
Russian and Aussie current application parameters.
Abstract
Isokinetic exercises are a type of exercise that can be performed both concentrically and eccentrically at various angular velocities while applying resistance to the muscles at each point of the range of motion. These exercises are known to have many benefits compared to other exercises. Electrotherapy modalities are a popular treatment used by physiotherapists for a variety of purposes, such as muscle strengthening, endurance, spasticity management, pain control, circulation enhancement, and edema control. Kilohertz-frequency alternating currents were introduced in the pioneering work of Kots as a new form of neuromuscular electrical stimulation that was believed to solve some of the limitations of conventional electrical stimulation. Russian current is a medium-frequency alternating current that is delivered in bursts, with the carrier frequency ranging from 1000 to 10,000 Hz and any burst frequency being acceptable. Aussie currents are utilized in clinics at 1000 Hz, modulated in 50 Hz intervals with a pulse duration of 2 msec. Medium-frequency currents, particularly Russian and Aussie currents in isokinetic training, provide muscle strength contraction and endurance, increased blood circulation, and specific physiological effects. Considering the person’s health status, existing injuries, or other health problems, Russian and Aussie currents can be used effectively in isokinetic training at appropriate levels under the guidance of a physician and physiotherapist.
Keywords
- isokinetic contraction
- strength dynamometer
- electrostimulation
- Russian current
- physiotherapy
1. Introduction
1.1 Isokinetic training
Isokinetic Exercises (IE) was first described by James Perrine in the 1960s. During IE, force is generated at a constant speed throughout the range of motion of the joint, and maximum force is generated in the muscle at every angle of the movement during contraction [1]. IE is a continuous constant speed training module. The speed of movement is constant except for acceleration at the beginning and deceleration at the end [2]. Isokinetic force is the highest torque (rotational moment) value developed during contraction at a given speed. IE can be performed concentrically and eccentrically at different angular velocities applies resistance to the muscles at each point of the range of motion and is well known to have many advantages over other exercises [3]. IE provides better strengthening compared to isometric and isotonic exercises because it allows eccentric contractions that can provide more strength and endurance increase in the muscle throughout the entire range of motion [4]. IE provides usable and reliable data at low, medium, and high speed for assessment and rehabilitation programs. IE can be used as a personalized muscle-strengthening technique. It offers a gradual and safe exercise program with objective measurement of muscle strength increase. While exercise offers great selectivity in movement, it produces faster strength gains and less muscle sensitivity than isotonic training. In addition, heart rate and blood pressure increases are lower than isometric exercise [5]. It has been reported that IE provides many benefits such as muscle strength, muscle endurance, and enzyme activities [6].
The isokinetic training used for the knee joint eliminates the bioarticular function of the hamstrings. The position of extended hip flexion from the trunk and increased hip flexion from the corresponding femur make the typical hamstring tension more functional as a mechanism [7]. Isokinetic training is the only safe way to load dynamically contracted muscles to maximum capacity throughout their entire range in a continuous movement using functional positions or isolated in correct biomechanical positions. Isokinetic contraction engages more muscle fibers than any other exercise method (Figure 1) [8]. The mechanism of isokinetic training has been explained by improvement in muscle performance, speed-specific adaptation of motor units within the muscle, and speed-specific adaptation in the nervous system. However, differences in the direction of the transfer effect can be explained by differences in sample size, muscle fiber distribution, and training duration and intensity [9]. Vidmar et al. studied, that the peak torque of the traditional training group before treatment was concentric 176.6, eccentric 109.1, and after treatment peak torque was concentric 205.7 and eccentric 128.8. In the isokinetic training group, pre-treatment peak torque concentric 165.1, eccentric 97.7, post-treatment peak torque concentric 206.0, and eccentric 162.1 [10]. Isokinetic eccentric training appears to have a greater effect on quadriceps muscle mass and muscle mass than traditional eccentric training [10].
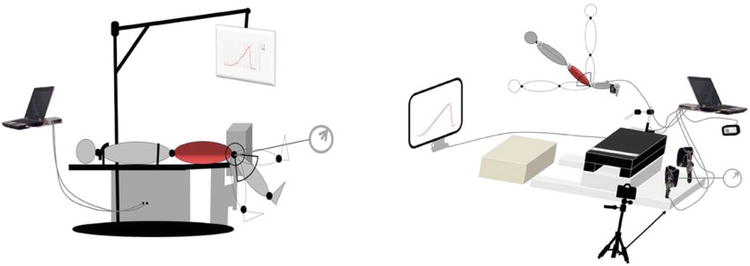
Figure 1.
Isokinetic dynamometer mechanism and effects of isokinetic training.
Petrucci et al. [11] review reported that in two studies included in their systematic review, isokinetic training produced significant differences (p < 0.05) in terms of increased muscle mass compared to the isotonic group. Tsaklis et al. [12] showed in their study that pre-post differences in muscle mass were higher in the isokinetic group, but no significant results were obtained. Therefore, it is recommended in the study that isokinetic training should be preferentially used instead of traditional isotonic to improve postoperative muscle mass. Sekir et al. [13] study, the peak torque concentric evertor of the ankle joint on the injured side before exercise was 15.54, the inverter 14.79, and the peak torque concentric evertor after exercise was 17.21, the invertor 16.50. The peak torque concentric evertor of the intact side ankle joint before exercise was 16.96, inverter 17.46, and the peak torque concentric evertor after exercise was 17.38, inverter 16.92. After the treatment, it is observed that the muscle strength between the injured and intact sides is similar. It is stated that the functional capacity of the injured ankle reaches the same level as the healthy ankle.
1.2 Isokinetic dynamometers
Assessing muscular strength using an isokinetic device is now widely used for various purposes, including rehabilitation of muscular and connective tissue injuries [14]. After quantitative measurement of muscle strength, the range of motion in which the muscle is weak can be determined. An appropriate exercise program can then be designed for the patient [15]. In addition, it allows kinematic analysis of movement in parameters such as determining agonist/antagonist muscle strength ratios, comparing both sides in limb segments, and measuring muscle work capacity and endurance. Isokinetic testing measures muscles or muscle groups in isolation. In cases where weak muscles are compensated by strong muscles, functional capacity is fully assessed. Measurements can be repeated and speed of movement can be determined (Figure 2) [4].

Figure 2.
Isokinetic dynamometer.
The isokinetic dynamometer is recognized as a valid method of assessing muscle strength and is often used as a reference standard for other strength assessments [16, 17]. An isokinetic dynamometer allows the assessment of muscle function with an appropriate resistance at a constant angular velocity, allowing maximum force production through a prescribed range of motion. In clinical practice, isokinetic dynamometers are often preferred to monitor progress during rehabilitation [17].
Isokinetic dynamometers can assess muscle strength in both the concentric and eccentric phases of movement. Eccentric muscle activity is superior to concentric contraction in many ways. Approximately 40–60% more strength gain can be achieved with eccentric muscle contraction. It also has a beneficial effect on inflammation by altering blood flow [3].
In isokinetic dynamometry, the speed of the moving segment cannot exceed a predetermined speed, no matter how much force is applied. It is therefore safe to use in the rehabilitation of patients with muscle and ligament injuries. In addition, these machines provide an objective measure of muscle strength, power, and endurance. As a result, they are increasingly being used to assess muscle performance. Isokinetic equipment is now used for strength training and rehabilitation, as well as to determine muscle balance and strength [17].
Current isokinetic dynamometer systems allow assessment in both concentric and eccentric exercise modes. The dynamometer shows the value of the developing force moment at each moment. In addition, the muscle is maximally loaded at a predetermined constant speed and during dynamic movement [18]. The most important data recorded by the isokinetic dynamometer is the battery torque or maximum force moment, which indicates the highest force value recorded during the test. Another variable provided by the isokinetic dynamometer is “work”, which is the product of force moment and angular distance.
Isokinetic dynamometers are mostly used to analyze peak torque data [19]. Isokinetic dynamometers are used to perform exercises at maximum intensity and constant angular velocity throughout the range of motion. This allows the exercise to be performed at the individual’s maximum strength level at each joint angle and minimizes the risk of overloading the patient’s tolerance. Isokinetic exercise is included in rehabilitation programs to optimize muscular strength, particularly in the treatment of elite athletes [10].
Studies have reported increases in maximal strength and endurance performance with IE [20]. Isokinetic dynamometers are the gold standard for assessing muscle strength, allowing us to determine the agonist/antagonist ratio through different angular velocities. It is also considered an effective tool for improving muscle function. Isokinetic dynamometry was introduced as a trade name in the late 1960s with the first Cybex I machine. Since then, much research has been conducted in the field of rehabilitation and sports performance, with the knee joint being the most studied and the hip to a lesser extent [20].
Isokinetic dynamometers are widely used in both clinical and research settings. In the literature, most studies using isokinetic dynamometers have focused on knee flexors and extensors, with less attention paid to the hip joint (14). In a systematic review, isokinetic knee flexion and extension force measurements using a wide range of angular velocities were reported to provide moderate to good reliability [14]. Although the reliability of isokinetic assessments is influenced by factors such as the position of the person, movement speed, muscle contraction, and pelvic stability, according to the results of the meta-analysis, they have produced measurements with higher reliability [20].
1.3 Isokinetic strength measurement
Determination of angular velocities There is a wide range of angular velocities used to test the quadriceps and hamstring group muscles. In 1989, Borges preferred a very low speed of 12°/sec, while at the other end of the spectrum. Ghena et al. [6] tested subjects at speeds up to 500°/sec. For the knee joint, velocities above 180°/sec are defined as high velocities [6, 21]. The gain increase at high angular velocities and whether it provides meaningful data is controversial. In the isokinetic dynamometer, as the angular speed increases, the maximum torque decreases. Again, some studies reported that very little muscle force change was detected at speeds above 300°/sec in the knee, and the maximum change was obtained between 30 and 120°/sec [22]. In conclusion, in light of the studies in the literature, the angular velocities between 60 and 180°/sec are the ones that are comfortable for the patient during isokinetic testing and allow for obtaining adequate and reliable data in terms of muscle performance [23].
The isokinetic dynamometer is the gold standard for measuring peak torque, work, and force as a function of angular velocity, as well as the agonist/antagonist muscle force ratio. Peak torque is a good indicator of maximum muscle tension, and strength tests are performed at low speeds (30–60°/s), while endurance and total work tests are performed at high speeds (180–300°/s). Total work is the sum of all the work performed in one set. Total work is used to measure endurance in isokinetic testing [24].
When the literature is examined, it is stated that electrotherapy methods should be combined with isokinetic training and the use of electrophysical agents [25, 26, 27]. Isokinetic training can be used in many diseases. Isokinetic training is as effective as traditional isotonic training in regaining strength and balance between hamstrings and quadriceps and results in better adaptation in muscle mass. As a result, isokinetic training is included as one of the main strength restoration strategies after knee surgery rehabilitation, especially in the early and intermediate stages when strength restoration is one of the main goals [28]. In a study, it was reported that Russian Current and High Voltage Pulsed Current (HVPC), which can be added to isokinetic strengthening exercises, have the same effect on muscle strength and endurance. It has been shown that both currents can be used to increase muscle endurance. Therefore, physiotherapists can plan a program that includes electrotherapy methods and isokinetic training, especially if they want to improve muscular endurance [29].
Advertisement
2. Limitations
When systematic reviews and meta-analyses were examined, it was determined that although isokinetic strength assessment is the gold standard, its general role is limited. However, best evidence syntheses, coupled with considerations of costs and the specialized training required to perform isokinetic strength testing, make this test difficult to use as a screening tool. For measurement, the patient who is being measured must be well informed and the professional who will make the measurement must be able to use the isokinetic dynamometer well. In addition, although measurements can be made in every region thanks to the apparatus in the device, it is difficult and time-consuming to use. Since the patient’s motivation to perform the movement comes into play during the measurement, there may be problems with measurement consistency.
Advertisement
3. Electrotherapy methods
Electrotherapy modalities are a popular treatment used by physiotherapists for a variety of purposes including muscle strengthening, endurance, spasticity management, pain control, circulation enhancement, and edema control [30]. Medium-frequency currents are typically 2 kHz or 4 kHz modulated alternating currents [31]. The kilohertz-frequency alternating current waveform is a sinusoidal, triangular, or rectangular-shaped biphasic current. They are transmitted continuously or in bursts. It is defined as a current with a carrier frequency of 1.0–10.0 kHz and is usually modulated with a low frequency (1–120 Hz) because continuous alternating current rapidly causes neuromuscular fatigue due to high frequency [32]. Medium-frequency currents have a carrier frequency (excitation without pauses in the pulse) and a modulation frequency (the number of times the current modulates or changes in one second). The currents must have an excitation and rest period to resemble a voluntary contraction. These values are adjustable, the unit is sec. The greater the pulse duration and frequency, the greater the contraction. Increasing these parameters will increase discomfort and fatigue [33]. In the classical literature, mid-frequency neuromuscular electrical stimulation includes Russian currents and interference currents [31]. Neo-Russian currents, which differ from traditional Russian currents in various technical aspects, are included in this list. Aussie currents, which have recently been more widely used and attracted attention, are among these currents [34].
Kilohertz alternating current was proposed in the pioneering work of Kots as a new type of neuromuscular electrical stimulation (NMES) that would address some of the limitations of conventional electrical stimulation. There is evidence to suggest that kilohertz alternating current (hereafter referred to as Russian current) increases maximal voluntary isometric contraction by up to 40%. It has been reported that kilohertz alternating current produces suprathreshold stimuli with bursts long enough to generate multiple nerve fiber action potentials, producing smaller perturbations per burst and more force than conventional NMES [32].
Advertisement
4. Russian current
Russian Current (RA) was developed by Yakov Kots in the late 1970s to strengthen the quadriceps of Russian Olympic athletes. RA was developed as an electrical muscle stimulation to increase strength gains [35]. The key feature of RA is its ability to produce a large muscle contraction with repetitive external loading [36].
RA is a medium frequency alternating current transmitted in bursts where the carrier frequency is between 1000 and 10,000 Hz and any burst frequency can be used. The RA protocol medium frequency alternating carrier frequency is 2500 Hz. It is a 50-burst modulated current per second during 10 msec rest and 10 msec stimulation. The theoretical basis for its use is that the skin provides less resistance to the high carrier frequency of 2500 Hz and the RA stimulates almost all motor units of the muscle to contract simultaneously leading to greater muscle hypertrophy. This allows less electrical energy to be dissipated peripherally and more electrical energy to penetrate the muscle and stimulate more fiber release [36]. RA has gained popularity among athletes with Kots’ reports of strength gain, 2500 Hz frequencies, 50 Hz bursts, and 50% duty cycle [37]. The RA protocol used in the clinic uses a medium frequency alternating current carrier frequency of 2500 Hz and a burst frequency of 50 bursts/second [38]. Akınoğlu et al. [39] evaluated isokinetic training with Russian current (RC) and high voltage pulsed current (HVPC) modality before and after treatment with isokinetic tests. Knee extension peak torque values 180°/sec before treatment RC is 161.60, HVPC is 157.50, after treatment, RC is 185.10, HVPC is 178.45. Quadriceps muscle 180°/sec muscular endurance before treatment RC is 72.02, HVPC is 69.88, post-treatment RC is 79.75, HVPC is 73.43. After the treatment, peak torque and muscular endurance increased.
Advertisement
5. Aussie current
Aussie Current (AC) is a 1 kHz or 4 kHz low-frequency alternating current that can modulate the duty cycle by 20%. Aussie currents are used in the clinic at 1000 Hz, modulated in 50 Hz ranges with a pulse duration of 2 msec [37]. AA can vary between 1 and 180 mA according to the sensitivity of the patient. A burst modulation frequency between 100 and 120 Hz is used for pain. It is a current that is rarely described in the physiotherapy literature, but its use as a way of increasing blood flow to the muscles as well as reducing pain has attracted attention [40].
Cittadino et al. [37] compared RA and AC applied to the hand in their study. Muscle strength and thickness of hand muscles were examined. In both evaluations, the average muscle thickness and effect sizes of the groups were determined as RA group 1.3 and AC group 1.7 in the first evaluation of the superficial flexors, and RA group 1.6 and AC group 1.7 after the treatment. The deep flexors were 1.7 in the RA group and 2.3 in the AC group at the first evaluation, and after treatment, they were 2.0 in the RA group and 2.3 in the AC group. No significant difference was found between the groups after treatment.
Dantas et al. [40] study, the authors compared RC and AC, as well as two other low-frequency currents with a phase duration of 200 or 500 us. The results showed that the maximum voluntary contraction torque applied in isolation was AC: 76.9%; and RC: 70.1%. Average torque AC: 92.1 percent; RC: 92.3 percent. There is no significant difference between the average torques. All currents are stated to produce similar levels of discomfort. Similar results were obtained by Ward et al., but both AC and RC have lower disturbance levels compared to low-frequency currents [41]. Medeiros et al. [42] also compared 1 and 4 kHz with two low-frequency currents with similar phase durations and observed that they presented similar levels of induced torque and discomfort. This form of treatment is relatively new and there are few studies examining its clinical effects. Current studies indicate that a new current, known as AC, can produce higher torque [43]. AC has a variety of therapeutic effects for individuals, including greater comfort, motor and sensory stimulation, and the capacity to produce greater muscle power torque [34]. Rodrigo et al. [43] reported that neuromuscular electrical stimulation provided by AC increased quadriceps muscle endurance in sedentary individuals and modulation with a 4 msec burst showed better effects. Dantas et al. [40] reported that Aussie current and low-frequency current were superior to Russian current for stimulating isometric knee extension torque. This information is thought to be important in making decisions regarding physiotherapy protocols for muscle strengthening [40]. AC has been reported to have better torque and force gains compared to other electrotherapy modulations. It causes less discomfort to the patient and shows higher individual tolerance (Table 1).
| Frequency (Hz) | Bursts (Hz) | Duty cycle (%) | Rest and stimulation | |
|---|---|---|---|---|
| Russian current | 2500 | 50 | 50 | 10 msec rest and 10 msec stimulation |
| Aussie current | 1000 | 50 | 20 | 2 msec stimulation |
Table 1.
Advertisement
6. Burst modality medium frequency currents (Russian and Aussie currents) in isokinetic training
The movement of the extremities in isokinetic training is performed at a predetermined speed during the joint movement process, except for the instantaneous acceleration at the beginning and deceleration at the end of the movement, known as isokinetic strength training [44]. Isokinetic training has been reported in research to be more effective than traditional isotonic training in restoring strength and balance between hamstrings and quadriceps. It causes better adaptations in muscle mass. Isokinetic training is among the most important methods in the development of functional mobility [28]. Vidmar et al. reported that isokinetic muscle strength training had a greater effect on muscle mass and strength of quadriceps femoris in recreational athletes after anterior cruciate ligament reconstruction than traditional training [10]. Some studies show that isokinetic training not only improves pain and dysfunction but also has a beneficial effect on the level of inflammatory biomarkers for college football players with traumatic osteoarthritis after anterior cruciate ligament injury and knee anterior cruciate ligament reconstruction revision patients [45, 46].
Isokinetic exercises are an exercise method used to increase muscle strength and improve performance.
These exercises are usually based on working with resistance and aim to work the muscles at maximum strength. The use of medium-frequency currents, especially Russian and Aussie currents in isokinetic training, provides muscle strength contraction and endurance, and increased blood circulation, along with certain physiological effects [29, 37]. Considering the health status of the person, existing injuries, or other health problems, Russ and Aussie currents can be used effectively in isokinetic training at appropriate levels under the guidance of a physician and physiotherapist.
From the literature review, it is seen that kHz current is a clinical alternative to add torque and muscle hypertrophy in healthy individuals. Although the force increase in the muscles occurs with other currents, it is seen that this increase occurs the most with the Russian current [47]. Since Aussie currents and Russian currents are similar in parameters, it is thought to be effective with isokinetic training. Although Aussie currents are few in the literature, no studies are used with isokinetic training. More research needs to be done on this subject. In addition, there are differences between the studies in terms of the parameters of the mid-frequency currents used. Therefore, more research can be done on current parameters.
Advertisement
7. Conclusions
Isokinetic training is a treatment modality used in the literature in the treatment of many diseases and is the best method for muscle strengthening. Burst modality medium frequency alternating currents are used in the literature. However, there are few studies conducted with isokinetic training. Although studies are showing that the Russian Current is effective among these currents, few studies are showing the effectiveness of Aussie currents. Since Aussie currents are more conformable than Russian currents, they can be used more frequently on patients.
Advertisement
Acknowledgments
We would like to inform you that this study is a part of the PhD Thesis by the first author, which was supported by the Muğla Sıtkı Koçman University Scientific Research Projects Coordination Office (Project Grant Number 21/125/01/3/4, and the title “Comparison of the Efficacy of Russian and Aussie Currents with Isokinetic Exercise in Individuals with Patellofemoral Pain Syndrome: Randomized Controlled Study”).
References
- 1.
Tugba K, Kaya E, Akinoglu B, Karaaslan Y, Un Yildirim N, Hasanoglu A. The effects of isokinetic strength training on strength at different angular velocities: A pilot study. Turkish. Journal of Sports Medicine. 2017; 52 (3):77-83. DOI: 10.5152/tjsm.2017.073 - 2.
McAlindon TE, Bannuru RR, Sullivan MC, Arden NK, Berenbaum F, et al. OARSI guidelines for the non-surgical management of knee osteoarthritis. Osteoarthritis and Cartilage. 2014, 2014; 22 (3):363-388. DOI: 10.1016/j.joca.2014.01.003 - 3.
Toprak EK, Ünver F, Kılıç Erkek Ö, Korkmaz H, Oymak B, Özdemir Y, et al. Aktif erkek bireylerde tek seans uygulanan izokinetik egzersizin DNA hasarı üzerine etkilerinin incelenmesi. Pamukkale Medical Journal. 2019; 12 (1):33-40. DOI: 10.31362/patd.46351 - 4.
Gökçen N, Benlidayı İC, Başaran S. Isokinetic test and exercises in knee osteoarthritis. Archives Medical Review Journal. 2015; 24 (2):228-238 - 5.
Coudeyre E, Jegu AG, Giustanini M, Marrel JP, Edouard P, Pereira B. Isokinetic muscle strengthening for knee osteoarthritis: A systematic review of randomized controlled trials with meta-analysis. Annals of Physical and Rehabilitation Medicine. 2016; 59 (3):207-215. DOI: 10.1016/j.rehab.2016.01.013 - 6.
Ghena DR, Kurth AL, Thomas M, Mayhew J. Torque characteristics of the quadriceps and hamstring muscles during concentric and eccentric loading. The Journal of Orthopaedic and Sports Physical Therapy. 1991; 14 (4):149-154. DOI: 10.2519/jospt.1991.14.4.149 - 7.
Brown R, Greig M. The influence of isokinetic dynamometer configuration on eccentric hamstring strength metrics: Implications for testing and training. Research in Sports Medicine. 2024; 32 (1):98-106 - 8.
Davies GJ, Ellenbecker TS, Andrews JR, Harrelson GL, Wilk KE. Application of isokinetics in testing and rehabilitation. Physical Rehabilitation of the Injured Athlete. 2004 - 9.
DA BVB. Isokinetic dynamometry applications and limitations. Sports Medicine. 1989; 8 (2):101-116 - 10.
Vidmar MF, Baroni BM, Michelin AF, Mezzomo M, Lugokenski R, Pimentel GL, et al. Isokinetic eccentric training is more effective than constant load eccentric training for quadriceps rehabilitation following anterior cruciate ligament reconstruction: A randomized controlled trial. Brazilian Journal of Physical Therapy. 2020; 24 (5):424-432. DOI: 10.1016/j.bjpt.2019.07.003 - 11.
Petrucci A, Guglielmino D, Pecci J, Pareja Galeano H. The effects of isokinetic training in athletes after knee surgery: A systematic review. The Physician and Sportmedicine. 2023:1-8 - 12.
Tsaklis P, Abatzides G. ACL rehabilitation program using a combined isokinetic and isotonic strengthening protocol. Isokinetics and Exercise Science. 2002; 10 (4):211-219 - 13.
Sekir U, Yildiz Y, Hazneci B, Ors F, Aydin T. Effect of isokinetic training on strength, functionality and proprioception in athletes with functional ankle instability. Knee Surgery, Sports Traumatology, Arthroscopy. 2007; 15 :654-664 - 14.
Zapparoli FY, Riberto M. Isokinetic evaluation of the hip flexor and extensor muscles: A systematic review. Journal of Sport Rehabilitation. 2017; 26 (6):556-566. DOI: 10.1123/jsr.2016-0036 - 15.
Bergamin M, Gobbo S, Bullo V, Vendramin B, Duregon F, Frizziero A, et al. Reliability of a device for the knee and ankle isometric and isokinetic strength testing in older adults. Muscles, Ligaments and Tendons Journal. 2017; 7 (2):323-330. DOI: 10.11138/mltj/2017.7.2.323 - 16.
Stark T, Walker B, Phillips JK, Fejer R, Beck R. Hand-held dynamometry correlation with the gold standard isokinetic dynamometry: A systematic review. PM & R: The Journal of Injury, Function, and Rehabilitation. 2011; 3 (5):472-479. DOI: 10.1016/j.pmrj.2010.10.025 - 17.
Habets B, Staal JB, Tijssen M, van Cingel R. Intrarater reliability of the Humac NORM isokinetic dynamometer for strength measurements of the knee and shoulder muscles. BMC Research Notes. 2018; 11 (1):15. DOI: 10.1186/s13104-018-3128-9 - 18.
Şahin Ö. Rehabilitasyonda izokinetik değerlendirmeler. Cumhuriyet Tıp Dergisi. 2010; 32 (4):386-396 - 19.
Muñoz-Bermejo L, Pérez-Gómez J, Manzano F, Collado-Mateo D, Villafaina S, Adsuar JC. Reliability of isokinetic knee strength measurements in children: A systematic review and meta-analysis. PLoS One. 2019; 14 (12):1-15. DOI: 10.1371/journal.pone.0226274 - 20.
Contreras-Díaz G, Chirosa-Ríos LJ, Chirosa-Ríos I, Intelangelo L, Jerez-Mayorga D, Martinez-Garcia D. Reliability of isokinetic hip flexor and extensor strength measurements in healthy subjects and athletes: A systematic review and meta-analysis. International Journal of Environmental Research and Public Health. 2021; 18 (21):11326-11329. DOI: 10.3390/ijerph182111326 - 21.
Borges O. Isometric and isokinetic knee extension and flexion torque in men and women aged 20-70. Scandinavian Journal of Rehabilitation Medicine. 1989; 21 (1):45-53 - 22.
Montgomery LC, Douglass LW, Deuster PA. Reliability of an isokinetic test of muscle strength and endurance. The Journal of Orthopaedic and Sports Physical Therapy. 1989; 10 (8):315-322. DOI: 10.2519/jospt.1989.10.8.315 - 23.
Dvir Z. Clinical applicability of isokinetics: A review. Clinical Biomechanics (Bristol, Avon). 1991; 6 (3):133-144. DOI: 10.1016/0268-0033(91)90024-K - 24.
Saral I, Agirman M, Basat H, Surucu S, Mahirogullari M, Cakar E. A comparison of isokinetic muscle strength in patients with chondromalacia patella: A cross-sectional study. European Review for Medical and Pharmacological Sciences. 2022; 26 (21):7771-7778. DOI: 10.26355/eurrev_202211_30126 - 25.
Arhos E, Ito N, Giordana A, Nolan JRTP, Snyder-Mackler L, Silberagel KG. Who’s afraid of electrical Stimülation? Let’s Re-visit the application of NMES at the knee. Journal of orthopaedic sports. Physical Therapy. 2024; 54 (2):1-6 - 26.
Carvalho MTX, Guesser Pinheiro VH, Alberton CL. Effectiveness of neuromuscular electrical stimulation training combined with exercise on patient-reported outcomes measures in people with knee osteoarthritis: A systematic review and meta-analysis. Physiotherapy Research Internationa. 2023; 29 (1):e2062 - 27.
Yeşilöz Ö, Aksoy MH. The effectiveness of peroneal nerve stimulation combined with neuromuscular electrical stimulation in the management of knee osteoarthritis: A randomized controlled single-blind study. Turkish Journal of Physical Medicine and Rehabilitation. 2023; 69 (3):317 - 28.
Petrucci A, Guglielmino D, Pecci J, Pareja GH. The effects of isokinetic training in athletes after knee surgery: A systematic review. The Physician and Sportsmedicine, (just-accepted). 2023 - 29.
Akıncıoğlu B, Kocahan T. Russsian current versus high voltage current with isokinetic training on the quadriceps muscle strength and endurance. Journal of Exercise Rehabilitation. 2020; 16 (3):272 - 30.
AR Lucas-Toumbourou S, McCarthy B. A comparison of the analgesic efficacy of medium-frequency alternating current and TENS. Physiotherapy. 2009; 95 (4):280-288. DOI: 10.1016/j.physio Ward.2009.06.005 - 31.
Ward AR, Robertson AW, Sensory RVJ. Sensory, motor, and pain thresholds for stimulation with medium frequency. Alternating Current. 1998; 79 :273-278. DOI: 10.1016/S0003-9993(98)90006-5 - 32.
Vaz MA, Frasson VB. Low-frequency pulsed current versus kilohertz-frequency alternating currents: A scoping literatüre review. Archives of Physical Medicine and Rehabilitation. 2018; 99 (4):792-805. DOI: 10.1016/j.apmr.2017.12.001 - 33.
Becher M, Springer S, Braun-Benyamin O, Laufer Y. The effect of an ınterphase ınterval on electrically ınduced dorsiflexion force and fatigue in subjects with an upper motor neuron lesion. Artificial Organs. 2016; 40 (8):778-785. DOI: 10.1111/aor.12698 - 34.
Baptista GB, Cardoso J, Ferreira B. Comparative analysis of the effect between FES, RUSSA, and AUSSIE therapeutic currents in individuals with hypertonia spastic post-stroke case study. British Journal of Medicine and Medical Research. 2017; 19 (8):1-9. DOI: 10.9734/BUMMER/2017/30644 - 35.
Lima EPF, Rodrigues GBOO. A Estımulação Russa No Fortalecımento Da Musculatura Abdomınal. ABCD. Arquivos Brasileiros de Cirurgia Digestiva (São Paulo). 2012; 25 (2):125-128 Erişim Adresi: scielo.br/j/abcd/a/XhQcdtsdPqtHr5PnQ7Bn4tc/abstract /?lang=pt - 36.
Şahan N. Diz osteoartritli hastalarda quadriceps femoris kasına uygulanan iki farklı elektroterapi akımının etkilerinin karşılaştırılması. Journal of Exercise Therapy and Rehabilitation. 2020; 7 (2):109-118. Erişim Adresi: dergipark.org.tr/en/pub/jetr/issue/56637/577905 - 37.
Cittadin GL, Ansolin GZ, Furtado Santana NP, Tonini TL, Buzanello Azevedo MR, de Albuquerque CE, et al. Comparison between Russian and Aussie currents in the grip strength and thickness muscles of the non-dominant hand: A double-blind, prospective, randomized-controlled study. Turkish Journal of Physical Medicine and Rehabilitation. 2020; 66 (4):423-428. DOI: 10.5606/tftrd.2020.4718 - 38.
Ganesh GS, Kumari R, Pattnaik M, Mohanty P, Kaur P, Dakshinamoorthy A. Effectiveness of faradic and Russian currents on plantar flexor muscle spasticity, ankle motor recovery, and functional gait in stroke patients. Physiotherapy Research International. 2018; 23 (2):1-8. DOI: 10.1002/pri.1705 - 39.
Akinoglu B, Kocahan T. Russian current versus high voltage current with isokinetic training on the quadriceps muscle strength and endurance. Journal of Exercise Rehabilitation. 2020; 16 (3):272-278. DOI: 10.12965/jer.2040260.130 - 40.
Dantas LO, Vieira A, Siqueira ALJ, Salvini TF, Durigan JLQ. Comparison between the effects of 4 different electrical stimulation current waveforms on isometric knee extension torque and perceived discomfort in healthy women. Muscle & Nerve. 2015; 51 (1):76-82. DOI: 10.1002/mus.24280 - 41.
Ward AR, Oliver WG, Buccella D. Wrist extensor torque production and discomfort associated with low-frequency and burst-modulated kilohertz-frequency currents. Physical Therapy. 2006; 86 :1360-1367 - 42.
Medeiros FV, Bottaro M, Vieira A, Lucas TP, Modesto KA, Bo APL, et al. Kilohertz and low-frequency electrical stimulation with the same pulse duration have similar efficiency for inducing isometric knee extension torque and discomfort. American Journal of Physical Medicine & Rehabilitation. 2017; 96 :388-394 - 43.
de Carvalho AR, Reginato A, Reginato GA, Schuck KSR, Neves M, Bertolini GRF. Aussie current and quadriceps muscle endurance: A randomized clinical trial. Sport Sciences for Health. 2023; 19 (2):565-572 - 44.
Ren Y, Yue T, Qi F. Isokinetic strength training improves motor function in a Chinese classical dancer with knee injury: A case repost. In: 2021 International Conference on Health Bih Data and Smart Sports(HBDSS). Guilin, China. 2021. pp. 60-64. DOI: 10.1109/HBDSS54392.2021.00020 - 45.
Nambi G. Effects of isokinetic knee muscle training on bone morphogenetic proteins and inflammatory biomarkers in post-traumatic osteoarthritis after anterior cruciate ligament injury: A randomized trial. Journal of Rehabilitation Medicine. 2020:9 - 46.
Lee SEK, de Lira CAB, Nouailhetas VLA, Vancini RL, Andrade MS. Do isometric, isotonic and/or isokinetic strength training produce different strength outcomes. Journal of Bodywork and Movement Therapies. 2018; 22 :430-437 - 47.
Ke P, Pereira KL, Stachelski RA, Azevedo MRB, De Crvallo AR, Bertolini GRF. KiloHertz currents on aspects of muscle function: A scoping review. Journal of Bodywork and Movement Therapies. 2022; 32 :110-119