Open Access is an initiative that aims to make scientific research freely available to all. To date our community has made over 100 million downloads. It’s based on principles of collaboration, unobstructed discovery, and, most importantly, scientific progression. As PhD students, we found it difficult to access the research we needed, so we decided to create a new Open Access publisher that levels the playing field for scientists across the world. How? By making research easy to access, and puts the academic needs of the researchers before the business interests of publishers.
We are a community of more than 103,000 authors and editors from 3,291 institutions spanning 160 countries, including Nobel Prize winners and some of the world’s most-cited researchers. Publishing on IntechOpen allows authors to earn citations and find new collaborators, meaning more people see your work not only from your own field of study, but from other related fields too.
In recent decades, hepatocellular carcinoma (HCC) has appeared as main indication (40–60%) of liver transplantation (LT) — one of the most effective treatments for the disease. Inclusion criteria play a pivot role in order to improve the survival outcomes, as well as to minimize the recurrent rate after LT. Indications for LT in HCC, previously based on static staging (principally tumor burden), turned to a more active process with supplementary tumor biology in response to local-regional treatment. This enables patients beyond the widely-accepted Milan criteria (MC) to access LT without discouraging outcomes. Though considered too strict, MC remains the cornerstone of inclusion criteria, while many others which increasing extend beyond Milan have been applied. The LT inclusion criteria for HCC vary according to each institution, region, and country (whether it performs deceased-donor LT or living donor LT) and adapted over time. These criteria in fact were the truly predictive models for the risk of recurrent, and therefore the survival outcome post-LT. This chapter focuses on recent inclusion criteria and liver allocation policy for LT in HCC throughout the world.
General Surgery Department, Hue Central Hospital, Hue City, Vietnam
*Address all correspondence to: hoangducnammd@gmail.com
1. Introduction
Hepatocellular carcinoma (HCC) is the sixth most frequent new tumor (>800,000 new cases annually worldwide), with a constantly poor long-term survival, resulting in atop 900,000 yearly deaths (the fourth most common cause of cancer-related mortality) [1]. In adults, HCC is the most frequent primary liver cancer [2]. A total of 70–90% of cases arise on a setting of chronic liver disease (mostly viral hepatitis and alcoholic liver disease) [3, 4]. The majority of HCC patients do not fit curative resection or LT when diagnosis [3].
Historically, HCC was associated with poor overall anticipation. LT was first recognized a prospective cure for the disease since the first case was performed in an adult HCC patient [5]. Thomas Starzl (USA, 1967) and Sir Roy Calne (Cambridge, England, 1968) were successful pioneers in human orthotopic liver transplantation (OLT) [6]. Early outcomes of LT in HCC were poor with high early HCC recurrence suggested that the recipients had advanced disease [4]. However, with the awareness that patients with smaller HCC nodules profit better from LT, particular criteria were proposed to help decision-making [7]. Mazzaferro et al. had milestone report that LT for HCC with certain limited criteria resulted in significant improval of recurrence-free and overall survival at 4 years, evidently specify the vitalness of patient selection [8].
The apparent attraction of LT against other modalities in HCC treatment is the ability to exclude the cancer and the primitive liver cirrhosis at the same time, thus reducing the risk of HCC recurrent on the remnant liver [5]. There is constantly considerable discrepancy worldwide between LT patients demand and liver graft supply. This inquire a reasonable selection of potential candidates in order to identify the suitable HCC patients anticipated to gain the superior benefit from the procedure while not disadvantaging non-cancer patients in the same waiting list for LT. HCC patients are aimed to achieve a long-term LT results equivalent to those transplanted for other etiology (e.g., liver cirrhosis, acute liver failure..). That is, conforming to the primary principle of transplant utility, LT should be limited in patients with expected 5-year survival over 70% and recurring <10–15% [9].
Allocation rules and priorities, as well as special treatment strategies in the waiting list, have, accordingly, been established and are still being refined to warrant fairness between patients listed for HCC and non-HCC causes [9].
The staging systems of HCC are clinically useful for management orientation; the decision-making should be individualized based on patient factors, tumor burden, pathological, hepatic function, etiology of liver disease, and biological tumor criteria [10]. There are also interactions between patient-tumor factors and treatment efficacy. No staging system is applicable to every HCC patient. Furthermore, most of the existed criteria composed of preoperative imaging studies for evaluation the tumor burden without the critical results from pathological analysis of explanted livers. Therefore, there was always disproportionate evaluation of the Milan criteria pre- and post-operatively [10].
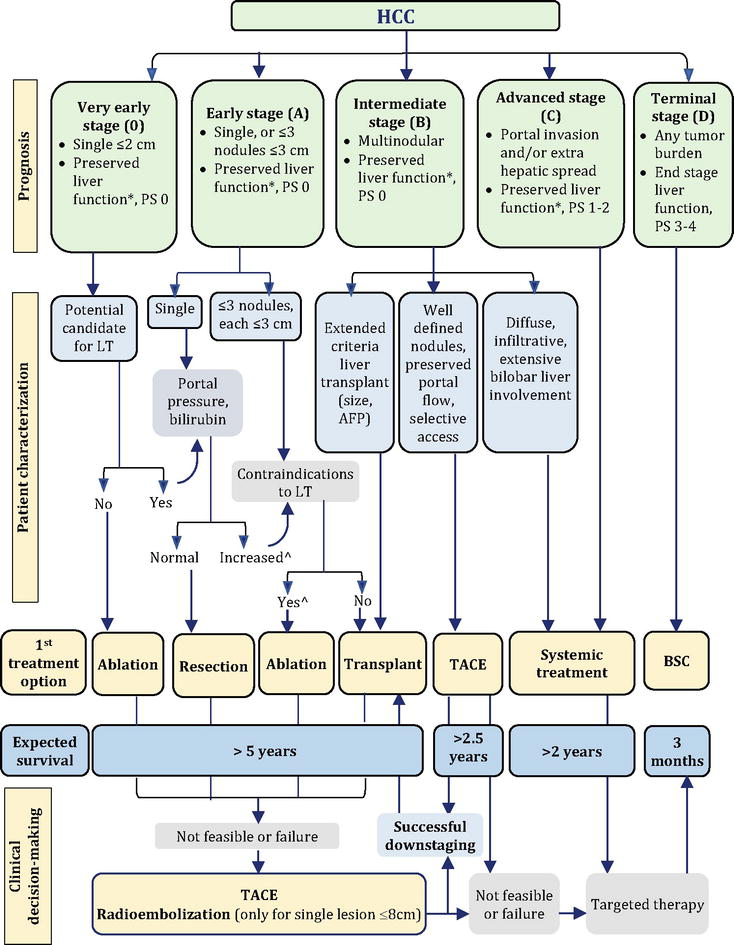
At 2010 AHPBA (American Hepato-Pancreato-Biliary Association) HCC consensus conference, there existed 18 HCC staging or scoring systems in use worldwide [11]. Modified TNM classification of UNOS (United Network for Organ Sharing) (Table 1) together with BCLC (Barcelona Clinic Liver Cancer) (Figure 1) were among the most practical and universally used staging systems for HCC.
T1
1 nodule <1.9 cm
T2
1 nodule 2.0–5.0 cm; 2 or 3 nodules, all <3.0 cm
T3
1 nodule >5.0 cm; 2 or 3 nodules, at least one >3.0 cm
T4a
4 or more nodules, any size
T4b
T2,T3 or T4a plus gross intrahepatic portal or hepatic vein involvement as indicated by CT, MRI or ultrasound
N1
Regional (porta hepatis) nodes, involved
M1
Metastatic disease, including extrahepatic portal or hepatic vein involvement
Stage I
T1
Stage II
T2
Stage III
T3
Stage IVA1
T4a
Stage IVA2
T4b
Stage IVB
Any N1, any M1
Table 1.
UNOS modified TNM staging classification for HCC [12].
T3 lesions that meet UCSF criteria (single lesion ≤6.5 cm or 2–3 lesions none >3 cm with a total tumor diameter of ≤8 cm) were classified as T3A. The other patients with T3 HCC exceeding these criteria were classified as T3B.
Figure 1.
Modified BCLC staging and treatment strategy in 2022 [13]. * except for those with tumor burden acceptable for transplant. ^ resection may be considered for single peripheral HCC with adequate remnant liver volume AFP, alpha-fetoprotein; ALBI, albumin-bilirubin; BSC, best supportive care; ECOG-PS, eastern cooperative oncology group-performance status; LT, liver transplantation; MELD, model of end-stage liver disease; TACE, transarterial chemoembolization.
The TNM classification, though widely chosen for cancer staging, has inferior capability in anticipating long-term survival for HCC [14]. However, despite these facts, TNM is still a referred utility for pathological reports of explant liver. Limitations of this system are based on imaging and not actual histological findings, and imaging can underestimate tumor burden in stage II patients by 27 to 33%. Moreover, the severity of cirrhosis, critical for prognosis, is not part of TNM, and this system does not reflect survival after LT [15].
The superiority of BCLC staging system is its integration of liver function (Child-Pugh score), tumor characteristics (the number and size of nodules, vascular invasion, and extrahepatic spread), and performance status (Figure 1). It is the only system that recommends the best available management for each stage.
3. Liver graft allocation policies, prioritization on the waiting list
With obvious chronic organ shortage worldwide and in the setting of death-donation liver transplant (DDLT), allocation policies have frequently refined during the last decades in order to diminish waiting-list mortality while assuring of best survival for HCC patients after LT.
3.1 Model of end-stage liver disease (MELD) score
The MELD score, an objective measure incorporating three quantitative values (serum creatinine, international normalized ratio [INR], and serum bilirubin), has proven to be a strong predictor of short-term mortality (3-month) in cirrhotic patients, including LT candidates [5]. It is then used to prioritize patients for DDLT; however, it underestimates the mortality risk in HCC patients because their biologic MELD was usually low. Accordingly, patients with HCC within Milan criteria (MC: single lesion ≤5 cm or up to 3 lesions ≤3 cm) were provided with additional MELD exception points starting in 2002 to balance their risk of tumor progression while awaiting LT compared to the 3-month liver-related mortality risk of non-HCC patients [16]. In 2002, the MELD score was proposed as the core system for organ allocation and implemented in the US first, then in most Western countries [5].
HCC patients are generally prioritized on the wait list for DDLT aiming to preclude tumor-advancement exceeding acceptable inclusion criteria, which sequentially leads to dropout from the wait list and deceased from cancer. In the US, despite the UNOS allocation system assigned some priority to HCC patients, dropout rates from tumor advancement were up to 25% at 1 year and 43% in 2 years’ wait time by 2001 [15].
In 2005, HCC patients within MC in the US irrespective of their biologic MELD score are listed with a score of 22 (Table 2). This resulted in a six-fold increase in LT for HCC and raising the concern non-HCC patients on the waiting list could be disbenefit by the allocation [17]. Ensuing data indicated extra-MELD points often over-emphasizing the risk of tumor advancement and consequent fatality. Therefore, this MELD priority program has since been revised occasionally (Table 2) [16].
Year
MELD Exception Points
2002
29 for T2 lesions
24 for T1 lesions
2003
24 for T2 lesions
20 for T1 lesions
2004
24 for T2 lesions
No exception points for T1 lesions
2005
22 for T2 lesions
No exception points for T1 lesions
2015
Natural MELD score at time of listing for T2 lesions
28, after 6 months
Maximum of 34 MELD exception points
Proposed changes
Requirement for locoregional therapy in patients with 2–3 cm HCC prior to applying for MELD exception points
Allowing exception points for select patients with T3 HCC who are downstaged to T2
The “cap and delay” policy revision (2015) required a six-month interval before LT based on their assigned HCC-exception score to earn a MELD of 28 (Table 2). By extending the wait time, poor biologic tumors will be identified and vain LT may be preceded [18]. In the US in the 2 years just before and just after the policy change, HCC candidates had a 37% lower risk of wait-list death/dropout prepolicy and a comparable risk of death/drop-out postpolicy, establishing fairness between HCC and non-HCC candidates in wait list [19].
3.2 Organ procurement and transplantation network (OPTN)/united network for organ sharing (UNOS)
The traditional MELD score was not generated to anticipate the mortality risk in HCC patients with cirrhosis. Furthermore, some regions in the US, the wait time for OLT can be up to 24 months. Therefore, a supplemental system for prioritization was developed by the OPTN/UNOS that would provide these patients access to an allograft before their HCC advances beyond MC (Table 3). Notably, in 2016, the OPTN adopted a downstaging protocol for patients with HCC tumor burden beyond MC.
Selection for automatic exception score:
AFP < 1000 ng/mL. If AFP ≥1000 ng/mL, it must fall below and remain <500 ng/mL after treatment.
AND
Patients within Milan criteria: 1–2 tumors between 1 and 3 cm, or 1 tumor between 2 and 5 cm.
OR
Downstaged to Milan criteria by liver-directed therapy from initial downstaging criteria: one tumor between 5 and 8 cm, 2–3 none greater than 5 cm and sum <8 cm, 4–5 lesions all less than 3 cm and sum <8 cm.
Awarded MELD exception score:
MMaT-3. After six-month wait, patients are awarded a fixed score of three points lower than median MELD at transplantation (MMaT-3) for patients transplanted within the area of distribution where the candidate is listed (distribution is a concentric circle model as of February 4, 2020.) MMaT is recalculated every 6 months based on data of the 1 year before.
Appeal to National Liver Review Board:
Pathway for patients outside of above criteria or who may require a higher priority score. Center must provide adequate medical justification for prioritization over other waiting candidates.
4. Current inclusion criteria for primary LT in HCC patients
The term liver transplant discussed here refers to primary LT. The LT inclusion criteria vary according to each institution, region, and country (whether it performs deceased-donor LT or Living Donor LT), and it may eventually change. These criteria in fact were the truly predictive models for the risk of recurrent, and therefore the survival outcome. They may comprise simply the radiologic factors, in combination with serologic factors, or recruiting pathological factors, responses to locoregional treatments.
4.1 Preliminary and Milan criteria
Initiative outcomes of OLT for HCC were dismal [21]. Early series of Thomas Starzl in the US and Roy Calne, Rudolf Pichlmayr, and Henri Bismuth in Europe encountered many HCC patients, including children; the longest survival was only 16 months and few survived more than 1 year [22]. Until the 1990s, poor outcomes in terms of overall recurrent rate (40% in 2 years with 81% mortality) and universal tumor recurrence of HCC brought the transplant community to abandon the procedure for primary liver tumors. HCC was proclaimed a relative contraindication to LT by the US Department of Health and Human Services in 1989 [20, 22].
Bismuth et al. were the first to recognize the efficacy and safety of LT in early-stage HCC. They determined definitive Paul-Brousse Hospital Criteria “less than two tumor nodules and a maximum tumor diameter < 3 cm” had lower recurrence after LT when compared to liver resection (Table 4) [42].
11 variables including liver related and non-related factors
86.3% at 5Y: (highest score)
—
Table 4.
Criteria based on deceased-donor liver transplantation [2, 23].
Number of patients.
Survival of patients who met the criteria (compared with patients who did not meet the criteria).
Not clearly indicated DDLT or LDLT (mixed data).
Detailed criteria for AFP, RETREAT, and MORAL (USA) scores are summarized in Table 5.
Survival and Recurrent Rate of the patients beyond Milan criteria but within vs. beyond Up to Seven criteria, each.
Comparable to patients with tumors within MC.
Training set (Italy): HCV 56.9%, HBV 21.1%; validation set (China): HCV 2.6%, HBV 96.2%.
All criteria require no macrovascular invasion.
HBV, HCV: hepatitis B, C virus; RFS, recurrence-free survival; RR, recurrence rate; VI, vascular invasion; TTV: Total Tumor Volume; TTD: Total Tumor Diameter; RETREAT, Risk Estimation of Tumor Recurrence After Transplant; mVI, microvascular invasion; NLR, neutrophil-to-lymphocyte ratio; LiTES-HCC, Liver Transplant Expected Survival-HCC. nY, n-years.
Point
AFP model
Total score > 2: 50.6% of 5-year recurrence rate
Tumor diameter:
≤3 cm
0
3–6 cm
1
>6 cm
4
Number of tumors:
1–3
0
≥4
2
AFP (ng/mL):
≤ 100
0
100–1000
2
>1000
3
RETREAT
Score 5 or more: 75.2% of 5-year recurrence rate
AFP at LT (ng/mL):
0–20
0
21–99
1
100–999
2
≥1000
3
Microvascular invasion
Present
2
Largest diameter + No. of viable tumors on explant
≤ 1 cm
0
1.1–4.9 cm
1
5–9.9 cm
2
≥10 cm
3
MORAL (USA)
Pre-MORAL: Score > 10: 17.9% of 1-year RFS
Preoperative NLR, ≥5
6
Maximum AFP, >200 ng/mL
4
Largest tumor size, >3 cm
3
Post-MORAL (pathology): Score > 10:
22.1% of 5-year RFS:
Grade 4 tumors, present
6
Vascular invasion, present
2
Largest size, >3 cm
3
Tumor number, >3
2
Table 5.
Specific criteria of AFP, RETREAT, and MORAL (USA) models [23].
RETREAT, Risk Estimation of Tumor Recurrence After Transplant; LT, liver transplantation; NLR, neutrophil-to-lymphocyte ratio; RFS, recurrence-free survival.
In 1996, Mazzaferro et al. published a benchmark study found that limited LT selection criteria (single tumor ≤ 5 cm or up to three tumors, each ≤ 3 cm, without macrovascular invasion or extrahepatic spread) led to similar outcomes when compared with non-HCC patients [8]. These Milan criteria (MC) were used by the United Network for Organ Sharing (UNOS) since 2002 to arrange the listing priority of HCC patients [21]. Consequently, MC has been included in the BCLC pretransplant staging, the American Association for the Study of Liver Diseases (AASLD), and the European Association for the Study of the Liver-European Organization for Research and Treatment of Cancer (EASL-EORTC) practice guidelines [43].
With extensive organ shortage worldwide, it is universally agreed to constrain LT to HCC cases within MC, particularly in the scene of DDLT. Although MC significantly contributed to LT clinical practice at first with prognostic potency and helped revival this demanding procedure; they are restricted, precluding certain candidates who can gain from LT [23]. In addition, these criteria are based only on the preoperative radiological aspect and lack of related factors that can impact HCC recurrence, especially tumor biology.
4.2 UCSF criteria
About 25% of recipients were eventually found exceeding the Milan criteria on the explant histology post-LT, regardless their 5-year survival was above 50% [43]. This led to initial expansion of the LT criteria for HCC with the University of California San Francisco (UCSF) criteria, which was less strictive (Table 4). With this modest extension of selection, the favorable improvement in survival of HCC with LT was still maintained.
4.3 Other extended criteria
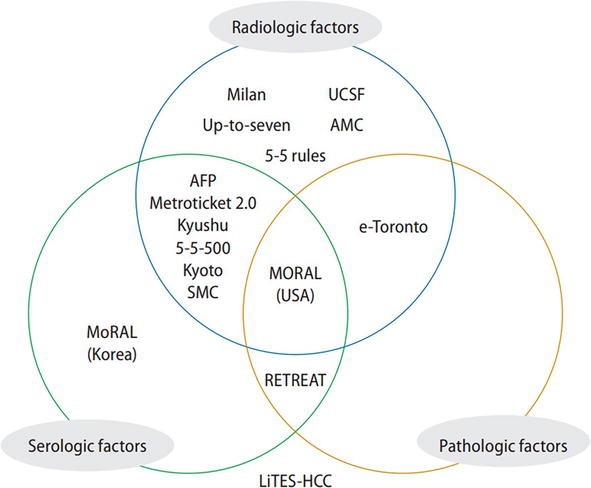
Promising results of OLT relying on MC have encouraged inclusion more HCC candidates on the wait list. Extending the selection criteria might show excellent outcomes [9]. There have been more and more incorporated factors composing various inclusion criteria (Figure 2). However, MC remains the landmark for LTindications in HCC candidates and the basis for comparison with other proposed criteria [44].
Figure 2.
Major prediction models based on recruited factors (reproduced with permission from [23]). AMC, Asan medical Center; SMC, Samsung medical Center; RETREAT, risk estimation of tumor recurrence after transplant; LiTES-HCC, liver transplant expected survival-hepatocellular carcinoma.
Theoretically, at least three different schemes may be scheduled for the extension of the HCC criteria transplantation with deceased-donor grafts in Milan-out HCC patients, living donor LT for patients beyond MC, and successful downstaging to MC before LT in patients primarily Milan out [43]. Furthermore, practicing on expanded criteria emphasizes two crucial points that have to be defined a priori [22]:
What should be considered as an acceptable posttransplant outcome in HCC?
How much the extension of criteria disadvantages other non-HCC candidates?
4.3.1 Composite models combining tumor burden and biomarkers
AFP and descarboxy-prothrombin (DCP) were found to be relevant to the risk of recurrence at various cutoff values and independent from tumor burden (Table 6) [35]. In particular, pre-LT AFP and DCP levels, which reflect tumor differentiation as well as macro- and microvascular invasion [35], can be considered as a representative marker of cancer aggressiveness. Finally, increasing of AFP while on the waiting list negatively impacted outcome [33, 60].
“French AFP model” or AFP score (Table 4): Based on above ground, a first composite model combining AFP values and tumor features at listing, followed by a quarterly reassessment during pre-LT follow-up was designed and prospectively validated in France [35]. This model was proved more accurate than MC to predict recurrence in patients meeting or not Milan criteria. This score has been validated in Italy [61], Spain [62], and Latin America [63]. The model was adopted by the French Organization for Organ Sharing (Agence de la Biomédecine) in 2013 as the official tool to select HCC patients, lead to a major change in LT indications policy there.
Metroticket 2.0 (2018) (Table 4): In general, the “metro-ticket paradigm” best demonstrates the present occasion; the further stretch we cover away from the standard criteria, the higher the price we will have to pay in terms of greater recurrence [40].
A-P Level (Hokkaido Group, Japan, 2007) [10] and A-P 200 criteria (Pusan National University Yangsan Hospital, South Korea, 2016) [53]. Within MC, patients exceeding the A-P 200 criteria had significantly worse 3-year disease-free survival (DFS) compared to the ones within the A-P 200 criteria (56% vs. 90.7%, P = .012). Patients exceeding Milan criteria, those within the A-P 200 criteria had a significantly higher 3-year DFS compared to the one exceeding the A-P 200 criteria (88.2% vs. 24.3%, P = .003). This A-P 200 criteria was also externally validated from another major LT center (Yonsei University College of Medicine, Korea) and observed similar results [53].
Survival of patients who met the criteria (compared with those who did not meet the criteria).
Survival of the patients beyond MC but within MoRAL score ≤ 314.8.
All criteria require neither extrahepatic metastasis nor macrovascular invasion.
NANB: non-A non-B hepatitis; PIVKA-II, prothrombin induced by vitamin K absence-II;
nY: n-years. MC-in: within MC; MC-out: exceeding of MC. SFSG: Small-for-Size Graft.
4.3.2 Tumor histology
The groups of Padova [64] and Toronto [65] found that in T3-HCC without poorly differentiated cancer on tumor biopsy before LT, and 5-year DFS rates >70% could be achieved. This again emphasizes the crucial importance of tumor biology in evaluation of the recurrent risk. The main drawback of this factor is the risk of tumor seeding along the needle tract and by sample effect (not properly manifest the precise tumor pathology) [66].
4.3.3 18 FDG pet CT
Certain retrospective studies from Germany and Korea have persistently shown that tumors with high FDG uptake have a significantly higher risk of recurrence compared to HCC with no or lower uptake because high SUV is significantly associated with poor differentiation and microvascular invasion (Table 4) [67]. In a recent Korean study, the combination of the positive FDG-PET study and AFP level > 200 ng/mL could better predict tumor recurrence after LDLT than MC. Moreover, LT in low SUV and low AFP pre-LT values was related with 80% 5-year survival rates, regardless of MC or tumor burden [56].
UCSF criteria combined with the FDG-PET condition can anticipate tumor recurrence after LDLT (tumor recurrence is earlier in cases with positive FDG-PET results) (a retrospective study in 2016 in Taiwan) [68].
This indicates that tumor biology might predict the recurrence risk better than tumor staging [9]. Impressively, 18 FDG PET-CT before LT can reveal undiagnosed extrahepatic metastases or additional intrahepatic tumors, enabling restaging of HCC in 10% of candidates [69].
4.3.4 Other recent prognostic variables and scores
Diverse parameters recently have been found valuable or validated as prognostic indicators or liberated risk factors for HCC recurrence after LT:
GRWR (graft-to-recipient body weight ratio) (Table 6)
Preoperative CRP (C-reactive protein): CRP >1 mg/dL was a separate risk factor for HCC recurrence with a 5-y recurrence rate of 27.4 vs. 16.4% (Meischl et al. 2019) [70].
ALBI grade: It was measured employing pre-transplant serum albumin and bilirubin. Post-LT HCC recurrence rates were 10.5, 15.9, and 68.2% in ALBI grades 1, 2, and 3, correspondingly. Together with AFP and CRP, ALBI grades 1 or 2 were determined as an isolated predictor of RFS. ALBI grade 3 proved to be the strongest indicator of microvascular invasion (Kornberg et al. 2019) [71].
The Hazard Associated with Liver Transplantation for Hepatocellular Carcinoma (HALTHCC) model determined as: (2.31*lin(AFP)) + (1.33*tumor burden score) + (0.25*MELD-Na) − (5.57*Asia). This score predicted overall survival, recurrence rate, and vascular invasion, poorly differentiated components on explant pathology (Firl et al., 2019) [72].
LDLT has been applied extensively in Asia as aforementioned, and many major centers soon recognized the crucial roles of AFP and PIVKA-II as the main recurrent predictors of HCC post-LT. Tumor burden had also been significantly expanded (Table 6).
5. Management in the waiting list: Downstaging or bridging therapy
Organ shortage is one of the main drawbacks of OLT. With biologic MELD score generally low, HCC candidates for LT are often struggled with prolonged wait times for DDLT. This may result in tumor growth exceeding the MC while in the wait list.
Median wait time of a HCC candidate ranges from 3 to 15 months [9]. Subsequently, whereas drop-out rate from LT wait list is around 15–30% due to HCC advancement, downstaging, and bridging management should be provided in patients with an estimating wait time for LT over 6 months [73]. That is, once they are registered for LT, and wait time of longer than 6 months is anticipated, locoregional therapies (LRT) for HCC will be carried out in order to satisfy certain criteria for OLT (downstaging strategy) or to assure the remnant tumors still stay within MC (bridging therapy) [2, 17].
LT after successful downstaging should aim to gain a 5-year survival equivalent to that of HCC recipients undergone LT without necessity of downstaging [44].
Bridging therapy approaches should be determined by pluridisciplinary board meetings, transarterial chemoembolization (TACE) was the most common modality. Approximately 25% of LT applicants are suitable to bridging management (probable curing), such as thermoablation or liver resection. Emergent approaches for instance radioembolization (TARE), stereotactic external beam radiotherapy (SBRT), and still tyrosinekinase inhibitors (sorafenib, levantinib…) were less recommended. Tiny central tumors in compensated liver cirrhosis were more suitable to treat with RFA, whereas larger tumors but sustained liver function are treated with TACE/TARE. In decompensated liver cirrhosis and larger tumor size, external radiotherapy may be recommended without increasing the risk of furthermore decline of liver function [74].
Results of bridging management, evaluated with tumor size and AFP levels, should be carefully and routinely rechecked until LT. Tumor advancement [75] and AFP rising [60] during bridging therapies anticipate recurrence post-LT. Patients advancing beyond LT criteria should be resigned from the wait list. Conversely, candidates initially out of inclusion criteria can be effectively down-staged and, thereafter, registered for LT [76]. Downstaging within Milan (T2) criteria is achievable in 40% of those cases. The risk of HCC recurrence after a downstaging procedure is about 15% but still consistent with admissible 5-year survival rates roughly 70% [9].
To standardize downstaging criteria in the USA, UNOS/OPTN adopted the UNOS/Region 5 down-staging protocol (UNOS-DS; Table 7) in 2017, candidates who successfully downstaged to within MC qualified to obtain automatic MELD exception after the mandatory six-month waiting period [77].
Registered Criteria:
HCC out of Milan criteria but fulfilled one of the following:
Single lesion 5.1–8 cm
2–3 lesions each ≤5 cm with total tumor diameter ≤ 8 cm
4–5 lesions each ≤3 cm with total tumor diameter ≤ 8 cm
Without vascular invasion or extrahepatic spread on cross-sectional imaging
criteria for successful downstaging:
Residual tumor burden fulfilled Milan criteria (1 lesion ≤5 cm, 2–3 lesions ≤3 cm):
Only effective tumor(s) are counted; tumor size estimations should not comprise necrotic regions after treatment.
If more than one area of remnant tumor enhancement, then the size of the entire lesion should be calculated toward the overall tumor burden
Criteria for downstaging failure and dropout of wait list:
Advancement of tumor(s) exceeding registration/qualification criteria for downstaging (described above)
Tumor macroscopic vascular invasion on cross-sectional imaging
Lymph node or extrahepatic metastasis
Tumor progress in the type of infiltration
In UNOS present principle, once AFP ≥ 1000 ng/mL, LT is not attempted until this marker drops below 500 ng/mL after LRT
Schedule of LT in regard to downstaging:
Minimal monitoring interval is supposed to be at least 3 months of tumor steadiness from accomplished downstaging to LT.
In UNOS present principle, candidates must reside inner of Milan criteria for 6 months after accomplished downstaging to receive MELD exception points.
The inclusion criteria, aim, and protocols of downstaging still differ between centers; however, the general and initial aim is fulfilled Milan criteria (MC-IN) [78]. The European Association for the Study of the Liver (EASL) proposes LT only for MC-IN candidates after downstaging. The UCSF group introduced their downstaging protocol and defined the “success of downstaging” criteria, allowing more candidates to profit from LRT before LT (Table 8) [23]. Recent AASLD guidelines recommended that candidates beyond MC (T3) can be registered for LT after effective downstaging into MC [81]. Recent prospective studies and essential updates of HCC-downstaging before LT were summarized in the Tables 9 and 10.
Single lesion: >5 cm and ≤ 8 cm; 2–3 lesions: at least one lesion >3 cm and ≤ 5 cm, total diameter ≤ 8 cm; 4–5 lesions: each ≤3 cm, total diameter ≤ 8 cm
DDLT: within UNOS criteria T2 LDLT: within UCSF criteria
LRT corresponded with better OS (HR 0.84 [0.73–0.96]) and HCC-specific survival (HR 0.76 [0.59–0.98]) post-LT. RFA was highly effective for OS and HCC-specific survival after LT.
In regard to number of pretreatments, recurrent rate was considerably greater in the ≥5 pretreatments group than the 0 group. Nevertheless, those fulfilled Kyoto criteria. no considerable differences in recurrent rates between groups.
407 HCC recipients with AFP > 1000 ng/mL at LT wait list
5-y OS: AFP >1000 at LT; 48.8%, AFP to 101–499; 67.0%, AFP to <100; 88.4% 5-y HCC recurrent probability: AFP >1000; 35.0%, AFP to 101–499; 13.3%, AFP to <100; 7.2% In multivariate analysis, AFP decrease to 101–499 was related with a > 2-fold decrease in posttransplant mortality (P = .01) and a nearly 3-fold decrease in HCC recurrence (P = .02) [91]
UNOS database of 3819 HCC LT; constantly fulfilled Milan (n = 3276), UNOS-DS (n = 422), and AC-DS (n = 121)
On explant, vascular invasion presented in 23.7% of AC-DS versus 16.9% of UNOS-DS and 14.4% of Milan (P = .002). Within DS groups, risk of post-LT death was higher in SWR or MWR and with AFP >100 ng/mL at LT. The 3-y HCC recurrence probability was 6.9% for Milan, 12.8% for UNOS-DS, and 16.7% for AC-DS (P < .001). In DS groups, AFP >100 was the only separate predictor of HCC recurrence. [92]
HCC burden measured at three points on the initial wait list (I), maximum (M) total tumor diameter, and last (L) exception petition. Classification: (A) < Milan (B) Milan (C) > Milan to UCSF (D) > UCSF. 1233 (7%) had any post-LT rHCC. rHCC rates were higher in RH-IML group CCC (15%) and DDD (18%). Low recurrence rates: M and L tumor burden did not exceed Milan (class A or B), effective downstaging when L was A(<Milan), and M tumor burden did not exceed I
4109 patients for validation between 2015 and 2017
compared to patients without cPR, cPR patients were younger; had lower MELD scores, AFP levels, and NLR; were more probable having tumors within MC and fewer LRT treatments; and had significantly lower 1-, 3-, and 5-y incidence of post-LT recurrence (1.3, 3.5, and 5.2% vs. 6.2, 13.5, and 16.4%; P < .001) and higher general survival (92, 84, and 75 vs. 90, 78, and 68%; P < .001). Multivariable predictors of cPR included age, sex, liver disease diagnosis, MELD, AFP, NLR, radiographic Milan status, and number of LRT treatments.
Table 10.
Essential updates of downstaging HCC before liver transplantation [70].
Abbreviations: AC-DS, all-comers downstaging; SWR: short wait regions; MWR: mild wait regions; cPR, complete pathological response; HR, hazard ratio; Kyoto criteria, tumor number ≤ 10, maximal diameter of each tumor ≤5 cm, and DCP levels of ≤400 mAU/mL; OS, overall survival; rHCC, recurrent HCC; UCSF criteria, 1 tumor >5 cm and up to 6.5 cm or 3 tumors each up to 4.5 cm; UNOS-DS, (one lesion >5 cm and ≤ 8 cm; 2–3 lesions each ≤5 cm; or 4–5 lesions each ≤3 cm with total tumor diameter ≤ 8 cm) downstaging [70].
Due to important shortage of donated organs, with additional challenge of equal allocation of available organs among cancer vs. non-cancer recipients, certain surgical strategies have been established. All these approaches contribute the so-called “marginal graft” (also specified as “extended criteria livers”). Marginal grafts explication incorporates: (i) Living donor right lobe graft, cadaveric liver division (split the whole liver from cadaveric donors to two recipients of different size), (ii) serious hepato-steatosis (i.e., macrovesicular >60%), and (iii) organs harvested from heartbeat brain death (DBD donors) and even from non-heartbeat (circulation-death - DCD donors) [6].
LDLT has flourished in eastern countries (especially Japan, South Korea, Taiwan..) due to significant cadaveric organ shortage. Though DDLT has recently accounted above 90% of LT in the Western world, LDLT is predominant in many Asian centers [5]. LDLT has also been utilized in Western countries (with well-established programs for DBD or DCD programs), because of persistent organ shortage, prolong wait times related with wait-list mortality, disqualified because of health problems, or tumor advancement exceeding eligible criteria [44].
Concern still remains whether LDLT for HCC attains equivalent outcomes with DDLT, especially in MC-out candidates. Also, tumor recurrent rate has been reported higher in LDLT than DDLT [95]. However, at least two systematic reviews [96, 97] found no evidence to demonstrate this trend. Theoretically, several hypotheses were made on greater recurrent rates in LDLT: (1) Because of relative brief wait time for LDLT candidates, advancement of aggressive HCC biology could be neglected; while they might fall out from the wait list in DDLT setting and could not access to LT. This is the renown “fast-track effect.” (2) Growth factors and cytokines produced during speedy regeneration of the partial grafts might contribute to tumor advancement and recurrence. Nevertheless, there is lack of prospective study on this issue previously [98].
LDLT is more favorable than DDLT in reduced wait time, superior quality graft with better liver function, reduced ischemic time, and pretransplant treatment optimization for HCC that might contribute to enhanced survival of recipients with LDLT [98]. In the setting of LDLT, organs are donated as private gifts and not the public resources to allocate. Accordingly, many Asian centers have adopted their own extended inclusion criteria for LDLT for HCC with equivalent long-standing consequences based on HCC tumor burden [99].
7. Re-transplantation for HCC patient: The indications, considerations
HCC recurrence after LT mainly affects the liver graft itself and extrahepatic metastasis, commonly lungs, bone, and lymph nodes [9].
Retransplantation (ReLT) remains the only life-rescuing alternative in case of graft failure. Anyway, in spite of current ameliorations, its survival result was obviously unsatisfactory in comparison with primary LT [100]. According to European Liver Transplant Registry (ELTR) study (1998–2009), HCC recurrence was the indication in only 11% of cases [101].
Utilization of deceased-donor organs is usually justified for graft failure after LDLT. ReLT due to graft failure after LDLT was uncommon, but results are still favorable when required. The panel allowed reLT in LDLT recipients who initially fulfilled accepted criteria for LT. However, based on utility, justice, and equity, they would not support reLT for those previously exceeding these criteria since these patients would have been disqualified for DDLT in that priority. Acceptance reLT for this kind of patients would interfere others on the DDLT wait list and raise an “ethical dilemma” [44, 52]. It is the enigma of the “200% mortality rate” not only this recipient who ultimately diseases from cancer recurrence after transplantation but also other potential candidates, who rather obtain that graft but then advance to liver failure, disqualified from the list or died while waiting [22, 100].
ReLT recipients frequently present higher mean MELD than those of primary LT [102]. The MELD threshold for survival benefit (SB) from ReLT is 21, which is higher than the MELD threshold of 15 for primary LT. The mortality risk or graft failure after ReLT is 3.5–8.3 times higher than those without ReLT for recurrent candidates with MELD <21 [103].
Whereas there is no current agreement, 1-year predictable survival of at least 50% should be considered as effective reLT [100]. Several models for risk-predictor have been suggested so far to help avoid ineffective reLT and to facilitate the best judgment in allocation of organs in short supply. Rosen proposed the most frequently employed risk score for reLT in 1999 and validated in 2003 [104]. This score established three different risk levels (low, medium, and high) based on four predictive components (recipient age, serum bilirubin, serum creatinine, and spell between premier and retransplantation). The 5-year survival was 68%, 62%, and 38% for low, intermediate and high risk, correspondingly. Concerns for this score still remained in recent years because it was developed before the MELD epoch, it does not investigate donor features and diverse recipients risk factors, and it is arithmetic complex [100]. The UCLA group [105] in 2011 developed a new risk stratification scoring that appoints one or two points for preoperative clinical features such as recipient age > 55 years, MELD >27, history of prior reLT, serum albumin <2.5 g/dL, interval of reLT within 15–180 days, necessity of ventilation before reLT, donor age > 45 years and intraoperative features like over-transfusion during reLT (>30 pRBC units). These points are added up to rank recipients into four risk categories (RC). Their 5-year survival was 79, 59, 49, and 22% for RS I, II,III, and IV, respectively, [100].
In general, retransplant in HCC recurrence after LT is not plausible (Recommendation in the Table 11), whereas various provided managements, such as LRT and systemic, have been employed, even in a compound manner, in an effort to extend survival [22].
Evaluation of HCC candidates to access LT
Evidence Level
Strength of recommendation
1. When considering treatment options for HCC patients, the BCLC staging system is the preferred staging system to assess the prognosis of patients with HCC
2b (P)
Strong
2. The TNM system (seventh edn), including pathological examination of the explanted liver, should be used for determining prognosis after transplantation with the addition of assessment of microvascular invasion.
2b (P)
Strong
3. Either dynamic CT or dynamic MRI with the presence of arterial enhancement followed by washout on portal venous or delayed imaging is the best noninvasive test to make a diagnosis in cirrhotic patients suspected of having HCC and for preoperative staging.
1b (D)
Strong
4. Extrahepatic staging should include CT of the chest and CT or MRI of the abdomen and pelvis.
3b (D)
Strong
5. Tumor biopsy is not required in cirrhotic patients considered for liver transplantation who have high-quality dynamic CT or MRI findings typical for HCC and a lesion larger than 1 cm according to current AASLD guidelines.
1b (D)
Weak
6. For patients with lesions smaller or equal to 10 mm, noninvasive imaging does not allow an accurate diagnosis and should not be used to make a decision for or against transplantation.
1b (D)
Strong
Criteria for listing candidates with HCC/liver cirrhosis for DDLT
7. Liver transplantation should be reserved for HCC patients who have a predicted 5-year survival comparable to non-HCC patients.
NA
Weak
8. Preoperative assessment of the size of the largest tumor or total diameter of tumors should be the main consideration in selecting patients with HCC for liver transplantation.
2a (P)
Strong
9. The Milan criteria are currently the benchmark for the selection of HCC patients for liver transplantation, and the basis for comparison with other suggested criteria.
2a (P)
Strong
10. A modest expansion of the number of potential candidates may be considered on the basis of several studies showing comparable survival for patients outside the Milan criteria.
3b P)
Weak
11. Patients with worse prognoses may be considered for liver transplantation outside the Milan criteria if the dynamics of the waiting list allow it without undue prejudice to other recipients with a better prognosis.
NA
Weak
12. α-fetoprotein concentrations add prognostic information in HCC patients and may be used for making decisions regarding transplantation in combination with imaging criteria.
2b (P)
Weak
13. Biomarkers other than α-fetoprotein cannot yet be used for clinical decision-making regarding liver transplantation for HCC
2b (P)
Strong
14. Indication for liver transplantation in HCC should not rely on microvascular invasion because it cannot be reliably detected prior to transplantation.
2b (P)
Strong
Criteria for HCC candidates with non-cirrhotic livers
15. The Milan criteria and its modifications are not applicable to patients with HCC developing in a non-cirrhotic liver. Such patients with non-resectable HCC and absence of macrovascular invasion and extrahepatic spread may be considered as appropriate candidates for liver transplantation.
4 (P)
Weak
16. Patients with HCC in non-cirrhotic liver who were treated by resection, and have intrahepatic recurrence of HCC and no evidence of lymph node or macrovascular invasion, may be considered for salvage transplantation.
4 (P)
Weak
Role of downstaging
17. Transplantation may be considered after successful downstaging.
5 (P)
Weak
18. Liver transplantation after successful downstaging should achieve a 5-year survival comparable to that of HCC patients who meet the criteria for liver transplantation without requiring downstaging.
5 (P)
Strong
19. Criteria for successful downstaging should include tumor size and number of viable tumors.
4 (P)
Strong
20. α-fetoprotein concentrations before and after downstaging may add additional information.
4 (P)
Weak
21. Based on existing evidence, no recommendation can be made for preferring a specific locoregional therapy for downstaging over others.
NA
None
Managing patients on the waiting list
22. Periodic waiting-list monitoring should be performed by imaging (dynamic CT, dynamic MRI, or contrast-enhanced ultrasonography) and α-fetoprotein measurements.
5 (P)
Strong
23. Based on current absence of evidence, no recommendation can be made on bridging therapy in patients with UNOS T1 (≤2 cm) HCC
NA
None
24. In patients with UNOS T2 (one nodule 2–5 cm or three or more nodules each ≤3 cm) HCC (Milan criteria) and a likely waiting time longer than 6 months, locoregional therapy may be appropriate.
4P
Weak
25. No recommendation can be made for preferring any type of locoregional therapy to others.
5 (P)
Strong
26. Patients found to have progressed beyond criteria acceptable for listing for liver transplantation should be placed on hold and considered for downstaging.
5 (P)
Strong
27. Patients with progressive disease in whom locoregional intervention is not considered appropriate, or is ineffective, should be removed from the waiting list.
5 (P)
Strong
Role of LDLT
28. LDLT is acceptable for HCC patients who have an expected 5-year survival similar to comparably staged patients receiving a deceased- donor liver. In LDLT, careful attention should be given to psychosocial considerations regarding both donor and recipient
NA
Weak
29. LDLT must be restricted to centers of excellence in liver surgery and liver transplantation to minimize donor risk and maximize recipient outcome.
NA
Strong
30. In patients following LDLT for HCC within the accepted regional criteria for DDLT, retransplantation for graft failure is justified.
5 (P)
Weak
31. In patients following LDLT for HCC outside the accepted regional criteria for DDLT, retransplantation for graft failure using a deceased- donor organ is not recommended.
5 (P)
Strong
Posttransplant management
32. Post transplant monitoring may include 6–12 monthly contrast-enhanced CT or MRI imaging and α-fetoprotein measurements.
5 (P)
Weak
33. There is currently insufficient evidence from clinical trials to base a recommendation for choosing the type or dose of immunosuppression therapy to influence the incidence of HCC recurrence or its prognosis.
NA
None
34. Based on current evidence, no recommendation can be made on the use of mTOR inhibitors solely to reduce the risk of HCC recurrence outside clinical trials.
NA
None
35. The current evidence does not justify the routine use of adjuvant antitumor therapy after liver transplantation for HCC outside of a controlled clinical trial.
NA
Weak
36. HCC recurrence after liver transplantation may be treated by surgery for resectable lesions or by locoregional therapy or systemic therapy (including sorafenib) for unresectable lesions.
4 (P)
Weak
37. Liver retransplantation is not appropriate treatment for recurrent HCC.
NA
Strong
Table 11.
Recommendations for liver transplantation for HCC: An international consensus conference report in 2010 [44].
Level of evidence for each recommendation refers to the Oxford classification. P = prognosis. D = diagnosis. NA = not applicable.
8. Contraindications of liver transplantation in the HCC patients
Contraindications of LT comprise clinical and psychosocial reasons and could be further defined as liver and non-liver relative and absolute contraindications. Clinically major factors to preclude surgery as severe cardio-pulmonary disorders, ongoing sepsis, widespread portal and visceral venous thrombosis, and progressed or metastatic cancer. Relative contraindications differ between centers and include advanced age or acquired immune deficiency syndrome (AIDS), but this may be individualized considered. Psychosocial contraindications comprise inadequate or without social assistance, unstable psychiatric disorder, ongoing addiction, or limited insurance for post-LT medicaments [106]. Outcomes of LT for HCC can considerably differ between patients with the same morphologic HCC registration criteria; thus, plenty of these contraindications are relative or transitory instead of absolute.
Metastasis out of liver is generally considered an obvious contraindication for LT [6]. To most Western centers, portal vein or hepatic veins macroscopic invasion are absolute contraindications for LT, considering it is the most important and independent risk factor for posttransplant HCC recurrence, and thus for critical diminution in survival [107].
In the US, current UNOS organ distribution strategy [108] defines the following cases to be contraindications to LT and/or will not be provided MELD exception for HCC [5]:
Main portal or hepatic veins macroscopic invasion;
Extrahepatic tumor spread;
Fractured HCC;
Early stage (T1): Resection feasible (solitary tumor <2 cm);
History of HCC steadily cured >2 years ago without recurrence;
Tumor number and size advancement despite LRT; or those who were exceeding conventional inclusion criteria;
Serum AFP consistently >1000 ng/mL and unable to go down below 500.
Similarly in France and Canada, the AFP level ≥ 1000 ng/dL is disqualified to access for DDLT [35, 65].
9. Current recommendations for liver transplantation for HCC
9.1 International consensus conference report in 2010
Though LT is an extensively recognized treatment modality for HCC, arguments still persist and no single guideline was universally approved. An international agreement assembly in Swiss (2010), revised recent practices regarding liver transplantation in HCC and to build globally acknowledged declarations and guidance (Table 11) [44].
9.2 EASL clinical practice guidelines recommendations (2018)
The clinical practice guidelines will be extracted here its recent (2018) advice for the clinical management, particularly relevant to LT for HCC (Table 12).
Recommendations.
LT is recommended as the first-line option for HCC within Milan criteria but unfit to liver resection (evidence high; recommendation strong). Milan criteria are the benchmark for the selection of patients with HCC for LT and the basis for comparison with other suggested criteria.
Agreements on extended criteria for LT in HCC have not been achieved. Patients exceeding Milan criteria can be considered for LT after successful downstaging to fulfill these criteria, within defined protocols (evidence moderate; recommendation weak).
Combination criteria that consider surrogates of tumor biology (AFP) and response to neoadjuvant treatments (bridging or downstaging tumors) together with tumor burden are likely to replace conventional criteria to access LT. Combined criteria should be investigated and determined a priori, validated prospectively, and auditable at any time (evidence low; recommendation strong).
Tumor vascular invasion and extrahepatic metastases are absolute contraindications for LT in HCC (evidence high).
There is no contraindication to use marginal cadaveric grafts for LT in HCC patients (evidence moderate). Prioritizing a cadaveric graft allocation, for patients with or without HCC, within a common waiting list, is complex, and no system can serve all regions. Prioritization criteria for HCC should at least include tumor burden, tumor biology indicators, waiting time, and response to tumor treatment (evidence moderate; recommendation strong).
Transplant benefit may need to be considered alongside the conventional transplant principles of urgency and utility in decision-making, regarding patient selection and prioritization, depending on list composition and dynamics (evidence moderate; recommendation weak).
In LT candidates with HCC, the use of pre-transplant (neoadjuvant) LRT is recommended if feasible as it reduces the risk of pre-LT dropout and aims at reducing post-LT recurrence, particularly when complete or partial tumor response is achieved (evidence low; recommendation strong).
Although the contribution of living donation to LT for HCC in Europe is still marginal, living donor LT for HCC remains an option to be explored in selected patients and in experienced centers, according to waiting list time and dynamics, and within donor-recipient double equipoise principles (evidence low).
Table 12.
EASL clinical practice guidelines recommendations (2018) [6].
9.3 The UNOS 2022 recommendation: Adult MELD exceptions for HCC
LT candidate receives a MELD or a PELD score (if age < 12) for organ distribution. This score reflects the patient’s illness severity by 3-month mortality risk without LT. When the formal score does not express the candidate’s actual medical urgency, their LT program may need an exception score. A candidate fulfills criteria for one of nine diagnoses in policy is permitted for a standardized MELD exception. If the candidate unfits criteria for standardized exception, Review Board should study this request (Table 13) [108].
Principle
Application and considerations
Autonomy
Does the donor have enough information regarding the circumstances of living donation to provide adequate informed consent? Is there “right to donate”? Considerations of donor’s actual motivation for undertaking an LDLT?
Nonmaleficence
How do transplant teams respect the principle of “do no harm” knowing that living donors assume medical risk without any direct medical benefit? How can transplant teams minimize donor risks, with medical and psychosocial complications? [110]
Utility
Assigned to optimization of posttransplant results. Concentrated on posttransplant prognosis with intention to diminish HCC recurrence and extending survival [22]. Despite donor pool improval, should LDLT be inspired, even likely not comparable recipient results?
Urgency
Diminish mortality risk before LT. Typically devoted to non-HCC/cirrhotic patients, with worse short-term outcomes while on the waiting list because of a rapid deterioration of liver function. It is ethical enigma; donated organs are distributed to the “sickest patient first” among non-cancer candidates, but to the “earliest patient first” among HCC candidates for LT, irrespective of their survival prospects with other treatment modalities.
Beneficence
Rating patients with the pure survival benefit and optimization survival gain after LT. Necessity for policy adjustments so as to preclude vain LT or give prioritization to higher risk of recurrence patients.
Equity
Should “social worth” criteria have incorporated into the organ allocation system, hence demanding LDLT consideration?
Table 13.
Application and considering principles of medical ethics in LDLT settings [22, 110].
The main issue in LDLT is donor safety because of the risk of complications or death, even if small. Currently, the reported morbidity and mortality of living donor hepatectomy is 16 and 0.2%, respectively [109]. The concept of “double equipoise” was proposed to describe the balance between the recipient’s survival benefit with LDLT and the risk of a complication or death of a healthy donor [44]. LDLT for patients with HCC is still controversial with the ethical dilemma to risk a healthy person for a recipient that has a fatal disease with a high risk of recurrence.
With obvious benefit of DDLT, LDLT presents ethical challenges as to respect principles of medical ethics, including autonomy, nonmaleficence, beneficence.
11. Conclusions and future directions
Liver malignancies (with HCC in >97% of cases) have become the main indications (40–60%) of liver transplantation (LT) over the last decades.
Anticipation of outcomes in LT for HCC continues to be a challenge. A practical staging system for HCC which is also a powerful predictor for recurrent after LT is yet to be reached with universally acceptance. Tumor biology characters by AFP and PIVKA-II (DCP) should be put on top of tumor morphology.
LT indications for HCC, initially relied on static staging, have converted to a dynamic process comprising treatment-response and tumor biology and should focus on candidates with predicted recurrent-free rate of >70% as with non-HCC patients. This will enable more candidates exceeding MC to access LT while securing their acceptable outcomes.
Inclusion criteria for LT in HCC patients differ between centers and regions. With justified selection, liver transplantation would be a potential management to cure the liver cancer patient, especially in the setting of underlying liver cirrhosis.
LDLT is really an excellent and effective alternative in regions with scarce of deceased-donor organs. Together with ethical issues and the “double equipoise” concept, much consideration should be raised on how far we can expand the LT indication for HCC patients. Especially in the scenario of failure of primary LT on a far advanced HCC patient that requires a retransplant sharing the same donor pool of DDLT as it could obviously negatively impact another candidate that should have received that organ.
Acknowledgments
Thanks to Professor Kim Jong Man (Dept of Surgery, SMC, Sungkyunkwan University School of Medicine, Seoul, Korea) for his kind mentorship and sharing the copyright of material using in this chapter.
References
1.World Health Organization. Global cancer observatory. Available from: https://gco.iarc.fr/. 2022. [Accessed: December 20, 2022]
2.Ziogas IA, Tsoulfas G. The evolution of criteria for liver transplantation for hepatocellular carcinoma: From Milan to San Francisco and all around the world ! Revista de la Facultad de Medicina Humana. 2017;17(3):56-69
3.Arslanoglu A, Seyal AR, Sodagari F, Sahin A, Miller FH, Salem R, et al. Current guidelines for the diagnosis and Management of Hepatocellular Carcinoma: A comparative review. AJR. American Journal of Roentgenology. 2016;207(5):W88-W98. DOI: 10.2214/AJR.15.15490. Epub 2016 Aug 4
4.Maggs JRL, Suddle AR, Aluvihare V, Heneghan MA. Systematic review: The role of liver transplantation in the management of hepatocellular carcinoma. Alimentary Pharmacology & Therapeutics. 2012;35:1113-1134
5.Terrault NA, Francoz C, Berenguer M, Charlton M, Heimbach J. Liver transplantation 2023: Status report, current and future challenges. Clinical Gastroenterology and Hepatology: The Official Clinical Practice Journal of the American Gastroenterological Association. 2023;21(8):2150-2166. DOI: 10.1016/j.cgh.2023.04.005
6.EASL Clinical Practice Guidelines. Management of hepatocellular carcinoma. Journal of Hepatology. 2018;69(1):182-236
7.Mahmud N. Selection for liver transplantation: Indications and evaluation. Current Hepatology Reports. 2020;19:203-212
8.Mazzaferro V, Regalia E, Doci R, Andreola S, Pulvirenti A, Bozzetti F, et al. Liver transplantation for the treatment of small hepatocellular carcinomas in patients with cirrhosis. The New England Journal of Medicine. 1996;334:693-699
9.Duvoux C, Lerut JP. Selection criteria and outcome of liver transplantation for neoplastic liver diseases. In: Burra P, editor. Textbook of Liver Transplantation. Springer: Cham; 2022. pp. 55-72
10.Todo S, Furukawa H, Tada M, Japanese Liver Transplantation Study Group. Extending indication: Role of living donor liver transplantation for hepatocellular carcinoma. Liver Transplantation. 2007;13(11 Suppl. 2):S48-S54
11.Vauthey JN, Dixon E, Abdalla EK, et al. Pretreatment assessment of hepatocellular carcinoma: Expert consensus statement. HPB: The Official Journal of the International Hepato Pancreato Biliary Association. 2010;12(5):289-299
12.Yao FY, Xiao L, Bass NM, Kerlan R, Ascher NL, Roberts JP. Liver transplantation for hepatocellular carcinoma: Validation of the UCSF-expanded criteria based on preoperative imaging. American Journal of Transplantation. 2007;7(11):2587-2596. DOI: 10.1111/j.1600-6143.2007.01965.x
13.Reig M, Forner A, Rimola J, et al. BCLC strategy for prognosis prediction and treatment recommendation: The 2022 update. Journal of Hepatology. 2022;76(3):681-693
14.Yao FY, Ferrell L, Bass NM, Watson JJ, Bacchetti P, Venook A, et al. Liver transplantation for hepatocellular carcinoma: Expansion of the tumor size limits does not adversely impact survival. Hepatology. 2001;33:1394-1403
15.Onaca N, Stone MJ, Fulmer JM, Klintmalm. Transplantation for primary hepatic malignancy. In: Busuttil RW, Klintmalm GBG, editors. Transplantation of the Liver. 3rd ed. Philadelphia: Elsevier Saunders; 2015. pp. 189-204
16.Rich NE, Parikh ND, Singal AG. Hepatocellular carcinoma and liver transplantation: Changing patterns and practices. Current Treatment Options in Gastroenterology. 2017;15:296-304. DOI: 10.1007/s11938-017-0133-3
17.Singal AK, Kamath PS. Management of the patient on the waiting list, scoring systems, and priority. In: Burra P, editor. Textbook of Liver Transplantation. Springer: Cham; 2022. pp. 121-132
18.Halazun KJ, Patzer RE, Rana AA, et al. Standing the test of time: Outcomes of a decade of prioritizing patients with hepatocellular carcinoma, results of the UNOS natural geographic experiment. Hepatology. 2014;60(6):1957-1962
19.Ishaque T, Massie AB, Bowring MG, et al. Liver transplantation and waitlist mortality for HCC and non-HCC candidates following the 2015 HCC exception policy change. American Journal of Transplantation. 2019;19(2):564-572
20.Heimbach JK. Evolution of liver transplant selection criteria and U.S. allocation policy for patients with hepatocellular carcinoma. Seminars in Liver Disease. 2020;40:358-364
21.Azzam AZ. Liver transplantation as a management of hepatocellular carcinoma. World Journal of Hepatology. 2015;7(10):1347-1354
22.Bhoori S, Mazzaferro V. Current challenges in liver transplantation for hepatocellular carcinoma [published correction appears in best Pract res Clin Gastroenterol. 2014 Dec;28(6):1115-6]. Best Practice & Research. Clinical Gastroenterology. 2014;28(5):867-879. DOI: 10.1016/j.bpg.2014.08.001
23.Kim SJ, Kim JM. Prediction models of hepatocellular carcinoma recurrence after liver transplantation: A comprehensive review. Clinical and Molecular Hepatology. 2022;28(4):739-753
24.Bismuth H, Chiche L, Adam R, Castaing D, Diamond T, Dennison A. Liver resection versus transplantation for hepatocellular carcinoma in cirrhotic patients. Annals of Surgery. 1993;218:145-151
25.Herrero JI, Sangro B, Quiroga J, Pardo F, Herraiz M, Cienfuegos JA, et al. Influence of tumor characteristics on the outcome of liver transplantation among patients with liver cirrhosis and hepatocellular carcinoma. Liver Transplantation: Official Publication of the American Association for the Study of Liver Diseases and the International Liver Transplantation Society. 2001;7:631-636. DOI: 10.1053/jlts.2001.25458
26.Roayaie S, Frischer JS, Emre SH, et al. Long-term results with multimodal adjuvant therapy and liver transplantation for the treatment of hepatocellular carcinomas larger than 5 centimeters. Annals of Surgery. 2002;235(4):533-539. DOI: 10.1097/00000658-200204000-00012
27.Kneteman NM, Oberholzer J, Saghier MA, et al. Sirolimus-based immunosuppression for liver transplantation in the presence of extended criteria for hepatocellular carcinoma. Liver Transplantation. 2004;10(10):1301-1311. DOI: 10.1002/lt.20237
28.Onaca N, Davis GL, Goldstein RM, Jennings LW, Klintmalm GB. Expanded criteria for liver transplantation in patients with hepatocellular carcinoma: A report from the international registry of hepatic Tumors in liver transplantation. Liver Transplantation. 2007;13(3):391-399
30.Silva M, Moya A, Berenguer M, et al. Expanded criteria for liver transplantation in patients with cirrhosis and hepatocellular carcinoma. Liver Transplantation. 2008;14(10):1449-1460
31.Mazzaferro V, Llovet JM, Miceli R, et al. Predicting survival after liver transplantation in patients with hepatocellular carcinoma beyond the Milan criteria: A retrospective, exploratory analysis. The Lancet Oncology. 2009;10(1):35-43. DOI: 10.1016/S1470-2045(08)70284-5
32.Toso C, Asthana S, Bigam DL, Shapiro AM, Kneteman NM. Reassessing selection criteria prior to liver transplantation for hepatocellular carcinoma utilizing the scientific registry of transplant recipients database. Hepatology. 2009;49(3):832-838. DOI: 10.1002/hep.22693
33.Lai Q , Avolio AW, Graziadei I, Otto G, Rossi M, Tisone G, et al. Alpha-fetoprotein and modified response evaluation criteria in solid tumors progression after locoregional therapy as predictors of hepatocellular cancer recurrence and death after transplantation. Liver Transplantation. 2013;19(10):1108-1118
34.DuBay D, Sandroussi C, Sandhu L, et al. Liver transplantation for advanced hepatocellular carcinoma using poor tumor differentiation on biopsy as an exclusion criterion. Annals of Surgery. 2011;253(1):166-172
35.Duvoux C, Roudot-Thoraval F, Decaens T, et al. Liver transplantation for hepatocellular carcinoma: A model including alpha-fetoprotein improves the performance of Milan criteria. Gastroenterology. 2012;143:986-994, e3. quiz e14–e15
36.Grąt M, Kornasiewicz O, Lewandowski Z, et al. Combination of morphologic criteria and α-fetoprotein in selection of patients with hepatocellular carcinoma for liver transplantation minimizes the problem of posttransplant tumor recurrence. World Journal of Surgery. 2014;38(10):2698-2707
37.Mehta N, Heimbach J, Harnois DM, et al. Validation of a risk estimation of tumor recurrence after transplant (RETREAT) score for hepatocellular carcinoma recurrence after liver transplant. JAMA Oncology. 2017;3(4):493-500. DOI: 10.1001/jamaoncol.2016.5116
38.Mehta N, Dodge JL, Roberts JP, Yao FY. Validation of the prognostic power of the RETREAT score for hepatocellular carcinoma recurrence using the UNOS database. American Journal of Transplantation. 2018;18(5):1206-1213. DOI: 10.1111/ajt.14549
39.Halazun KJ, Najjar M, Abdelmessih RM, et al. Recurrence after liver transplantation for hepatocellular carcinoma: A new moral to the story. Annals of Surgery. 2017;265(3):557-564
40.Mazzaferro V, Sposito C, Zhou J, Pinna AD, De Carlis L, Fan J, et al. Metroticket 2.0 model for analysis of competing risks of death after liver transplantation for hepatocellular carcinoma. Gastroenterology. 2018;154:128-139
41.Goldberg D, Mantero A, Newcomb C, Delgado C, Forde KA, Kaplan DE, et al. Predicting survival after liver transplantation in patients with hepatocellular carcinoma using the LiTES-HCC score. Journal of Hepatology. 2021;74:1398-1406
42.Bismuth H, Majno PE, Adam R. Liver transplantation for hepatocellular carcinoma. Seminars in Liver Disease. 1999;19:311-322. DOI: 10.1055/s-2007-1007120
43.Pavel MC, Fuster J. Expansion of the hepatocellular carcinoma Milan criteria in liver transplantation: Future directions. World Journal of Gastroenterology. 2018;24(32):3626-3636
44.Clavien PA, Lesurtel M, Bossuyt PM, et al. Recommendations for liver transplantation for hepatocellular carcinoma: An international consensus conference report. The Lancet Oncology. 2012;13(1):e11-e22
45.Sugawara Y, Tamura S, Makuuchi M. Living donor liver transplantation for hepatocellular carcinoma: Tokyo university series. Digestive Diseases. 2007;25(4):310-312. DOI: 10.1159/000106910
46.Lee SG, Hwang S, Moon DB, et al. Expanded indication criteria of living donor liver transplantation for hepatocellular carcinoma at one large-volume center. Liver Transplantation. 2008;14(7):935-945
47.Soejima Y, Taketomi A, Yoshizumi T, et al. Extended indication for living donor liver transplantation in patients with hepatocellular carcinoma. Transplantation. 2007;83(7):893-899
48.Chan SC, Fan ST, Lo CM, et al. A decade of right liver adult-to-adult living donor liver transplantation: The recipient mid-term outcomes. Annals of Surgery. 2008;248(3):411-419
49.Concejero A, Chen CL, Wang CC, et al. Living donor liver transplantation for hepatocellular carcinoma: A single-center experience in Taiwan. Transplantation. 2008;85(3):398-406
50.Taketomi A, Sanefuji K, Soejima Y, et al. Impact of des-gamma-carboxy prothrombin and tumor size on the recurrence of hepatocellular carcinoma after living donor liver transplantation. Transplantation. 2009;87(4):531-537. DOI: 10.1097/TP.0b013e3181943bee
51.Ito T, Takada Y, Ueda M, Haga H, Maetani Y, Oike F, et al. Expansion of selection criteria for patients with hepatocellular carcinoma in living donor liver transplantation. Liver Transplantation. 2007;13:1637-1644
52.Furukawa H, Shimamura T, Suzuki T, et al. Liver transplantation for hepatocellular carcinoma: The Japanese experience. Journal of Hepato-Biliary-Pancreatic Sciences. 2010;17:533-538
53.Yang K, Lee TB, Choi BH, Park YM, Ryu JH, Joo DJ, et al. Development and applicability of the A-P 200 criteria for liver transplantation for hepatocellular carcinoma. Transplantation Proceedings. 2016;48(10):3317-3322. DOI: 10.1016/j.transproceed.2016.08.050
54.Kaido T, Mori A, Ogura Y, et al. Living donor liver transplantation for recurrent hepatocellular carcinoma after liver resection. Surgery. 2012;151(1):55-60. DOI: 10.1016/j.surg.2011.06.032
55.Kim JM, Kwon CH, Joh JW, et al. Expanded criteria for liver transplantation in patients with hepatocellular carcinoma. Transplantation Proceedings. 2014;46(3):726-729
56.Hong G, Suh KS, Suh SW, et al. Alpha-fetoprotein and (18)F-FDG positron emission tomography predict tumor recurrence better than Milan criteria in living donor liver transplantation. Journal of Hepatology. 2016;64(4):852-859. DOI: 10.1016/j.jhep.2015.11.033
57.Lee JH, Cho Y, Kim HY, et al. Serum tumor markers provide refined prognostication in selecting liver transplantation candidate for hepatocellular carcinoma patients beyond the Milan criteria. Annals of Surgery. 2016;263(5):842-850. DOI: 10.1097/SLA.0000000000001578
58.Lee EC, Kim SH, Shim JR, Park SJ. Small-for-size grafts increase recurrence of hepatocellular carcinoma in liver transplantation beyond Milan criteria. Liver Transplantation. 2018;24(1):35-43
59.Shimamura T, Akamatsu N, Fujiyoshi M, et al. Expanded living-donor liver transplantation criteria for patients with hepatocellular carcinoma based on the Japanese nationwide survey: The 5-5-500 rule - A retrospective study. Transplant International. 2019;32(4):356-368
60.Vibert E, Azoulay D, Hoti E, Iacopinelli S, Samuel D, Salloum C, et al. Progression of alphafetoprotein before liver transplantation for hepatocellular carcinoma in cirrhotic patients: A critical factor. American Journal of Transplantation. 2010;10:129-137
61.Notarpaolo A, Layese R, Magistri P, Gambato M, Colledan M, Magini G, et al. Validation of the AFP model as a predictor of HCC recurrence in patients with viral hepatitis-related cirrhosis who had received a liver transplant for HCC. Journal of Hepatology. 2017;66(3):552-559
62.Varona MA, Soriano A, Aguirre-Jaime A, Garrido S, Oton E, Diaz D, et al. Risk factors of hepatocellular carcinoma recurrence after liver transplantation: Accuracy of the alpha-fetoprotein model in a single-center experience. Transplantation Proceedings. 2015;47(1):84-89
63.Piñero F, Tisi Baña M, de Ataide EC, Hoyos Duque S, Marciano S, Varón A, et al. Liver transplantation for hepatocellular carcinoma: Evaluation of the alpha-fetoprotein model in a multicenter cohort from Latin America. Liver International. 2016;36(11):1657-1667
64.Cillo U, Vitale A, Bassanello M, et al. Liver transplantation for the treatment of moderately or well-differentiated hepatocellular carcinoma. Annals of Surgery. 2004;239(2):150-159
65.Sapisochin G, Goldaracena N, Laurence JM, et al. The extended Toronto criteria for liver transplantation in patients with hepatocellular carcinoma: A prospective validation study. Hepatology. 2016;64:2077-2088
66.Decaens T, Roudot-Thoraval F, Badran H, et al. Impact of tumour differentiation to select patients before liver transplantation for hepatocellular carcinoma. Liver International. 2011;31(6):792-801
67.Lin C-C, Elsarawy AMAA, Chen C-L. Living Donor Liver Transplantation for Hepatocellular Carcinoma. London, UK: InTechOpen; 2017. DOI: 10.5772/65109
68.Hsu C-C, Chen C-L, Wang C-C, Lin C-C, Yong C-C, Wang S-H, et al. Combination of FDG-PET and UCSF criteria for predicting HCC recurrence after living donor liver transplantation. Transplantation. 2016;100(9):1925-1932
69.Chalaye J, Costentin CE, Luciani A, et al. Positron emission tomography/computed tomography with 18F-fluorocholine improve tumor staging and treatment allocation in patients with hepatocellular carcinoma. Journal of Hepatology. 2018;69(2):336-344
70.Meischl T, Rasoul-Rockenschaub S, Györi G, et al. C-reactive protein is an independent predictor for hepatocellular carcinoma recurrence after liver transplantation. PLoS One. 2019;14(5):e0216677. DOI: 10.1371/journal.pone.0216677 [Accessed: May 29, 2019]
71.Kornberg A, Witt U, Schernhammer M, et al. The role of preoperative albumin-bilirubin grade for oncological risk stratification in liver transplant patients with hepatocellular carcinoma. Journal of Surgical Oncology. 2019;120(7):1126-1136. DOI: 10.1002/jso.25721
72.Firl DJ, Sasaki K, Agopian VG, et al. Charting the path forward for risk prediction in liver transplant for hepatocellular carcinoma: International validation of HALTHCC among 4,089 patients. Hepatology. 2020;71(2):569-582. DOI: 10.1002/hep.30838
73.Aloia TA, Adam R, Samuel D, Azoulay D, Castaing D. A decision analysis model identifies the interval of efficacy for transarterial chemoembolization (TACE) in cirrhotic patients with hepatocellular carcinoma awaiting liver transplantation. Journal of Gastrointestinal Surgery. 2007;11:1328-1332
74.Kollmann D, Selzner N, Selzner M. Bridging to liver transplantation in HCC patients. Langenbeck's Archives of Surgery. 2017 Sep;402(6):863-871. DOI: 10.1007/s00423-017-1609-2
75.Lai Q , Avolio AW, Manzia TM, Sorge R, Agnes S, Tisone G, et al. Combination of biological and morphological parameters for the selection of patients with hepatocellular carcinoma waiting for liver transplantation. Clinical Transplantation. 2012;26(2):E125-E131
76.Yao FY, Mehta N, Flemming J, et al. Downstaging of hepatocellular cancer before liver transplant: Long-term outcome compared to tumors within Milan criteria. Hepatology. 2015;61(6):1968-1977
77.Mehta N. Liver transplantation criteria for hepatocellular carcinoma, including Posttransplant management. Clinics in Liver Disease. 2021;17(5):332-336. Published 2021 Jun 4. DOI: 10.1002/cld.1054
78.Ravaioli M, Grazi GL, Piscaglia F, et al. Liver transplantation for hepatocellular carcinoma: Results of down-staging in patients initially outside the Milan selection criteria. American Journal of Transplantation. 2008;8(12):2547-2557
79.Lai Q , Nicolini D, Inostroza Nunez M, et al. A novel prognostic index in patients with hepatocellular cancer waiting for liver transplantation: Time-radiological-response-alpha-fetoprotein-INflammation (TRAIN) score. Annals of Surgery. 2016;264(5):787-796
80.Mazzaferro V, Citterio D, Bhoori S, et al. Liver transplantation in hepatocellular carcinoma after tumour downstaging (XXL): A randomised, controlled, phase 2b/3 trial [published correction appears in lancet Oncol. 2020 Aug;21(8):e373]. The Lancet Oncology. 2020;21(7):947-956
81.Heimbach JK, Kulik LM, Finn RS, et al. AASLD guidelines for the treatment of hepatocellular carcinoma. Hepatology. 2018;67(1):358-380. DOI: 10.1002/hep.29086
82.Graziadei IW, Sandmueller H, Waldenberger P, Koenigsrainer A, Nachbaur K, Jaschke W, et al. Chemoembolization followed by liver transplantation for hepatocellular carcinoma impedes tumor progression while on the waiting list and leads to excellent outcome. Liver Transplantation. 2003;9:557-563. DOI: 10.1053/jlts.2003.50106
83.Otto G, Herber S, Heise M, et al. Response to transarterial chemoembolization as a biological selection criterion for liver transplantation in hepatocellular carcinoma. Liver Transplantation. 2006;12(8):1260-1267. DOI: 10.1002/lt.20837
84.Millonig G, Graziadei IW, Freund MC, Jaschke W, Stadlmann S, Ladurner R, et al. Response to preoperative chemoembolization correlates with outcome after liver transplantation in patients with hepatocellular carcinoma. Liver Transplantation. 2007;13:272-279
85.Chapman WC, Majella Doyle MB, Stuart JE, et al. Outcomes of neoadjuvant transarterial chemoembolization to downstage hepatocellular carcinoma before liver transplantation. Annals of Surgery. 2008;248(4):617-625
86.Lewandowski RJ, Kulik LM, Riaz A, et al. A comparative analysis of transarterial downstaging for hepatocellular carcinoma: Chemoembolization versus radioembolization. American Journal of Transplantation. 2009;9(8):1920-1928
87.De Luna W, Sze DY, Ahmed A, et al. Transarterial chemoinfusion for hepatocellular carcinoma as downstaging therapy and a bridge toward liver transplantation. American Journal of Transplantation. 2009;9(5):1158-1168
88.Jang JW, You CR, Kim CW, et al. Benefit of downsizing hepatocellular carcinoma in a liver transplant population. Alimentary Pharmacology & Therapeutics. 2010;31(3):415-423. DOI: 10.1111/j.1365-2036.2009.04167.x
89.Pommergaard HC, Rostved AA, Adam R, et al. Locoregional treatments before liver transplantation for hepatocellular carcinoma: A study from the European liver transplant registry. Transplant International. 2018;31(5):531-539. DOI: 10.1111/tri.13123
90.Ogawa K, Kaido T, Okajima H, et al. Impact of pretreatments on outcomes after living donor liver transplantation for hepatocellular carcinoma. Journal of Hepato-Biliary-Pancreatic Sciences. 2019;26(2):73-81
91.Mehta N, Dodge JL, Roberts JP, Hirose R, Yao FY. Alpha-fetoprotein decrease from > 1,000 to < 500 ng/mL in patients with hepatocellular carcinoma leads to improved Posttransplant outcomes. Hepatology. 2019;69(3):1193-1205
92.Sinha J, Mehta N, Dodge JL, Poltavskiy E, Roberts J, Yao F. Are there upper limits in tumor burden for down-staging of hepatocellular carcinoma to liver transplant? Analysis of the all-comers protocol. Hepatology. 2019;70(4):1185-1196
93.Vutien P, Dodge J, Bambha KM, et al. A simple measure of hepatocellular carcinoma burden predicts tumor recurrence after liver transplantation: The recurrent hepatocellular carcinoma-initial, maximum, last classification. Liver Transplantation. 2019;25(4):559-570
94.DiNorcia J, Florman SS, Haydel B, et al. Pathologic response to Pretransplant Locoregional therapy is predictive of patient outcome after liver transplantation for hepatocellular carcinoma: Analysis from the US Multicenter HCC transplant consortium. Annals of Surgery. 2020;271(4):616-624
95.Fisher RA, Kulik LM, Freise CE, Lok AS, Shearon TH, Brown RS Jr, et al. Hepatocellular carcinoma recurrence and death following living and deceased donor liver transplantation. American Journal of Transplantation. 2007;7(6):1601-1608
96.Liang W, Wu L, Ling X, et al. Living donor liver transplantation versus deceased donor liver transplantation for hepatocellular carcinoma: A meta-analysis. Liver Transplantation. 2012;18(10):1226-1236. DOI: 10.1002/lt.23490
97.Cauley RP, Potanos K, Fullington N, et al. The effect of graft type on mortality in liver transplantation for hepatocellular carcinoma. Annals of Transplantation. 2015;20:175-185. Published 2015 Mar 30. DOI: 10.12659/AOT.892613
98.Kim KH, Park JI. Living-related liver transplantation. In: Burra P, editor. Textbook of Liver Transplantation. Vol. 2022. Switzerland AG: Springer, Champions; 2022. pp. 203-218
99.Lee HW, Suh KS. Expansion of the criteria for living donor liver transplantation for hepatocellular carcinoma. Current Opinion in Organ Transplantation. 2016;21(2):231-237
100.Cillo U, Bertacco A. Liver Retransplantation. In: Burra P, editor. Textbook of Liver Transplantation. Cham: Springer; 2022. DOI: 10.1007/978-3-030-82930-8_24
101.Adam R, Karam V, Delvart V, O’Grady J, Mirza D, Klempnauer J, et al. Evolution of indications and results of liver transplantation in Europe. A report from the European liver transplant registry (ELTR). Journal of Hepatology. 2012;57:675-688
102.Kim HJ, Larson JJ, Lim YS, et al. Impact of MELD on waitlist outcome of retransplant candidates. American Journal of Transplantation. 2010;10(12):2652-2657
103.Biggins SW, Gralla J, Dodge JL, et al. Survival benefit of repeat liver transplantation in the United States: A serial MELD analysis by hepatitis C status and donor risk index. American Journal of Transplantation. 2014;14(11):2588-2594. DOI: 10.1111/ajt.12867
104.Rosen HR, Prieto M, Casanovas-Taltavull T, et al. Validation and refinement of survival models for liver retransplantation. Hepatology. 2003;38(2):460-469
105.Hong JC, Kaldas FM, Kositamongkol P, et al. Predictive index for long-term survival after retransplantation of the liver in adult recipients: Analysis of a 26-year experience in a single center. Annals of Surgery. 2011;254(3):444-448; discussion 448-9
106.Pomposelli JJ, Simpson MA, Simon C, Pomfret EA. Liver transplantation. In: JLR F, editor. Transplantation. 5th ed. New York, Oxford: Saunders Elsevier; 2014. pp. 127-148
107.Andreou A, Bahra M, Schmelzle M, Öllinger R, Sucher R, Sauer IM, et al. Predictive factors for extrahepatic recurrence of hepatocellular carcinoma following liver transplantation. Clinical Transplantation. 2016;30:819-827
108.Organ Procurement and Transplantation Network. UNOS Organ Allocation policy. 2023. Available from: https://optn.transplant. hrsa.gov/media/2846/liver_guidance_hcc_201706.pdf. [Accessed: December 28, 2022]
109.Ince V, Sahin TT, Akbulut S, Yilmaz S. Liver transplantation for hepatocellular carcinoma: Historical evolution of transplantation criteria. World Journal of Clinical Cases. 2022;10(29):10413-10427
110.Nizamuddin I, Gordon EJ, Levitsky J. Ethical issues when considering liver donor versus deceased donor liver transplantation. Clinical Liver Disease (Hoboken). 2021;17(2):71-74. DOI: 10.1002/cld.982 [Accessed: February 28, 2021]
Written By
Nam Hoang Duc
Submitted: 23 September 2023Reviewed: 30 September 2023Published: 05 April 2024