 Open access peer-reviewed chapter
Open access peer-reviewed chapter
Abstract
The emergence of severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) variants has been considered responsible for the prolonged continuation of the coronavirus disease 2019 (COVID-19) pandemic. The fast dissemination of these variants presents a challenge for current vaccines. Next-generation vaccinations must be manufactured and distributed quickly to stop the pandemic. To combat existing variations and stop the development of new ones, coordinated surveillance, the designing of new vaccines, and broad-scale immunization are required. Clinical trials are still being conducted to assess the efficacy of the vaccination against various SARS-CoV-2 variants.
Keywords
- mutant
- variants
- serology
- omicron
- SARS-CoV-2
- COVID-19
1. Introduction
Since its emergence, coronavirus disease 2019 (COVID-19) has resulted in 520,912,257 and 6,272,408 confirmed cases and deaths, respectively. Scientists have been reported to produce a variety of vaccines, with 198 in preliminary stages of development and 156 in worldwide clinical trials. There have been 11,713,606,779 doses of vaccine provided since May 16, 2022. The total number of confirmed infections has dramatically grown after October 11, 2021, yet there has not been a discernible change in the COVID-19 incidence since that date. As a result, there is now a greater chance of developing new mutations, such as variants of concern (VOC) and variants of interest (VOI), which have a greater potential of spreading and infecting others while being less likely to be recognized by host antibodies. This chapter will keep track of the most recent SARS-CoV-2 variations and mutations, provide an overview of therapeutic studies, and discuss current pandemic-fighting issues and potential solutions.
2. Origin of SARS-CoV-2
Severe acute respiratory syndrome coronavirus 2 (SARSCoV2) shares approximately eighty percent (79%) homology with SARS-CoV, and other highly deadly human coronaviruses have been zoonotic in origin. A significant quantity of antibodies against SARS-CoV-2 were discovered in isolates of the virus of Himalayan palm tree civets and raccoon dogs. Bats serve as a major reservoir for several SARS-like viruses due to their infection with SARS-CoV-2 and other ancestors of the SARS virus. Horseshoe bats that had taken up residence in caverns in the Yunan region of mainland China were found as the first reservoir for the emergence of SARS-CoV-2. The distance in time and space between the ancient Yunnan caves and the initial appearance of SARS-CoV-2, however, emphasizes how challenging it is to find out the virus transmission pathways. SARS-CoV-2 originated in China in 2019, disseminated through dense populations of live animals that may have been infected with SARS-CoV2, and is now globally transmitted through human-to-human transmission, with higher susceptibility in carnivores such as cats, ferrets, and raccoon dogs. Further investigation is needed to determine its potential in animal populations. The natural origin of SARS-CoV-2 lineages is depicted in Figure 1.
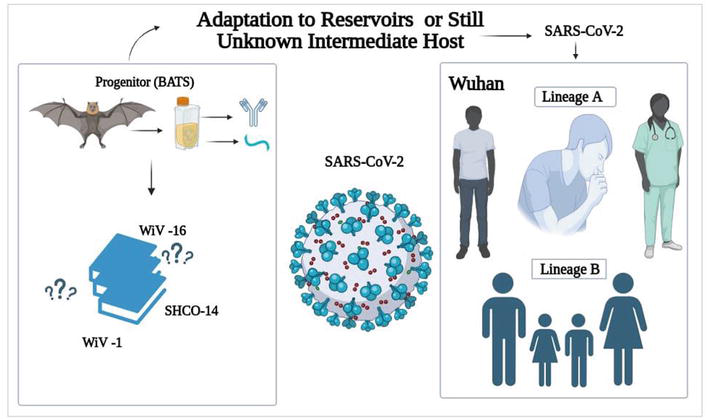
Figure 1.
Natural origin of SARSCoV2 lineages.
3. SARS-CoV-2 and evolutionary lineages
A ribonucleic acid (RNA) virus called SARS-CoV-2 possesses a 3-to-5 exonuclease enabling high-fidelity reproduction. As a consequence of the COVID-19 pandemic, nearly three thousand (2920) genomes were collected between December 2019 and April 2022, and these variants of the SARS-CoV-2 virus are unique. These genetic lineages have been identified and followed using Nextstrain, Pango, and the Global Initiative on Sharing All Influenza Data (GISAID). The World Health Organization (WHO) has named two VOIs and VOCs using Greek alphabet letters to prevent confusion. Despite mutations, it replicates efficiently, with an evolution rate of 2 mutations per month between 2019 and 2020. The 614G variant of SARS-CoV-2 has gained global attention due to its superior viral entry and replication efficiency and its higher fitness compared to the 614D variant. Consequently, variants of concern (VOC) have emerged.
The ecological behavior of SARS-CoV-2 emphasizes the potential for cross-species transmission, evident in cases involving farmed minks, dogs, cats, and lions in zoos. When animals are infected, the virus has the opportunity to evolve and adapt, as observed in minks in the Netherlands and Denmark. Infections in animals carrying the human SARS-CoV-2 strain might lead to recombination events, potentially giving rise to hybrid viruses with pandemic potential. The newly discovered VOCs and VOIs of SARS-CoV-2 have been reported to indicate worse clinical symptoms, higher transmissibility, diagnostic detection challenges, escape from vaccine-induced or innate immunity, and adverse therapeutic responses. The most important variants are Alpha, Beta, and Gamma. The Delta variant’s frequency increased rapidly, with Omicron currently accounting for 5% [1]. Detailed information regarding the dates and countries of emergence of SARS-CoV-2 variants have been depicted in Figure 2.
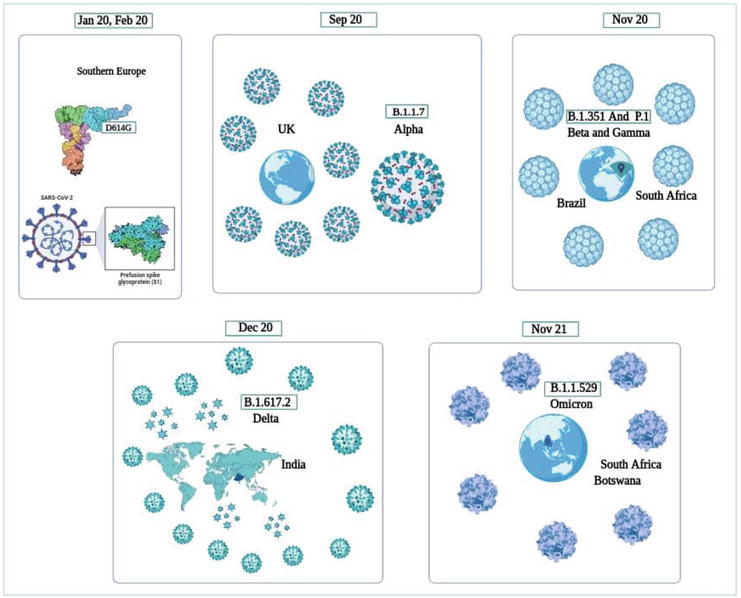
Figure 2.
Emergence of SARS-CoV-2 variants.
4. SARS-CoV-2 variants and their characteristics
Current COVID-19 vaccines elicit broad immune responses, protecting new virus variants such as Omicron; more research is needed to determine their effectiveness. Variants are divided into several classes by the WHO and the Center for Disease Control and Prevention (CDC). A SARS-CoV-2’s VOI differs from earlier strains of the virus in that it has alterations that are possibly to blame for the virus’s enhanced transmissibility and the capacity to elude diagnostic tests, evade immunity, or cause severe illnesses. A VOC is potentially transmissible and more likely to induce new infections. This category includes the delta and omicron versions. A high-impact variant is one from which current immunizations do not offer protection. There are no any SARS-CoV-2 variants in this category right now. The WHO classified VOCs of SARS-CoV-2 with enhanced virulence, transmissibility, and resistance to current therapeutic vaccines, diagnostics, and other such medical techniques. Notable VOCs include alpha (α), beta (β), gamma (γ), delta (δ), and omicron. The SARS-CoV-2 lifecycle begins with the S1 receptor-binding domain (RBD) and angiotensin-converting enzyme 2 (ACE2) interacting, causing the S protein to divide into S2 subunits. The S protein is degraded by the furin that further triggers the virus particles to enter the cellular membrane of the host cell. Sixteen nonstructural proteins are produced, which are followed by their translation into replicase protein and their destruction by proteases. Double-membrane vesicles (DMVs) aid in RNA replication, whereas E, M, and S proteins create mature virions for infection. The mechanism of SARS-CoV-2 infection is depicted in Figure 3.
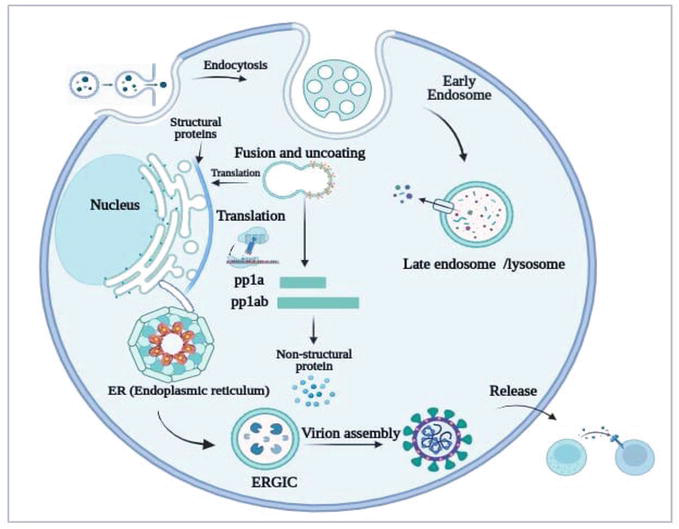
Figure 3.
Mechanistic pathway of SARS-CoV-2 infection: The replication process of SARS-CoV-2 involves the development of DMVs (double-membrane vesicles) in host cells. Viral RNAs are retained in DMVs and transferred for assembly or translation to the cytosol. Structural proteins form viral particles, whereas sgRNAs encode auxiliary proteins. N protein and RNA synthesis occur in the cytoplasm, whereas E, M, and S proteins are produced in the ER (endoplasmic reticulum). Two thirds of the genome’s replicase genes are translated into two big polyproteins, pp1a and pp1ab, and from there, sixteen types of nonstructural proteins (NSP) are produced. The viral RNA-N complex, E, M, and S proteins then enter the ERGIC, where mature virions are assembled. The ERGIC further undergoes significant N-glycosylation, controlling protein folding, stability, infectiousness, and immunological evasion [
The initial stage in replication is the development of DMVs (vesicles with double membranes) in a host cell brought by the COVID-19 infection. NSP3 and NSP4 stimulate the replication of both sgRNA (subgenomic RNA) and gRNAs (genomic RNAs) and cause the endoplasmic reticulum’s (ER) reorganization into DMV [3]. The viral RNAs are retained in DMVs and either transferred via double-membrane-spanning pores for the viral assembly or to the cytosol for translation [4]. Structural proteins assemble gRNA into viral particles, whereas sgRNAs encode auxiliary and conserved structural proteins. RNA and N protein synthesis takes place in the cytoplasm, whereas S, M, and E proteins are produced in the endoplasmic reticulum, or ER, and transported to the Golgi system. The SARS-CoV-2 genome consists of replicase genes translated into pp1a and pp1ab polyproteins, processed into 16 NSPs, and assembled in the ERGIC compartment. These virions then escape the Golgi apparatus and cell membrane. In the ERGIC, the S protein monomer undergoes substantial N-glycosylation modification as well. In addition to controlling protein folding, glycosylation of virus proteins additionally influences virus stability, infectiousness, and immunological evasion (Figure 3). Studies have discovered 26 mutations, which tend to include six of interest (K417T, N501Y, P681H, L452R, and L18F), with a prevalence rate of more than 75% in at least one lineage across VOCs (five) and VOIs (two). These mutations were found in at least 20% of countries, with N501Y, E484Q , K417N, T478K, S477N, L452R, and E484Q associated with increased ACE2 binding.
4.1 Alpha (α-variant lineage-B.1.1.7)
In 2020 and 2021, three variant strains B.1.351, P.1 COVs, and B.1.1.7, first appeared in the UK (United Kingdom), South Africa, and Brazil. Increased transmission and decreased neutralization that may tend to have an impact on monoclonal antibodies are well-known characteristics of the alpha and beta versions. Mortality and hospitalization to the intensive care unit have risen with alpha variants. Alpha is significantly protected against by the BNT162b2 vaccine; however, the mRNA-1273 vaccine exhibits less neutralization. Gamma variations are less susceptible to therapies and past vaccines and convalescent-serum neutralization.
B.1.1.7, first discovered in September 2020 in the UK and later in the US, has 17 mutations in its genome. Notably, there were eight mutations in the spike protein of the Alpha version, including the deletion of D1118H, N501Y, T716I, A570D, P681H, S982A, D144, and D69–70. The B.1.1.7 protein undergoes amino acid changes that improve ACE2 affinity and RBD accessibility, which may become the reason for enhanced transmissibility.
The protein SARS-CoV2-S is destabilized by the N501Y mutation, which also increases RBD-ACE2 affinity and accelerates the propagation of SARS-CoV-2. Additionally, compared to those infected with other variations, those exposed to the variant lineages of B.1.1.7 suffered from a considerably severe illness and had a greater risk of dying.
4.2 Beta (β- variant lineage 20H and/or B.1.351)
Beta variant has been found responsible for the emergence of the second wave of COVID-19 in the Bay of Nelson Mandela. It was discovered in South Africa (SA) by the end of 2020 [5].
The β-form of the spike protein has nine mutations, which include L18F, N501Y, R246I, E484K, D215G, K417N, A701V, D614G, and D80A. It has been reported that there have been three changes made to the receptor binding domain (RBD) to enhance receptor affinity.
The E484K mutation alters antibody binding to the receptor-binding domain, whereas the N501Y substitution is found in fast-expanding lineages. These mutations play critical roles in disease transmission and outbreaks, increasing compatibility towards human ACE2, and their combination enhances this attraction.
The Beta variant of SARS-CoV-2 has a unique amino acid alteration, P71L, in its E protein, linked to illness severity and death rate, but its impact remains uncertain. It may have a selective advantage.
4.3 Gamma (γ-P.1 lineage)
Eleven mutations in spike protein and three mutations in the region of the receptor-binding domain resulted in the emergence of γ -P.1 variant lineage, which was initially discovered in January 2021 in the United States of America (USA) [6].
Eleven mutations, including L18F, R190S, T1027I, N501Y, K417T, and E484K, D138Y, P26S, H655Y, V1176, and T20N, have been found in the variant’s spike protein. In addition, three changes (K417N, L18F, and E484K) in the RBD of the Gamma (γ) version are comparable to those in the Beta (β) variant.
4.4 Delta (δ-variant lineage B.1.617.2)
Since its discovery in India in 2020, the Delta (-B.1.617.2) mutant lineage has quickly expanded and boosted transmissibility in homes and indoor sports. Additionally, it lessens the neutralization of monoclonal emergency use authorization (EUA) antibody therapies. The efficiency of the Delta vaccine is just 33%, whereas the efficacy of the ChAdOx1 and BNT162b2 nCoV-19 vaccines after two doses is still more than 67%. In April 2021, it was discovered that it had a major effect on the COVID-19 pandemic’s second wave. The Delta variety, which was discovered for the first time in the United States (US) in March 2021, is extremely contagious and prevalent in many nations. It has 11 mutations in the spike protein. It possesses eleven mutations in the protein known as spike [6].
4.5 Omicron (SARS-CoV-2 variant lineage B.1.1.529)
The latest SARS-CoV-2 variant, VOC “Omicron” was first reported in November 2021 in the South Africa (SA) region. This variant has exhibited 50 mutations, thirty-two of which were targeting spike protein and three of which affect the cleavage site of furin and so increase infectivity. The lineage B.1.1.529VOC variant is considered the most contagious form identified and may resist immune defenses provided by current vaccinations or prior infections. According to GISAID, the virus had 6950 cases and had spread to 86 nations and territories by December 16, 2021. Recent research revealed that following immunization with the Pfizer-BioNTech (BNT162b2) vaccine, serum’s neutralization activity against the Omicron variation was forty-one (41.4) times below the original strain; however, the escape was only partially successful. The Omicron variant has a significant capacity to overcome previous infection-related immunity (Ferré et al., 2022).
Since its discovery in November 2021 in South Africa, the Omicron variety has been found in more than 100 nations and areas worldwide. The WHO classified it as a VOC and categorized it among those variants under monitoring. Omicron has 50 mutations, 30 on the surface S protein, 20 novels in the S1 domain, eight in neglected tropical diseases (NTDs), and 15 in RBD. These modifications may improve RBD-ACE2 interaction and accelerate transmission. Omicron’s 3-day incubation time and cold-like symptoms are attributed to its insertion sequence. Omicron, unlike typical influenza, exhibits distinct symptoms such as smell and taste loss, persists in the body, and can reactivate, potentially leading to fatalities. The CDC detected the omicron virus in New York City’s wastewater 10 days before the US first reported illness and South Africa confirmed its presence. Researchers in California, Texas, and France also identified variants. The discovery of omicron presence in certain areas during a specific period holds significant implications for the detection and spread of the virus [7].
4.6 Lambda (λ- C.37 variant lineage) and mu (μ- B.1.621 variant lineage)
The WHO has identified two variants as Lambda (λ) and Mu (μ) lineage variants. The L452Q mutation within RBD of the spike protein, which was initially found in C.37 in Peru and Chile in 2020, improves the virus’s virulence, transmissibility, and infectivity. Recent research demonstrates lower susceptibility to neutralization by convalescent sera and the monoclonal antibody REGN10987 as well as a three (3.05) time reduction in neutralization as compared to the wild-type virus. When compared to the WA1 strain, B.1.621, which was discovered for the first time in January 2021 in Colombia, had a 2.3-fold lower neutralizing antibody response.
5. Major physiological differences among mutant strains
There are now 4 SARS-CoV-2’s VOCs, that is, α- (B.1.1.7), β- (B.1.351), γ - (P.1), and (δ) delta (B.1.617.2). They have shown D614G mutation, which confers higher infectivity, most likely because of alterations in receptor binding or fusion. The N501Y mutation is carried out by α, β, and γ, boosting their receptor-binding efficacy and cellular entrance. Fortunately, combining mutations may result in more conformational alterations and different alterations. VOCs, for example, have varying receptor-binding sites. Separation from the receptor requires the most effort, followed by β/γ or delta.
5.1 Plaque sizes
In Vero E6 cells, all these variations had a distinct plaque size. Beta had the greatest mean plaque size, next to gamma, delta, and alpha. In Vero E6 Transmembrane Protease, Serine2 (TMPRSS2) cells, a comparable result with varied plaque diameters was found. There are various variables of plaque size, including receptor-binding affinities heat stability and viral reproduction rate. If a variation is more stable at physiological temperatures and produces more offspring viruses, it creates larger infectious viral particles, attacking a greater number of cells and raising plaque size.
5.2 Thermal stability
The beta version is the most stable of the 4 VOCs at 4, 24, and 37°C. With a half-life nearly double that of γ or delta, β has the strongest thermal stability. Except for alpha, there is a link between heat stability and plaque size. Interestingly, despite its small plaque size, alpha has a relatively extended half-life, implying an alternate process.
5.3 Viral replication rates
Although there are no substantial changes in viral RNA replica number, Alpha has fewer pathogenic particles than the other versions. Furthermore, alpha and gamma intracellular viral RNA concentrations are substantially lower than those of the other VOCs. Alpha’s viral replication rate is probably inadequate, which contributes to its limited plaque size [8].
6. How to control novel varieties and recurrent outbreaks?
Controlling the pandemic is challenging because of recurrent outbreaks and novel varieties. Effective vaccinations and antiviral therapies are crucial in the early stages, but anti-inflammatory and immunomodulatory therapy could be more effective in later stages. SARS-CoV-2 infection suppression requires monoclonal antibodies, nanobodies, recovered plasma, mini proteins, soluble ACE2, and receptor ACE2 traps, targeting host proteases like furin and TMPRSS2 [9]. The development of a disease is greatly influenced by immune responses, and the SARS-CoV-2 evasion pathways are still poorly known. Immunomodulators have antiviral effects, but their effectiveness in treating COVID-19 remains uncertain. Traditional Chinese medicine effectively combats viruses through immune modulation, whereas vaccine development involves selecting antigens, enhancing sequences, screening nucleotides, evaluating the immune response, and conducting safety tests, with RNA vaccines being the most effective [10]. The mechanistic pathways indicating various mechanisms of antiviral CoV19 therapeutics by inhibiting SARS-CoV-2 entrance, preventing SARS-CoV-2 replication, application of immunomodulators, and vaccine development have been shown in Figure 4.
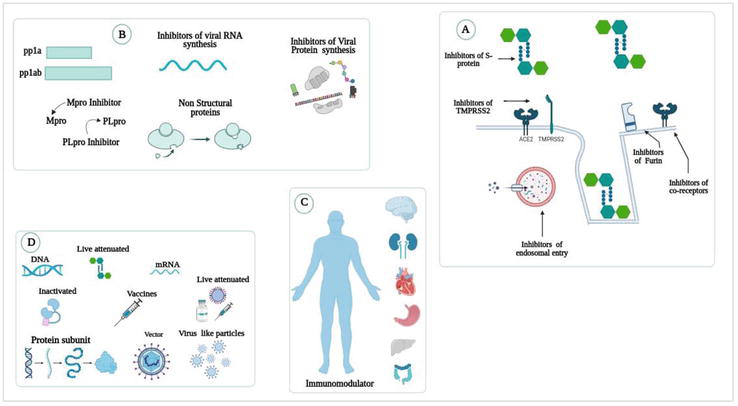
Figure 4.
Antiviral CoV19 therapeutics. A) Inhibition of SARSCoV2 entrance, B) inhibition of SARSCoV2 replication, C) Immunomodulators, and D) vaccine development. * pp1a, pp1ab: Large polyproteins; Mpro:Main protease inhibitor; Plpro:Papain-like protease.
Inhibiting the initial stages (
Antiviral therapy uses blocking viral proteins and RNA synthesis to reduce viral replication. Mpro and PLpro, proteases crucial for viral replication, have potential therapeutic targets. Mpro inhibitors are now in various phases of preclinical and clinical research (Figure 4B) [12]. The immune system’s role in SARS-COV-2 evasion is not fully understood, and the therapeutic benefits of immunomodulators such as ivermectin and interferon on COVID-19 are debatable. The first CoV19 antibody developed by China fetched international approval in December 2021. It has been given commercial approval under the name BRII-196/BRII-198 (Figure 4C) [13, 14].
There are currently almost 340 vaccines widely available against the SARS-CoV-2. One hundred and twenty-two are being applied in various clinical trials. Thirty vaccines, however, are regularly being used worldwide. Primary types include inactivated, attenuated live, DNA/RNA, vector-based, and unidentified forms. RNA vaccines are the most effective vaccines worldwide (Figure 4D) [15, 16]. Future vaccines are expected to offer protection against both current and upcoming SARS-CoV-2 variant strains.
7. COVID-19 vaccine effectiveness on SARS-CoV-2 variants
COVID-19 precise inoculations sanctioned under EUA are distributed into four kinds: inactivated, viral vector, nucleic acid, and subunit. These vaccines rely on the SARS-CoV-2’s S protein to induce neutralizing antibodies. However, the advent of SARS-CoV-2 variants led to hurdles in vaccine improvement. Mutations on the spike protein resulted in improved transmission, severe ailment, diminished neutralization, and invulnerable invasion. VOCs are highly contagious and are related to greater hospitalization rates and death.
7.1 Alpha variant and clinical vaccine trials
The vaccine ChAdOx1, tested against α-variant, showed lower neutralization activity in contradiction to non-Alpha variants. Defensive efficiencies against Alpha (α) and non-Alpha variants were reportedly found at 70% and 81%, respectively. The NVX-CoV2373 vaccine, which was tested contrary to the Alpha variant, exhibited an efficiency of 86.30% in contrast to α variants and 96.40% against non-Alpha variants. The vaccine also showed a 51.0% efficiency in contrast to the β variant. Both vaccines showed acceptable protection against α variant and non-Alpha variants, but their effectiveness must be assessed in a greater population. Additional investigation is required to assess the immunogenicity, efficacy, and shelter of these vaccines [17].
7.2 Beta variant and clinical vaccine trials
The vaccine ChAdOx1-nCoV-19 was invented by AstraZeneca followed by the approval from the University of Oxford to check COVID-19 in adults. A South African trial found that the inoculation’s effectiveness against the β-variant was 10.40%, indicating a substandard shield against mild to moderate COVID-19 triggered by β variant. The Ad26.COV2.S vaccine, a nonreplicating human adenovirus type 26 vector, was accepted for checking COVID-19 in persons over teenage years under EUA. A Phase 3 study assessed the usefulness and protection of this vaccine for the preclusion of β-variant in adults aged above 18 years. In animal prototypes, the NVX-CoV2373 vaccine, which contains Matrix-M1 adjuvant, and the full-length of SARS-CoV-2’s spike protein has shown adequate security, robust neutralizing antibodies, and cellular immune reactivity. However, the efficiency of this inoculation in a situation of continuing β variant transmission is immediately assessed.
7.3 Delta variant and clinical vaccine trials
The Delta variant of COVID-19 has become the dominant variant due to its enlarged transmissibility in indoor game locations. Studies show that neutralizing antibody titers decrease after BNT162b2 vaccination against Delta and β variants compared to α variants. However, larger sample sizes are needed for verification. A Phase 3 randomized, placebo-controlled, double-blind therapeutic trial in India evaluated the efficacy of BBV152 vaccination against the Delta variant, achieving a 65.2% success rate [18].
8. Current challenges of combating SARS-CoV-2’s VOCs
The COVID-19 outbreak has been a notable global health emergency, and management has become more difficult as a result of the development and rapid spread of variations of concern (VOCs). VOCs may be more suitable because they are antigenically different from the original SARS-associated viruses that caused the first outbreak of the disease and looked to be able to reinfect humans more successfully. The epidemic, which also caused social and economic problems, caused millions of deaths. There are concerns that the emergence and propagation of novel strains of infections might indicate that our global struggle against the pandemic may need to extend much longer than planned. The next great health disaster to impact society may be COVID-19.
It is noteworthy that COVID-19 immunizations were approved in less than a year, both in human history and in the area of medicine. Numerous obstacles still exist, including the need for storage, transportation, and the universal provision of vaccinations to more than 7 billion people. In other countries, the lack of vaccines and slow supplies make it more difficult to contain the pandemic and may encourage the creation of novel varieties that might lengthen the spread of the disease.
VOCs reduce the analytical techniques’ RT-PCR-based identification sensitivity, which results in false-negative detection. Vaccine hesitancy, an increasing worry, may thwart efforts to combat the virus and boost societal confidence, particularly in underserved communities. Because of their increased virulence and transmission, the recently discovered SARS-CoV-2 VOCs provide new, global approaches to controlling this epidemic. COVID-19 vaccines are manufactured using a variety of machines and stages that target spike protein and receptor-binding characteristics. Efficacy ranges from 65–95%, with RNA vaccines having an efficacy as high as 95%. The aforementioned vaccines require two administrations with a gap of 20–30 days to be effective to provide protection. However, because the virus is constantly changing, recently created vaccinations seem to be ineffective. It is crucial to monitor the emergence of the SARS-associated animal species considering the uncertainty of total eradication. The current vaccination campaign may not provide complete protection to all individuals or subpopulations, leaving certain areas susceptible. The virus may persist due to ongoing risks of infection and the potential for additional dispersion among vulnerable human hosts.
9. Pragmatic future strategies
The widespread distribution of VOCs, which have enhanced transmission and impeded the effectiveness of vaccinations and monoclonal antibodies, has worsened the current SARS-CoV-2 epidemic. Strategies include preserving public separation, proper sanitation, and mask use are essential to lowering morbidity and death. Nonpharmaceutical interventions (
As virus duplication suggests multiple experimental COVID-19 demonstrations, antiviral medication is advised for treating mild to moderate SARS-CoV-2 disease. Antiviral medications such as ivermectin, hydroxychloroquine, nitazoxanide, azithromycin, chloroquine, ritonavir/lopinavir, and remdesivir can prevent viral entry, TMPRSS2, viral membrane fusion, endocytosis, and the RNA-dependent RNA polymerase. Monoclonal antibodies, PAC-MAN (widely known as prophylactic antiviral CRISPR in human cells), and designed recombinant soluble ACE2 are also considered additional therapies for VOCs.
Genomic monitoring/surveillance of SARS-CoV-2 variations is an additional strategy that will be used in the future to predict the pandemic at an early stage and initiate operative strategies to stop the propagation of SARS-CoV-2 variants and prevent the spread of other dangerous viruses. The effectiveness of current vaccinations varies, with some demonstrating diminished efficiency against VOCs. For protection against any virus or strain that belongs to a certain viral group, a universal vaccination is required. However, manufacturing such a vaccination requires new technologies and more investments. Identifying novel SARS-CoV-2 variants is critical for tracking the epidemic and viral progression. Current diagnostic assays identify specific viral genes or protein targets; however, mutations can reduce test sensitivity. Bacillus Calmette-Guerin (BCG) vaccination of children has been demonstrated to reduce COVID-19 cases and mortality rates globally. The BCG vaccine has been proven to enhance the immune system’s ability to combat other bacteria, including tuberculosis.
Since the COVID-19 epidemic is the worst in a century, nations must cooperate to contain it. It is imperative that vaccines are distributed quickly, fairly, and with strong international coordination, all under the direction of the WHO. To avoid human contact and reverse zoonoses, animal immunizations are also required. It is vital to keep track of the progression of the illness and put in place a long-lasting strategy for the global genomic analysis of SARS-CoV-2. Because of the possibility of novel variations originating through interactions between the wild-type and vaccine strains, live attenuated vaccinations should be avoided.
Genomic monitoring is essential for assessing new variations and experimental statistics to calculate potential dangers. International procedures and legal frameworks are required for quick accessibility to viral components. The development of multivalent vaccinations against present and potential variations, the targeting of protein sequences with low mutation risk, and the pursuit of an ideal vaccine that is effective against all variant types, free of cold-chain restrictions, and noninjectable are some prospective possibilities.
10. Conclusions
A significant accomplishment is the development of effective vaccines against SARS-CoV-2 during the 16 months of the COVID-19 pandemic, with 95% effectiveness and 8.090 billion doses distributed across 184 countries. However, the emergence of variants, which is an indication of alarm, poses a serious challenge to tracking the pandemic’s progress. The Omicron variant of SARS-CoV-2, along with five other significant mutations, have made it difficult to eradicate the virus. Recovery from the pandemic will take time because it has already had significant negative effects on the economy and public health. High-throughput technology and innovative vaccines will be required to address these problems, including multivalent vaccinations that provide long-term protection from all variants.
Abbreviations
Angiotensin-converting enzyme 2 | |
Bacillus Calmette-Guerin | |
Double-membrane vesicles | |
Endoplasmic Reticulum | |
Endoplasmic Reticulum-Golgi Intermediate Compartment | |
Emergency Use Authorization | |
Global Initiative on Sharing All Influenza Data | |
Genomic RNA | |
Main Protease Inhibitor | |
Nonpharmaceutical Interventions | |
Non-structural Protein | |
Neglected Tropical Diseases | |
Papain-like Protease | |
Large Polyproteins | |
Receptor Binding Domain | |
Ribonucleic Acid | |
South Africa | |
Sub-genomic RNA | |
Transmembrane Protease, Serine2 | |
United Kingdom | |
United States | |
United States of America | |
Variants of Concern | |
Variants of Interest | |
World Health Organization |
References
- 1.
Pagani I, Ghezzi S, Alberti S, Poli G, Vicenzi E. Origin and evolution of SARS-CoV-2. The European Physical Journal Plus. 2023; 138 :157. DOI: 10.1140/epjp/s13360-023-03719-6 - 2.
Li J, Jia H, Tian M, Wu N, Yang X, Qi J, et al. SARS-CoV-2 and emerging variants: Unmasking structure, function, infection, and immune escape mechanisms. Frontiers in Cellular and Infection Microbiology. 2022; 12 :3-4. DOI: 10.3389/fcimb.2022.869832 - 3.
Tabata K, Prasad V, Paul D, Lee J-Y, Pham M-T, Twu W-I, et al. Convergent use of phosphatidic acid for hepatitis C virus and SARS-CoV-2 replication organelle formation. Nature Communications. 2021; 12 :7276. DOI: 10.1038/s41467-021-27511-1 - 4.
Zhang H, Zhang H. Entry, egress and vertical transmission of SARS-CoV-2. Journal of Molecular Cell Biology. 2021; 13 :168-174. DOI: 10.1093/jmcb/mjab013 - 5.
Tegally H, Wilkinson E, Giovanetti M, Iranzadeh A, Fonseca V, Giandhari J, et al. Detection of a SARS-CoV-2 variant of concern in South Africa. Nature. 2021; 592 :438-443. DOI: 10.1038/s41586-021-03402-9 - 6.
Cascella M, Rajnik M, Aleem A, Dulebohn SC, Di Napoli R. Features, Evaluation, and Treatment of Coronavirus (COVID-19). 2023 Aug 18. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2023 Jan–. PMID: 32150360 - 7.
Scovino AM, Dahab EC, Vieira GF, Freire-de-Lima L, Freire-de-Lima CG, Morrot A. SARS-CoV-2’s variants of concern: A brief characterization. Frontiers in Immunology. 2022; 13 :6-7. DOI: 10.3389/fimmu.2022.834098 - 8.
Jeong GU, Yoon GY, Moon HW, Lee W, Hwang I, Kim H, et al. Comparison of plaque size, thermal stability, and replication rate among SARS-CoV-2 variants of concern. Viruses. 2021; 14 :55. DOI: 10.3390/v14010055 - 9.
Raja RK, Nguyen-Tri P, Balasubramani G, Alagarsamy A, Hazir S, Ladhari S, et al. SARS-CoV-2 and its new variants: A comprehensive review on nanotechnological application insights into potential approaches. Applied Nanoscience. 2023; 13 :65-93. DOI: 10.1007/s13204-021-01900-w - 10.
Luban J, Sattler RA, Mühlberger E, Graci JD, Cao L, Weetall M, et al. The DHODH inhibitor PTC299 arrests SARS-CoV-2 replication and suppresses induction of inflammatory cytokines. Virus Research. 2021; 292 :198246. DOI: 10.1016/j.virusres.2020.198246 - 11.
Corti D, Purcell LA, Snell G, Veesler D. Tackling COVID-19 with neutralizing monoclonal antibodies. Cell. 2021; 184 :3086-3108. DOI: 10.1016/j.cell.2021.05.005 - 12.
Şimşek Yavuz S, Komşuoğlu Çelikyurt İ. An update of anti-viral treatment of COVID-19. Turk. Journal of Medical Sciences. 2021; 51 :3372-3390. DOI: 10.3906/sag-2106-250 - 13.
Caly L, Druce JD, Catton MG, Jans DA, Wagstaff KM. The FDA-approved drug ivermectin inhibits the replication of SARS-CoV-2 in vitro. Antiviral Research. 2020; 178 :104787. DOI: 10.1016/j.antiviral.2020.104787 - 14.
Alavi Darazam I, Shokouhi S, Pourhoseingholi MA, Naghibi Irvani SS, Mokhtari M, Shabani M, et al. Role of interferon therapy in severe COVID-19: The COVIFERON randomized controlled trial. Scientific Reports. 2021; 11 :8059. DOI: 10.1038/s41598-021-86859-y - 15.
London School of Hygiene & Tropical Medicine. COVID-19 Vaccine Tracker. https://Vac-LshtmShinyappsIo/Ncov_vaccine_landscape/ - 16.
Ling Y, Zhong J, Luo J. Safety and effectiveness of SARS-CoV-2 vaccines: A systematic review and meta-analysis. Journal of Medical Virology. 2021; 93 :6486-6495. DOI: 10.1002/jmv.27203 - 17.
Zhang J, Zeng H, Gu J, Li H, Zheng L, Zou Q. Progress and prospects on vaccine development against SARS-CoV-2. Vaccines (Basel). 2020; 8 :153. DOI: 10.3390/vaccines8020153 - 18.
Backer V, Sjöbring U, Sonne J, Weiss A, Hostrup M, Johansen HK, et al. A randomized, double-blind, placebo-controlled phase 1 trial of inhaled and intranasal niclosamide: A broad spectrum antiviral candidate for treatment of COVID-19. The Lancet Regional Health - Europe. 2021; 4 :100084. DOI: 10.1016/j.lanepe.2021.100084