
Abstract
Loneliness could both precede and follow poor mental health of adolescents. Since the last decade, the mental health problems in adolescence have become widespread and heavier; it is important to address what role loneliness has in predicting and maintaining mental health problems. This chapter summarizes research data that connect loneliness with specific internalizing problems in adolescence–non-suicidal self-injury, suicidal thoughts, and attempts and deliberate self-harm, with or without suicidal intention. Findings of different studies are discussed in the context of the interpersonal theory of suicide, the integrated motivational-volitional model of suicidal behavior, Nock’s integrated theoretical model of NSSI, as well as the evolutionary theory of loneliness. Since the COVID-19 pandemic and resulting public health measures had major impacts on mental health, including on self-harm, and as loneliness increased due to social distancing and isolation, practical implications for the future crisis are proposed in order to save adolescents’ mental health.
Keywords
- loneliness
- non-suicidal self-injury (NSSI)
- deliberate self-harm (DSH)
- suicide
- peer relations
- adolescence
1. Introduction
Adolescence represents a developmental phase marked by an escalation in internalizing issues, such as depression and anxiety, as well as an elevated risk of engaging in self-aggressive behaviors like self-injury and suicidal tendencies [1, 2]. Over the past decade, the prevalence and severity of mental health problems during adolescence have intensified [3, 4]. Addressing the role of loneliness in predicting and perpetuating mental health problems is crucial in light of these trends. This chapter seeks to elucidate the relationship between loneliness and specific manifestations of self-harm and internalizing problems in adolescence, such as non-suicidal self-injury (NSSI), suicidal ideations and attempts, and deliberate self-harm, with or without suicidal intent. Despite their distinctiveness and varied operationalizations, these issues often intertwine, and the boundary between NSSI and suicidality is frequently indistinct during adolescence. Huang et al. [5] emphasize the intricate connection between NSSI and suicide, highlighting its significance as a substantial public health concern that jeopardizes the daily lives and both the physical and mental well-being of adolescents.
Suicide stands out as a leading cause of death among individuals aged 10–24 years [6, 7], with suicidality in childhood serving as a predictor for adult psychiatric morbidity, mortality, and general mental health challenges [8]. Nock et al. [9] report that one-third of adolescents with suicidal ideation progress to developing a suicide plan, and approximately 60% of those with a plan attempt suicide. NSSI typically emerges between the ages of 11 and 15 years [10, 11], with lifetime prevalence ranging from 8 to 47% in community samples during adolescence [1, 11, 12, 13] and an annual incidence of around 19% [14]. Despite NSSI’s exclusion of suicidal intent by definition, various researchers have identified a direct association between deliberate self-harm and suicide attempts [13]. Adolescence is additionally characterized by a heightened incidence of loneliness. The adolescent experience of loneliness differs from that of children or adults, given developmental changes in identity, autonomy, individuation, and social orientation [15]. Loneliness, generally described as an unpleasant and distressing subjective experience, occurs when an individual perceives a lack of acceptance, isolation, or a dearth of contact with others [16, 17]. It is crucial to recognize that quantitative aspects of social isolation inadequately measure loneliness and the absence of social support and connections [18]. Both those with numerous friends and those without it may experience loneliness. Nevertheless, adolescents struggling to form and maintain positive peer relationships or dissatisfied with such relationships tend to report heightened loneliness [19]. Scholars debate whether loneliness is a unidimensional or multifaceted construct, with emotional loneliness linked to deficiencies in family or romantic bonds and social loneliness related to friendships. Additionally, they differentiate between current and prolonged (chronic) loneliness, with the latter posing an increased risk of mental health problems due to its interference with social, cognitive, and physiological development [15]. The Centers for Disease Control and Prevention [20] posit that connectedness, as the antithesis of loneliness, is a vital factor influencing suicidal behavior. Connectedness is described as a sense of interpersonal closeness with the broader social world or individuals, characterized by feelings of caring, belonging, trust, value, and respect. It also entails satisfaction with one’s environment or relationships [21]. A consensus exists that connectedness derives from interpersonal affiliations with individuals and institutions, providing emotional and instrumental support through interconnected social systems (e.g., families, schools, peer groups, and communities). Social connection refers to an individual’s subjective perception of the closeness of their interpersonal relationships in social life [5]. The CDC’s emphasis on enhancing connectedness as a comprehensive framework for suicide prevention underscores the fundamental importance of social connection in human well-being, guiding research, intervention, and policy efforts capable of accommodating diverse approaches [21]. In recent years, particularly during and after the COVID-19 pandemic, numerous studies have affirmed a connection between the mental well-being of adolescents, feelings of loneliness, and their sense of social connectedness. A comprehensive study in Hungary [22] focusing on adolescents and young adults revealed that students with fewer friends who frequently experience loneliness face an increased likelihood of feeling hopeless, thereby jeopardizing their mental health. Females and younger adolescents are identified as being at a higher risk of poor mental health. Amid the pandemic lockdown, adolescents reporting heightened loneliness exhibited significantly more pronounced symptoms of mental health issues [23]. Moreover, individuals with low levels of school and peer connectedness prior to the pandemic demonstrated poorer mental health and well-being both during the lockdown and shortly after returning to school [24, 25]. An Australian study emphasized the predictive nature of quality friendships before the COVID-19 school closures on elevated levels of positive mental well-being during that period. However, despite these positive connections, there were notable increases in depression symptoms, internalizing and externalizing symptoms, as well as a considerable decrease in positive mental well-being at various points over time (before, during, and after the pandemic) [26].
While these studies are primarily centered on the COVID-19 pandemic, earlier research has consistently highlighted the strong association between loneliness and various mental health problems, including depression, anxiety, and suicidal thoughts. Loneliness is also identified as a risk factor for adolescents engaging in health-risk behaviors such as tobacco and alcohol use, as well as risky sexual activities, social-environmental risk factors like bullying, and overall lower positive mental health and self-esteem [27, 28].
The subsequent chapter delves into different theoretical approaches explaining the link between loneliness and specific mental health issues such as suicidality and non-suicidal self-injury (NSSI). Subsequently, pertinent empirical data on these topics are presented, and finally, practical implications derived from these results are addressed.
2. Theoretical approaches that explain the relationship between loneliness and suicidality
Already in the nineteenth century, French sociologist Durkheim (1897) [21] proposed that suicide arises from a lack of social connection to others. This chapter delves into four contemporary theories connecting loneliness and suicidality, including non-suicidal self-harm behaviors such as NSSI. All these theories have emerged more than a century after Durkheim’s initial hypothesis.
Foremost among these theories is the
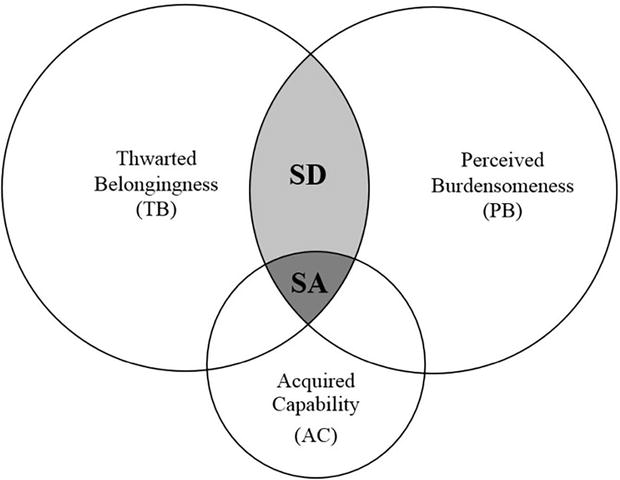
Figure 1.
The interpersonal theory of suicide by Joiner [
The Integrated motivational volitional model of suicidal behavior (IMV) [30] (Figure 2 in Appendix) aligns with the notion that loneliness precedes suicidal ideation [31]. The IMV model identifies three phases of suicidality: (1) pre-motivational, incorporating background factors (e.g., family suicide) and triggering events (e.g., traumatic incidents); (2) motivational, where suicidal ideation forms through feelings of defeat, humiliation, and entrapment; and (3) volitional, culminating in suicidal behavior enactment. Thwarted belongingness, a motivational moderator in IMV, moderates the relationship between entrapment and suicidal ideation. Loneliness also significantly moderates between defeat and entrapment [31], implying that lonely individuals experiencing defeat are more prone to entrapment and subsequent suicidal ideation. Conversely, strong social connections act as a protective factor, weakening the links between humiliation/defeat and entrapment and between entrapment and suicidality.

Figure 2.
The integrated motivational-volitional model of suicidal behavior by O’Connor and Kirtley [
Regarding NSSI, Nock [32] formulated the Integrated theoretical model of NSSI (Figure 3 in Appendix), asserting that social relational distress may prompt NSSI engagement, serving the positive social function of obtaining support or enhancing affiliation with others. This model highlights two crucial relationships between the interpersonal context and NSSI. In the first place, negative interpersonal experiences, including loneliness, often precede NSSI. Behaviorally, loneliness can be characterized by greater use of expressive suppression and regulating emotions by actively rejecting or withdrawing from others [33]. This means that both interpersonal vulnerability factors (such as poor distress tolerance and poor emotional regulation that are connected to loneliness) and interpersonal vulnerability factors (poor communication skills and social problem-solving that are typical for isolated children) simultaneously lead to inappropriate stress response and, according to, for example, self-punishment hypothesis [32] results in NSSI. On the other hand, NSSI behaviors resulting from relational distress could be accompanied by desired consequences such as companionship, support, or intimacy, emphasizing high friendship quality, which is posited in social signaling hypothesis [32]. Thus, loneliness can exhibit both positive and negative connections to NSSI, as demonstrated in subsequent research findings.

Figure 3.
Integrated theoretical model of the development and maintenance of self-injury [
Lastly, the Evolutionary theory of loneliness (ETL) [34] elucidates the processes underlying loneliness. The theory posits that feelings of loneliness emerge and persist over time, affecting physiological and mental health, including suicidal behavior and NSSI. Loneliness, according to ETL, operates through a social distress mechanism, motivating individuals to repair and maintain social ties [35]. Loneliness is considered a signaling function akin to physical pain, with an innate human desire to connect with others for protection against potential threats. Failure to fulfill this need for social connection results in reported feelings of loneliness [36]. Loneliness can impact friendship quality negatively, as evidenced by associations with poor social skills or negative cognitive biases leading to unfavorable friendship experiences [37]. Simultaneously, the feeling of loneliness may motivate adolescents to seek close connections with peers, as observed in the Integrated Theoretical Model of NSSI.
In summary, humans possess a strong need and desire for connection with others, and thwarting this need leads to feelings of loneliness. Loneliness signals the absence or threat to vital social bonds, prompting individuals to either repair existing social ties or establish new relationships. While some individuals successfully reconnect, thereby resolving the situation, prolonged or chronic loneliness occurs when individuals fail to establish or re-establish social ties. This chronic loneliness can trigger adverse cognitive and physiological processes detrimental to health and well-being [15], including NSSI and suicidal behaviors.
3. Research findings connecting loneliness with NSSI and suicidality
Adolescents’ encounters with solitude significantly influence cognition, emotion, and behavior, with notable implications for mental health [5]. Loneliness has been consistently linked to non-suicidal self-injury (NSSI) and suicidal tendencies, as validated by various studies explored in this chapter. A meta-analysis by McClelland et al. [38] affirms that heightened loneliness correlates with increased individual NSSI, establishing an independent prospective link between loneliness and self-injurious behavior [31]. Those experiencing loneliness are more prone to reporting suicidal thoughts and behaviors compared to their counterparts [18]. This narrative review emphasizes the substantial impact of both objective conditions (e.g., being alone) and the subjective experience of loneliness on suicidal outcomes, particularly suicidal attempts (SA) and ideations (SI). Loneliness emerges as a consistent transcultural factor associated with both SI and SA.
Numerous observational studies reinforce the positive association between social isolation constructs and suicidal outcomes [18]. For instance, a cohort study tracking 832 American children until adolescence reveals that persistent and escalating loneliness in early life predicts SI at age 15 [39]. The Global School-Based Student Health Surveys (GSHS) data from 32 countries, analyzed by McKinnon et al. [40], identifies loneliness as a primary risk factor for SI and suicidal plans (SP), surpassing factors like limited parental support and bullying. Loneliness also surfaces as a risk factor for deliberate self-harm among adolescents in a national Finnish study [41]. However, a European study by Brunstein Klomek et al. [42] reports that loneliness is specifically linked to repetitive direct self-injurious behavior, but not occasional instances. It could be assumed that repetitive NSSI is a product or symptom of more serious mental health problems, which are connected also with poorer social functioning, resulting in higher levels of loneliness. On the other hand, occasional NSSI could be result of poor coping, attention seeking, social imitation of peer’s habits, and it is not necessarily connected with social problems and loneliness.
Loneliness and suicidality often intertwine with mental health problems such as depression and traumatic social issues like bullying. Depression and loneliness emerge as crucial risk factors for suicidality across age groups, with depression acting as a mediator between academic stress, loneliness, and subsequent suicidal behavior [38]. That means that children and youth who experience loneliness are at a greater risk of becoming depressed, and one of the ways of dealing with that depression could be engaging in NSSI and/or having suicidal thoughts and behaviors. Moreover, longitudinal studies, such as the one by Lin et al. [43], uncover the mediating effect of self-esteem and the moderating effect of peer attachment on the relationship between cybervictimization and NSSI among Chinese adolescents. High peer attachment, resulting with lower feeling of loneliness, mitigates the negative effects of cybervictimization, safeguarding self-esteem and reducing the likelihood of NSSI.
The role of loneliness in NSSI is complex, with studies suggesting bidirectional associations and potential mediating factors. For instance, Gandhi et al. [44] reveal that individuals engaging in NSSI report higher levels of parent-related loneliness, even after accounting for age, gender, and depression. Adolescents who have engaged in NSSI throughout their lives also indicated elevated levels of loneliness linked to peers, even when considering gender and age as controlling factors. The association between peer-related loneliness and NSSI might be influenced by depression and other mental health problems, as previously discussed. Physiologically, chronic loneliness can activate the Hypothalamo-Pituitary–Adrenal (HPA) axis, leading to persistent cortisol elevation and potential DNA methylation aberrations, increasing vulnerability to NSSI. Different facets of loneliness have been explored in relation to adolescent suicidality and NSSI. Social and family loneliness are significantly associated with poorer mental well-being (i.e., depression and suicidal ideation), while social and romantic loneliness are more strongly linked to eating disorders and self-harm [45]. Moreover, loneliness was a stronger moderator between entrapment and suicidal ideation than between defeat and entrapment, which is in accordance to earlier mentioned IMV model. In another study, depression partially mediated between family loneliness and global loneliness in relation to suicidal ideation, and at the same time, it fully mediated between romantic loneliness and suicidal ideation [31]. The integrated theoretical model of NSSI by Nock provides a framework for understanding the interplay of psychological resilience and loneliness in the context of child maltreatment and NSSI [46]. Child maltreatment had an indirect impact NSSI, with both psychological resilience and loneliness serving as mediators. Children who experience maltreatment in the family are less resilient; they isolate themselves from friends and became lonely due to both weak relationships with their parents and with peers, and as a result, they feel lonely. The product of this psychological state could be NSSI. These results provide theoretical support for inhibiting adolescents’ NSSI by promoting psychological resilience and reducing the feeling of loneliness.
In the cross-sectional study using data from a nation-wide survey of high school students in Denmark (29,086 students) [47], each type of social disconnectedness was positively associated with mental health problems (including suicidal ideation and non-suicidal self-injury) and negatively associated with mental well-being. In all cases, the presence of loneliness played a significant mediating role in the connections observed. Adolescents facing various forms of social disconnectedness within the school environment, such as a lack of support from classmates or teachers, absence of class social cohesion, or not feeling integrated into the school community, demonstrated an increased susceptibility to mental health issues. Notably, inadequate support from classmates emerged as the most influential factor, followed by insufficient support from teachers or a sense of exclusion from the broader school community, in relation to the majority of the assessed outcomes [15]. Conclusively, when adolescents’ social support networks are disrupted, additional risk factors, such as loneliness and/or depression, may increase their NSSI and suicidal behavior [5].
Exploring the role of self-control in the context of loneliness and mental health, Huang et al. [5] find a positive correlation between self-control and adolescent loneliness and NSSI. Self-control mediates the relationship between loneliness and NSSI, while social connection moderates this relationship. The lack of self-control is associated with increased loneliness, potentially leading to social exclusion and diminished self-control once more. This impact of self-control could be understood also through emotional regulation (children with external locus of control also have poorer emotional regulation strategies), which we already discussed as related to NSSI.
Loneliness appears to have a dual relationship with the mental health of adolescents, both preceding and following periods of poor mental health. The connection between loneliness and NSSI is likely bidirectional. Psychologically, loneliness can disrupt self-regulatory mechanisms (such as emotional regulation), prompting individuals to engage in behaviors they would otherwise avoid just to alleviate the negative affect associated with loneliness [44]. Conversely, involvement in NSSI may lead to feelings of shame, guilt, and regret, intensifying social isolation. Beyond the emotional consequences, the physical impact of NSSI, coupled with the fear of stigmatization, can further contribute to social isolation. NSSI is often stigmatized, with potential negative repercussions for mental health and social relationships [48]. It can serve as a trigger for relationship issues, as it may be disapproved of and perceived as deviant, resulting in avoidance, isolation, or rejection. Research by De Luca et al. [49] with thirteen-year-olds in the USA highlighted that NSSI consistently elevated the risk of various peer problems. Adolescents engaging in NSSI may shape their social environment in a manner that deprives them of positive social contexts crucial for their development. Consequently, NSSI may heighten the risk of victimization and, through increases in depressive symptoms, contribute to heightened stress within friendships [49]. On the contrary, Wang et al. [37] conducted a comparison between adolescents who were either left in the care of others (social welfare system) or remained with their parents. Their findings indicated that loneliness could impact friendship quality both negatively and positively, mediated by NSSI. Increased loneliness predicted higher instances of NSSI, which, in turn, correlated with elevated friendship quality among left-behind adolescents. This outcome contributes to the existing literature on the interpersonal function of NSSI [50], suggesting that left-behind adolescents may employ NSSI as a means to reinforce their friendships when experiencing loneliness. This positive consequence of NSSI could be especially evident among youth in care because children in children homes and foster families are those who have mental health problems more often and where self-injury behavior is more expected. In one way, these problematic behaviors serve as signs of help-seeking and provide more prominent attention and help from others (both children and adults). If the help is assured, mental health problems could diminish. Moreover, while social connection is a fundamental human need, parental absence, as experienced by left-behind adolescents, may diminish the emotional bond between parents and children, leading to heightened feelings of loneliness. As peers become a significant aspect of social relationships for adolescents, those who lack an intimate parent–child connection, such as left-behind adolescents, are inclined to seek close emotional bonds with their friends. In alignment with the interpersonal function, they might use NSSI to evoke concern from their friends or share it as a secret, thus strengthening their friendships through such self-disclosure [49].
In the context of the COVID-19 pandemic, loneliness and mental health problems, particularly among adolescents, have gained increased attention. The pandemic, with its associated social distancing and isolation measures, has intensified loneliness, leading to a surge in self-harm presentations by children globally [51]. Prolonged isolation can induce severe depression and loneliness, providing a motivation for self-harm as a means to alleviate inner pain [5]. Despite the effectiveness of regulations in protecting physical health, changes in social interaction during the pandemic have contributed to increased distress, perceived loneliness, and a decline in mental health [36]. Social isolation, even when voluntary, poses a risk to mental well-being, particularly during a pandemic such as COVID-19.
In summary, the scientific literature reviewed here underscores the intricate relationship between loneliness, NSSI, and suicidal tendencies among adolescents. The bidirectional nature of this association, along with various mediating and moderating factors, highlights the complexity of these phenomena. Understanding these relationships is crucial for developing effective interventions to promote mental health and prevent self-harming behaviors among adolescents.
4. Practical implications of presented data regarding loneliness and suicidality in adolescence
The CDC’s emphasis on enhancing connectedness as a comprehensive guiding framework for suicide prevention is rooted in a foundational recognition of the pivotal role of social connection in human well-being. This approach has paved the way for research, interventions, and policies capable of accommodating diverse strategies [21]. In this final section, we will delve into practical implications aimed at preserving and enhancing adolescents’ mental health, with a specific focus on reducing loneliness.
To address loneliness effectively, four primary strategies have been delineated: (1) developing or refining social skills, (2) augmenting social support, (3) increasing opportunities for social contacts, and (4) targeting maladaptive social cognition [52]. In order to fulfill these tasks and to combat adolescent loneliness, there should be a vivid collaboration of different stakeholders through different institutions. In the first place, schools play a crucial role as major partners in promoting the mental health of children and adolescents, ensuring reach to all students, not solely those with recognized issues. Loneliness often goes unnoticed, underscoring the necessity for preventive programs emphasizing peer group belonging, particularly in school settings, with family involvement being another valuable approach [49].
Balanced approaches encompass both school-focused strategies and individual-level interventions, including enhancing self-control, building self-esteem, and acquiring effective coping strategies. Universal, school-based programs like the Youth Aware of Mental Health (YAM) can mitigate stigma, raise mental health awareness, and enhance overall support, as well as equip youth with emotion regulation and problem-solving skills [53]. When intervening in adolescent NSSI and suicidality, prioritizing the strengthening of social connections between adolescents and their peers is crucial in overcoming mental health challenges [5]. Positive relationships contribute to loneliness reduction, fostering self-confidence and instilling a sense of belonging.
Furthermore, in the school context, there is a need to foster openness among adults regarding taboo topics such as NSSI and suicide. Schools with strong social networks connecting adults with adolescents offer more avenues for help-seeking and help-giving interactions compared to those lacking such networks [54]. Developing competent adults capable of detecting and responding to students’ distress is essential. The connectedness between youth and adults enhances opportunities for soliciting and activating assistance, increases the likelihood of noticing signs of distress, and provides a sense of utility, meaning, and purpose [21]. Studies within mental health services literature underscore that strong ties with adults in key social settings enhance adolescents’ willingness to seek help for emotional problems, including suicide concerns [54].
Given that parents are primary facilitators of professional services and assistance, their awareness and willingness to identify problems are critical [55]. Linkages between social systems, such as those involving schools and families, are crucial for early detection and response to adolescents facing difficulties. Adolescents experiencing low connectedness across multiple social contexts are less likely to be noticed and assisted in times of distress [21]. Early detection of loneliness in young people by caregivers and teachers emerges as a logical initial step for youth suicide prevention programs [51].
Still, educational and health system are not enough. Social policy should empower social welfare system to, first, recognize and then appropriately approach youth who are in greater risk of being lonely and have mental health problems. In literature, we can recognize different groups of young people who have more mental health problems and are more isolate than their (privileged) peers—for example, those with different physical disabilities [56, 57], who are raised in financial deprived families [13, 57], those who are placed in institutions or foster families [37], and LGBTQ+ youth [58, 59]. These minor groups of children and adolescents should get priority in strategic action plans of reducing loneliness and building adolescents’ mental health.
Finally, in the context of future global crises, such as the COVID-19 pandemic, it is imperative to incorporate considerations for mental health alongside physical well-being and to develop a tailored mental health intervention plan. This is particularly significant in the case of children and adolescents, where their social interactions play a pivotal role in overall well-being and mental health. Consequently, any health prevention measures implemented should carefully account for and avoid interference with the primary developmental tasks integral to this phase of their lives. More concretely, in this pandemic, adolescents who had closer relationships with their parents and those who experienced connectedness with peers and adults reported significantly fewer severe symptoms of mental health difficulties and lower levels of loneliness during the period of isolation [23, 60]. Additionally, students who attended school virtually had more mental health problems (including suicide attempts) than those attending school in-person [61], and a large part of this difference could be explained by school and family connectedness. From these results, we can conclude that future crisis policies and strategies should, on one hand, aim to protect children who are not safe in their own homes and for whom home isolation puts them at a greater risk of adverse experiences. On the other hand, future strategies should provide adolescents with opportunities to connect and stay in touch with their peers in the school setting.
5. Conclusion
In conclusion, this comprehensive exploration has delved into the intricate relationship between loneliness and self-harm behaviors, particularly in the context of adolescence. The prevalence and severity of mental health problems during this developmental phase have heightened in recent years, making it imperative to understand the role of loneliness in predicting and perpetuating these challenges. Loneliness, a subjective and distressing experience, manifests uniquely in adolescence due to developmental changes in identity, autonomy, and social orientation.
The Centers for Disease Control and Prevention (CDC) advocate for connectedness as a crucial factor influencing suicidal behavior, emphasizing the importance of social bonds in human well-being. This guiding framework has shaped research, interventions, and policies capable of accommodating diverse strategies. The theoretical perspectives presented, including the Interpersonal theory of suicide, the Integrated motivational volitional model of suicidal behavior, the Integrated Theoretical model of NSSI, and the Evolutionary theory of loneliness, collectively contribute to understanding the complex interplay between loneliness and self-harm behaviors.
Research findings corroborate the positive association between loneliness and non-suicidal self-injury (NSSI) as well as suicidal tendencies among adolescents. The bidirectional relationship, coupled with various mediating and moderating factors, underscores the complexity of these phenomena. The impact of loneliness on mental well-being extends beyond the individual, influencing social and family dynamics, friendships, and overall psychological resilience.
Practical implications derived from the presented data highlight the importance of school-focused and individual-level interventions to address loneliness effectively. Strategies such as developing social skills, augmenting social support, increasing opportunities for social contacts, and targeting maladaptive social cognition emerge as key components. Schools, as major partners in promoting mental health, need to foster openness among adults, encourage strong social networks, and develop competent individuals capable of detecting and responding to distress.
Parental awareness and willingness to identify problems are critical, emphasizing the need for linkages between social systems to facilitate early detection and response to adolescents facing difficulties. The early detection of loneliness in young people, particularly in the school setting, emerges as a logical initial step for youth suicide prevention programs.
In the context of the COVID-19 pandemic, the heightened focus on loneliness and mental health problems among adolescents underscores the need for adaptive interventions. The pandemic-induced social distancing and isolation measures have intensified loneliness, contributing to a surge in self-harm presentations. Acknowledging the complexity of these challenges, understanding the bidirectional relationship between loneliness and self-harm, and implementing multifaceted interventions are essential for promoting the mental health and well-being of adolescents.
In summary, this exploration contributes to the ongoing discourse on adolescent mental health, emphasizing the centrality of addressing loneliness as a preventive measure against self-harm behaviors. The multifaceted strategies and interventions discussed aim to create a holistic approach that recognizes the interconnectedness of social, psychological, and environmental factors influencing adolescents’ mental well-being.
Acknowledgments
This chapter was funded by the Croatian Science Foundation, and it is part of the scientific project Family Economic Hardship, Psychosocial Problems and Educational Outcomes of Adolescents in the Time of Economic Crisis, led by PhD Marina Ajduković.
References
- 1.
Klonsky DE, Muehlenkamp J, Lewis S, Walsh B. Nonsuicidal self-injury advances in psychotherapy evidence-based practice [Internet]. Available from: https://pubengine2.s3.eu-central-1.amazonaws.com/preview/99.110005/9781616763374_preview.pdf - 2.
Miller DN. Child and Adolescent Suicidal Behaviour – School Based Prevention, Assessment and Intervention. New York, London: The Guilford Press; 2011 - 3.
Rezo Bagarić I, Sušac N, Rajhvajn BL. Samoozljeđivanje i suicidalnost srednjoškolaca prije i tijekom pandemije COVID-19. Socijalna Psihijatrija. 2023; 51 (1):3-29 - 4.
Blomqvist I, Henje Blom E, Hägglöf B, Hammarström A. Increase of internalized mental health symptoms among adolescents during the last three decades. European Journal of Public Health. 2019; 29 (5):925-931 - 5.
Huang X, Liu H, Lan Z, Deng F. The effect of loneliness on non-suicidal self-injury behavior in Chinese junior high school adolescents: A moderated mediation model. Psychology Research and Behavior Management. 2023; 16 :1831-1843 - 6.
Bachmann S. Epidemiology of suicide and the psychiatric perspective. International Journal of Environmental Research and Public Health. [Internet]. 2018; 15 (7):1425. Available from:https://www.mdpi.com/1660-4601/15/7/1425 - 7.
Curtin SC, Heron M. Death rates due to suicide and homicide among persons aged 10-24: United States, 2000-2017. In: NCHS Data Brief, No. 352. Hyattsville, MD: National Center for Health Statistics; 2019. Available from: https://www.cdc.gov/nchs/data/databriefs/db352-h.pdf - 8.
Copeland WE, Goldston DB, Costello EJ. Adult associations of childhood suicidal thoughts and Behaviors: A prospective, longitudinal analysis. Journal of the American Academy of Child & Adolescent Psychiatry. 2017; 56 (11):958-965.e4 - 9.
Nock MK, Green JG, Hwang I, McLaughlin KA, Sampson NA, Zaslavsky AM, et al. Prevalence, correlates, and treatment of lifetime suicidal behavior among adolescents. JAMA Psychiatry. 2013; 70 (3):300 - 10.
Rodav O, Levy S, Hamdan S. Clinical characteristics and functions of non-suicide self-injury in youth. European Psychiatry [Internet]. 2014; 29 (8):503-508. Available from:https://www.sciencedirect.com/science/article/pii/S0924933814000418 - 11.
Cipriano A, Cella S, Cotrufo P. Nonsuicidal self-injury: A systematic review. Frontiers in Psychology. 2017; 8 (8). Available from:https://www.frontiersin.org/articles/10.3389/fpsyg.2017.01946/full - 12.
Plener PL, Kaess M, Schmahl C, Pollak S, Fegert JM, Brown RC. Nonsuicidal self-injury in adolescents. Deutsches Aerzteblatt Online [Internet]. 2018; 115 (3):23-30. Available from:https://www.ncbi.nlm.nih.gov/pmc/articles/PMC5787659/ - 13.
Rajhvajn Bulat L, Sušac N, Ajduković M. Predicting prolonged non-suicidal self-injury behaviour and suicidal ideations in adolescence – The role of personal and environmental factors. Current Psychology. 2023:1-12 - 14.
Gillies D, Christou MA, Dixon AC, Featherston OJ, Rapti I, Garcia-Anguita A, et al. Prevalence and characteristics of self-harm in adolescents: Meta-analyses of community-based studies 1990-2015. Journal of the American Academy of Child and Adolescent Psychiatry [Internet]. 2018; 57 (10):733-741. Available from:https://www.ncbi.nlm.nih.gov/pubmed/30274648 - 15.
Ma J, Batterham PJ, Calear AL, Han J. A systematic review of the predictions of the Interpersonal–psychological theory of suicidal behavior. Clinical Psychology Review. 2016; 46 :34-45. DOI: 10.1016/j.cpr.2016.04.008 - 16.
Smoyak SA. Loneliness: A sourcebook of current theory, research and therapy. Journal of Psychosocial Nursing and Mental Health Services. 1984; 22 (6):40-41 - 17.
de Jong-Gierveld J. Developing and testing a model of loneliness. Journal of Personality and Social Psychology. 1987; 53 (1):119-128 - 18.
Calati R, Ferrari C, Brittner M, Oasi O, Olié E, Carvalho AF, et al. Suicidal thoughts and behaviors and social isolation: A narrative review of the literature. Journal of Affective Disorders. 2019; 245 :653-667 - 19.
Lodder GMA, Scholte RHJ, Goossens L, Verhagen M. Loneliness in early adolescence: Friendship quantity, friendship quality, and dyadic processes. Journal of Clinical Child & Adolescent Psychology. 2015; 46 (5):709-720 - 20.
Centers for Disease Control and Prevention, National Center for Injury Prevention and Control. Strategic direction for the prevention of suicidal behavior: Promoting individual, family, and community connectedness to prevent suicidal behavior. 2008. Available from: http://www.cdc.gov/ViolencePrevention/overview/strategicdirections.html - 21.
Whitlock J, Wyman PA, Moore SR. Connectedness and suicide prevention in adolescents: Pathways and implications. Suicide and Life-Threatening Behavior. 2014; 44 (3):246-272 - 22.
Takács J, Katona ZB, Ihász F. A large sample cross-sectional study on mental health challenges among adolescents and young adults during the COVID-19 pandemic at-risk group for loneliness and hopelessness during the COVID-19 pandemic. Journal of Affective Disorders. 2023; 325 :770-777. DOI: 10.1016/j.jad.2023.01.067 - 23.
Cooper K, Hards E, Moltrecht B, Reynolds S, Shum A, McElroy E, et al. Loneliness, social relationships, and mental health in adolescents during the COVID-19 pandemic. Journal of Affective Disorders. 2021; 289 :98-104. DOI: 10.1016/j.jad.2021.04.016 - 24.
Widnall E, Winstone L, Plackett R, Adams EA, Haworth CMA, Mars B, et al. Impact of school and peer connectedness on adolescent mental health and well-being outcomes during the COVID-19 pandemic: A longitudinal panel survey. International Journal of Environmental Research and Public Health. 2022; 19 (11):6768. DOI: 10.3390/ijerph19116768 - 25.
Jones SE, Ethier KA, Hertz M, DeGue S, Le VD, Thornton J, et al. Mental health, suicidality, and connectedness among high school students during the COVID-19 pandemic - Adolescent behaviors and experiences survey, United States, January-June 2021. MMWR Supplements. 2022; 71 (3):16-21. DOI: 10.15585/mmwr.su7103a3 - 26.
Houghton S, Kyron M, Hunter SC, Lawrence D, Hattie J, Carroll A, et al. Adolescents' longitudinal trajectories of mental health and loneliness: The impact of COVID-19 school closures. Journal of Adolescence. 2022; 94 (2):191-205. DOI: 10.1002/jad.12017 - 27.
Lyyra N, Thorsteinsson EB, Eriksson C, Madsen KR, Tolvanen A, Löfstedt P, et al. The association between loneliness, mental well-being, and self-esteem among adolescents in four Nordic countries. International Journal of Environmental Research and Public Health. 2021; 18 (14):7405. DOI: 10.3390/ijerph18147405 - 28.
Pengpid S, Peltzer K. Loneliness is associated with poor mental health, social-environmental factors, and health risk behaviours among national samples of in-school adolescents in four Caribbean countries. Psychology, Health & Medicine. 2022; 27 (3):559-570. DOI: 10.1080/13548506.2021.1883071 - 29.
Joiner T. Why People Die by Suicide. Cambridge, MA: Harvard University Press; 2005 - 30.
O’Connor RC, Kirtley OJ. The integrated motivational–volitional model of suicidal behaviour. Philosophical Transactions of the Royal Society B: Biological Sciences [Internet]. 2018; 373 (1754):20170268. DOI: 10.1098/rstb.2017.0268 - 31.
McClelland H, Evans JJ, O’Connor RC. The association of family, social and romantic loneliness in relation to suicidal ideation and self-injurious behaviours. Journal of Psychiatric Research. 2023; 158 :330-340 - 32.
Nock MK. Self-injury. Annual Review of Clinical Psychology. 2010; 6 (1):339-363 - 33.
Preece DA, Goldenberg A, Becerra R, Boyes M, Hasking P, Gross JJ. Loneliness and emotion regulation. Personality and Individual Differences. 2021; 180 :110974. ISSN 0191-8869. DOI: 10.1016/j.paid.2021.110974 - 34.
Cacioppo JT, Cacioppo S. Loneliness in the modern age: An evolutionary theory of loneliness (ETL). In: Olson JM, editor. Advances in Experimental Social Psychology. Cambridge, MA: Elsevier Academic Press; 2018. pp. 127-197 - 35.
Cacioppo JT, Hawkley LC. Social isolation and health, with an emphasis on underlying mechanisms. Perspectives in Biology and Medicine. [Internet]. 2003; 46 (3 Suppl.):S39-S52. Available from:https://pubmed.ncbi.nlm.nih.gov/14563073/ - 36.
Keller FM, Derksen C, Kötting L, Dahmen A, Lippke S. Distress, loneliness, and mental health during the COVID-19 pandemic: Test of the extension of the evolutionary theory of loneliness. Applied Psychology: Health and Well-Being. 2022; 15 (1):24-48 - 37.
Wang Q , Wang H, Liu X. Loneliness, non-suicidal self-injury, and friendship quality among Chinese left-behind adolescents: The role of parent-child cohesion. Journal of Affective Disorders. 2020; 271 :193-200 - 38.
McClelland H, Evans JJ, Nowland R, Ferguson E, O’Connor RC. Loneliness as a predictor of suicidal ideation and behaviour: A systematic review and meta-analysis of prospective studies. Journal of Affective Disorders. 2020; 274 :880-896 - 39.
Schinka KC, van Dulmen MHM, Mata AD, Bossarte R, Swahn M. Psychosocial predictors and outcomes of loneliness trajectories from childhood to early adolescence. Journal of Adolescence [Internet]. 2013; 36 (6):1251-1260. Available from:https://www.sciencedirect.com/science/article/pii/S0140197113001085 - 40.
McKinnon B, Gariépy G, Sentenac M, Elgar FJ. Adolescent suicidal behaviours in 32 low- and middle-income countries. Bulletin of the World Health Organization [Internet]. 2016; 94 (5):340-50F. Available from:https://www.who.int/bulletin/volumes/94/5/15-163295/en/ - 41.
Rönkä AR, Taanila A, Koiranen M, Sunnari V, Rautio A. Associations of deliberate self-harm with loneliness, self-rated health and life satisfaction in adolescence: Northern Finland birth cohort 1986 study. International Journal of Circumpolar Health [Internet]. 2013; 72 (1):21085. Available from:https://www.ncbi.nlm.nih.gov/pmc/articles/PMC3753134/ - 42.
Brunstein Klomek A, Snir A, Apter A, Carli V, Wasserman C, Hadlaczky G, et al. Association between victimization by bullying and direct self injurious behavior among adolescence in Europe: A ten-country study. European Child & Adolescent Psychiatry. 2016; 25 (11):1183-1193 - 43.
Lin S, Li Y, Sheng J, Wang L, Han Y, Yang X, et al. Cybervictimization and non-suicidal self-injury among Chinese adolescents: A longitudinal moderated mediation model. Journal of Affective Disorders. 2023; 329 (5):470-476. DOI: 10.1016/j.jad.2023.02.124 - 44.
Gandhi A, Luyckx K, Goossens L, Maitra S, Claes L. Association between non-suicidal self-injury, parents and peers related loneliness, and attitude towards aloneness in Flemish adolescents: An empirical note. Psychologica Belgica. 2018; 58 (1):3-12 - 45.
Lasgaard M, Goossens L, Bramsen RH, Trillingsgaard T, Elklit A. Different sources of loneliness are associated with different forms of psychopathology in adolescence. Journal of Research in Personality. 2011; 45 (2):233-237 - 46.
He N, Xiang Y. Child maltreatment and nonsuicidal self-injury among Chinese adolescents: The mediating effect of psychological resilience and loneliness. Children and Youth Services Review. 2022; 133 :106335 - 47.
Santini ZI, Pisinger VSC, Nielsen L, Madsen KR, Nelausen MK, Koyanagi A, et al. Social disconnectedness, loneliness, and mental health among adolescents in Danish high schools: A Nationwide cross-sectional study. Frontiers in Behavioral Neuroscience. 2021; 15 :632906 - 48.
You J, Leung F, Lai CM, Fu K. The associations between non-suicidal self-injury and borderline personality disorder features among Chinese adolescents. Journal of Personality Disorders. 2012; 26 (2):226-237 - 49.
De Luca L, Giletta M, Menesini E, Prinstein MJ. Reciprocal associations between peer problems and non-suicidal self-injury throughout adolescence. Journal of Child Psychology and Psychiatry. 2022; 63 (12):1486-1495 - 50.
Nock MK. Why do people hurt themselves? Current Directions in Psychological Science. [Internet]. 2009; 18 (2):78-83. Available from:https://www.ncbi.nlm.nih.gov/pmc/articles/PMC2744421/ - 51.
Zhu S, Li X, Wong PWC. Risk and protective factors in suicidal behaviour among young people in Hong Kong: A comparison study between children and adolescents. Psychiatry Research. 2023; 321 :115059 - 52.
Masi CM, Chen HY, Hawkley LC, Cacioppo JT. A meta-analysis of interventions to reduce loneliness. Personality and Social Psychology Review [Internet]. 2010; 15 (3):219-266. Available from:https://www.ncbi.nlm.nih.gov/pmc/articles/PMC3865701/ - 53.
Lindow JC, Hughes JL, South C, Minhajuddin A, Gutierrez L, Bannister E, et al. The youth aware of mental health intervention: Impact on help seeking, mental health knowledge, and stigma in U.S. Adolescents. Journal of Adolescent Health. 2020; 67 (1):101-107 - 54.
Pisani AR, Schmeelk-Cone K, Gunzler D, Petrova M, Goldston DB, Tu X, et al. Associations between suicidal high school students’ help-seeking and their attitudes and perceptions of social environment. Journal of Youth and Adolescence [Internet]. 2012; 41 (10):1312-1324. Available from:https://www.ncbi.nlm.nih.gov/pmc/articles/PMC3534737/ - 55.
Logan DE, King CA. Parental facilitation of adolescent mental health service utilization: A conceptual and empirical review. Clinical Psychology: Science and Practice. 2001; 8 (3):319-333 - 56.
Houghton S, Kyron M, Lawrence D, Hunter SC, Hattie J, Carroll A, et al. Longitudinal trajectories of mental health and loneliness for Australian adolescents with or without neurodevelopmental disorders: The impact of COVID-19 school lockdowns. Journal of Child Psychology and Psychiatry. 2022; 63 (11):1332-1343. DOI: 10.1111/jcpp.13579 - 57.
Denche-Zamorano A, García- Gil MÁ, Mendoza-Muñoz M, Barrios-Fernandez S. Sadness and loneliness in adolescents with physical, sensory, or health problems in low/middle-income countries. Children (Basel). 2023; 10 (6):996. DOI: 10.3390/children10060996 - 58.
Thompson SJ, Johnston L. Risk factors of gay, lesbian, and bisexual adolescents. Journal of Human Behavior in the Social Environment. 2004; 8 (2-3):111-128. DOI: 10.1300/J137v08n02_07 - 59.
Pompili M, Lester D, Forte A, Seretti ME, Erbuto D, Lamis DA, et al. Bisexuality and suicide: A systematic review of the current literature. The Journal of Sexual Medicine. 2014; 11 (8):1903-1913. DOI: 10.1111/jsm.12581 - 60.
Oberle E, Ji XR, Alkawaja M, Molyneux TM, Kerai S, Thomson KC, et al. Connections matter: Adolescent social connectedness profiles and mental well-being over time. Journal of Adolescence. 2024; 96 (1):31-48. DOI: 10.1002/jad.12250. Epub 2023 Sep 22 - 61.
Hertz MF, Kilmer G, Verlenden J, Liddon N, Rasberry CN, Barrios LC, et al. Adolescent mental health, connectedness, and mode of school instruction during COVID-19. The Journal of Adolescent Health. 2022; 70 (1):57-63. DOI: 10.1016/j.jadohealth.2021.10.021. Epub 2021 Oct 22