI: 10.1007/s11914-013-0154-3 - 60.
Avancini A, Benato G, at al. Exercise and bone health in Cancer: Enemy or ally? Cancers (Basel). 2022; 14 (24):6078. DOI: 10.3390/cancers14246078 - 61.
Almstedt HC, Grote S, et al. Combined aerobic and resistance training improves bone health of female cancer survivors. Bone Reports. 2016; 5 :274-279. DOI: 10.1016/j.bonr.2016.09.003 - 62.
Winters-Stone KM, Schwartz A, Nail LM. A review of exercise interventions to improve bone health in adult cancer survivors. Journal of Cancer Survivorship. 2010; 4 (3):187-201. DOI: 10.1007/s11764-010-0122-1. Epub 2010 Apr 7 - 63.
Waltman NL, Twiss JJ, Ott CD, Gross GJ, Lindsey AM, Moore TE, et al. The effect of weight training on bone mineral density and bone turnover in postmenopausal breast cancer survivors with bone loss: A 24-month randomized controlled trial. Osteoporosis International. 2010; 21 (8):1361-1369. DOI: 10.1007/s00198-009-1083-y. Epub 2009 Oct 3 - 64.
Knobf MT, Insogna K, DiPietro L, Fennie C, Thompson AS. An aerobic weight-loaded pilot exercise intervention for breast cancer survivors: Bone remodeling and body composition outcomes. Biological Research for Nursing. 2008; 10 (1):34-43. DOI: 10.1177/1099800408320579 - 65.
Chipperfield K, Fletcher J, et al. Factors associated with adherence to physical activity guidelines in patients with prostate cancer. Psycho-Oncology. 2013; 22 (11):2478-2486. DOI: 10.1002/pon.3310. Epub 2013 Jun 7 - 66.
Pelman R, Elterman D. Lifestyle and disease, male health and risks. Revista Médica Clínica Las Condes. 2014; 25 :25-29. DOI: 10.1016/S0716-8640(14)70006-9 - 67.
Cagliari M, Bressi B, et al. Feasibility and safety of physical exercise to preserve bone health in men with prostate Cancer receiving androgen deprivation therapy: A systematic review. Physical Therapy. 2022; 102 (3):pzab288. DOI: 10.1093/ptj/pzab288 - 68.
Ligibel JA, Alfano CM, et al. American Society of Clinical Oncology position statement on obesity and cancer. Journal of Clinical Oncology. 2014; 32 (31):3568-3574. DOI: 10.1200/JCO.2014.58.4680. Epub 2014 Oct 1 - 69.
Finkelstein EA, Trogdon JG, Cohen JW, Dietz W. Annual medical spending attributable to obesity: Payer-and service-specific estimates. Health Affairs (Millwood). 2009; 28 (5):w822-w831. DOI: 10.1377/hlthaff.28.5.w822. Epub 2009 Jul 27 - 70.
Blanchard CM, Courneya KS, Stein K, American Cancer Society’s SCS-II. Cancer survivors’ adherence to lifestyle behavior recommendations and associations with health-related quality of life: Results from the American Cancer Society’s SCS-II. Journal of Clinical Oncology. 2008; 26 (13):2198-2204. DOI: 10.1200/JCO.2007.14.6217 - 71.
Travis LB, Demark Wahnefried W, Allan JM, Wood ME, Ng AK. Aetiology, genetics and prevention of secondary neoplasms in adult cancer survivors. Nature Reviews. Clinical Oncology. 2013; 10 (5):289-301. DOI: 10.1038/nrclinonc.2013.41. Epub 2013 Mar 26 - 72.
Larson EA, Dalamaga M, Magkos F. The role of exercise in obesity-related cancers: Current evidence and biological mechanisms. Seminars in Cancer Biology. 2023; 91 :16-26. DOI: 10.1016/j.semcancer.2023.02.008. Epub 2023 Mar 5 - 73.
Soares Falcetta F, de Araújo Vianna Träsel H, de Almeida FK, et al. Effects of physical exercise after treatment of early breast cancer: systematic review and meta-analysis. Breast Cancer Research and Treatment. 2018; 170 :455-476. DOI: 10.1007/s10549-018-4786-y - 74.
Brown JC, Sarwer DB, Troxel AB, et al. A randomized trial of exercise and diet on body composition in survivors of breast cancer with overweight or obesity. Breast Cancer Research and Treatment. 2021; 189 :145-154 - 75.
Joaquim A, Leão I, et al. Impact of physical exercise programs in breast cancer survivors on health-related quality of life, physical fitness, and body composition: Evidence from systematic reviews and meta-analyses. Front. Oncologia. 2022; 12 :955505. DOI: 10.3389/fonc.2022.955505 - 76.
Murtezani A, Ibraimi Z, Bakalli A, Krasniqi S, Disha ED, Kurtishi I. The effect of aerobic exercise on quality of life among breast cancer survivors: A randomized controlled trial. Journal of Cancer Research and Therapeutics. 1900; 10 (3):658-664 - 77.
Singh B, Spence RR, Steele ML, Sandler CX, Peake JM, Hayes SC. A systematic review and meta-analysis of the safety, feasibility, and effect of exercise in women with stage ii+ breast cancer. Archives of Physical Medicine and Rehabilitation. 2018; 99 (12):2621-2636. DOI: 10.1016/j.apmr.2018.03.026