
Abstract
WHO estimated over 56 million people across the world require palliative care each year. Seventy-six percent of these are from low- and-middle-income countries. Due to the aging population, urbanization, and physical inactivity among others, chronic health problems are expanding. The number of individuals with such health problems is increasing. Even though access to palliative care is a patient’s right and a duty of care provider, provision of comprehensive and integrated palliative care remains non-existent in Ethiopia. Within the health facilities where alleviation of pain and suffering is believed to improve quality of life, access to opioids is at best limited. Psychosocial needs and financial instability are primarily caused by persisting pain and diminishing livelihood. In Ethiopia, palliative care failed to pay attention to such components as social, economic, and spiritual support that are equally desirable to improve quality of life of those with chronic diseases. Coordinated care mechanisms are compromised with an inadequate understanding of the scope of palliative care, how to integrate different resources and lack of model that defines and guide provision of comprehensive palliative care.
Keywords
- palliative care
- comprehensive care
- continuum of care
- community-based care
- Ethiopia
1. Introduction
World Health Organization (WHO) defines palliative care (PC) as an approach designed to be safe and effective to improve patients and their families’ quality of life by preventing and relieving physical, psychological, social, and spiritual sufferings [1]. Through PC, individuals get relief from persistent pain while families cope with consequent challenges including bereavement to enhance the quality of life [2].
The development of palliative care is associated with movement of hospice centers with travelers where in ancient times sick travelers took rest. Such movement associated to sick travelers and dying patients have eventually developed into a center, which ultimately advanced into a formal palliative care service provided in conjunction with active treatment, and, as death nears [3]. It was in 1967 that Dr. Cicely Saunders, widely regarded as the founder of the modern hospice movement, opened the first team-based facility in the United Kingdom [4]. Palliative Medicine emerged as a medical specialty as a response to cancer and other chronic life-threatening illness. In the developing world, particularly sub-Saharan Africa, it had been the only available option for HIV/AIDS care before the era of antiretroviral drugs and remains relevant despite improved ART access [5].
Palliative care is an important agenda of the world health. In 2014, the World Health Assembly requested the Director General to ensure that PC is an integral component of all relevant global disease control and health system plans as well as consists into country and regional cooperation plans [6]. The resolution has clearly stated that it is the ethical duty of healthcare providers and the governmental organizations that support the delivery of healthcare to provide relief from pain, whether it is physical, psychological, or spiritual. This includes establishing appropriate local and national palliative care policies, supporting ongoing training and education on palliative care, providing budgetary support, ensuring appropriate access to necessary medications, supporting training programs, and ongoing education on palliative care [6].
Currently, PC is acknowledged as a necessary service in the Universal Health Coverage (UHC) package, which ensures that everyone has access to promotive, preventive, curative, rehabilitative, and palliative health services of adequate quality to be beneficial without putting the user in a financially difficult situation [7]. Whether a patient receives care in their own home, at community, at facility, at hospice inpatient unit, or at outpatient clinic holistic PC should be available wherever such care is needed [8]. Successful implementation of the PC program depends on how the different outlets are coordinated [9]. Studies revealed that patients and their caregivers prefer continued and comprehensive care service. Such continuity of care requires not only functional linkages between care outlets but also well-defined referral pathways and relevant capacities [10, 11, 12, 13]. This chapter aims to describe the experience of palliative care in Ethiopia and discuss the importance to initiate a comprehensive care approach in consideration of what local culture offers.
2. Palliative care in Ethiopia
Globally, the use of traditional and complementary or alternative medicines are increasing in both developed and developing countries [14]. A sizeable number of people receiving modern medical care for chronic, incurable illnesses, use herbs and non-prescription drugs as well as communal prayers and holy water (Tsebel). There are initiatives in place to involve religious leaders in the treatment of critically ill patients [15].
In Ethiopia, a comprehensive palliative care movement has started in response to the HIV/AIDS epidemic. Inconsistencies between the number of patients, qualified caregivers and lack of adequate services and resources in the healthcare systems for people living with HIV/AIDS have led to the idea of providing healthcare services for this vulnerable population at home [16]. Nonetheless, such service is not standardized nor the component of it remains disintegrated.
Home-based care (HBC) focuses on comfort and the alleviation of suffering, similar to hospice care. Home-based care programs were developed with a view to assisting caregivers at family level in providing AIDS-related care yet such services could not cope with the increasing demand for treatment and care. Evidences reveal that such care is provided either by NGOs, government health clinics, or community groups with an additional role to improve adherence to antiretroviral therapy [17, 18]. Community members and minimally trained HBC volunteers filled the void by providing basic services, dispelling myths about HIV/AIDS, and reintegrating patients into the community [5, 19].
Home and community-based care (HCBC) is deeply ingrained in Ethiopian culture and has long predated the development of the contemporary medical system. When hospitals overflowed and sick people had to be sent home during the early stages of the HIV/AIDS epidemics, there was a significant shift. Thus, community members and minimally trained home care workers filled the void by providing basic services. Prior to antiretroviral treatment (ART), HIV had a rapid downward trajectory and care focused on comfort and alleviation of suffering similar to hospice care. There was no standardized training material and toolkit for patient care at the home level, and support from healthcare institutions was minimal. More organized initiatives in HCBC were introduced in the year 2000 when care and support services assessments were performed in the Oromia region of Jimma and Nekemte by The Organization for Social Services for AIDS (OSSA) and the Amhara region of Adama, Asela, Shashemene, and Zeway by the Family Guidance Association of Ethiopia (FGAE) [5]. Sensitization sessions on the fundamental ideas of HCBC, the roles and duties of different community groups, stakeholders, and the requirements for selecting volunteer caregivers were held in order to address the unmet needs of the patients, and caregivers, limitations of the organizational capabilities which include Non-Governmental Organizations (NGOs), Kebeles, (the smallest unit of Urban Dwellers) Self-Help Public Associations, and Idirs (community self-help associations) [5].
The Addis Ababa HCBC program was launched in September 2003 with the support of Family Health International (FHI), the Addis Ababa HIV/AIDS Prevention and Control Office (HAPCO), and Addis Ababa Health Bureau. The implementation of the program was started with 20
According to assessments done in the beginning of 2000 by the African Palliative Care Association (APCA) and the World Health Organization (WHO), there were no institutions in Ethiopia that met the requirements for palliative care. Hospice Ethiopia was established in 2003 and offered the first multidisciplinary approach to healthcare, serving as a paradigm for future growth. Additional insights were gained from Ethiopia’s early 2000 response to HIV/AIDS, which bolstered the country’s overall healthcare delivery system. There are numerous additional groups involved in the Addis Ababa HCBC scene. Since 2003, Hospice Ethiopia has provided education and services [21].
In order to prepare guidelines for the standardization and implementation of PC, a technical working group (TWG) comprising stakeholders in the field was established in March 2011 under the direction of the Federal Ministry of Health (FMOH) of Ethiopia. Local morphine manufacture began in 2011, and the Ethiopian Public Health Association (EPHA) developed a pain training module in 2015, and PC was integrated into the public health system.
Over the last 10 years, the Federal Ministry of Health (FMOH) has created national palliative care standards, incorporated palliative care into the National Annual Plan, and integrated palliative care for the first time in the Ethiopian Hospital Services as part of the execution of policy of transformation guidelines. Palliative care was included in the Ethiopian Primary Health Care Clinical Guidelines. These recommendations were created using data from the Practical Approach to Care Kit (PACK), an integrated approach tool focused on symptoms that assist primary healthcare providers in making clinical decisions [22, 23].
FMOH has also been working on providing training for multi-disciplinary teams at hospitals, and some health centers both in Addis Ababa and the regions. FMOH has created a hub-and-spoke model for adult care, with the hospital serving as the hub and the hospital team connecting to community services and health centers. To create a multidisciplinary hospital team, in-service training for physicians, nurses, social workers, and pharmacists has been designed. The FMOH is working to increase the availability of drugs including morphine, as this is still a concern [22].
3. Disease dynamics and current state of palliative care in Ethiopia
The past century has shown a marked increase in life expectancy due to improved lifestyles, diagnostic facilities, and medical care as well as technological advances. Such an increase in life expectancy is not without cost. The vivid cost is complexities and burden of diseases that compromise the quality of life [24].
The WHO predicted an Epidemiological Transition due to a sharp increase in non-communicable diseases. While this may be the case in rich nations, many resource-constrained nations will likely experience a “triple epidemic,” in which accidents, non-communicable diseases, and communicable diseases all have a significant impact. Among the 65 million annual deaths globally, 45 million are due to chronic illnesses, of these, 60% require palliative care. It is, therefore, crucial that we begin considering culturally competent and economically viable models of care for chronic illnesses as soon as possible rather than later [25].
As science has advanced and life expectancy has increased, PCs have become more and more important. The necessity of combining PC into routine care services is underscored by the rising prevalence of cancer, mental illness, chronic non-communicable diseases, and their related treatments [26]. There are different models of care being used for palliative care implementation including home-based, community-based, facility-based, and hospice-based care in Ethiopia [22]. Studies have shown that home-based palliative care is a preferred model by patients and family caregivers which is required to smoothen the continuum of palliative care from the facility level through the integration of the service to the current chain of health delivery system [27, 28, 29].
PC should be provided in the context of the continuum of care, yet studies showed that there are barriers ranging from structural to individual levels for adequate and continuum provision of PC [30]. Misconceptions about palliative care as under recognized specialty, lack of trained palliative care providers; late involvement of inpatient palliative care, lack of community hospice services, inadequate palliative care education and training, financial barriers, attitudes and beliefs around PC, and geographical barriers were commonly mentioned [30, 31].
Lack of access to basic and specialized palliative care training and education for healthcare workers, limited opioid availability, legal and regulatory restrictions on oral morphine and strong opioids, costs for transportation and healthcare services, turn-over of trained staff, overwhelmed health workers, physical inaccessibility, lack of holistic care model, lack of defined palliative care package, and the absence of established structure and care model for implementing palliative care continuity from facility to, community and home as key hindering provision of comprehensive palliative care service in Ethiopia [27, 28, 32].
Even though Ethiopia has a strong Primary Health Care (PHC) structure building from the community to specialized facility level with a very diverse and rich culture of community support groups such as “Idirs”, Family kin system, Faith Based Organizations (FBOs), Civil Society Organization (CSOs), and Hospice centers, such resources are not translated to develop, and integrate PC services thereby contributing to meeting national and regional commitments to improve quality of life of chronically ill patients [22].
Ethiopians have long placed high value on their strong social fabric and sense of community responsibility for the sick. The culture of community support in Ethiopia is particularly strong since it takes into account the psycho-social aspects of a patient’s illness in addition to their physical one. This approach is particularly relevant in palliative care where the emphasis is in addressing the “total pain” of patients and families. Stoicism is highly regarded in Ethiopian society, and expressing one’s grief is seen as a sign of weakness or a lack of bravery. Pain management is therefore not given much thought. Ethiopia’s low per capita opioid use suggests that even in established institutions, moderate-to-severe pain is not being adequately managed.
For their medical requirements, the majority of Ethiopians still turn to traditional healers, spiritual guidance, and home medicines. A considerable percentage of people seeking modern medical care for chronic, incurable illnesses also use herbal remedies, non-prescription medications, and/or religious practices like communal prayers and tebel (holy water). It is advised to make an effort to involve religious and community leaders in the care of patients with serious illnesses in order to allay their fears that pursuing modern treatment will conflict with the divine intervention required to recover [33].
Ensuring the continuity of care and attending to patient needs as they move through the referral routes between community, home, and facility-based treatments is a crucial aspect of PC service. Even though the majority of Ethiopians live in rural areas, PC is still mostly donor-dependent and concentrated in urban areas [34]. A study conducted in Addis Ababa and Sidama region reported that the majority of female cancer patients suffered from moderate to severe pain and there was an unmet need in psychosocial, spiritual, economic, and emotional support [28]. Another study done in rural part of Ethiopia reported that there are extensive unmet palliative care needs in Ethiopia.
Untreated pain and high costs of illness are the major contributors to psychosocial distress and financial crisis in the Ethiopian population [29, 35]. The majority of PC services in Ethiopia are focused on pain management, with little attention paid to other necessary components such as social, economic, and spiritual support. Coordinated care mechanisms has severely compromised, patient needs are not into consideration, and there is an inadequate translation of local resources to provide comprehensive care at various levels [22, 27].
4. A way of forward-call for comprehensive care approach
Evidence suggests that policymakers, medical professionals, and community members may not be fully aware of the comprehensive palliative care options available, which contributes to Ethiopia’s poor palliative care practice. Lack of a comprehensive approach, poor stakeholder collaboration, and a dearth of funding and human resources all have an impact on the provision of palliative care. Thus, for millions of Ethiopians, access to comprehensive palliative care is either nonexistent or severely restricted [29].
Studies carried out in Ethiopia suggested additional studies on the underlying reasons for the dearth of integrated palliative care services and to design culturally relevant approaches. It is essential to have sincere discussions to raise awareness among decision-makers, healthcare professionals, and patient advocates about the importance of palliative care, shift tasks to primary care for improved access, and translate key terminologies and the concept of palliative care into working (official) language to support community ownership [27, 29, 35].
The Federal Ministry of Health’s dedicated leadership and the active participation of all stakeholders, as well as the integration of palliative care into the continuum of care and preservice curriculums are also critical milestones which shall be in place. To the best of our knowledge, however, no comprehensive effort exists (Figure 1) that offers patients and caregivers ongoing support at the community level following the first course of treatment in the facilities.
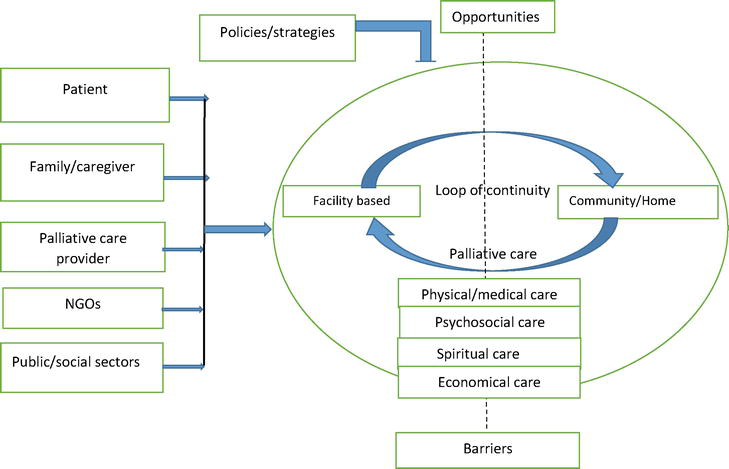
Figure 1.
Comprehensive palliative care model.
Such comprehensive care approach could enhance the quality of life for those who are terminally, and chronically ill, as well as their families, and caregivers. Palliative care ought to be considered an integral aspect of healthcare, not limited to patients nearing the end of life. To guarantee sustainability and accessibility, palliative care ought to be developed within the framework of the current healthcare system, taking into account the cultural and social background as well as the requirements of patients and caregivers. Palliative care must begin early in order to be effective; as the disease progresses and the objectives of treatment shift, symptom-based care will become increasingly important and curative measures will become less common. Models that are both economically and culturally suitable have been developed and shown to work well in nations with limited resources, such Rwanda and Uganda. Because hospice and palliative care in these two nations support a long-lasting framework of community initiation and ownership, they can be used as a model for care in resource-constrained areas. It is the duty of national health systems to integrate PC with early detection, treatment, and prevention initiatives throughout the continuum of care.
5. Conclusion
Ethiopia has poor and fragmented palliative care services; the country’s support systems are not well-coordinated nor do they have clear referral procedures or strategic guidelines to guarantee that palliative care is included in the country’s overall healthcare strategy. Volunteers and other providers lack the tools and competencies needed to fulfill the expanding needs of palliative care. Patients’ knowledge on what to do if they continue to demand care is remaining weak. Family and spiritual support as the most preferred services are generally accessible but should be reinforced. There is a fear associated with end-of-life planning, even though it has been shown to be rather effective. The palliative care continuum involves various stakeholders, including homes, health facilities, NGOs, and community structures, who should collaborate to improve quality of life.
Palliative care delivery mainly depends on NGOs based in urban settings, however, community volunteers had no chance to reach the hospitals to support patients besides primary healthcare units such as health centers, primary hospitals were missed in the process since palliative care provision is only provided in few specialized hospitals in Ethiopia. There is no responsible structure for the implementation of palliative care. Policy directions and guidance are missing as such in other departments like non-communicable disease, maternal, and child health.
Given Ethiopia’s dearth of all-inclusive palliative care choices and the difficulties faced by participants and caregivers in programs, it is imperative that care professionals receive continual training and supervision within a well-defined organizational structure. The preference for home and community-based care in line with what is culturally acceptable necessitates the active participation of like-minded stakeholders in the community.
The continuum of care can be maintained by initiating a care model that holds the health system accountable to have a well-functioning system but also work in close collaboration with different stakeholders at the community level including a culturally established care system. Given Ethiopia is known to have multiple cultures, it is important to carry out studies to identify more robust local care system that could be developed to contribute to improved care to patients.
6. Recommendations
In response to the global call for comprehensive palliative care, the Ethiopian palliative care initiatives, competencies, and available resources at different level need to be studied and documented to inform the role of multiple sectors. It would be crucial for the nation to create a comprehensive care model that, on the one hand, outlines the responsibilities of various sectors and skills and, on the other hand, defines referral pathways with a continuum of care. Such an effort might raise people’s quality of life and enhance Ethiopia’s response to its commitment to universal health coverage.
References
- 1.
Organization WH. World Health Organization definition of palliative care. World Health Organization Website. 2014. Available from: http://www.whoint/cancer/palliative/definition/en - 2.
WHO. Integrating Palliative Care and Symptom Relief into Paediatrics: A WHO Guide for Health-Care Planners, Implementers and Managers. Geneva: World Health Organization; 2018. Available from: https://creativecommons.org/licenses/by-nc-sa/3.0/igo - 3.
Williams MA, Wheeler MS. Palliative care: What is it? Home Healthcare Now. 2001; 19 (9):550-556 - 4.
Twycross RG. Introducing Palliative Care. Radcliffe Publishing; 2003. Available from: Amazon.com - 5.
World Health Organization. A community health approach to palliative care for HIV/AIDS and cancer patients in Sub-Saharan Africa. World Health Organization; 2004. Available from: https://iris.who.int/handle/10665/42919 - 6.
World Health Organization. Strengthening of palliative care as a component of integrated treatment throughout the life course. Journal of Pain and Palliative Care Pharmacotherapy. Jun 2014; 28 (2):130-134. DOI: 10.3109/15360288.2014.911801. Epub 2014 Apr 29. PMID: 24779434 - 7.
Downing J, Rajagopal M, de Lima L, Knaul F. Universal Health coverage and serious health-related suffering: A case for children and young people. In: Downing J, editor. Children’s Palliative Care: An International Case-Based Manual. Cham: Springer; 2020. pp. 13-23. DOI: 10.1007/978-3-030-27375-0_2 - 8.
Boston P, Bruce A, Schreiber R. Existential suffering in the palliative care setting: An integrated literature review. Journal of Pain and Symptom Management. 2011; 41 (3):604-618 - 9.
Graham F, Clark D. The changing model of palliative care. Medicine. 2008; 36 (2):64-66 - 10.
Bainbridge D, Brazil K, Krueger P, Ploeg J, Taniguchi A. A proposed systems approach to the evaluation of integrated palliative care. BMC Palliative Care. 2010; 9 (1):1-12 - 11.
Shamieh O, Hui D. A comprehensive palliative care program at a tertiary cancer center in Jordan. American Journal of Hospice and Palliative Medicine®. 2015; 32 (2):238-242 - 12.
Payne S, Eastham R, Hughes S, Varey S, Hasselaar J, Preston N. Enhancing integrated palliative care: What models are appropriate? A cross-case analysis. BMC Palliative Care. 2017; 16 (1):1-10 - 13.
Krakauer EL, Kane K, Kwete X, Afshan G, Bazzett-Matabele L, Ruthnie Bien-Aimé DD, et al. Essential package of palliative care for women with cervical cancer: Responding to the suffering of a highly vulnerable population. JCO Global Oncology. 2021; 7 :873-885 - 14.
Teshome-Bahire W. Initiation of healers in Ethiopia: A case study. Collegium Antropologicum. 2000; 24 (2):555-563 - 15.
Bishaw M. Promoting traditional medicine in Ethiopia: A brief historical review of government policy. Social Science & Medicine. 1991; 33 (2):193-200 - 16.
Larki M, Roudsari RL. Home-based care, the missing link in caring of patients living with HIV/AIDS and their family members: A narrative review. International Journal of Community Based Nursing and Midwifery. 2020; 8 (3):190 - 17.
Uys L. Guest editorial: Longer-term aid to combat AIDS. Journal of Advanced Nursing. Oct 2003; 44 (1):1-2. DOI: 10.1046/j.1365-2648.2003.02787.x. PMID: 12956663 - 18.
Wood EM, Zani B, Esterhuizen TM, Young T. Nurse led home-based care for people with HIV/AIDS. BMC Health Services Research. 2018; 18 (1):1-13 - 19.
Gispen MEC. Human Rights and Drug Control: Access to Controlled Essential Medicines in Resource-Constrained Countries. Utrecht University Repository (Dissertation); 2017 - 20.
HIV/AIDS prevention and control Office annual report for 2011. HAPCO, Addis Ababa, Ethiopia (Un-published report) - 21.
African Palliative Care Association (APCA). Standards for Providing Quality Palliative Care Across Africa. Kampala, Uganda: Elton John AIDS Foundation; 2010 - 22.
Mamo Y, Habte A, Abreha A, Ayers N, Abathun E, Reid E, et al. The evolution of hospice and palliative care in Ethiopia: From historic milestones to future directions. Ethiopian Journal of Health Development. 2020; 34 (4):310-312 - 23.
Cornick R, Picken S, Wattrus C, Awotiwon A, Carkeek E, Hannington J, et al. The practical approach to care kit (PACK) guide: Developing a clinical decision support tool to simplify, standardise and strengthen primary healthcare delivery. BMJ Global Health. 2018; 3 (Suppl. 5):e000962 - 24.
Crimmins EM. Lifespan and healthspan: Past, present, and promise. The Gerontologist. 2015; 55 (6):901-911 - 25.
Benziger CP, Roth GA, Moran AE. The global burden of disease study and the preventable burden of NCD. Global Heart. 2016; 11 (4):393-397 - 26.
Castro JA, Hannon B, Zimmermann C. Integrating palliative care into oncology care worldwide: The right Care in the Right Place at the right time. Current Treatment Options in Oncology. 2023; 24 (4):353-372 - 27.
Abate Y, Solomon K, Azmera YM, de Fouw M, Kaba M. Barrier analysis for continuity of palliative care from health facility to household among adult cancer patients in Addis Ababa, Ethiopia. BMC Palliative Care. 2023; 22 (1):1-9 - 28.
Kaba M, de Fouw M, Deribe KS, Abathun E, Peters AAW, Beltman JJ. Palliative care needs and preferences of female patients and their caregivers in Ethiopia: A rapid program evaluation in Addis Ababa and Sidama zone. PLoS One. 2021; 16 (4):e0248738 - 29.
Aregay A, O’Connor M, Stow J, et al. Palliative care in Ethiopia’s rural and regional health care settings: A qualitative study of enabling factors and implementation challenges. BMC Palliat Care; 2023; 22 :156. DOI: 10.1186/s12904-023-01283-5 - 30.
Abu-Odah H, Molassiotis A, Liu J. Challenges on the provision of palliative care for patients with cancer in low-and middle-income countries: A systematic review of reviews. BMC Palliative Care. 2020; 19 :1-16 - 31.
Cheng S-Y, Dy S, Hu W-Y, Chen C-Y, Chiu T-Y. Factors affecting the improvement of quality of dying of terminally ill patients with cancer through palliative care: A ten-year experience. Journal of Palliative Medicine. 2012; 15 (8):854-862 - 32.
Amare N, Gintamo B, Tukeni KN, Gebremichael EH, Abera EG. The prevalence of cancer patients requiring palliative care and its associated factors at St. Paul Hospital, Addis Ababa, Ethiopia: A cross-sectional study. Risk Management and Healthcare Policy. 28 Jun 2023; 16 :1203-1214. DOI: 10.2147/RMHP.S415532. PMID: 37404288; PMCID: PMC10315136 - 33.
Kassaye KD, Amberbir A, Getachew B, Mussema Y. A historical overview of traditional medicine practices and policy in Ethiopia. Ethiopian Journal of Health Development. 2006; 20 (2):127-134 - 34.
Reid E, Abathun E, Diribi J, Mamo Y, Hall P, Fallon M, et al. Rationale and study design: A randomized controlled trial of early palliative care in newly diagnosed cancer patients in Addis Ababa, Ethiopia. Contemporary Clinical Trials Communications. 2020; 18 :100564 - 35.
Aregay A, O’Connor M, Stow J, Ayers N, Lee S. Palliative care in Ethiopia’s rural and regional health care settings: A qualitative study of enabling factors and implementation challenges. BMC Palliative Care. 2023; 22 (1):156