Open Access is an initiative that aims to make scientific research freely available to all. To date our community has made over 100 million downloads. It’s based on principles of collaboration, unobstructed discovery, and, most importantly, scientific progression. As PhD students, we found it difficult to access the research we needed, so we decided to create a new Open Access publisher that levels the playing field for scientists across the world. How? By making research easy to access, and puts the academic needs of the researchers before the business interests of publishers.
We are a community of more than 103,000 authors and editors from 3,291 institutions spanning 160 countries, including Nobel Prize winners and some of the world’s most-cited researchers. Publishing on IntechOpen allows authors to earn citations and find new collaborators, meaning more people see your work not only from your own field of study, but from other related fields too.
The chapter delves into the intricate relationship between proton therapy and its impact on biological systems, shaping the landscape of modern cancer treatment. Proton accelerators and beam delivery systems are discussed, followed by analyses of proton beam characterization, penumbra, and Bragg peak phenomena, and their impact on biological responses. Cellular responses to proton radiation encompass cell cycle dynamics, pathways to cell death, mitotic catastrophe, and senescence, oxygen enhancement ratios in hypoxic tumors, and modulation of inflammatory and immune responses. Radiobiological modeling emerges as a predictive tool. Linear-Quadratic models, biophysical models for radiosensitivity, clinical outcome modeling, and the advent of radiogenomics and personalized medicine shape treatment strategies. Pediatric patients demand specialized consideration. Unique aspects, late effects, clinical outcomes, and long-term follow-up, coupled with advancements in pediatric proton therapy, form the crux of this section. Spot-scanning and pencil beam scanning techniques, FLASH proton therapy, heavy ion therapy, and innovative approaches like radioprotectors and combining proton therapy with immunotherapy pave the way for the next era in cancer treatment. This chapter navigates the dynamic interplay of radiobiology, technology, and patient care, fostering a comprehensive understanding of proton therapy’s potential in oncological practice.
VIAN—Krystyna Kiel Oncology Center, Kutaisi, Georgia
Mariam Pkhaladze
VIAN—Krystyna Kiel Oncology Center, Kutaisi, Georgia
Mikheil Atskvereli
VIAN—Krystyna Kiel Oncology Center, Kutaisi, Georgia
*Address all correspondence to: enatelauri@vian.health
1. Introduction
Radiobiology encompasses a realm within clinical and fundamental medical sciences, focusing on the examination of how ionizing radiation impacts living organisms, particularly delving into the ramifications of radiation exposure on health. At the same time, radiotherapy has consistently upheld its status as a highly efficacious approach for treating cancer, finding its place in the management of approximately half of all patients at some stage of their care journey. Radiation treatment is commonly employed at various stages of cancer care, and it’s often administered through photon-based intensity-modulated external beam therapy. However, technological advancements and research have enabled the development of charged particle therapies like intensity-modulated proton therapy. Proton beams have the unique property of depositing most of their energy at the end of their path, known as the Bragg peak. This feature allows clinicians to deliver higher radiation doses to cancerous cells while sparing the surrounding healthy tissue. Unlike photon beams, which are low linear energy transfer (LET), proton beams, particularly those in the spread-out Bragg peak (SOBP), are high LET. This gives proton therapy not just a physical advantage in dose distribution, but also unique biological benefits compared to traditional photon radiation. While there is a wealth of research on how tumors and healthy tissues react to photon-based therapies, the biological responses to proton therapy are not yet fully understood. Without a doubt, radiobiology has proven to be highly productive in generating novel concepts and pinpointing potentially valuable mechanisms for treatment. This has resulted in the emergence of various innovative treatment approaches. Unfortunately, only a handful of these strategies have yielded evident clinical advantages thus far. However, the capacity of laboratory science to provide comprehensive guidance to radiotherapists for selecting precise protocols remains constrained by the insufficiency of theoretical and experimental models. Consequently, the ultimate selection of a protocol will invariably require reliance on outcomes from clinical trials.
Radiation interactions with matter lie at the heart of understanding the intricate dance between particles and materials. This phenomenon forms the cornerstone of not only particle physics but also finds extensive application in medical imaging, radiation therapy, and diverse scientific fields (Table 1). Delving into the depths of these interactions provides crucial insights into the behavior of radiation as it traverses various substances, yielding valuable information that underpins both theoretical understanding and practical applications. The fundamental understanding of radiation-matter interactions is anchored in the profound concepts of ionization and excitation. Ionization involves the removal of electrons from atoms, resulting in charged species and the potential for subsequent chemical reactions. Excitation, on the other hand, involves the elevation of electrons to higher energy levels without complete detachment. These processes unravel the intricacies of particle behavior as they lose energy to the surrounding matter [6].
Photoelectric effect
In the photoelectric effect, an incident photon is absorbed by an atom, causing an inner-shell electron to be ejected. This mechanism is predominant at lower photon energies and is more probable in elements with higher atomic numbers (Z) [1].
Compton scattering
In Compton scattering, the incident photon is scattered by an electron, causing a change in the photon's direction and energy. The scattered photon has less energy, and the electron gains the energy difference [2].
Pair production
In pair production, a photon with energy greater than 1.02 MeV interacts near the nucleus and creates an electron-positron pair. The photon’s energy is transformed into mass, following Einstein’s E = mc2 equation [3].
Coherent scattering
Also known as Rayleigh or classical scattering, coherent scattering involves the scattering of low-energy photons without any energy transfer [1].
Alpha particle interaction
Alpha particles have a + 2 charge and interact with matter through Coulomb forces. They have low penetration ability and can be stopped by a sheet of paper or skin [4].
Beta particle interaction
Beta particles are high-speed electrons or positrons. Their interaction with matter involves ionization and excitation of atoms along their path [5].
Table 1.
Mechanisms of interaction.
The comprehension of these interactions has led to the development of medical imaging modalities that have revolutionized healthcare. In X-ray computed tomography (CT), the attenuation of X-rays as they pass through different tissues is harnessed to create detailed cross-sectional images. Understanding radiation interactions assists in optimizing CT protocols balancing image quality and patient dose. Similarly, positron emission tomography (PET) exploits the interaction between emitted positrons and electrons in the surrounding tissue, creating images that provide insights into metabolic processes at the molecular level [7]. Radiation therapy, a cornerstone of cancer treatment, harnesses the power of radiation-matter interactions to target and destroy cancer cells while minimizing damage to healthy tissues. Knowledge of these interactions aids in designing treatment plans that deliver precise doses to tumor sites based on tissue composition and density. Modern techniques like intensity-modulated radiation therapy (IMRT) and proton therapy rely on accurate predictions of radiation behavior in different tissues, optimizing treatment outcomes.
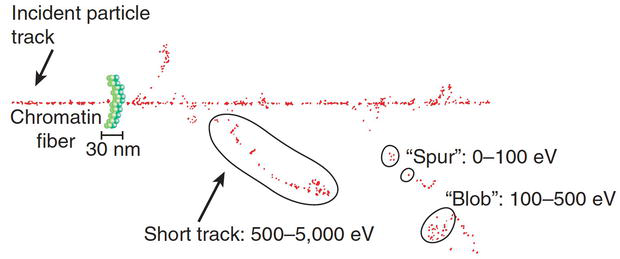
Ionizing radiation bestows its energy upon the medium it traverses, an interaction intrinsic to its path. The pivotal aspect of ionizing radiation’s interaction with biological matter lies in the stochastic and discrete nature of energy deposition. Energy is distributed in progressively energetic packets referred to as “spurs” (when around 100 eV is deposited), “blobs” (for 100–500 eV), or “short tracks” (encompassing 500–5000 eV), with each packet leaving in its wake roughly three to several dozen ionized atoms. This depiction is visualized in Figure 1, accompanied by a proportionally scaled segment of (interphase) chromatin. The discrete nature of these energy deposition occurrences leads to a significant observation: while the average energy deposited within a macroscopic volume of biological material is modest, the distribution of this energy on a microscopic level can be substantial. This inherent characteristic contributes to ionizing radiation’s exceptional effectiveness in generating biological damage. For instance, the energy deposited in a 70-kg human that results in a 50% probability of death amounts to approximately 70 calories, equivalent to the energy absorbed from a single sip of hot coffee. Notably, the distinction lies in the uniform distribution of energy in the coffee sip, as opposed to the random and discrete nature of ionizing radiation [8].
Figure 1.
Charged particle tracking through an absorbing medium, illustrating the random and discrete energy-deposition events along the track. Each event can be classified according to the amount of energy deposited locally, which determines how many ionized atoms will be produced. A segment of chromatin is shown approximately to scale.
Molecules directly struck by a spur or blob encounter a relatively elevated radiation dose, signifying substantial energy deposition within a confined volume. In the context of photons and charged particles, this energy deposition prompts the expulsion of orbital electrons from atoms, converting the target molecule initially into an ion pair and subsequently into a free radical [9]. Furthermore, the liberated electrons—themselves energetic charged particles—can instigate additional ionizations. Conversely, for uncharged particles like neutrons, interaction occurs between the incident particles and the nuclei of atoms within the absorbing medium. This interaction triggers the emission of recoil protons (charged particles) and lower-energy neutrons. This sequence of events, encompassing ionization, free radical generation, and release of secondary charged particles, persists until the entire energy of the incident photon or particle is dissipated. These interactions conclude within a mere picosecond following the initial energy transfer. Beyond this juncture, the ensuing chemical reactions of the resulting free radicals assume prominence, thus shaping the radiation response in subsequent time frames. The interaction of radiation with matter can produce various physical and chemical changes, which have both beneficial and harmful implications [4, 5].
Understanding radiation interactions with matter is vital for various applications like radiation therapy, radiography, and radiation shielding. Proper shielding materials and techniques can mitigate radiation exposure, depending on the type and energy of the radiation involved [10]. Understanding the mechanisms of how radiation interacts with matter is critical for harnessing its beneficial applications and mitigating its harmful effects. Each type of radiation interaction has specific characteristics, which must be accounted for in both technological applications and safety protocols.
Protons are ionized particles that can be propelled and directed into biological tissue to release their energy. The most prevalent form of heavy ion radiation treatment is proton therapy. What sets protons apart from conventional X-ray beams is their unique energy deposition profile: they provide a minimal radiation dose to the superficial, healthy tissues, peak at the depth where the tumor resides, and essentially offer no residual radiation to tissues beyond the tumor. This energy distribution is in stark contrast to that of x-rays, where the highest energy is generally absorbed by tissues closer to the surface. The Relative Biological Effectiveness (RBE) for protons stands at roughly 1.1, indicating only a slight biological advantage over x-rays or electrons (Table 2). The principal merit of proton therapy, therefore, lies in its optimized dose distribution [11].
X-ray
1
Gamma-rays
1
Beta particles
1
Protons
1.1–2
Alpha particles
20
Table 2.
The relative biological effectiveness for different types of radiation.
The generation of proton beams involves the use of cyclotrons or synchrotrons to propel ionized hydrogen atoms to energy levels exceeding 160 Mega Electron Volts (MeV). The machinery required for this process is generally more expansive and costly compared to traditional linear accelerators, often requiring dedicated facilities. Protons behave differently from electrons in that they deposit their energy increasingly as they travel deeper into the tissue, leading to a concentrated area of dose deposition known as the Bragg peak. By adjusting the energy of the proton beams, the Bragg peak can be precisely positioned to maximize the dose at the tumor site, thereby minimizing exposure to healthy tissue. To ensure comprehensive treatment, a technique known as a Spread-Out Bragg Peak (SOBP) is employed, which involves adjusting the proton energy or using varying modulators to cover the entire target area with a uniform dose [12].
Clinical applications of proton therapy have primarily focused on prostate cancer, though empirical evidence proving its superiority in this context is still lacking. Proton therapy is especially advantageous for treating pediatric malignancies, particularly those of the central nervous system, due to its minimal impact on healthy tissues. Research on utilizing protons for treating lung cancer and other anatomical sites is underway. Given the substantial costs associated with proton therapy equipment and specialized facilities, there is an ongoing debate on whether the benefits justify the investment. Despite the lack of definitive evidence so far, the number of facilities offering proton therapy continues to grow even in developing countries.
Understanding radiation interactions with matter is indispensable in radiobiology, particularly in the context of proton therapy—an advanced form of radiotherapy that exploits the unique physical and biological properties of protons:
Depth-dose distribution and penetration: unlike photons, protons have a mass and charge, leading to distinct depth-dose distributions. Proton beams can be modulated to deliver a more conformal dose to complex-shaped tumors, thanks to the unique control over the penetration depth afforded by manipulating the proton’s initial kinetic energy [12].
biological interactions: Linear Energy Transfer (LET) and Relative Biological effectiveness (RBE) [8].
Linear Energy Transfer (LET)—Protons exhibit a higher Linear Energy Transfer (LET) than photons, resulting in denser ionization tracks within the biological tissue. High-LET radiations are known to induce complex DNA damage, which is less amenable to repair mechanisms, thus enhancing the cytotoxic potential of the radiation.
Relative Biological Effectiveness (RBE)—The elevated LET of protons translates to a higher Relative Biological Effectiveness (RBE) compared to photons. RBE values are not constants but vary as a function of several variables including LET, dose, cell type, and even the phase of the cell cycle at the time of irradiation.
Normal tissues exhibit different levels of radiosensitivity based on cellular turnover, oxygenation status, and inherent DNA repair mechanisms. Cells in the G2 and M phases of the cell cycle are generally more radiosensitive than those in the G1 and S phases. Radiation can lead to various levels of cellular damage in normal tissues, ranging from sublethal damage repair to apoptosis and necrosis Organs like the skin, gut, and bone marrow are particularly sensitive due to their rapid cellular turnover. Tumors are often heterogeneous, comprising cells with varying degrees of radiosensitivity. Cancer stem cells within tumors may exhibit radioresistance, complicating eradication [13, 14, 15, 16].
Tumor hypoxia is associated with increased radioresistance, largely due to the decreased availability of molecular oxygen that acts as a radiosensitizer. Many tumors have aberrant DNA repair mechanisms, which may either increase radiosensitivity due to impaired repair or promote radioresistance by more effective sublethal damage repair. Understanding the radiosensitivity of normal and tumor tissues allows for better planning and optimization of radiation therapy. New approaches like hypofractionation and targeted radionuclide therapy are being explored to maximize tumor cell kill while minimizing normal tissue damage [17, 18, 19]. Radiosensitivity varies significantly between normal tissues and tumor cells, with a multitude of factors contributing to these differences. Understanding these factors is critical for the effective use of radiation in medical applications and for mitigating the adverse effects of radiation exposure.
The cellular damage resulting from radiation primarily targets DNA, inducing single- or double-strand breaks. The efficiency of DNA repair mechanisms, including base excision repair and homologous recombination, varies between normal tissues and tumor cells, thereby contributing to their differential radiosensitivity. Apoptosis and Cell-Cycle Checkpoints—both normal and tumor cells have inherent mechanisms that determine their radiosensitivity, such as apoptosis and cell-cycle checkpoints. However, many tumor cells often have defects in these pathways, which may both enhance and compromise their radiosensitivity depending on the specific molecular context. The alpha-beta ratio (α/β ratio) is a metric widely used to quantify radiosensitivity, with a lower ratio generally indicating higher radiosensitivity. The α/β ratio for normal tissues often differs from that of tumor cells, a factor that must be considered in treatment planning [20]. The intrinsic radiosensitivity characteristics of tissues impact dose fractionation strategies in proton therapy. Sparing normal tissues while maximizing the dose to tumor cells is a primary goal that can be optimized by leveraging our understanding of radiosensitivity. In proton therapy, the higher RBE due to elevated LET can affect both tumor and normal tissue. Therefore, the differential radiosensitivity of normal and tumor tissues must be accurately incorporated into treatment planning algorithms. The advent of high throughput “omics” technologies and systems biology approaches are poised to bring new insights into the factors influencing radiosensitivity, which could lead to even more precise and personalized radiation therapy regimens.
Proton beam therapy relies on specialized accelerators to produce a high-energy beam of protons. The most commonly used accelerators for this purpose are cyclotrons and synchrotrons. A cyclotron uses a fixed magnetic field and variable electric field to accelerate protons in a spiral path, whereas a synchrotron uses a variable magnetic and electric field to accelerate protons in a circular path. Once the protons are accelerated to the desired energy level, they are delivered to the patient using a beam delivery system. The two primary methods for proton beam delivery are passive scattering and pencil beam scanning (PBS). In the passive scattering technique, the proton beam is broadened using a scatterer and then shaped using a collimator and compensator to conform to the target volume. In the PBS method, a narrow “pencil” beam of protons is scanned across the target volume, which allows for better dose conformity [21, 22].
Characterizing a proton beam involves several important parameters, including energy, fluence, and dose distribution. The energy of the beam determines its penetration depth in tissue. Proton beams are often characterized by their Bragg peak, where the dose deposition is maximized. The fluence of the beam indicates the number of protons per unit area and plays a role in the overall dose delivered to the tissue [23]. Additionally, imaging techniques like Positron Emission Tomography (PET) can be employed for in-vivo dose verification, thus adding another layer of safety and precision [24].
A unique characteristic of proton beams is the Bragg peak, a region where the energy deposition reaches a maximum, allowing for the precise targeting of cancer cells while sparing surrounding healthy tissue [21]. The “penumbra” refers to the region around the target volume where the dose falls off rapidly. In conventional X-ray therapy, the penumbra is relatively large, which can result in a higher dose to surrounding tissues. However, in proton therapy, the penumbra can be much smaller, allowing for a more targeted treatment [25].
The physical properties of the proton beam have a direct impact on its biological efficacy. Due to the Bragg peak, proton beams can deliver a higher dose to the target tissue while minimizing the dose to surrounding tissues. However, it’s also important to note that high-linear energy transfer (LET) radiation like proton beams can produce complex DNA damage, which may result in different biological responses compared to low-LET radiation like X-rays. Moreover, proton therapy allows for hypofractionation, delivering higher doses per fraction, thus potentially reducing the overall treatment time [26, 27]. Research is ongoing to understand the biological consequences of varying beam properties, including energy, fluence, and dose rate, and their impact on the therapeutic ratio.
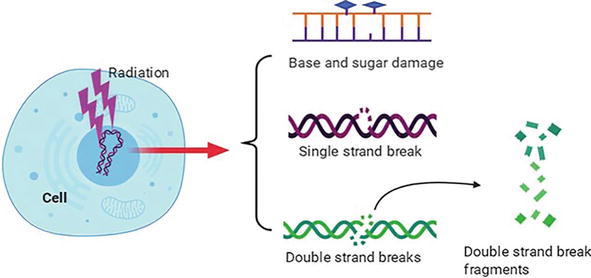
Understanding proton-induced DNA damage is essential for assessing the biological effectiveness and safety of proton therapy. This section elucidates various forms of DNA damage induced by protons, the repair mechanisms involved, and the biological significance of such damage. One of the most significant types of DNA damage caused by proton radiation is the double-strand break (DSB). DSBs occur when both strands of the DNA helix are severed, which could lead to chromosomal aberrations if not accurately repaired. Proton beams, owing to their high linear energy transfer (LET), are effective in inducing DSBs, which could make them more effective in killing cancer cells (Figure 2). Unlike conventional X-rays, high-LET radiation like protons can cause clustered DNA damage, where multiple types of lesions occur in proximity. This makes the repair process more complicated and increases the likelihood of misrepair and mutagenesis. Clustered DNA damage could include a combination of single-strand breaks, double-strand breaks, and base lesions, which collectively present a considerable challenge to cellular repair machinery [28, 29, 30, 31].
Figure 2.
DNA image induced by ionizing radiation. The major types of DNA damage induced by IR include base and sugar damage, single-strand breaks, double-strand breaks, clustered DNA damage, and covalent intrastrand or interstrand crosslinking.
The cellular machinery employs various mechanisms to repair DNA damage caused by proton radiation. These mechanisms include Non-Homologous End Joining (NHEJ) and Homologous Recombination (HR) for repairing double-strand breaks. For clustered DNA damage, specialized proteins like Rad52 and the MRN complex are involved in recognizing and flagging these complex lesions for repair. However, it’s essential to note that the efficiency of these repair mechanisms can vary depending on various factors, such as the cell cycle phase and the presence of oxygen, which can modulate the effectiveness of proton therapy [32, 33, 34].
The biological implications of proton-induced DNA damage are multi-faceted. On the one hand, the effectiveness of proton beams in causing double-strand breaks and clustered damage makes it a potent therapeutic modality for cancer treatment. However, the complexity of proton-induced damage also raises concerns about the long-term effects, such as secondary cancers and normal tissue complications. Understanding these biological outcomes is crucial for optimizing proton therapy parameters, like dose and fractionation, to maximize therapeutic gain while minimizing collateral damage to normal tissues [29, 35, 36].
5. Cellular and molecular responses to proton radiation
Understanding the complex cellular and molecular responses to proton radiation is key to unlocking the full therapeutic potential of this modality. This section will delve into various pathways and mechanisms activated in response to proton radiation, including cell cycle arrest, cell death pathways, and the involvement of hypoxic conditions and immune responses. Exposure to proton radiation can trigger a series of cellular events leading to cell cycle arrest, primarily at the G1/S and G2/M checkpoints. This halt in the cell cycle allows cells to repair damaged DNA before proceeding to cell division, thus minimizing the risk of mutations and genomic instability. Several cell death pathways may be activated by proton radiation, including apoptosis, necrosis, and autophagy. The choice between these pathways is influenced by several factors, such as the extent of DNA damage, cellular context, and the activation of specific signaling pathways like p53 [37, 38, 39, 40].
In cases where cell cycle checkpoints are bypassed or malfunctioning, cells may enter a state known as mitotic catastrophe. This is an onco-suppressive mechanism leading to the death of cells that have undergone aberrant mitosis [41]. Senescence is another cellular fate in response to proton irradiation. It leads to a state of irreversible growth arrest but not to cell death. The senescent cells, however, secrete pro-inflammatory cytokines, which can have a complex influence on the tumor microenvironment [42]. The presence of oxygen can significantly impact the efficacy of radiation therapies, including proton therapy. The oxygen enhancement ratio (OER) is a measure of how much more effective radiation is in the presence of oxygen compared to hypoxic conditions. Proton beams have been suggested to have a lower OER compared to X-rays, making them potentially more effective in treating hypoxic tumors [43].
Proton radiation can modulate the tumor microenvironment, particularly affecting the inflammatory and immune responses. For instance, protons can stimulate the release of cytokines such as IL-6 and TNF-α, which play roles in both promoting and suppressing tumor growth [44]. Furthermore, proton radiation has been shown to increase the presentation of tumor antigens, thereby enhancing the anti-tumor immune response [45]. Understanding these complex interactions can guide the optimization of proton therapy regimens and may pave the way for combination treatments involving immunotherapies.
6. Radiobiological models and treatment outcome prediction
The translation of proton therapy from a conceptual tool to a clinically effective treatment requires an integration of radiobiological knowledge with technological advances. Radiobiological models serve as invaluable instruments in predicting treatment outcomes, identifying the best treatment regimens, and offering personalized therapeutic approaches. This section elaborates on various models and their significance in optimizing proton therapy.
The Linear-Quadratic (LQ) model is commonly used to describe the dose-response relationship for cell survival after radiation exposure. Originally developed for photon radiation, the LQ model has been adapted to fit the complex biological responses to proton therapy [46]. The model estimates cell survival by considering both linear and quadratic terms of radiation dose, with alpha and beta as tissue-specific constants. In proton therapy, the LQ model can be adjusted to account for the variations in Linear Energy Transfer (LET) along the Bragg peak, thus providing a more accurate description of the dose-response relationship [47]. Apart from the LQ model, there are biophysical models like the Microdosimetric Kinetic Model (MKM) and the Local Effect Model (LEM), which aim to predict cellular radiosensitivity. These models consider the geometric and molecular complexities of cellular structures, thereby offering a more nuanced understanding of proton-induced biological effects [48, 49]. Such models are particularly useful in the treatment planning stage to optimize the dose distribution based on the predicted radiosensitivity of both tumor and normal tissues.
Beyond theoretical predictions, radiobiological models have been increasingly incorporated into clinical research to predict outcomes for specific cancers treated with proton therapy. By integrating various clinical, dosimetric, and biological factors, these models can estimate treatment efficacy, survival rates, and the risk of complications [50]. For instance, models that incorporate tumor volume, prescribed dose, and patient age have been developed to predict the probability of tumor control and normal tissue toxicity in treatments like head and neck or prostate cancers [51].
With the advent of high-throughput genomic technologies, the field of radiogenomics has emerged to identify genetic markers that could predict individual responses to radiation. Integrating radiogenomic data into radiobiological models opens the door to personalized proton therapy, where treatment plans are tailored to the individual’s unique genetic and molecular profile. By leveraging machine learning algorithms and big data analytics, researchers are making strides in identifying robust radiogenomic markers that could be implemented in routine clinical practice [52, 53, 54].
One of the significant challenges in radiation therapy, including proton therapy, is striking a balance between maximizing tumor control and minimizing normal tissue toxicity. Understanding the early and late effects of proton radiation on normal tissues is paramount for optimizing treatment plans and improving patient outcomes. This section will explore the different types of radiation-induced effects and how normal tissue tolerances are considered in proton therapy.
7.1 Radiation-induced early effects
Proton therapy has been gaining traction as a preferred modality for cancer treatment due to its ability to deliver highly conformal doses of radiation to the target while sparing surrounding normal tissues [55, 56]. However, like any other form of radiation therapy, proton therapy is not devoid of side effects. It is crucial to understand the early adverse effects induced by proton therapy to establish safe and efficient treatment protocols. This section aims to elucidate the early adverse effects of proton radiation therapy, offering a comprehensive review of the underlying mechanisms, clinical manifestations, and mitigation strategies.
Radiation-induced early effects are typically observed during or shortly after the course of treatment and may include skin erythema, mucositis, and acute gastrointestinal symptoms. These effects are usually reversible but can have an impact on the patient’s quality of life and compliance with the treatment regimen. The nature and severity of early effects can vary depending on the tissue type, dose per fraction, and total dose, among other factors [57, 58, 59].
One of the key factors contributing to early adverse effects in proton therapy is the interaction of proton beams with biological tissues. Unlike traditional photon beams, proton beams have high linear energy transfer (LET), especially at the Bragg peak, where most of the energy is deposited [60]. High LET radiation is more efficient at ionizing biological molecules, increasing the risk of early tissue reactions including inflammation and skin erythema [61].
Gastrointestinal (GI) toxicity is a common early side effect observed in patients undergoing proton therapy for abdominal and pelvic malignancies [62]. Symptoms may include nausea, vomiting, and diarrhea. Early GI toxicity is believed to result from the radiation-induced apoptosis of the rapidly dividing epithelial cells lining the GI tract [63]. Radiation dermatitis is another frequently reported early adverse effect of proton therapy [64]. This usually presents as redness, itching, or even skin ulceration at the site of radiation. The likelihood of developing dermatitis is dependent on various factors such as dose, fractionation, and individual patient sensitivity [65]. In instances where radiation fields include bone marrow, patients may experience early hematological changes including leucopenia and thrombocytopenia [66]. These conditions can lead to increased susceptibility to infections and may require dose modifications or delays in treatment [67].
Efforts to mitigate these early adverse effects include modifying treatment plans, optimizing dose distribution, and incorporating pharmaceutical interventions such as anti-inflammatory medications or antihistamines [68, 69]. Additionally, advancements in proton therapy technology, such as pencil-beam scanning, hold promise for minimizing these early adverse effects by allowing more precise dose distributions [70].
Understanding the early adverse effects of proton therapy is pivotal for clinicians to make informed decisions about treatment protocols. While proton therapy offers several advantages over traditional photon-based treatments, early adverse effects such as GI toxicity, dermatitis, and hematological changes remain areas of concern that necessitate ongoing research and clinical attention.
7.2 Radiation-induced late effects
In contrast to early effects, radiation-induced late effects may manifest several months or years post-treatment and can have a more severe impact on the patient’s long-term well-being. These can include fibrosis, cognitive impairment, and secondary cancers. Late effects are particularly concerning because they are often irreversible and can progressively worsen over time. Research has shown that proton therapy may offer a lower incidence of late effects compared to conventional photon therapy, primarily because of its precision and reduced scatter [71, 72, 73].
Late cardiopulmonary complications can manifest as myocardial fibrosis, coronary artery disease, or even lung fibrosis [74]. Studies suggest that these effects might be attributed to the scattering of protons in tissues with high atomic numbers, such as bones surrounding the chest cavity [75]. Patients treated with proton therapy for brain tumors may face delayed neurological effects, including cognitive decline and neuroendocrine dysfunction [76]. These adverse effects are thought to stem from the high linear energy transfer (LET) properties of protons causing greater damage to sensitive neural structures [77]. One of the most concerning late effects is the increased risk of secondary malignancies. Unlike photon radiation, which dissipates energy throughout the treatment volume, protons deposit the majority of their energy at the Bragg peak. However, the entrance dose and neutron scatter can still induce DNA mutations that may lead to secondary cancers [78]. Late effects can also impact the musculoskeletal system, causing fibrosis or even necrosis of the bone and surrounding tissues [79]. These are particularly of concern in pediatric populations, where proton therapy is commonly used to treat bone tumors [80]. Late gastrointestinal complications like strictures or fistulas can occur post-treatment for abdominal and pelvic cancers. These are thought to result from the delayed effects of radiation on the vascular supply and fibroblast proliferation in the gut lining [81].
Several strategies have been proposed for the management and mitigation of late adverse effects. Dose-volume histograms and biological effective dose (BED) calculations are used to predict the risk of late toxicity. Hypofractionation and integration of radioprotective drugs are being investigated as potential strategies to minimize the incidence of late effects [62, 82]. While proton therapy offers a sophisticated and precise approach to cancer treatment, clinicians must remain vigilant for potential late adverse effects. Ongoing research aims to further understand these complications and develop effective strategies for their prevention and management.
7.3 Normal tissue tolerance in proton therapy
Normal tissue tolerance is a critical parameter in treatment planning. Radiation oncologists must understand the dose-volume constraints for various organs at risk (OARs) to minimize normal tissue toxicity. In proton therapy, the normal tissue complication probability (NTCP) models are frequently employed to predict the likelihood of adverse effects in normal tissues. Given the distinct dosimetric profile of proton beams, especially the sharp dose fall-off beyond the Bragg peak, treatment planning in proton therapy often allows for better sparing of normal tissues. However, it is essential to continuously update and refine these models based on accumulating clinical evidence to ensure their applicability and accuracy in proton therapy settings [21, 83, 84].
Pediatric patients present a unique challenge in the context of radiation oncology, with considerations that are markedly different from adult populations. Proton therapy, known for its precision and reduced off-target effects, has been increasingly adopted for the treatment of pediatric malignancies. This section explores the unique considerations for pediatric patients undergoing proton therapy, the long-term effects of the treatment, clinical outcomes, and advancements in the field. Pediatric patients have a higher sensitivity to radiation, largely due to their developing tissues and organs. They are also at greater risk for secondary malignancies later in life following radiation exposure [85]. Proton therapy can be especially beneficial for this demographic because its precise targeting minimizes exposure to surrounding tissues, thereby reducing both immediate and long-term side effects [86]. Another challenge in pediatric proton therapy is the issue of growth and development. Treatment plans need to be adaptable to the physiological changes that occur as the child grows. This often requires more frequent adjustments to treatment plans compared to adults.
The late effects of proton therapy on pediatric patients can be profound, given their longer life expectancy post-treatment. Late effects may include growth abnormalities, neurocognitive deficits, and hormonal imbalances [73]. However, proton therapy’s precision often results in fewer such effects compared to traditional photon radiation [87]. Understanding the long-term consequences requires extensive follow-up studies to inform future clinical practice. Therefore, a multi-disciplinary approach involving oncologists, endocrinologists, and neurologists is often necessary for monitoring and managing late effects in pediatric patients.
The long-term follow-up of pediatric patients treated with proton therapy shows promising outcomes. For various pediatric cancers, including medulloblastoma and rhabdomyosarcoma, proton therapy has demonstrated comparable or superior survival rates with reduced toxicity compared to photon therapy [88]. Long-term studies also show lower rates of secondary malignancies [89]. However, long-term follow-up is critical, given the vulnerability of this population to late effects. Regular assessments are essential for the early detection of any secondary malignancies or other complications.
9. Advanced techniques and combinatorial approaches in proton therapy
Advancements in radiation oncology have led to new and refined methods in proton therapy. This section explores some of these cutting-edge approaches, including advanced scanning techniques, FLASH proton therapy, heavy ion therapy, and the integration of proton therapy with pharmacological agents and immunotherapy. Spot-scanning and pencil beam scanning are two advanced techniques that offer enhanced dose conformity in proton therapy. These approaches are particularly useful for treating tumors with complex shapes and those located near critical structures [47]. Spot-scanning employs individual spots of radiation that are distributed layer by layer to construct a three-dimensional dose distribution [90]. Pencil beam scanning is a more advanced version, using a narrow proton beam that can be modulated in intensity. These techniques offer higher flexibility in shaping the dose distribution, thereby reducing the dose to surrounding normal tissue and increasing the dose to the target volume.
FLASH proton therapy is an innovative approach delivering extremely high dose rates within ultra-short periods. Preliminary studies suggest that FLASH therapy might offer a greater therapeutic index by reducing toxicity to normal tissues while maintaining or enhancing the tumor-killing effect [91, 92]. The exact mechanisms behind these phenomena are still under investigation. Heavy ion therapy, such as carbon ion therapy, provides another option for increasing the biological effectiveness of radiation. Carbon ions offer a higher linear energy transfer (LET) compared to protons, making them potentially more effective for hypoxic or radioresistant tumors [93]. Ongoing research aims to determine the optimal use cases for heavy ion therapy and its comparative effectiveness against proton therapy [94].
Pharmacological agents such as radioprotectors can be employed to minimize toxicity to normal tissues, while radiosensitizers can enhance the tumor-killing effect of radiation [95]. When used in combination with proton therapy, these agents may offer new ways to improve the therapeutic ratio. However, the use of these agents needs to be carefully considered due to their potential interactions and side effects.
There is growing interest in combining proton therapy with immunotherapeutic agents to exploit potential synergies in cancer treatment. Proton therapy may induce immunogenic cell death, which can be further augmented by checkpoint inhibitors and other immunotherapeutic strategies. Clinical trials are underway to evaluate the effectiveness of this combinatorial approach [96, 97].
The realm of proton radiobiology has evolved substantially over the years, demonstrating a complex interplay of physical, biological, and clinical factors that culminate in therapeutic outcomes. From its inception, proton therapy has been heralded as a significant step forward in radiation oncology, with its key feature being the ability to deliver highly conformal radiation doses to tumors while sparing adjacent healthy tissues. Nevertheless, while the physical aspects of proton therapy have been relatively well understood, it’s only in recent years that the biological underpinnings have begun to be elucidated in greater detail.
The interaction of protons with biological tissues, particularly at the cellular and sub-cellular levels, offers both opportunities and challenges. The advantageous dose distributions characterized by the Bragg peak provide the theoretical underpinning for the utility of proton therapy. However, biological factors such as variable radiosensitivity across cell types, DNA repair mechanisms, and the influence of the tumor microenvironment add layers of complexity that require a multidisciplinary approach to unravel. The use of proton therapy in special populations, such as pediatric patients, has drawn significant attention. Here, the reduction of late effects and secondary malignancies becomes particularly crucial, and proton therapy holds the promise of more favorable outcomes. However, these benefits need to be systematically validated through long-term follow-up studies, incorporating advances in treatment planning and delivery.
Advancements in treatment techniques, such as spot-scanning, pencil beam scanning, and FLASH proton therapy, offer new avenues to improve dose delivery and possibly therapeutic outcomes. Moreover, combinatorial approaches incorporating heavy ion therapy, radioprotectors, radiosensitizers, and immunotherapy provide exciting prospects for enhancing the effectiveness of proton therapy. These advancements are particularly critical when considering the varied response of different tumor types and anatomical locations to proton therapy.
Despite these developments, several challenges remain. The limited availability of proton therapy centers, the high costs associated with the technology, and the need for more definitive comparative studies to validate its superiority over traditional therapies are all hurdles that the field must overcome. Furthermore, as more becomes known about the biological mechanisms underpinning the interactions between protons and tissues, there will be a growing need for models that can integrate these diverse sets of data into predictive frameworks for patient outcomes.
In conclusion, the field of proton radiobiology is a dynamic and evolving discipline that holds great promise for improving cancer treatment. As we continue to accumulate more data and refine our understanding of both the physical and biological aspects of this modality, it is crucial that we also focus on translating these findings into clinical practice. This will require a concerted effort from physicists, biologists, clinicians, and policymakers alike to ensure that the full therapeutic potential of proton therapy is realized.
Acknowledgments
We want to thank the people working at JCS VIAN and Krystyna Kiel Oncology Center for their encouragement and advice that led to the completion of this paper.
We also thank our friends and colleagues for their encouragement and words of advice.
Special thanks to our mentor—Krystyna Kiel, MD.
Finally, if not for our families, who supports us all the time, we would never be able to work on this extraordinary project.
Conflict of interest
The authors declared no potential conflicts of interest concerning the research, authorship, and/or publication of this article. This research did not receive a specific grant from funding agencies in the public, commercial, or not-for-profit sectors.
References
1.Podgorsak EB, Hendee WR. Radiation physics for medical physicists. Medical Physics. 2005;33(1):249
2.Turner JE. Atoms, radiation and radiation protection 3 comp rev and enl ed. Weinheim, Germany: Wiley-VCH; 2007. 607 p. ISBN 978-3-527-40606-7. Worldcat
3.Krane KS, Halliday D. Introductory Nuclear Physics. Kanada: John Wiley & Sons. Inc.; 1988
4.Knoll GF. Radiation Detection and Measurement. 4th Edition. Hoboken, Germany: John Wiley & Sons; 2010. pp. 217. ISBN: 0470131489, 9780470131480
5.Attix FH. Introduction to Radiological Physics and Radiation Dosimetry. Germany: John Wiley & Sons; 2008. ISBN: 978-3-527-61714-2
7.Hall EJ, Giaccia AJ. Technologies Inc. Radiobiology for the Radiologist. 7th ed. Philadelphia: Wolters Kluwer Health and Lippincott Williams & Wilkins; 2012. Available from: http://ovidsp.ovid.com/ovidweb.cgi?T=JS&PAGE=booktext&NEWS=N&DF=bookdb&AN=01438882/7th_Edition&XPATH=/PG(0)
9.Mettler FA, Upton AC. Medical Effects of Ionizing Radiation. 3rd ed. AJNR: American Journal of Neuroradiology. Philadelphia: Saunders Elsevier; 2009;30(2):e30. doi: 10.3174/ajnr.A1289. PMCID: PMC7051411
10.Martin A. Radiation Protection: A Guide for Scientists, Regulators, and Physicians. London, UK: Harvard University Press; 2006. ISBN: 9780674007406
11.Tseng YD, Halasz L. Description of proton therapy. In: Principles of Neurological Surgery. Philadelphia, PA: Elsevier; 2018. pp. 736-744. ISBN: 978-0-323-43140-8
12.Mohan R. Principles of proton beam therapy. In: Proton Therapy: Indications, Techniques and Outcomes. Philadelphia, Pennsylvania: Elsevier; 2020. p. 14-24. DOI: 10.1016/B978-0-323-73349-6.00011-X
13.Pacelli R, Mansi L, Hall E, Giaccia AJ. Radiobiology for the radiologist. European Journal of Nuclear Medicine and Molecular Imaging. 6th ed. Philadelphia, USA: Lippincott Wilkins & Williams; 2006;34:965-966. DOI: 10.1007/s00259-007-0383-8. ISBN: 0-7817-4151-3
14.Harrington L, Bristow RG, Hill RP, Tannock IF. Introduction to cancer biology. The Basic Science of Oncology. 2005;4:1-3
15.Bristow RG, Hill RP. Hypoxia, DNA repair and genetic instability. Nature Reviews Cancer. 2008;8(3):180-192. DOI: 10.1038/nrc2344
16.Diehn M, Cho RW, Lobo NA, Kalisky T, Dorie MJ, Kulp AN, et al. Association of reactive oxygen species levels and radioresistance in cancer stem cells. Nature. 2009;458(7239):780-783
17.Brown JM, Wilson WR. Exploiting tumour hypoxia in cancer treatment. Nature Reviews Cancer. 2004;4(6):437-447
18.Helleday T, Petermann E, Lundin C, Hodgson B, Sharma RA. DNA repair pathways as targets for cancer therapy. Nature Reviews Cancer. 2008;8(3):193-204
19.Baumann M, Krause M, Overgaard J, Debus J, Bentzen SM, Daartz J, et al. Radiation oncology in the era of precision medicine. Nature Reviews Cancer. 2016;16(4):234-249
20.Van Leeuwen CM, Oei AL, Crezee J, Bel A, Franken NA, Stalpers LJ, et al. The alfa and beta of tumours: A review of parameters of the linear-quadratic model, derived from clinical radiotherapy studies. Radiation Oncology. 2018;13(1):1-1
26.Girdhani S, Sachs R, Hlatky L. Biological effects of proton radiation: What we know and don’t know. Radiation Research. 2013;179(3):257-272
27.Kirkby C, Mackay RI. An introduction to proton therapy physics. Physics in Medicine & Biology. 2013;58(11):R221
28.Löbrich M, Jeggo PA. The impact of a negligent G2/M checkpoint on genomic instability and cancer induction. Nature Reviews Cancer. 2007;7(11):861-869
29.Sørensen BS, Bassler N, Nielsen S, Horsman MR, Grzanka L, Spejlborg H, et al. Relative biological effectiveness (RBE) and distal edge effects of proton radiation on early damage in vivo. Acta Oncologica. 2017;56(11):1387-1391
30.Sage E, Shikazono N. Radiation-induced clustered DNA lesions: Repair and mutagenesis. Free Radical Biology and Medicine. 2017;107:125-135
31.Goodhead DT. Initial events in the cellular effects of ionizing radiations: Clustered damage in DNA. International Journal of Radiation Biology. 1994;65(1):7-17
32.Chapman JR, Taylor MR, Boulton SJ. Playing the end game: DNA double-strand break repair pathway choice. Molecular Cell. 2012;47(4):497-510
33.Stenerlöw B, Karlsson KH, Cooper B, Rydberg B. Measurement of prompt DNA double-strand breaks in mammalian cells without including heat-labile sites: Results for cells deficient in nonhomologous end joining. Radiation Research. 2003;159(4):502-510
34.Chaudhary P, Marshall TI, Perozziello FM, Manti L, Currell FJ, Hanton F, et al. Relative biological effectiveness variation along monoenergetic and modulated Bragg peaks of a 62-MeV therapeutic proton beam: A preclinical assessment. International Journal of Radiation Oncology, Biology and Physics. 2014;90(1):27-35
35.Friedland W, Schmitt E, Kundrát P, Dingfelder M, Baiocco G, Barbieri S, et al. Comprehensive track-structure based evaluation of DNA damage by light ions from radiotherapy-relevant energies down to stopping. Scientific Reports. 2017;7(1):45161
36.Newhauser WD, Durante M. Assessing the risk of second malignancies after modern radiotherapy. Nature Reviews Cancer. 2011;11(6):438-448
37.Bartek J, Lukas J. Mammalian G1-and S-phase checkpoints in response to DNA damage. Current Opinion in Cell Biology. 2001;13(6):738-747
38.Sancar A, Lindsey-Boltz LA, Ünsal-Kaçmaz K, Linn S. Molecular mechanisms of mammalian DNA repair and the DNA damage checkpoints. Annual Review of Biochemistry. 2004;73(1):39-85
39.Galluzzi L, Vitale I, Abrams JM, Alnemri ES, Baehrecke EH, Blagosklonny MV, et al. Molecular definitions of cell death subroutines: Recommendations of the nomenclature committee on cell death 2012. Cell Death & Differentiation. 2012;19(1):107-120
40.Haupt S, Berger M, Goldberg Z, Haupt Y. Apoptosis-the p53 network. Journal of Cell Science. 2003;116(20):4077-4085
41.Klein K, He K, Younes AI, Barsoumian HB, Chen D, Ozgen T, et al. Role of mitochondria in cancer immune evasion and potential therapeutic approaches. Frontiers in immunology. 2020;11:2622
42.Campisi J. Aging, cellular senescence, and cancer. Annual Review of Physiology. 2013;75:685-705
43.Wenzl T, Wilkens JJ. Modelling of the oxygen enhancement ratio for ion beam radiation therapy. Physics in Medicine & Biology. 2011;56(11):3251
44.Deng L, Liang H, Xu M, Yang X, Burnette B, Arina A, et al. STING-dependent cytosolic DNA sensing promotes radiation-induced type I interferon-dependent antitumor immunity in immunogenic tumors. Immunity. 2014;41(5):843-852
45.Durante M, Formenti SC. Radiation-induced chromosomal aberrations and immunotherapy: Micronuclei, cytosolic DNA, and interferon-production pathway. Frontiers in Oncology. 2018;8:192
46.Fowler JF. The linear-quadratic formula and progress in fractionated radiotherapy. The British Journal of Radiology. 1989;62(740):679-694
47.Paganetti H. Relative biological effectiveness (RBE) values for proton beam therapy. Variations as a function of biological endpoint, dose, and linear energy transfer. Physics in Medicine & Biology. 2014;59(22):R419
48.Hawkins RB. A statistical theory of cell killing by radiation of varying linear energy transfer. Radiation Research. 1994;140(3):366-374
49.Elsässer T, Scholz M. Cluster effects within the local effect model. Radiation Research. 2007;167(3):319-329
50.Cheng Q , Roelofs E, Ramaekers BL, Eekers D, van Soest J, Lustberg T, et al. Development and evaluation of an online three-level proton vs photon decision support prototype for head and neck cancer–comparison of dose, toxicity and cost-effectiveness. Radiotherapy and Oncology. 2016;118(2):281-285
51.Fontanilla HP, Klopp AH, Lindberg ME, Jhingran A, Kelly P, Takiar V, et al. Anatomic distribution of [18F] fluorodeoxyglucose-avid lymph nodes in patients with cervical cancer. Practical Radiation Oncology. 2013;3(1):45-53
52.West C, Rosenstein BS. Establishment of a radiogenomics consortium. International Journal of Radiation Oncology, Biology, Physics. 2010;76(5):1295-1296
53.Kerns SL, West L, et al. Radiogenomics: The search for genetic predictors of radiotherapy response. Future Oncology. 2014;10(15):2391-2406
54.Scott JG, Berglund A, Schell MJ, Mihaylov I, Fulp WJ, Yue B, et al. A genome-based model for adjusting radiotherapy dose (GARD): A retrospective, cohort-based study. The Lancet Oncology. 2017;18(2):202-211
55.Mohan R. A review of proton therapy–current status and future directions. Precision Radiation Oncology. 2022;6(2):164-176
57.Bentzen SM, Constine LS, Deasy JO, Eisbruch A, Jackson A, Marks LB, et al. Quantitative analyses of Normal tissue effects in the clinic (QUANTEC): An introduction to the scientific issues. International Journal of Radiation Oncology, Biology, Physics. 2010;76(3):S3-S9
58.Jd C. Toxicity criteria of the radiation therapy oncology group (RTOG) and the European organization for research and treatment of cancer (EORTC). International Journal of Radiation Oncology, Biology, Physics. 1995;31:1341-1346
59.Marks LB, Yorke ED, Jackson A, Ten Haken RK, Constine LS, Eisbruch A, et al. Use of normal tissue complication probability models in the clinic. International Journal of Radiation Oncology, Biology, Physics. 2010;76(3):S10-S19
60.Fager M, Toma-Dasu I, Kirk M, Dolney D, Diffenderfer ES, Vapiwala N, et al. Linear energy transfer painting with proton therapy: A means of reducing radiation doses with equivalent clinical effectiveness. International Journal of Radiation Oncology, Biology, Physics. 2015;91(5):1057-1064
61.MacDonald SM, Patel SA, Hickey S, Specht M, Isakoff SJ, Gadd M, et al. Proton therapy for breast cancer after mastectomy: Early outcomes of a prospective clinical trial. International Journal of Radiation Oncology, Biology, Physics. 2013;86(3):484-490
62.Dutz A, Agolli L, Baumann M, Troost EG, Krause M, Hölscher T, et al. Early and late side effects, dosimetric parameters and quality of life after proton beam therapy and IMRT for prostate cancer: A matched-pair analysis. Acta Oncologica. 2019;58(6):916-925
63.Classen J, Belka C, Paulsen F, Budach W, Hoffmann W, Bamberg M. Radiation-induced gastrointestinal toxicity. Pathophysiology, approaches to treatment and prophylaxis. Strahlentherapie und Onkologie: Organ der Deutschen Rontgengesellschaft...[et al]. 1998;174:82-84
64.Liang X, Bradley JA, Zheng D, Rutenberg M, Yeung D, Mendenhall N, et al. Prognostic factors of radiation dermatitis following passive-scattering proton therapy for breast cancer. Radiation Oncology. 2018;13(1):1-8
65.Arimura T, Ogino T, Yoshiura T, Toi Y, Kawabata M, Chuman I, et al. Effect of film dressing on acute radiation dermatitis secondary to proton beam therapy. International Journal of Radiation Oncology, Biology, Physics. 2016;95(1):472-476
66.Vennarini S, Del Baldo G, Lorentini S, Pertile R, Fabozzi F, Merli P, et al. Acute hematological toxicity during cranio-spinal proton therapy in pediatric brain embryonal tumors. Cancers. 2022;14(7):1653
67.Song S, Park HJ, Yoon JH, Kim DW, Park J, Shin D, et al. Proton beam therapy reduces the incidence of acute haematological and gastrointestinal toxicities associated with craniospinal irradiation in pediatric brain tumors. Acta Oncologica. 2014;53(9):1158-1164
68.Langendijk JA, Lambin P, De Ruysscher D, Widder J, Bos M, Verheij M. Selection of patients for radiotherapy with protons aiming at reduction of side effects: The model-based approach. Radiotherapy and Oncology. 2013;107(3):267-273
69.Jones B, McMahon SJ, Prise KM. The radiobiology of proton therapy: Challenges and opportunities around relative biological effectiveness. Clinical Oncology. 2018;30(5):285-292
70.Rana S, Bennouna J, Samuel EJ, Gutierrez AN. Development and long-term stability of a comprehensive daily QA program for a modern pencil beam scanning (PBS) proton therapy delivery system. Journal of Applied Clinical Medical Physics. 2019;20(4):29-44
71.Hoffmann A, Oborn B, Moteabbed M, Yan S, Bortfeld T, Knopf A, et al. MR-guided proton therapy: A review and a preview. Radiation Oncology. 2020;15(1):1-3
72.Ming X, Wang W, Shahnazi K, Sun J, Zhang Q , Li P, et al. Dosimetric comparison between carbon, proton and photon radiation for renal retroperitoneal soft tissue sarcoma recurrence or metastasis after radical nephrectomy. International Journal of Radiation Biology. 2022;98(2):183-190
73.Thomas H, Timmermann B. Paediatric proton therapy. The British Journal of Radiology. 2020;93(1107):20190601
74.Nathan YY, DeWees TA, Voss MM, Breen WG, Chiang JS, Ding JX, et al. Cardiopulmonary toxicity following intensity-modulated proton therapy (IMPT) versus intensity-modulated radiation therapy (IMRT) for stage III non-small cell lung cancer. Clinical Lung Cancer. 2022;23(8):e526-e535
75.Kim C, Kim YJ, Lee N, Ahn SH, Kim KH, Kim H, et al. Evaluation of the dosimetric effect of scattered protons in clinical practice in passive scattering proton therapy. Journal of Applied Clinical Medical Physics. 2021;22(6):104-118
76.Bahn E, Bauer J, Harrabi S, Herfarth K, Debus J, Alber M. Late contrast enhancing brain lesions in proton-treated patients with low-grade glioma: Clinical evidence for increased periventricular sensitivity and variable RBE. International Journal of Radiation Oncology, Biology, Physics. 2020;107(3):571-578
77.Onorato G, Di Schiavi E, Di Cunto F. Understanding the effects of deep space radiation on nervous system: The role of genetically tractable experimental models. Frontiers in Physics. 2020;8:362
78.Xiang M, Chang DT, Pollom EL. Second cancer risk after primary cancer treatment with three-dimensional conformal, intensity-modulated, or proton beam radiation therapy. Cancer. 2020;126(15):3560-3568
79.Uezono H, Indelicato DJ, Rotondo RL, Vega RB, Bradfield SM, Morris CG, et al. Treatment outcomes after proton therapy for Ewing sarcoma of the pelvis. International Journal of Radiation Oncology, Biology, Physics. 2020;107(5):974-981
80.Greenberger BA, Yock TI. The role of proton therapy in pediatric malignancies: Recent advances and future directions. Seminars in Oncology. New York: Grune & Stratton; 2020;47(1):8-22. DOI: 10.1053/j.seminoncol.2020.02.002. ISSN: 093-7754
81.Vapiwala N, Wong JK, Handorf E, Paly J, Grewal A, Tendulkar R, et al. A pooled toxicity analysis of moderately hypofractionated proton beam therapy and intensity modulated radiation therapy in early-stage prostate cancer patients. International Journal of Radiation Oncology, Biology, Physics. 2021;110(4):1082-1089
82.De Marzi L, Patriarca A, Scher N, Thariat J, Vidal M. Exploiting the full potential of proton therapy: An update on the specifics and innovations towards spatial or temporal optimisation of dose delivery. Cancer/Radiothérapie. 2020;24(6-7):691-698
83.Kutcher GJ, Burman C, Brewster L, Goitein M, Mohan R. Histogram reduction method for calculating complication probabilities for three-dimensional treatment planning evaluations. International Journal of Radiation Oncology, Biology, Physics. 1991;21(1):137-146
84.Joiner MC, van der Kogel A. Basic Clinical Radiobiology. 4th ed. London: CRC Press; 2009. DOI: 10.1201/b15450. ISBN: 9780429190896
85.Bhatia S, Armenian SH, Armstrong GT, van Dulmen-den Broeder E, Hawkins MM, Kremer LC, et al. Collaborative research in childhood Cancer survivorship: The current landscape. Journal of Clinical Oncology : Official Journal of the American Society of Clinical Oncology. 2015;33(27):3055-3064
86.Ladra MM, Szymonifka JD, Mahajan A, Friedmann AM, Yong Yeap B, Goebel CP, et al. Preliminary results of a phase II trial of proton radiotherapy for pediatric rhabdomyosarcoma. Journal of Clinical Oncology : Official Journal of the American Society of Clinical Oncology. 2014;32(33):3762-3770
87.Greenberger BA, Pulsifer MB, Ebb DH, MacDonald SM, Jones RM, Butler WE, et al. Clinical outcomes and late endocrine, neurocognitive, and visual profiles of proton radiation for pediatric low-grade gliomas. International Journal of Radiation Oncology, Biology, Physics. 2014;89(5):1060-1068
88.Jimenez RB, Sethi R, Depauw N, Pulsifer MB, Adams J, McBride SM, et al. Proton radiation therapy for pediatric medulloblastoma and supratentorial primitive neuroectodermal tumors: Outcomes for very young children treated with upfront chemotherapy. International Journal of Radiation Oncology, Biology, Physics. 2013;87(1):120-126
89.Chung CS, Yock TI, Nelson K, Xu Y, Keating NL, Tarbell NJ. Incidence of second malignancies among patients treated with proton versus photon radiation. International Journal of Radiation Oncology, Biology, Physics. 2013;87(1):46-52
90.Lomax AJ, Böhringer T, Bolsi A, Coray D, Emert F, Goitein G, et al. Treatment planning and verification of proton therapy using spot scanning: Initial experiences. Medical Physics. 2004;31(11):3150-3157
91.Favaudon V, Caplier L, Monceau V, Pouzoulet F, Sayarath M, Fouillade C, et al. Ultrahigh dose-rate FLASH irradiation increases the differential response between normal and tumor tissue in mice. Science Translational Medicine. 2014;6(245):245ra93
92.Vozenin MC, De Fornel P, Petersson K, Favaudon V, Jaccard M, Germond JF, et al. The advantage of FLASH radiotherapy confirmed in Mini-pig and Cat-cancer patients. Clinical Cancer Research : An Official Journal of the American Association for Cancer Research. 2019;25(1):35-42
93.Durante M, Orecchia R, Loeffler JS. Charged-particle therapy in cancer: Clinical uses and future perspectives. Nature Reviews. Clinical Oncology. 2017;14(8):483-495
94.Baumann BC, Mitra N, Harton JG, Xiao Y, Wojcieszynski AP, Gabriel PE, et al. Comparative effectiveness of proton vs photon therapy as part of concurrent chemoradiotherapy for locally advanced cancer. JAMA Oncology. 2020;6(2):237-246
95.Barker HE, Paget JT, Khan AA, Harrington KJ. The tumour microenvironment after radiotherapy: Mechanisms of resistance and recurrence. Nature Reviews. Cancer. 2015;15(7):409-425
96.Gandhi SJ, Minn AJ, Vonderheide RH, Wherry EJ, Hahn SM, Maity A. Awakening the immune system with radiation: Optimal dose and fractionation. Cancer Letters. 2015;368(2):185-190
97.Galluzzi L, Buqué A, Kepp O, Zitvogel L, Kroemer G. Immunological effects of conventional chemotherapy and targeted anticancer agents. Cancer Cell. 2015;28(6):690-714
Written By
Eter Natelauri, Mariam Pkhaladze and Mikheil Atskvereli
Submitted: 17 September 2023Reviewed: 26 September 2023Published: 01 February 2024