
Abstract
Boxing is the ultimate contact sport in which the objective is to knock down an opponent by striking the opponent in the head and abdomen with knuckle punches while wearing minimal protective gear. Sports trauma and injury surveys of professional and amateur boxers in Japan and overseas have reported athletes suffering not only from orthopaedic disorders, such as lacerations and fractures, but also from acute subdural haematomas after knockouts and even chronic traumatic encephalopathy after retiring from boxing. Efforts have been made to improve boxing safety by improving the protective equipment and revising competition rules. However, the nature of the sport has not allowed significant results to be achieved. The primary prevention of trauma and injury during boxing involves avoiding attacks by an opponent. This chapter focuses on the performance of boxing from a scientific perspective, mainly the improvement of defensive techniques, and examines the usefulness of quantitative motion analysis software developed specifically for boxing. The fusion of boxing and technology is a step towards the construction of a new support system for the primary prevention of sports injuries and its potential has been explored.
Keywords
- boxing
- analysis software
- performance
- injury prevention
- technical assistance
1. Introduction
Boxing is a contact sport in which fighters strike each other directly with their fists on the head, face, and abdomen. Amateur boxers, such as those competing in the Olympic Games, wear headgear and are judged based on the number of clean punches they land on their opponents, whereas professional boxers wear no protective gear other than a mouth guard and are judged based on the damage or knockout they inflict on their opponents. In general, professional boxers are paid by their gyms through the sale and purchase of tickets, endorsement fees from sponsors’ names and logos on their outfits, and fight money given by the promoter, whether the fighter wins or loses. In the modern era, athletes’ livelihoods are supported by pay-per-view viewership. Top athletes have an increasing number of sponsors and additional sources of income, such as endorsements, television appearances, joint product development with companies, book sales, and speaking engagements. According to a 2015 Forbes article, the top-earning celebrity in the world, with an annual income of $300 million, was Pro Bobo, ranking first on the list of the world’s highest-earning celebrities. Topping the list of the world’s highest-earning celebrities, with an annual income of USD 300 million, was Floyd Mayweather Jr. The fact that Floyd Mayweather Jr. was able to take first place ahead of football, which is said to have the world’s largest athlete population, musicians supported by passionate fans, and holiday stars strutting down the red carpets, shows the potential of boxing as a professional sport. The fact that Floyd Mayweather Jr. was ranked number one ahead of the musicians and the holiday stars strutting down the red carpet shows the potential of boxing as a professional sport.
Despite its glamourous world, boxing, due to its sporting characteristics, causes a high incidence of sports injuries and disorders. In a trauma and injury survey involving amateur boxing, orthopaedic conditions, such as lacerations and fractures and cranial nerve conditions, such as acute subdural haematoma were frequently observed, and fatal accidents caused by these conditions have been reported [1]. Although improvements have been made with respect to the protective equipment and the rules of sports have been reviewed, it is difficult to say that the number of traumatic injuries and disabilities has decreased [2, 3]. The primary prevention of trauma and injury during boxing involves avoiding attacks by an opponent. This requires improving defensive techniques to avoid being attacked by the opponent and simultaneously improving offensive techniques to increase the rate of hitting the opponent, which is a strategy to prevent trauma and injury by ending the fight early. Boxers, who are often forced to lose weight as a fight approach, are trained based on nutritional and training science. However, it remains to be seen whether technical strategies in boxing offences and defence have been addressed from a scientific perspective.
This chapter begins with an overview of the origins of boxing in order to understand the sport. Next, the current status of sports-related disorders in boxing and the mental characteristics of boxers are summarised. Therefore, this chapter explores the possibilities of merging sports and technology by presenting findings from the development and operation of quantitative motion analysis software, specifically for boxing.
2. Origins of the sport of boxing
2.1 Ancient Olympics and fist-fighting
The origins of boxing are unclear; however, there is evidence of boxing-like games (fisticuffs) in Egyptian and Mesopotamian civilisations as early as 3000 BC, as evidenced by murals and vases. Boxer figures, thought to date from 1600 BC to 1200 BC or earlier, have also been found throughout the Mediterranean. However, it is from the ancient Greek period that continuity with modern boxing was most likely established. The earliest record of a fistfight for a prize is found in Homer’s heroic epic poem The Iliad (c. 750 BC), which dates back to ancient Greeks [4]. The image of two fighters, cloth wrapped around their waists and a cowhide wrapped around their fists, fist-to-fist, is preserved in a mural in Akrotiri, Santorini, in the northern part of Greek Crete. The city state of Polis was born in Greece in the 8th century BC, when Homer’s heroic epic was written. Agriculture and herding were carried out by slaves, whereas the aristocracy and wealthy citizens participated in sports. For ancient Greeks, it was of utmost importance that various religious rites of the ancient world be performed according to their traditions. During rites and festivals, athletic competitions were often organised, such as funeral games, the most important of which were the Ancient Olympics. The most important of these was the Olympic Games, held as a festival in Olympia in the domain of the god Zeus. The first games were held in 776 BC, and the compilation of records of the Ancient Olympic champions began around 400 BC. Although there is some dispute as to whether this is an accurate account of what happened approximately 300 years before the compilation began, it seems certain that the games were held every four years without interruption for at least 1000 years, from 6th century BC to 4th century AD [5]. Pugilism was introduced in the 23rd century (688 BC) and was a popular sport. Socrates, a famous philosopher, was a fist-fighting enthusiast person who travelled from Athens to Olympia for three days and three nights to watch the games.
2.2 Rules of fistfighting
The exact rules for fisticuffs at that time were not known; however, analogies can be drawn from vase paintings, murals, dictionaries, and descriptions in the literature. These rules are significantly different from those of modern boxing. First, the shape of the playing field was unknown; however, no ropes were used to divide it. There was no class system based on weights or other criteria. The match combinations were also determined by lot. Once a match began, the fighters were required to stay close to each other and fight without resting. The referees used ladders and stick-like devices to encourage fighters to hit each other in close proximity. Referees would sometimes hit fighters who clinched, as clinching was forbidden. There was no round system or time limit; however, the referees allowed fighters to take breaks during a bout if they agreed. Forbidden were holds, blows to the groin, etc., which are common in wrestling [6]. Victory or defeat was decided by one side holding up one or two fingers to signal surrender or by the other side fainting; there were no draws or judges’ scores.
2.3 Changes in fittings in fistfighting
The only fastening device was a cord wrapped around the fist. In 5th century BC, athletes began to use soft cowhide cords, called himantes to secure their wrists and fingers and wrap around their arms. However, the himantes were complicated and time-consuming to wind; therefore, a ready-made fastening device was developed in the form of a coiled leather cord. The “sharp strap” (oxeis himantes) was the first official boxing glove in history. The fingers were held in place using hard leather straps and the inside was made of wool to protect the hand. This type of equipment was used until the end of the 2nd century during the Roman period [7]. This was followed by the infamous caestus, which was reinforced with iron and lead. Reinforced with iron and lead, it was not as much a glove as a weapon in itself (Figure 1). Changes in the first attachment also changed the fisticuffs. In the early days, when soft leather straps were used, contestants competed with agile offensive and defensive techniques. However, when ‘sharp straps’ were introduced, the damage caused by a single strike shifted the movement to a defensive focus. Later, when the caestus was introduced, the game became a bloody and destructive spectacle and a contest of facial and physical destruction.

Figure 1.
Originally, the himantes was a thin leather strap wrapped around the wrist to secure the finger joints (two left), evolving into a glove in the 4th century (two middle) and a kaestus (two right) reinforced with iron or lead in the Roman period [Andronikos M, 1981].
2.4 End of the ancient Olympic games and the codification of fist-fighting rules
The end of fistfighting in antiquity is said to be due to the total ban on pagan rituals issued by Theodosius I as a result of the nationalisation of Christianity in Rome; however, the last recorded tournament was the 291st in 385 AD. At this time, fist fights were held along with wrestling, pankration, and athletics [8]. In other words, it can be said with certainty that fisticuffs were held during the ancient Olympic Games for more than thousand years. The first codification of the rules of fistfighting was in 1743 and is known as the “Broughton Rules” [2]. The round ended when the opponent was down. The interval between the rounds was 30 s [4]. Striking at a downed opponent or grabbing the opponent from the waist down, such as the thighs and buttocks, was prohibited [5]. No decision can be made until the second referee declares a defeat. (vi) Regardless of the prior arrangement between individuals, the winner received two-thirds of the prize money, which was distributed on stage. (vii) To avoid disputes, two judges are selected from the audience and their decisions are absolute [9]. This earliest codified rule, which led to the current boxing rules, was established to minimise interference with spectators and guarantee the fairness of betting. Betting was the mainstay of entertainment and for betting to be fair, the fights themselves had to be fair. This was the reason for the codification and disclosure of the rules, and the spirit of fair play was also emphasised for betting. The London Prize Ring Rules, which came into force in the following century, stipulated that all bets were to be stopped if the match was not settled [10]. The rules were laid down with wagering in mind, and the subsequent introduction of three weight classes - lightweight, middleweight, and heavyweight - was also because it was more interesting as a betting game.
2.5 From prize-fighting to glove boxing
The decline in prize-fights, in which fighters fought with their bare hands, was a major factor in boxing. In 1841, the Fist Fighting Club was formed in London, an elegant association of patrons that provided facilities for prize-fights, developed a bounty system, tightened rules, and banished the practice of cheating. Because of their efforts, prize-fights enjoyed their heyday. Throughout the 19th century, the crackdown on prize-fights was tightened in three stages: first, as a threat to public safety and society; second, from the moral point of view of cruelty; and finally, as a threat to the lives and health of those involved. Prize fights were popular until then because the nobility and gentry were patrons of the fights; however, the endless number of betting-related illegalities led to a loss of confidence in the fairness of the fights, and they stopped being patrons [11]. It was natural that the decline began as soon as this happened, and prize fights disappeared from this stage in the late 19th century. However, for boxing to exist, prize fighting had to decline. The history of boxing divides the period from the 17th century to the 1860s as the era of bare-knuckle fighting and the period after that as the era of glove boxing, called sparring. When learning kung-fu in classes as a ‘noble art of self-defence’, the practice of kung-fu was referred to as sparring. The ability to expand sparring enthusiasm by selling safe gloves became the foundation of modern boxing, and the decline of prize fighting was the tailwind of the era of glove boxing.
2.6 Development of glove boxing
In the 1860s, sparring was introduced into physical education in public schools and rose to the status of a youth discipline. It was precisely during this period that sparring rules were codified as competition, and the era of glove boxing can be said to have begun in 1867 with the ‘Queensbury Rules’. The rules have the following characteristics: (1) the prohibition of wrestling acts, such as grabbing and throwing; (2) the introduction of a round system with each round lasting three minutes and an interval of one minute; (3) the introduction of a ten-count after a down; (4) wearing gloves; and (5) wearing shoes without non-slip soles [12]. In the tournament, there were three weight classes–lightweight, middleweight, and heavyweight–and points were awarded in three three-minute rounds. A modern boxing framework has already been implemented using these rules. In the UK, the Amateur Boxing Association was formed in 1880 and grew into a national governing body that overtook the Queensbury Rules. Simultaneously, the establishment of the Queensbury Rules, where time is clearly defined, can be regarded as the establishment of boxing as a modern sport.
2.7 From fisticuffs to modern boxing as a competition
Historically, Britain, the founder of industrial capitalism, developed into a world empire in the 17th century, controlling the seven seas, and had colonies all over the world. In colonies with no stable legal system, confrontations through fistfighting were sometimes used as a means of adjudication. Therefore, being a master of fencing was also useful in demonstrating one’s superiority as a ruler. In medieval Europe, fencing skills were a mark of nobility; similarly, in the colonies of the United States, Canada, and Australia, fisticuffs were a mark of dignity for the conquerors [11]. In the 19th century, therefore, in these New World countries, pugilism based on the Broughton and London Prize Ring Rules spread widely. While prizefighting began to decline in the United Kingdom, the United States became the home of prizefighting and boxing from the 1860s onwards. Boxing spread from the USA to the rest of the world as popular culture and was internationalised. The influence of mass media and visual entertainment, such as newspapers, television, and films, played a major role in this worldview, in which people of all birth and upbringing can become successful with a single fist. As boxing became popular in several countries, its popularity became immense among men and women of all ages.
In modern professional boxing, men are divided into 17 weight classes and women into 18 classes to eliminate unfairness due to weight differences and ensure the safety of boxers. Ranks were also defined according to the boxing results, and the number of rounds was accordingly limited. The weight of the gloves differs according to rank, and fighters must wear bandages to protect their fists, mouth guards to protect their teeth and oral cavity, and foul cups to protect their lower abdomen. Weigh-ins are now conducted the day before the competition, and some organisations stipulate a range of recovery increases after the weigh-in. Efforts are being made to protect the fairness of the competition and the health and lives of the fighters from all aspects, such as thorough rule meetings attended by judges and both sides, the introduction of a standing-down system, the right to stop fights by the ringside doctor, and doping tests. Although the environment surrounding boxing has changed over time, the only thing that is common to both the era of firefighting and the current transformation of boxing into a sport is that the pride and prestige of each country are at stake and fights attract the hearts of numerous people.
3. Sports disorders in boxing
Sports include professional sports, amateur sports as a competition, and sports as a hobby, recreation, health promotion, or exercise therapy, and sports can be said to be one of the most popular forms of activity among people to this day. However, sports injuries caused by various factors are an unavoidable problem in all sports and must be resolved, although the degree of injury varies. Boxing is one of the contact sports with the highest incidence of trauma and disability [13]. Trauma and injury investigations targeting boxing athletes have been conducted in the USA [1, 14, 15], Australia [16, 17], the UK [18], and other countries, focusing on the occurrence of head injuries. In Japan, investigations on head injuries and disorders have been conducted in professional and amateur boxers, as well as investigations on oral trauma, trauma to the hand and face, which are direct sites of attack, and disorders of the trunk and lower limbs [19, 20, 21, 22]. These results show that several sports injuries and disorders are common during boxing, including concussion, intracranial haemorrhage, facial lacerations, retinal detachment, orbital floor fractures, nasal bone fractures, rib fractures, organ injuries, and back pain [1, 19, 23, 24, 25]. In this section, sports disorders observed to occur in boxing are discussed.
3.1 Acute subdural haematoma
Acute subdural haematoma (ASH) is a major cause of boxing-related fatalities. As a basic reference for the occurrence of ASH, during the 23-year period from 1978 to 2000, 45 cases of ASH in official matches (31,808 fights in total) were recognised by the Japan Boxing Commission (JBC), of which 15 were fatal. The ASH rate was 0.14% per match, almost twice that of other countries, and the probability of death was 0.24 per 1000 athletes. ASH was not necessarily more common in heavyweight or inexperienced fighters; however, it was more common in flyweights and super flyweights, more common in 10-round fights (JBC-certified A class), and less common in 4-round fights (JBC-certified C class). Furthermore, ASH was found to be more common in fights lost by knockout and occurred significantly in the latter part of the fight. In comparison with other sports, the fatal accident probabilities in jockeying, hang gliding, and college football in the USA were reported to be 12.8, 5.1, and 0.3 per 1000, respectively, indicating that professional boxing does not have a particularly high fatal accident rate. However, they may include causes other than ASH. In addition, boxing is the only sport in which the goal is to knock out an opponent with a direct blow to the head, which is undeniably different from other sports in which accidental injuries occur. In American football, a representative contact sport in which players collide violently with each other, a number of fatal accidents occurred in 1970, which became a social problem. This shows the recommendation of the medical doctors’ efforts, as well as the fact that direct blows to the head were dangerous. In Japan, efforts have been made to avoid the occurrence of ASH in professional and amateur boxing [26]. Specifically, efforts have been made to establish a backup system for specialised medical facilities that are relatively close to the fight venue, abolish scheduled 15-round fights, conduct weigh-ins on the day before the fight, and educate boxing professionals by doctors on health management and accident cases. Since 1983, major organisations worldwide have changed from 15-round systems to 12-round systems. The move to avoid ASH was accelerated as much as possible.
Although the impact strength of the punch itself is a factor in the occurrence of ASH, as it often occurs in the second half of the match, fatigue or a mild concussion state may cause a decrease in the muscle tone of the neck muscle group, contributing to the acceleration of the head caused by the blow. Moreover, owing to the unique strategy of boxing, few athletes tend to hydrate adequately during matches, which may lead to excessive dehydration and may be a factor in the development of ASH. Therefore, regardless of previous medical efforts, boxing should be recognised as a sport in which ASH may occur. Earlier stoppage of fights and hydration within acceptable limits are recommended for fights scheduled for longer rounds.
3.2 Concussion
Although sports-related neurological trauma tends to focus on severe cases, sending patients with impaired consciousness and neurological symptoms to the emergency department immediately after injury is not controversial, and the treatment plan and prognosis do not change significantly regardless of the injury mechanism. In fact, seemingly minor ‘concussions’ can be considered a major problem [27, 28]. In boxing, high-intensity, practical sparring is often included in the training menu as official fights approach. Professional boxers, like amateur boxers, spar with headgear, to prevent trauma. Although headgear is effective in preventing skin lacerations and fractures, it cannot be said to play a role in preventing damage to the cranial nerves, that is concussion. This is supported by the fact that concussion-related injuries have been observed in sparring sessions and official amateur fights, even when headgear is worn. Some concussions diagnosed on the training ground or in the competition are later found to be haemorrhages or cerebral contusions after a medical examination, and even specialists find it difficult to distinguish between these immediately after onset [29]. In a survey of 632 professional boxers on the effects of punching, what ‘works’ for the athlete was concussion-related accounted for more than 90% of the cases [26]. The specific punches that led to this were said to be straight punches to the jaw; however, in reality, they were more often hook punches that rotated the head to the jaw or side of the head. This may be related to the report by Gennareli [30] stating that diffuse injuries, as typified by concussions, are highly correlated with impacts that have a relatively long impact time and produce a rotational acceleration of the head.
In a large-scale survey in Japan, approximately 30% of boxers who had experienced a knockout experienced memory impairment, and approximately 80% had symptoms associated with post-concussion syndrome, such as headache, nausea, vomiting, tinnitus, and dizziness post-fight [26]. Notably, even in players who were knocked out, symptoms, such as headache and other symptoms often abated within a week. However, a problem arises in relation to the second impact syndrome [31, 32], which describes the possibility of more severe brain tissue damage if the player suffers another blow to the head in the presence of concussion-related symptoms, albeit transient. This condition occurs in boxing, football, and other sports, in which head trauma causes diffuse brain swelling and other severe disorders during concussion, resulting in a poor prognosis. In addition, when the symptoms of concussion persist for approximately three months, it is encompassed by the concept of post-concussion syndrome [33], and although its pathogenesis is unknown [34], it must be borne in mind that it can also lead to chronic brain injury with higher brain dysfunction and other complications. Therefore, in the daily healthcare of boxers, it is essential to avoid blows to the head or to seek medical attention during periods of post-concussion syndrome, as has been suggested in other countries.
Currently, guidelines for staged returns to competition after concussion have been proposed [35, 36]. The JBC extended the suspension period for knockout boxers from 45 to 60 days; however, concussions can still occur in daily practice. However, concussions can occur in daily practice because of the competitive nature of boxing. Therefore, it is necessary to take adequate measures against concussions by selecting sparring partners according to physique and experience, reviewing the number of rounds and interval times of sparring, providing hydration to prevent dehydration and maintain performance. Additionally, it is essential to undertake adequate measures against concussions usingconcussion recognition tool 5 (CRT5) and periodic head computed tomography (CT) and magnetic resonance imaging (MRI) examinations at medical institutions.
4. Boxing and technology
4.1 Acquiring the correct form for first-time learners
Information technology has been widely introduced in sports training in baseball, football, and tennis [37, 38]. Notably, virtual reality (VR) and augmented reality (AR) technologies, used for image training and feedback through visualisation have been introduced. Systems have also been proposed the use of skeletal information to learn the correct form in golf and dance [39, 40, 41]. Learning form is an important aspect of learning in several sports [42]. The same applies to boxing, in which the correct punching form is first taught by an instructor. However, there are cases in which direct instruction is difficult because of a lack of instructors in rural areas or boxing gyms in some areas. In such cases, when beginners in boxing competitions practice on their own, they may refer to videos or instructional books; however, there is no correct feedback from the learner; thus, there is a possibility that they may learn incorrect forms.
With the increase in health consciousness in the recent years, gamification has attracted attention in the field of fitness, and various digital contents based on boxing have been released. While there are several reviews on the effects of exercise in enabling effective interval training, the system does not require a correct punching form as long as the direction of the punch is consistent to a certain extent. Even if boxing training is for fitness purposes, training with the correct punching form reduces the burden on the body while increasing the exercise effect and preventing injuries. In other words, the benefits of acquiring the correct punching form are significant, even if not for competitive purposes. Till date, to establish a teaching method for beginners, there have been reports verifying the movements of experienced and inexperienced players from biomechanical elements using electromyography and floor reaction force measurements, as well as attempting to determine the indicators of correct form from the pelvis rotation angle, rotation angle speed, and rotation time using a three-dimensional movement analysis system [43, 44]. However, it has been difficult to utilise these methods as general teaching methods because of the time factor in analysis, cost of equipment for analysis devices, and practical movement guidance. Against this background, the integration of boxing and technology is at a stage of rapid development with the need for technological applications that make full use of VR and AR systems, making it easy to obtain appropriate feedback information on an individual basis.
4.2 The birth of quantitative movement analysis software specifically for boxing competitions
VR and AR systems are effective technological techniques for beginners to acquire correct form; however, boxing itself is an interpersonal sport in which fists exchange in front of each other to knock each other out. This requires skill in both attack and defence, as well as strong mental strength to overcome anxiety and fear. Therefore, before introducing scientific innovations in offence and defence, we will first discuss the psychological characteristics of boxers.
To achieve the best results and records in sporting situations, it is essential to optimise psychological conditioning prior to competition and technical and physical training [45]. Therefore, understanding the psychological state of athletes prior to competition is considered one of the preparatory steps to achieve the desired results [46]. Boxing is a life-threatening sport, as boxing causes orthopaedic disorders (Figure 2) as well as brain disorders such as punch-drink syndrome [27]. Although boxers are often featured for their extremely trimmed, refined bodies, as in other sports, they are a sport that emphasises the importance of physical and mental balance. This is because it requires a high level of emotional intelligence [47], including feelings, coping, and adaptation to changing conditions. There are numerous reports on competition anxiety in athletes [48, 49, 50, 51]. When looking at mental characteristics from the perspective of both competition anxiety and emotional intelligence, boxers tended to have higher competition anxiety than general reference values. Furthermore, by examining mental characteristics using the Emotional Intelligence Scale (a psychological test to assess emotional intelligence), it has been suggested that competition characteristics lead to differences in the corresponding domains in emotional intelligence. This is connected to the needs of the athletes, and in boxing, where the athletes are prone to mental instability, advice and guidance in the areas of “interpersonal response” and “situational response” are effective. In addition, the manner in which the athlete is approached must be considered, depending on whether the recipient is male or female [52, 53]. Regarding the differences in effective voice-overs according to sex, for example, male players tend to have a result-oriented mindset and, therefore, prefer simple, theoretical voice-overs that are directly related to winning or losing, whereas female players tend to focus on the process leading up to the result and sympathetic voice-overs that are more in tune with their emotions at the time are more effective. In contrast, female athletes tend to focus more on the process leading to the outcome, and sympathetic voice-overs that are more in tune with their emotions at the time are more effective.

Figure 2.
Typical examples of sports injuries (orthopaedic conditions) from boxing, from left to right: Eyelid laceration, nasal bone fracture, boxer’s fracture (second middle phalanx fracture).
The influence of mental characteristics and vocalisation on boxers was introduced; however, the root of competition anxiety is not anxiety about being hit by an opponent and suffering trauma or disability, but anxiety about losing a match and the future after losing. These factors have a significant influence on the boxers’ competition anxiety. We believe that these factors have a significant impact on boxers’ competitive anxiety. If this is the case, how one can scientifically work on strategies to win can be one of the factors in eliminating anxiety and bringing one closer to achieving the best performance. Training science is utilised to improve physical function, and strategies to maximise the effects of training are derived from nutritional science. There arises a question of how key offensive and defensive boxing techniques are tackled. In general, apart from physical training, boxers improve their offensive and defensive boxing skills through shadow boxing, sandbagging, mitting, and sparring. Once an opponent has been decided upon, the boxer and coach review the footage of previous fights to identify weaknesses and develop a strategy. However, the question remains as to whether this strategy is scientific. In many cases, strategies are constructed based on the senses of the players and coaches by repeatedly checking parts of the footage. This was probably because no analysis software was specifically designed for boxing. Therefore, we have spent two years developing a quantitative movement analysis software specifically for boxing, with the aim of preventing sports injuries and improving offensive and defensive performance.
4.3 Features of quantitative movement analysis software specific to boxing competitions
What does it take to develop the boxing strategy? It begins with an accurate understanding of one’s own characteristics as a boxer and those of one’s opponents. To achieve this, we built a system in which past match footage and current sparring footage were imported into a quantitative movement analysis software, and the following items were extracted as a result of the extraction of analysis points and quantitative analysis (Figure 3).
Number of attacks (total number and changes over time in each round)
Hits (total number of rounds)
Attack trends (types of single shots and combination patterns).
The type of attack (single or combination pattern types) that inflicted a hit.
Attack sites (total number of rounds).
Number of bullets (total and round)
Types of attacks (single-shot and combination pattern types).
Trends in defence (choice of defence methods for single and combined types).
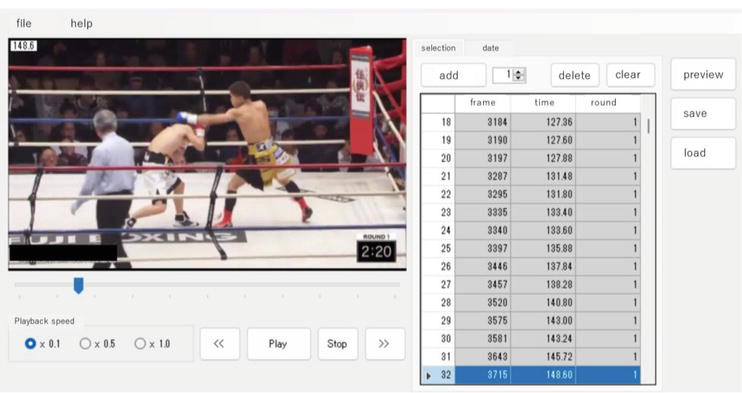
Figure 3.
Boxing-specific quantitative movement analysis software.*
*This software is designed to analyse athletic performance quantitatively by importing match footage into the software, extracting analysis points along the time axis, and selecting and inputting information such as the type of attack, type of defence, attacking area, and presence or absence of hits.
Points (i)–(v) clearly indicate the points that need to be strengthened from an offensive aspect. In (i), it is possible to ascertain the degree of aggressiveness throughout the match and whether the player was in control of the match. In addition, because the number of attacks accumulates every 60 s in each round, it is possible to grasp the relationship with the stamina within a round and throughout the match. In (ii), the accuracy of the attacks can be determined using step (iii), the attack pattern can be objectively understood. This is useful for correcting the ratio of single shots and combinations and the bias of combination patterns. (iv) It helps to check the accuracy of specific types of attacks. For example, in combination patterns, it is possible to determine the number and types of attacks that increase the hit rate. In (v), it is useful to determine the attack ratio between the head and abdomen to correct for the bias towards the attacking part.
Points (vi) to (viii) clarify the points that must be strengthened on the defensive side of the game. In (vi), the definition of “bullet” is a strike by an opponent to an unguarded part of the face or body. The overall defensive technique can be explored by understanding the rate of being hit by bullets throughout the match and the rate of being hit by bullets in each round. At point (vii), it is possible to determine the specific type of attack that results from being hit by the bullets. It is possible to clarify the relationship between the attack trajectory and the rate of being hit in the single and combination patterns. (viii) It provides an opportunity to review whether a defensive selection is appropriate for each attack by an opponent. In other words, it is useful for correcting the tendency or habit of being hit by a certain stance or the same defensive choice in a certain attack or combination pattern.
We believe that using this system [54] to analyse yourself and your opponents will help you build more scientifically based strategies, reduce competition anxiety, reduce sports injuries and disorders, and get closer to achieving the best performance.
5. Examples of the operation of boxing-specific quantitative movement analysis software
Herein, we present our efforts to improve competitive performance, mainly in defensive techniques, using boxing-specific quantitative movement analysis software.
5.1 Experiments
Efforts to prevent trauma and injury in boxing, as in other sports, began with the recognition of the importance of warming up and cooling down and have continued to the present day through repeated improvements in equipment, such as gloves, headgear, and mouthguards, and revisions to the rules of sports. In amateur boxing, the International Amateur Boxing Association revised its rules, and since the 1984 Los Angeles Olympic Games, Olympic-style boxing has been practiced using a points system without the aim of knocking out fighters. Most injuries occur in high school and university students. In particular, medical staff are required to propose and implement methods to scientifically and comprehensively prevent traumatic injuries and disorders from various perspectives, not only from the viewpoint of treatment, but also from returning to competition.
Therefore, this study developed a quantitative movement analysis software specifically for boxing competitions and focused on the changes in the rate of bullet hits throughout the match, positioning it as a basic study for the primary prevention of sports injuries.
5.1.1 Methods
5.1.1.1 Subjects
The subjects were active boxers (male, 12 subjects) with JBC-accredited professional boxing qualifications, mean age: 22.8 ± 4.3 years, and 4.2 ± 2.1 years (mean ± standard deviation) of competitive experience.
5.1.1.2 Experimental procedure
Based on the analysis software, six subjects were randomly assigned to the task condition (task group) and six to the control condition (control group). All subjects were quantitatively analysed using analysis software on the video footage of their first match after the start of the study to extract the subject’s overall shot rate for the match as a baseline evaluation measure. Subsequently, the subject group was given feedback on the analysis results to the trainers and players, and was subjected to a training program based on the analysis results for approximately three months until the next match, whereas the control group was not given the analysis results and was subjected to normal practice until the next match. Finally, the video footage of the second match after the start of the study was analysed in the same manner as that of the first match, and the overall rate of bullet hits was compared and verified between the groups before and after the intervention (Figure 4).
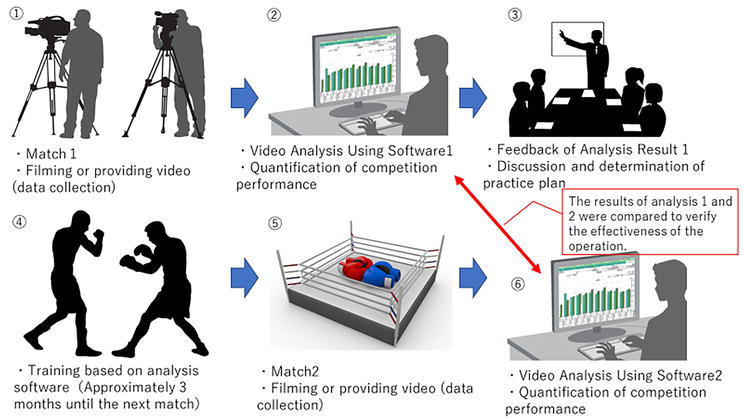
Figure 4.
Experimental methodology flow using boxing-specific quantitative movement analysis software.
Motion analysis software was developed specifically for boxing competitions to enable the quantitative evaluation of offensive and defensive performances. Specifically, the software was programmed to extract analysis points in the offence and defence based on match footage and to quantitatively analyse the choice of defence method for each type of attack, the attacking area, whether or not the fighter was hit, the number of hits, and the hit rate (Figure 3). These can be analysed over time in each round and output as a competition performance evaluation table so that players and trainers can easily understand the analysis results.
5.1.1.3 Statistical processing
Statistical analysis was performed using the bullet coverage rate for the entire match. A repeated-measures analysis of variance was conducted on the change in the bullet rate, with the measurement condition (first match × second match) and task condition (task group × control group) as the two factors, and the Bonferroni method was used for multiple comparisons. The statistical analysis software was SPSS25.0. J for Windows, and the significance level was set at 5%.
5.1.2 Results
The results of a comparison of the overall match exposure rate between “with/without analysis software” and “measurement period” showed no main effect for “with/without analysis software” [F (0.267), P = 0.5924] and a main effect for “measurement period” [F (3.682), P = 0.02]. There was no interaction between factors [F (0.363), P = 0.8577]. The results of the multiple comparison test in the ‘measurement period’ showed that the FTS group had a significantly lower rate of exposure after the intervention compared to before (P < 0.05). No significant differences were found between the pre- and post-intervention comparisons in the control group (P > 0.05).
5.1.3 Considerations
This study was positioned as basic research on the primary prevention of sports injuries in boxing; quantitative movement analysis software specific to boxing competitions was developed, and changes in the rate of exposure to bullets were verified from its operation.
The task group showed a significantly lower rate of bullet hits throughout the match after intervention. However, there was no significant change in the control group in the pre- and post-intervention comparisons. The reason for the low rate of hits in the entire match after the introduction of the analysis software was that the players themselves were able to quantitatively analyse the types of attacks in which they were hit, the combination patterns in which they were prone to being hit, and the types of defence they chose against each type of attack in which they were prone to being hit and to use this information as a numerical value and reference for the analysis of the game. It can be inferred that the players were able to implement a cautionary strategy based on an image of movement by looking back at numerical and visual images and that they were able to conduct training to efficiently improve their defensive skills until the next game based on the results of the analysis. As background, Sakamoto et al. [55] reported that combining observations of behaviour and images when performing motor imagery facilitated corticospinal tract excitability better than manipulations performed alone. Sakuraba et al. [56] also reported that appropriate attentional strategies based on individual-specific motor imagery can improve performance during motor learning tasks. In the present study, we did not add assessment items to the motor imagery; therefore, we were unable to observe the neurophysiological aspects of these changes. However, because the players and coaches were able to logically reflect on the match while receiving match footage, analysis materials, and feedback from the analysts, it is possible that during the feedback, the excitability of the corticospinal tracts was enhanced and motor-related areas, such as the supplementary motor cortex, were activated. Therefore, the task group also contributed to the construction and reproduction of motor images, such as the trajectories of the attacks that were being hit, the types of attacks, and the corresponding defence choices, which could have been reflected from a scientific perspective in the understanding and efforts of tailor-made countermeasure programs based on analysis software.
This study explored the possibility of primary prevention of sports injuries in boxing from a technological perspective using the index of the rate of bullet wounds in the entire match. Boxing is a sport in which the attack sites are limited to the head and abdomen, and as a result, brain damage tends to accumulate more than in other martial arts such as karate and kickboxing [57, 58]. Reducing the rate of exposure is directly related to reducing the risk of brain damage. It may also have the potential to preserve the lives of athletes and reduce the risk of chronic traumatic encephalopathy, a condition known as punch-drunk syndrome, in post-athletic lives.
In the future, neurophysiological evaluations during feedback using analysis software will be added, and the relevance of sex differences, age, competition history, and competition anxiety will be examined from various perspectives. We also aim to introduce programming techniques to improve the accuracy of the analysis and develop a technology that enables timely feedback of the analysis results during the competition interval.
Finally, we strongly believe in the potential of the fusion of sports and technology to brighten the future of athletes and will continue to explore this.
Acknowledgments
This study was part of a research program funded by Tokoha University. The funding source had no role in the study design/concept, data collection/analysis/interpretation, and manuscript preparation/submission.
References
- 1.
Bledsoe GH et al. Injury risk in professional boxing. Southern Medical Journal. 2005; 98 :994-998 - 2.
Siewe J et al. Injuries in competitive boxing: A prospective study. International Journal of Sports Medicine. 2015; 36 (3):249-253 - 3.
Teramoto M, Cross CL, Cushman DM, Willick SE. Boxing fatalities in relation to rule changes in Japan: Secondary data analysis. The Physician and Sports Medicine. 2018; 46 (3):349-354 - 4.
Homer. The Iliad of Homer. Seattle: Createspace Independent Publication; 2016. pp. 142-144 - 5.
Kruszewski A. From ancient patterns of hand-to-hand combat to a unique therapy of the future. International Journal of Environmental Research and Public Health. 2023; 20 (4):3553 - 6.
Poliakoff MB. Combat Sports in the Ancient World. New Haven and London: Yale University Press; 1987. pp. 149-157 - 7.
Miller SG. Ancient Greek Athletics. New Haven and London: Yale University Press; 2004. pp. 90-91 - 8.
Young DC. A Brief History of the Olympic Games. Wiley-Blackwell; 2004. pp. 5-6 - 9.
Anderson J. The Legality of Boxing: A Punch Drunk Love? London: Birkbeck Law Press; 2007. pp. 15-16 - 10.
Rodriguez RG. The Regulation of Boxing: A History and Comparative Analysis of Policies Among American States. McFarland Publishing; 2009. pp. 56-64 - 11.
Boddy K. Boxing: A Cultural History. London: Reaktion Books; 2019. pp. 26-54 - 12.
Harris B. Intolerance: Divided Societies on Trial. Vol. 182. Wildy: Simmonds and Hill Publishing; 2008 - 13.
Beth A, Tommasone, Tamara C, McLeod V. Contact sport concussion incidence. Journal of Athletic Training. 2006; 41 :470-474 - 14.
Jordan BD et al. Amateur boxing injuries at the US Olympic training Center. The Physician and Sportsmedicine. 1990; 18 :80-90 - 15.
Loosemore M, Knowles CH, Whyte GP. Amateur boxing and risk of chronic traumatic brain injury: Systematic review of observational studies. British Journal of Sports Medicine. 2008; 42 :5640567 - 16.
Zazryn TR et al. A 16 year study of injuries to professional boxers in the state of Victoria Australia. British Journal of Sports Medicine. 2003; 37 :321-324 - 17.
Zazryn TR et al. A prospective cohort study of injuries in amateur and professional boxing. British Journal of Sports Medicine. 2006; 40 :670-674 - 18.
Richard J, Butler MS. Neuropsychological investigation of amateur boxers. br. The Journal of Sports Medicine. 1994; 28 :187-190 - 19.
Ohashi G et al. Problems in the health management of professional boxers in Japan. British Journal of Sports Medicine. 2002; 36 :346-352 - 20.
Sawauchi S, Terao T, Tani S, Ogawa T, Abe T. Traumatic middle cerebral artery occlusion from boxing. Clinical Neuroscience. 1999; 6 (1):63-66 - 21.
Nagaoka M, Satoh T, Nagao S, Matsuzaki H. Extensor retinaculum graft for chronic boxer’s knuckle. The Journal of Hand Surgery. 2006; 31 (6):947-951 - 22.
Yoneoka Y, Takeda N, Inoue A, Ibuchi Y, Kumagai T, Sugai T, et al. Human Kluver-Bucy syndrome following acute subdural haematoma. Acta Neurochirurgica. 2004; 146 (11):1267-1270 - 23.
Kabir Singh Lota, Malliaropoulos N, Blach W, Kamitani T, Ikumi A, Korakakis V, et al. Rotational head acceleration and traumatic brain injury in combat sports: A systematic review. British Medical Bulletin. 2022; 141 (1):33-46 - 24.
Benjamin Todd Drury, Lehman TP, Rayan G. Hand and wrist injuries in boxing and the martial arts. Hand Clinics. 2017; 33 (1):97-106 - 25.
Jordan BD. Chronic traumatic brain injury associated with boxing. Seminars in Neurology. 2000; 20 (2):179-185 - 26.
Tani S et al. Acute subdural haematomas in boxer-correlation with diffuse brain injury. International Conference on Recent Advances in Neurotraumatology. 1994; 36 (5):325-328 - 27.
Förstl H, Haass C, Hemmer B, Meyer B, Halle M. Boxing-acute complications and late sequelae: From concussion to dementia. Deutsches Ärzteblatt International. 2010; 107 (47):835-839 - 28.
Makdissi M, Critchley ML, Cantu RC, et al. When should an athlete retire or discontinue participating in contact or collision a systematic review. British Journal of Sports Medicine. 2023; 57 (12):822-830 - 29.
Musumeci G, Ravalli S, Amorini AM, Lazzarino G. Concussion in sports. Journal of Functional Morphology and Kinesiology. 2019; 4 (2):37 - 30.
Gennareli TA. Head injury in man and experimental animals clinical aspect. Acta Neurochirurgica. 1983; 32 :1-13 - 31.
Saunders RL, Harbaugh RE. The second impact in catastrophic contact-sports and trauma. Journal of the American Medical Association. 1984; 252 :538-539 - 32.
Cantu RC. Second-impact syndrome. Clinics in Sports Medicine. 1998; 17 :37-44 - 33.
Lishman WA. Physiogenesis and psychogenesis in the ‘post concussional sydrome’. The British Journal of Psychiatry: The Journal of Mental Science. 1988; 153 :460-469 - 34.
Silverberg ND, Iverson GL. Etiology of the post-concussion syndrome: Physiogenesis and psychogenesis revisited. Neuro Rehabilitation. 2011; 29 :317-329 - 35.
McCrory P, Meeuwisse W, Johnston K. Consensus statement on concussion in sport: The 3rd international conference on concussion in sport held in Zurich, November 2008. British Journal of Sports Medicine. 2009; 43 (Suppl 1):76-90 - 36.
Mccrory P, Meeuwisse W, Johnston K, et al. Consensus statement on concussion in sport - the 3rd international conference on concussion in sport, held in Zurich, November 2008. Journal of Clinical Neuroscience. 2009; 16 :755-763 - 37.
van Biemen T, Müller D, Mann DL. Virtual reality as a representative training environment for football referees. Human Movement Science. 2023; 89 :103091 - 38.
Le Noury P, Buszard T, Reid M, Farrow D. Examining the representativeness of a virtual reality environment for the simulation of tennis performance. Performance. Journal of Sports Sciences. 2021; 39 (4):412-420 - 39.
Ikeda A, Tanaka Y, Hwang D-H, Kon H, Koike H. Golf training system using sonification and virtual shadow. In: ACM SIGGRAPH 2019 Emerging Technologies. Vol. 14. New York, NY, USA: Association for Computing Machinery; 2019. p. 2 - 40.
Chan JCP, Leung H, Tang JKT, Komura T. A virtual reality dance training system using motion capture technology. IEEE Transactions on Learning Technologies. 2011; 4 (2):187-195 - 41.
Kyan M, Sun G, Li H, Zhong L, Muneesawang P, Dong N, et al. An approach to ballet dance training through MS Kinect and visualization in a CAVE virtual reality environment. ACM Transactions on Intelligent Systems and Technology. 2015; 6 (2):23-37 - 42.
Craig CM, Berton E, Rao G, Fernandez L, Bootsma RJ. Judging where a ball will go: The case of curved free kicks in football. Die Naturwissenschaften. 2006; 93 (2):97-101 - 43.
Adamec J, Hofer P, Pittner S, Monticelli F, Graw M, Schöpfer J. Biomechanical assessment of various punching techniques. International Journal of Legal Medicine. 2021; 135 (3):853-859 - 44.
Whiting WC, Gregor RJ, Finerman GA. Kinematic analysis of human upper extremity movements in boxing. The American Journal of Sports Medicine. 1988; 16 (2):130-136 - 45.
Guidetti L, Franciosi E, Emerenziani GP, et al. Assessing basketball ability in players with mental retardation. British Journal of Sports Medicine. 2009; 43 (3):208-212 - 46.
Bales J, Bales K. Triathlon how to mentally prepare for the big race. Sports Medicine and Arthroscopy Review. 2012; 20 (4):217-219 - 47.
Lane AM, Meyer BB, Devonport TJ, et al. Validity of the emotional intelligence scale for use in sport. Journal of Sports Science and Medicine. 2009; 8 (2):289-295 - 48.
Filaire E, Sagnol M, Ferrand C, et al. Psychophysiological stress in judo athletes during competitions. The Journal of Sports Medicine and Physical Fitness. 2001; 41 (2):263-268 - 49.
Turner PE, Raglin JS. Variability in precompetition anxiety and performance in college track and field athletes. Medicine and Science in Sports and Exercise. 1996; 28 (3):378-. 385 - 50.
Tenenbaum G, Furst D, Weingarten G. A statistical reevaluation of the STAI anxiety questionnaire. Journal of Clinical Psychology. 1985; 41 (2):239-244 - 51.
Raglin JS, Morris MJ. Precompetition anxiety in female volleyball players-a test of ZOF theory in a team sport. British Journal of Sports Medicine. 1994; 28 (1):47-51 - 52.
Dilip R, Patel, Omar H, Terry M. Sport-related performance anxiety in young female athletes. Journal of Pediatric and Adolescent Gynecology. 2010; 23 (6):325-335 - 53.
Scott-Hamilton J, Schutte NS, Brown RF. Effects of a mindfulness intervention on sports-anxiety, pessimism, and flow in competitive cyclists. Applied Psychology. Health and Well-Being. 2016; 8 (1):85-103 - 54.
Nakamura K et al. Basic research on the primary prevention of boxing-related sports injuries with the development of a quantitative motion analysis software. Journal of Physical Therapy Science. 2021; 33 (6):495-498 - 55.
Sakamoto M, Muraoka T, Mizuguchi N, et al. Combining observation and imagery of an action enhances human corticospinal excitability. Neuroscience Research. 2009; 65 (1):23-27 - 56.
Sakuraba T, Hirai M, Watanabe E. Optimization of a motor learning attention-directing strategy based on an individual’s motor imagery ability. Brain Research. 2016; 234 (1):301-311 - 57.
Moseley IF. The neuroimaging evidence for chronic brain damage due to boxing. Neuroradiology. 2000; 42 :1-8 - 58.
Constantoyannis C, Partheni M. Fatal head injury from boxing: A case report from Greece. British Journal of Sports Medicine. 2004; 38 :78-79